")
Back to Journals » Infection and Drug Resistance » Volume 14
Clinical Efficacy of Cefoperazone-Sulbactam versus Piperacillin-Tazobactam in the Treatment of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia
Authors Chen CH , Tu CY, Chen WC, Kuo LK, Wang YT, Fu PK, Ku SC , Fang WF, Chen CM, Lai CC
Received 8 April 2021
Accepted for publication 9 June 2021
Published 16 June 2021 Volume 2021:14 Pages 2251—2258
DOI https://doi.org/10.2147/IDR.S313828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chia-Hung Chen,1 Chih-Yen Tu,1 Wei-Chih Chen,2 Li-Kuo Kuo,3 Yao-Tung Wang,4 Pin-Kuei Fu,5 Shih-Chi Ku,6 Wen-Feng Fang,7 Chin-Ming Chen,8 Chih-Cheng Lai9
1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan; 2Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan; 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan; 4Division of Pulmonary Medicine, Department of Internal Medicine, Chung Shan Medical University Hospital, Taichung, Taiwan; 5Department of Critical Care Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 6Division of Chest Medicine, Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan; 7Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 8Department of Intensive Care Medicine, Chi Mei Medical Center, Tainan, Taiwan; 9Department of Internal Medicine, Kaohsiung Veterans General Hospital, Tainan Branch, Tainan, Taiwan
Correspondence: Chih-Cheng Lai Email [email protected]
Objective: The aim of this study was to compare the usefulness of cefoperazone-sulbactam and that of piperacillin-tazobactam in the treatment of hospital-acquired pneumonia (HAP) and ventilator-associated pneumonia (VAP).
Methods: This retrospective study included the adult patients receiving cefoperazone-sulbactam or piperacillin-tazobactam against HAP/VAP in nine hospitals in Taiwan from March 1, 2018 to May 30, 2019. Primary outcome was clinical cure rate.
Results: A total of 410 patients were enrolled. Among them, 209 patients received cefoperazone-sulbactam and 201 patients received piperacillin-tazobactam. Overall, cefoperazone-sulbactam group had similar distribution of age, sex, or SOFA scores as piperacillin-tazobactam group. However, cefoperazone-sulbactam had higher comorbidity score and disease severity than piperacillin-tazobactam group (Charlson score: 6.5 ± 2.9 vs 5.7 ± 2.7, p < 0.001; APACHE II score: 21.4 ± 6.2 vs 19.3 ± 6.0, p = 0.002). Regarding clinical outcomes, no significant difference in clinical cure and failure rates was observed between cefoperazone-sulbactam and piperacillin-tazobactam group (clinical cure rate: 80.9% vs 80.1% and clinical failure rate: 17.2% vs 18.4%, p = 0.943). Moreover, no significant difference in clinical effectiveness and ineffectiveness rates was observed between cefoperazone-sulbactam and piperacillin-tazobactam group (clinical effective rate: 80.9% vs 80.6% and clinical ineffective rate: 17.7% vs 18.9%, p = 0.711). The all-cause mortality rates of the cefoperazone-sulbactam and piperacillin-tazobactam groups were similar (23.9% vs 20.9%, p = 0.48). After adjustment of Charlson score and APACHE II score, the similarities in these clinical outcomes did not change in overall patients and patients with HAP or VAP.
Conclusion: For treating adult patients with nosocomial pneumonia, cefoperazone-sulbactam was as effective as piperacillin-tazobactam.
Keywords: cefoperazone-sulbactam, hospital-acquired pneumonia, piperacillin-tazobactam, ventilator-associated pneumonia
Introduction
Hospital-acquired pneumonia (HAP) is the most common type of hospital-acquired infections,1,2 and ventilator-associated pneumonia (VAP) is also a common type of infection in intensive care units (ICUs).3 Importantly, both HAP and VAP are associated with high morbidity, mortality, and health-care expenditure.2–4 Although administration of appropriate antibiotics remains the most important treatment for patients with HAP/VAP,2,3 the emergence of antibiotic resistance among causative pathogens—multidrug resistant organisms (MDROs)—has largely limited therapeutic options. Gram-negative bacilli (GNB), such as Pseudomonas aeruginosa and Enterobacteriaceae, play an important role in HAP/VAP,5–7 and many kinds of antibiotic-resistance mechanism have been detected among these pathogens.8,9 Therefore, a combination of ß-lactam and ß-lactamase inhibitor as a broad-spectrum antibiotic was recommended as one of therapeutic options in the treatment of HAP/VAP.
Cefoperazone-sulbactam is one of combinations of ß-lactam and ß-lactamase inhibitors.10 Many studies have demonstrated its potent in vitro activity against commonly encountered respiratory pathogens and also MDROs, including ESBL-producing Escherichia coli and Klebsiella pneumoniae.10–15 However, very few clinical studies have assessed the effectiveness of cefoperazone-sulbactam for the treatment of HAP/VAP.16,17 We conducted this study to compare the clinical efficacy of cefoperazone-sulbactam with that of piperacillin-tazobactam, which is another commonly used ß-lactam and ß-lactamase inhibitor antibiotic in the treatment of HAP/VAP.
Methods
Study Design and Data Collection
This study was based on retrospective analyses, using clinical information extracted from BATTLE study, which investigated the efficacy and safety of Brosym® (TTY Biopharm Company, Taiwan) in the treatment of adult patients with severe community-acquired pneumonia (SCAP) and nosocomial pneumonia. The patients enrolled in BATTLE study were those receiving empirical cefoperazone-sulbactam or piperacillin-tazobactam for treating SCAP, HAP and VAP, in which study subjects were identified from the electronic database in each study sites. BATTLE study was conducted in eight medical centers and one regional hospital in Taiwan between March 2018 and May 2019. All three hospitals were located in north, central, and south Taiwan. The present study evaluated the clinical efficacy of cefoperazone-sulbactam or piperacillin-tazobactam for the treatment of HAP or VAP. The diagnosis of pneumonia was made based on the newly developed or progressive radiographic lung infiltration/consolidation in patients with 2 or more of the following: cough, fever, hypothermia, purulent sputum or respiratory secretion, and characteristic physical signs.3 In each study site, respiratory specimens and blood were routinely sampling for culture before prescribing antibiotics. In patients with HAP, pneumonia developed ≥ 48 hours after hospitalization; whereas in patients with VAP, pneumonia developed after receiving mechanical ventilation for more than 48 hours.3 In this study, primary dose of cefoperazone-sulbactam (1 gram/1 gram) was 4 g every 12 hours and piperacillin-tazobactam (2 gm/250 mg) was 4.5 g every 8 hours before dose adjustment according to renal function. Data pertaining to the demographic characteristics of the patients, their underlying disease/conditions, disease severity, microbiological information, antibiotic treatment, and clinical outcomes were retrospectively collected after obtaining approval from local ethics committees or institutional review boards. Informed consent was not required by the approving ethics committees because all data were collected on a routine basis, and the analysis was conducted retrospectively. All methods, including patient data confidentiality, were performed in accordance with the Declaration of Helsinki.
Outcome
The primary outcome measured was clinical cure rate, which was defined as the proportion of patients in which the clinical symptoms or signs resolved or improved 7 days after the end of treatment, and in which no additional antibiotics were required. In contrast, clinical failure was defined as one of the following scenarios: clinical symptoms or signs deteriorated or persisted during treatment and required additional antibiotics for management; death due to pneumonia after 3 days of antibiotic treatment; or the development of complications, such as empyema or a lung abscess. An indeterminate outcome was defined as one of the following: the patient was transferred to another hospital or refused further treatment; death due to pneumonia within 2 days of antibiotic treatment; death due to a cause other than pneumonia during treatment; or incomplete treatment due to allergy, severe adverse events, or other personal reasons. The secondary outcomes measured were the clinical effective rate, the risk of adverse events, and in-hospital mortality. Clinical effectiveness was defined as the improvement of clinical symptoms and signs; radiographic findings; or inflammation markers, such as white blood cell counts, procalcitonin, or c-reactive protein levels. Ineffectiveness was defined as when any one of the three criteria listed above was not achieved. Indeterminate effectiveness was defined as when the above three criteria could not be assessed.
Statistical Analysis
Continuous variables are reported as the mean and standard deviation (SD). Categorical variables are presented as frequency counts with percentages. The differences in baseline characteristics and clinical variables between the cefoperazone-sulbactam and piperacillin-tazobactam groups were evaluated using the Fisher’s exact test (for continuous variables) and the Wilcoxon rank sum test (for categorical variables). Significance was set at p <0.05 (two-tailed). Differences in the crude relative risk (RR) and adjusted RR (adjusted for propensity score) of the outcomes between the cefoperazone-sulbactam and piperacillin-tazobactam groups were calculated using Statistical Analysis System® (SAS) for Windows (Version 9.4 or higher, SAS Institute, Cary, North Carolina, USA).
Results
Demographic Data
During the study period, 410 patients (n = 345 in HAP, n = 65 in VAP) were enrolled. Of these, 209 patients received cefoperazone-sulbactam and 201 patients received piperacillin-tazobactam. The mean age of patients receiving cefoperazone-sulbactam was 75.1 ± 14.8 years and 141 (67.5%) were male. The median treatment duration was 9.0 days. Their Charlson, APACHE II, and SOFA scores were 6.5 (± 2.9), 21.4 (± 6.2), and 5.3 (± 2.9), respectively. Patients who received cefoperazone-sulbactam had higher occurrences of myocardial infarction, stroke and dementia than patients receiving piperacillin-tazobactam (all p < 0.05). In addition, the Charlson and APACHE II score were significantly higher in cefoperazone-sulbactam group than piperacillin-tazobactam group. In contrast, there were no significant differences in age, sex, or SOFA scores between patients receiving cefoperazone-sulbactam and piperacillin-tazobactam (Table 1).
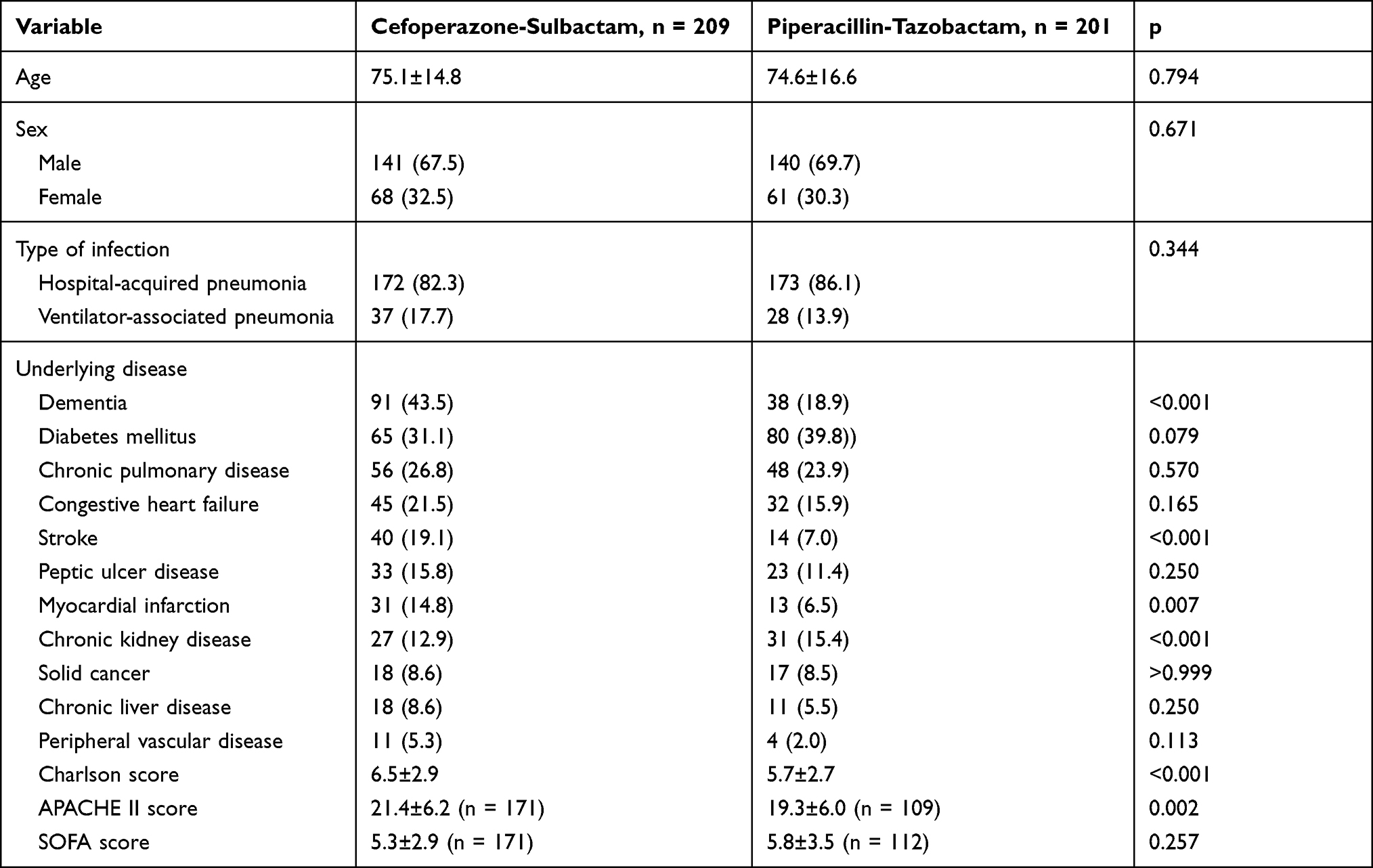 |
Table 1 Demographic Characteristics of the Patients Receiving Cefoperazone-Sulbactam and Piperacillin-Tazobactam |
Microbiologic Distribution
For all patients, blood and respiratory specimens were sampled for culture to identify pathogens; however, only 64.1% (n = 134) of cefoperazone-sulbactam group and 39.3% (n = 79) of piperacillin-tazobactam group had identified pathogens. In the cefoperazone-sulbactam group, P. aeruginosa (18.2%, n = 38) and Acinetobacter spp. (17.6%, n = 36) were the most common bacteria, followed by K. pneumoniae (17.2%, n = 32). Similar findings were observed in patients receiving piperacillin-tazobactam; the most common bacteria were P. aeruginosa (9.5%), followed by Acinetobacter spp. (9.0%) and K. pneumoniae (6.5%) (Table 2). In addition, concomitant bacteremia was found in 5.2% (n = 11) and 10.9% (n = 22) of patients receiving cefoperazone-sulbactam and piperacillin-tazobactam, respectively. No significant difference was observed in terms of microbiologic distribution and the incidence of concomitant bacteremia (all p > 0.05).
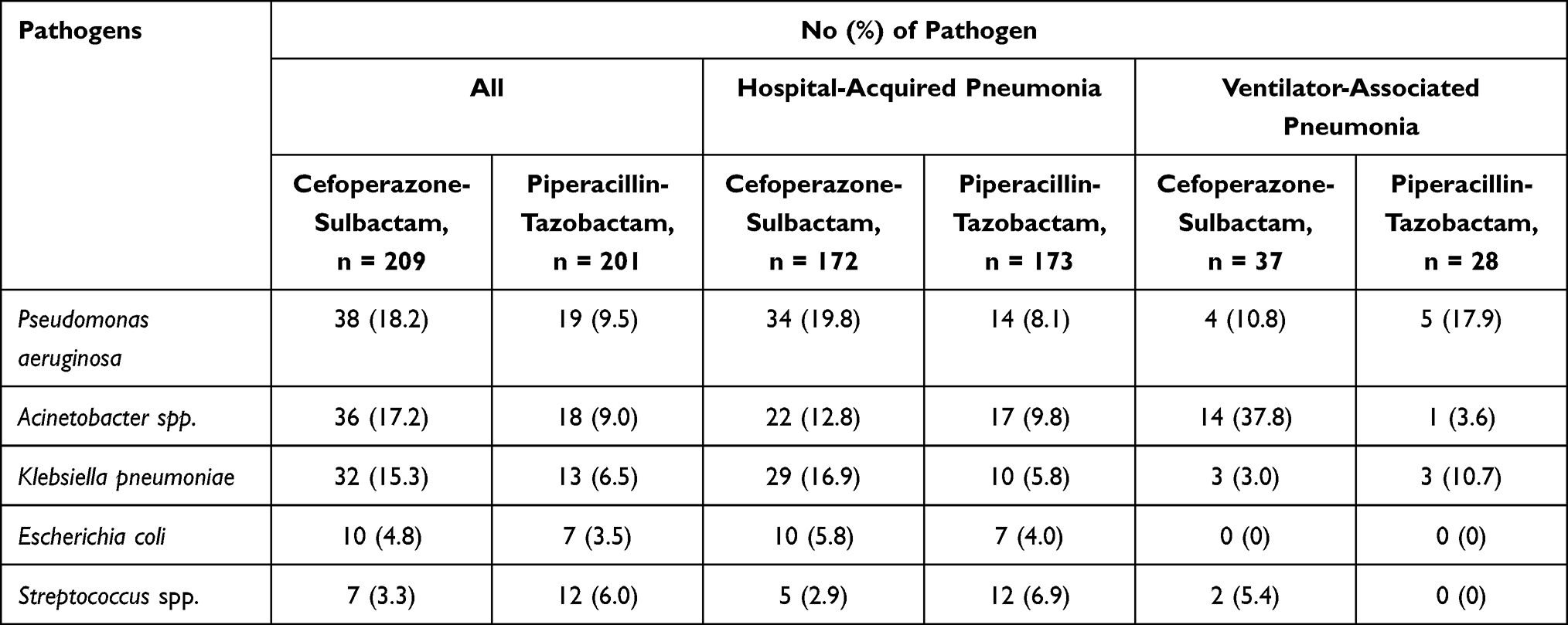 |
Table 2 Microbiological Distribution of Major Pathogens |
Outcomes
Cefoperazone-sulbactam group had their clinical cure rate of 80.9% and the clinical failure rate was 17.2%. Overall, these clinical outcomes of cefoperazone-sulbactam group were similar to those of piperacillin-tazobactam group (p = 0.943). Regarding secondary outcomes, the cefoperazone-sulbactam group had a clinical effective rate of 80.9% and an ineffective rate of 17.7%, which were similar to piperacillin-tazobactam group (p = 0.711). The all-cause mortality of the cefoperazone-sulbactam group and piperacillin-tazobactam was similar, too (23.9% vs 20.9%, p = 0.480). A similar trend was observed for pneumonia-related mortality (cefoperazone-sulbactam vs piperacillin-tazobactam, 12.9% vs 9.0%, p = 0.304; Table 3). Subgroup analysis based on the different study sites revealed no significant differences in the primary outcome (the clinical cure rate) or secondary outcomes (the clinical effective rate, in-hospital mortality, and pneumonia-related mortality) between patients who received cefoperazone-sulbactam and piperacillin-tazobactam in each hospital (data not shown, all p > 0.05). However, one site only enrolled patients in the cefoperazone-sulbactam group. In addition, the clinical outcome and mortality between patients receiving cefoperazone-sulbactam and piperacillin for HAP and VAP was similar (Figures 1 and 2). Among HAP patients, patients receiving cefoperazone-sulbactam had less requirement of mechanical ventilation (MV) and further ICU admission than those receiving piperacillin-tazobactam (MV use: 18.0% versus 34.7%, p = 0.0007; ICU admission: 15.1% versus 36.4%, p < 0.0001). Moreover, the clinical cure rate between cefoperazone-sulbactam and piperacillin-tazobactam group did not differ for causative pathogens, including E. coli (90.0% [9/10] vs 71.4% [5/7]), K. pneumoniae (81.3% [26/32] vs 76.9% [10/13]), P. aeruginosa (76.3% [29/38] vs 78.9% [15/19]) and Acinetobacter spp. (77.8% [28/36] vs 61.1% [11/18]) (all p > 0.05). Regarding the adverse events, only one patient in cefoperazone-sulbactam group had skin rash and two patients in piperacillin-tazobactam had diarrhea group. Among cefoperazone-sulbactam group, only 30 patients had received international normalized ratio (INR) test during both pre- and post-treatment after one week. No significant difference between the pre- and post-treatment INR was found in this population (1.10 ± 0.15 versus 1.19 ± 0.21, p = 0.06) and no significant bleeding was reported in both groups.
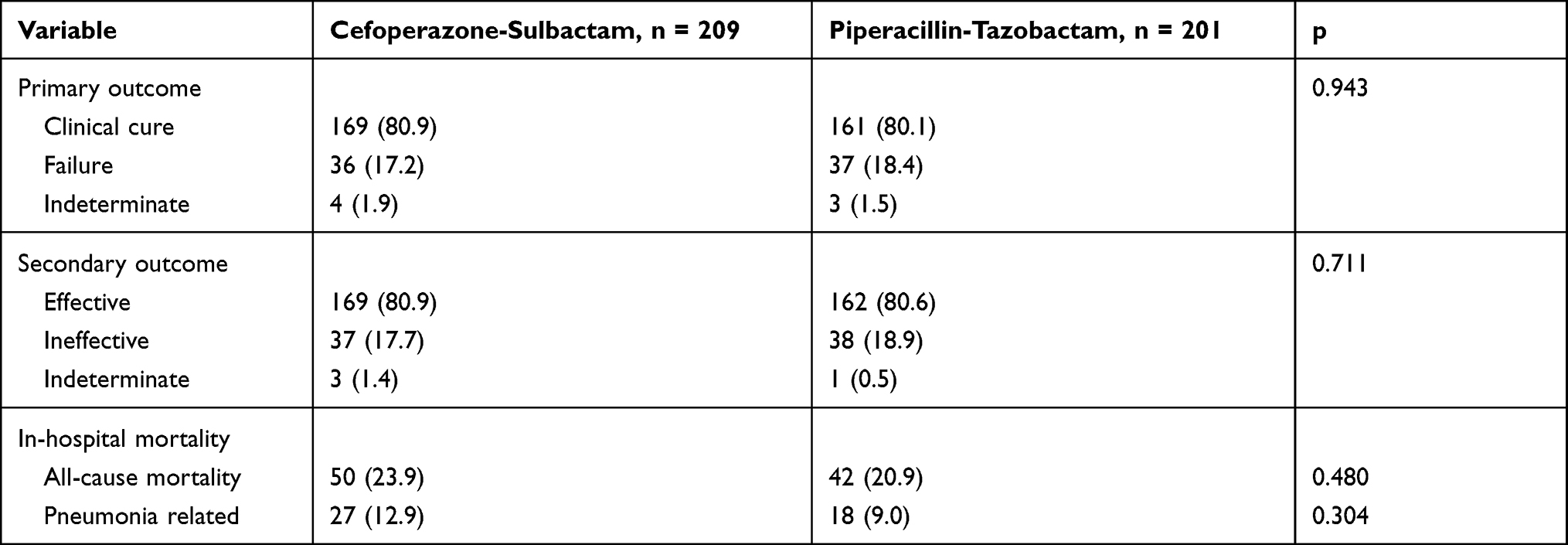 |
Table 3 Clinical Outcomes Between Cefoperazone-Sulbactam and Piperacillin-Tazobactam Groups |
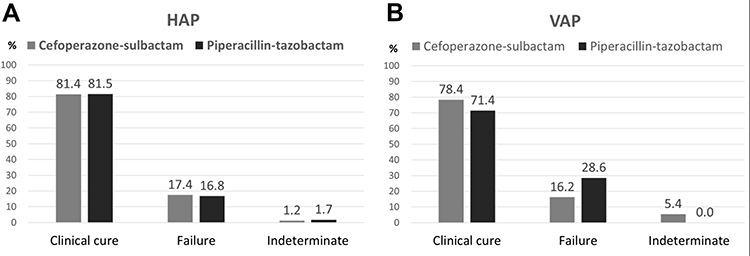 |
Figure 1 Clinical outcome of patients receiving cefoperazone-sulbactam and piperacillin-tazobactam for hospital-acquired pneumonia (HAP) (A) and ventilator-associated pneumonia (VAP) (B). |
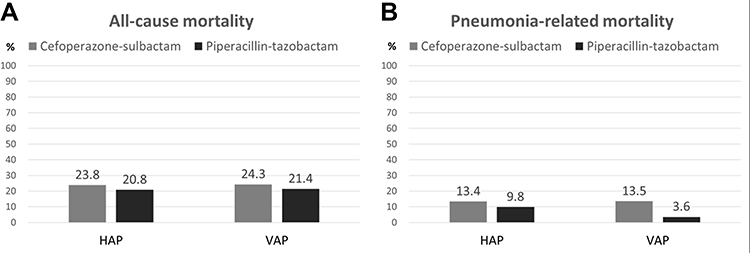 |
Figure 2 All-cause mortality (A) and pneumonia-related mortality (B) of patients receiving cefoperazone-sulbactam and piperacillin-tazobactam for hospital-acquired pneumonia (HAP) and ventilator associated pneumonia (VAP). |
Outcome Analysis
Because different comorbidities and disease severity were found between the cefoperazone-sulbactam and piperacillin-tazobactam groups, we used propensity score method to adjust for these two confounding factors. After adjusting the APACHE II and Charlson scores, the clinical cure rate of cefoperazone-sulbactam remained comparable to that of piperacillin-tazobactam (adjusted RR [aRR], 0.93; 95% confidence interval [95% CI], 0.82–1.05) in the overall population (Table 3). No significant difference was observed in terms of the clinical cure rate of cefoperazone-sulbactam and piperacillin-tazobactam in the treatment patients with HAP (aRR, 0.89; 95% CI, 0.77–1.03), and VAP (aRR, 1.33; 95% CI, 0.33–1.92) (Table 4). Regarding secondary outcomes, cefoperazone-sulbactam was comparable to piperacillin in terms of clinical efficacy rate, in-hospital mortality, and pneumonia-related mortality, which remained unchanged in the overall population, HAP, and VAP groups (Table 3).
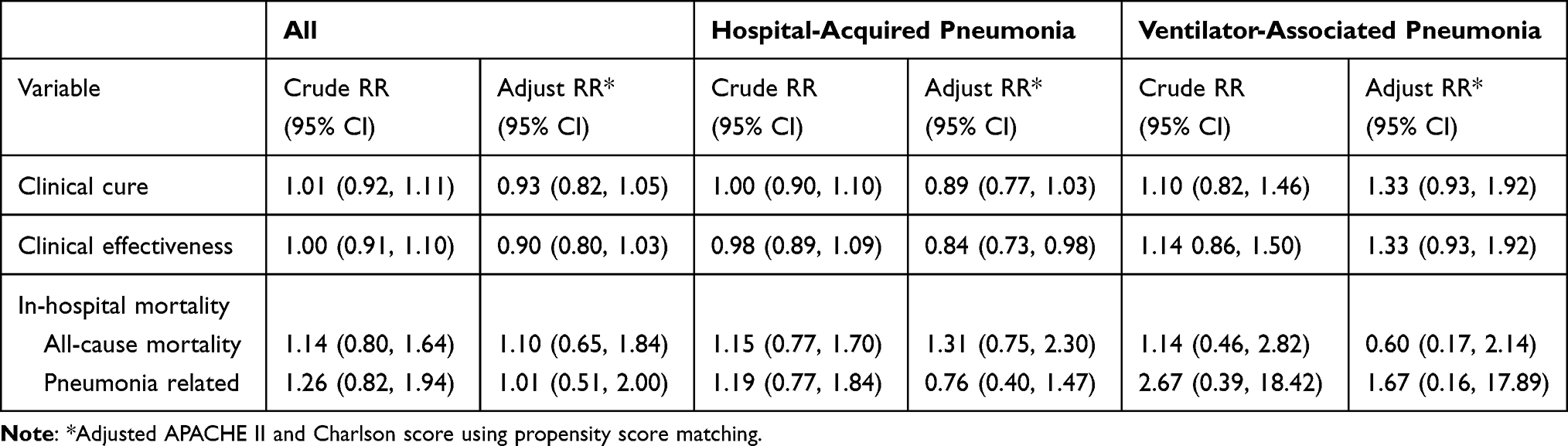 |
Table 4 Outcome Analysis |
Discussion
This retrospective study determined the clinical efficacy of cefoperazone-sulbactam for treating patients with HAP/VAP; it was comparable to piperacillin-tazobactam in terms of both primary and secondary outcomes. First, the clinical cure and failure rate of cefoperazone-sulbactam were similar to those of piperacillin-tazobactam. Moreover, there was no statistically significant difference between the clinical effective and ineffective rates of cefoperazone-sulbactam and piperacillin-tazobactam. Second, the all-cause and pneumonia-related mortality of patients receiving cefoperazone-sulbactam was similar to that of patients receiving piperacillin-tazobactam. Third, cefoperazone-sulbactam was found to be comparable to piperacillin-tazobactam in all analyses, including the subgroup analysis based on the study sites, causative pathogens and the HAP and VAP groups. Finally, after adjustment for Charlson and APACHE II scores, cefoperazone-sulbactam exhibited similar clinical outcomes compared with piperacillin-tazobactam in the HAP/VAP, HAP, and VAP groups. Furthermore, the mortality rate of HAP/VAP, when treated with cefoperazone-sulbactam, was 23.9%, which was consistent with the findings of previous studies.7,18,19 Similar to the findings of the ASPECT-NP trial,7 the rates of 28-day all-cause mortality in patients with nosocomial pneumonia were 24.0% (87/362) and 25.3% (92/364) among the ceftolozane-tazobactam and meropenem groups, respectively. A similar finding was shown in another retrospective analysis of patients with HAP/VAP, in which the 30-day mortality was 18.1%–22.8%.18 Therefore, our results suggest that cefoperazone-sulbactam, like piperacillin-tazobactam, could be an effective therapeutic option for the management of patients with HAP/VAP.
In this study, P. aeruginosa, Acinetobacter spp., and K. pneumoniae were found to be the most common pathogens causing HAP/VAP, which was in line with previous studies.7,19–21 In the REPROVE trial,6 P. aeruginosa and K. pneumoniae were the most common GNBs causing nosocomial pneumonia, followed by Enterobacter cloacae and E. coli, whereas, in the ASPECT-NP trial,7 Enterobacteriaceae and P. aeruginosa were the predominant gram-negative pathogens. Together, these findings suggest that broad-spectrum antibiotics should be used in the treatment of HAP/VAP, to ensure they act against these prevalent pathogens. An in vitro study22 showed that the susceptibility rates of E. coli, K. pneumoniae, Citrobacter freundii, Serratia marcescens, and Proteus mirabilis to cefoperazone-sulbactam were all ≥90%, and only ≤15% of P. aeruginosa, Acinetobacter spp., and Enterobacter cloacae strains were resistant to cefoperazone-sulbactam. Even for MDROs, the susceptibility rates of ESBL- E. coli, ESBL- K. pneumoniae, carbapenem-resistant E. coli, and carbapenem-resistant A. baumannii to cefoperazone-sulbactam were 97.0%, 75.8%, 67.6% and 68%, respectively.23 Only carbapenem-resistant P. aeruginosa displayed high resistance against cefoperazone-sulbactam.11,23 Therefore, cefoperazone-sulbactam could be an appropriate antibiotic for patients the treatment of patients with HAP/VAP caused by most GNBs.
Safety, especially in the context of coagulopathy, is a serious concern for clinicians prescribing cefoperazone-sulbactam.24–26 No significant difference in pre- and post-treatment INR was observed in 30 patients receiving cefoperazone, but most of the patients did not have the assessment of coagulation disorder in this study. According to retrospective review of medical chart, no patients receiving cefoperazone-sulbactam had significant bleeding. In addition, only one patient reported skin rash during the use of cefoperazone-sulbactam, but no serious adverse events related to cefoperazone-sulbactam were reported in this retrospective study. Therefore, based on the present findings, cefoperazone-sulbactam was well tolerated.
This study had several limitations. First, unlike a randomized controlled study, this retrospective study could not ensure that baseline characteristics and disease severity were equal between the cefoperazone-sulbactam and piperacillin-tazobactam groups. Therefore, we used propensity score method to adjust the baseline characteristics and disease severity and showed that the clinical efficacy of cefoperazone-sulbactam remained comparable to piperacillin-tazobactam. Second, because the in vitro activity of cefoperazone-sulbactam was not assessed in most study sites, only 18 clinical isolates had results of cefoperazone-sulbactam susceptibility tests, and two of them, including one P. aeruginosa and one K. pneumoniae isolates were not susceptible to cefoperazone-sulbactam. Therefore, we were unable to evaluate the cefoperazone-sulbactam resistance rate of causative pathogens and their impact on the clinical outcome. In addition, susceptibility of GNB could vary according to different sites, so the results of this comparison should be different and empirical treatment of late HAP/VAP should be made based on the local epidemiology. Third, although the risk of adverse events was evaluated in this study, some mild adverse events which may not have been recorded in the chart could have been missed. Thus, the risk of adverse events might have been underestimated. Forth, this study did not further classify the type of VAP – early or late VAP and did not measure the microbiological eradication rate. Further large-scale study is warranted to investigate these issues. Finally, most of subgroup analyses were based on small number, which might contribute to non-difference on the treatment outcome.
Conclusions
In the management of adult patients with HAP/VAP, cefoperazone-sulbactam is as effective as piperacillin-tazobactam.
Ethical Approval
This study was approved by the ethics committee of Taipei Veterans General Hospital (2019-08-006AC), Mackay Memorial Hospital (19MMHIS282e), Chung Shan Medical University Hospital (CS18126), Taichung Veterans General Hospital (CE18223A#2), National Taiwan University Hospital (201805123RINB), Kaohsiung Chang Gung Memorial Hospital (201900932B0C501), Chi Mei Medical Center (10806-008) and Chi Mei Medical Center, Liouying (10808-L01).
Acknowledgments
The abstract of this paper was presented at 2020 Annual Congress of Taiwan Society of Pulmonary and Critical Care Medicine and Taiwan Society of Thoracic Surgeons, Taiwan Association of Thoracic & Cardiovascular Surgery Joint Conference – Cefoperazone-sulbactam versus piperacillin-tazobactam in the treatment of nosocomial pneumonia with interim findings.
Funding
No funding was received.
Disclosure
The authors declare that they have no competing interests.
References
1. Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. 2014;370:1198–11208. doi:10.1056/NEJMoa1306801
2. Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61–e111.
3. Chou CC, Shen CF, Chen SJ, et al. Infectious Diseases Society of Taiwan; Taiwan Society of Pulmonary and Critical Care Medicine, Medical Foundation in Memory of Dr. Deh-Lin Cheng;; Foundation of Professor Wei-Chuan Hsieh for Infectious Diseases Research and Education;; CY Lee’s Research Foundation for Pediatric Infectious Diseases and Vaccines,; 4th Guidelines Recommendations for Evidence-based Antimicrobial agents use in Taiwan (GREAT) working group. Recommendations and guidelines for the treatment of pneumonia in Taiwan. J Microbiol Immunol Infect. 2019;52:172–99. doi:10.1016/j.jmii.2018.11.004
4. Kollef MH, Hamilton CW, Ernst FR. Economic impact of ventilator-associated pneumonia in a large matched cohort. Infect Control Hosp Epidemiol. 2012;33:250–256. doi:10.1086/664049
5. Jones RN. Microbial etiologies of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Clin Infect Dis. 2010;51:S81–7. doi:10.1086/653053
6. Torres A, Zhong N, Pachl J, et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): a randomised, double-blind, Phase 3 non-inferiority trial. Lancet Infect Dis. 2018;18:285–295. doi:10.1016/S1473-3099(17)30747-8
7. Kollef MH, Nováček M, Kivistik Ü, et al. Ceftolozane-tazobactam versus meropenem for treatment of nosocomial pneumonia (ASPECT-NP): a randomised, controlled, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2019;19:1299–1311. doi:10.1016/S1473-3099(19)30403-7
8. MacVane SH. Antimicrobial resistance in the intensive care unit: a focus on gram-negative bacterial infections. J Intensive Care Med. 2017;32:25–37. doi:10.1177/0885066615619895
9. Kaye KS, Pogue JM. Infections caused by resistant gram-negative bacteria: epidemiology and management. Pharmacotherapy. 2015;35:949–962. doi:10.1002/phar.1636
10. Lai CC, Chen CC, Lu YC, Lin TP, Chuang YC, Tang HJ. Appropriate composites of cefoperazone-sulbactam against multidrug-resistant organisms. Infect Drug Resist. 2018;11:1441–1445. doi:10.2147/IDR.S175257
11. Lai CC, Chen CC, Lu YC, Chuang YC, Tang HJ. In vitro activity of cefoperazone and cefoperazone-sulbactam against carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa. Infect Drug Resist. 2019;12:25–29. doi:10.2147/IDR.S181201
12. Sheu MJ, Chen CC, Lu YC, et al. In vitro antimicrobial activity of various cefoperazone/sulbactam products. Antibiotics (Basel). 2020;9(2):77. doi:10.3390/antibiotics9020077
13. Patankar M, Sukumaran S, Chhibba A, Nayak U, Sequeira L. Comparative in-vitro activity of cefoperazone-tazobactam and cefoperazone-sulbactam combinations against ESBL pathogens in respiratory and urinary infections. J Assoc Physicians India. 2012;60:22–24.
14. Sader HS, Carvalhaes CG, Streit JM, Castanheira M, Flamm RK. Antimicrobial activity of cefoperazone-sulbactam tested against Gram-Negative organisms from Europe, Asia-Pacific, and Latin America. Int J Infect Dis. 2020;91:32–37. doi:10.1016/j.ijid.2019.11.006
15. Xia J, Zhang D, Xu Y, Gong M, Zhou Y, Fang X. A retrospective analysis of carbapenem-resistant Acinetobacter baumannii-mediated nosocomial pneumonia and the in vitro therapeutic benefit of cefoperazone/sulbactam. Int J Infect Dis. 2014;23:90–93. doi:10.1016/j.ijid.2014.01.017
16. Liu JW, Chen YH, Lee WS, et al. Randomized noninferiority trial of cefoperazone-sulbactam versus cefepime in the treatment of hospital-acquired and healthcare-associated pneumonia. Antimicrob Agents Chemother. 2019;63:e00023–19. doi:10.1128/AAC.00023-19
17. Xin X, Jian L, Xia X, et al. A multicentre clinical study on the injection of ceftriaxone/sulbactam compared with cefoperazone/sulbactam in the treatment of respiratory and urinary tract infections. Ann Clin Microbiol Antimicrob. 2013;12:38. doi:10.1186/1476-0711-12-38
18. Liu WD, Shih MC, Chuang YC, Wang JT, Sheng WH. Comparative efficacy of doripenem versus meropenem for hospital-acquired and ventilator-associated pneumonia. J Microbiol Immunol Infect. 2019;52:788–795. doi:10.1016/j.jmii.2019.04.008
19. Chao CM, Chen CC, Huang HL, Chuang YC, Lai CC, Tang HJ. Clinical experience of patients receiving doripenem-containing regimens for the treatment of healthcare-associated infections. PLoS One. 2016;11:e0167522. doi:10.1371/journal.pone.0167522
20. Chung DR, Song JH, Kim SH, et al. High prevalence of multidrug-resistant nonfermenters in hospital-acquired pneumonia in Asia. Am J Respir Crit Care Med. 2011;184:1409–1417. doi:10.1164/rccm.201102-0349OC
21. Ismail B, Shafei MN, Harun A, Ali S, Omar M, Deris ZZ. Predictors of polymyxin B treatment failure in Gram-negative healthcare-associated infections among critically ill patients. J Microbiol Immunol Infect. 2018;51:763–769. doi:10.1016/j.jmii.2017.03.007
22. Jean SS, Liao CH, Sheng WH, Lee WS, Hsueh PR. Comparison of commonly used antimicrobial susceptibility testing methods for evaluating susceptibilities of clinical isolates of Enterobacteriaceae and nonfermentative gram-negative bacilli to cefoperazone-sulbactam. J Microbiol Immunol Infect. 2017;50:454–463. doi:10.1016/j.jmii.2015.08.024
23. Chang PC, Chen CC, Lu YC, et al. The impact of inoculum size on the activity of cefoperazone-sulbactam against multidrug resistant organisms. J Microbiol Immunol Infect. 2018;51:207–213. doi:10.1016/j.jmii.2017.08.026
24. Cai Z, Yang W, He Y, et al. Cefoperazone/sulbactam-induced abdominal wall hematoma and upper gastrointestinal bleeding: a case report and review of the literature. Drug Saf Case Rep. 2016;3:2. doi:10.1007/s40800-016-0025-9
25. Hu HR. Fatal Vitamin K-dependent coagulopathy associated with cefoperazone/sulbactam: a case report. Drug Saf Case Rep. 2019;6:6. doi:10.1007/s40800-019-0100-0
26. Wang W, Liu Y, Yu C, et al. Cefoperazone-sulbactam and risk of coagulation disorders or bleeding: a retrospective cohort study. Expert Opin Drug Saf. 2020;19:339–347. doi:10.1080/14740338.2020.1713090
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.