")
Back to Journals » Drug Design, Development and Therapy » Volume 8
Clinical efficacy of second-generation tyrosine kinase inhibitors in imatinib-resistant gastrointestinal stromal tumors: a meta-analysis of recent clinical trials
Authors Wu L, Zhang Z, Yao H, Liu K, Wen Y, Xiong L
Received 10 March 2014
Accepted for publication 17 April 2014
Published 30 October 2014 Volume 2014:8 Pages 2061—2067
DOI https://doi.org/10.2147/DDDT.S63840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Lile Wu, Zhongqiang Zhang, Hongliang Yao, Kuijie Liu, Yu Wen, Li Xiong
Department of General Surgery, Second Xiangya Hospital of Central South University, Changsha, People's Republic of China
Background: Primary and secondary resistance to imatinib, a selective receptor tyrosine kinase inhibitor (TKI), is a serious clinical problem in the control of advanced gastrointestinal stromal tumors (GIST). Here we report on a meta-analysis we performed to evaluate the efficacy of second-generation TKIs in the treatment of patients with imatinib-resistant GIST.
Methods: Randomized controlled trials evaluating the clinical efficacy of second-generation TKIs were identified by searching PubMed and EMBASE from 2000 to February 2014. Outcomes subjected to analysis were progression-free survival and overall survival. Statistical analyses were performed using Review Manager version 5.1.0 (Cochrane Collaboration, Oxford, UK). Weighted hazard ratios (HR) with 95% confidence intervals (CIs) were calculated for the outcomes. Fixed-effects or random-effects models were used, depending on the degree of heterogeneity across the selected studies.
Results: Three randomized controlled trials were selected for meta-analysis. Among imatinib-resistant or imatinib-intolerant patients, 541 received second-generation TKIs (sunitinib, nilotinib, or regorafenib) and 267 controls received placebo or best supportive care. Progression-free survival was significantly improved in the TKI-treated group (HR 0.38; 95% CI 0.24–0.59; P<0.0001). No statistically significant difference was detected in overall survival between the treatment group and the control group (HR 0.85; 95% CI 0.71–1.03; P=0.09). In the subgroup of patients who were resistant or intolerant to both imatinib and sunitinib, TKI therapy (nilotinib or regorafenib) improved progression-free survival (HR 0.40; 95% CI 0.19–0.84; P=0.02) but not overall survival (HR 0.83; 95% CI 0.63–1.08; P=0.17). Regorafenib was shown to be effective in terms of progression-free survival across different subpopulations of patients who were resistant to both imatinib and sunitinib.
Conclusion: Second-generation TKIs (sunitinib, nilotinib, and regorafenib) are effective in improving progression-free survival but not overall survival in patients with GIST who are resistant or intolerant to imatinib or to imatinib and sunitinib. Regorafenib is promising as a third-line treatment option for patients with advanced GIST.
Keywords: tyrosine kinase inhibitor, gastrointestinal stromal tumor, imatinib, nilotinib, regorafenib
Introduction
Gastrointestinal stromal tumors (GIST) are the most common gastrointestinal mesenchymal tumors.1–3 Approximately 85% of GIST have mutations in the proto-oncogene KIT which encodes a tyrosine kinase receptor. About 8% of GIST are associated with mutations in the gene for platelet-derived growth factor receptor alpha (PDGFRA).4,5 Whereas surgery, chemotherapy, and radiotherapy are the treatments of choice in the early stages of GIST, they are ineffective in unresectable and/or metastatic GIST.6 Elucidation of the molecular mechanism underlying GIST as a mutation-driven cancer has led to the development of targeted tyrosine kinase inhibitor (TKI) therapies that have revolutionized treatment options and significantly improved the clinical outcomes for patients with GIST.7 The current first-line treatment of choice for unresectable and advanced metastatic GIST is imatinib mesylate.8 Imatinib mesylate is a selective TKI of KIT, PDGFRA, and ABL via competitive binding with their ATP binding domains. Nearly 80% of patients with GIST have responses to imatinib, and the 2-year survival in advanced GIST reaches as high as 75%–80%. However, imatinib therapy is not effective in patients with wild-type KIT/PDGFRA, and more than 80% of those who are initially responsive to imatinib eventually develop resistance to the drug, with secondary mutations located in KIT exons.9,10 The first second-generation TKI approved for the treatment of imatinib-resistant GIST patients was sunitinib malate.11,12 Sunitinib malate is an inhibitor of KIT, vascular endothelial growth factor receptor (VEGR), and PDGFRA,13,14 and has been shown to be more effective against wild-type KIT kinase than imatinib. Sunitinib is currently the second-line treatment of choice for imatinib-resistant patients. Other second-generation TKIs are currently in development, some of which have been tested for efficacy in clinical trials.15–18 Recently, two Phase III clinical trials have been completed for second-generation TKIs, ie, nilotinib and regorafenib.19,20 Like imatinib, nilotinib has an inhibitory effect on KIT and PDGFRA, and is also used as a potent BCR-ABL receptor TKI.21,22 Regorafenib is a novel broad TKI that blocks the activity of various receptor tyrosine kinases, such as the VEGF receptor, KIT, RET, RAF1, BRAF, fibroblast growth factor receptor, and PDGF receptor.23 With the increasing number of next-generation TKIs being developed for the treatment of imatinib-resistant GIST, it has become necessary to systematically evaluate their clinical efficacy. Here we report on a meta-analysis we performed using data from the most up-to-date randomized controlled trials to evaluate the efficacy of second-generation TKIs with regard to progression-free survival and overall survival in patients with advanced GIST.
Materials and methods
Databases and search strategy
We searched the PubMed (from 2000 to February 2014) and EMBASE (from 2000 to February 2014) databases for relevant studies. Search terms used for PubMed were: “gastrointestinal”[All Fields] AND “stromal”[All Fields] AND (“tumor”[All Fields] OR “tumour”[All Fields] OR “tumors”[All Fields] OR “tumours”[All Fields]) OR “GIST”[All Fields] AND “imatinib”[All Fields] AND (“resistant”[All Fields] OR “resistance”[All Fields] OR “failure”[All Fields]) AND (Clinical Trial[ptyp] AND (“2000/01/01”[PDAT]: “2014/2/28”[PDAT])). Search terms used for EMBASE were: “gastrointestinal” and “stromal” and (“tumor”/exp or “tumour”/exp or “tumors” or “tumours”) and “imatinib”/exp and (“resistant” or “resistance” or “failure”) and [controlled clinical trial]/lim and [2000–2014]/py.
Selection criteria
Eligible studies were selected based on the following criteria: study design (randomized controlled trial); subjects (GIST tolerant to previous imatinib and/or other lines of treatment); and intervention (TKI versus placebo or best supportive care as control). Two authors (LW and LX) independently conducted the study selection based on these criteria. Any discrepancy was resolved by group discussion between all authors.
Quality assessment
The quality of the included trials was assessed using the Jadad score (0–5, with a score ≥3 indicating high quality).24
Outcomes
The primary outcomes for assessment of TKI efficacy were progression-free survival and overall survival.
Data extraction and statistical analysis
The following information was extracted from the selected studies: author, publication year, trial phase, number of patients enrolled, treatment regimen, median age, sex percentage, prior experience with imatinib and other lines of cancer therapy, median progression-free survival, and median overall survival. The data were extracted by two reviewers (LW and LX) from selected studies independently. Any disagreement was discussed and consensus was reached for all issues. The hazard ratio (HR) and associated 95% confidence interval (CI) for progression-free survival and overall survival were used to assess treatment efficacy. The χ2 Cochrane’s Q test was used to detect heterogeneity (variability in the intervention effects) across different studies. The random-effects or fixed-effects inverse variance weighted method was used for the pooled efficacy analysis depending on the results of heterogeneity testing.25 All analyses were performed using Review Manager version 5.1.0 (Cochrane Collaboration, Oxford, UK).
Results
Study identification and characteristics
A total of 105 unique records were identified by our search strategy. After initial screening by title and abstract, 32 relevant randomized controlled trials were selected for further screening. Twenty-eight studies did not include standard or placebo controls and were excluded. Full-text manuscripts were retrieved for the remaining four studies. One study was excluded because it contained redundant data that were included in a later complete report. Three studies that met our inclusion criteria were selected for the final meta-analysis (Figure 1).12,19,20 The Jadad score for these studies was 5, indicating high quality. The study characteristics are summarized in Table 1.
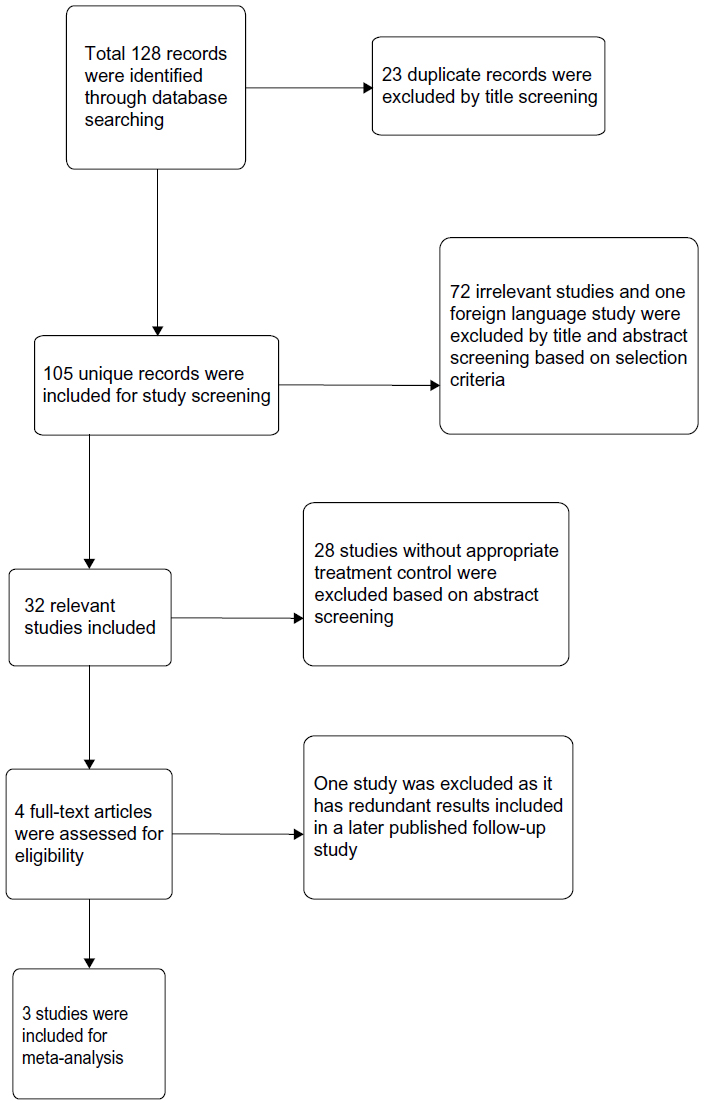 | Figure 1 Flow diagram of study selection. |
 | Table 1 Study characteristics and quality assessment |
Baseline patient demographics, median progression-free survival, and overall survival
Baseline patient demographics, median progression-free survival, and overall survival for the three studies are summarized in Table 2. More than 90% of the patients in these studies had resistance to imatinib. Patients in the nilotinib and regorafenib studies had previously been treated with both imatinib and sunitinib. Overall survival in the regorafenib study was at the interim analysis stage, so no final data were available.
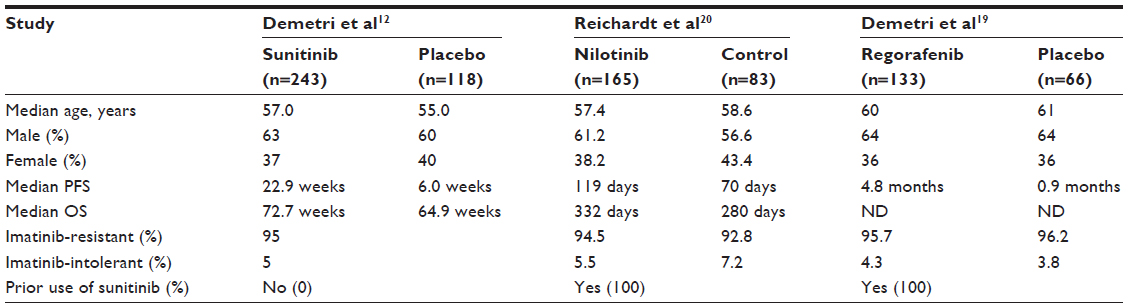 | Table 2 Major baseline patient demographics, median progression-free survival and overall survival from selected studies |
Overall progression-free survival and overall survival
Heterogeneity was found across the three studies for progression-free survival (I2=81%, P=0.005), which may have resulted from differences in interventions and prestudy treatments used in the different studies. Therefore, a random model was used for meta-analysis of progression-free survival. No heterogeneity was shown for overall survival (I2=0%, P=0.92) and a fixed model was applied for analysis of overall survival. Among patients who were resistant or intolerant to imatinib, 541 received TKIs (sunitinib, nilotinib, or regorafenib) and 267 patients received placebo or best supportive care as controls. Progression-free survival was significantly improved in the TKI-treated group when compared with the control group (HR 0.38; 95% CI 0.24–0.59; P<0.0001, Figure 2). No statistically significant difference was detected in overall survival between the treatment group and the control group (HR 0.85; 95% CI 0.71–1.03; P=0.09, Figure 3). In the subgroup of patients who were resistant or intolerant to both imatinib and sunitinib, a total of 298 received TKIs (nilotinib or regorafenib) and 149 received placebo or best supportive care. Progression-free survival was significantly improved in the TKI-treated group (HR 0.40; 95% CI 0.19–0.84; P=0.02, Figure 2). No statistically significant difference was detected in overall survival between the treatment group and the control group (HR 0.83; 95% CI 0.63–1.08; P=0.17, Figure 3). Discordance of the progression-free survival result was reported in the study of nilotinib.18 While blinded central radiology review showed no significant difference between the treatment group and the control group, local investigator assessment revealed that progression-free survival was significantly longer in the treatment group. Data from the local investigator assessment was used for the meta-analysis because a high discordance rate was documented for the central reviewers.
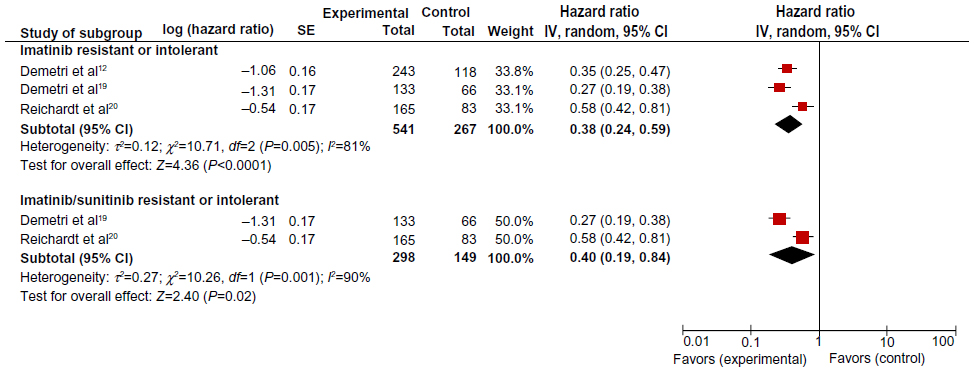 | Figure 2 Forest plot of hazard ratios comparing progression-free survival in tyrosine kinase inhibitor treatment group versus the control group. Hazard ratios for each trial are represented by the squares, and the horizontal line crossing the square represents the 95% confidence interval. |
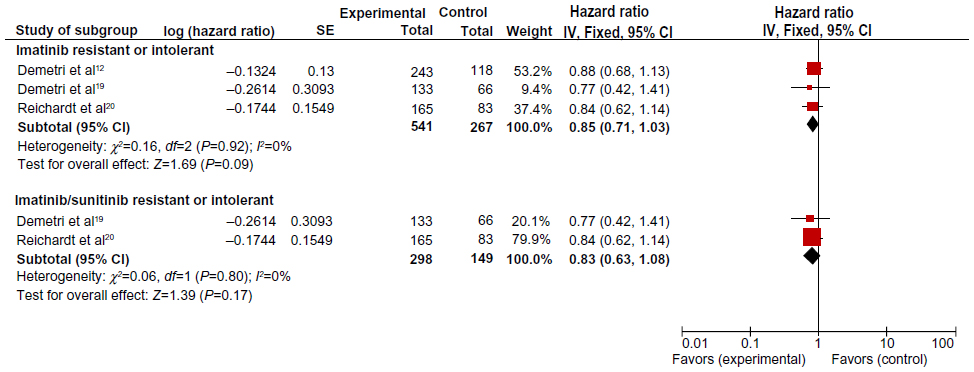 | Figure 3 Forest plot of hazard ratios comparing overall survival in tyrosine kinase inhibitor treatment versus control group. Hazard ratios for each trial are represented by the squares, and the horizontal line crossing the square represents the 95% confidence interval. |
Assessment of publication bias
A Begg’s funnel plot was used to assess for publication bias in the studies selected for meta-analysis.26 The result showed no obvious asymmetry, indicating no publication bias (Figure 4). However, because only three studies qualified for the meta-analysis, publication bias may occur when studies with negative results are not submitted for publication by investigators.
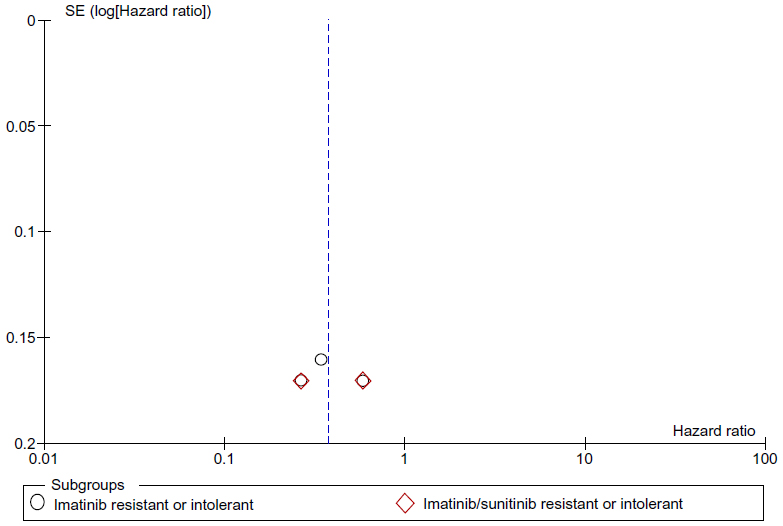 | Figure 4 Funnel plot of studies selected for meta-analysis. |
Discussion
Despite the successful outcomes using imatinib in the treatment of unresectable and/or metastatic GIST, more than 80% of patients with advanced GIST eventually develop resistance to this drug. Several structurally distinct TKIs have been developed to overcome the problem of imatinib resistance. Among these second-generation TKIs, only sunitinib has been approved for use as a second-line treatment option for imatinib-resistant GIST. However, resistance to sunitinib has also developed in previously responsive patients.27 Recently, two novel TKI inhibitors, nilotinib and regorafenib, have been shown to be promising in the control of both imatinib-resistant and sunitinib-resistant GIST. Our meta-analysis of three randomized controlled Phase III trials showed that progression-free survival was significantly improved in imatinib-resistant patients treated with sunitinib, nilotinib, or regorafenib. Improved progression-free survival was also observed in imatinib-resistant and sunitinib-resistant patients treated with nilotinib or regorafenib. However, overall survival was not improved in these studies.
The ineffectiveness of second-generation TKIs with regard to overall survival in patients with resistance to imatinib or resistance to both imatinib and sunitinib may result from multiple lines of prior treatment. Indeed, in the nilotinib study, 16.5% of patients in the intent-to-treat population had had more than two prior lines of treatment,20 and 43% of patients in the regorafenib study had received three or more previous lines of anticancer therapy.11 A post hoc analysis of the true effect of nilotinib in a well defined patient population (with exactly one prior regimen each of imatinib and sunitinib) showed significantly improved overall survival in the nilotinib group (HR 0.67; 95% CI 0.48–0.95; P=0.02). The ineffectiveness of second-generation TKIs with regard to overall survival may also result from drug selection against KIT/PDGFRA mutation. It is known that about 10%–15% of adults with GIST do not have any mutations in the KIT and PDGFRA genes.28 Treatment with TKIs may eventually result in uncontrolled growth of wild-type KIT/PDGFRA that is resistant to TKI therapy. Due to the complexity of the pretreatment history and differences in mutational status in patients with advanced GIST, a well defined selection criterion is warranted in future clinical trial design to provide a more accurate evaluation of the clinical efficacy of second-generation TKIs.
With the efficacy data available for the subgroups in these studies, regorafenib was shown to be effective in progression-free survival across different subpopulations, including multiple lines of prior treatment, ethnic group, age, and different forms of KIT mutation.19 These results are comparable with those observed in the sunitinib study.11 Given the discrepant results for progression-free survival in the nilotinib study and the lack of efficacy data in the different subpopulations, regorafenib is a more promising candidate than nilotinib as a third-line treatment option for patients with GIST who are resistant to both imatinib and sunitinib.
Conclusion
Second-generation TKIs (sunitinib, nilotinib, and regorafenib) are effective for improving progression-free survival but not overall survival in patients with imatinib-resistant GIST. Nilotinib and regorafenib significantly improve progression-free survival, but are not effective in terms of overall survival in patients with GIST resistant to both imatinib and sunitinib. Regorafenib is a promising candidate as a third-line treatment option for patients with advanced GIST.
Acknowledgments
This study was funded by the Science and Technology Program of Changsha Science & Technology Bureau (K1205018-31); the Hunan Provincial Natural Science Foundation of China (12JJ5048), the Xiang Development and Reform Commission (No. 2012[1493]), and the Hunan Province Science and Technology (2013WK3029, 2012FJ3129).
Disclosure
The authors report no conflicts of interest in this work.
References
Miettinen M, Lasota J. Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med. 2008;130:1466–1478. | |
Corless CL, Barnett CM, Heinrich MC. Gastrointestinal stromal tumours: origin and molecular oncology. Nat Rev Cancer. 2011;11:865–878. | |
Mullady DK, Tan BR. A multidisciplinary approach to the diagnosis and treatment of gastrointestinal stromal tumor. J Clin Gastroenterol. 2013;47:578–585. | |
Angelini S, Ravegnini G, Fletcher JA, Maffei F, Hrelia P. Clinical relevance of pharmacogenetics in gastrointestinal stromal tumor treatment in the era of personalized therapy. Pharmacogenomics. 2013;14:941–956. | |
Heinrich MC, Corless CL, Demetri GD, et al. Kinase mutations and imatinib response in patients with metastatic gastrointestinal stromal tumor. J Clin Oncol. 2003;21:4342–4349. | |
Judson I, Leahy M, Whelan J, et al. A guideline for the management of gastrointestinal stromal tumour (GIST). Sarcoma. 2002;6:83–87. | |
Antonescu CR. The GIST paradigm: lessons for other kinase-driven cancers. J Pathol. 2011;223:251–261. | |
Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;347:472–480. | |
Antonescu CR, Besmer P, Guo T, et al. Acquired resistance to imatinib in gastrointestinal stromal tumor occurs through secondary gene mutation. Clin Cancer Res. 2005;11:4182–4190. | |
Gounder MM, Maki RG. Molecular basis for primary and secondary tyrosine kinase inhibitor resistance in gastrointestinal stromal tumor. Cancer Chemother Pharmacol. 2011;67:S25–S43. | |
Demetri GD, van Oosterom AT, Garrett CR, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomized controlled trial. Lancet. 2006;368:1329–1338. | |
Demetri GD, Garrett CR, Schöffski P, et al. Complete longitudinal analyses of the randomized, placebo-controlled, phase III trial of sunitinib in patients with gastrointestinal stromal tumor following imatinib failure. Clin Cancer Res. 2012;18:3170–3179. | |
Abrams TJ, Lee LB, Murray LJ, Pryer NK, Cherrington JM. SU11248 inhibits KIT and platelet-derived growth factor receptor beta in preclinical models of human small cell lung cancer. Mol Cancer Ther. 2003;2:471–478. | |
Mendel DB, Laird AD, Xin X, et al. In vivo antitumor activity of SU11248, a novel tyrosine kinase inhibitor targeting vascular endothelial growth factor and platelet-derived growth factor receptors: determination of a pharmacokinetic/pharmacodynamic relationship. Clin Cancer Res. 2003;9:327–337. | |
Le Cesne A, Blay JY, Bui BN, et al. Phase II study of oral masitinib mesilate in imatinib-naïve patients with locally advanced or metastatic gastro-intestinal stromal tumour (GIST). Eur J Cancer. 2010;46:1344–1351. | |
Benjamin RS, Schöffski P, Hartmann JT, et al. Efficacy and safety of motesanib, an oral inhibitor of VEGF, PDGF and Kit receptors, in patients with imatinib-resistant gastrointestinal stromal tumors. Cancer Chemother Pharmacol. 2011;68:69–77. | |
Park SH, Ryu MH, Ryoo BY, et al. Sorafenib in patients with metastatic gastrointestinal stromal tumors who failed two or more prior tyrosine kinase inhibitors: a phase II study of Korean gastrointestinal stromal tumors study group. Invest New Drugs. 2012;30:2377–2383. | |
Joensuu H, De Braud F, Grignagni G, et al. Vatalanib for metastatic gastrointestinal stromal tumour (GIST) resistant to imatinib: final results of a phase II study. Br J Cancer. 2011;104:1686–1690. | |
Demetri GD, Reichardt P, Kang YK, et al. Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID): an international, multicenter, randomized, placebo-controlled, phase 3 trial. Lancet. 2013;381:295–302. | |
Reichardt P, Blay JY, Gelderblom H, et al. Phase III study of nilotinib versus best supportive care with or without a TKI in patients with gastrointestinal stromal tumors resistant to or intolerant of imatinib and sunitinib. Ann Oncol. 2012;23:1680–1687. | |
Blay JY, von Mehren M. Nilotinib: a novel, selective tyrosine kinase inhibitor. Semin Oncol. 2011;38:S3–S9. | |
Manley PW, Drueckes P, Fendrich G, et al. Extended kinase profile and properties of the protein kinase inhibitor nilotinib. Biochim Biophys Acta. 2010;1804:445–453. | |
Wilhelm SM, Dumas J, Adnane L, et al. Regorafenib (BAY 73-4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int J Cancer. 2011;129:245–255. | |
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1–12. | |
The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. Available from: http://handbook.cochrane.org/. Accessed May 31, 2014. | |
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101. | |
Wang WL, Conley A, Reynoso D, et al. Mechanisms of resistance to imatinib and sunitinib in gastrointestinal stromal tumor. Cancer Chemother Pharmacol. 2011;67:S15–S24. | |
Nannini M, Biasco G, Astolfi A, Pantaleo MA. An overview on molecular biology of KIT/PDGFRA wild type (WT) gastrointestinal stromal tumours (GIST). J Med Genet. 2013;50:653–661. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.