")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Evaluation of Meropenem-Vaborbactam Combination for the Treatment of Urinary Tract Infection: Evidence to Date
Received 12 March 2021
Accepted for publication 16 June 2021
Published 26 January 2023 Volume 2023:16 Pages 555—568
DOI https://doi.org/10.2147/IDR.S187360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Fischer Herald,1 Rodrigo M Burgos1,2
1Department of Pharmacy Practice, College of Pharmacy, University of Illinois Chicago, Chicago, IL, USA; 2Department of Medicine, College of Medicine, University of Illinois Chicago, Chicago, IL, USA
Correspondence: Fischer Herald 833 South Wood Street, Room 164, M/C 886, Chicago, IL, 60612, USA Tel +1 312 996 1654 Fax +1 312 413 1797 Email [email protected]
Abstract: As antimicrobial resistance continues to grow, one of the biggest threats includes the members of the Enterobacterales order presenting with carbapenem resistance (CRE). Meropenem-vaborbactam, along with other beta-lactam/beta-lactamase agents, has been developed to help combat this growing concern and is currently approved to treat complicated urinary tract infections (cUTI), as well as acute pyelonephritis (AP), in the USA. Vaborbactam is a novel beta-lactamase inhibitor designed specifically to optimize and restore the activity of meropenem against resistant Enterobacterales. Vaborbactam inhibits a number of beta-lactamases, including in vitro activity against extended-spectrum beta-lactamases (ESBL) and the Klebsiella pneumoniae carbapenemase (KPC) group. KPC represents one of the most clinically relevant carbapenemase in the USA, accounting for the majority of carbapenemase-producing CRE. Meropenem-vaborbactam has been studied in the two Phase 3, noninferiority trials, TANGO I and TANGO II. TANGO I compared meropenem-vaborbactam against piperacillin-tazobactam in patients with cUTIs and was found to be noninferior for overall success and microbial eradication. TANGO II expanded to other disease states (bacteremia, hospital-acquired/ventilator-associated bacterial pneumonia [HAP/VAP], complicated intra-abdominal infection [cIAI], cUTI/AP) and was found to be noninferior against best available therapy (BAT) with respect to clinical cure at the end of treatment and the test of cure. Meropenem-vaborbactam maintained the established safety profile of meropenem alone, with headache as the most common adverse event in both phase 3 studies. Overall, clinical efficacy has been demonstrated and suggests the use of meropenem-vaborbactam for the treatment of cUTI is an option.
Keywords: meropenem, vaborbactam, complicated urinary tract infections, pyelonephritis
Introduction
In the era of significant antimicrobial resistance spanning across the globe, the human species is in a constant arms race against microbes as they continue to develop mechanisms to routinely render our therapies ineffective.1 One of the most common bacterial infections whose etiology stems from resistant organisms is the urinary tract infection (UTI).2 These infections are commonly treated in symptomatic patients with a range of antibiotics including cephalosporins, aminoglycosides, fluoroquinolones and carbapenems.3 Many institutions rely upon local susceptibility data to empirically select an appropriate agent, yet with the emergence of increasingly resistant organisms, that is oftentimes a broader agent such as a carbapenem.4 As the widespread use of broad-spectrum agents continues, organisms commonly causing UTIs, such as the Enterobacterales, develop resistance.5
As the first carbapenem/beta-lactamase inhibitor combination, meropenem-vaborbactam finds its utility in this era.6 It offers an antibacterial choice with a broad spectrum of activity, rendering some of the most resistant organisms inactive.6 Meropenem-vaborbactam is currently indicated for adult patients (≥ 18 years of age) with complicated urinary tract infections (cUTI) including pyelonephritis caused by Escherichia coli, Klebsiella pneumoniae, and Enterobacter cloacae species complex when susceptible.7 The introduction of the novel beta-lactamase inhibitor vaborbactam to the already US Food and Drug Administration (FDA)-approved carbapenem, meropenem, significantly reduced the MIC for K. pneumoniae carbapenemase (KPC) producing strains of Enterobacterales when studied in vitro.6 This is promising data as KPC-producing organisms are a common threat across many institutions, with few treatment options currently available as recognized by the Centers for Disease Control and Prevention as well as the World Health Organization.8 With this expansion of coverage to the original carbapenem, there are still notable exceptions to other organisms already harboring carbapenem resistance including carbapenem-resistant Acinetobacter baumannii, Pseudomonas aeruginosa, and Stenotrophomonas maltophilia.9 The purpose of this review is to evaluate the evidence to date for the treatment of urinary tract infections with meropenem-vaborbactam.
Search Strategy/Methods
A literature search was conducted on MEDLINE and PubMed from 1950 to January 2021 using the following terms: Vabomere OR (meropenem OR RPX-2014) OR (vaborbactam OR RPX-7009) AND (complicated urinary tract infection OR acute pyelonephritis). A search was also conducted for abstracts and posters at the following professional conferences: European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), IDWeek, American Society for Microbiology (ASM) Microbe, and Making a Difference in Infectious Diseases (MAD-ID). The literature was limited to English language studies that described clinical efficacy, safety, in vitro activity, pharmacokinetics and pharmacodynamics. Literature on Phase 1 and Phase 2 studies, case reports and those with no data representing cUTI patient population were not included. There were 150 results identified of which 91 were excluded with above criteria.
Mechanism of Action
Meropenem binds to penicillin-binding proteins (PBPs), which prevents bacterial transpeptidation of peptidoglycan, which ultimately inhibits cell wall synthesis.10,11 Its highest binding affinity is for PBP2 followed by PBP3 in E. coli and P. aeruginosa, and to PBP1 in Staphylococcus aureus.12,13 Meropenem remains stable against most beta-lactamases from Gram-negative or Gram-positive organisms such as penicillinases and cephalosporinases, but is not stable against carbapenemases.7 Vaborbactam forms a reversible, covalent bond between its boronate moiety and the catalytic serine in serine beta-lactamases, and its affinity is highest for serine carbapenemases in Amber class A and C.14 With this bond, vaborbactam protects meropenem from hydrolysis by these enzymes.
In vitro Activity
The combination of meropenem and vaborbactam has shown in vitro activity against Citrobacter freundii, Citrobacter koseri, E. cloacae species complex, E. coli, E. aerogenes, K. pneumoniae, Klebsiella oxytoca, Morganella morganii, indole-positive Proteeae spp., Proteus mirabilis, Providencia spp., P. aeruginosa, and Serratia marcescens, but not against A. baumannii or S. maltophilia.7
The spectrum of vaborbactam’s beta-lactamase inhibition was determined with a panel of engineered E. coli and K. pneumoniae isolates that produced Amber class A–D enzymes.15 The E. coli strains expressing class A ESBLs (SHV, TEM, CTX-M) or class C enzymes (DHA, MIR, FOX, CMY, AmpC) had similar meropenem susceptibility to a control strain without beta-lactamase expression (MIC ≤0.03 µg/mL). The addition of vaborbactam 4 µg/mL lowered the meropenem MICs in strains producing class A carbapenemases KPC-2/3 (2 µg/mL), SME-2 (16 µg/mL) and NMC-A (1 µg/mL) down to the MICs of the control strain (≤0.03 µg/mL), but did not decrease meropenem MICs in strains expressing class B VIM-1 (1 µg/mL) and NDM-1 (16 µg/mL) or class D OXA-48 (0.125 µg/mL) carbapenemases. In K. pneumoniae strains without permeability defects, strains that produced KPC-2/3 showed increased meropenem MICs (0.5 µg/mL), which the addition of vaborbactam 4 µg/mL decreased (≤0.06 µg/mL). In K. pneumoniae strains with permeability defects, all strains expressing beta-lactamase had an increase in meropenem MIC, most notably in strains producing KPC-2/3 and OXA-48 with a 128-fold increase in MIC (64 µg/mL). The addition of vaborbactam 4 µg/mL lowered meropenem MICs in most trains including those producing KPC enzymes (2 µg/mL) but did not decrease the MIC in the strain producing OXA-48 (64 µg/mL).
The percent of carbapenemase-producing Enterobacterales with a meropenem susceptibility breakpoint of ≤1 µg/mL (established by the Clinical and Laboratory Standards Institute, CLSI) increased from 2.2% to 93.7% with the addition of vaborbactam 8 µg/mL in an in vitro study of 315 isolates of genetic diversity from 2000 to 2013 and multiple countries.16 Of the 315 isolates, 308 were KPC-producers, and the addition of vaborbactam 8 µg/mL increased the proportion of isolates inhibited at the ≤1 µg/mL meropenem CLSI susceptibility breakpoint from 0.5% to 93.3% in 208 K. pneumoniae, from 19% to 100% in 21 E. coli, from 0% to 100% in 14 Klebsiella oxytoca, and 0% to 100% in 12 Citrobacter freundii.
One of the largest in vitro studies assessed the activity of meropenem-vaborbactam against 10,426 Enterobacterales collected in 2014 from 31 countries.9 Meropenem alone inhibited 97.3% of isolates at ≤1 µg/mL, and 99.1% were inhibited with the addition of vaborbactam 8 µg/mL. The MIC50/MIC90 was 16/>32 µg/mL in 265 carbapenem-resistant Enterobacterales (CRE), 0.06/32 µg/mL in 1210 multi-drug resistant (MDR) isolates, and 0.5/32 µg/mL in 161 extensively drug-resistant (XDR) isolates with meropenem alone. These MIC50/MIC90 decreased with the addition of vaborbactam to 0.5/32 µg/mL in CRE, 0.03/1 µg/mL in MDR, and remained similar (0.5/32 µg/mL) in XDR isolates. In this study, it was also observed that the addition of vaborbactam did not enhance meropenem activity against isolates producing Amber class B metallo-beta-lactamases or class D oxacillinases.
An in vitro analysis of 4500 isolates from New York City hospital between 2013 and 2014 demonstrated that the addition of vaborbactam 8 µg/mL increased the percent of meropenem-susceptible isolates at the ≤1 µg/mL CLSI susceptibility breakpoint as follows: 99.9% of 2770 E. coli to 100%; 96.7% of 211 Enterobacter spp. to 100%; and 88% of 894 K. pneumoniae to 99.8%.17 In contrast, the number of isolates to experience a ≥4-fold decrease in meropenem MIC was observed only in 2/84 meropenem-resistant A. baumannii and in 6/98 meropenem-resistant P. aeruginosa, possibly due to resistance other than KPC production.
An in vitro study of 991 KPC-producing Enterobacterales from global surveillance collected between 2014 and 2015, and demonstrated a decrease in meropenem MIC50 and MIC90 from 32 and >32 µg/mL to 0.06 and 1 µg/mL, respectively, after the addition of vaborbactam 8 µg/mL.58 The broadest meropenem-vaborbactam MIC ranges were observed for K. pneumoniae (≤0.03 to >32 μg/mL) and S. marcescens (≤0.03 to 2 μg/mL) isolates compared to the other Enterobacterales species in this study. There were no differences in meropenem-vaborbactam activity based on KPC type or in ESBL or AmpC co-producers, and of the KPC isolates that only co-produced ESBL CTX-M and/or SHV, 99.1% (343/346) were susceptible to meropenem-vaborbactam by the ≤4 μg/mL FDA criteria at the time.
An in vitro study of 9295 Enterobacterales collected in 2016 and 2017 from hospitals in the United States determined that the proportion of isolates inhibited at an FDA-established (at the time) meropenem/vaborbactam susceptibility breakpoint of ≤4/8 µg/mL was 98.8% with meropenem alone and >99.9% with meropenem-vaborbactam.18 In the case of 105 carbapenem-resistant organisms (53 K. pneumoniae, 19 E. cloacae, 9 S. marcescens), meropenem alone inhibited 3.8% of isolates, but meropenem-vaborbactam inhibited 99.0%.
An in vitro analysis of 6846 Enterobacterales from 40 European hospitals collected from 2014 to 2019 in patients with pneumonia observed the following proportions of meropenem-susceptible isolates (CLSI criteria) with meropenem alone vs in combination with vaborbactam, respectively: 94.5% vs 97.% in 6846 Enterobacterales; 75.7% vs 89.5% in 1368 ESBL-phenotype isolates; 98.6% vs 100% in 1045 non-carbapenem-resistant ESBL isolates; 3.6% vs 56.6% in 362 CRE; 0% vs 100% in KPC-producing isolates; and 6.4% vs 21% in 157 isolates with metallo-beta-lactamases (50 NDM, 14 VM) or OXA-48 carbapenemases.19
An analysis of 130 K. pneumoniae ST258 from a surveillance system around the world, a common carbapenemase-producing type that is frequently associated with outbreaks, showed meropenem susceptibility (CLSI) in 23.1% of isolates, but increased to 99.2% with the addition of vaborbactam 8 µg/mL.20 In this analysis, 98 isolates exhibited KPC production, with the most common carbapenemases being KPC-2 in 73 isolates followed by KPC-3 in 25.
An in vitro comparison of beta-lactam inhibitors, including vaborbactam, tazobactam and clavulanic acid, assessed their ability to restore the activity of aztreonam, carbenicillin, ceftazidime and meropenem in isogenic strains of P. aeruginosa that expressed Amber class A serine carbapenemases BKC-1 and FRI-1.21 Only the addition of vaborbactam 4 µg/mL demonstrated a decrease in meropenem MIC in these strains producing BKC-1 and FRI-1 enzymes. Vaborbactam also decreased MICs for aztreonam, carbenicillin and ceftazidime.
In order to determine the concentrations of meropenem and vaborbactam needed to prevent the selection of single-step mutations and characterize any selected mutations, 18 strains of KPC-producing K. pneumoniae with meropenem MIC values ranging from ≤0.06 to 32 µg/mL were assessed in vitro.22 With a resistance mutation frequency of <1 x 10−8 as the threshold for reduced mutant selection, 14/18 isolates remained under this threshold at a concentration of meropenem 8 µg/mL and vaborbactam 8 µg/mL, and the remaining 4 isolates were able to remain under this threshold by increasing the meropenem concentration to 16 µg/mL and vaborbactam remaining at 8 µg/mL.
The in vitro activity of meropenem-vaborbactam was assessed as the MIC and minimum bactericidal concentration (MBC) in the presence of various concentrations of bovine-derived lung surfactant in 12 KPC-producing organisms: 7 K. pneumoniae, 1 E. cloacae, 1 S. marcescens, 2 P. aeruginosa, and 1 A. baumannii.23 Both the MIC and MBC of meropenem alone ranged from 16 to >256 µcg/mL, and from 0.015 to 8 µg/mL when in combination with vaborbactam, either in the presence or absence of surfactant. In this study, activity of meropenem alone or with vaborbactam was not affected when tested with lung surfactant.
Susceptibility criteria for Enterobacterales based on a regimen of meropenem 2 g and vaborbactam 2 g infused over 3 hr every 8 hr have been established for MIC values (meropenem/vaborbactam) and for disc diffusion zone of inhibition diameters as follows: susceptible with MIC ≤ 4/8 µg/mL or ≥18 mm; intermediate with MIC 8/8 µg/mL or 15–17 mm; and resistant with MIC ≥ 16/8 µg/mL or ≤14 mm.24
Pharmacokinetics and Metabolism
In 295 patients receiving meropenem 2 g and vaborbactam 2 g infused over 3 hr every 8 hr (dose-adjusted for renal function in 35 patients), the mean maximum plasma concentration (Cmax) values for meropenem and vaborbactam were 57.3 and 71.3 μg/mL, the AUC values from time 0 to hour24 (AUC0–24) were 650 and 835 μg • h/mL at steady state, the volume of distribution at steady state (Vss) 20.2 L and 18.6 L, and half-life (t1/2) 2.3 h and 2.25 h, respectively.7 These parameters are summarized in Table 1.
 |
Table 1 In vitro Activity of Varying Meropenem Concentrations Combined with Vaborbactam 8 µg/mL Against Common Gram-Negative Organisms in Different Analyses: Multiple Countries, 2014;9 Multiple Countries, 2000–2013;16 New York City, 2013–2014;17 Multiple Countries, 2014–2015;58 US, 2016;59 Multiple Countries 2016–201920 |
In healthy adults receiving meropenem 2 g and vaborbactam 2 infused over 3 hr every 8 hr for 7 days, pharmacokinetic parameters were estimated.6,25 After a single dose, the parameters for meropenem and vaborbactam ranged as follows: Cmax 45.7–48.83 µg/mL and 50.1–51.66 µg/mL; AUC from 0 to infinity (AUC0-∞) was 139.3–142.55 μg • h/mL and 165.3–170.44 μg • h/mL; Vss was 21.70–21.75 L and 21.84–22.0 L; t1/2 was 1.3–1.5 hr and 1.90–1.98 hr, respectively. Also in healthy adults, after multiple doses, the parameters for meropenem and vaborbactam were as follows: Cmax 42.5–43.35 µg/mL and 54.7–55.61 µg/mL; AUC0-∞ was 137.71 μg • h/mL and 190.43 μg • h/mL; Vss was 20.8–21.0 L and 17.5–19.3 L; t1/2 was 1.07–1.2 h and 1.37–1.6 h, respectively.
The plasma protein binding is close to 2% for meropenem and 33% for vaborbactam.7,26 In healthy adults who received meropenem 2 g and vaborbactam 2 g infused over 3 h for 3 doses, the epithelial lining fluid penetration relative to unbound plasma concentration was 65% for meropenem and 79% for vaborbactam, and alveolar macrophage concentrations were only detected for vaborbactam (2.28 to 6.94 µg/mL).27
Meropenem is hydrolyzed to an inactive metabolite at about 22% of the dose eliminated in the urine, and vaborbactam does not undergo metabolism.7 Both meropenem (40–60%) and vaborbactam (75–95%) are mainly renally excreted as unchanged drug within 24–48 h. No drug–drug interactions with meropenem or vaborbactam were seen in clinical trials with healthy adults, but since meropenem is a substrate of the organic anion transporters (OAT) 1 and 3, an increase in systemic exposure and half-life with concomitant OAT inhibitors such as probenecid is expected. Additionally, meropenem is associated with a reduction in serum valproic acid concentrations that can lead to loss of seizure control, for which anticonvulsant therapeutic drug monitor and/or supplementation should be considered.28–32 Based on in vitro data, vaborbactam is not an inhibitor of CYP1A2, CYP2B6, CYP2B8, CYP2C9, CYP2C19, CYP2D6, CYP3A4, OAT1, OAT3, OATP1B1, OATP1B3, organic cation transporter (OCT) 1, OCT2, breast cancer resistance protein (BCRP), or P-glycoprotein (P-gp), and is not an inducer of CYP1A2, CYP2B6, or CYP3A4.7 Vaborbactam is not a substrate of OAT1, OAT3, OCT2, BCRP, or P-gp.7
Pharmacodynamics
The percent of time the unbound concentration remains above the MIC (%fT > MIC) is associated with meropenem activity, with a goal of 20% for bacteriostatic activity and 40% for bactericidal activity.33–36 For vaborbactam, the 24 h unbound AUC (fAUC0-24) of vaborbactam-to-meropenem/vaborbactam MIC ratio describes its effect when administered with meropenem the best.37 Both in vitro and in vivo models demonstrated that pharmacokinetic and pharmacodynamic parameters correlated with bactericidal activity and suppression of resistance are attained with simulated human doses of meropenem 2 g and vaborbactam 2 g infused over 3 hr every 8 hr.38,39 In Monte Carlo simulations, meropenem-vaborbactam doses adjusted to varying degrees of renal impairment (see Table 2 for dosing) with MIC values of 8/8 µg/mL, the probabilities of pharmacokinetic-pharmacodynamic target attainment were ≥90% for Enterobacterales (including KPC-producers) and P. aeruginosa.40
 |
Table 2 Dosing and Pharmacokinetic Parameters of Meropenem/Vaborbactam7,26 |
Therapeutic Efficacy in Complicated Urinary Tract Infections
Tango I
The phase 3, international, double-blind, randomized clinical trial termed Targeting Antibiotic Non-Susceptible Gram-Negative Organisms (TANGO I) was a head-to-head analysis on the effect of meropenem-vaborbactam vs piperacillin-tazobactam in patients with complicated urinary tract infections.41 The objective of this study was to assess the efficacy of meropenem/vaborbactam in subjects with cUTI including AP. Patients included were ≥18 years of age with a documented or suspected cUTI or AP, 185 kg or less, and needing at least 5 days of antibiotics. Patients were excluded from the trial if they required either an antibiotic in addition to meropenem-vaborbactam or antifungal therapy. They were also excluded if they had received an antibiotic within 48 hr prior to randomization (a single dose of short acting oral or intravenous antibiotic was allowed) and had an estimated creatinine clearance <30 mL/min. Patients receiving more than 48 hr of an antibiotic could still be enrolled if they failed treatment or if further developed cUTI or AP.
The investigators in TANGO I defined cUTI and AP based on the FDA criteria.41,42 Indwelling catheters were removed or replaced within 12 hr of randomization if possible. With 550 patients being randomized (274 randomized to receive meropenem-vaborbactam and 276 randomized to receive piperacillin-tazobactam), this noninferiority trial set a margin of −15% when comparing the two. This trial set out to satisfy both the FDA as well as the European Medicines Agency (EMA) criteria for approval.42,43
The primary endpoint per the FDA was defined as the overall success as a composite outcome of clinical cure (complete resolution or significant improvement of baseline signs and symptoms of cUTI or AP) and microbial eradication (baseline pathogens reduced to <104 Colony Forming Units (CFU)/mL of urine) at end of intravenous treatment in the microbiologic modified intent-to-treat (m-MITT) population.41 The primary endpoint per the EMA was defined as microbial eradication (baseline pathogens reduced to <103 CFU/mL of urine) at a test-of-cure visit in the m-MITT and microbiologic evaluable populations (ME).
Randomization was 1:1, went by geographic region (North America, Europe, Asia Pacific and the rest of the world) and type of infection (AP, cUTI with removable focus, and cUTI with non-removable focus).41 Patients in the meropenem-vaborbactam arm of the study received 2 g/2 g via 3-hour intravenous infusion every 8 hr, while patients in the piperacillin-tazobactam group received 4 g/0.5 g over 30 minutes every 8 hr for up to 10 total days of treatment (receiving at least 5 days of therapy). Patients in both groups were able to transition to oral therapy with levofloxacin 500 mg every 24 hr if they had received 15 or more doses of intravenous therapy and met prespecified criteria for improvement with respect to fever, urinary symptoms, nausea, vomiting, abdominal pain. If levofloxacin was contraindicated, the patients may have received trimethoprim-sulfamethoxazole, cefdinir, cefixime or cefpodoxime. The end of treatment (oral + intravenous) was evaluated at day 10 unless the patient was bacteremic, and the test of cure was evaluated from day 15 up to day 19.
The patient population was made up of 60 different sites from 17 countries with baseline characteristics with no significant differences between the two study groups.41 In patients who received ≥1 dose of study drug (MITT population), the mean age was approximately 53 years and a majority of the patients were female (approximately 66%) and White (approximately 93%). The primary indication for treatment in the meropenem-vaborbactam group was AP in 59.2%, and cUTI making up 40.8% of this population. The piperacillin-tazobactam group had a similar proportion of patients with AP (59%) and cUTI (41%). On average, patients presented with 3.5 symptoms and the most common baseline pathogen was E. coli in both groups (65.1% vs 64.3%, respectively) followed by K. pneumoniae (15.6% vs 15.4%). The mean treatment duration of intravenous therapy was 8 days in each group. After intravenous therapy, 93.6% of patients in the meropenem-vaborbactam group and 95.1% of those receiving piperacillin-tazobactam switched to oral levofloxacin with a total duration of intravenous and oral therapy of approximately 10 days in each group. Baseline resistance to meropenem was present in 3/192 (1.6%) of the m-MITT isolates treated with meropenem-vaborbactam, and baseline resistance to piperacillin-tazobactam was present in 19/182 (10.4%) of the m-MITT isolates treated with piperacillin-tazobactam.41,44
At the end of the study, in the m-MITT population, the FDA primary endpoint of overall success occurred in 98.4% of the patients who received meropenem-vaborbactam vs 94.0% with piperacillin-tazobactam (difference of 4.5% [95% CI, 0.7% to 9.1%]; P < 0.001 for noninferiority).41 The EMA endpoint was also met with microbial eradication in the m-MITT population occurring in 66.7% of the meropenem-vaborbactam group and 57.7% in the piperacillin-tazobactam group (difference of 9.0% [95% CI, −0.9% to 18.7%]; P < 0.001 for noninferiority). Thus, the study met noninferiority when comparing the two agents. Although the study was not powered to evaluate secondary endpoints between the two groups, key secondary endpoints included noninferiority for overall success, clinical cure, and microbial eradication and are reported as part of the study publication.41
Of note are outcomes by pathogen in TANGO I, which were presented at a conference but were not part of the peer-reviewed publication.61 Clinical cure rates at end-of-treatment visit in the m-MITT population for meropenem-vaborbactam compared to piperacillin-tazobactam were 123/125 (98.4%) vs 110/117 (94.0%) for E. coli; 19/30 (96.7%) vs 28/28 (100.0%) for K. pneumoniae; 6/6 (100.0%) vs 12/12 (100.0%) for P. mirabilis; 10/10 (100.0%) vs 5/5 (100.0%) for E. cloacae species complex; and 5/5 (100.0%) vs 10/10 (100.0%) for P. aeruginosa. Microbial eradication rates at the test-of-cure visit, also in the m-MITT populatio, were 89/125 (71.2%) vs 68/117 (58.1%) for E. coli; 19/30 (63.3%) vs 14/28 (50.0%) for K. pneumoniae; 3/6 (50.0%) vs 9/12 (75.0%) for P. mirabilis; 9/10 (90.0%) vs 3/5 (60.0%) for E. cloacae species complex; and 5/5 (100.0%) vs 3/10 (30.0%) for P. aeruginosa in the meropenem-vaborbactam group compared to pipearcillin-tazobactam, respectively.
This study demonstrated that when treating patients with cUTIs, including pyelonephritis, where the pathogen has been identified, meropenem-vaborbactam resulted in an improvement or resolution of symptoms and microbial eradication.41 It is important to note, however, that baseline resistance to treatment was lower in the meropenem-vaborbactam arm, which makes the value of vaborbactam more difficult to ascertain.
Tango II
After TANGO I had established the safety and effectiveness of meropenem-vaborbactam in cUTI and AP, researchers sought to expand the use of this agent and evaluate its effectiveness against the best available therapy (BAT) for CRE infections. This trial, TANGO II, was a phase 3, multinational, open-label, randomized controlled trial including patients with cUTI, AP, HAP/VAP, bacteremia or cIAI.45 For all types of infections, efficacy endpoints were evaluated for clinical cure at the End of Treatment (EOT) and Test of Cure (TOC) occurring 7 days after EOT. Primary efficacy endpoints were also evaluated for each disease based on FDA guidelines in the microbiologic-CRE-modified intent-to-treat (mCRE-MITT) populations. Specifically, for the cUTI/AP subgroup, a composite endpoint of clinical cure and microbiologic eradication was used at the TOC visit.
Seventy-seven patients were randomized in this trial in a 2:1 ratio to either meropenem-vaborbactam or BAT stratified by infection type and region (North America, Europe, Asia Pacific, rest of world).45 Of note, principal investigators and staff were not blinded to treatment assignments, but a blinded adjudication committee was used to assess clinical outcomes. Patients were included if ≥18 years of age, with confirmed or suspected CRE pathogen requiring ≥7 days of intravenous therapy. Suspected CRE pathogen included evidence in culture or molecular testing within the previous 90 days. Patients could also be enrolled if the isolated organism was not susceptible to their initial treatment, if they had received ≤24 hr of therapy before enrollment or had clinical deterioration/failure after ≥48 hr of therapy. Exclusion criteria consisted of hypersensitivity to beta-lactam antibiotics, confirmed CRE infection producing New Delhi metallo (NDM)-, Verona integron-encoded metallo-, imipenemase-metallo-, or oxacillinase-encoded beta-lactamases. Patients with Acute Physiology and Chronic Health Evaluation II (APACHE) score of >30 or immediately life-threatening disease were excluded along with those on continuous renal replacement therapy. Patients were included into the cUTI and AP cohort with similar criteria as those enrolled in TANGO I.
Patients received meropenem-vaborbactam for 7–14 days of treatment as monotherapy (2 g-2 g) via intravenous infusion over 3 hr every 8 hr.45 The best available therapy, at the discretion of the investigator, included monotherapy or combination of polymyxins, carbapenems, aminoglycosides, or tigecycline, or monotherapy with ceftazidime-avibactam. For those with severe renal impairment (estimate creatinine clearance <50 mL/min), dose modifications were made based on the study protocol (meropenem-vaborbactam) or the local institution protocols (BAT).
A total of 32 patients received meropenem-vaborbactam and 15 received BAT in the mCRE-MITT population.45 A total of 16 patients (34.0%) in the study were treated for cUTI or AP, 12 (37.5%) with meropenem-vaborbactam and 4 (26.7%) with BAT. The mean age in the cohort was 62.5 years and 70.2% of the population had a creatinine clearance >50 mL/min. The baseline pathogens identified in the cUTI/AP population included K. pneumonia (12/16), E. coli (2/16), E. cloacae sp. (2/16), P. aeruginosa (1/16).44 Overall in the study, 78.7% of patients were enrolled as confirmed CRE, 72.7% of K. pneumoniae were KPC producers, and 17% of the patients were in the intensive care unit (ICU).45
In patients with cUTI/AP in the mCRE-MITT population, overall success rates at EOT were numerically higher among patients who received meropenem–vaborbactam (75.0% or 9/12) than those who received BAT [75.0% (50.0% or 2/4); overall success rates at TOC were 33.3% (4/12) for meropenem–vaborbactam and 50.0% (2/4) for BAT].45 This resulted in relative differences in overall success of 50% at EOT and −33.4% at TOC (EOT + 7d), and absolute differences in overall success of 25% at EOT and −16.7% at TOC, respectively. Clinical cure rates and microbial cure rates were consistent with overall success rates.46
A post hoc analysis of patients without prior antimicrobial failure in the mCRE-MITT population with all infection types also showed improved clinical cure and microbiologic cure rates in patients at EOT and TOC.47 The meropenem-vaborbactam 28-day all-cause mortality was 4.3% (1/23) vs 33.3% (5/15) in BAT in this population without prior antimicrobial failure. However, no 28-day all-cause mortality has been reported in patients with cUTI/AP specifically.
Primary endpoints in TANGO I are discussed earlier, and Table 3 summarizes cUTI/AP endpoints from TANGO II. There were no other available prospective trials found outside of these phase 3 studies. A case series of patients with CRE bacteremia treated with meropenem-vaborbactam described 1/5 patients with UTI as their infectious source.48 The patient in this case series was not included in the evaluation of overall clinical efficacy of meropenem-vaborbactam evaluated in this review.
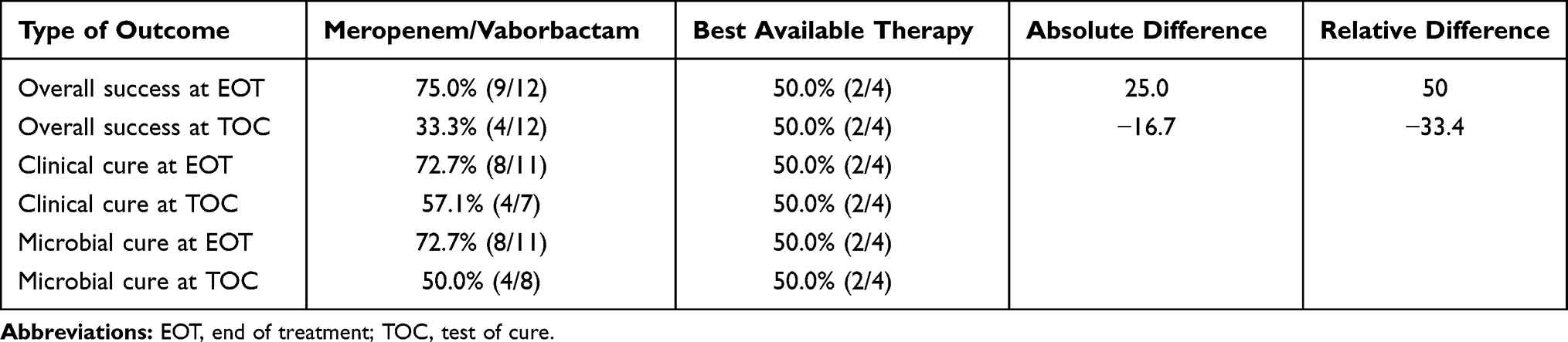 |
Table 3 Results from TANGO II Comparing Meropenem 2 g/Vaborbactam 2 g Infused Over 3 Hr Q8h or Adjusted Dose versus Best Available Therapy for the Treatment of Confirmed CRE Infections in the mCRE-MITT Population in Patients Treated for cUTI or AP45,46 |
Safety and Tolerability
During the phase 3 clinical trial TANGO I, patients in the MITT population receiving meropenem-vaborbactam vs patients receiving piperacillin-tazobactam experienced treatment-related adverse events (TAEs) in 15.1% vs 12.8%, TAEs leading to study drug discontinuation were reported in 2.6% vs 5.1%, TAEs leading to study discontinuation were 1.1% in each arm, and serious AEs (SAEs) were reported in 4.0% vs 4.4%, respectively.41 The most frequently reported adverse reactions leading to discontinuation were hypersensitivity (1.1% or 3/272) and infusion-related reactions (0.7% or 2/272).7 The most common side effect in the meropenem-vaborbactam group was headache (8.8% vs 4.4%) with all instances falling in the mild to moderate category and no cases of headache leading to trial disenrollment of a patient. Adverse effects overall were similar across both treatment groups.
In MITT population of the second phase 3 clinical trial TANGO II, meropenem-vaborbactam was associated with fewer TEAEs [84% (42/50) vs 92% (23/25)], severe TEAEs [24% (12/50) vs 44% (11/25)], and SAEs [34% (17/50) vs 44% (11/25)] than the BAT group, respectively.45 Nephrotoxicity was also associated with fewer cases in the meropenem-vaborbactam group. Serum creatinine of ≥ 0.5 mg/dL [14.0% (7/50) vs 24.0% (6/25)] and renal impairment according to RIFLE criteria [2.1% (1/48) vs 8.3% (2/24)] were less frequent with meropenem–vaborbactam than with BAT. Of note, side effects in this study were much higher on a percentage basis. This is likely attributed to the patients in this study having a greater severity of illness and a variety of comorbidities in comparison to the TANGO I population. The BAT therapy also consisted of regimens including polymyxins and aminoglycosides, both carrying considerable toxicity risk. Adverse events from both TANGO I and TANGO II are summarized in Table 4.
 |
Table 4 Adverse Reactions in MITT Populations, TANGO I & TANGO II7,41,45 |
Clostridioides difficile-associated diarrhea (CDAD) was noted in one patient in the TANGO II population while none reported within the TANGO I population.40,45 It is known that broad-spectrum agents such as the fluoroquinolones, later generation cephalosporins, and carbapenems all increase the risk of developing CDI.49 The risk of CDAD has also been noted with other FDA-approved extended spectrum beta-lactam/beta-lactamase inhibitor combinations.50,51 As use of this agent continues to expand, it will be imperative to assess this risk when choosing to treat patients with meropenem-vaborbactam.
The development of resistance in a patient population already at risk for multidrug resistant organisms (MDROs), ensuring a reasonable lack of collateral damage with the use of newer, broad-spectrum agents is an important consideration. A retrospective, multicenter cohort of adults with CRE infections who received meropenem-vaborbactam or ceftazidime-avibactam for ≥72 hr.52 Secondary endpoints in this study included 90-day CRE infection recurrence and development of resistance in those with recurrent infection. Patients with a localized cUTI were excluded from the analysis, but bacteremia with cUTI as the primary source of infection was present in 3.8% (1/26) in the meropenem-vaborbactam group and in 12.4% (13/105) in the ceftazidime-avibactam group, recurrent CRE infection observed in 11% (3/26) vs 14.3% (15/105). Of those with recurrent infection, a drug MIC increase was observed in 0% vs 40% (6/15), and emergence of drug resistance in 0% vs 20% (3/15), respectively. Although a small sample size is not powered to detect differences, these data suggest meropenem-vaborbactam may provide some protection against the development of furthering CRE resistance patterns in comparison to ceftazidime-avibactam.52
A safety summary of these two trials can be found in Table 4, including a pooled summary of adverse events in these two phase-3 trials for easy reference. However, because no meta-analytical techniques were applied, the pooled data may be subject to Simpson’s paradox bias and may not reflect the true nature of the adverse reactions experienced during the independent phase 3 trials.53
Current Place in Therapy
Antibiotics have long been used in treating patients with urinary tract infections.54 cUTIs have a higher propensity to harbor resistant organisms than other infectious disease states,55 and continued development and evaluation of agents with activity against these organisms are needed. Meropenem-vaborbactam is a promising agent in this era of antimicrobial resistance. With significantly lower drug MICs when compared to meropenem for KPC-producing Enterobacteriacea,15 meropenem-vaborbactam will be a key player for practitioners when seeking treatment for these infections.
When deciding to use meropenem-vaborbactam in clinical practice for treatment of a cUTI, it is important to understand where the agent currently falls in therapy and what it is approved to treat. The FDA has approved meropenem-vaborbactam for the treatment in patients 18 years of age and older with cUTI, including pyelonephritis, caused by the following susceptible microorganisms: E. coli, K. pneumoniae, and E. cloacae species complex. This indication stems primarily from the research and data collected during the TANGO I trial, in which meropenem-vaborbactam was compared to piperacillin-tazobactam for treatment of cUTI.7,41 Of note, piperacillin-tazobactam is not FDA-approved for the treatment of cUTI, but is used commonly and effectively for the treatment of these infections. It is also important to note a different dosing scheme of 4.5 g every 8 hr of piperacillin-tazobactam used in TANGO I compared to the standard 3.375 g administered every 6 hr for patients with a creatinine clearance > 40mL/min.
In this study, there were a low number of patients with resistant organisms as defined by CLSI/EUCAST criteria (1.6% for meropenem).24,41,56 The two most common pathogens harboring gram-negative resistance in the urinary tract were E. coli and K. pneumoniae. Analyzing the efficacy of an agent’s activity against a relatively rare incidence is a common hindrance across many studies. Understandably, TANGO I did not analyze the CRE population as it would have been unethical to administer piperacillin-tazobactam in patients identified with a CRE. However, in vitro data along with pharmacokinetic and pharmacodynamic properties of the drug suggest that meropenem-vaborbactam will maintain efficacy in the face of these KPC-producing organisms.
The second phase 3 clinical trial in which meropenem-vaborbactam was studied, TANGO II, presented a larger number of enrolled patients with confirmed CRE infections (>50%).45 This study also assessed its efficacy in different disease states against best available therapy, with 34.0% (16/47) of indications being cUTI or AP. Greater than 40% of the population met SIRS criteria and 18% of them were located in an ICU setting. In comparison to the TANGO I cohort of patients, these patients were more critically ill (by SIRS definition) and experienced a higher rate of confirmed CRE infections. Although the number of cUTIs or AP in this study was small, its efficacy given the severity of infections with resistant organisms can be reassuring when treating Enterobacterales within the urinary tract, particularly KPC producers.
With no significant safety signals stemming from the two phase 3 clinical trials, meropenem-vaborbactam appears to be safe to use in the studied patient population. The drug was well tolerated with low incidence of discontinuation from the studies due to significant adverse reactions. In addition, decades of experience with meropenem alone can provide some insight into its safety profile. However, close vigilance for adverse events, including the development of CDAD post-treatment, should remain beyond clinical trials. Close vigilance will also be important as overuse of this agent may lead to a different resistance profile. It is also important to note the locations where these phase 3 trials took place since the potential advantages of this agent may not hold in other geographic locations where the populations and resistance patterns are different.
Since meropenem-vaborbactam was approved in 2017, other beta-lactam/beta-lactamase inhibitor combinations have also been studied in the treatment of CRE infections, and as of this writting, in the United States, meropenem-vaborbactam has only been approved by the FDA for cUTI/AP.7,50,51,57,60 This is in contrast to other extended spectrum beta-lactam/beta-lactamase inhibitor combinations (i.e. ceftazidime-avibactam, ceftolozane-tazobactam and imipenem-cilastatin-relebactam), which have additional FDA indications for HAP/VAP and cIAI (in combination with metronidazole in the case of ceftazidime-avibactam and ceftolozane-tazobactam).7,50,51,57 Based on data in cUTI/AP, meropenem-vaborbactam only has FDA indications for E. cloacae species complex, E. coli and K. pneumoniae, whereas additional organisms are listed for the other agents: P. aeruginosa for ceftazidime-avibactam, ceftolozane-tazobactam and imipenem-cilastatin-relebactam; P. mirabilis for ceftazidime-avibactam and ceftolozane-tazobactam; C. freundii for ceftazidime-avibactam; and K. aerogenes for imipenem-cilastatin-relebactam.7,50,51,57
With respect to carbapenem-resistant organisms, only meropenem-vaborbactam, ceftazidime-avibactam and imipenem-cilastatin-relebactam are expected to have activity against Ambler Class A serine-carbapenemase-producine (KPC) organisms, but not ceftolozane-tazobactam; only ceftazidime-avibactam is expected to have activity against Class D OXA-type-producine (OXA-48) organisms; and none of these agents are expected to have activity against Class B metallo-beta-lactamase-producing organisms.60 Additionally, none of these agents are expected to have activity against carbapenem-resistant A. baumannii or S. maltophilia. Only ceftazidime-avibactam, ceftolozane-tazobactam and imipenem-cilastatin-relebactam are expected to have activity against carbapenem-resistant P. aeruginosa, but not meropenem-vaborbactam.
Additionally, when considering the place in therapy for meropenem-vaborbactam, factors such as availability, cost, local antibiograms should all play a key role in that decision-making process. As discussed earlier, consideration must be given to the organism’s mechanism of resistance, and the clinician should keep in mind that organisms with Amber class B and D resistance will not be appropriately addressed by meropenem-vaborbactam.58
Conclusion
Clinical data support the use of meropenem-vaborbactam for the treatment of complicated urinary tract infections and acute pyelonephritis. In vitro and clinical data support its role and utility in the setting of carbapenem-resistant Enterobacterales due to KPC production. Clinical data also suggest meropenem-vaborbactam is well tolerated. Clinicians could consider meropenem-vaborbactam as an option for the treatment of complicated urinary tract infections and pyelonephritis, particularly in patients with documented or suspected KPC-producing CRE infections. Caution is warranted against overuse, or use in populations outside of those seen in phase 3 trials as new resistance profiles may emerge.
Disclosure
Dr Rodrigo M Burgos reports clinical investigator for investigator-initiated research from Merck & Co., Inc, clinical investigator for industry-sponsored research from Moderna Inc, and Janssen Vaccines & Prevention B.V., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Gajdács M, Albericio F. Antibiotic resistance: from bench to patients. Antibiotics (Basel). 2019;8(3):129. doi:10.3390/antibiotics8030129
2. Centers for Disease Control and Prevention (US). Antibiotic Resistance Threats in the United States, 2019. Centers for Disease Control and Prevention (US); 2019. Available from: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf.
3. Behzadi P, Urbán E, Matuz M, Benkő R, Gajdács M. The role of gram-negative bacteria in urinary tract infections: current concepts and therapeutic options. Adv Exp Med Biol. 2021;1323:35–69. doi:10.1007/5584_2020_566
4. O’Neill J. Tackling drug-resistant infections globally: final report and recommendations. London: HM Government and Wellcome Trust; 2016. Review on Antimicrobial Resistance, chaired by Jim O’Neill. Available from: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf.
5. Jacoby GA, Munoz-Price LS. The new beta-lactamases. N Engl J Med. 2005;352(4):380–391. doi:10.1056/NEJMra041359
6. Rubino CM, Bhavnani SM, Loutit JS, et al. Phase 1 study of the safety, tolerability, and pharmacokinetics of vaborbactam and meropenem alone and in combination following single and multiple doses in healthy adult subjects. Antimicrob Agents Chemother. 2018;62(4):e02228–17. doi:10.1128/AAC.02228-17
7. Vabomere® (meropenem and vaborbactam) [package insert]. In the Treatment of Cutiarm Yourself for Battle Against Serious Gram-Negative Pathogens with Vabomere®1*. Lincolnshire, IL: Melinta Therapeutics, Inc.; 2021.
8. World Health Organization (WHO). Global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics; 2021. Available from: https://www.who.int/medicines/publications/global-priority-list-antibiotic-resistant-bacteria/en/.
9. Castanheira M, Huband MD, Mendes RE, Flamm RK. Meropenem-vaborbactam tested against contemporary gram-negative isolates collected worldwide during 2014, including carbapenem-resistant, KPC-producing, multidrug-resistant, and extensively drug-resistant Enterobacteriaceae. Antimicrob Agents Chemother. 2017;61(9):e00567–17. doi:10.1128/AAC.00567-17
10. Codjoe FS, Donkor ES. Carbapenem resistance: a review. Med Sci (Basel). 2017;6(1):1. doi:10.3390/medsci6010001
11. Papp-Wallace KM, Endimiani A, Taracila MA, Bonomo RA. Carbapenems: past, present, and future. Antimicrob Agents Chemother. 2011;55(11):4943–4960. doi:10.1128/AAC.00296-11
12. Kohler J, Dorso KL, Young K, et al. In vitro activities of the potent, broad-spectrum carbapenem MK-0826 (L-749,345) against broad-spectrum β-lactamase- and extended-spectrum β-lactamase- producing K. pneumoniae and E. coli clinical isolates. Antimicrob Agents Chemother. 1999;43:1170–1176. doi:10.1128/AAC.43.5.1170
13. Yang Y, Bhachech N, Bush K. Biochemical comparison of imipenem, meropenem and biapenem: permeability, binding to penicillin-binding proteins, and stability to hydrolysis by beta-lactamases. J Antimicrob Chemother. 1995;35(1):75–84. doi:10.1093/jac/35.1.75
14. Hecker SJ, Reddy KR, Totrov M, et al. Discovery of a cyclic boronic acid b-lactamase inhibitor (RPX7009) with utility vs Class A serine carbapenemases. J Med Chem. 2015;58(9):3682–3692. doi:10.1021/acs.jmedchem.5b00127
15. Lomovskaya O, Sun D, Rubio-Aparicio D, et al. Vaborbactam: spectrum of beta-lactamase inhibition and impact of resistance mechanisms on activity in Enterobacteriaceae. Antimicrob Agents Chemother. 2017;61(11):e01443–17. doi:10.1128/AAC.01443-17
16. Castanheira M, Rhomberg PR, Flamm RK, Jones RN. Effect of the β-lactamase inhibitor vaborbactam combined with meropenem against serine carbapenemase-producing enterobacteriaceae. Antimicrob Agents Chemother. 2016;60(9):5454–5458. doi:10.1128/AAC.00711-16
17. Lapuebla A, Abdallah M, Olafisoye O, et al. Activity of meropenem combined with RPX7009, a novel β-lactamase inhibitor, against Gram-negative clinical isolates in New York City. Antimicrob Agents Chemother. 2015;59(8):4856–4860. doi:10.1128/AAC.00843-15
18. Castanheira M, Doyle TB, Kantro V, Mendes RE, Shortridge D. Activity of meropenem-vaborbactam and characterization of carbapenem resistance mechanisms among carbapenem-resistant enterobacteriaceae from United States hospitals (2016–2017).
19. Shortridge D, Deshpande L, Duncan L, Streit J, Castanheira M. Activity of meropenem-vaborbactam and single-agent comparators against Enterobacterales isolates, including KPC-producing isolates, from European patients hospitalized with pneumonia including ventilator-associated pneumonia (2014–2019).
20. Shortridge D, Deshpande L, Doyle T, Streit J, Castanheira M. Activity of meropenem-vaborbactam and comparators against globally disseminated Klebsiella pneumoniae sequence type 258.
21. Lomovskaya O, Tsivkovski R. Vaborbactam (RPX7009) plus meropenem is active against the newly discovered BKC-1 and FRI-1 carbapenemases.
22. Sun D, Rubio-Aparicio D, Nelson K, Dudley MN, Lomovskaya O. Meropenem-vaborbactam resistance selection, resistance prevention, and molecular mechanisms in mutant of KPC-producing Klebsiella pneumoniae. Antimicrob Agents Chemother. 2017;61(12):e01694–17. doi:10.1128/AAC.01694-17
23. Rubio-Aparicio D, Loutit J, Dudley M, Lomovskaya O. Potency of meropenem-vaborbactam in lung surfactant. Antimicrob Agents Chemother. 2017;62(1):e01702–17. doi:10.1128/AAC.01702-17
24. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing.
25. Griffith D, Rubino C, Loutit J, Morgan E, White D, Dudley M. A phase 1 study of the safety, tolerability, and pharmacokinetics of the β-lactamase inhibitor RPX7009 alone, meropenem alone, and both in combination (Carbavance) TID for 7 days in healthy adult subjects. Open Forum Infect Dis. 2014;1(S1):S154–155. doi:10.1093/ofid/ofu052.267
26. Griffith D, Loutit J, Morgan E, et al. Phase 1 study of the safety, tolerability, and pharmacokinetics of the beta-lactamase inhibitorRPX7009 in healthy adult subjects. Antimicrob Agents Chemother. 2016;60(10):6326–6332. doi:10.1128/AAC.00568-16
27. Wenzler E, Gotfried MH, Loutit JS, et al. Meropenem-RPX7009 concentrations in plasma, epithelial lining fluid, and alveolar macrophages of healthy adult subjects. Antimicrob Agents Chemother. 2015;59(12):7232–7239. doi:10.1128/AAC.01713-15
28. Coves-Orts FJ, Borras-Blasco J, Navarro-Ruiz A, Murcia-López A, Palacios-Ortega F. Acute seizures due to a probable interaction between valproic acid and meropenem. Ann Pharmacother. 2005;39(3):533–537. doi:10.1345/aph.1E358
29. De Turck BJG, Diltoer MW, Cornelis PJ, et al. Lowering of plasma valproic acid concentrations during concomitant therapy with meropenem and amikacin. J Antimicrob Chemother. 1998;42(4):563–564. doi:10.1093/jac/42.4.563
30. Haroutiunian S, Ratz Y, Rabinovich B, Adam M, Hoffman A. Valproic acid plasma concentration decreases in a dose-independent manner following administration of meropenem: a retrospective study. J Clin Pharmacol. 2009;49(11):1363–1369. doi:10.1177/0091270009334377
31. Nacarkucuk E, Saglam H, Okan M. Meropenem decreases serum level of valproic acid. Pediatr Neurol. 2004;31(3):232–234. doi:10.1016/j.pediatrneurol.2004.03.014
32. Spriet I, Goyens J, Meersseman W, Wilmer A, Willems L, Van Paesschen W. Interaction between valproate and meropenem: a retrospective study. Ann Pharmacother. 2007;41(7–8):1130–1136. doi:10.1345/aph.1K079
33. Craig WA, Ebert S, Watanabe Y. Differences in time above MIC (T > MIC) required for efficacy of β-lactams in animal infection T 1 MIC models [abstract 86]. In: Program and Abstracts of the 35th Interscience Conference on Antimicrobial Agents and Chemotherapy (New Orleans). Washington, DC: American Society for Microbiology; 1993.
34. Ong CR, Tessier PR, Li C, Nightingale CH, Nicolau DP. Comparative in vivo efficacy of meropenem, imipenem, and cefepime against Pseudomonas aeruginosa expressing MexA-MexB-OprM efflux pumps. Diagn Microbiol Infect Dis. 2007;57(2):153–161. doi:10.1016/j.diagmicrobio.2006.06.014
35. Mattoes HM, Kuti JL, Drusano GL, Nicolau DP. Optimizing antimicrobial pharmacodynamics: dosage strategies for meropenem. Clin Ther. 2004;26(8):1187–1198. doi:10.1016/s0149-2918(04)80001-8
36. Maglio D, Banevicius MA, Sutherland C, Babalola C, Nightingale CH, Nicolau DP. Pharmacodynamic profile of ertapenem against Klebsiella pneumoniae and Escherichia coli in a murine thigh model. Antimicrob Agents Chemother. 2005;49(1):276–280. doi:10.1128/AAC.49.1.276-280.2005
37. Griffith D, Sabet M, Tarazi Z, Lomovskaya O, Dudley MN. Pharmacokinetics/pharmacodynamics of vaborbactam, a novel beta-lactamase inhibitor, in combination with meropenem. Antimicrob Agents Chemother. 2019;63(1):e01659–18. doi:10.1128/AAC.01659-18
38. Sabet M, Tarazi Z, Nolan T, et al. Activity of meropenem-vaborbactam in mouse models of infection due to KPC-producing carbapenem-resistant Enterobacteriaceae. Antimicrob Agents Chemother. 2017;62(1):e01446–17. doi:10.1128/AAC.01446-17
39. Sabet M, Tarazi Z, Rubio-Aparicio D, et al. Activity of simulated human dosage regimens of meropenem and vaborbactam against carbapenem- resistant Enterobacteriaceae in an in vitro hollow-fiber model. Antimicrob Agents Chemother. 2018;62(2):e01969–17. doi:10.1128/AAC.01969-17
40. Bhavnani SM, Trang M, Griffith DC, et al. Meropenem-vaborbactam pharmacokinetic pharmacodynamic target attainment analyses as support for dose selection in patients with normal renal function and varying degrees of renal impairment.
41. Kaye KS, Bhowmick T, Metallidis S, et al. Effect of meropenem-vaborbactam vs piperacillin-tazobactam on clinical cure or improvement and microbial eradication in complicated urinary tract infection: the TANGO I randomized clinical trial. JAMA. 2018;319(8):788–799. doi:10.1001/jama.2018.0438
42. US Food and Drug Administration (FDA). Complicated urinary tract infections: developing drugs for treatment: guidance for industry; 2021. Available from: https://www.fda.gov/downloads/Drugs/Guidances/ucm070981.pdf.
43. European Medicines Agency (EMA). Addendum to the guideline on the evaluation of medicinal products indicated for treatment of bacterial infections; 2021. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2013/11/WC500153953.pdf.
44. FDA. FDA medical review: vabomere (meropenem and vaborbactam), 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/209776Orig1s000MedR.pdf.
45. Wunderink RG, Giamarellos-Bourboulis EJ, Rahav G, et al. Effect and safety of meropenem–vaborbactam versus best-available therapy in patients with carbapenem-resistant Enterobacteriaceae infections: the TANGO II randomized clinical trial. Infect Dis Ther. 2018;7:439–455. doi:10.1007/s40121-018-0214-1
46. Wunderink R, Giamarellos-Bourboulis EJ, Rahav G, et al. Meropenem-vaborbactam (VABOMERE) vs. best available therapy for carbapenem-resistant Enterobacteriaceae infections in TANGO II: primary outcomes by site of infection.
47. Bassetti M, Giacobbe DR, Patel N, Tillotson G, Massey J. Efficacy and safety of meropenem–vaborbactam versus best available therapy for the treatment of carbapenem-resistant enterobacteriaceae infections in patients without prior antimicrobial failure: a post hoc analysis. Adv Ther. 2019;36(7):1771–1777. doi:10.1007/s12325-019-00981-y
48. Alosaimy S, Jorgensen SCJ, Lagnf AM et al. Meropenem vaborbactam in patients with carbapenem resistant enterobacteriaceae gram-negative bloodstream infection: a case series.
49. Ge IY, Fevrier HB, Conell C. reducing risk of clostridium difficile infection and overall use of antibiotic in the outpatient treatment of urinary tract infection. Ther Adv Urol. 2018;10:283–293. doi:10.1177/1756287218783871
50. Avycaz® [package insert]. Verona, Italy: ACS Dobfar S.p.A.; 2022.
51. Zerbaxa® [package insert]. Rahway, NJ: Merck Sharp & Dohme LLC; 2022.
52. Ackley R, Roshdy D, Meredith J, et al. Meropenem-vaborbactam vs ceftazidime-avibactam for treatment of carbapenem-resistant Enterobacteriaceae infections. Antimicrob Agents Chemother. 2020;64(5):e02313–19. doi:10.1128/AAC.02313-19
53. Wang B, Wu P, Kwan B, Tu XM, Feng C. Simpson’s paradox: examples. Shanghai Arch Psychiatry. 2018;30(2):139–143. doi:10.11919/j.issn.1002-0829.218026
54. Jancel T, Dudas V. Management of uncomplicated urinary tract infections. West J Med. 2002;176(1):51–55. doi:10.1136/ewjm.176.1.51
55. Gajdács M, Bátori Z, Ábrók M, Lázár A, Burián K. Characterization of resistance in gram-negative urinary isolates using existing and novel indicators of clinical relevance: a 10-year data analysis. Life (Basel). 2020;10(2):16. doi:10.3390/life10020016
56. European Committee on Antimicrobial Susceptibility Testing (EUCAST). EUCAST criteria; 2021. Available from: http://www.eucast.org/.
57. Recarbrio® [package insert]. Rahway, NJ: Merck Sharp & Dohme LLC; 2022.
58. Hackel MA, Lomovskaya O, Dudley MN, et al. In vitro activity of meropenem-vaborbactam against clinical isolates of KPC-positive Enterobacteriaceae. Antimicrob Agents Chemother. 2018;62(1):e01907–17. doi:10.1128/AAC.01904-17
59. Castanheira M, Woosley LN, Huband MD, Flamm RK. Activity against Enterobacteriaceae isolates, including carbapenem-resistant and carbapenemase-producing isolates, collected in United States (US) hospitals during 2016.
60. Doi Y. Treatment options for carbapenem-resistant gram-negative bacterial infections. Clin Infect Dis. 2019;69(Suppl 7):S565–S575. doi:10.1093/cid/ciz830
61. Walsh TJ, Bhowmick T, Darouiche RO, et al. Per pathogen outcomes of meropenem-vaborbactam (M-V) versus piperacillin-tazobactam (P-T) in the treatment of adults with complicated urinary tract infections (cUTI), including acute pyelonephritis (AP), in TANGO 1, a phase 3 randomized, double-blind, double-dummy trial. Poster presentated at the: 27th Annual European Congress of Clinical Microbiology and Infectious Diseases. Apr 2019; Vienna, Austria.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.