Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Clinical Disease Burden in Patients with Chronic Obstructive Pulmonary Disease and Type 2 Inflammation in Japan: A Retrospective Database Analysis (EUROS Study)
Authors Muro S ![]() , Orimo M, Sunaga Y
, Orimo M, Sunaga Y ![]() , Inokuchi S
, Inokuchi S ![]() , Tokuda M
, Tokuda M ![]() , Ishida M
, Ishida M ![]()
Received 3 December 2025
Accepted for publication 22 May 2026
Published 30 June 2026 Volume 2026:21 586341
DOI https://doi.org/10.2147/COPD.S586341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Prof. Dr. Zijing Zhou
Shigeo Muro1, Mami Orimo2, Yoshinori Sunaga3, Shoichiro Inokuchi4, Makoto Tokuda4, Masato Ishida2
1Department of Respiratory Medicine, Nara Medical University, Nara, Japan; 2Respiratory and Rhinology Medical, Sanofi K.K., Tokyo, Japan; 3Real World Evidence Generation Partnering, Sanofi K.K., Tokyo, Japan; 4Real World Evidence Division, Pharmaceutical Division Business Unit, JMDC Inc., Tokyo, Japan
Correspondence: Masato Ishida, Respiratory & Rhinology Medical Head, Alliance Immunology, Specialty Care Medical, Sanofi K.K., Tokyo Opera City Tower, 3-20-2 Nishi-Shinjuku, Tokyo, 163-1488, Japan, Tel +81-70-4023-4256, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality globally. Preventing COPD exacerbations is a primary goal in disease management. A subset of patients with COPD exhibits type 2 inflammation (T2I), but the clinical implications of T2I in Japanese patients are not understood.
Patients and Methods: We used a nationwide Japanese electronic medical records database to evaluate the clinical implications of T2I in COPD, focusing on COPD exacerbations and major adverse cardiovascular events (MACE). T2I was based on blood eosinophil counts and defined as low (< 100 cells/μL), intermediate (100– 300 cells/μL) or high (> 300 cells/μL). Eosinophil counts were assessed from outpatient measurements during a 12-month baseline period, with the highest value used to define T2I status. The patients were identified during the study period from January 1, 2010, and September 30, 2023.
Results: Of 10,321 eligible patients, 67.3% were male; the median age was 75.0 years. The adjusted incidence rate of combined moderate and severe COPD exacerbations was significantly higher in patients with high T2I compared with intermediate T2I (rate ratio [RR]: 1.16, 95% confidence interval [CI]: 1.08, 1.24). Exacerbation incidence was also higher in high versus low T2I (RR: 1.21, 95% CI: 1.08, 1.37). No statistically significant differences were observed in MACE incidence; compared with the intermediate T2I group, the adjusted rate of MACE was numerically lower in the low T2I group and higher in the high T2I group.
Conclusion: T2I was associated primarily with an increased risk of moderate COPD exacerbations, a clinically meaningful driver of clinical burden and healthcare utilization in Japan. Cardiovascular analyses were underpowered. These findings highlight the potential clinical relevance of T2I for risk stratification in COPD and the need for further studies to refine eosinophil-based endotyping and clarify its implications for treatment response in this population.
Keywords: chronic obstructive pulmonary disease, electronic health records, eosinophils, exacerbations, real-world study, type 2 inflammation
Introduction
Chronic obstructive pulmonary disease (COPD), one of the leading causes of morbidity and the fourth most common cause of mortality worldwide, is characterized by persistent respiratory symptoms and airflow limitation due to abnormalities in the airways (bronchitis, bronchiolitis) and/or alveoli (emphysema).1–3 Treatment strategies for COPD focus on symptom control and prevention of COPD exacerbations (the acute worsening of symptoms), with long-acting bronchodilators recommended as first-line treatment in both global and Japanese guidelines.1,4
Although recommendations on the management and treatment of COPD are largely consistent between global and Japanese guidelines,1,4 the frequency of COPD exacerbations varies between countries, with multiple studies reporting that exacerbations are less frequent in Japanese people compared with those from Western countries.5,6 In addition, the characteristics of individuals with COPD in Japan differ from those in Western countries, with Japanese patients typically having a lower body mass index (BMI) and a greater likelihood of having an emphysema endotype.5 These differences suggest that biomarkers of exacerbation risk, including type 2 inflammatory markers, may function differently across populations.
COPD is a clinically heterogeneous disease that has traditionally been classified into emphysema-dominant and chronic bronchitis (CB)-dominant subtypes.7 However, increasing evidence suggests that COPD encompasses a broader range of phenotypes beyond this binary classification.8 In particular, a subset of patients with COPD exhibits type 2 inflammation, a distinct immunological profile characterized by elevated levels of interleukin (IL)-4, IL-5, and IL-13, and associated immune cell activation.9 This inflammatory endotype is often identified through biomarkers, such as blood eosinophil counts, fractional exhaled nitric oxide (FeNO), and cytokine profiles in respiratory specimens.10 Blood eosinophil count is the most widely accessible biomarker for approximating this endotype, given its association with COPD exacerbations, airway inflammatory patterns, and response to inhaled corticosteroids (ICS). Furthermore, blood eosinophils correlate with several type 2 signatures in sputum or bronchial samples and have been incorporated into treatment frameworks such as the GOLD report.11
However, the definition and classification of type 2 inflammation in COPD has yet to be fully elucidated, as blood eosinophil levels fluctuate over time and intermittent eosinophilia is common.12,13 While elevated peripheral blood eosinophil levels are associated with exacerbations,14 and it is estimated that up to 40% of patients with COPD have a type 2 inflammation phenotype/endotype,15,16 the prevalence and clinical significance of type 2 inflammation in COPD remains incompletely understood. In particular, the temporal variability of type 2 inflammation biomarkers, their prognostic relevance and cardiovascular implications, especially in Japanese patients, are not well established. Real‑world evidence is essential to capture the heterogeneity of eosinophil profiles, comorbidities, and treatment patterns encountered in routine care that are difficult to assess in controlled selected population. Large‑scale electronic medical records (EMR) data therefore provides an important opportunity to characterize type 2 inflammatory phenotypes and their clinical consequences in unselected COPD populations.
Exacerbations constitute a major component of the clinical disease burden of COPD, as they are closely linked to accelerated disease progression, impaired health status, and substantial healthcare utilization. Accordingly, evaluating the relationship between type 2 inflammation and the risk of exacerbations provides important insights into the clinical burden experienced by patients with COPD.
Furthermore, Japanese data on the relationship between type 2 inflammation and clinical outcomes, such as exacerbation risk and cardiovascular disease, are limited. To address these knowledge gaps, this study aimed to investigate the differences in characteristics and prognoses, including COPD exacerbations and cardiovascular outcomes, according to type 2 inflammation status in Japanese patients with COPD. Therefore, we aimed to determine whether higher baseline type 2 inflammation - operationalized by blood eosinophil counts - is associated with an increased risk of subsequent COPD exacerbations in a nationwide Japanese EMR cohort. We hypothesized that exacerbation risk would increase across higher type 2 inflammation strata.
Materials and Methods
Study Design, Setting and Data Source
The EUROS retrospective cohort study used real-world data from a nationwide EMR database in Japan that is maintained by the Health, Clinic, and Education Information Evaluation Institute (HCEI, Kyoto, Japan) and supported by JMDC Inc. (Tokyo, Japan).17 The database integrates medical records from 90 healthcare institutions across Japan, including both primary care clinics and specialty hospitals. The study covered the period from the earliest available date for each patient until March 31, 2024. The database undergoes routine internal quality checks, including the standardization of diagnosis codes and medical procedures, the adjustment or removal of suspected erroneous laboratory values, and ensuring the continuity of longitudinal records. In addition, the validity of this database for epidemiologic analyses has been demonstrated in prior validation studies,18–20 supporting its suitability for use in real‑world outcome research. The study protocol was approved by the MINS ethics review committee (approval number: MINS-REC-204224). This study was conducted in accordance with the guidelines for Good Pharmacovigilance Practices (GVPs) and Good Pharmacoepidemiology Practices (GPPs) issued by the International Society for Pharmacoepidemiology (ISPE), the Declaration of Helsinki and its amendments, as well as all applicable national guidelines, laws, and regulations. As this was a retrospective analysis of anonymized patient data, informed consent was not required from patients.
Patient Inclusion and Exclusion Criteria
The study included patients with a documented diagnosis of COPD, identified using the International Classification of Diseases 10th Revision (ICD-10) codes J41–J44 (Supplementary Table 1), that was recorded between January 1, 2010, and September 30, 2023. The index date was defined as the date of the first recorded diagnosis of COPD for outpatients or the discharge date for inpatients with COPD as the primary diagnosis. Eligible patients were required to be ≥40 years old at the index date, have 365 days of continuous enrollment in the EMR database prior to the study initiation, and have ≥2 recorded blood eosinophil measurements in an outpatient setting during the pre-index period (defined as starting from 365 days before the index date). A follow-up duration of ≥180 days was also required. In addition, patients were required to have received ≥1 medication for COPD, as defined by World Health Organization-Anatomical Therapeutic Chemical (WHO-ATC) codes (Supplementary Table 2), and patients were followed for up to a maximum of 1095 days (3 years) after the index date, or until death or the last available visit, whichever occurred first. The medications listed in Supplementary Table 2 include inhalants such as short-acting muscarinic antagonists (SAMA), long-acting muscarinic antagonists (LAMA), short-acting β2-agonists (SABA), long-acting β2-agonists (LABA), combinations of LABA/inhaled corticosteroid (ICS), LAMA/LABA, LAMA/LABA/ICS, as well as methylxanthines, which could be administered orally or intravenously.
To minimize confounding from non‑COPD causes of eosinophilia, we excluded patients with predefined ICD‑10 codes for conditions associated with secondary eosinophilia such as allergic bronchopulmonary aspergillosis and eosinophilic granulomatosis with polyangiitis (EGPA), or if they had prolonged systemic glucocorticoid use (≥28 days of continuous use with a prednisolone-equivalent dose of ≥5 mg/day) during the pre-index period without a prior diagnosis of asthma. To distinguish asthma and asthma-COPD overlap (ACO), asthma was identified independently using asthma-specific ICD-10 codes, and patients with both COPD and asthma codes were classified as having possible ACO.
Exposure and Outcomes
Definitions of Type 2 Inflammation
Patients were classified into three type 2 inflammation groups based on the highest recorded blood eosinophil count during the pre-index period as follows: (1) high type 2 inflammation for eosinophil counts >300 cells/μL; (2) intermediate type 2 inflammation for counts of 100–300 cells/μL; and (3) low type 2 inflammation for counts <100 cells/μL. If multiple eosinophil measurements were recorded on the same day, the highest value was used. These groups were based on eosinophil counts measured in an outpatient setting to reduce bias and variability caused by measurements taken during hospitalization. This eosinophil-based classification was used as the exposure indicator of type 2 inflammatory phenotype and was not intended as a diagnostic categorization of “eosinophilic COPD”. The classification of type 2 inflammation based on peripheral blood eosinophil counts (<100, 100–300, and >300 cells/μL) was chosen according to thresholds widely adopted in major COPD and asthma guidelines and cohort studies. These cut-offs are aligned with the GOLD 2024 report,21 the ECLIPSE cohort,14 the NOVELTY population study,5 and the ERS/ATS severe asthma guidelines,22 where similar eosinophil categories have been shown to reflect type 2 inflammatory activity and predict ICS responsiveness.
Alternative definitions of type 2 inflammation were evaluated in several sensitivity analyses.21,23,24 First, patients were classified as type 2 inflammation–positive if they had ≥2 eosinophil measurements >300 cells/μL during day −365 to day 1095. Second, a beta-distribution approach was applied using all eosinophil results from day −365 to day 0, categorizing patients as persistent-high, persistent-low, or intermittent based on posterior probabilities. Third, type 2 inflammation was defined using the mean eosinophil count from day −365 to day 0, applying the same thresholds as in the main analysis. Finally, an alternative threshold was tested by classifying patients as type 2 inflammation–positive if their maximum eosinophil count was >150 cells/μL during day −365 to day 0. Detailed methodology for these analyses is provided in Supplementary Material 1.
Primary Outcome
The primary outcome was the incidence of COPD exacerbations. Moderate exacerbations were defined as a new prescription for systemic glucocorticoids (≥20 mg/day prednisolone-equivalent for ≤14 days) or a new prescription for antibiotics in an outpatient setting. Severe exacerbations were defined as hospitalizations with either infectious codes for COPD exacerbation or codes associated with respiratory failure for COPD exacerbations as the primary diagnosis (Supplementary Table 1), identified using diagnosis procedure combination (DPC) hospital records.
Secondary Outcomes
Secondary outcomes included the incidence of major adverse cardiovascular events (MACE), defined as a composite of hospitalization for acute coronary syndrome, stroke, or heart failure, or cardiovascular death (Supplementary Table 1); MACE were identified using validated ICD‑10 coding algorithms reported in prior literature. Components of MACE were selected based on evidence of acceptable diagnostic accuracy in Japanese claims data.25–28 Prior studies have demonstrated acceptable accuracy of these codes for epidemiologic analyses and systemic glucocorticoid use, including short-term use (≥20 mg/day prednisolone-equivalent for ≤14 days), continuous use (≥14-day supply with a 14-day grace period), mean daily dose, and proportion of days covered (PDC) for systemic glucocorticoids as a measure of medication adherence.25–28
Additional outcomes included healthcare utilization metrics (such as number of emergency room visits [Supplementary Table 1] and duration of hospitalization for COPD exacerbations), and medication use patterns, including but not limited to prescriptions for LABA, LAMA, ICS, and combination therapies (Supplementary Table 2).
Statistical Analysis
Baseline characteristics were summarized using means and standard deviations (SDs) for normally distributed continuous variables, and median and interquartile range (IQR) for non-normally distributed variables. Categorical variables were expressed as counts and percentages.
Comparisons between groups were performed using t-tests or analysis of variance (ANOVA) for normally distributed continuous variables, Mann–Whitney U-tests or Kruskal–Wallis tests for non-normally distributed variables, and χ2 tests for categorical variables.
Missing data were handled according to the TARMOS framework.29 The association between patient backgrounds and key confounders, such as smoking history (indicated by the Brinkman Index score and pack-years, where scores of 0, ≥1 to <400, and ≥400 indicate 0, >0 to <20, and ≥20 pack-years, respectively) and BMI, were investigated using a regression model to understand the missing mechanism. Multivariate imputation with chained equations (MICE) was applied as multiple imputation methods under the assumption of “missing at random” (MAR) for missing smoking history and BMI values, when the proportion of missing data exceeded 5%. This MAR assumption was considered justifiable because the confounders were extracted from the simplified discharge summaries recorded in the DPC data; therefore, the missingness is strongly associated with hospitalization. The missing mechanism could be considered MAR explained by only the observed data such as other medical history. MICE could work well under this assumption. Rubin’s rule was applied to integrate the results from the multiple datasets with imputation. Otherwise, complete case analysis was performed. To enhance transparency, we evaluated predictors of missingness for smoking history and BMI to confirm that missingness was largely explained by observable clinical characteristics, consistent with a MAR mechanism. These diagnostic checks supported the use of multiple imputation, and sensitivity analyses confirmed that the covariate-adjusted estimates based on the imputed datasets were consistent with the crude estimates obtained without adjustment.
Incidence rates for COPD exacerbations and secondary outcomes were reported per 100 patient-years, with 95% confidence intervals (CIs) estimated using negative binomial models. Negative binomial regression models were used to estimate and compare incidence rates across type 2 inflammation groups, adjusting for the covariates of age, sex, smoking history, BMI, lung cancer, malignancy (excluding nonmelanoma skin cancer and lung cancer), and other relevant confounders. A generalized additive model (GAM) analysis was used to explore the non-linear relationship between exacerbation risk and type 2 inflammation status. COPD exacerbation risk across type 2 inflammation status was investigated in patients with or without bronchial asthma and in patients with a smoking history in the post-hoc analysis.
Associations between baseline characteristics and COPD exacerbation risk were assessed using negative binomial regression models, with results reported as age- and sex-adjusted estimates with 95% CIs. In addition, variable importance was explored in a gradient boosting machine (GBM) model for COPD exacerbations, considering the non-linear relationship between COPD exacerbations and baseline characteristics. In this analysis, COPD exacerbations were treated as a binary outcome (≥2 exacerbations per year, yes or no). Variable importance was summarized using beeswarm plots of SHapley Additive exPlanations (SHAP) values, and model performance was evaluated using the area under the receiver operating characteristic curve (AUC).
Python (Python Software Foundation, version 3.12.7) and R (R foundation, version 4.4.2 or 4.3.3) were used to conduct statistical analyses.
Results
Baseline Patient and Clinical Characteristics
A total of 138,123 patients with a COPD diagnosis were initially identified. After applying inclusion and exclusion criteria, 10,321 patients were included in the study population (Figure 1). Of these, type 2 inflammation status was classified as low in 1423 patients (13.8%; median eosinophil count 69.6 cells/μL), intermediate in 4895 patients (47.4%; median eosinophil count 189.6 cells/μL), and high in 4003 patients (38.8%; median eosinophil count 485.0 cells/μL; Table 1).
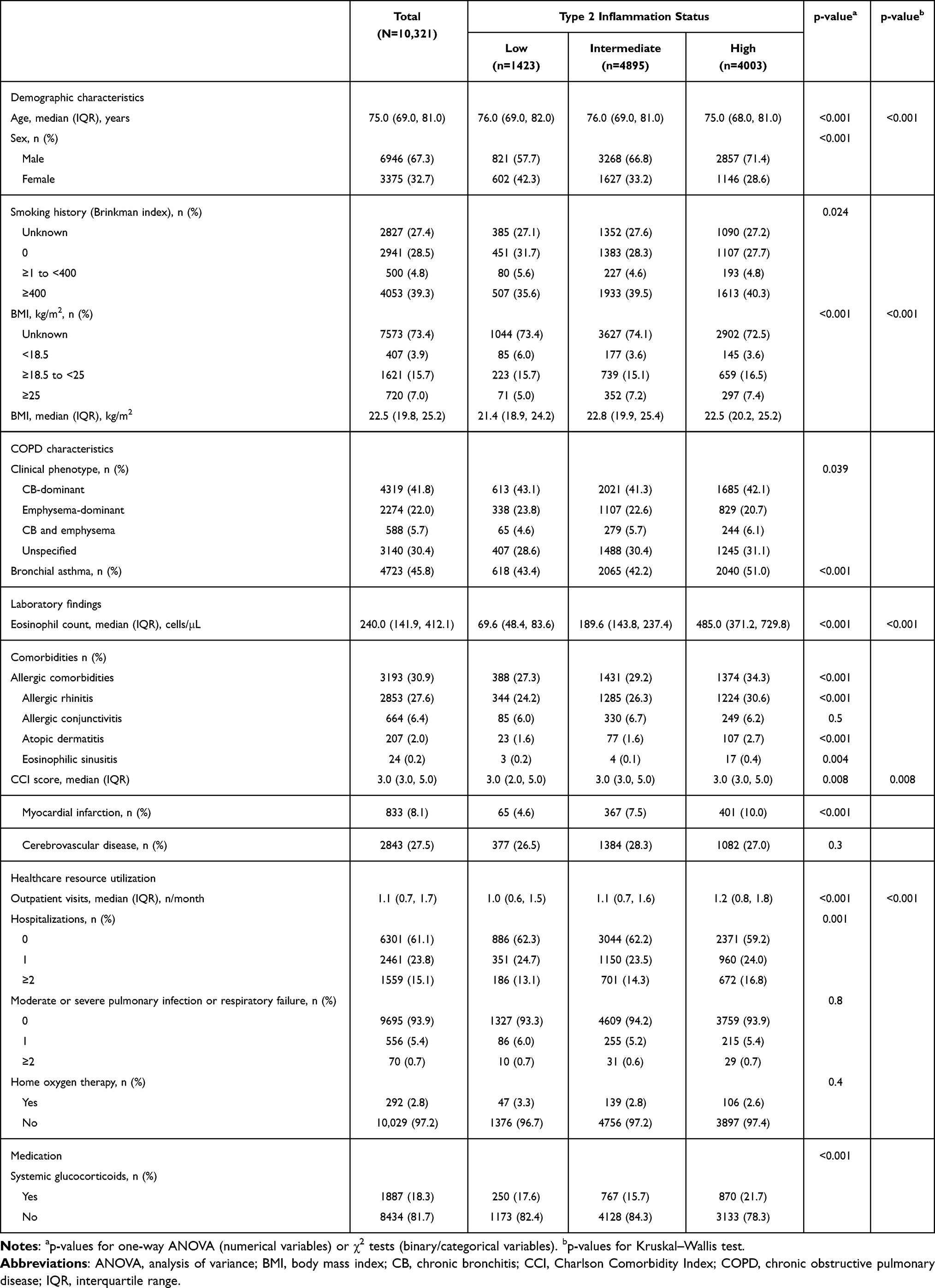 |
Table 1 Baseline Demographic and Clinical Characteristics |
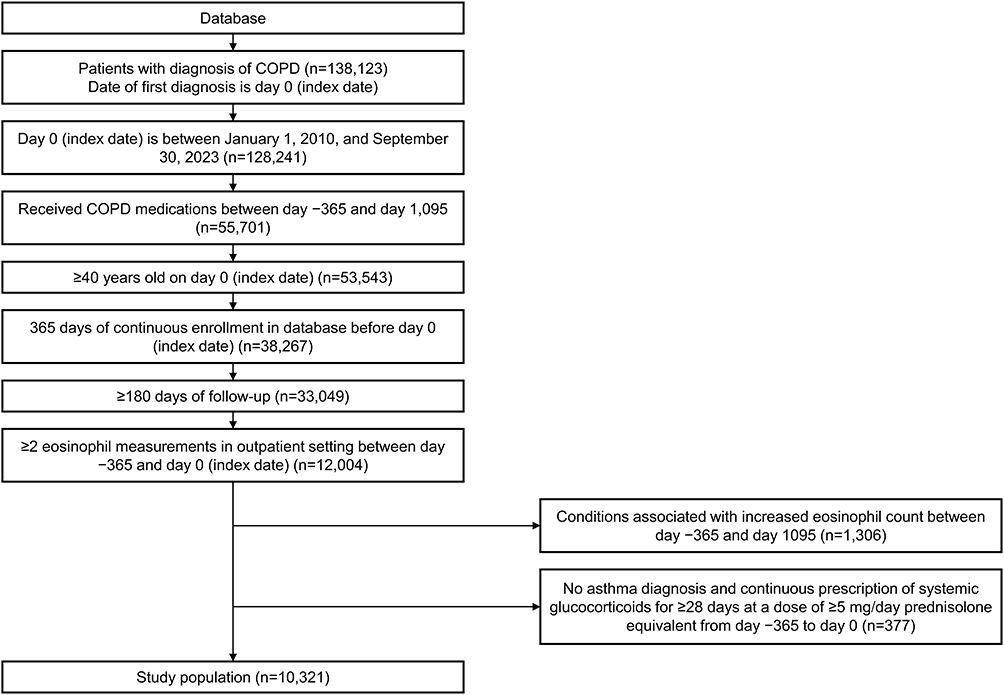 |
Figure 1 Patient flow diagram. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Among the included patients, 67.3% were male and the median (IQR) age was 75.0 (69.0–81.0) years (Table 1). Smoking history varied across the cohort, with 39.3% of patients having a Brinkman Index of ≥400. The proportion of never-smokers was 28.5%, while a substantial proportion (27.4%) had an unknown smoking status.
CB-dominant COPD was the most common clinical phenotype (41.8%), followed by unspecified type (30.4%), and emphysema-dominant (22.0%) COPD, while the combined CB and emphysema phenotype was relatively rare (5.7%). A history of bronchial asthma was present in 45.8% of patients; patients with high levels of type 2 inflammation were more likely to have bronchial asthma (51.0%) than those with low (43.4%) or intermediate (42.2%) levels of type 2 inflammation (p<0.001).
The median (IQR) Charlson Comorbidity Index (CCI) score was 3 (3.0–5.0) in the total study population; the CCI score was also 3 in each type 2 inflammation level status group (Table 1). The proportion of patients with myocardial infarction was 8.1% in the total study population, and was lower in the group with low levels of type 2 inflammation (4.6%) than in the groups with intermediate (7.5%) and high levels (10.0%) of inflammation. The proportion of patients with cerebrovascular disease was 27.5% in the total population, and was similar across type 2 inflammation level groups (26.5–28.3%). A complete summary of CCI items is provided in Supplementary Table 3.
In terms of healthcare utilization in the pre-index year (Day −365 to 0), the median (IQR) number of outpatient visits was 1.1 (0.7–1.7) per month, with 15.1% of patients having experienced ≥2 hospitalizations.
Primary Outcome: Incidence of COPD Exacerbations
There was a consistent trend of increased risk for COPD exacerbations in patients with high levels of type 2 inflammation versus those with intermediate or low levels. The adjusted incidence rate of combined moderate and severe COPD exacerbations was significantly higher in patients with high levels of type 2 inflammation compared with those with intermediate levels (rate ratio: 1.16, 95% CI: 1.08, 1.24; Figure 2 and Supplementary Table 4), while there was no difference in the adjusted incidence rate of combined moderate and severe COPD exacerbations between low and intermediate levels of type 2 inflammation (rate ratio: 0.95, 95% CI: 0.86, 1.05). The incidence of combined moderate and severe, and moderate COPD exacerbations was significantly higher (by 21% and 25%, respectively) in the high type 2 inflammation group versus the low type 2 inflammation group (Supplementary Table 4), while there was no significant difference between patients with high and low type 2 inflammation in the incidence of severe exacerbations (rate ratio: 1.14; 95% CI: 0.94, 1.39).
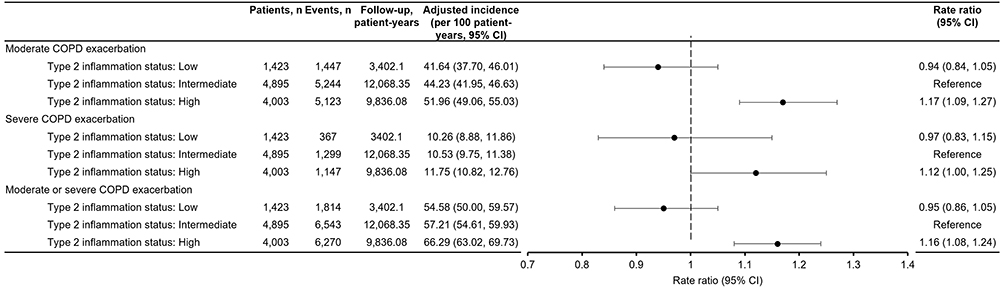 |
Figure 2 Adjusted incidence rates and rate ratios for COPD exacerbations (primary outcome) by type 2 inflammation status. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease. |
To understand the influence of missing data on the COPD exacerbation analysis, predictors of missing data for smoking history (Supplementary Table 5) and BMI (Supplementary Table 6) were evaluated. The proportions of missing data were 27.4% and 73.4% for smoking history and BMI, respectively. Thus, multiple imputations were applied to accommodate these missing data. As anticipated, a higher proportion of patients with missing data on smoking history and BMI was observed among patients who were generally in better physical condition and less likely to be hospitalized. Specifically, missingness was more common in younger patients, those without severe comorbidities, and those with no prior hospitalizations (Supplementary Tables 5 and 6). The exacerbation incidence rates adjusted with covariates were similar to the crude incidence rates without any adjustments (Supplementary Table 4).
Among patients with bronchial asthma, a similar trend was observed, with a higher exacerbation incidence rate in the high type 2 inflammatory group versus the low or intermediate groups (Supplementary Table 4), while among patients without bronchial asthma, the same trend across the type 2 inflammatory groups was observed, but it was not considered significant.
In patients with a smoking history, the incidence rate of exacerbations was increased in the high type 2 inflammatory group versus the intermediate and low groups (Supplementary Table 7). This analysis was conducted to assess the robustness of the findings, as the original dataset included several patients who had never smoked, despite COPD typically requiring a history of smoking.
Sensitivity Analyses
Sensitivity analyses using alternative definitions and thresholds for type 2 inflammation largely supported the findings of the main analysis (Supplementary Figure 1). The results of the first, third, and fourth sensitivity analyses were consistent with the main analysis, showing a higher incidence of COPD exacerbations in patients classified as type 2 inflammation high or positive. In contrast, the second sensitivity analysis revealed a different trend: patients with persistently low or high eosinophil levels had a lower incidence of moderate COPD exacerbations and of combined moderate and severe COPD exacerbations compared with those classified as having intermediate eosinophil levels, but no significant difference was observed for severe COPD exacerbations.
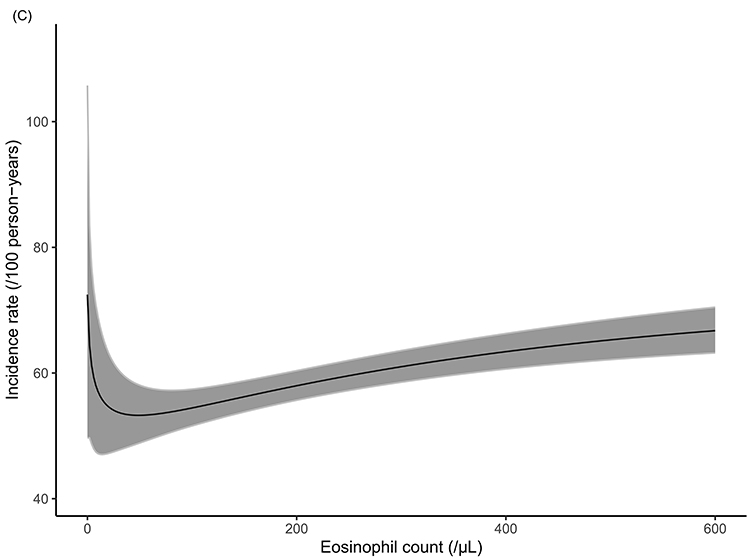
In addition, GAM was employed to model the incidence rate of COPD exacerbations across the range of eosinophil levels (Figure 3). For moderate COPD exacerbations (Figure 3A), the incidence rate exhibited a sharp decline at very low eosinophil counts, followed by a relatively gradual increase. The CI was narrow across most of the eosinophil range, indicating a relatively stable association. For severe COPD exacerbations (Figure 3B), the incidence rate showed a steep rise at the lowest eosinophil levels, followed by a relative plateau. The wider CIs in this figure suggest greater variability compared with the CIs in Figure 3A and C. When considering moderate and severe exacerbations combined (Figure 3C), the overall pattern closely resembled that observed for moderate exacerbations.
Figure 3 Relationship between eosinophil counts and the incidence rate of (A) moderate COPD exacerbations, (B) severe COPD exacerbations, and (C) moderate and severe COPD exacerbations. The grey shaded areas denote 95% confidence intervals. Abbreviation: COPD, chronic obstructive pulmonary disease. Figure 3 continued.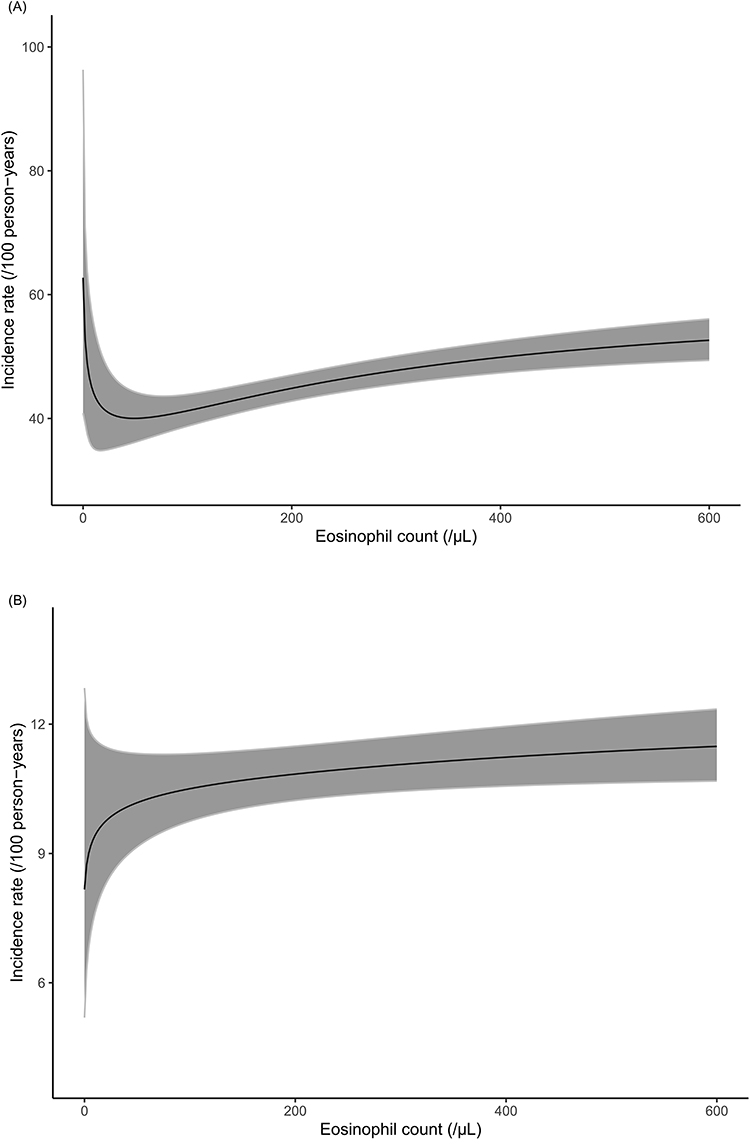
Variable Importance Analysis for Estimation of Risk
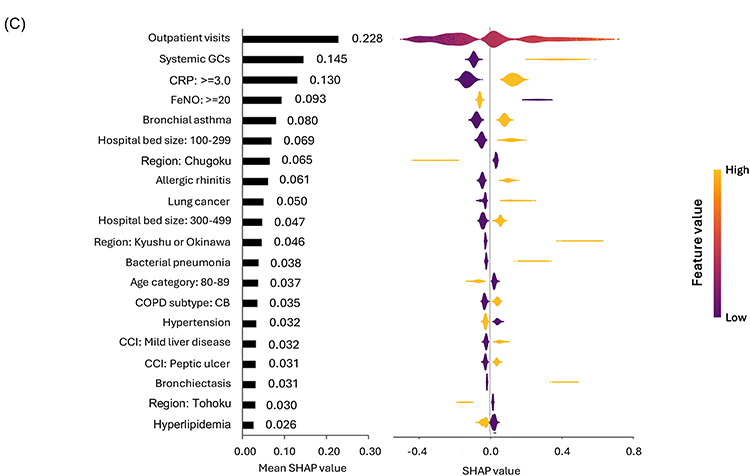
To further evaluate the factors that influenced the risk of COPD exacerbations, an association between patient characteristics and exacerbations was analyzed using a GBM model. The predictive performance of the model, as assessed by the AUC, showed 0.686 for moderate, 0.729 for severe, and 0.677 for moderate or severe exacerbations. Beeswarm plots were used to summarize the most important variables in the model (Figure 4).
Figure 4 Variable importance ranking analysis for (A) moderate, (B) severe, and (C) moderate and severe COPD exacerbation. The beeswarm plots provide an overview of SHAP values for selected features, with rows representing each feature ranked by the mean absolute SHAP value. The individual dots in each row are the SHAP values for that particular feature in each sample of the dataset. For Hb, x = 11.0 g/dL for females and 13.0 g/dL for males. Model performance: AUC = 0.686 (moderate), 0.729 (severe), 0.677 (moderate/severe). Abbreviations: BMI, body mass index; CB, chronic bronchitis; CCI, Charlson Comorbidity Index; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; DM, diabetes mellitus; FeNO, fractional exhaled nitric oxide; GCs, glucocorticoids; Hb, hemoglobin; SHAP, SHapley Additive exPlanations; WBC, white blood cell count. Figure 4 continued.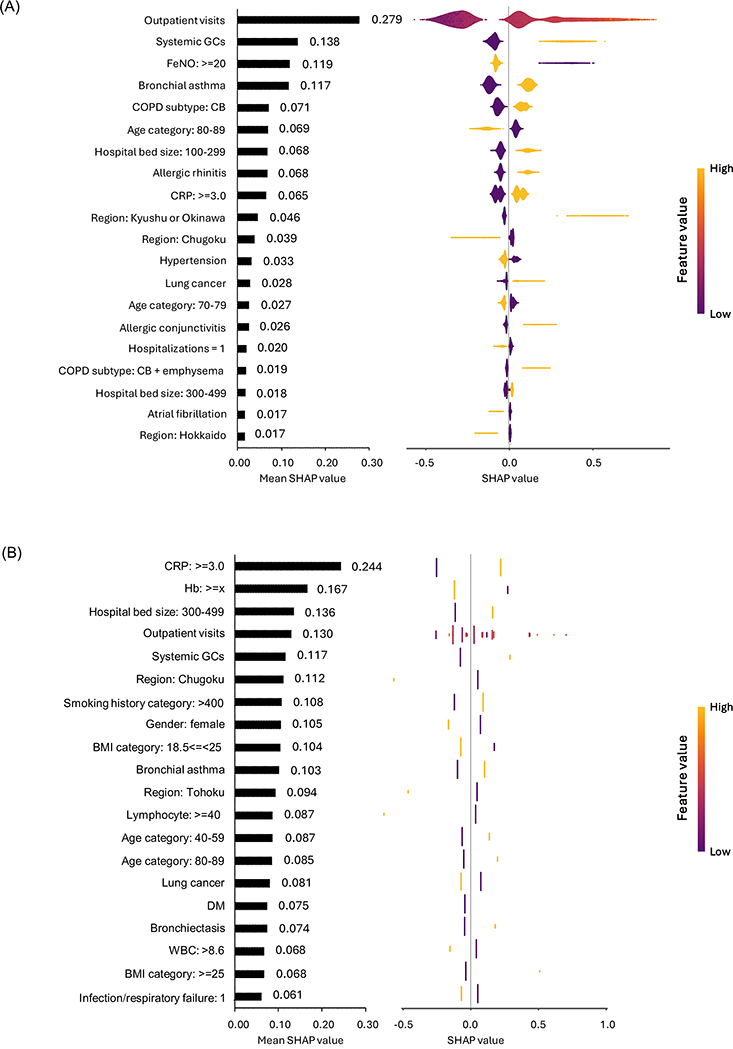
For moderate exacerbations, the highest-ranking variables included outpatient visits (mean absolute SHAP: 0.28), systemic glucocorticoid use (0.14), FeNO ≥20 ppb (0.12), and bronchial asthma (0.12; Figure 4A). COPD subtype (CB), CRP ≥3.0 mg/L, and allergic conditions (rhinitis, conjunctivitis) also contributed to risk estimation.
For severe exacerbations, the model identified CRP ≥3.0 mg/L (0.24), hemoglobin level (0.17), and systemic glucocorticoid use (0.12) as key drivers (Figure 4B). Compared with moderate exacerbations, the impact of outpatient visits was slightly lower (0.13), and regional variation appeared more prominent. Unlike moderate exacerbations, smoking history (Brinkman Index >400) and BMI category (18.5–25 kg/m2) were potential contributors in this setting.
When analyzing combined moderate and severe exacerbations, the most important factors were largely the same as for moderate exacerbations, with outpatient visits (0.23), systemic glucocorticoid use (0.15), and CRP ≥3.0 mg/L (0.13) ranking highest (Figure 4C).
Secondary Outcomes
MACE
No statistically significant differences were observed in MACE incidence between the groups (Figure 5). Compared with patients with intermediate levels of type 2 inflammation, the adjusted incidence rate of MACE was numerically lower in the low type 2 inflammation group (rate ratio: 0.81, 95% CI: 0.60, 1.09) and higher in the high type 2 inflammation group (rate ratio: 1.06, 95% CI: 0.87, 1.29), but neither comparison reached statistical significance. Similarly, when comparing the high and low type 2 inflammation groups, the adjusted rate ratio was 1.30 (95% CI: 0.91, 1.88), indicating no clear association (Supplementary Table 8).
 |
Figure 5 Adjusted incidence rates and rate ratios for MACE (secondary outcome) by type 2 inflammation status. Abbreviations: CI, confidence interval; MACE, major adverse cardiovascular event. |
Sensitivity analyses confirmed the absence of a meaningful relationship between type 2 inflammation and MACE risk (Supplementary Figure 2).
Other Secondary Outcomes
The proportion of patients who had short-term use of oral and intravenous systemic glucocorticoids was greater in patients with high type 2 inflammation (27.7%) compared with patients with low (21.2%) or intermediate (22.3%) type 2 inflammation (Table 2 and Supplementary Table 9). There was a corresponding difference in the incidence rate of oral and intravenous systemic glucocorticoid use; 60.1 versus 42.5 events per 100 patient-years in the high and low type 2 inflammation groups, respectively.
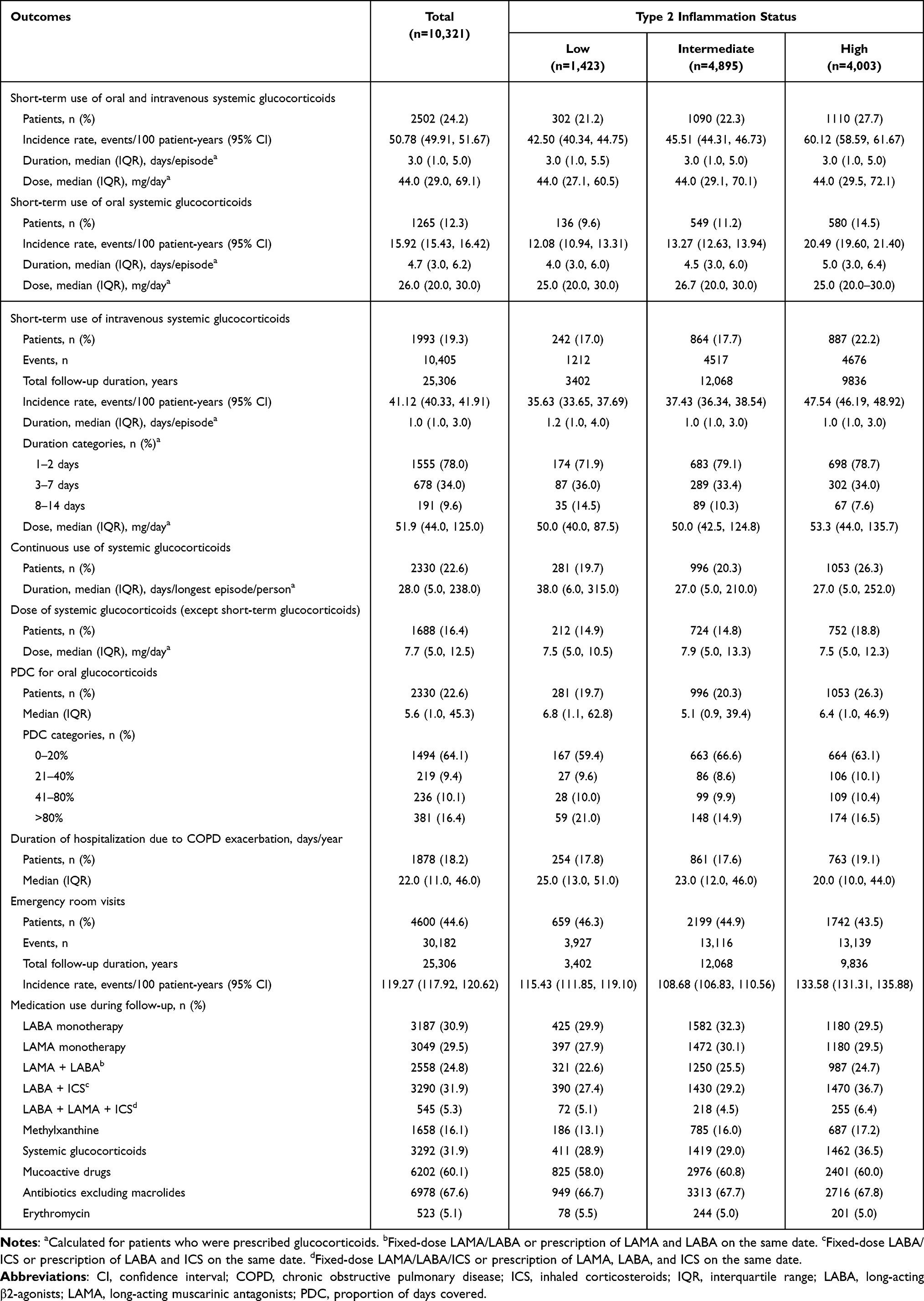 |
Table 2 Other Secondary Outcomes – Medication Use and Health Resource Utilization |
When short-term use of oral and intravenous systemic glucocorticoids were evaluated separately, their use was similar to that described above, with both patient percentages and incidence rates being lowest in the low type 2 inflammation group and greatest in the high type 2 inflammation group across all medication types.
Continuous use of systemic glucocorticoids was reported in 19.7% of patients in the low type 2 inflammation group, 20.3% in the intermediate type 2 inflammation group, and 26.3% in the high type 2 inflammation group. The median duration of the longest episode was highest in the low- type 2 inflammation group (38.0 days) and lowest in the intermediate- and high-type 2 inflammation groups (both 27.0 days). The median PDC for oral glucocorticoids was 6.8%, 5.1%, and 6.4%, respectively; 64.1% of all patients had a PDC value of 0–20%. However, 16.4% of patients had a PDC value >80%, suggesting continuous long-term use.
The incidence of emergency room visits was similar across the type 2 inflammation groups. The incidence rate was lowest in the intermediate type 2 inflammation group (108.68 events per 100 patient-years) and highest in the high type 2 inflammation group (133.58 events per 100 patient-years).
The incidence of hospitalization due to COPD exacerbation was also similar across the type 2 inflammation groups. The median hospitalization duration was longest in the low type 2 inflammation group (25.0 days) and shortest in the high type 2 inflammation group (20.0 days).
Regarding medication use, LABA + ICS use was more frequent in the high type 2 inflammation group (36.7%) compared with the low (27.4%) and intermediate type 2 inflammation groups (29.2%). The use of LABA + LAMA + ICS was also more common in the high type 2 inflammation group (6.4%) than in the other groups (5.1% in low and 4.5% in intermediate). Mucoactive drug use was consistent across groups, ranging from 58.0% to 60.8%.
Discussion
This real-world, retrospective analysis of Japanese patients with COPD demonstrated a significant association between type 2 inflammation and the risk of moderate COPD exacerbations. Patients with high levels of type 2 inflammation, as defined by blood eosinophil counts, exhibited a 21% and 16% higher incidence of moderate or severe exacerbations compared with those with low and intermediate type 2 inflammation, respectively. Although a similar numerical trend was observed for severe exacerbations, the association did not reach statistical significance, likely due to the relatively high variability caused by the low frequency of severe exacerbations. Ad-hoc analyses based on patients with or without asthma or those with a smoking history demonstrated similar findings to our primary analysis and sensitivity analyses; using alternative eosinophil thresholds to define type 2 inflammation largely confirmed the robustness of these findings, except for those related to the persistence of type 2 inflammation. In our cohort, estimates for MACE were numerically higher with increased type 2 inflammation but CIs were wide and crossed the null. The adjusted rate of MACE was also numerically greater in patients with high levels of type 2 inflammation, representing a 30% (and 6%) increase compared with the low (and intermediate) type 2 inflammation groups. This pattern most likely reflects limited statistical power due to the relatively small number of cardiovascular events. Accordingly, these findings should be interpreted cautiously and considered exploratory. At the same time, the epidemiologic literature relating eosinophils to cardiovascular risk remains mixed, and definitive inference requires larger datasets with richer cardiovascular phenotyping and adjudication. Moreover, previous research suggests that type 2 inflammatory pathways may contribute to cardiovascular vulnerability through systemic eosinophilic activation, endothelial dysfunction, and pro‑thrombotic mechanisms,30 although our data cannot confirm this relationship. Furthermore, because this analysis was secondary and exploratory in nature, we did not adjust for baseline cardiovascular comorbidities or prior MACE events, introducing residual confounding. Therefore, the potential relationship between type 2 inflammation and cardiovascular risk should be interpreted with caution and warrants further investigation in well-designed studies to evaluate cardiovascular outcomes.
Furthermore, type 2 inflammation was associated with increased systemic glucocorticoid use. No clear associations with healthcare resource utilization emerged from this analysis. Taken together, these findings highlight the clinical impact of type 2 inflammation on COPD exacerbations and treatment patterns. Given that exacerbations represent a central contributor to the clinical disease burden of COPD, our findings, showing an association between type 2 inflammation and an increased risk of moderate exacerbations, highlight an important aspect of this burden. In addition, while patient characteristics and healthcare resource utilization may differ, the association between type 2 inflammation and exacerbation risk in COPD observed in our study is consistent with findings from Western database studies. Therefore, we believe that our results are generalizable.
The biological mechanisms linking type 2 inflammation with COPD exacerbations may involve several overlapping pathways. Eosinophils can contribute to airway epithelial injury, mucus hypersecretion, and increased susceptibility to viral infections through type 2 cytokines such as IL-4, IL-5, and IL-13. These mechanisms may amplify airway inflammatory tone and predispose patients to exacerbations, which are more sensitive to fluctuations in airway inflammation. In addition, variability in eosinophil levels may reflect instability in inflammatory networks, potentially increasing vulnerability to environmental and infectious triggers.
Clinically, the finding that moderate exacerbations primarily drive this association is notable, as moderate events constitute the majority of COPD-related healthcare utilization in Japan and contribute significantly to long-term symptom burden and functional decline. These results support the role of blood eosinophils as an accessible biomarker for identifying patients at increased risk of moderate exacerbations and for informing more personalized treatment strategies, including optimization of inhaled corticosteroid use. The findings of this real-world study align with a growing body of evidence indicating that type 2 inflammation is a relevant factor in COPD, particularly in relation to exacerbation risk. A meta-analysis of 21 studies, comprising over 79,000 patients with COPD, confirmed that higher blood eosinophil levels were associated with an increased risk of moderate and severe exacerbations, though the strength of this association depended on the eosinophil threshold used.31 Specifically, eosinophil counts ≥300 cells/µL were associated with a 21% increased incidence of moderate or severe exacerbations, while lower thresholds did not consistently predict exacerbation frequency. Eosinophil counts of ≥300 cells/µL are usually adopted as a threshold in studies of patients with moderate-to-severe COPD, such as in the ECLIPSE study, where a higher risk of exacerbations was observed above this threshold.32 The present study reproduced the usefulness of a threshold of 300 cells/µL as a potential predictor of COPD exacerbation. A retrospective analysis of 481 patients with COPD in Japan found that blood eosinophil percentage during a stable period was the strongest independent predictor of frequent exacerbations (defined as >2 exacerbations per year) in patients who had COPD exacerbations.33 However, the association between exacerbations and eosinophils remains controversial, with some studies suggesting a limited or non-existent association.12,34,35 Another study in a Japanese hospital-based cohort of 135 patients did not identify a significant relationship between baseline blood eosinophils and exacerbation risk, suggesting that the predictive value of eosinophils may depend on the threshold of the eosinophil count, the definition of a COPD exacerbation, patient characteristics such as disease severity, and treatment exposure.35 Outside of Japan, multiple real-world studies have examined the relationship between eosinophilic inflammation and COPD exacerbations. A population-based study in Spain stratified patients with COPD by blood eosinophil count and found that, while very low and very high eosinophil levels were associated with slightly increased exacerbation rates, ie, a U-shape distribution of COPD exacerbations across eosinophil counts, no single eosinophil threshold reliably predicted exacerbation risk.34 Similarly, an analysis of the Copenhagen General Population Study found a higher rate of moderate exacerbations in patients with the lowest and highest eosinophil levels.36 The findings from the Spanish and Copenhagen studies were aligned with the U-shape distribution on moderate COPD exacerbations we observed with our GAM model. In addition, several studies that were not included in the aforementioned meta-analysis31 provided negative findings: Hastie et al analyzed the SPIROMICS cohort and found no evidence linking high blood eosinophil counts (≥200 cells/μL) with COPD exacerbations, concluding that blood eosinophils alone are not a reliable biomarker for exacerbations;37 Zysman et al, in a French cohort, observed no difference in exacerbation rates between eosinophilic and non-eosinophilic groups, regardless of the cutoff values used (2%, 3%, or 4%);38 and Negewo et al reported no significant difference in blood eosinophil counts between frequent and non-frequent exacerbators.39
Although Asian patients with COPD exhibit several distinctive clinical features compared with Western populations - such as lower BMI, a higher prevalence of bronchiectasis, and different environmental exposures as highlighted in the Asian Pacific Society of Respirology position statement40 - current evidence indicates that the relationship between blood eosinophil counts and exacerbation risk is largely consistent across regions. Multiple cohort studies from China, South Korea, Taiwan, and Thailand have demonstrated that elevated eosinophil counts (≥300 cells/μL) predict future moderate-to-severe exacerbations to a similar extent as in Western cohorts.41–48 Two Asian studies have also examined the variability or persistence of eosinophilia, although their definitions of “persistent high eosinophils” differ substantially from ours (eg, inpatient measurements or only two time points several years apart).46,47 These studies generally report that patients with persistently high eosinophil levels exhibit increased exacerbation risk. On the other hand, recent work using non-linear modeling approaches in Korean populations has suggested a non-linear, U‑shaped association between eosinophils and exacerbation risk,41 resembling the pattern observed in our analysis. Taken together, the available Asian evidence supports that the eosinophil–exacerbation association is broadly consistent with Western findings, and that non-linear risk patterns may emerge when eosinophils are modeled flexibly, aligning with the results of our study.
These findings suggest that viewing eosinophil count as a prognostic marker for COPD exacerbation risk is complex. The observed U-shaped relationship of exacerbation risk suggests that there is a pattern beyond a simple linear relationship, and that different mechanisms are associated with increased exacerbation risk in patients with different phenotypes. For example, lower eosinophil count may indicate a neutrophilic or less pronounced type 2 inflammatory phenotype. In addition, as highlighted by Miravitlles et al, there has been some discussion around the variability of eosinophil levels and COPD exacerbations, suggesting that fluctuating levels may be associated with a higher frequency of exacerbations than a persistently high or low level of eosinophils.34 This discussion on the relationship between eosinophil stability and COPD exacerbations may offer a plausible explanation for the different results observed in the second sensitivity analysis, which considered the persistence of eosinophil levels, compared with the other sensitivity analyses. On the other hand, a high eosinophil count (≥300 cells/μL) is not only recognized as a biomarker for increased exacerbation risk, but also as a predictor of favorable response to ICS, as recommended in the Global Initiative for GOLD guidelines.1 Therefore, the lower exacerbation risk observed in patients with persistently high eosinophil levels in our study may reflect effective disease control achieved through ICS therapy, rather than an absence of underlying risk. This pattern may also reflect the combined influence of phenotype stability and treatment patterns. Although ICS or occasional OCS use could partially mediate this association, these patients had a median eosinophil level of approximately 485 cells/μL and secondary causes of eosinophilia were systematically excluded, making prolonged corticosteroid use an unlikely sole explanation. Because treatment escalation is often triggered by prior exacerbations and evolving disease severity, some degree of reverse causation or partial mediation may contribute to the observed pattern and should be considered when interpreting these findings. Of note, patients in the high type 2 inflammatory group had a greater use of systemic glucocorticoids, which brings an additional clinical burden to patients related to the adverse events of steroids. Further research into this complex topic is warranted as such understanding is essential for developing more precise phenotyping strategies and personalized treatment approaches, such as the use of targeted biologics (for example, dupilumab).
Clinically, the finding that moderate exacerbations primarily drive this association is notable, as moderate events constitute the majority of COPD-related healthcare utilization in Japan and contribute significantly to long-term symptom burden and functional decline. These results support the role of blood eosinophils as an accessible biomarker for identifying patients at increased risk of moderate exacerbations and for informing more personalized treatment strategies, including optimization of inhaled corticosteroid use.
It is also important to highlight that approximately half of the COPD patients in this analysis had comorbid bronchial asthma; however, the increased risk of COPD exacerbation was observed regardless of the presence or absence of bronchial asthma. While this study did not specifically aim to analyze asthma-COPD overlap (ACO), this topic warrants further investigation due to the clinical relevance of ACO.4
This study has several limitations that should be considered when interpreting the findings. First, as a retrospective analysis using real-world EMR data, the study is subject to potential data misclassification and incomplete data capture, particularly regarding COPD diagnoses, exacerbation events, and medication adherence. Thus, this limitation could cause potential biases due to unobserved covariates. Despite the use of validated algorithms, some degree of misclassification of cardiovascular events may remain due to the inherent limitations of claims‑based coding. Exacerbations were identified using diagnostic codes and treatment algorithms within the EMR database, which may be susceptible to misclassification, particularly for under-ascertainment of moderate exacerbations managed outside the contributing institution or treated without systemic corticosteroids or antibiotics in outpatient settings. Variability in coding practices, treatment decisions, and documentation could influence the accuracy of exacerbation classification. Although validated definitions were applied,49,50 some misclassification is unavoidable in EMR-based studies.
Second, since eosinophil levels fluctuate over time and blood eosinophil counts were used to classify type 2 inflammation, a single measurement of eosinophils may not fully capture the dynamic nature of inflammation and may lead to type 2 inflammation misclassification. Because the database did not provide consistent information on measurement timing relative to exacerbations, we were unable to evaluate dynamic changes in eosinophil levels. Furthermore, although we used only outpatient measurements to minimize the influence of hospitalization‑related eosinophil variability, this approach may not fully capture short‑term fluctuations that occur during periods of disease instability. In particular, some evidence suggests that not only absolute eosinophil level, but also temporal variability may contribute to exacerbation; however, such instability could not be assessed in our analysis due to infrequent and non-standardized testing intervals. The primary definition of type 2 inflammation relied on the highest outpatient eosinophil count during the baseline period, which may be susceptible to transient elevations and may not fully capture persistent inflammatory status. To address this conceptual limitation, we conducted multiple sensitivity analyses using alternative definitions, including repeated high measurements, mean eosinophil levels, and a probabilistic approach based on the distribution of serial eosinophil counts. These analyses yielded general consistent patterns; however, some degree of type 2 inflammation exposure misclassification remains unavoidable.
Third, the lack of data on standardized spirometry, and imaging scans in the database precluded assessment of lung function decline, which is an important marker of disease progression. Spirometry results, including forced expiratory volume in 1 second (FEV1) and FEV1/forced vital capacity (FVC) ratio, were not available in this EMR dataset. Accordingly, airflow limitation severity could not be assessed, which represents a key limitation of this study. The lack of spirometry results may introduce residual confounding. Computed tomography–based left atrial appendage measurements were also unavailable, preventing assessment of emphysema severity or structural lung changes. As a result, we could not use imaging to differentiate COPD from conditions such as asthma or bronchiectasis, which may introduce some degree of diagnostic misclassification inherent to EMR‑based studies. The status of these markers could be a potential confounding factor. A further limitation is that FeNO and type 2–related cytokines (eg, IL-4, IL-5, IL-13) were not routinely captured in the EMR database and therefore could not be evaluated. As FeNO is not a standard component of Japanese EMR systems and is not reimbursed for COPD under the national insurance scheme, its measurement is inconsistent across institutions. As a result, the assessment of type 2 inflammation may be less comprehensive.
Fourth, the eligible patients for this study were required to have at least 6 months of follow-up and at least 1 year of data before the index date, and were considered relatively stable This means that patients with severe COPD, who may have died early or been transferred to other institutions due to their disease severity, may have been excluded from the study population. These criteria may have introduced selection bias, leading to an underestimation of exacerbation rates.
Fifth, medication exposure was categorized descriptively using mutually exclusive regimen groups, but treatment variables were not included in the primary regression models. Because real‑world prescribing decisions, particularly for inhaled corticosteroids, are influenced by both prior exacerbations and type 2 inflammatory status, medication use functions as a partially time‑varying confounder and mediator. Proper adjustment would require specialized causal modeling (eg, time-updated models), which was beyond the scope of this study. Therefore, residual confounding by treatment cannot be excluded.
Sixth, we did not explicitly model seasonal variation in exacerbations, although the cohort’s mean follow‑up exceeded two years (2.45 years, 25306 person-years on 10321 patients), the study population collectively experienced multiple seasonal cycles.
Seventh, BMI data were missing for 73.4% of the study population. Although multiple imputation was applied, the extremely high degree of missingness may limit the reliability of imputed values and the stability of adjusted estimates - particularly for MACE, for which BMI is an important confounder. Importantly, in Japanese and other East‑Asian populations, BMI distributions are generally lower than in Western cohorts, yet both low and high BMI have been associated with increased cardiovascular mortality, and long‑term underweight or BMI decline has been linked to higher mortality in Japanese cohorts. Consequently, residual confounding and reduced precision cannot be excluded, and results involving cardiovascular outcomes should be interpreted with caution. In addition, missing data for smoking history and BMI were handled using multiple imputation under the assumption of MAR, informed by observed associations with age, comorbidity burden, and hospitalization history. Although diagnostic checks suggested that missingness was largely explained by observable factors and that imputed and crude results were similar, the MAR assumption cannot be fully verified. Therefore, some residual confounding due to missing or unmeasured variables cannot be excluded.
Eighth, this study required patients to have at least two eosinophil measurements during the baseline period, which may preferentially include more stable patients who attend regular outpatient visits. Consequently, individuals with more severe, unstable, or less frequently monitored COPD may be underrepresented. This selection mechanism may introduce bias and limit the generalizability of the findings to the broader COPD population.
Ninth, the analysis of MACE was limited by a relatively small number of events, resulting in wide CIs and insufficient statistical power to detect associations of modest magnitude. As a secondary and exploratory analysis, these findings should be interpreted with caution and considered hypothesis-generating.
Tenth, the study period (2020–2022) overlapped with the COVID‑19 pandemic, during which changes in healthcare utilization, reduced respiratory viral transmission, and altered patient behavior may have influenced the recorded frequency of COPD exacerbations, outpatient visits, and medication use. As the database did not capture pandemic‑specific contextual factors, these effects could not be fully accounted for and may have influenced the observed incidence patterns.
Finally, as this study was conducted in a Japanese population, the generalizability of the findings to other ethnic and geographic populations remains uncertain. While this is an acknowledged limitation, it should be noted that a significant evidence gap exists in the availability of large-scale, Japan‑specific real-world data on COPD, with most evidence derived from Western populations. Thus, this study provides important and novel findings with regards to (i) population differences (Japan has a distinct COPD phenotype distribution, smoking patterns, environmental exposures, and healthcare access, which influence disease burden and treatment patterns); (ii) healthcare system characteristics (Japan’s universal insurance system and high diagnostic imaging utilization create a unique real-world context not captured in Western datasets); and (iii) clinical relevance for local practice (the findings allow clinicians and policymakers to better understand risk profiles and clinical burden specifically within the Japanese population, addressing a gap in evidence that has previously required extrapolation from Western cohorts). By placing internationally observed associations within a Japanese real-world setting, the study provides important contextual validity and supports more regionally appropriate COPD management strategies.
Conclusions
This database analysis provides real-world evidence that type 2 inflammation assessed by blood eosinophil levels is primarily associated with an increased risk of moderate exacerbations in Japanese patients with COPD. A similar trend was observed for severe exacerbations, but no statistically significant difference was confirmed. Furthermore, despite not being statistically significant, there was a numerically higher risk of MACE in patients with higher levels of type 2 inflammation. These findings support the growing recognition of type 2 inflammation as a clinically relevant endotype in COPD, particularly in the context of exacerbation risk. Further research is warranted to refine the classification of COPD with type 2 inflammation, to better understand its implications for disease progression and treatment response, and to explore whether targeting type 2 inflammatory pathways has potential clinical relevance in this population. In addition, the present findings suggest that routine assessment of blood eosinophil levels may help support risk stratification and inform treatment decisions considering its variable nature. Continued investigation is also needed to determine how this endotype guides personalized management and to evaluate its role in long-term clinical outcomes. Although statistical significance was limited for some outcomes, the consistent directional trends observed in this study highlight signals that warrant confirmation in larger, prospective studies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the MINS Ethics Review Committee (approval No. MINS‑REC‑204224). This study used retrospectively collected, fully anonymized EMR data. Under Japanese ethical guidelines and institutional policy, research using non‑identifiable secondary data is exempt from the requirement to obtain individual informed consent. Accordingly, the ethics committee confirmed that an informed‑consent waiver was applicable. The study was conducted in accordance with the Declaration of Helsinki and relevant national regulations.
Consent for Publication
Not applicable, as this study did not include any individual person’s identifiable data.
Acknowledgments
We would like to thank Georgii Filatov who assisted in the preparation of the outline of the manuscript on behalf of Springer Health+ and Nireshnee Ramchundar, PhD, of Springer Health+ who assisted in the preparation of the first draft. This medical writing assistance was funded by Sanofi.
Previous publication: This paper was presented at the European Respiratory Society (ERS) 2025 Congress, in session “Novel biomarkers and advances in patient stratification to predict airways disease progression and responsiveness to treatments”, and published in the European Respiratory Journal. Reference: Muro S, Orimo M, Sunaga Y et al. Real-world evidence among COPD patients in Japan: a retrospective analysis to investigate the disease burden of COPD patients with type2 inflammation with electronic medical record (EUROS study). Eur Respir J. 2025;66(Suppl 69):PA1504. https://doi.org/10.1183/13993003.congress-2025.PA1504.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Sanofi. The sponsor contributed to the study design and coordination with the data provider, and supported medical writing. Data analyses were conducted by the JMDC’s analysts according to a prespecified statistical analysis plan under both the supervision of the academic author and sponsor-employed authors. The academic author retained full access to the results and had final responsibility for data interpretation and the decision to submit the manuscript. The sponsor did not have unilateral authority over data analysis or conclusions. This observational study did not specifically evaluate any Sanofi product, nor did it perform comparative effectiveness analyses among branded medications. Medication exposures, where described, were classified into non‑proprietary regimen categories for descriptive or sensitivity purposes only.
Disclosure
Shigeo Muro has received lecture and advisory fees from Sanofi, Novartis Pharma, GlaxoSmithKline, and AstraZeneca; lecture fees from Boehringer Ingelheim; and a research grant from ROHTO Pharmaceutical Co., Ltd. Mami Orimo, Yoshinori Sunaga, and Masato Ishida are employees of Sanofi K.K. and may hold stock/stock options in the company. Shoichiro Inokuchi and Makoto Tokuda are employees of JMDC Inc. Shoichiro Inokuchi also reports personal fees from Information-technology Promotion Agency, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2025 report. 2025. Available from: https://goldcopd.org/2025-gold-report/.
2. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–21. doi:10.1016/S2213-2600(20)30105-3
3. GBD Forecasting Collaborators. Burden of disease scenarios for 204 countries and territories, 2022-2050: a forecasting analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2204–2256. doi:10.1016/S0140-6736(24)00685-8
4. Shibata Y, Kawayama T, Muro S, et al. Management goals and stable phase management of patients with chronic obstructive pulmonary disease in the Japanese Respiratory Society guideline for the management of chronic obstructive pulmonary disease 2022 (6th edition). Respir Investig. 2023;61(6):773–780. doi:10.1016/j.resinv.2023.08.007
5. Kawayama T, Takahashi K, Ikeda T, et al. Exacerbation rates in Japanese patients with obstructive lung disease: a subanalysis of the prospective, observational NOVELTY study. Allergol Int. 2024;73(1):71–80. doi:10.1016/j.alit.2023.08.003
6. Ishii T, Nishimura M, Akimoto A, et al. Understanding low COPD exacerbation rates in Japan: a review and comparison with other countries. Int J Chron Obstruct Pulmon Dis. 2018;13:3459–3471. doi:10.2147/COPD.S165187
7. Corlateanu A, Mendez Y, Wang Y, et al. “Chronic obstructive pulmonary disease and phenotypes: a state-of-the-art”. Pulmonology. 2020;26(2):95–100. doi:10.1016/j.pulmoe.2019.10.006
8. Barnes PJ. Inflammatory endotypes in COPD. Allergy. 2019;74(7):1249–1256. doi:10.1111/all.13760
9. Garudadri S, Woodruff PG. Targeting chronic obstructive pulmonary disease phenotypes, endotypes, and biomarkers. Ann Am Thorac Soc. 2018;15(Suppl 4):S234–s238. doi:10.1513/AnnalsATS.201808-533MG
10. Phillips KM, Lavere PF, Hanania NA, et al. The emerging biomarkers in chronic obstructive pulmonary disease: a narrative review. Diagnostics. 2025;15(10):1245. doi:10.3390/diagnostics15101245
11. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2026 report. 2026. Available from: https://goldcopd.org/2026-gold-report-and-pocket-guide/.
12. Casanova C, Celli BR, de-Torres JP, et al. Prevalence of persistent blood eosinophilia: relation to outcomes in patients with COPD. Eur Respir J. 2017;50(5):1701162. doi:10.1183/13993003.01162-2017
13. Martínez-Gestoso S, García-Sanz MT, Calvo-álvarez U, et al. Variability of blood eosinophil count and prognosis of COPD exacerbations. Ann Med. 2021;53(1):1152–1158. doi:10.1080/07853890.2021.1949489
14. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
15. Singh D, Kolsum U, Brightling CE, et al. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44(6):1697–1700. doi:10.1183/09031936.00162414
16. Leigh R, Pizzichini MM, Morris MM, et al. Stable COPD: predicting benefit from high-dose inhaled corticosteroid treatment. Eur Respir J. 2006;27(5):964–971. doi:10.1183/09031936.06.00072105
17. Okumura Y, Fujiwara T, Tokumasu H, et al. A new electronic medical record database linked to claims data and discharge abstract data (the RWD database) in Japan: study design and profile. Ann Clin Epidemiol. 2024;6(3):58–64. doi:10.37737/ace.24009
18. Fujiwara T, Kanemitsu T, Tajima K, et al. Accuracy of algorithms to identify patients with a diagnosis of major cancers and cancer-related adverse events in an administrative database: a validation study in an acute care hospital in Japan. BMJ Open. 2022;12(7):e055459. doi:10.1136/bmjopen-2021-055459
19. Ono Y, Taneda Y, Takeshima T, et al. Validity of claims diagnosis codes for cardiovascular diseases in diabetes patients in Japanese administrative database. Clin Epidemiol. 2020;12:367–375. doi:10.2147/CLEP.S245555
20. Wakabayashi Y, Eitoku M, Suganuma N. Characterization and selection of Japanese electronic health record databases used as data sources for non-interventional observational studies. BMC Med Inform Decis Mak. 2021;21(1):167. doi:10.1186/s12911-021-01526-6
21. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for prevention, diagnosis and management of COPD: 2024 report. 2024. Available from: https://goldcopd.org/2024-gold-report/.
22. Holguin F, Cardet JC, Chung KF, et al. Management of severe asthma: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2020;55(1):1900588. doi:10.1183/13993003.00588-2019
23. Vanetti M, Visca D, Ardesi F, et al. Eosinophils in chronic obstructive pulmonary disease. Ther Adv Respir Dis. 2025;19:17534666251335800. doi:10.1177/17534666251335800
24. Barnes N, Ishii T, Hizawa N, et al. The distribution of blood eosinophil levels in a Japanese COPD clinical trial database and in the rest of the world. Int J Chron Obstruct Pulmon Dis. 2018;13:433–440. doi:10.2147/COPD.S144108
25. Bosco E, Hsueh L, McConeghy KW, et al. Major adverse cardiovascular event definitions used in observational analysis of administrative databases: a systematic review. BMC Med Res Methodol. 2021;21(1):241. doi:10.1186/s12874-021-01440-5
26. Nakai M, Iwanaga Y, Sumita Y, et al. Validation of acute myocardial infarction and heart failure diagnoses in hospitalized patients with the nationwide claim-based JROAD-DPC database. Circ Rep. 2021;3(3):131–136. doi:10.1253/circrep.CR-21-0004
27. Yamana H, Moriwaki M, Horiguchi H, et al. Validity of diagnoses, procedures, and laboratory data in Japanese administrative data. J Epidemiol. 2017;27(10):476–482. doi:10.1016/j.je.2016.09.009
28. Fujihara K, Yamada-Harada M, Matsubayashi Y, et al. Accuracy of Japanese claims data in identifying diabetes-related complications. Pharmacoepidemiol Drug Saf. 2021;30(5):594–601. doi:10.1002/pds.5213
29. Lee KJ, Tilling KM, Cornish RP, et al. Framework for the treatment and reporting of missing data in observational studies: the treatment and reporting of missing data in observational studies framework. J Clin Epidemiol. 2021;134:79–88. doi:10.1016/j.jclinepi.2021.01.008
30. Feng X, Liu Y, Qin H, et al. The relationship between blood eosinophil count and cardiovascular outcomes in prediabetes and diabetes patients with acute coronary syndrome: insights from a large Asian cohort analysis. Endocrine. 2025;90(3):1297–1310. doi:10.1007/s12020-025-04462-x
31. Chen F, Yang M, Wang H, et al. High blood eosinophils predict the risk of COPD exacerbation: a systematic review and meta-analysis. PLoS One. 2024;19(10):e0302318. doi:10.1371/journal.pone.0302318
32. Yun JH, Lamb A, Chase R, et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141(6):2037–2047.e2010. doi:10.1016/j.jaci.2018.04.010
33. Tashiro H, Kurihara Y, Takahashi K, et al. Clinical features of Japanese patients with exacerbations of chronic obstructive pulmonary disease. BMC Pulm Med. 2020;20(1):318. doi:10.1186/s12890-020-01362-w
34. Miravitlles M, Monteagudo M, Solntseva I, et al. Blood eosinophil counts and their variability and risk of exacerbations in COPD: a population-based study. Arch Bronconeumol. 2021;57(1):13–20. doi:10.1016/j.arbres.2019.12.015
35. Nishimura K, Kusunose M, Sanda R, et al. Is blood eosinophil count a biomarker for chronic obstructive pulmonary disease in a real-world clinical setting? Predictive property and longitudinal stability in Japanese patients. Diagnostics. 2021;11(3):404. doi:10.3390/diagnostics11030404
36. Vedel-Krogh S, Nielsen SF, Lange P, et al. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen general population study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
37. Hastie AT, Martinez FJ, Curtis JL, et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(12):956–967. doi:10.1016/S2213-2600(17)30432-0
38. Zysman M, Deslee G, Caillaud D, et al. Relationship between blood eosinophils, clinical characteristics, and mortality in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1819–1824. doi:10.2147/COPD.S129787
39. Negewo NA, McDonald VM, Baines KJ, et al. Peripheral blood eosinophils: a surrogate marker for airway eosinophilia in stable COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:1495–1504. doi:10.2147/COPD.S100338
40. Rhee CK, Chau NQ, Yunus F, et al. Management of COPD in Asia: a position statement of the Asian Pacific Society of Respirology. Respirology. 2019;24(10):1018–1025. doi:10.1111/resp.13633
41. Kim SH, Rhee CK, Lee WY, et al. Blood eosinophil counts and exacerbation risk in stable COPD with ≤1 moderate exacerbation on dual bronchodilator therapy. Heart Lung. 2026;76:60–65. doi:10.1016/j.hrtlng.2025.11.010
42. Wu X, Deng Z, Wu F, et al. Clinical characteristics and 2-year outcomes of chronic obstructive pulmonary disease patients with high blood eosinophil counts: a population-based prospective cohort study in China. Arch Bronconeumol. 2024;60(7):402–409. doi:10.1016/j.arbres.2024.03.029
43. Hsu W-H, Shiau B-W, Lai -C-C, et al. Association between eosinophil count and prognosis in chronic obstructive pulmonary disease patients. Front Med. 2025;12:1525709. doi:10.3389/fmed.2025.1525709
44. Jo YS, Moon JY, Park YB, et al. Longitudinal changes in forced expiratory volume in 1 s in patients with eosinophilic chronic obstructive pulmonary disease. BMC Pulm Med. 2022;22(1):91. doi:10.1186/s12890-022-01873-8
45. Song JH, Lee CH, Kim JW, et al. Clinical implications of blood eosinophil count in patients with non-asthma-COPD overlap syndrome COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:2455–2464. doi:10.2147/COPD.S129321
46. Peng J, Wu X, Wen X, et al. Persistent and unstable eosinophil levels in the sputum and blood: impact on the clinical prognosis of patients with chronic obstructive pulmonary disease. J Thorac Dis. 2025;17(12):11307–11320. doi:10.21037/jtd-2025-1885
47. Guan L, Li J, Liang L, et al. Blood eosinophil stability predicts clinical outcomes in hospitalized patients with acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2025;20:2913–2923. doi:10.2147/COPD.S536911
48. Kaenmuang P, Navasakulpong A, Geater SL, et al. Blood eosinophil count stability and clinical outcomes in patients with chronic obstructive pulmonary disease in a high endemic area of parasitic infection: a prospective study. Chronic Obstr Pulm Dis. 2024;11(4):350–358. doi:10.15326/jcopdf.2023.0492
49. Mapel DW, Roberts MH, Sama S, et al. Development and validation of a healthcare utilization-based algorithm to identify acute exacerbations of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:1687–1698. doi:10.2147/COPD.S302241
50. Yamada H, Matsumoto I, Makita N, et al. Effect of timing of bronchodilator therapy initiation on exacerbations in patients with chronic obstructive pulmonary disease: a retrospective cohort study. Respir Res. 2022;23(1):255. doi:10.1186/s12931-022-02184-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.