")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Efficacy and Safety Evaluation of Ceftazidime-Avibactam in the Treatment of Klebsiella pneumoniae Infection: A Retrospective Analysis from a Hospital in China
Authors Xu J , Luo C, Huang L, Xiao X, Liu L, Yang Z
Received 11 September 2023
Accepted for publication 4 November 2023
Published 14 November 2023 Volume 2023:16 Pages 7227—7237
DOI https://doi.org/10.2147/IDR.S435882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jia Xu,1,* Chengjia Luo,1,* Liang Huang,2 Xi Xiao,3 Ling Liu,1 Zhiling Yang1
1Department of Clinical Pharmacy, Hunan Provincial People’s Hospital (The First-Affiliated Hospital of Hunan Normal University), Changsha, 410016, People’s Republic of China; 2Department of Rehabilitation, Hunan Provincial People’s Hospital (The First-Affiliated Hospital of Hunan Normal University), Changsha, 410016, People’s Republic of China; 3Department of Clinical Laboratory, Hunan Provincial People’s Hospital (The First-Affiliated Hospital of Hunan Normal University), Changsha, 410016, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhiling Yang, Tel +86 0737-84762738, Email [email protected]
Background: Ceftazidime-avibactam (CAZ-AVI) is a new cephalosporin/β-lactamase inhibitor combination that received clinical approval in China in 2019. This study aims to investigate the efficacy and safety of CAZ-AVI in the treatment of Klebsiella pneumoniae (KP) infection in a hospital, and differences in efficacy among various infection sites and between monotherapy and combination therapy, providing valuable insights for its further application.
Methods: Patients who used CAZ-AVI between January 2019 and April 2023 were identified through the hospital information system. Demographic information, details of the infection site, KP strain’s drug sensitivity report, treatment duration, combination therapies, adverse drug reactions (ADR), and 28-day survival were recorded. Clinical and microbiological efficacies were analyzed using SPSS 23.0 software to compare different infection sites and combination therapies.
Results: The overall effective clinical response (CR) rate of CAZ-AVI against KP infection was 62.13%, with a favorable microbial response (MR) rate was 65.68% and a 28-day survival rate was 63.91%. No significant difference occurred in effective CR and 28-day survival rate among different infection sites (P = 0.709 and 0.862, respectively). The favorable MR rate for abdominal infections was slightly lower than that for other sites of infection (P = 0.021). No significant differences in effective CR, favorable MR, and 28-day survival between monotherapy and combination therapy were present (P values were 0.649, 0.123, and 0.280, respectively). The incidence of ADR was 1.78%, including increased creatinine, elevated transaminase, hematuria, and thrombocytopenia.
Conclusion: CAZ-AVI demonstrates good clinical efficacy and safety in the treatment of KP infections. The clinical efficacy of CAZ-AVI was similar across different infection sites, and combination therapy did not show an advantage over monotherapy. Further studies are warranted. It should be noted that CAZ-AVI may induce thrombocytopenia and hematuria.
Keywords: ceftazidime-avibactam, Klebsiella pneumoniae, carbapenem-resistant Enterobacteriaceae, urethral hemorrhage, thrombocytopenia, combination therapy
Introduction
Despite continuous improvement in living standards worldwide, infectious diseases remain a topic of public health concern. In recent years, the pandemic coronavirus disease 2019 (COVID-19) has led people to pay more attention to preventing and controlling infectious diseases.1 In addition to viral infections such as COVID-19, bacterial infections cause many human diseases; the emergence and continuous evolution of drug-resistant bacteria especially creates great difficulties in clinical treatment.2 In particular, the incidence of carbapenem-resistant organism (CRO) infections has shown a significant upward trend, which has become one of the major challenges in the medical field. The production of carbapenemases plays an essential role in carbapenem resistance. Since the genes that encode carbapenemases are located on plasmids and other mobile genetic elements, the determinants of carbapenem resistance have rapidly spread in many regions of the world.3 Data presented in Zhejiang Province, China, indicate that the prevalence of carbapenem-resistant Klebsiella pneumoniae (CRKP) has increased from 2.5% in 2008 to 15.8% in 2018, and this trend is further increasing among ICU patients.4,5 In addition, for patients with indwelling catheters, biofilm formation is another important mechanism of drug resistance in Klebsiella pneumoniae (KP).6,7 Previous studies have shown that Ethylenediaminetetraacetic acid (EDTA) can be used as an adjuvant against biofilms, and it has synergistic antibacterial effects with aztreonam, colistin, and ceftazidime-avibactam (CAZ-AVI).8–10
CAZ-AVI is a widely studied antimicrobial agent, originally developed by Pfizer Inc. for the treatment of drug-resistant bacterial infections. Its compound formulation consists of ceftazidime (CAZ) and avibactam (AVI). CAZ is a third-generation cephalosporin that targets gram-negative bacteria, particularly those in the Enterobacteriaceae family.11 AVI is a synthetic non-β-lactam, β-lactamase inhibitor that inhibits the activities of Ambler class A serine carbapenem enzymes such as Klebsiella pneumoniae carbapenemas [KPC], class C [AmpC] enzymes, and some class D [OXA] β-lactamases, but has no activity against class B [metallo-beta-lactamases] enzymes and almost no activity against Acinetobacter baumannii(AB).12,13 Since AVI inhibits carbapenem enzyme activity, CAZ-AVI is used to treat multidrug-resistant organisms (MDRO), especially carbapenem-resistant Enterobacteriaceae (CRE).14 CAZ-AVI was approved by the Food and Drug Administration (FDA) in the United States on 25 February 2015, and in the European Union (EU) on 24 June 2016. In China, CAZ-AVI was approved by the National Medical Products Administration (NMPA) on 21 May 2019. Approved adult indications include complex intra-abdominal infection (cIAI), hospital-acquired pneumonia (HAP), and the treatment of infections caused by gram-negative aerobic microorganisms in adult patients with limited treatment options.
CAZ-AVI has been widely used clinically since its development, and previous clinical studies have shown that it has good clinical and antimicrobial efficacy.15,16 However, few real-world studies on CAZ-AVI exist, especially for KP infection. In addition, drug resistance to CAZ-AVI has been reported in some regions.10,17,18 The purpose of this study is to retrospectively investigate the clinical efficacy and safety of CAZ-AVI against KP in a Chinese hospital, to investigate differences in the efficacy of CAZ-AVI for infection sites, and to investigate differences among different combination treatment schemes based on CAZ-AVI. This work will provide a reference for further clinical application of CAZ-AVI treatment use.
Materials and Methods
Study Design
A retrospective questionnaire was designed to collect basic information about patients, infection characteristics, pathogenic microorganism characteristics, drug use, clinical efficacy, drug-related adverse reactions, and other information. Cases retrieved from January 2019 to April 2023 with CAZ-AVI use indicated in the medical order information from the Hospital Information System (HIS) were screened according to the following inclusion and exclusion criteria.
Inclusion Criteria
a) The use of CAZ-AVI was confirmed by verified doctor’s order, and the medication time was ≥3 days. b) The attending doctor had diagnosed bacterial infection at the corresponding site according to guidelines, eg, pneumonia guidelines,19 abdominal infection guidelines,20 urinary tract infection guidelines,21 or positive blood culture. The main diagnostic points included fever and other symptoms of systemic infection or signs of local infection; imaging findings suggesting infection; systemic infection indicators such as from blood tests, procalcitonin (PCT), C-reactive protein (CRP), or local specimen examinations such as urine testing, specimen Gram staining, etc. suggesting the presence of bacterial infection. c) The pathogenic culture of qualified specimens indicated a single KP infection or multiple pathogenic bacteria, one of which was KP. d) If the infection site was suspected to be infected with gram-positive bacteria or the specimen culture suggested the presence of gram-positive bacteria such as MRSA, Enterococcus faecium, or Enterococcus faecalis, and it was treated with vancomycin, linezolid, and daptomycin, the case was also included in this study.
Exclusion Criteria
a) The doctor’s order information contained CAZ-AVI but it was not administered or was administered for <3 days. b) The culture of pathogenic microorganisms showed no KP. c) The culture of pathogenic microorganisms showed KP, but combined with the patient’s signs and laboratory examination, and considering the potential that the specimen was contaminated using pathogen colonization status, it was concluded that CAZ-AVI was given inappropriately, resulting in the inability to evaluate the curative effect. d) The dosage was not adjusted according to the requirements of the drug instructions based on the renal function (Cockcroft-Gault calculation formula), leading to inappropriate doses. e) Cases where the blood concentration of CAZ-AVI may have been affected by the combined use of probenecid, chloramphenicol, and other drugs during the medication period or medical measures such as hemofiltration or peritoneal dialysis.
Combination medication is defined as the antibiotics that were used before CAZ-AVI was started and continued to be used during the period of CAZ-AVI administration, or antibiotics added within 3 days after the start of CAZ-AVI.
Evaluation of Efficacy and Safety
In this study, the evaluation of the curative effect includes clinical and microbiological responses. Based on previous clinical trials of CAZ-AVI15,22 and our clinical practice knowledge, we divided clinical response (CR) into effective response, failure, and uncertainty. In this study, an effective response was defined as, following treatment with CAZ-AVI, the patient survived and the symptoms or signs of infection disappeared or significantly improved such that the infection index returned to normal or significantly decreased, allowing anti-infective treatment to be reduced or discontinued until discharge. Failure was defined as non-response to CAZ-AVI treatment for more than 3 days, including 1. Clinical symptoms and signs did not improve or worsened, bacterial infection indicators did not decrease or continued to rise, with ascending ladder antibiotics required, and 2. death resulted from the aggravation of infection after 5 days of treatment. Uncertainty was defined as the patient dying before the minimum course of treatment (<5 days) or CAZ-AVI treatment terminated because the patient was discharged from the hospital, resulting in unevaluated efficacy.
Microbial response (MR) was divided into favorable, unfavorable, and indeterminate responses. Favorable was defined as no KP was found in the follow-up specimen cultures from all infection sites or the follow-up specimen culture was not effective but the clinical response was evaluated as cured. Unfavorable was defined as microbiological culture showing persistence of KP or susceptibility results showing an increase in minimum inhibitory concentration (MIC) of CAZ-AVI relative to baseline MIC or inhibition zone diameter relative to baseline decreased, or if an effective specimen culture was not obtained but the CR was evaluated as treatment failure. Indeterminate was defined as failure to obtain an appropriate source sample for culture, and the subject’s CR was assessed as uncertain. The 28-day survival rate was also used to facilitate treatment efficacy evaluation. Cases with infection at a single site were screened, and differences in the CR and MR of CAZ-AVI at different infection sites were compared. Differences in CR and MR under different combination therapy regimens of CAZ-AVI were also analyzed. The Naranjo’s adverse drug reactions (ADRs) probability scale was used to evaluate the correlation of adverse events in the use of CAZ-AVI.23
Statistical Analysis
All statistical analyses were performed with the SPSS 23.0 statistical package (IBM Corp., Armonk, NY, USA). Values are presented as median (range) for continuous variables such as age and course of treatment, and number (% rate) for categorical variables. Differences among subgroups were assessed using P-values derived from the Pearson Chi-square test for the comparison of categorical variables. For all comparisons, P <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 275 cases with CAZ-AVI included in the medical order information were identified in the HIS. Based on the exclusion criteria, 106 cases were excluded, including 34 cases that did not use CAZ-AVI after verifying the doctor’s order information and 72 cases whose etiological culture was non-KP and the course of treatment was <3 days. Thus, 169 cases were included in this study. The basic information of 169 patients is shown in Table 1. Males accounted for 76.33% of patients included in the study and the median age was 57 years (range 14–96 years). Some patient cases were complicated with additional basic diseases, mostly, cardiovascular diseases, accounting for 44.28% of complex cases. Some patient cases (13.61%) were complicated by COVID-19 infection. In terms of the distribution of infection sites, mainly pulmonary, abdominal, and bloodstream infections were observed; patients with infection at the above sites accounted for 66.86%, 36.09%, and 30.18%, respectively. AB infection was present in 8.88% of patients and Pseudomonas aeruginosa (PA) infection in 5.92%. The median course of treatment for CAZ-AVI was 10 days (range 3–45 days). Patients treated only with CAZ-AVI made up 26.63% of study cases; 34.91% were combined with one antibiotic, 38.46% were combined with more than two antibiotics, and the maximum combination used five drugs including anti-gram-positive bacteria and fungal drugs.
 |
Table 1 Basic Demographic Characteristics of Patients, Infection Status, and Characteristics of Combined Use (n=169) |
Drug-Resistant Characteristics of KP and the Detection of Carbapenem-Resistant Genes
A total of 179 strains of KP were obtained from the infection sites of 169 patients, and the resistance rate of KP to various antibiotics was calculated, as shown in Figure 1, using the Kirby-Bauer disk diffusion method. Using a 30/20 µg drug sensitivity test paper, a bacteriostatic zone diameter of ≤20 mm was judged as drug resistance, and a bacteriostatic zone diameter ≥21 mm was judged as sensitive. The MIC of other antimicrobials was estimated using the microbroth dilution method and the determination standard from the Clinical and Laboratory Standards Institute (CLSI). Of the 179 KP strains collected, 125 strains were tested for sensitivity to CAZ-AVI, and the resistance rate to CAZ-AVI was 3.2%. A drug sensitivity test to tigecycline was carried out in 164 cases, and the resistance rate was 50.00%. In addition, the resistance rates of the 179 strains to ceftazidime, meropenem, amikacin, and colistin were 93.26%, 92.05%, 75.84%, and 14.12%, respectively. We also detected carbapenem-resistance genes in some KP strains. In 43 cases tested for blaKPC, the positivity rate was 65.12%; in 27 cases tested for blaOXA-48, 3.70% were positive; and in 26 cases tested for blaIMP, blaVIM, and blaNDM, the positive rates were 3.85%, 0.00%, and 15.38%, respectively.
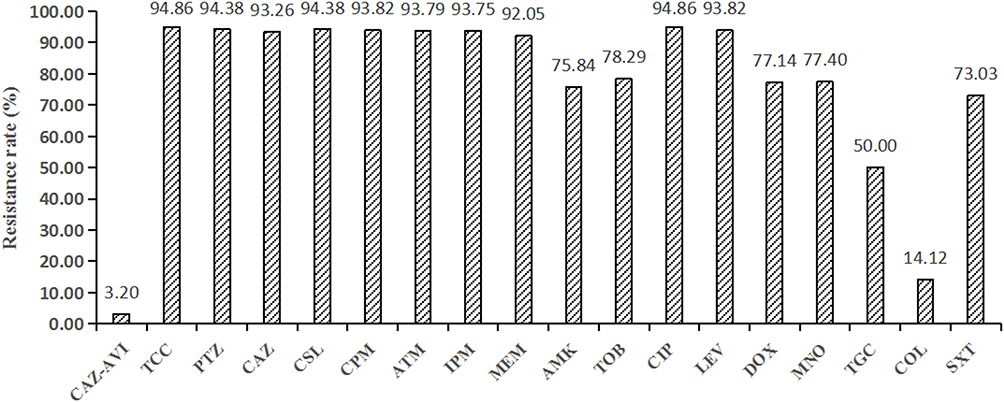 |
Figure 1 Drug resistance rates of KP (n = 179). Abbreviations: CAZ-AVI, ceftazidime-avibactam (n = 125); TCC, ticarcillin-clavulanic acid; PTZ, piperacillin-tazobactam; CAZ, ceftazidime; CSL, cefoperazone-sulbactam; CPM, cefepime; ATM, aztreonam; IPM, imipenem; MEM, meropenem; AMK, amikacin; TOB, tobramycin; CIP, ciprofloxacin; LEV, levofloxacin; DOX, doxycycline; MNO, minocycline; TGC, tigecycline (n = 164); COL, colistin; SXT, trimethoprim-sulfamethoxazole. |
Efficacy Evaluation
CR, MR, and 28-Day Survival
The CR, MR and 28-day survival data for 169 patients with KP infection given CAZ-AVI are presented in Table 2. The effective CR rate of CAZ-AVI for KP infection was 62.13%, and 65.68% of patients achieved a favorable MR. The 28-day survival rate was 63.91% (108 patients).
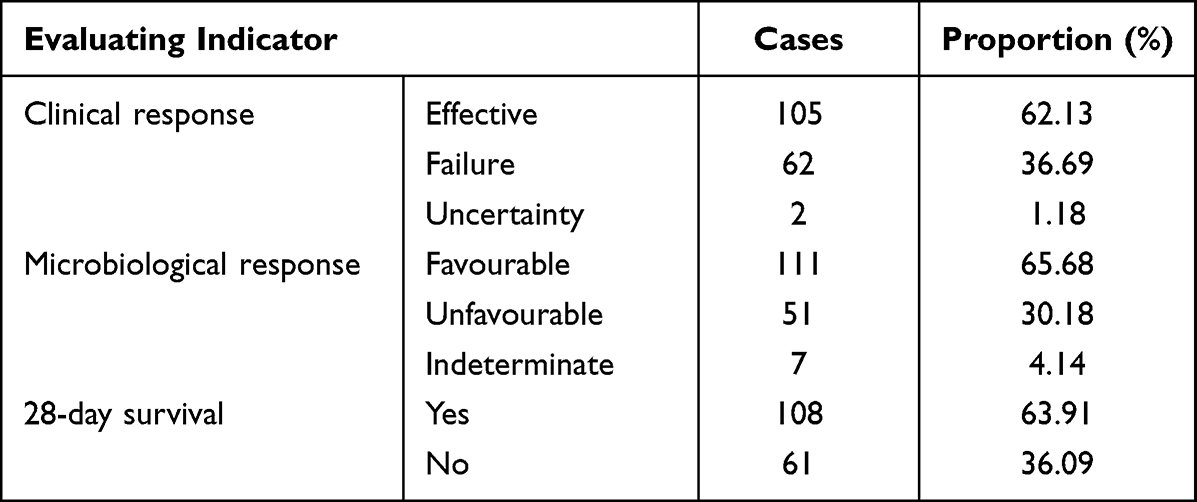 |
Table 2 CR, MR, and 28-Day Survival Data in the Study (n=169) |
Subgroup Analysis of the Therapeutic Effect of CAZ-AVI in Different Infection Sites
Of the 169 patients, 107 had a single-site infection, including lung (67), abdominal cavity (26), blood (10), and urinary tract (4). CAZ-AVI had the greatest effective CR rate for bloodstream infections, reaching 80% (Table 3). For MR, the favorable response rate for urinary tract infections reached 100%. The highest 28-day survival rate was for patients with bloodstream infections, at 80%. The Chi-square test was used to compare the differences among infection sites. No significant difference in CR or 28-day survival rate occurred. The favorable MR rate differed statistically among infection sites, with a low favorable MR rate of 46.15% in abdominal infections (P = 0.021).
 |
Table 3 The Difference in the Therapeutic Effect of CAZ-AVI on KP Infection in Different Sites (n=107) |
Subgroup Analysis of the Therapeutic Effect of Different Combined Treatment Regimens Based on CAZ-AVI
Of the 169 patients in this study, 136 patients were selected to analyze the efficacy of different combination subgroups based on CAZ-AVI. The details of each combination, the number of patients, and the therapeutic effect data are presented in Table 4. In terms of CR, the combination of CAZ-AVI with meropenem was the most effective, with a clinical effective rate of 80%, while CAZ-AVI combined with aztreonam was the least effective at 43.8%. In terms of MR, CAZ-AVI combined with fosfomycin or quinolones had highly favorable MR rates (100%), while CAZ-AVI combined with tigecycline or aztreonam had favorable MR rates of only 50%. In terms of the 28-day survival rate. The combination of CAZ-AVI with meropenem had the highest (80%) 28-day survival rate, while the combination of CAZ-AVI and tigecycline had the lowest survival rate at 40%. The chi-square test indicated no significant differences in CR, MR, and 28-day survival rate among the seven groups (P >0.05).
 |
Table 4 The Differences in the Efficacy of Different Combinations of CAZ-AVI in the Treatment of KP Infection (n=136) |
Safety Evaluation
In 169 patients, three cases of drug-related adverse events occurred during the use of CAZ-AVI, for an incidence rate of 1.78%. One case showed moderately elevated creatinine levels (three times the basic value and two times the normal upper limit); one case showed mild diarrhea and elevated transaminase (alanine transaminase and glutamic oxalic transaminase were four times and three times the normal upper limit, respectively); and one case showed moderate urethral hemorrhage with thrombocytopenia (half the basic level and below the normal lower limit). According to Naranjo’s ADRs probability scale, these events had scores of 3, 3, and 5, respectively. The correlation evaluation of ADRs was thus possible, possible, and probable, respectively.
Discussion
This is a retrospective study of CAZ-AVI in the treatment of KP infection. The efficacy and safety of CAZ-AVI in the treatment of KP infection in a clinical setting were retrospectively analyzed for the first time in a Chinese hospital. The therapeutic effects of CAZ-AVI at different infection sites were compared, and the therapeutic effects of different combinations of antibiotics were compared. In the past, some scholars have made retrospective studies on the efficacy of CAZ-AVI in the treatment of KP, but previous research focused mostly on bloodstream infections.24–27 Cases included in this study covered pulmonary, abdominal, blood, and urinary tract infections, and the majority were pulmonary infections. In this study, the vast majority of KP strains were not screened for drug-resistance genes, and clinicians do not screen for drug-resistance genes in most clinical settings in China. Clinician choice to use CAZ-AVI is mostly based on experience or drug sensitivity reports, so the efficacy evaluation results of this study are closer to “real-world values” than previous studies.
CAZ-AVI was mainly used in patients with carbapenem-resistant KP infection in this hospital. According to the statistical data on drug resistance, the proportion of strains resistant to meropenem was 92.05%. However, even when the resistance rate of the studied strain to colistin reached 14.12%, the sensitivity of CAZ-AVI was still good, with a resistance rate of 3.2%. This is consistent with other published studies from China (3.7%).28 In this study, a small number of KP drug-resistance genes were detected; the positive expression rate of blaNDM was 15.38%, and of blaIMP was 3.7%. The lack of inhibition of metallo-beta-lactamases by AVI may be one reason for the resistance of KP to CAZ-AVI in this study. In addition, other studies have shown that the mechanism of drug resistance of KP to CAZ-AVI may be related to a mutation of the KPC enzyme,17,29 the high expression of wild-type KPC enzyme, and the deletion of membrane porin.30,31
The effective CR rate of CAZ-AVI against KP in the current study was 62.13%, the favorable MR rate was 65.8%, and the 28-day survival rate was 63.91%. Several clinical studies of CAZ-AVI have previously been reported. In a summary and analysis of five clinical studies of CAZ-AVI for infection sites including abdominal, urinary tract, and pulmonary, an overall effective CR rate of 92.2%, and a favorable MR rate of 84.9% were observed.32 A similar curative effect was found for CRKP infection, despite differences in patient structure and infection sites compared to previous retrospective studies.24,25 The efficacy of CAZ-AVI in clinical studies appears to be superior to that of real-world retrospective studies. We suggest the following possible reasons. 1) In clinical studies, the recruitment of subjects is typically directed to a particular site of infection, without considering specific pathogen infection. Escherichia coli is the most common pathogen, followed by PA, with KP accounting for only a small proportion. 2) In clinical studies, most infectious pathogens are sensitive bacteria, with carbapenem-resistant bacteria accounting for only a small proportion. 3) In the real-world retrospective study, most patients have multiple underlying diseases, making cases more severe and complex than those in Phase III clinical studies. In the current study, a small number of patients had severe COVID-19 infection, and the taxed immune system of these patients may have led to a poorer prognosis.33 4) In this real-world study, patients are sometimes co-infected with other pathogens such as AB, in addition to KP. From the antibacterial spectrum, although CAZ-AVI maintains good activity against KP, Escherichia coli, and PA, its activity against AB is weak. In the case of combined infection with AB, even if the sensitive KP is eliminated by CAZ-AVI, the presence of AB still affects the therapeutic effect. Some studies have shown that the detection of drug-resistance genes before testing the drug sensitivity of KP can help to improve the effective CR rate.34 This is because the identification of drug-resistance genes can predict the sensitivity of CAZ-AVI, allowing for more rapid control of the disease. Other studies have shown that prolonging the infusion time based on the pharmacokinetic/pharmacodynamic (PK/PD) characteristics of CAZ-AVI also helps to improve clinical efficacy.35,36
We found no significant difference in CR and 28-day survival rates for lung, abdominal cavity, blood, and urinary tract infections. MR, however, did differ for infections at different sites, with a lower favorable rate for abdominal infections and a higher favorable rate for urinary tract infections. The efficacy of antibiotics in the body typically depends on whether the drug can reach an effective therapeutic concentration at the site of infection, which is related to the tissue distribution of the drug in the body. In mice pneumonia models, the concentration of AVI in alveolar epithelial lining fluid is about 24% that of plasma concentration.37 In human studies, the protein binding rate of AVI is low (8%), leaving more than 90% of drug free to act quickly.38 In various single intravenous injection doses, the steady-state distribution volume of AVI was 15–25 L, which slightly exceeds the circulating blood volume, indicating mild to moderate tissue distribution of AVI is likely.39 In terms of metabolism and excretion, AVI is metabolized very little by the liver, and more than 85% of it is excreted in urine.40 Pharmacokinetic characteristics of AVI suggest that because it has good distribution in the blood, it is well-distributed in the lungs and abdominal cavity, which have an abundant blood supply and is mainly excreted from the urinary tract. Thus, CAZ-AVI can help CAZ have a good antibacterial effect in the blood, lung, abdominal cavity and urinary tract, which may explain why no significant difference in clinical efficacy among different infection sites occurred in this study. In terms of microbiological efficacy in abdominal infections, studies have shown that the efficacy of CAZ-AVI combined with metronidazole in abdominal infection is similar to meropenem.41–43 In the current study, when CAZ-AVI was used in the treatment of abdominal infection, most times metronidazole was not used, which may be a factor leading to the low favorable MR rate for abdominal infections, but this remains to be further studied.
Subgroup analysis of CAZ-AVI in monotherapy versus in combination therapy with other antibiotics indicated that CAZ-AVI combined with colistin, meropenem, tigecycline, fosfomycin, quinolones or aztreonam did not show better clinical or microbiological efficacy than CAZ-AVI alone and did not significantly increase survival rate. This finding is consistent with the results of a previous meta-analysis and a clinical study.24,51 However, in vitro studies have shown that CAZ-AVI combined with meropenem has a synergistic effect on carbapenem-resistant Pseudomonas aeruginosa (CRPA) and CAZ-AVI combined with fosfomycin has a synergistic effect on CRKP.44–46 Besides, in vitro, studies have demonstrated significant synergy between CAZ-AVI and aztreonam in most Metallo-β-Lactamase-producing Enterobacterales.47,48 Clinical studies have also shown that CAZ-AVI combined with aztreonam can reduce the mortality of patients with metallo-β-lactamase-producing KP infection.49 However, this study did not find a significant advantage in using the combination of CAZ-AVI and aztreonam to combat KP infection, which may be attributed to previous studies mainly targeting strains producing metalloenzymes, while the proportion of metalloenzyme-producing strains in this study was small. The difference in results among combination CAZ-AVI treatments in different studies in vivo seems likely to reflect the fact that the body environment is more complex than the laboratory environment used in clinical studies. Whether combination therapy is of benefit in the real world still needs further investigation.
CAZ-AVI demonstrates good clinical safety in the treatment of KP infections. The increase of creatinine and transaminase observed in some patients in our study has also been reported in previous studies.50 However, a patient with urethral hemorrhage and thrombocytopenia occurred in this study, which has not been previously reported. Whether this was related to CAZ-induced thrombocytopenia is unclear;52 the mechanism of this adverse event is not clear and needs more attention.
This study has some limitations. It is only a single-center retrospective study because drug-resistant KP distribution varies greatly among different regions and even between different hospitals. This may lead to regional differences in clinical effectiveness. Therefore, further multicenter studies are urgently needed to evaluate the clinical effectiveness and safety of CAZ-AVI.
Conclusions
Overall, CAZ-AVI demonstrates promising clinical and microbiological efficacy and safety in the treatment of KP infections at this hospital. We found that CAZ-AVI provides comparable clinical benefits for KP-induced pulmonary, bloodstream, abdominal, and urinary tract infections. It is worth noting that CAZ-AVI exhibits a higher rate of urinary excretion compared to tigecycline and lower nephrotoxicity than colistin, potentially leading to improved effectiveness and safety in treating extensively drug-resistant KP urinary tract infections. However, for abdominal infections, concurrent anaerobic bacterial infections may be present, and combination therapy with metronidazole may be necessary to enhance microbiological efficacy. Furthermore, although we did not observe statistically significant differences between monotherapy and combination therapy in the treatment of KP infections, further research is needed. Specifically, for KP strains producing metallo-beta-lactamases, the addition of aztreonam may be required in clinical practice. Additionally, it is important to note that CAZ-AVI may pose a risk of thrombocytopenia and hematuria, necessitating close monitoring of platelet count and urinalysis during clinical administration.
Ethics and Consent Statements
This study was approved by the Ethics Committee of Hunan Provincial People’s Hospital (The first-affiliated hospital of Hunan Normal University) (NO: LY-2023-19). We certify that the study was conducted following the Declaration of Helsinki and appropriate informed consent was obtained from all individuals included in the study. Data anonymization processing was carried out when collecting patients’ information.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Jia Xu and Chengjia Luo are co-first authors for this study. All authors declared no conflicts of interest in this work.
References
1. Niemi MEK, Daly MJ, Ganna A. The human genetic epidemiology of COVID-19. Nat Rev Genet. 2022;23(9):533–546. doi:10.1038/s41576-022-00478-5
2. De Oliveira DMP, Forde BM, Kidd TJ, et al. Antimicrobial resistance in ESKAPE pathogens. Clin Microbiol Rev. 2020;33(3). doi:10.1128/CMR.00181-19
3. Chukamnerd A, Pomwised R, Jeenkeawpiam K, Sakunrang C, Chusri S, Surachat K. Genomic insights into blaNDM-carrying carbapenem-resistant Klebsiella pneumoniae clinical isolates from a university hospital in Thailand. Microbiol Res. 2022;263:127136. doi:10.1016/j.micres.2022.127136
4. Qin X, Wu S, Hao M, et al. The colonization of carbapenem-resistant Klebsiella pneumoniae: epidemiology, resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. 2020;221(Supplement_2):S206–S214. doi:10.1093/INFDIS/JIZ622
5. Hu Y, Liu C, Shen Z, et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in patients from Zhejiang, China, 2008–2018. Emerg Microbes Infect. 2020;9(1):1771–1779. doi:10.1080/22221751.2020.1799721
6. Guerra MES, Destro G, Vieira B, et al. Klebsiella pneumoniae Biofilms and Their Role in Disease Pathogenesis. Front Cell Infect Microbiol. 2022;12. doi:10.3389/fcimb.2022.877995
7. Shein AMS, Hongsing P, Abe S, et al. Will There Ever Be Cure for Chronic, Life-Changing Colistin-Resistant Klebsiella pneumoniae in Urinary Tract Infection? Front Med. 2021;8. doi:10.3389/fmed.2021.806849
8. Shein AMS, Wannigama DL, Higgins PG, et al. Novel colistin-EDTA combination for successful eradication of colistin-resistant Klebsiella pneumoniae catheter-related biofilm infections. Sci Rep. 2021;11(1). doi:10.1038/s41598-021-01052-5
9. Shein AMS, Wannigama DL, Higgins PG, et al. High prevalence of mgrB-mediated colistin resistance among carbapenem-resistant Klebsiella pneumoniae is associated with biofilm formation, and can be overcome by colistin-EDTA combination therapy. Sci Rep. 2022. doi:10.1038/s41598-022-17083-5
10. Wannigama DL, Sithu Shein AM, Hurst C, et al. Ca-EDTA restores the activity of ceftazidime-avibactam or aztreonam against carbapenemase-producing Klebsiella pneumoniae infections. iScience. 2023;26(7):107215. doi:10.1016/j.isci.2023.107215
11. Richards DM, Brogden RN. Ceftazidime: a Review of its Antibacterial Activity, Pharmacokinetic Properties and Therapeutic Use. Drugs. 1985. doi:10.2165/00003495-198529020-00002
12. Yahav D, Giske CG, Gramatniece A, Abodakpi H, Tam VH, Leibovici L. New β-lactam–β-lactamase inhibitor combinations. Clin Microbiol Rev. 2021;34(2). doi:10.1128/CMR.00115-20
13. Zhanel GG, Lawson CD, Adam H, et al. Ceftazidime-avibactam: a novel cephalosporin/β-lactamase inhibitor combination. Drugs. 2013;73(2):159–177. doi:10.1007/s40265-013-0013-7
14. Krapp F, Grant JL, Sutton SH, Ozer EA, Barr VO. Treating complicated carbapenem-resistant Enterobacteriaceae infections with ceftazidime/avibactam: a retrospective study with molecular strain characterisation. Int J Antimicrob Agents. 2017;49(6):770–773. doi:10.1016/j.ijantimicag.2017.01.018
15. Carmeli Y, Armstrong J, Laud PJ, et al. Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): a randomised, pathogen-directed. Lancet Infect Dis. 2016;16(6):661–673. doi:10.1016/S1473-3099(16)30004-4
16. Lucasti C, Popescu I, Ramesh MK, Lipka J, Sable C. Comparative study of the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infections in hospitalized adults: results of a randomized, double-blind, Phase II trial. J Antimicrob Chemother. 2013;68(5):1183–1192. doi:10.1093/jac/dks523
17. Shields RK, Chen L, Cheng S, et al. Emergence of ceftazidime-avibactam resistance due to plasmid-borne blaKPC-3 mutations during treatment of carbapenem-resistant Klebsiella pneumoniae infections. Antimicrob Agents Chemother. 2017;61(3). doi:10.1128/AAC.02097-16
18. Di Bella S, Giacobbe DR, Maraolo AE, et al. Resistance to ceftazidime/avibactam in infections and colonisations by KPC-producing Enterobacterales: a systematic review of observational clinical studies. J Glob Antimicrob Resist. 2021;25:268–281. doi:10.1016/j.jgar.2021.04.001
19. Grief SN, Loza JK. Guidelines for the Evaluation and Treatment of Pneumonia. Prim Care - Clin off Pract. 2018;45(3):485–503. doi:10.1016/j.pop.2018.04.001
20. Sartelli M, Chichom-Mefire A, Labricciosa FM, et al. The management of intra-abdominal infections from a global perspective: 2017 WSES guidelines for management of intra-abdominal infections. World J Emerg Surg. 2017. doi:10.1186/s13017-017-0141-6
21. Choe HS, Lee SJ, Yang SS, et al. Summary of the UAA-AAUS guidelines for urinary tract infections. Int J Urol. 2018;25(3):175–185. doi:10.1111/iju.13493
22. Mendes RE, Castanheira M, Woosley LN, Stone GG, Bradford PA, Flamm RK. Characterization of -lactamase content of ceftazidime-resistant pathogens recovered during the pathogen-directed Phase 3 REPRISE trial for ceftazidime-avibactam: correlation of efficacy against -lactamase producers. Antimicrob Agents Chemother. 2019;63(6). doi:10.1128/AAC.02655-18
23. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
24. Tumbarello M, Raffaelli F, Giannella M, et al. Ceftazidime-Avibactam Use for Klebsiella pneumoniae Carbapenemase–Producing K. pneumoniae Infections: a Retrospective Observational Multicenter Study. Clin Infect Dis. 2021;73(9):1664–1676. doi:10.1093/cid/ciab176
25. Karaiskos I, Daikos GL, Gkoufa A, et al. Ceftazidime/avibactam in the era of carbapenemase-producing Klebsiella pneumoniae: experience from a national registry study. J Antimicrob Chemother. 2021;76(3):775–783. doi:10.1093/jac/dkaa503
26. Tumbarello M, Trecarichi EM, Corona A, et al. Efficacy of Ceftazidime-Avibactam Salvage Therapy in Patients With Infections Caused by Klebsiella pneumoniae Carbapenemase–producing K. pneumoniae. Clin Infect Dis. 2019;68(3):355–364. doi:10.1093/cid/ciy492
27. Lima O, Sousa A, Longueira-Suárez R, et al. Ceftazidime–avibactam treatment in bacteremia caused by OXA-48 carbapenemase-producing Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2022;41(9):1173–1182. doi:10.1007/s10096-022-04482-9
28. Zhang P, Shi Q, Hu H, et al. Emergence of ceftazidime/avibactam resistance in carbapenem-resistant Klebsiella pneumoniae in China. Clin Microbiol Infect. 2020;26(1):124.e1–124.e4. doi:10.1016/j.cmi.2019.08.020
29. Findlay J, Poirel L, Juhas M, Nordmann P. KPC-mediated resistance to ceftazidime-avibactam and collateral effects in Klebsiella pneumoniae. Antimicrob Agents Chemother. 2021;65(9). doi:10.1128/AAC.00890-21
30. Shields RK, Clancy CJ, Hao B, et al. Effects of Klebsiella pneumoniae Carbapenemase Subtypes, Extended-Spectrum β-Lactamases, and Porin Mutations on the In Vitro Activity of Ceftazidime-Avibactam against Carbapenem-Resistant K. pneumoniae. Antimicrob Agents Chemother. 2015;59(9):5793–5797. doi:10.1128/AAC.00548-15
31. Venditti C, Butera O, Meledandri M, et al. Molecular analysis of clinical isolates of ceftazidime-avibactam-resistant Klebsiella pneumoniae. Clin Microbiol Infect. 2021;27(7):1040.e1–1040.e6. doi:10.1016/j.cmi.2021.03.001
32. Mazuski JE, Wagenlehner F, Torres A, et al. Clinical and Microbiological Outcomes of Ceftazidime-Avibactam Treatment in Adults with Gram-Negative Bacteremia: a Subset Analysis from the Phase 3 Clinical Trial Program. Infect Dis Ther. 2021;10(4):2399–2414. doi:10.1007/s40121-021-00506-7
33. Napoli C, Benincasa G, Criscuolo C, Faenza M, Liberato C, Rusciano M. Immune reactivity during COVID-19: implications for treatment. Immunol Lett. 2021;231:28–34. doi:10.1016/j.imlet.2021.01.001
34. Satlin MJ, Chen L, Gomez-Simmonds A, et al. Impact of a Rapid Molecular Test for Klebsiella pneumoniae Carbapenemase and Ceftazidime-Avibactam Use on Outcomes after Bacteremia Caused by Carbapenem-Resistant Enterobacterales. Clin Infect Dis. 2022;75(12):2066–2075. doi:10.1093/cid/ciac354
35. Jacobs DM, DiTursi S, Ruh C, et al. Combination treatment with extended-infusion ceftazidime/avibactam for a KPC-3-producing Klebsiella pneumoniae bacteraemia in a kidney and pancreas transplant patient. Int J Antimicrob Agents. 2016;48(2):225–227. doi:10.1016/j.ijantimicag.2016.06.002
36. Gatti M, Pascale R, Cojutti PG, et al. A descriptive pharmacokinetic/pharmacodynamic analysis of continuous infusion ceftazidime-avibactam in a case series of critically ill renal patients treated for documented carbapenem-resistant Gram-negative bloodstream infections and/or ventilator-associ. Int J Antimicrob Agents. 2023. doi:10.1016/j.ijantimicag.2022.106699
37. Berkhout J, Melchers MJ, Van Mil AC, et al. Pharmacokinetics and penetration of ceftazidime and avibactam into epithelial lining fluid in thigh- and lung-infected mice. Antimicrob Agents Chemother. 2015;59(4):2299–2304. doi:10.1128/AAC.04627-14
38. Zasowski EJ, Rybak JM, Rybak MJ. The β-Lactams Strike Back: ceftazidime-Avibactam. Pharmacotherapy. 2015;35(8):755–770. doi:10.1002/phar.1622
39. Merdjan H, Rangaraju M, Tarral A. Safety and Pharmacokinetics of Single and Multiple Ascending Doses of Avibactam Alone and in Combination with Ceftazidime in Healthy Male Volunteers: results of Two Randomized, Placebo-Controlled Studies. Clin Drug Investig. 2015;35(5):307–317. doi:10.1007/s40261-015-0283-9
40. Vishwanathan K, Mair S, Gupta A, et al. Assessment of the mass balance recovery and metabolite profile of avibactam in humans and in vitro drug-drug interaction potentials. Drug Metab Dispos. 2014;42(5):932–942. doi:10.1124/dmd.113.055335
41. Qin X, Tran BG, Kim MJ, et al. A randomised, double-blind, phase 3 study comparing the efficacy and safety of ceftazidime/avibactam plus metronidazole versus meropenem for complicated intra-abdominal infections in hospitalised adults in Asia. Int J Antimicrob Agents. 2017;49(5):579–588. doi:10.1016/j.ijantimicag.2017.01.010
42. Rodgers P, Kamat S, Adhav C. Ceftazidime-avibactam plus metronidazole vs. meropenem in complicated intra-abdominal infections: Indian subset from RECLAIM. J Infect Dev Ctries. 2022;16(02):305–313. doi:10.3855/jidc.14912
43. Mazuski JE, Gasink LB, Armstrong J, et al. Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: results from a randomized, controlled, double-blind, phase 3 program. Clin Infect Dis. 2016;62(11):1380–1389. doi:10.1093/cid/ciw133
44. Maraki S, Mavromanolaki VE, Moraitis P, et al. Ceftazidime-avibactam, meropenen-vaborbactam, and imipenem-relebactam in combination with aztreonam against multidrug-resistant, metallo-β-lactamase-producing Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2021;40(8):1755–1759. doi:10.1007/s10096-021-04197-3
45. Khan A, Erickson SG, Pettaway C, Arias CA, Miller WR, Bhatti MM. Evaluation of susceptibility testing methods for aztreonam and ceftazidime-avibactam combination therapy on extensively drug-resistant gram-negative organisms. Antimicrob Agents Chemother. 2021;65(11):1–13. doi:10.1128/AAC.00846-21
46. Mikhail S, Singh NB, Kebriaei R, et al. Evaluation of the synergy of ceftazidime-avibactam in combination with meropenem, amikacin, aztreonam, colistin, or fosfomycin against well-characterized multidrug-resistant Klebsiella pneumoniae and pseudomonas aeruginosa. Antimicrob Agents Chemother. 2019;63(8):1–10. doi:10.1128/AAC.00779-19
47. Rawson TM, Brzeska-Trafny I, Maxfield R, et al. A practical laboratory method to determine ceftazidime-avibactam-aztreonam synergy in patients with New Delhi metallo-beta-lactamase (NDM)–producing Enterobacterales infection. J Glob Antimicrob Resist. 2022;29:558–562. doi:10.1016/j.jgar.2022.01.025
48. Marshall S, Hujer AM, Rojas LJ, et al. Can ceftazidime-avibactam and aztreonam overcome β-lactam resistance conferred by metallo-β-lactamases in Enterobacteriaceae? Antimicrob Agents Chemother. 2017;61(4). doi:10.1128/AAC.02243-16
49. Falcone M, Daikos GL, Tiseo G, et al. Efficacy of Ceftazidime-avibactam plus Aztreonam in Patients with Bloodstream Infections Caused by Metallo-β-lactamase-Producing Enterobacterales. Clin Infect Dis. 2021;72(11):1871–1878. doi:10.1093/cid/ciaa586
50. Cheng K, Newell P, Chow JW, et al. Safety Profile of Ceftazidime–Avibactam: pooled Data from the Adult Phase II and Phase III Clinical Trial Programme. Drug Saf. 2020;43(8):751–766. doi:10.1007/s40264-020-00934-3
51. Onorato L, Di Caprio G, Signoriello S, Coppola N. Efficacy of ceftazidime/avibactam in monotherapy or combination therapy against carbapenem-resistant Gram-negative bacteria: a meta-analysis. Int J Antimicrob Agents. 2019;54(6):735–740. doi:10.1016/j.ijantimicag.2019.08.025
52. Domingo-Chiva E, Díaz-Rangel M, Monsalve-Naharro JÁ, Cuesta-Montero P, Catalá-Ripoll JV, García-Martínez EM. Ceftazidime-induced thrombocytopenia. Rev Española Anestesiol y Reanim (English Ed. 2017;64(10):590–593. doi:10.1016/j.redare.2017.03.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.