Back to Journals » Journal of Pain Research » Volume 18
Clinical Efficacy and Plasma Metabolomics Analysis of Acupuncture for Migraine Treatment
Authors Gao L ![]() , Chen Y, Xie C, Zhang Z
, Chen Y, Xie C, Zhang Z ![]() , Yan Q, Fu QX
, Yan Q, Fu QX ![]() , Sun M, Zhao L
, Sun M, Zhao L
Received 13 June 2025
Accepted for publication 18 September 2025
Published 9 October 2025 Volume 2025:18 Pages 5283—5301
DOI https://doi.org/10.2147/JPR.S546838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Lei Gao,1,* Ying Chen,1,* Chaorong Xie,1 ZhiYang Zhang,1 Qinyi Yan,1 Qi Xuan Fu,1 Mingsheng Sun,1 Ling Zhao1– 3
1Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Key Laboratory of Acupuncture for Senile Disease (Chengdu University of TCM), Ministry of Education, Chengdu, Sichuan, People’s Republic of China; 3Acupuncture & Chronobiology Key Laboratory of Sichuan Province, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Zhao, Email [email protected]
Purpose: Migraine, a prevalent neurological disorder characterized by recurrent, debilitating headaches, poses significant challenges due to limited understanding of its pathophysiology and variable treatment outcomes. Acupuncture has emerged as a promising intervention, yet its clinical efficacy and underlying metabolic mechanisms remain underexplored. This study aimed to evaluate the therapeutic effects of true acupuncture (TA) compared to sham acupuncture (SA) in migraine patients and to elucidate associated metabolic changes using non-targeted plasma metabolomics.
Patients and Methods: Fifty-two migraine patients were randomized into TA and SA groups, receiving 12 sessions of acupuncture over four weeks, with clinical assessments and plasma sample collection at baseline and week 4.
Results: The TA group exhibited a significant reduction in migraine attack frequency (p< 0.05) compared to baseline, while the SA group showed no significant change (p> 0.05). Additionally, the TA group demonstrated greater improvements in attack frequency, duration, visual analog scale (VAS) scores, and migraine-specific quality of life (MSQ) emotional and dysfunction subscales compared to the SA group (p< 0.05). Metabolomic analysis identified distinct metabolic profiles. TA was associated with five key metabolites, including the lipid regulators 1-oleoyl-sn-glycero-3-phosphoethanolamine (LysoPE) and Pe (16:0/19,20-epdpe), which correlated with reduced attack duration and improved quality of life scores. In contrast, metabolic changes in the SA group were less pronounced. Pathway analysis revealed that TA predominantly modulated amino acid and pyrimidine metabolism.
Conclusion: These findings indicate that TA is more effective than SA in alleviating migraine symptoms, likely through specific regulation of metabolic pathways. The identified metabolites offer potential biomarkers for evaluating treatment response, though further validation is required.
Keywords: migraine, acupuncture, metabolomics, lipid metabolism, amino acid metabolism
Introduction
Migraine, a debilitating neurological disorder, affects approximately one billion individuals globally and ranks as the second leading cause of disability.1,2 Its hallmark features, recurrent unilateral headaches, nausea, vomiting, and sensory hypersensitivity, stem from intricate neurovascular mechanisms, including cortical spreading depression and trigeminovascular system activation.3,4 While pharmacological interventions such as triptans offer relief for some, their limitations, adverse effects, variable efficacy, and cost, have fueled exploration of acupuncture, a traditional Chinese medicine (TCM) modality designed to restore Qi balance and mitigate migraine symptoms.5 Preliminary evidence from randomized controlled trials (RCTs) suggests acupuncture’s potential in migraine prophylaxis, particularly through the stimulation of specific acupoints like Fengchi (GB20) and Taichong (LR3) along the Gallbladder and Liver meridians; however, the underlying metabolic mechanisms remain underexplored, necessitating novel investigations into its therapeutic specificity.6–8
Emerging evidence highlights metabolic dysregulation as a key factor associated with migraine pathogenesis, with studies demonstrating altered profiles of amino acids (eg, arginine) and lipids (eg, lysophosphatidylethanolamine, LysoPE) linked to nitric oxide (NO) imbalance, neuroinflammation, and vascular dysfunction.9,10 These biochemical changes closely mirror TCM paradigms, wherein migraines stem from liver Yang hyperactivity or blood stasis, disrupting Qi flow and blood circulation, which precipitate neuroinflammatory and vascular imbalances that sustain headache pathology.11–13 Metabolomics, a powerful tool for profiling small-molecule metabolites, provides a bridge between TCM’s holistic framework and biomedical science by elucidating how acupuncture may modulate metabolic pathways linked to TCM syndromes. Previous research has identified metabolic signatures in migraine patients, such as decreased arginine and elevated LysoPE levels, implicating NO dysregulation and inflammatory processes.9,14 Parallel studies in chronic pain and depression suggest that acupuncture influences lipid and amino acid metabolism, hinting at broader systemic effects.12,15 However, metabolomic analyses of acupuncture in migraine, particularly comparing true acupuncture (TA) to sham acupuncture (SA), remain underexplored, leaving critical gaps in understanding its specific therapeutic contributions.
This study addresses these deficiencies through an RCT evaluating TA versus SA in migraine patients, utilizing untargeted metabolomics via ultra-high-performance liquid chromatography coupled with Quadrupole Exactive-Orbitrap MS (UHPLC-Q Exactive-Orbitrap MS). We hypothesize that TA will be more effective than SA in reducing the frequency and severity of migraines, accompanied by distinct metabolic alterations, particularly in amino acid and lipid pathways. Secondary outcomes include emotional well-being, a critical dimension given the high comorbidity of anxiety and depression in migraineurs and acupuncture’s purported ability to harmonize the Shen (mind-spirit). The Vanquish LC UHPLC system, paired with a Q Exactive series mass spectrometer (Thermo) utilizing electrospray ionization in positive and negative ion modes, was employed for its high resolution and sensitivity, facilitating comprehensive detection of plasma metabolites. By synthesizing clinical outcomes with metabolomic profiles, this study seeks to clarify acupuncture’s mechanistic underpinnings, advancing its integration into evidence-based migraine care and enriching the scientific foundation of TCM.
Materials and Methods
Study Design and Participants
This study was a randomized, single-blind, sham-controlled trial conducted at the Acupuncture and Neurology Departments of the Affiliated Hospital of Chengdu University of Traditional Chinese Medicine from June 2020 to August 2021, recruiting 52 patients with episodic migraine without aura diagnosed per the International Headache Society’s classification standard (Figure 1). The trial adhered to the Declaration of Helsinki, was approved by the Chengdu University of Traditional Chinese Medicine Ethics Committee (Approval 2020KL-003), and was registered at Chinese Clinical Trial Registry (ChiCTR2000032308).
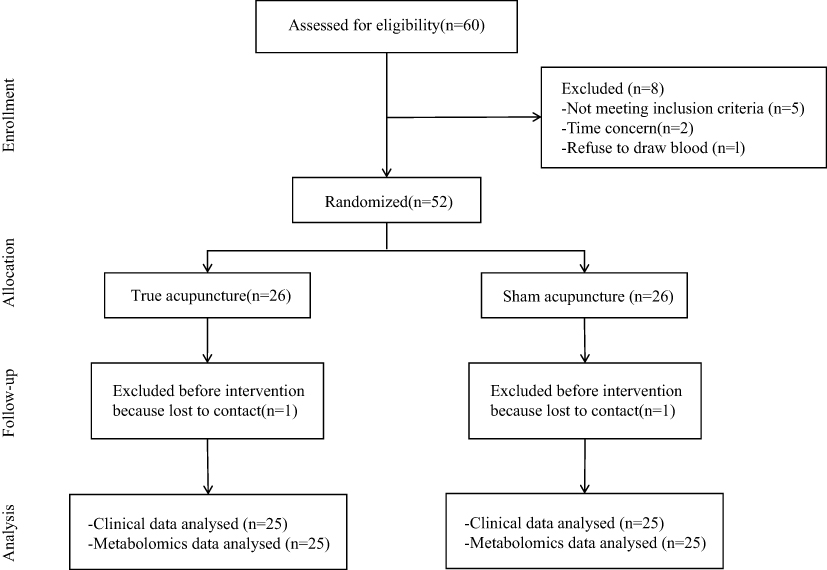 |
Figure 1 Study Design and Participant Flow. This flowchart illustrates the study design and participant progression. A total of 50 eligible patients, aged 18–55 years and diagnosed with migraine according to the International Classification of Headache Disorders, 3rd edition (ICHD-3), were enrolled. Participants were randomized on a 1:1 basis to receive either true acupuncture (TA) or sham acupuncture (SA) for a 4-week treatment period. The diagram also outlines the schedule for clinical and metabolomic assessments. |
Written informed consent was obtained from all participants prior to enrollment. The study included adults aged 18–55 years, male or female, with a confirmed diagnosis of episodic migraine without aura per the International Classification of Headache Disorders, 3rd edition (ICHD-3),16 and migraine onset before age 50. Eligibility required a documented migraine history of at least one year, with more than or equal to 2 attacks per month and fewer than 15 headache days per month over a three-month baseline period, moderate headache severity at baseline (Visual Analog Scale score 3–7), completion of a baseline headache diary, and willingness to adhere to the study protocol.
The study excluded individuals with other primary or unexplained headaches, serious systemic diseases, head trauma, mental or intellectual disorders hindering questionnaire completion, bleeding tendencies, allergies, skin diseases, pregnancy or lactation, inability to record a headache diary, long-term analgesic or alcohol use, recent acupuncture or preventive treatments within 4 weeks, or participation in similar studies within 3 months, ensuring a homogeneous cohort free from confounders.
Randomization and Blinding
Participants were randomly assigned to either the true acupuncture (TA) group or the sham acupuncture (SA) group in a 1:1 ratio using a computer-generated random sequence. Participants were blinded to their group assignment, while acupuncturists were not blinded due to the nature of the intervention. Outcome assessors and statisticians remained blinded to group allocation throughout the study.
Acupuncture Interventions and Co-Interventions
The TA group received acupuncture at five standardized acupoints based on TCM theory targeting the Shaoyang and Du meridians, including mandatory acupoints Fengchi (GB20), Shuaigu (GB8), and Baihui (GV20), with two additional acupoints selected according to headache location and TCM syndrome differentiation, as informed by a validated clinical acupoint protocol for migraine treatment.17 Additional acupoints were individualized based on TCM syndrome differentiation and headache location, using the Four Diagnostic Methods (inspection, auscultation, inquiry, palpation) and a validated TCM syndrome questionnaire: Waiguan (TE5) and Yanglingquan (GB34) for Shaoyang headache, Kunlun (BL60) and Houxi (SI3) for Taiyang headache, Hegu (LI4) and Neiting (ST44) for Yangming headache, and Taichong (LR3) and Neiguan (PC6) for Jueyin headache. For the TA group, disposable sterile stainless steel needles (0.25 mm diameter, 25–40 mm length; Hwato, Suzhou, China) were inserted into five acupoints using the Park Sham Device (PSD, Dong-bang Acupuncture Inc., Seoul, Korea) to ensure precise needle placement, with depths of 0.3–1 cm to elicit Deqi sensation (soreness, numbness, or distension) through lifting-thrusting, twirling, or scraping techniques. Needles were retained for 30 minutes per session, with manual stimulation every 15 minutes, over 12 sessions (3 per week) for 4 weeks, following a standardized protocol to minimize acupuncturist bias.
The SA group underwent sham acupuncture using the Park Sham Device (PSD) kit (Dong-bang Acupuncture Inc., Seoul, Korea), involving removal of the adhesive ring from the PSD base and insertion of recyclable blunt needles at the same five acupoints as the TA group [eg, Fengchi (GB20), Shuaigu (GB8), Baihui (GV20)]. Blunt needles were applied superficially without manipulation to avoid Deqi sensation, mimicking the TA group’s procedure while minimizing physiological effects, though non-specific responses may occur, as noted in prior acupuncture trials.7 The Park Sham Device is a validated tool designed to blind participants effectively, as the blunt needle retracts into the handle, providing a pricking sensation without skin penetration, making the intervention indistinguishable from true acupuncture for the patient. The number, frequency, and duration of sessions were identical to the TA group (12 sessions over 4 weeks). Participants were permitted to use acute migraine medications (eg, ibuprofen, triptans) as needed, with usage recorded in a headache diary detailing drug type, dose, and frequency.
Clinical Outcomes
The primary outcome was the change in monthly migraine attack frequency from baseline to the end of the 4-week treatment period, assessed using a standardized headache diary. Participants recorded migraine occurrences, including date and duration, as they happened, using a validated headache diary template based on International Headache Society guidelines. Diaries were collected weekly to ensure compliance.
To comprehensively evaluate the impact of acupuncture on migraine and patient well-being, secondary outcomes were assessed at baseline and week 4, focusing on multiple dimensions of disease severity and quality of life. Migraine attack duration, measured in hours per attack, was documented in the headache diary to gauge changes in episode length. The duration during which individuals were unable to work, study, or perform household duties due to headaches was also recorded to assess the impact on functional status. Pain intensity was quantified using the Visual Analog Scale (VAS, 0–10), administered by blinded assessors during clinic visits to ensure objectivity. To further capture functional impairment, headache-related disability was evaluated with the Headache Impact Test-6 (HIT-6), completed by participants during clinic visits. Quality of life, particularly emotional functioning, was assessed using the Migraine-Specific Quality of Life Questionnaire (MSQ), with a focus on its emotional functional subscale, also completed during clinic visits. In addition, acute medication use was tracked as days per month, with dose and frequency recorded in the headache diary to monitor treatment reliance. At the end of the study, we determined the maintenance of blinding of patients by asking them whether they believed they had received genuine real acupuncture treatment. Safety was monitored through adverse event reports collected via participant feedback and clinic assessments throughout the study.
Metabolomic Profiling
Fasting venous blood samples (3–5 mL) were collected from participants at baseline and within one week post-treatment (week 4) between 08:00 and 09:00 after overnight fasting and water abstinence, using heparin-anticoagulated tubes, placed in an ice bath, and centrifuged at 1000 × g for 15 minutes at 4°C within 30 minutes to obtain plasma, which was stored at −70°C with proper labeling and documentation. Plasma samples were thawed slowly at 4°C, mixed with a pre-chilled methanol/acetonitrile/water solution (2:2:1, v/v), vortexed, sonicated at low temperature for 30 minutes, incubated at −20°C for 10 minutes, and centrifuged at 14,000 × g for 20 minutes at 4°C. The supernatant was vacuum-dried, reconstituted in 100 µL of acetonitrile/water (1:1, v/v), vortexed, centrifuged at 14,000 × g for 15 minutes at 4°C, and the supernatant was used for analysis.
Untargeted metabolomics was performed using a Vanquish LC ultra-high-performance liquid chromatography (UHPLC) system coupled with a Q Exactive series mass spectrometer (Thermo, USA) employing electrospray ionization (ESI) in positive and negative ion modes. Chromatographic separation was achieved on a HILIC column (2.1 mm × 100 mm, 1.8 µm) at 25°C, with a flow rate of 0.3 mL/min and an injection volume of 2 µL. The mobile phase consisted of water with 25 mM ammonium acetate and 25 mM ammonia (A) and acetonitrile (B), using the following gradient elution: 0–1.5 min, 98% B; 1.5–12 min, 98–2% B; 12–14 min, 2% B; 14–14.1 min, 2–98% B; 14.1–17 min, 98% B. Samples were maintained at 4°C in the autosampler, analyzed in random order, with QC samples inserted to monitor system stability and data reliability. Mass spectrometry was conducted with a primary scan range of m/z 80–1200 (resolution 60,000, accumulation time 100 ms) and secondary segmented acquisition from m/z 70–1200 (resolution 30,000, accumulation time 50 ms, dynamic exclusion 4 s). ESI source parameters included: auxiliary gas 1 (60), auxiliary gas 2 (60), curtain gas (30 psi), source temperature 600°C, spray voltage ±5500 V.
Raw mass spectrometry files were first converted to the.mzXML format using ProteoWizard; subsequently, XCMS was employed for chromatographic peak alignment, retention-time correction, and extraction of peak areas. The resulting dataset then underwent metabolite structure elucidation, systematic data preprocessing, and rigorous quality assessment of experimental measurements before downstream statistical analysis. Metabolite annotation was achieved by querying a locally curated standards library (Shanghai Applied Protein Technology) [Luo et al, 2017; Zhaobing et al, 2018], matching retention times, accurate masses (mass error < 10 ppm), MS/MS fragmentation spectra, and collision energies. All putative identifications were subjected to meticulous manual review, securing confidence at Level 2 or higher. Multivariate statistical analyses, including principal component analysis (PCA) and orthogonal partial least squares-discriminant analysis (OPLS-DA), were performed using SIMCA 14.1 (Umetrics, Sweden). Significantly differential metabolites were identified solely by an OPLS-DA variable importance in projection (VIP) score exceeding 1 combined with a t-test P value below 0.05. Pathway analysis was conducted using MetaboAnalyst 5.0, integrating the Kyoto Encyclopedia of Genes and Genomes (KEGG) database.
Treatment and Analytical Assurance
Acupuncturists were licensed practitioners with at least five years of training and three years of experience, trained to follow standardized protocols to ensure treatment fidelity. Regular monitoring included video audits of 10% of sessions. Quality control (QC) samples, prepared by pooling equal aliquots of all plasma samples, were injected every 10 samples during UHPLC-Q Exactive-Orbitrap MS analysis to assess system stability. In our study, QC samples revealed that over 80% of detected peaks exhibited relative standard deviations (RSDs) of ≤30%, confirming analytical reliability.
Statistical Analysis
Based on a previous acupuncture trial reporting a 35% reduction in migraine frequency with TA versus 12% with SA (effect size = 0.8), a sample size of 50 participants (25 per group) was calculated to detect a 30% reduction in the TA group and 10% in the SA group, with 80% power, 5% significance level, and 15% dropout rate. This sample size may be underpowered for metabolomic analyses due to high variability. Clinical outcomes were analyzed using an intention-to-treat approach, with continuous variables (eg, migraine frequency, VAS scores) compared via t-tests or Mann–Whitney U-tests based on normality, and changes over time assessed by repeated-measures ANOVA. Categorical variables (eg, adverse events) were analyzed using chi-square tests. Metabolomic data were evaluated with t-tests for differential metabolites and Pearson’s correlation for associations with clinical outcomes and TCM syndromes. All analyses were conducted using SPSS 25.0 (IBM, USA), with p < 0.05 considered significant.
Results
Baseline Demographics and Clinical Characteristics
A total of 52 migraine patients were initially enrolled in this study. However, two participants, one from the true acupuncture (TA) group and one from the sham acupuncture (SA) group, withdrew due to dissatisfaction with the treatment, leaving 50 subjects for the final analysis. Baseline demographic and clinical characteristics, as summarized in Table 1, showed no significant differences between the TA and SA groups. These characteristics included age, sex, marital status, height, weight, education level, duration of illness, use of acute pain medication, and baseline migraine severity metrics such as the number of migraine attacks, attack duration, inability to work or perform daily activities, visual analog scale (VAS) scores, Headache Impact Test-6 (HIT-6) scores, and Migraine-Specific Quality of Life (MSQ) scores.
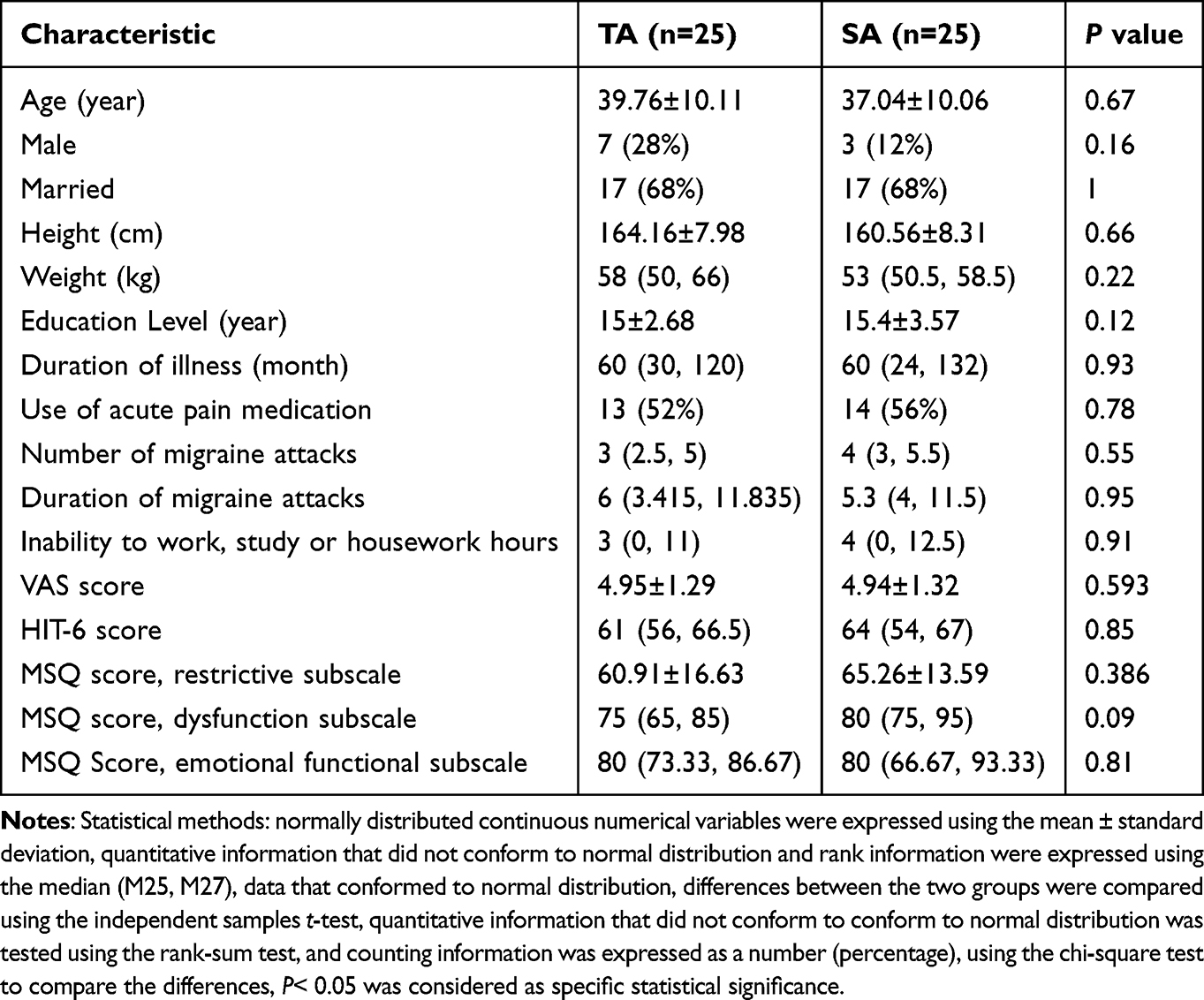 |
Table 1 Baseline Characteristics of 50 Patients Included in the Intention-to-Treat Analysis |
True Acupuncture Alleviates Migraine Frequency and Severity
The primary outcome, evaluated as the number of migraine attacks in the past four weeks at the end of the treatment course (four weeks post-enrollment), revealed notable differences between the groups. The TA group exhibited a significant reduction in migraine attacks compared to baseline (P < 0.05), while the SA group showed no significant change (P > 0.05). Moreover, the TA group reported significantly fewer migraine attacks than the SA group at the end of treatment (P < 0.05), as detailed in Table 2.
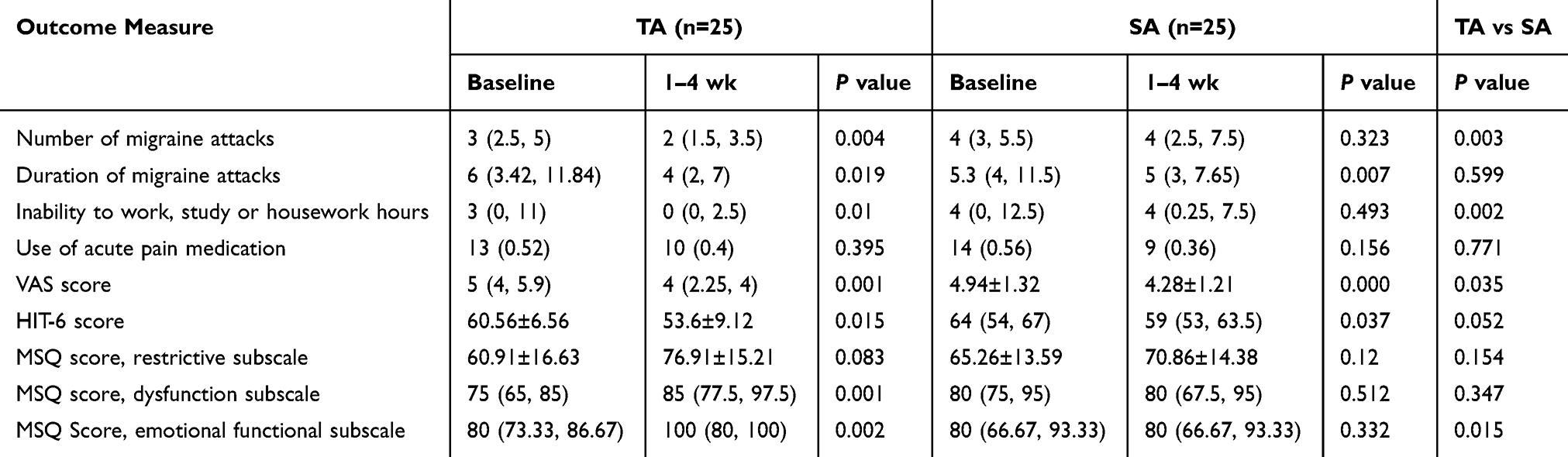 |
Table 2 Analysis of Clinical Outcomes |
Regarding secondary outcomes, both groups demonstrated improvements across multiple measures by the end of the treatment period. The TA group experienced significant reductions in the duration of migraine attacks, inability to work or perform daily activities, VAS scores, and HIT-6 scores, alongside improvements in the MSQ dysfunction and emotional functional subscales. The SA group also showed decreases in attack duration, VAS scores, and HIT-6 scores. However, between-group comparisons indicated significantly greater improvements in the TA group for inability to work or perform daily activities, VAS scores, and the MSQ emotional functional subscale (P < 0.05). Neither group exhibited significant changes in the use of acute pain medication or the MSQ restrictive subscale, as presented in Table 2.
Evaluation of Credibility for Patient Blinding
At the end of the study, we assessed the credibility of blinding of treatment. We found no significant difference in the proportion of participants in the SA group who believed they were receiving real acupuncture treatment compared to the TA group (P=0.235) (Table 3).
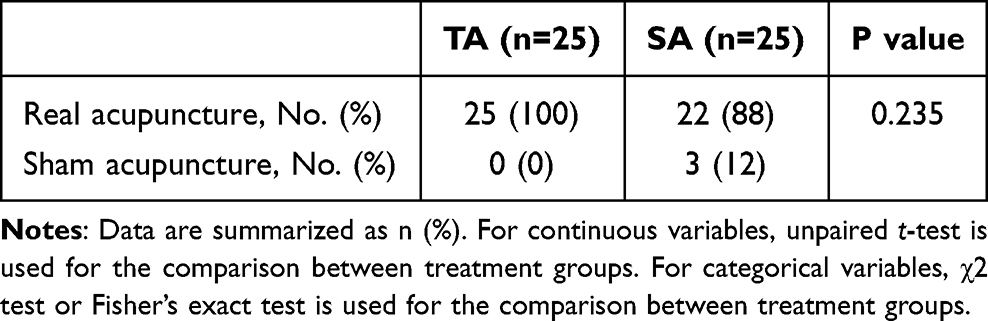 |
Table 3 Credibility of Sham Acupuncture for Patient Blinding |
Validated Metabolite Characterization
To ensure the reliability of the metabolomic analysis, principal component analysis (PCA) was conducted on quality control (QC) samples and all plasma samples. The PCA plot demonstrated tight clustering of QC samples, confirming high instrument stability and excellent data repeatability throughout the analytical process (Figure 2).
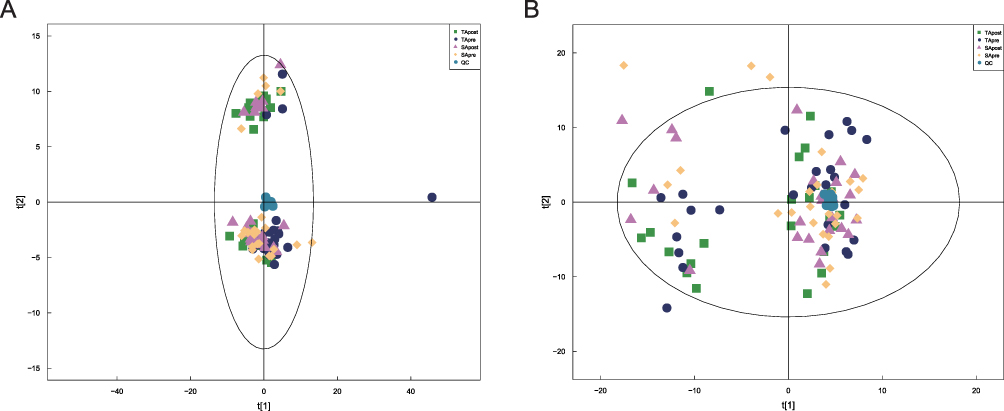 |
Figure 2 Principal component analysis of population sample. (A) Positive ion mode; (B) Negative ion mode. |
Using an in-house database (Shanghai Applied Protein Technology) and a locally constructed database of standardized products from Zhongke New Life, a total of 1,155 metabolites were identified across positive and negative ion modes, 774 in positive ion mode and 381 in negative ion mode. Structural verification was performed manually, with all identifications meeting or exceeding Level 2 criteria. The identified metabolites predominantly comprised lipids and lipid-like molecules (n=400) and organic acids and derivatives (n=175), with additional categories such as organoheterocyclic compounds (n=159) and benzenoids (n=124) also well-represented (Figure 3).
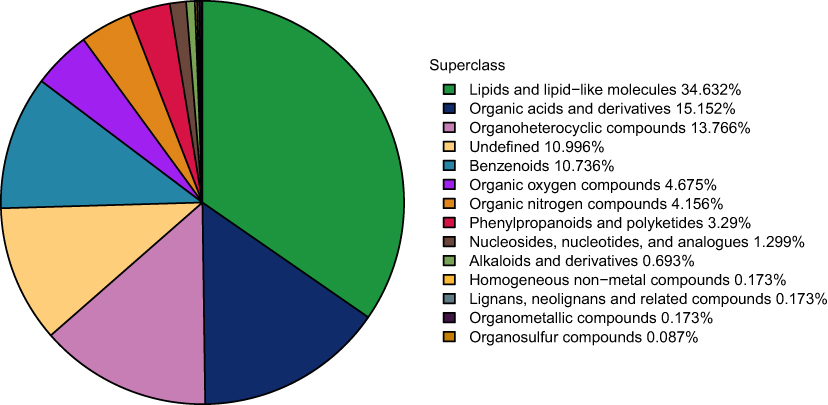 |
Figure 3 The proportion of the identified metabolites in each chemical category. The different colored blocks in the figure express different chemical classification attribution entries, and the percentage represents the percentage of that chemical classification attribution in the metabolite number to the number of all identified metabolites. Metabolites with no chemical classification attribution are defined as undefined. |
Detection of Treatment-Specific Differential Metabolites
Differential metabolites were determined using variable importance in projection (VIP) scores ≥1 from the first two principal components of the orthogonal partial least squares discriminant analysis (OPLS-DA) model, coupled with P-values <0.05 (Figure 4 and Table S1). The model’s robustness was validated by a Q² value >0.5 from 7-fold cross-validation and permutation tests to rule out overfitting, as shown in Table 4 and Figure 5. Across the comparison groups, integrating data from both ion modes, the analysis identified 73 differential metabolites between TApre and SApre (36 upregulated, 37 downregulated), 109 between TApost and SApost (31 upregulated, 78 downregulated), 88 between TApre and TApost (25 upregulated, 63 downregulated), and 40 between SApre and SApost (3 upregulated, 37 downregulated), as summarized in Table 5 and Figure 6.
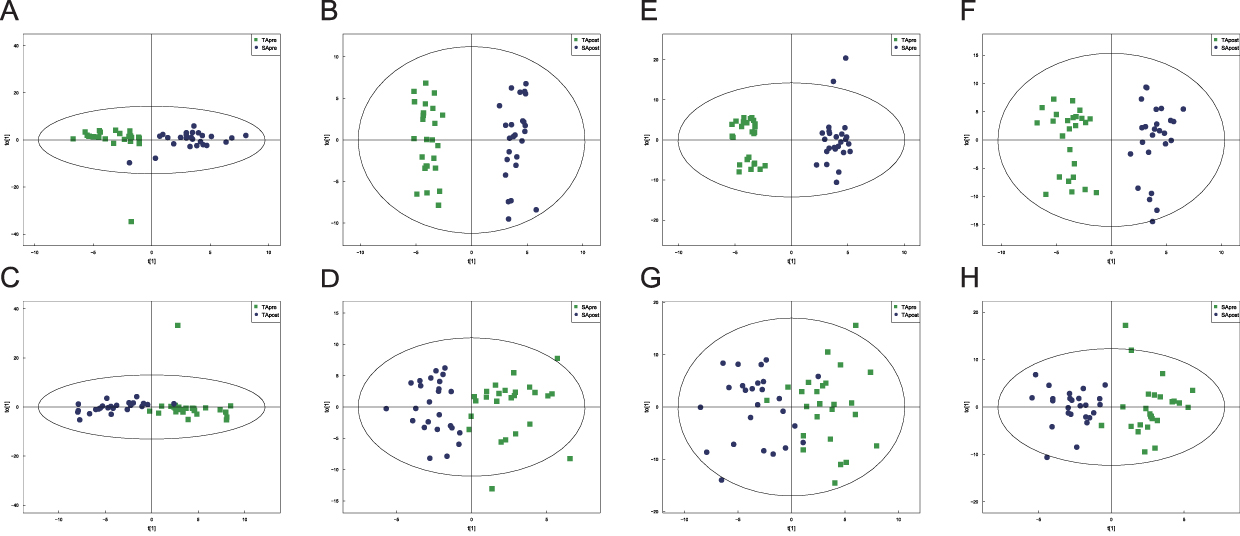 |
Figure 4 OPLS-DA results between groups. The OPLS-DA score plots of the positive ion mode (A–D) and negative ion mode (E–H). t[1] represents principal component 1, to[1] represents principal component 2, and ellipses represent 95% confidence intervals. Dots of the same color indicate individual biological replicates within a group, and the distribution status of the dots reflects the degree of variation between and within groups. (A and E) TApre vs SApre comparison. (B and F) TApost vs SApost comparison. (C and G) TApre vs TApost comparison. (D and H) SApre vs SApost comparison. |
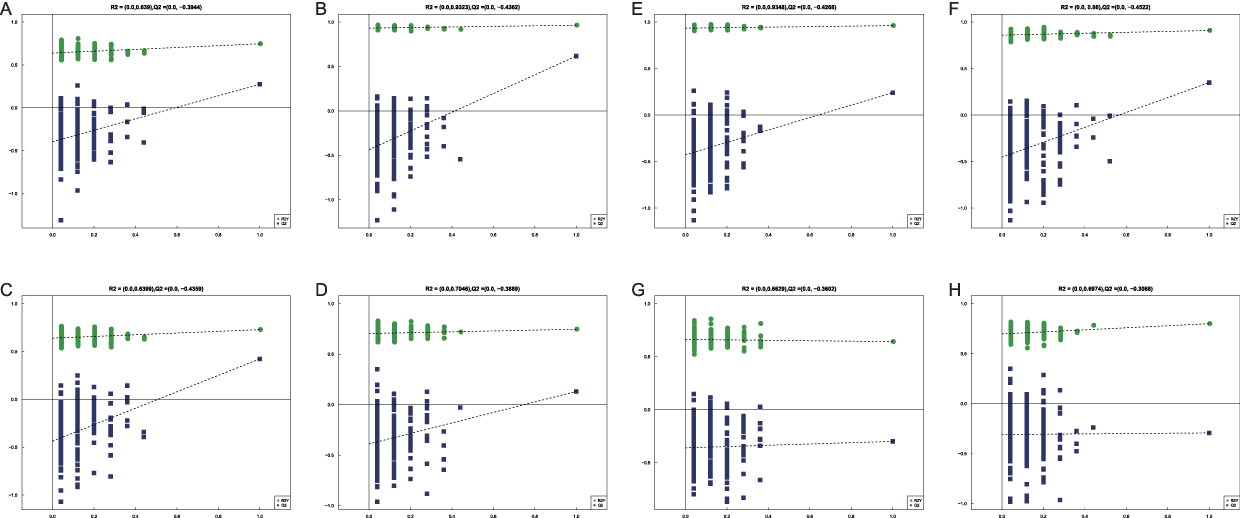 |
Figure 5 Validation of the Orthogonal Projections to Latent Structures Discriminant Analysis (OPLS-DA) Model. The validation plots of the positive ion mode (A–D) and negative ion mode (E–H). The abscissa in the figure indicates the permutation retention degree, namely the proportion consistent with the sequence of the Y variable of the original model. The ordinate represents the values of R2 and Q2. The green dots signify R2, and the blue dots represent Q2. The two dotted lines respectively denote the regression lines of R2 and Q2. The R2 and Q2 in the upper right corner indicate that the permutation retention degree is equal to 1, that is, the R2 and Q2 values of the original model. The validation plots correspond to the OPLS-DA models shown in Figure 4: (A and E) TApre vs SApre model validation. (B and F) TApost vs SApost model validation. (C and G) TApre vs TApost model validation. (D and H) SApre vs SApost model validation. |
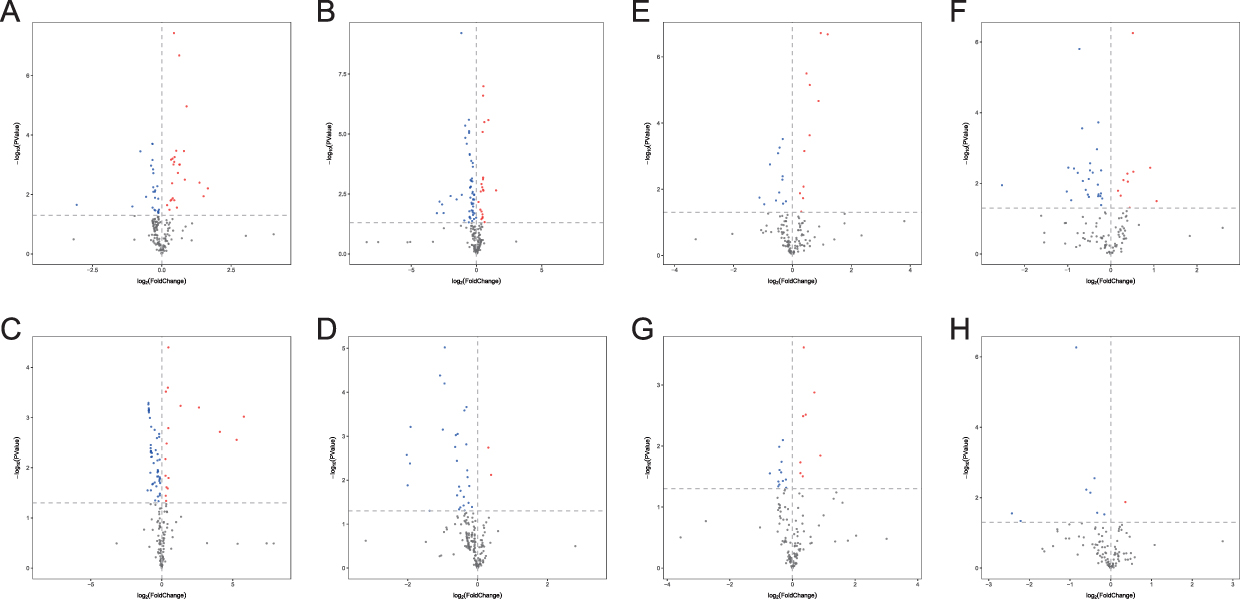 |
Figure 6 Results of volcano plot analysis. The volcano plots of the positive ion mode (A–D) and negative ion mode (E–H). Blue indicates significantly down-regulated differential metabolites, and red indicated significantly up-regulated differential metabolites, black indicates metabolites with no significant difference. The volcano plots correspond to the four group comparisons: (A and E) TApre vs SApre. (B and F) TApost vs SApost. (C and G) TApre vs TApost. (D and H) SApre vs SApost. |
 |
Table 4 Model Evaluation Parameters Q2 |
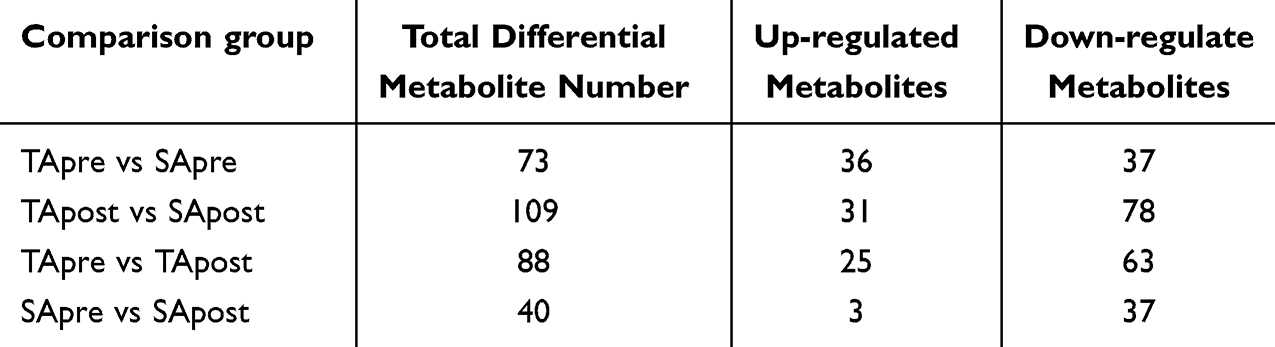 |
Table 5 Differential Metabolites Identified in Positive and Negative Ion Modes |
Metabolites Correlated with Reduced Migraine Symptoms
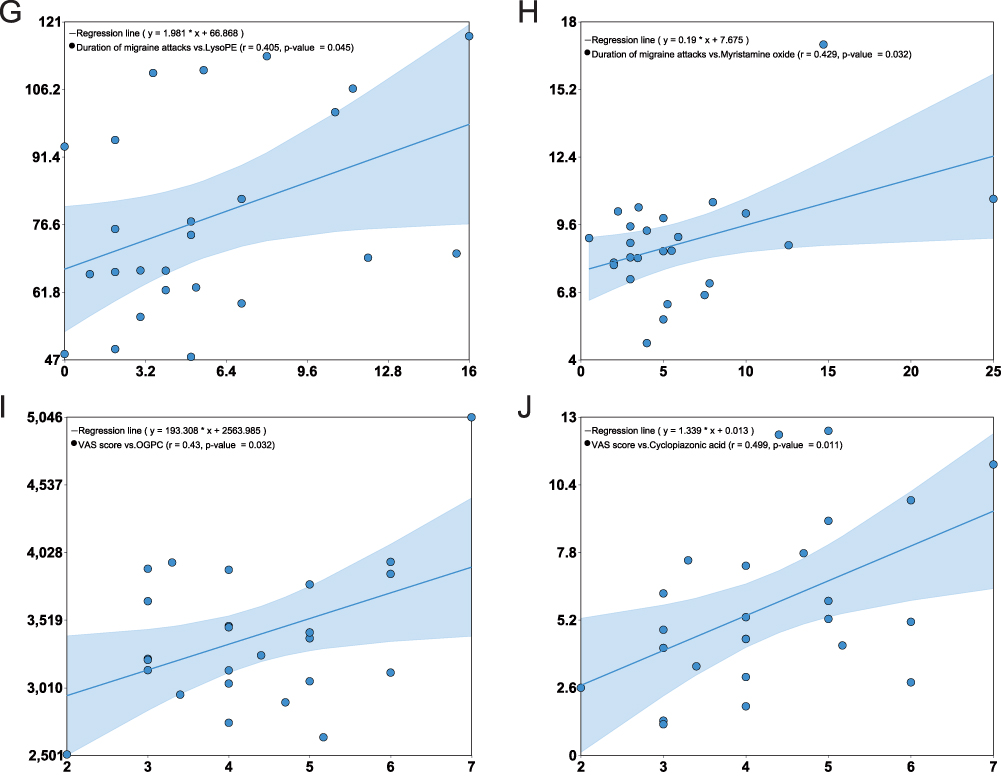
Correlation analyses elucidated the relationships between differential metabolites and clinical efficacy indicators. In the TA group, LysoPE was positively correlated with the duration of migraine attacks (r=0.405, p<0.05) but negatively correlated with the MSQ emotional functional subscale (r=−0.458, p<0.05), suggesting its potential role in emotional well-being. Pe (16:0/19,20-epdpe) showed negative correlations with both attack duration (r=−0.401, p<0.05) and VAS scores (r=−0.418, p<0.05), indicating a possible link to pain reduction. Additionally, Sm d34:1 and linoleoylglycine were positively associated with the MSQ emotional functional subscale (r=0.433 and r=0.459, respectively; p<0.05), while N, N’-dimethylurea was negatively correlated with the MSQ restrictive subscale (r=−0.432, p<0.05). These findings, alongside post-treatment trends in metabolite concentrations, are detailed in Table 6 and Figure 7. In the SA group, myristamine oxide exhibited a positive correlation with attack duration (r=0.429, p<0.05), while 1-oleoyl-sn-glycero-3-phosphocholine (OGPC) and cyclopiazonic acid were positively associated with VAS scores (r=0.43 and r=0.499, respectively; p<0.05). The observed reductions in these metabolites post-treatment aligned with decreases in attack duration and pain intensity.
Figure 7 Continued. Figure 7 Correlations Between Metabolite Levels and Clinical Outcomes. This figure presents the significant correlations (P < 0.05) between changes in metabolite levels and clinical outcomes for the TA group (A–G) and the SA group (H–J). The horizontal axis represents clinical outcomes, and the vertical axis represents metabolite levels. In the TA group: (A) A negative correlation was observed between PE (16:0/19,20-epDPE) and migraine duration (r = −0.401). (B) A negative correlation was found between PE(16:0/19,20-epDPE) and VAS scores (r = −0.418). (C) A negative correlation was found between N, N’-dimethylurea and MSQ restrictive subscale (r = −0.432). (D) A positive correlation was identified between SM(d34:1) and MSQ emotional subscale (r = 0.433). (E) A positive correlation was identified between linoleoylglycine and MSQ emotional subscale (r = 0.459). (F) A negative correlation was found between LysoPE and MSQ emotional subscale (r = −0.458). (G) A positive correlation was identified between LysoPE and migraine duration (r = 0.405). In the SA group: (H) Myristamine oxide was positively correlated with migraine duration (r = 0.429). (I) OGPC showed a positive correlation with VAS scores (r = 0.43). (J) Cyclopiazonic acid was positively correlated with VAS scores (r = 0.499). An asterisk (*) denotes a statistically significant correlation (p < 0.05).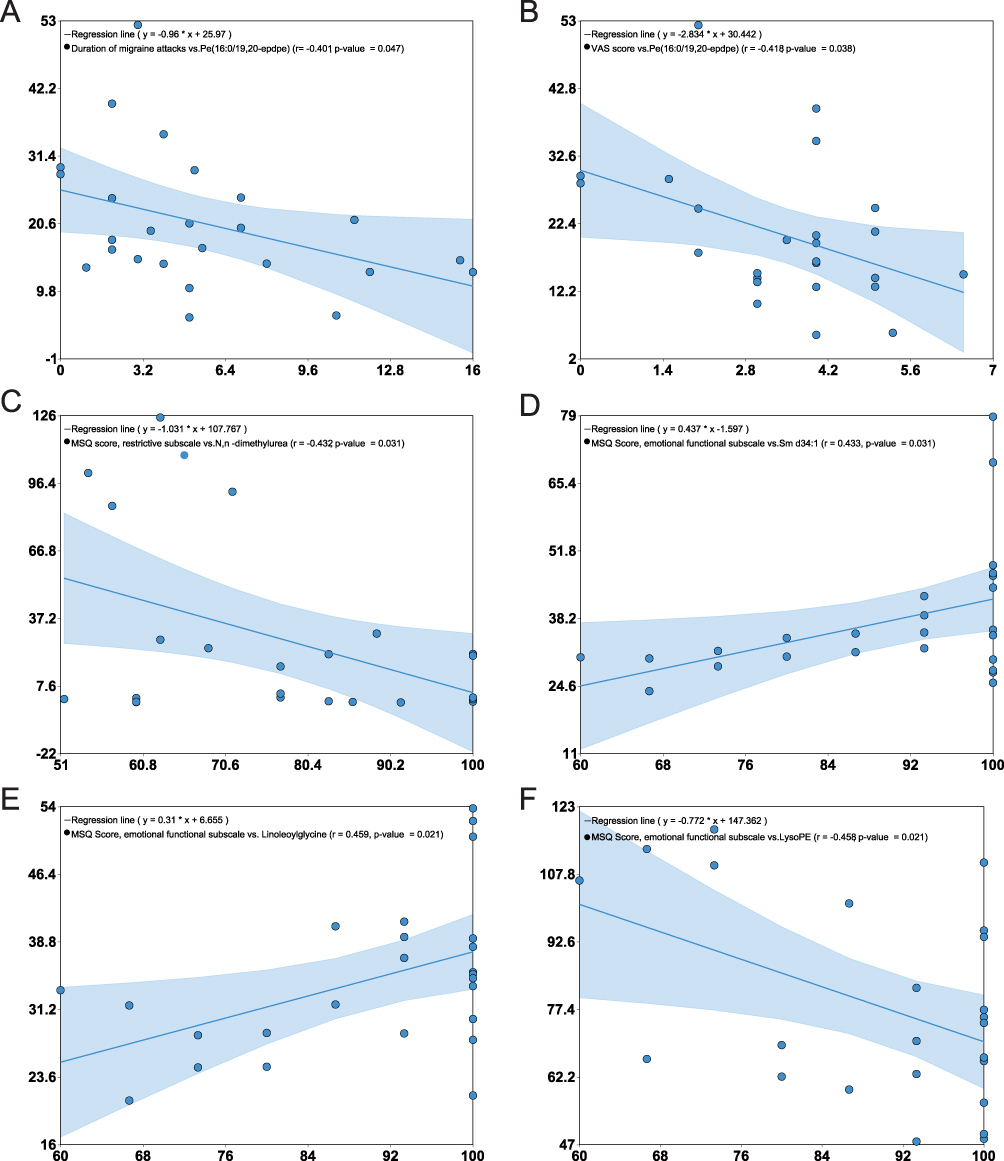
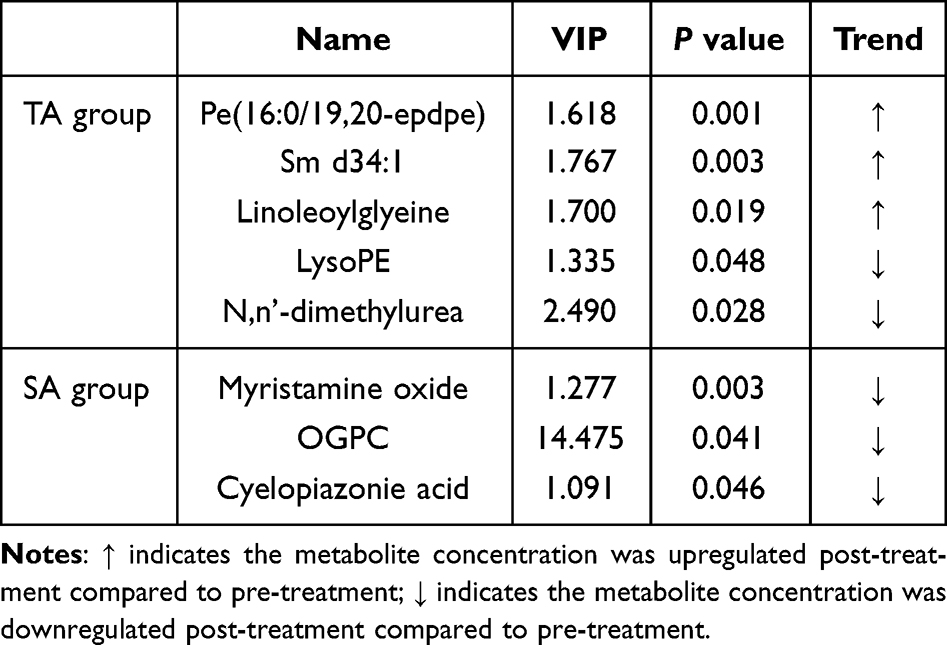 |
Table 6 Details of Relevant Differential Metabolites |
TA-Modulated Amino Acid and Pyrimidine Metabolism Pathways
Pathway analysis of the 88 differential metabolites in the TA group, performed using the Metabo Analyst database, identified 14 associated pathways, with five showing significant enrichment (P<0.05): arginine biosynthesis, glycine, serine and threonine metabolism, phenylalanine, tyrosine and tryptophan biosynthesis, arginine and proline metabolism, and pyrimidine metabolism. Key metabolites, including arginine, L-citrulline, creatine, and phenylpyruvate, underscored these pathways’ relevance. In the SA group, 40 differential metabolites were linked to two primary pathways, with glycerophospholipid metabolism significantly enriched (p<0.05), particularly involving LysoPC (18:1/0:0) (Figure 8 and Table S2).
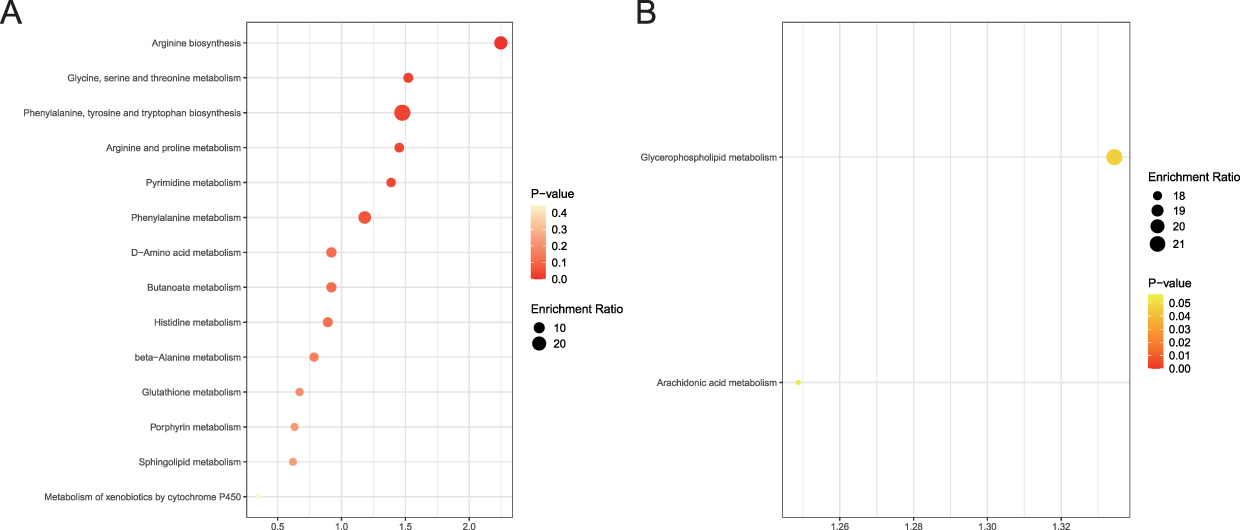 |
Figure 8 Metabolic Pathway Enrichment Analysis. This figure displays the metabolic pathways that were significantly enriched (P < 0.05) in each treatment group. (A) In the TA group, pathways primarily related to amino acid and pyrimidine metabolism were enriched, as determined by the Kyoto Encyclopedia of Genes and Genomes (KEGG). (B) In the SA group, enriched pathways were predominantly associated with lipid metabolism. The x-axis represents the enrichment factor, and the size of each dot corresponds to the number of metabolites identified in that pathway. |
Discussion
This study demonstrates that true acupuncture (TA) significantly outperforms sham acupuncture (SA) in reducing migraine attack frequency and severity, while metabolomic analysis reveals distinct biochemical changes underpinning TA’s therapeutic effects. By integrating clinical outcomes with metabolic profiles, we provide novel insights into acupuncture’s mechanisms, bridging traditional Chinese medicine (TCM) principles with modern biomedical frameworks. Specifically, TA significantly modulates amino acid and pyrimidine metabolism pathways, alongside influencing lipid metabolites associated with symptom relief, whereas SA predominantly affects glycerophospholipid metabolism pathways. These metabolic distinctions align with TCM’s focus on restoring Qi and blood flow, providing a scientific basis for TA’s efficacy in migraine management.
True acupuncture’s clinical efficacy for migraines is evident in its significant reduction in attack frequency (p < 0.05) compared to SA, corroborating prior randomized controlled trials (RCTs).5,6 The TA group’s improvements in secondary outcomes, attack duration, visual analog scale (VAS) scores, Headache Impact Test-6 (HIT-6) scores, and Migraine-Specific Quality of Life (MSQ) emotional functional subscale, highlight its multifaceted benefits. Notably, the enhanced MSQ emotional functional subscale suggests that acupuncture mitigates the psychological burden of migraines, a critical finding given the high prevalence of anxiety and depression among patients. This finding resonates with the modern biopsychosocial model of pain, which acknowledges the interplay between physiological, psychological, and social factors in chronic conditions like migraine. From a neurobiological perspective, acupuncture is thought to modulate limbic and paralimbic structures involved in emotion and pain processing.18,19 These results align with the holistic treatment philosophy of TCM, which, through acupoint stimulation, exerts a dual therapeutic effect of pain alleviation and emotional regulation. This integrated approach leads to concurrent improvements in both the physiological and psychological dimensions of migraine, providing a potential bridge between ancient therapeutic concepts and contemporary neuroscience. The absence of significant changes in acute pain medication use and MSQ restrictive subscale may reflect the 4-week treatment duration, shorter than the 8–12 weeks typical in acupuncture trials. Alternatively, patient adherence to medication habits or placebo effects in the SA group, potentially elicited by superficial needling, could contribute to these null findings.
Metabolomic analysis reveals distinct biochemical mechanisms underlying TA’s efficacy, identifying 1,155 metabolites, with 88 showing significant pre- and post-treatment differences in the TA group compared to 40 in the SA group. These findings not only suggest that TA exerts a broader and more systematic influence on metabolic regulation, but also provide molecular-level evidence supporting the specificity and therapeutic superiority of acupoint stimulation. Particularly noteworthy is that lipid and lipid-like molecules—numbering 400 in total—predominated among the differentially expressed metabolites, underscoring the pivotal role of lipid metabolism in acupuncture-induced effects. This observation is consistent with recent advances in migraine research, which have established lipid metabolism dysregulation as a key pathological mechanism underlying migraine pathogenesis, with implications for neuroinflammation, vascular function, and pain modulation.10,14,20
TA specifically downregulates the expression of the pro-inflammatory lipid mediator LysoPE, the level of which is positively correlated with the duration of migraine attacks. Concurrently, TA significantly upregulates the anti-inflammatory lipid mediator PE(16:0/19,20-epDPE), which exhibits a significant negative correlation with both attack duration and VAS score. Both LysoPE and PE(16:0/19,20-epDPE) belong to the class of Glycerophosphoethanolamines. Current evidence suggests that this class of bioactive lipids may modulate inflammatory processes by suppressing inflammasome activation.21 Moreover, the regulatory role of sphingolipid Sm d34:1 provides additional evidence that acupuncture may lower the risk of migraine attacks through modulation of the ceramide metabolic pathway.14 The positive correlation with the MSQ emotional function subscale underscores the link between lipid metabolism and emotional well-being, aligning with the traditional Chinese medicine concept of mind-body regulation. Collectively, these findings indicate that acupuncture may mitigate the inflammatory profile characteristic of migraines and contribute to the restoration of metabolic homeostasis. In contrast, SA’s limited metabolic impact, evidenced by correlations of myristamine oxide with attack duration and OGPC with VAS scores, suggests non-specific effects.
Pathway analysis revealed that TA treatment significantly enriched arginine biosynthesis and glycine, serine, and threonine metabolism (p < 0.05). Specifically, TA modulates the arginine biosynthesis pathway, thereby enhancing nitric oxide production and improving cerebral microcirculatory perfusion. These regulatory effects are consistent with findings from previous studies indicating the critical role of arginine metabolism in migraine pathophysiology.12,22,23 The metabolic products of glycine and serine contribute to the inhibition of neural transmission and the enhancement of antioxidant defense mechanisms, thereby preventing excessive neuronal excitation.24 By modulating its associated pathways, TA may inhibit NMDA receptor activation, attenuate cortical spreading depression—a key mechanism underlying migraine aura and pain—and ultimately disrupt the cascade of migraine attacks.25
Notably, this study represents the first attempt to associate the therapeutic mechanism of acupuncture with pyrimidine metabolism. While direct evidence linking pyrimidine metabolism to migraine remains lacking, accumulating indirect evidence indicates that this metabolic pathway may play a crucial role in migraine pathogenesis. Research has demonstrated that uridine, a central metabolite in pyrimidine metabolism, can promote creatine phosphate synthesis through the activation of mitochondrial ATP-sensitive potassium channels, enhance cellular antioxidant defenses, and modulate mitochondrial function.26,27 Given the central role of mitochondrial dysfunction in migraine pathogenesis, the disruption of cerebral energy metabolism during migraine attacks may lead to oxidative stress, impaired glutamatergic neurotransmission, and neurogenic inflammation.28 Acupuncture may disrupt the pathological progression of migraine through the regulation of pyrimidine metabolism and the restoration of cerebral energy homeostasis. This newly identified metabolic pathway offers a novel perspective for elucidating the multi-target therapeutic mechanisms of acupuncture.
Metabolomics analysis further underscores the mechanistic distinctions between acupuncture and sham acupuncture. Although sham acupuncture (SA) can induce alterations in certain lipid metabolic pathways, such as glycerophospholipid metabolism, it lacks comprehensive regulation of amino acid and pyrimidine metabolic networks. These findings suggest that SA may elicit limited placebo effects via non-specific mechanisms, whereas true acupuncture (TA) exerts maximal therapeutic effects through synergistic modulation of multiple metabolic pathways.
In summary, metabolomics has elucidated the multi-dimensional regulatory mechanisms underlying acupuncture’s therapeutic effects on migraine from a systems biology perspective. By synergistically modulating the three core metabolic networks—lipid metabolism, amino acid metabolism, and pyrimidine metabolism. Acupuncture exerts its therapeutic actions across multiple physiological levels, including anti-inflammatory effects, neural regulation, vascular function improvement, energy homeostasis restoration, and mitochondrial function protection. These findings not only provide robust scientific evidence supporting the efficacy of acupuncture but also offer novel insights and potential targets for metabolic-based therapeutic strategies in migraine treatment.
At present, there is no universally accepted method for calculating the sample size in metabolomics. Clinical studies on migraine-related metabolomics mostly adopt a sample design of 10 to 30 cases per group.12,29,30 However, considering the significant inter-individual variation characteristics of metabolomics data, despite each group having a sample size of 25 cases in this study, there may still be certain limitations in terms of statistical power. Consequently, the study may be underpowered to detect more subtle metabolic changes, and the findings should be interpreted with caution. However, this research provides valuable preliminary data and serves as a hypothesis-generating study that paves the way for larger, more definitive trials. The 4-week treatment duration, shorter than typical TCM protocols (8–12 weeks), may explain null findings in functional outcomes. Non-penetrating sham devices were employed to minimize the non-specific effects associated with superficial needling in the SA protocol. While this method effectively blinds participants and controls for the ritual of needling, it does not differentiate between acupoint-specific effects and the general physiological effects of tactile stimulation at those locations. Future studies could incorporate an additional control group, as suggested, using either sham needling at non-acupoints or true needling at irrelevant acupoints. Such a design would help to further dismantle the components of acupuncture’s efficacy and isolate the specific contributions of acupoint location versus the act of needling itself. Despite these constraints, the findings advocate for acupuncture’s integration into evidence-based migraine care and underscore metabolomics’ potential to validate TCM’s therapeutic principles.
Conclusion
This study demonstrates that true acupuncture (TA) significantly outperforms sham acupuncture in reducing migraine frequency, duration, and severity, while improving emotional well-being and quality of life. Non-targeted plasma metabolomics revealed that TA exerts anti-inflammatory, neuroregulatory, and energy homeostasis-restoring effects through the regulation of lipid, amino acid, and pyrimidine metabolism, thereby providing a theoretical foundation for the biomedical mechanisms underlying acupuncture. Key metabolites—including LysoPE, PE(16:0/19,20-epDPE), SM d34:1, linoleoylglycine, and N,N’-dimethylurea—emerging as potential biomarkers. However, given the study’s modest sample size and short duration, these findings on metabolic biomarkers should be considered preliminary, and the generalizability of the results is limited. Future research should prioritize larger, longer-term randomized controlled trials, multi-omics approaches, and acupoint-specific metabolic profiles to optimize protocols and establish acupuncture as a cost-effective, personalized therapy for migraine management.
Abbreviations
TA, true acupuncture; SA, sham acupuncture; LysoPE, 1-oleoyl-sn-glycero-3-phosphoethanolamine; OGPC, 1-oleoyl-sn-glycero-3-phosphocholine; UHPLC-Q-Exactive-Orbitrap-MS, ultra-high performance liquid chromatography with Q-Exactive Orbitrap tandem mass spectrometry; PSD, Park Sham Device; VAS, visual analog scale; MSQ, migraine-specific quality of life; HIT-6, Headache Impact Test-6; OPLS-DA, Orthogonal partial least squares discriminant analysis; PE, phosphatidylethanolamine; APS, antiphospholipid syndrome; LysoPC, lysophosphatidylcholine; ATP, adenosine triphosphate.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board and ethics committee of Chengdu University of Traditional Chinese Medicine (NO. 2020KL-003). Written informed consent will be obtained from patients prior to enrolment in the study.
Consent for Publication
All authors have reviewed and approved the final manuscript and consent to its publication.
Acknowledgments
Lei Gao and Ying Chen are co-first authors for this study. We thank Shanghai Applied Protein Technology Biotechnology Co., LTD, for technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Key Research and Development Program (No. 2019YFC1709700) and the National Natural Science Foundation (No. 82430124). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ashina M, Buse DC, Ashina H, et al. Migraine: integrated approaches to clinical management and emerging treatments. Lancet. 2021;397(10283):1505–1518. doi:10.1016/S0140-6736(20)32342-4
2. Steiner TJ, Stovner LJ, Jensen R, et al. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21(1):137. doi:10.1186/s10194-020-01208-0
3. Skyhøj Olsen T. Migraine with and without aura: the same disease due to cerebral vasospasm of different intensity. A hypothesis based on CBF studies during migraine. Headache. 1990;30(5):269–272. doi:10.1111/j.1526-4610.1990.hed3005269.x
4. Ashina M, Hansen JM, Do TP, et al. Migraine and the trigeminovascular system-40 years and counting. Lancet Neurol. 2019;18(8):795–804. doi:10.1016/S1474-4422(19)30185-1
5. Fan SQ, Jin S, Tang T-C, et al. Efficacy of acupuncture for migraine prophylaxis: a trial sequential meta-analysis. J Neurol. 2021;268(11):4128–4137. doi:10.1007/s00415-020-10178-x
6. Zhao L, Chen J, Li Y, et al. The long-term effect of acupuncture for migraine prophylaxis: a randomized clinical trial. JAMA Intern Med. 2017;177(4):508–515. doi:10.1001/jamainternmed.2016.9378
7. Xu S, Yu L, Luo X, et al. Manual acupuncture versus sham acupuncture and usual care for prophylaxis of episodic migraine without aura: multicentre, randomised clinical trial. BMJ. 2020;368:m697. doi:10.1136/bmj.m697
8. Linde K, Allais G, Brinkhaus B, et al. Acupuncture for the prevention of episodic migraine. Cochrane Database Syst Rev. 2016;2016(6):Cd001218. doi:10.1002/14651858.CD001218.pub3
9. Ren C, Liu J, Zhou J, et al. Low levels of serum serotonin and amino acids identified in migraine patients. Biochem Biophys Res Commun. 2018;496(2):267–273. doi:10.1016/j.bbrc.2017.11.203
10. Onderwater GLJ, Ligthart L, Bot M, et al. Large-scale plasma metabolome analysis reveals alterations in HDL metabolism in migraine. Neurology. 2019;92(16):e1899–e1911. doi:10.1212/WNL.0000000000007313
11. Wen Z, He M, Peng C, et al. Metabolomics and 16S rRNA gene sequencing analyses of changes in the intestinal flora and biomarkers induced by Gastrodia-Uncaria treatment in a rat model of chronic migraine. Front Pharmacol. 2019;10:1425. doi:10.3389/fphar.2019.01425
12. Liu L, Li W, Wang L, et al. Proteomic and metabolomic profiling of acupuncture for migraine reveals a correlative link via energy metabolism. Front Neurosci. 2022;16:1013328. doi:10.3389/fnins.2022.1013328
13. Gross EC, Lisicki M, Fischer D, et al. The metabolic face of migraine - from pathophysiology to treatment. Nat Rev Neurol. 2019;15(11):627–643. doi:10.1038/s41582-019-0255-4
14. Peterlin BL, Mielke MM, Dickens AM, et al. Interictal, circulating sphingolipids in women with episodic migraine: a case-control study. Neurology. 2015;85(14):1214–1223. doi:10.1212/WNL.0000000000002004
15. Gao Z, Liu X, Yu S, et al. Electroacupuncture at acupoints reverses plasma glutamate, lipid, and LDL/VLDL in an acute migraine rat model: a 1 H NMR-based metabolomic study. Evid Based Complement Alternat Med. 2014;2014:659268. doi:10.1155/2014/659268
16. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
17. Li Y, Liang F, Yang X, et al. Acupuncture for treating acute attacks of migraine: a randomized controlled trial. Headache. 2009;49(6):805–816. doi:10.1111/j.1526-4610.2009.01424.x
18. Claunch JD, Chan S-T, Nixon EE, et al. Commonality and specificity of acupuncture action at three acupoints as evidenced by FMRI. Am J Chin Med. 2012;40(4):695–712. doi:10.1142/S0192415X12500528
19. Li YW, Li W, Wang S-T, et al. The autonomic nervous system: a potential link to the efficacy of acupuncture. Front Neurosci. 2022;16:1038945. doi:10.3389/fnins.2022.1038945
20. Liampas I, Mylonas KS, Brotis A, et al. Serum lipid abnormalities in migraine: a meta-analysis of observational studies. Headache. 2021;61(1):44–59. doi:10.1111/head.14039
21. Hao T, Zhang X, Liu Q, et al. Phosphatidylethanolamine exerts anti-inflammatory action by regulating mitochondrial function in macrophages of large yellow croaker (Larimichthys crocea). FASEB J. 2024;38(22):e70180. doi:10.1096/fj.202401279RR
22. Chen SF, Pan M-X, Tang J-C, et al. Arginine is neuroprotective through suppressing HIF-1α/LDHA-mediated inflammatory response after cerebral ischemia/reperfusion injury. Mol Brain. 2020;13(1):63. doi:10.1186/s13041-020-00601-9
23. Onderwater GLJ, van Dongen RM, Harms AC, et al. Cerebrospinal fluid and plasma amine profiles in interictal migraine. Ann Neurol. 2023;93(4):715–728. doi:10.1002/ana.26576
24. Ringlet S, Motta Z, Vandries L, et al. Glycine-gated extrasynaptic NMDARs activated during glutamate spillover drive burst firing in nigral dopamine neurons. Prog Neurobiol. 2025;249:102773. doi:10.1016/j.pneurobio.2025.102773
25. Kucharz K, Søndergaard Rasmussen I, Bach A, et al. PSD-95 uncoupling from NMDA receptors by Tat- N -dimer ameliorates neuronal depolarization in cortical spreading depression. J Cereb Blood Flow Metab. 2017;37(5):1820–1828. doi:10.1177/0271678X16645595
26. Krylova IB, Selina EN, Bulion VV, et al. Uridine treatment prevents myocardial injury in rat models of acute ischemia and ischemia/reperfusion by activating the mitochondrial ATP-dependent potassium channel. Sci Rep. 2021;11(1):16999. doi:10.1038/s41598-021-96562-7
27. Yokoyama S, Nakagawa I, Ogawa Y, et al. Ischemic postconditioning prevents surge of presynaptic glutamate release by activating mitochondrial ATP-dependent potassium channels in the mouse hippocampus. PLoS One. 2019;14(4):e0215104. doi:10.1371/journal.pone.0215104
28. Borkum JM. Brain energy deficit as a source of oxidative stress in migraine: a molecular basis for migraine susceptibility. Neurochem Res. 2021;46(8):1913–1932. doi:10.1007/s11064-021-03335-9
29. Aczél T, Körtési T, Kun J, et al. Identification of disease- and headache-specific mediators and pathways in migraine using blood transcriptomic and metabolomic analysis. J Headache Pain. 2021;22(1):117. doi:10.1186/s10194-021-01285-9
30. Li C, Li X, He K, et al. Discovery of the mechanisms of acupuncture in the treatment of migraine based on functional magnetic resonance imaging and omics. Front Med. 2023;17(5):993–1005. doi:10.1007/s11684-023-0989-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.