")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Features and Antibiotic Treatment of Neonatal Listeriosis: A Hospital-Based Study
Authors Zhang S , Li J, Wan L, Yu J, Chen S, Jin Z
Received 15 August 2023
Accepted for publication 4 October 2023
Published 11 October 2023 Volume 2023:16 Pages 6647—6659
DOI https://doi.org/10.2147/IDR.S431402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Shasha Zhang,1,* Jinchun Li,2,* Li Wan,1 Jing Yu,2 Sumei Chen,2 Zhengjiang Jin3
1Department of Pharmacy, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China; 2Department of Neonatology, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China; 3Department of Clinical Laboratory, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhengjiang Jin, Department of Clinical Laboratory, Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430070, People’s Republic of China, Email [email protected]
Purpose: To determine the clinical features, laboratory findings, antibiotic treatment, and outcomes of neonatal listeriosis in a specialized tertiary hospital in Wuhan, China.
Patients and Methods: We retrospectively analyzed the medical records of patients diagnosed with neonatal listeriosis at Maternal and Child Health Hospital of Hubei Province from January 2015 to December 2022. Listeriosis was indicated by positive culture for Listeria monocytogenes (LM).
Results: A total of 11 cases were included in our study. The incidence rate of neonatal listeriosis was 2.06 per 100,000 live births. Seventy-three percent of the cases were born prematurely, caused early onset sepsis. Respiratory distress (100%) was the most common and earliest symptom, followed by fever (64%) and rashes (27%). The levels of C-reactive protein (CRP) and procalcitonin (PCT) were elevated in 100% of the cases. The median time-to-positivity (TTP) of the culture was 15 hours (range 9– 28hours). Of the 11 neonates, 6 were cured, 2 showed improvement, and 3 died, with a mortality rate of 27%. There were statistically significant differences in Apgar score at 5 minutes (p=0.037) and CRP (p=0.025) between the survival group and fatality group. Ampicillin was sensitive to LM isolates and effective for therapy if initiated early.
Conclusion: Neonatal listeriosis is a rare but severe infection with a high mortality rate. Early identification and appropriate use of effective antibiotics are particularly critical for achieving positive outcomes. Apgar score and CRP are relevant indices for prognosis. Ampicillin is the first-line therapy and can be empirically administered to neonates suspected of having listeriosis.
Keywords: neonatal listeriosis, Listeria monocytogenes, clinical features, antibiotic treatment, Apgar score, C-reactive protein
Introduction
Listeria monocytogenes (LM) is a Gram-positive motile facultative anaerobe, which can be readily isolated from soil, water, and vegetation, including raw produce designated for human consumption without further processing.1,2 LM is responsible for listeriosis, an uncommon disease, but considered as the most severe foodborne infection in the European Union in terms of death and hospitalization.3 Listeriosis is predominantly affects immunocompromised individuals, such as the elderly, pregnant women and neonates.4
As an emerging infection of public health concern, many European countries and the United States have established monitoring systems of listeriosis and reported a lot.5–10 A prospective cohort study in France highlighted more serious outcomes of listeriosis than had been reported to date, with greater than 80% of infected mothers experiencing major fetal or neonatal complications.7 Neonatal listeriosis, which primarily occurs via congenital infection through vertical transmission by affected pregnancies,9 can result in sepsis and meningitis, with the highest mortality rate among human listeriosis, reaching up to 30% even in developed countries.7,11,12
Due to inadequate attention and so on, the incidence of listeriosis in Asia is lower.13 Actually, more emphasis on listeriosis should be placed in Asian countries. It was reported that Asians and Afro-Caribbean women had a disproportionally higher representation in the listeriosis population than Caucasian in England.9 Another study showed that higher rate ratios for listeriosis were found among non-Hispanic blacks and Asians compared to non-Hispanic whites in the United States.14 Evidences suggest that ethnicity is a significant risk factor for listeriosis, and Asian was one of the races with higher morbidity.
Therefore, the number of the listeriosis patients in China may be seriously underestimated. In 2019, Chinese scholars reported that perinatal listeriosis accounted for over 50% of all LM infections, leading to adverse outcomes such as miscarriage, stillbirth, and premature birth, as it is transmitted vertically through the placenta.15 Severe infections often occur in surviving newborns, with a mortality rate ranging from 20% to 46%, making it a significant contributor to neonatal mortality.15,16 Early identification and effective treatment are key to improving the prognosis. But there was limited data on neonatal listeriosis in China due to the absence of a nationwide surveillance. To enhance clinical comprehension and management of this disease, we conducted an analysis of the medical records of neonatal listeriosis patients over an 8-year period at a leading tertiary specialist hospital with the largest neonatology department in Hubei Province, China.
Materials and Methods
Research Object
We retrospectively analyzed the medical records of the patients, who admitted to the Department of Neonatology and confirmed neonatal listeriosis at the Maternal and Child Health Hospital of Hubei Province, in Wuhan, China. This hospital has a 200-bed neonatal intensive care unit. The study period was from January 2015 to December 2022. The neonatal period is defined as commencing on the birth date and ending 28 complete days after birth. Listeriosis was indicated by positive Listeria monocytogenes culture in sterile sites, usually blood or cerebrospinal fluid.
Study Design
We collected neonatal details including patient source, demographic characteristics, Apgar score, symptoms, supportive care, body temperature, laboratory findings, culture source, antibiotics therapy, hospital stay, diagnosis and clinical outcomes. Maternal medical records were also reviewed, including age, perinatal factors, delivery mode, laboratory findings, pre-delivery antibiotics, and concomitant diseases.
The incidence rate of neonatal listeriosis was calculated using the number of confirmed neonates born at our hospital as the numerator over the 8-year study period. The number of live births at the hospital during the same period is used as the denominator.
Microbiological Analysis
Microbial culture and identification were conducted according to routine diagnostic standard operating procedures used in the clinical laboratory of this study hospital: 1–3 mL of blood or cerebrospinal fluid was collected from neonates with suspected cases of sepsis, and this sample was cultured using an automated BacT/ALERT 3D system or BD BACTEC™ system. Incubation was continued until positive results were observed or for up to 5 days. Positive cultures were subcultured and identified to the species level by matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS; Bruker Daltonics, Germany). Antimicrobial susceptibility assays of all isolates were performed by using broth dilution method. The minimum inhibitory concentrations (MICs) of 5 antimicrobials were tested, including penicillin, ampicillin, cotrimoxazole, erythromycin and meropenem. And the MIC results were interpreted using the guidelines of the Clinical and Laboratory Standards Institute (CLSI) (Third Edition: M45).
Time-to-positivity (TTP) was defined as the time from blood culture collection to the time organism growth was reported by the microbiology laboratory at our hospital.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0. The measurement data conformed normal distribution were presented as mean ± standard deviation (SD) and compared using independent samples t-test. Non-parametric data were presented as median (minimum, maximum) and compared using the Mann–Whitney test. The enumeration data were described as n (%) and chi-squared tests were used for comparisons. The results were considered statistically significant at a two-tailed P-value of less than 0.05. Kaplan-Meier (K-M) curves were created by GraphPad 6.0.
Results
Incidence of Neonatal Listeriosis
A total of 11 confirmed cases of neonatal listeriosis were included in our study. As the neonatal emergency transport center of Hubei Province, 64% (7/11) of the cases were transferred from other hospitals, while 36% (4/11) were delivered in the Department of Obstetrics. Among 194,489 deliveries, the incidence rate was 2.06 per 100,000 live births.
The year and month distributions of neonatal listeriosis cases in our hospital are shown in Figures 1 and 2. The number of cases peaked at 2017 (5 cases), and then remained at the level of 1 case per year. Infections occurred in almost all seasons.
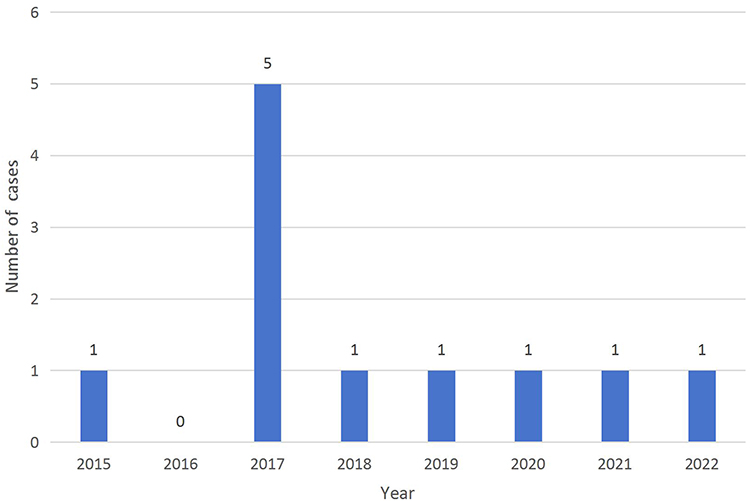 |
Figure 1 The year distribution of neonatal listeriosis cases. |
 |
Figure 2 The month distribution of neonatal listeriosis cases. |
Features of Neonatal Cases
The features of the 11 confirmed neonatal listeriosis cases are presented in Table 1 and Table 2. 73% (8/11) of the cases were born prematurely, with a median gestational age of 33.1 weeks (range 29.4–39.1 weeks). The median birth weight was 2000g (range 1100–3650g). The median Apgar score (5th minute) was 8 (range 6–10). 100% (11/11) of the cases showed signs of respiratory distress, which was the most common and earliest symptom. In addition, fever was present in 64% (7/11) of cases, and rashes were observed in 27% (3/11) of cases. Invasive ventilation was given to 64% (7/11) neonates, non-invasive ventilation to 18% (2/11), and high-flow nasal cannula to the remainder. 45% (5/11) cases received pulmonary surfactant, while 64% (7/11) cases taken the inotropic support to against shock.
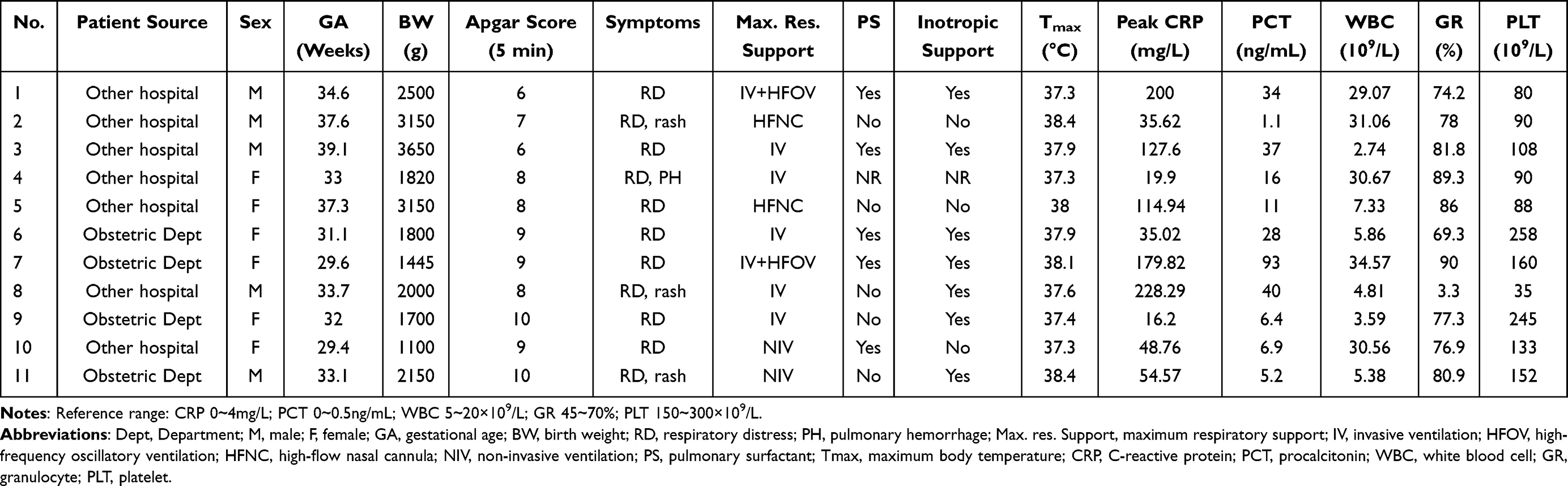 |
Table 1 Features of Neonatal Cases-1 |
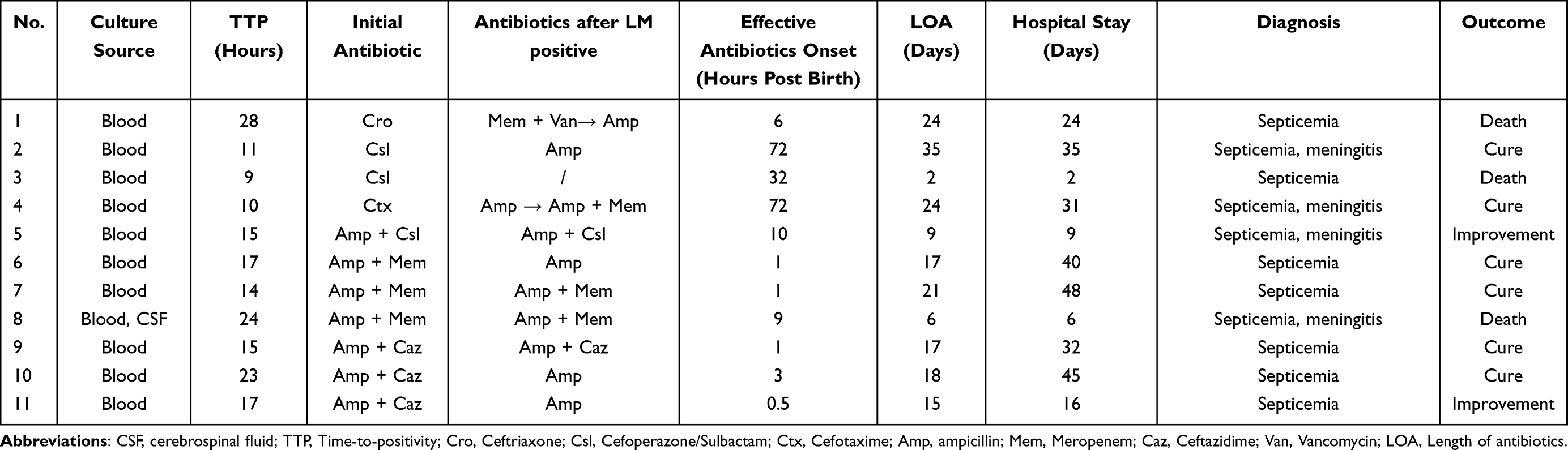 |
Table 2 Features of Neonatal Cases-2 |
In terms of laboratory findings, an increase of C-reactive protein (CRP) and procalcitonin (PCT) was present in 100% (11/11) of the cases. However, there was a wide variation in peripheral white blood cell (WBC) counts, ranging from 2.74 to 34.57. The proportion of granulocyte (GR) showed upward trend in 91% (10/11) cases, except Case 8. Platelet (PLT) counts were usually normal or decreased.
LM was isolated from the blood of all cases and diagnosed with early-onset sepsis. The median TTP of culture is 15 hours (range 9–28hours). Except for Case 3, all of the other neonates underwent lumbar punctures, and 4 of them were diagnosed with meningitis as well. The cerebrospinal fluid (CSF) culture of one case is positive (Case 8), and 3 cases showed a high polymorphonuclear leukocyte count (WCC ≥ 20 cells/mm3).
Antibiotic Treatment of Neonatal Cases
Empirical antibiotic therapy was administered in all cases. Cases 1–4 were treated with a third-generation cephalosporin alone, while cases 5–11 were treated with ampicillin in combination with meropenem or a third-generation cephalosporin. After LM isolation, the antibiotic treatment of Cases 1, 2, and 4 was adjusted, while Cases 5–11 were either left unchanged or de-escalated to ampicillin alone. Case 3 died before the culture results were available. The median time for administration of effective antibiotics was 6 hours (range 0.5–72hours). Results of sensitivity tests on 12 clinical isolates (2 from Case 8, obtained from blood and CSF respectively) of LM showed 100% sensitivity to penicillin, ampicillin, cotrimoxazole, erythromycin, and meropenem. The median length of antibiotic treatment was 17 days, compared to a median hospital stay of 31 days. Of the 11 neonates, 6 were cured, 2 showed improvement, and 3 died, with a mortality rate of 27%.
Comparison Between the Survival and Fatal Neonatal Cases
We divided the 11 neonates into two groups based on prognosis: 8 in the survival group and 3 in the fatal group. The features of both groups, including neonatal and maternal, are listed in Table 3. We compared them to identify prognostic factors for neonatal listeriosis. There was a statistically significant difference in Apgar score at 5 minutes (p = 0.037) and CRP (p = 0.025) between the two groups.
 |
Table 3 Comparison Between the Survival and Fatal Cases of Neonatal Listeriosis |
We continuously monitored the CRP levels of each neonate and recorded the day on which the CRP inflection point was observed, as well as the day it returned to normal. According to the Kaplan-Meier (K-M) curves shown in Figure 3, we found that the median time for the CRP inflection point in neonatal listeriosis is 3 days, and the median time for CRP back to normal is 7 days.
 |
Figure 3 Kaplan-Meier (K-M) curves of CRP. (A) K-M curve between event-free fraction of CRP inflection point and the days post birth. The occurrence of the CRP inflection point in each neonate with listeriosis was considered an event. As the days increase, the number of neonates with peak CRP levels also increased, while the fraction of event-free neonates gradually decreased. (B) K-M curve between event-free fraction of CRP back to normal and the days post birth. The occurrence of the CRP back to normal in each neonate with listeriosis was considered an event. As the days increased, the number of neonates with normal CRP levels also increased, while the fraction of event-free neonates gradually decreased. |
Features of Maternal Cases
An overview of the relevant maternal cases is summarized in Table 4. The median maternal age was 30 years (range 22–38years). All mothers had non-specific clinical manifestations before delivery: fever in 45% (5/11) cases, premature rupture of membranes in 36% (4/11) cases, abdominal pain in 18% (2/11) cases, and reduced fetal movement in 18% (2/11) cases. One mother (Case 1) was treated with antibiotics since she had a fever for 3 days.
 |
Table 4 Features of Maternal Cases |
Case 4 gave birth to a twin, whereas the other twin died in utero. The left 10 were singletons. 8 of the neonates were delivered by caesarean section and the other were delivered vaginally. In 45% (5/11) of the cases, there was intrauterine distress, and in 73% (8/11) of the cases, there was meconium-stained liquor.
Of the 4 mothers who gave birth at our hospital, 3 had elevated prenatal WBC counts and GR ratios. Case 6 was diagnosed with chorioamnionitis and had a positive blood culture for LM after delivery. Case 11 was clinically diagnosed with septicemia. Cases 7 and 9 were discharged without any symptoms of LM infection after receiving routine antibiotic prophylaxis following delivery. The follow-up of other 7 mothers were unknown.
Discussion
Listeriosis is a sporadic disease, occasionally outbreaks mostly related to LM contaminated food. In our study, all the cases occurred sporadically. Yu-Lin Tai et al reported an increase trend in incidence of neonatal listeriosis in Taiwan, from 0.94/10,000 neonatal admissions during 2000–2011 to 5.45/10,000 during 2012–2018.17 However, an opposite trend was reported in the UK, with the rate decreasing from 3.4/100,0009 to 1.8/100,000.12 In our study, the incidence of neonatal listeriosis was 2.06 per 100,000 live births, which is relatively low compared to the incidence mentioned above. Strict criteria to exclude suspected cases may have resulted in an underestimation of the incidence of neonatal listeriosis.
In immunocompetent individuals, listeriosis can present as a self-limited gastroenteritis.4 Pregnant women are at a high risk of infection, probably because of the impaired cell-mediated immune response and the decreased gastrointestinal motility.18,19 Sporadic listeriosis appears to be more common in spring and summer, with higher-risk products eaten in the warmer months.1 In our study, there was insufficient data to determine the predominant months or seasons, and the connection between pregnancy-associated listeriosis and food consumption was unclear.
LM infection rarely leads to maternal death; some cases may even be asymptomatic,2 which increasing the difficulty of therapy. Infected pregnant women may commonly have flu-like or pyelonephritis symptoms before the early onset of labor. Fever is the most common clinical manifestation, with a rate of 65–81%.2 Some mothers may be aware of reduced fetal movement and noticeable uterine contractions, or symptoms of threatened preterm birth, inclusive of abdominal pain, vaginal bleeding, or premature rupture of membranes.2 In our study, most of the mothers had non-specific symptoms during the prenatal period. Fever was the most common symptom, followed by premature rupture of membranes, abdominal pain, and reduced fetal movement, as reported in the literature. Meconium-stained liquor is often observed in mothers with listeriosis,17 and it was also present in 72% of the cases we studied.
Maternal infection with LM could lead to chorioamnionitis or meconium-stained amniotic fluid during delivery.2,10 Sometimes, symptoms resolve after delivery spontaneously.20 In our study, 50% of the 4 mothers who gave birth at our hospital were confirmed to have infectious diseases, while the others were discharged without any signs of infection.
It has been reported that early treatment of the mothers with LM infection is useful to prevent transplacental infection or treat the fetus in utero, and give birth to an uninfected baby.21 However, nonspecific symptoms and no-significant maternal risk factors make it difficult for obstetricians to recognize pregnancy-related listeriosis in advance.22 Similarly, in our study, less than 10% of mothers were treated with antibiotics before delivery, and the dosage was unknown.
Neonatal listeriosis occurs as a result of maternal chorioamnionitis or through passage through a birth canal colonized with Listeria from the gastrointestinal tract,1 which can be extremely severe. It is crucial for neonatologists to familiarize themselves with the related information on neonatal listeriosis due to latent bad outcomes and high mortality rate, even with treatment.23 Sisi Chen et al reported that the fatality rate of listeriosis was highest among neonates (23%) in mainland China, between 2008 and 2017, based on literature reviews.6 We have the similar mortality rate of 27%.
Neonatal listeriosis is the third most common cause of early-onset neonatal infection and the fourth most common cause of early-onset neonatal meningitis in the UK.9 Late-onset listeriosis is less common than early-onset disease.3 In our study, all cases were early-onset infection within the first 72 hours of life. Prematurity, fever, a diffuse maculopapular cutaneous eruption, and significant hepatic involvement with jaundice are all the characteristic clinical features of LM infected neonates.20 Most of our cases were born prematurely, and all cases occurred in the third trimester (29–40 weeks). Respiratory distress was observed in all cases, and the majority of them required invasive ventilation support. Typical rashes may facilitate early diagnosis of listeriosis, which were observed in 3 of our cases.
As an index to assess early neonatal condition, Apgar score has been routinely used worldwide for more than 60 years. Some studies proved that low Apgar score at 5 minutes was associated with an increased risk of neonatal death, across all gestational strata.24,25 The same conclusion was observed in our study. In the absence of significant differences in gestational age, Apgar score at 5 minutes was lower in the fatality group than in the survival group.
Laboratory findings, such as complete blood counts (CBCs) with differential, CRP, and PCT are most frequently used as sepsis biomarkers before culture results are obtained.26 Nevertheless, no statistically significant differences were observed in the comparison between the survival and fatal groups in terms of WBC counts, GR ratios, and PLT counts, except for CRP. WBC counts and absolute neutrophil counts (ANC) were more informative when they were low, rather than elevated, in association with increased odds of early-onset sepsis, whereas PLT counts showed less sensitivity and specificity.27 Serum CRP and PCT are two of the most thoroughly investigated laboratory markers, with elevations in all cases. CRP was considered to be an independently predictor of a positive blood culture and had the potential to guide the discontinuation of antibiotic therapy in studies of neonatal suspected sepsis.28 In our study, CRP levels reach their highest point at 3 days for neonatal listeriosis, similar to other bacterial infections. The median time for CRP to return to normal was 7 days, which was consistent with the median length of treatment (LOT) reported in the literature for neonatal sepsis.29 Compared to CRP, PCT was not continuously monitored due to the limitation of neonatal blood volume, which may partially explain the lack of statistical difference between the two groups. We also found that TTP was within 36 hours in all cases. This supports the same conclusion as a previous study, which found that 94% of pathogens could be identified within 36 hours of blood culture collection in neonatal early-onset sepsis.30
As for the therapy of neonatal listeriosis, antibiotics remain the cornerstone, and prompt administration is undoubtedly important, relevant to prevent complications, death, and long-lasting sequelae.2,31,32 The β-lactam antibiotics penicillin and aminopenicillins (ampicillin or amoxicillin) are the first-choice treatment, in combination with an aminoglycoside or not. Cephalosporin, fosfomycin and fluoroquinolones are resistant to LM because of lack or low affinity of enzyme catalyzing the final step of cell wall synthesis.23 In our study, Cases 1–4 were treated with cephalosporin initially, delayed the effective antibiotic onset time, with the consequence of death or combination of meningitis. In case 5 and 8, although ampicillin was chosen as the first choice before the positive culture results, they were transferred from other hospitals with a relatively late antibiotic onset time, receptively 10 and 9 hours after birth, which leading to meningitis as well. Due to the limitations of neonatal medication in China, aminoglycoside antibiotics were not used in all cases. No antibiotic resistance against first-line treatments of neonatal listeriosis was observed in our study. Ampicillin was proved to be effective in survival group with 100% sensitivity in culture. A change in the neonatal antibiotic medication strategy starting from 2017 in our hospital, using ampicillin alone or in combination with ceftazidime as the first-line empiric option, significantly improved neonatal listeriosis outcomes, as indicated by a reduction in the incidence of meningitis and an increase in the cure rate. Given the low positive culture rate but high mortality rate, we recommend immediate antibiotics with relevant safety profiles, such as penicillin or ampicillin, be empirically given to neonates at high risk of listeriosis.
Alternative therapies for listeriosis include sulfamethoxazole-co-trimoxazole, tetracycline, and erythromycin. However, not all of them are appropriate for neonates due to potential adverse drug reactions. Vancomycin, Meropenem, and Linezolid are also used to treat LM infections, but the current clinical evidence is insufficient to support their routine use.33 The evolution of bacteria towards resistance has been considerably accelerated in LM.34 This is particularly concerning in neonates, as there are fewer options for antibiotics available.
Relapses of listeriosis appear to be uncommon. 2 to 3 weeks of therapy is sufficient for most forms of listeriosis.1 Neonatal listeriosis in the first week of life, it is recommended to administer ampicillin or amoxicillin at a dosage of 100–300 mg/kg/day parenterally for 14 days. If listeriosis occurs 7 days post birth, a 21-day course of treatment is advised. In our study, the median duration of antibiotic treatment for sepsis cases was 17 days. The cases of meningitis in combination required a longer duration of treatment.
There are limitations to this study. Although our hospital served as a neonatal emergency transport center and received critically ill neonates from Hubei and nearby provinces, it was still a single-center retrospective study with a small sample size. The comparison was made between the survival group and the fatal group, both of which were confirmed cases of listeriosis, without control group for other neonatal infections. Long-term neurological follow-up of neonates was not conducted. Maternal data for cases transported from other hospitals was incomplete. Epidemiological investigations were not available.
Conclusion
Neonatal listeriosis is a rare but severe infection with a high mortality rate. More studies should be conducted in China to fully explore the profile of neonatal listeriosis. Neonates with unexplained premature birth, respiratory distress, fever, rash, and other clinical symptoms should be promptly sent for blood and cerebrospinal fluid pathogen culture. If Gram positive bacteria are detected within 36 hours, LM infection should be highly suspected. Early identification and application of sensitive antibiotics are particularly critical for neonatal outcomes. Apgar score and CRP are relevant to prognosis. Ampicillin is the first-line therapy and can be empirically administered to neonates suspected of having listeriosis. As a pregnancy-related disease, prevention is the best strategy to reduce morbidity. Dietary guidance for pregnant women is necessary to strengthen food safety awareness and help them avoid consuming contaminated food. In China, nationwide surveillance and public health alerts are urgently needed.
Ethical Approval
This study was approved by the Ethics Committee of Maternal and Child Health Hospital of Hubei Province (2023IEC045) and conducted in accordance with the Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was waived by our institutional review board due to the retrospective nature of our study, and data were anonymized and kept confidential.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schlech WF, Fischetti VA, Novick RP, et al. Epidemiology and clinical manifestations of listeria monocytogenes infection. Microbiol Spectr. 2019;7(3). doi:10.1128/microbiolspec.GPP3-0014-2018
2. Wang Z, Tao X, Liu S, Zhao Y, Yang X. An update review on listeria infection in pregnancy. Infect Drug Resist. 2021;14:1967–1978. doi:10.2147/IDR.S313675
3. McLauchlin J, Amar CFL, Grant KA. Neonatal cross-infection due to listeria monocytogenes. Epidemiol Infect. 2022;150:1–31. doi:10.1017/S0950268822000504
4. Charlier C, Disson O, Lecuit M. Maternal-neonatal listeriosis. Virulence. 2020;11(1):391–397. doi:10.1080/21505594.2020.1759287
5. Herrador Z, Gherasim A, López-Vélez R, Benito A. Listeriosis in Spain based on hospitalisation records, 1997 to 2015: need for greater awareness. Euro Surveill. 2019;24(21):22.
6. Chen S, Meng F, Sun X, et al. Epidemiology of human listeriosis in china during 2008–2017. Foodborne Pathog Dis. 2020;17(2):119–125. doi:10.1089/fpd.2019.2683
7. Charlier C, Perrodeau E, Leclercq A, et al. Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study. Lancet Infect Dis. 2017;17(5):510–519. doi:10.1016/S1473-3099(16)30521-7
8. Vallejo P, Cilla G, Lopez-Olaizola M, Vicente D, Marimon JM. Epidemiology and clinical features of listeriosis in Gipuzkoa, Spain, 2010–2020. Front Microbiol. 2022;13:894334. doi:10.3389/fmicb.2022.894334
9. Sapuan S, Kortsalioudaki C, Anthony M, et al. Neonatal listeriosis in the UK 2004–2014. J Infect. 2017;74(3):236–242. doi:10.1016/j.jinf.2016.11.007
10. Girard D, Leclercq A, Laurent E, Lecuit M, de Valk H, Goulet V. Pregnancy-related listeriosis in France, 1984 to 2011, with a focus on 606 cases from 1999 to 2011. Euro Surveill. 2014;19(38). doi:10.2807/1560-7917.ES2014.19.38.20909
11. Awofisayo A, Amar C, Ruggles R, et al. Pregnancy-associated listeriosis in England and Wales. Epidemiol Infect. 2015;143(2):249–256. doi:10.1017/S0950268814000594
12. Vergnano S, Godbole G, Simbo A, et al. Listeria infection in young infants: results from a national surveillance study in the UK and Ireland. Arch Dis Child. 2021;106(12):1207–1210. doi:10.1136/archdischild-2021-321602
13. Lu B, Yang J, Gao C, et al. Listeriosis cases and genetic diversity of their L. monocytogenes isolates inChina, 2008–2019. Front Cell Infect Microbiol. 2021;11:608352. doi:10.3389/fcimb.2021.608352
14. Pohl AM, Pouillot R, Bazaco MC, et al. Differences among incidence rates of invasive listeriosis in the U.S.FoodNetPopulation by age, sex, race/ethnicity, and pregnancy status, 2008–2016. Foodborne Pathog Dis. 2019;16(4):290–297. doi:10.1089/fpd.2018.2548
15. Fan Z, Xie J, Li Y, Wang H. Listeriosis in mainland China: a systematic review. Int J Infect Dis. 2019;81:17–24. doi:10.1016/j.ijid.2019.01.007
16. Wadhwa DR, Smith MA. Pregnancy-related listeriosis. Birth Defects Res. 2017;109(5):324–335. doi:10.1002/bdr2.1012
17. Tai YL, Chi H, Chiu NC, et al. Clinical features of neonatal listeriosis in Taiwan: a hospital-based study. J Microbiol Immunol Infect. 2020;53(6):866–874. doi:10.1016/j.jmii.2019.08.001
18. Wald A, Van Thiel DH, Hoechstetter L, et al. Effect of pregnancy on gastrointestinal transit. Dig Dis Sci. 1982;27(11):1015–1018. doi:10.1007/BF01391748
19. Sridama V, Pacini F, Yang SL, Moawad A, Reilly M, DeGroot LJ. Decreased levels of helper T cells: a possible cause of immunodeficiency in pregnancy. N Engl J Med. 1982;307(6):352–356. doi:10.1056/NEJM198208053070606
20. Mylonakis E, Paliou M, Hohmann EL, Calderwood SB, Wing EJ. Listeriosis during pregnancy: a case series and review of 222 cases. Medicine. 2002;81(4):260–269. doi:10.1097/00005792-200207000-00002
21. Charlier-Woerther C, Lecuit M. Listériose et grossesse [Listeriosis and pregnancy]. Presse Med. 2014;43(6 Pt 1):676–682. [French]. doi:10.1016/j.lpm.2014.03.006
22. Fouks Y, Amit S, Many A, Haham A, Mandel D, Shinar S. Listeriosis in pregnancy: under-diagnosis despite over-treatment. J Perinatol. 2018;38(1):26–30. doi:10.1038/jp.2017.145
23. Matle I, Mbatha KR, Madoroba E. A review of Listeria monocytogenes from meat and meat products: epidemiology, virulence factors, antimicrobial resistance and diagnosis. Onderstepoort J Vet Res. 2020;87(1):e1–e20. doi:10.4102/ojvr.v87i1.1869
24. Mu Y, Li M, Zhu J, et al. Apgar score and neonatal mortality in China: an observational study from a national surveillance system. BMC Pregnancy Childbirth. 2021;21(1):47. doi:10.1186/s12884-020-03533-3
25. Iliodromiti S, Mackay DF, Smith GC, Pell JP, Nelson SM. Apgar score and the risk of cause-specific infant mortality: a population-based cohort study. Lancet. 2014;384(9956):1749–1755. doi:10.1016/S0140-6736(14)61135-1
26. Cantey JB, Lee JH. Biomarkers for the Diagnosis of Neonatal Sepsis. Clin Perinatol. 2021;48(2):215–227. doi:10.1016/j.clp.2021.03.012
27. Hornik CP, Benjamin DK, Becker KC, et al. Use of the complete blood cell count in early-onset Neonatal Sepsis. Pediatr Infect Dis J. 2012;31(8):799–802. doi:10.1097/INF.0b013e318256905c
28. Iroh TP, Bendel CM. Diagnostics for neonatal sepsis: current approaches and future directions. Pediatr Res. 2017;82(4):574–583. doi:10.1038/pr.2017.134
29. Wagstaff JS, Durrant RJ, Newman MG, et al. Antibiotic treatment of suspected and confirmed neonatal sepsis within 28 days of birth: a retrospective analysis. Front Pharmacol. 2019;10:1191. doi:10.3389/fphar.2019.01191
30. Kuzniewicz MW, Mukhopadhyay S, Li S, Walsh EM, Puopolo KM. Time to positivity of neonatal blood cultures for early-onset Sepsis. Pediatr Infect Dis J. 2020;39(7):634–640. doi:10.1097/INF.0000000000002632
31. Weinberger J, Rhee C, Klompas M. A critical analysis of the literature on time-to-antibiotics in suspected Sepsis. J Infect Dis. 2020;222(Suppl 2):S110–S118. doi:10.1093/infdis/jiaa146
32. Koopmans MM, Brouwer MC, Vazquez-Boland JA, van de Beek D. Human Listeriosis. Clin Microbiol Rev. 2023;36(1):e6019. doi:10.1128/cmr.00060-19
33. Wu F, Nizar S, Zhang L, Wang F, Lin X, Zhou X. Clinical features and antibiotic treatment of early-onset neonatal listeriosis. J Int Med Res. 2022;50(8):1410681316. doi:10.1177/03000605221117207
34. Moreno LZ, Paixao R, Gobbi DD, et al. Characterization of antibiotic resistance in Listeria spp. Isolated from slaughterhouse environments, pork and human infections. J Infect Dev Ctries. 2014;8(4):416–423. doi:10.3855/jidc.4188
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.