Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Diagnosis Application of Metagenomic Next-Generation Sequencing of Plasma in Suspected Sepsis
Authors Wang L, Li S, Qin J, Tang T, Hong J, Tung TH, Xu C, Yu S, Qian J
Received 1 November 2022
Accepted for publication 2 February 2023
Published 14 February 2023 Volume 2023:16 Pages 891—901
DOI https://doi.org/10.2147/IDR.S395700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Lisha Wang,1 Shixiao Li,1 Jiajia Qin,1 Tianbin Tang,1 Jiawen Hong,1 Tao-Hsin Tung,2 Chunyan Xu,1 Sufei Yu,1 Jiao Qian1
1Department of Laboratory Medicine, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, Linhai, People’s Republic of China; 2Evidence-Based Medicine Center, Taizhou Hospital of Zhejiang Province, Wenzhou Medical University, Linhai, People’s Republic of China
Correspondence: Sufei Yu; Jiao Qian, Email [email protected]; [email protected]
Purpose: We analyzed the clinical concordance of mNGS test results from blood samples and improved the clinical efficiency of mNGS in the diagnosis of suspected sepsis pathogens.
Patients and Methods: In this study, 99 samples of suspected blood flow infection were included for plasma mNGS, and the correlation between mNGS results and blood culture results, serum inflammatory indices, clinical symptoms and antibiotic treatment was analyzed, as well as the comparison with the detection rate of BALF pathogens, as well as the classification of different pathogens in the mNGS results were analyzed.
Results: The mNGS pathogen detection rate was higher than that of traditional blood culture (83.02% vs 35.82%). The rate of the mNGS results being consistent with the clinical diagnosis was also higher than that of traditional blood culture (58.49% vs 20.75%). This study shows that bacteria and fungi are the main pathogens in sepsis, and viral sepsis is very rare. In this study, 32% of sepsis patients were secondary to pneumonia. Compared with the pathogen detection rate using alveolar lavage fluid, the detection rate from plasma mNGS was 62.5%. Samples were also easy to sample, noninvasive, and more convenient for clinical application.
Conclusion: This study shows that compared with blood culture, the detection rate of mNGS pathogen that meets the diagnosis of sepsis is higher. We need a combination of multiple indicators to monitor the early diagnosis and treatment of sepsis.
Keywords: clinical concordance, true positive rate, metagenomic next-generation sequencing, blood infection, sepsis
Introduction
Metagenomic next-generation sequencing (mNGS), a new pathogen detection technology, does not rely on sequence amplification of specific gene primers. It is increasingly used in clinical pathogen detection due to its short sequencing time1 and high sensitivity, and the approximate detection sensitivity range is 68%-88%.2,3 We found that the overall pathogen detection sensitivity using mNGS was significantly higher than that of conventional cultures, especially in blood samples. mNGS is also more sensitive in samples containing low levels of nucleic acids from microorganisms and, thus, is less affected by antimicrobial therapy.4 Additionally, the rate of positive mNGS results may be constant over different time points after sepsis.5
Severe cases of blood infection will lead to multiple organ failure, neurocognitive impairment, and even death.6,7 Therefore, rapid diagnosis and preliminary treatment are needed in clinics. Blood culture is the most commonly used method to identify pathogens in sepsis, but it is time-consuming and susceptible to contamination. The positive rate in culture is approximately 30–40%,8 and the spectrum of disease detection is limited. Therefore, mNGS shows great clinical value for pathogen detection in suspected sepsis.3 Plasma mNGS detects circulating free DNA (cfDNA), a small nucleic acid fragment filtered into the blood or sterile body fluid after microbial death and lysis.9 The commercial quantitative plasma mNGS test (ie, the Karius test) was first described in 2019 and used to study and evaluate the true clinical manifestations of the mNGS test in sepsis patients.3,10
However, there is great controversy in the clinical interpretation of mNGS tests, such as the judgment of low sequence number viruses and how to evaluate whether there are pathogenic bacteria for the detected suspected environmental or human-colonized microbial flora.11 Therefore, clarifying the concordance between mNGS and the actual clinical diagnosis can best reflect the clinical value of mNGS technology. In the clinical verification conducted by Timothy and other experts, 350 patients who met the diagnostic criteria of sepsis were tested. The diagnostic sensitivity of blood mNGS was 93.7%, and the detection consistency was 84.8% compared with the gold standard of microbial diagnosis.10 In this study, we aimed to analyze the concordance between the results of laboratory plasma mNGS reports and clinical diagnoses, hoping to improve doctors’ confidence in the results of mNGS so that mNGS can be better used for the early diagnosis of sepsis.
Materials and Methods
Study Population
We retrospectively reviewed 99 blood samples from 92 patients with suspected bloodstream infection from July 2021 to January 2022, The exclusion criteria were as follow: (1) Did not agree to take the mNGS detection. (2) Unqualified specimens and incomplete clinical data, such as those of patients who received mNGS detection in the outpatient department or those who did not receive follow-up treatment in our hospital. The 99 blood samples included 2 patients underwent a DNA mNGS test twice and 5 patients underwent DNA and RNA mNGS tests simultaneously. We also analyzed the mNGS results of blood samples and bronchoalveolar lavage fluid (BALF) samples from 8 patients with sepsis secondary to pneumonia and the sampling interval less than 24 hours. The study was approved by the ethics committee of Taizhou Hospital and was in line with the Declaration of Helsinki (No: K20220930).
In the clinic, pathogen diagnosis was made according to a comprehensive analysis of the clinical examinations, mainly based on conventional culture results, and the purpose of this study was to judge the clinical concordance of mNGS results with the blood culture results, clinical antibiotic adjustment, relevant inflammatory indicators and clinical symptoms.12 Then, the clinical efficiency of mNGS in the diagnosis of suspected sepsis pathogens could be improved. Experienced clinicians diagnose patients with sepsis according to the sepsis 3.0 diagnostic criteria jointly issued by the Society of Intensive Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM),13 in which the definition of sepsis is life-threatening organ dysfunction caused by the uncontrolled response of the body’s to infection. Sepsis 3.0 = infection + SOFA score ≥ 2, SOFA score: sequential organ failure score.
Clinical Data Collection
The clinical data collection of the selected subjects included sex, age, and basic diseases and complications, routine blood examination, procalcitonin (PCT), C-reactive protein (CRP), interleukin-6 (IL-6); EICU stay days, hospital stay days, breathing, heart rate; temperature (greater than 38.5 °C or not), experiential antibiotic use after admission and antibiotic use after sepsis and fever, blood culture results, and mNGS bacteria and sequence number results. The main observation index of clinical efficacy was whether the patient was discharged from the hospital or died.
For patients suspected of sepsis, blood was collected simultaneously for mNGS and blood culture within 24 hours. Blood culture was using Thermo Scientific culture bottles with two sets of aerobic and anaerobic culture respectively in the blood culture instrument BD BACTECTM FX40 (Becton Dickinson). VITEK ® MS mass spectrometer was used to identify the strains of Positive blood culture bottles. In addition, for some patients with sepsis secondary to pneumonia, blood and BALF were collected simultaneously within 24 hours for mNGS. The microbial nucleic acid sequences of the samples were analyzed by high-throughput sequencing technology, and then identified by comparing with the nucleic acid sequences of the existing microorganisms in the database.
Sample Processing and DNA Extraction
A volume of 3 mL of blood was drawn from patients, placed in a blood collection tubes, stored at room temperature for 3–5 minutes before plasma separation and centrifuged at 3000 rpm for 10 minutes at 4°C within 8 hours of collection, plasma was transferred to new sterile tubes. DNA was extracted from 300 μL of plasma using TIANamp Micro DNA Kit (DP316, TIANamp Biotech, Beijing, China) following the manufacturer’s instructions. The extracted DNA was used for DNA library construction.
BALF was collected based on the standard clinical procedure. BALF was inactivated at 65°C for 30 minutes immediately after collection. Add 2 times the volume of protease K, 37°C metal bath for 30 minutes. 0.5 mL Pretreatment sample and 7.2 μL Wall lysozyme which were putted into 1.5 mL microcentrifuge tube were mixed and centrifuged, and the metal bath is at 30°C for 10 minutes. Transfer the above to a new 1.5 mL microcentrifuge tube, and Rejoin 0.25 mL glass beads at 1500 RPM for 20 minutes, then 8000 RPM centrifugation for 30 seconds. 0.3 mL sample was separated into a new 1.5 mL microcentrifuge tube and DNA was extracted using the TIANamp Micro DNA Kit (DP316, TIANGEN BIOTECH) according to the manufacturer’s recommendation.
Library Construction and Sequencing
The library was constructed by DNA fragmentation, end repair, linker connection, and PCR. The fragment size of the Agilent 2100 Bioanalyzer quality control library was approximately 300 bp. A Qubit dsDNA HS assay kit (Thermo Fisher Scientific Inc.) was used to qualify the concentration of the DNA library. The constructed library was pooled and cyclized, and then DNA nanoball (DNB) nanospheres were generated by rolling ring replication (RCA). The prepared DNB nanospheres were loaded into the sequencing chip and sequenced using the BGISEQ-50 platform.14 The sequencing strategy was single-end 50 bp. At least 2 Gb of raw data was produced from each sample.
Bioinformatics Analysis
The low-quality reads were removed to obtain high-quality data. Via BWA (BWA: http://bio-bwa.sourceforge.net/) Alignment removes the data of human reference genome sequence from high-quality data.15 The remaining data were classified by aligning to the Pathogens metagenomics Database (PMDB, a commercial pathogen genome catalog developed and owned by BGI-Shenzhen, China). The version used in this study was PMDB v6.0, and it was used to obtain the sequence number that can match a certain pathogen, and judge the possible pathogen according to the sequence number and other clinical tests. In the interpretation of clinical samples, viral, bacterial and fungal pathogens were reported as positively detected if more than 3 aligned reads were detected in the sample. Parasites were reported as positively detected if more than 100 specifically aligned reads were detected in the sample. Strictly aligned sequence book of Mycobacterium tuberculosis is greater than 1. The reference database contains 6350 bacteria, 1064 fungi, 4945 viruses, and 234 parasites.
Statistics Analysis
First, categorical variables are reported as numbers (percentages). The chi-square test and Fisher’s exact test were used to evaluate independent binomial variables, and the difference of Clinical symptoms and laboratory inflammatory indicators were detected by the Mann–Whitney test. P < 0.05 was considered statistically significant. SPSS statistical package 22.0 software is used for statistical analysis, and plotted using GraphPad Prism 7 software. Furthermore, the sequencing reads of each sample were standardized according to the number of reads per million (RPM) of the total sequencing reads. Then, the cor. test function in R software (R-4.1.2) was used to calculate the Pearson correlation coefficient between each microbial ecological diversity index and clinical phenotype.
Results
Clinical Information
In our study, 99 blood samples (92 hospitalized patients, 62 males and 30 females) were enrolled for the mNGS test and mean age was 59.19±18.89 years. According to the definition of sepsis and SOFA score, 71 patients were diagnosed with sepsis, of which 61 patients had positive mNGS test results in blood samples. In-depth clinical evaluation revealed that 32 patients had sepsis secondary to pneumonia. The statistics for the clinical information are shown in Table 1.
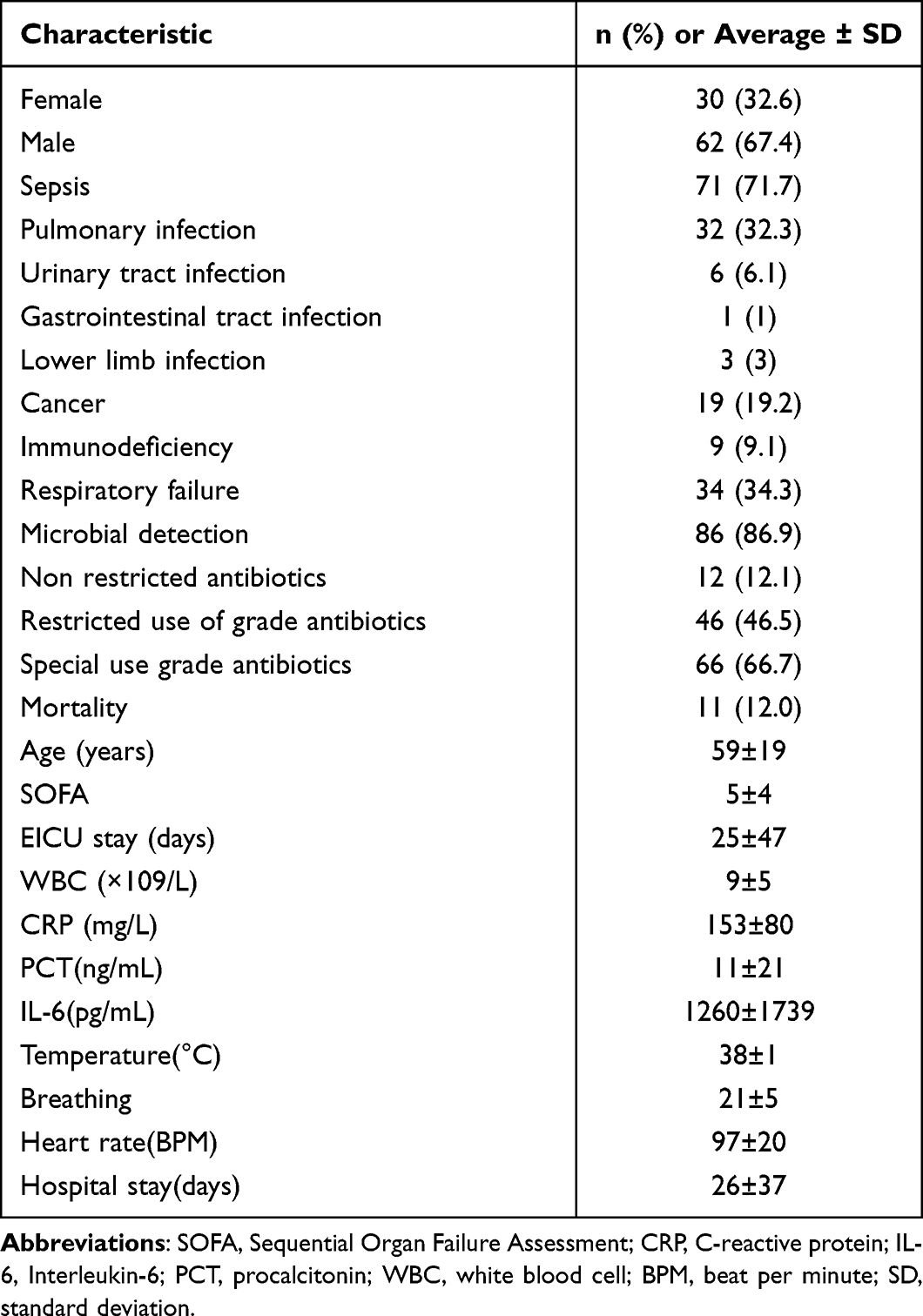 |
Table 1 Clinical Characteristics of mNGS Results of 99 Blood Samples |
mNGS Results and Clinical Concordance
Sixty-eight out of 99 blood samples tested by mNGS were submitted to blood culture at the same time. Figure 1A shows the original results comparing pathogen detection rates of different disease groups in mNGS and blood culture. Figure 1B shows the clinical concordance comparison of the detection rate of pathogens that met the clinical diagnosis under different disease groups for mNGS and blood culture. In the chi-square test of the positive rate, there were significant differences in mNGS and blood culture among the overall group, sepsis group, and unknown group. At the same time, there were no significant differences in the nonsepsis group because of the small number of samples. Figure 1C and D shows the consistency of the detection rate of mNGS and blood culture (positive 18.52% vs 10.47%; negative 9.26% vs 29.07%).
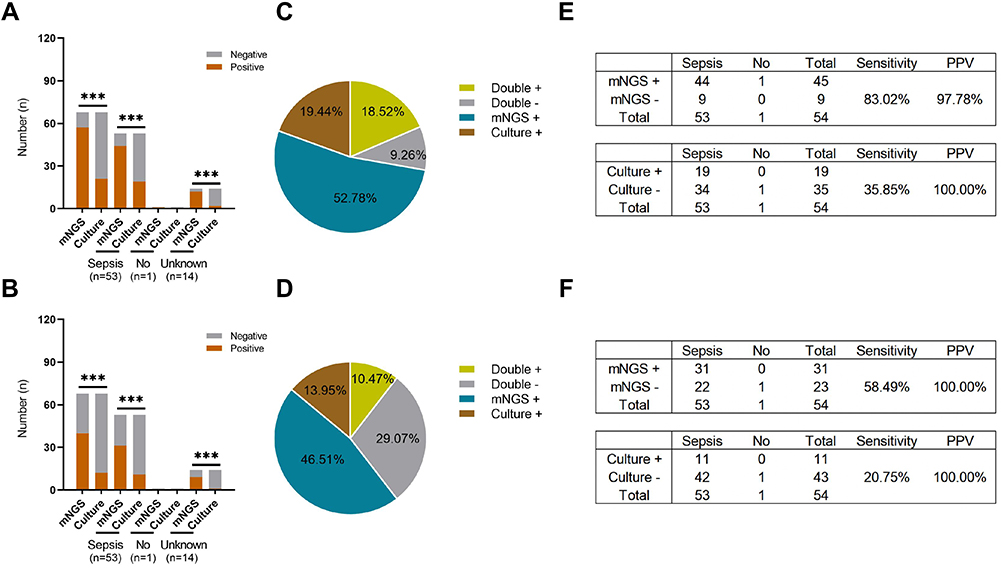 |
Figure 1 Comparison of the detection rate between the original results of mNGS and the clinical concordance results (true positive) and blood culture. (A and B) 68 specimens of mNGS and blood culture at the same time were divided into sepsis group, non-sepsis group and unknown group, (A) is the positive detection rate of the original report, and (B) is the positive detection rate of the clinical concordance report. In the overall group (P < 0.001), the sepsis group (P < 0.001) and the unknown group (P < 0.001), there were significant differences in mNGS and blood culture results, but there was no difference in the non-sepsis group due to the small number of samples (P > 0.05). (C and D) Clinical concordance of mNGS and blood culture in the original report and the clinical concordance report. (E and F) the two groups of tables show the comparison of detection sensitivity and positive predictive value of mNGS and blood culture in the original report and clinical concordance report. Abbreviation: PPV, positive predictive value. Notes: ***P < 0.001. +, positive. -, negative. |
The results of mNGS in 68 blood samples were further evaluated for sensitivity between laboratory results and clinical results in the sepsis and nonsepsis groups. In the laboratory results, the sensitivity of mNGS in the diagnosis of sepsis was 83.02%, and the positive predictive value was 97.78%; The sensitivity of blood culture in the diagnosis of sepsis was 35.85%, and the positive predictive value was 100%. In the clinical concordance results, the sensitivity of mNGS in the diagnosis of sepsis was 58.49%; and the sensitivity of blood culture was 20.75%. The results indicated that the detection sensitivity of mNGS was higher than that of blood culture (83.02% vs 35.85%, 58.49% vs 20.75%; P < 0.05). (Figure 1E and F).
Adjustment of the Medication Plan in the Clinical Concordance and Nonconcordance Groups of Sepsis Patients
In our study, among the patients diagnosed with sepsis, 61 cases had positive reports from mNGS, 43 cases were clinically concordant reports, and 24 of them were empirical treatments covering the pathogenic bacteria detected by mNGS. Therefore, clinicians continued treatment; In 7 cases, practical treatment covered part of the pathogenic bacteria detected by mNGS. At the same time, fungi or viruses were also detected by mNGS, so the doctor added antifungal or antiviral treatment to the original treatment. Two patients underwent mNGS detection after empirical treatment for a period of time. The number of mNGS detection sequences was small, and the laboratory inflammation index decreased. The doctor considered that the patient had no blood flow infection at present, so he stopped antibiotics. In one case, a part of empirical treatment covered the detection of pathogenic bacteria of mNGS detected particular pathogenic bacteria, such as Streptococcus suis and Leptospira interrogans, and doctors changed the drugs to more targeted treatment. One case was clinically pathogenic bacteria detected by mNGS, but the patient died due to serious illness. One case was clinically pathogenic bacteria detected by mNGS. However, during the treatment, the patient was repeatedly febrile and required to be transferred to a higher hospital. The outcome was unknown. Eighteen cases were clinical nonconcordant reports, and 18 cases of mNGS only detected a virus, but doctors did not use any antiviral drugs. The reason may be that there were too few viruses detected. However, 10 patients continued to use empirical treatment, and 8 patients were treated with high-efficiency antibiotics. Therefore, it was determined that these 18 patients were infected. The possible cause is that mNGS detected no pathogenic bacteria, or the patient was not infected by blood flow but was infected in other body parts.
Comparison of Relevant Indices Between the Clinical Concordance and Nonconcordance Groups in Patients with Sepsis
In the study, 61 patients diagnosed with sepsis had positive mNGS results, of which 43 were clinically concordant and 18 were clinically nonconcordant. First, Figure 2 shows the comparison of heart rate and respiration and inflammatory indices PCT and IL-6 between the clinical concordance group and the nonconcordance group based the mNGS results. It can be seen from the comparison in the figure that the heart rate and respiration of the patients in the clinical concordance group were faster than those in the nonconcordance group. The PCT and IL-6 of the patients in the clinical concordance group were also higher than those in the nonconcordance group, indicating that the patients in the clinical concordance group were more seriously ill than those in the nonconcordance group because the clinical concordance group had clear pathogenic bacteria in the blood flow, which is a serious sepsis disease. There are many reasons leading to clinical nonconcordance. It is possible that the patient is only locally infected and does not have systemic blood flow infection or that mNGS did not detect the pathogenic bacteria. Different clinical treatment schemes are different according to the severity of the disease, and the patient’s disease outcome may also be different. This finding also further verified the value of blood mNGS testing technology in the clinic.
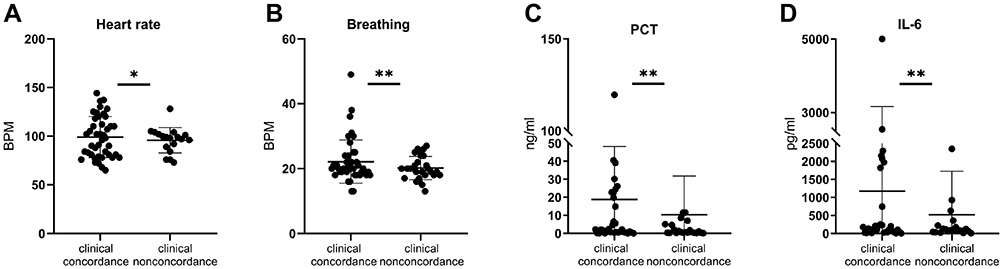 |
Figure 2 Comparison of relevant indexes between clinical concordance group and nonconcordance group. (A) The heart rate of patients in the clinical concordance group was significantly higher than that in the clinical nonconcordance group (P < 0.05 by Wilcoxon rank sum test). (B) The breathing of patients in the clinical concordance group was significantly higher than that in the clinical nonconcordance group (P < 0.01 by Wilcoxon rank sum test); (C) PCT in the clinical concordance group was significantly higher than that in the clinical nonconcordance group (P < 0.01 by Wilcoxon rank sum test). (D) IL-6 of patients in the clinical concordance group was significantly higher than that in the clinical nonconcordance group (P < 0.01 by Wilcoxon rank sum test). *P < 0.05, **P < 0.01. |
Comparison of the Distribution of Bacteria, Fungi, and Viruses in the Clinical Concordance and Nonconcordance Groups of mNGS in Patients with Sepsis
Figure 3 shows all pathogens detected by mNGS. The pathogens in the clinical concordance group with sepsis are mainly bacteria and fungi,11,16 among which the most common bacteria include Escherichia coli, Pseudomonas aeruginosa, Acinetobacter baumannii, Staphylococcus aureus, Klebsiella pneumonia, and Leptospira. The detected fungi include Marneffei basket fungus, Aspergillus, and Candida albicans.17 There were viruses detected from both the clinical concordance group and nonconcordance group, including human γ Herpes virus type 4 (EBV),18 human α Herpes virus type 1 (HSV1), human β Herpesvirus 6B, human β Herpes virus type 5 (CMV), and various subtypes of the macrocyclic virus,19 which were detected in both groups. Combined with clinical information, sepsis was not considered.
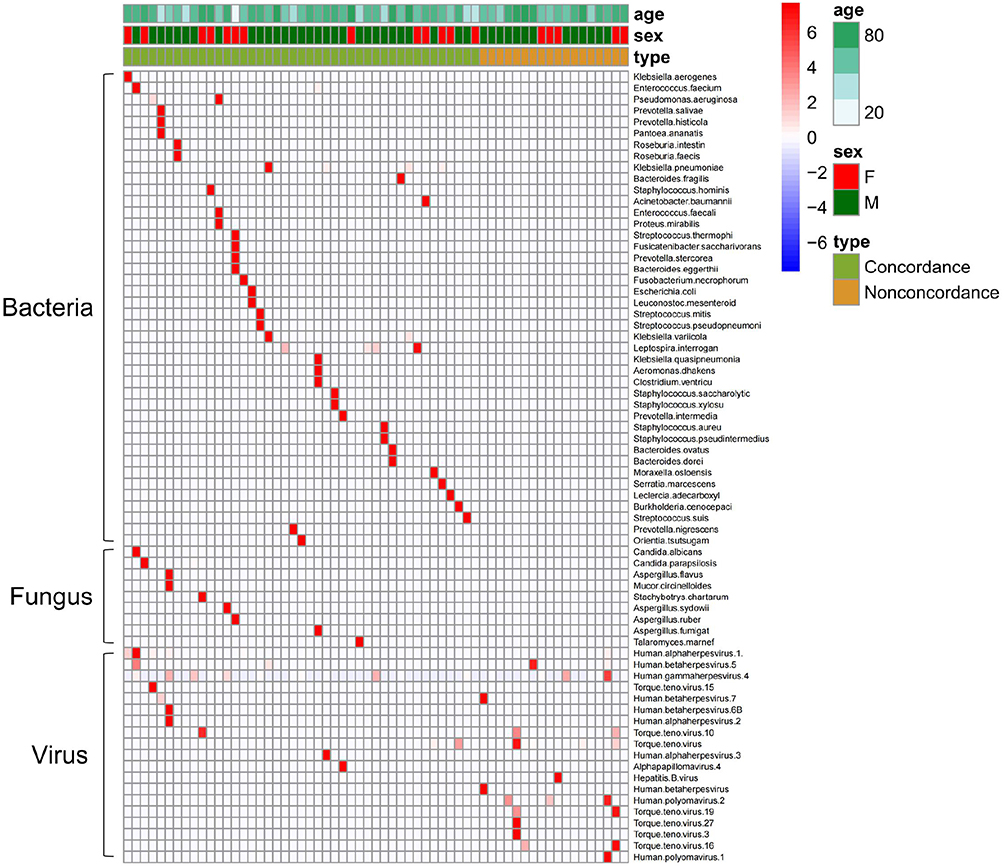 |
Figure 3 Comparison of the distribution of bacteria, fungi and viruses detected by mNGS between clinical concordance group and nonconcordance group. In the clinical concordance group, bacteria and fungi were mainly detected by mNGS; Only virus was detected in mNGS in the clinical nonconcordance group; Each row on the vertical plane represents a sample, and each row on the horizontal plane represents potential pathogenic bacteria; The top is the clinical phenotype, and the color block on the right represents the specific value of the clinical phenotype. |
Comparison of Pathogens Detected by Blood and BALF mNGS in Patients with Sepsis Secondary to Pulmonary Infection
Sepsis is a common secondary infection,20 and the primary focus is generally pulmonary infection, gastrointestinal infection, urinary infection,21 and lower limb ulceration infection. In this study, sepsis secondary to pulmonary infection was the most common, in which 8 patients underwent mNGS in alveolar lavage fluid and blood at the same time, as shown in Figure 4. Pathogenic bacteria were detected in the alveolar lavage fluid and blood samples of 5 patients (5/8). The detected bacteria included Acinetobacter baumannii, Pseudomonas aeruginosa, Staphylococcus aureus, and Klebsiella pneumonia, and the detected fungi were Lanobacteria marneffei and Aspergillus. It can be seen that only one or two kinds of pathogenic bacteria can be detected in mNGS of blood samples. However, with the detection of mNGS in alveolar lavage fluid as the primary focus, the types of pathogens are far more abundant than those in blood samples, and the detection abundance is much higher than that in blood samples (1000–10,000 times). The other 2 cases (2/8) had negative blood sample mNGS results, while pathogenic bacteria were detected in alveolar lavage fluid mNGS, including the common pathogenic bacteria Acinetobacter, Pseudomonas aeruginosa, and Stenotrophomonas maltophilia. Only Klebsiella pneumoniae was detected in 1 (1/8) blood sample mNGS, and the sequence number was low. A variety of bacteria dominated by Acinetobacter baumannii were detected in alveolar lavage fluid, and the sequence number was relatively high.
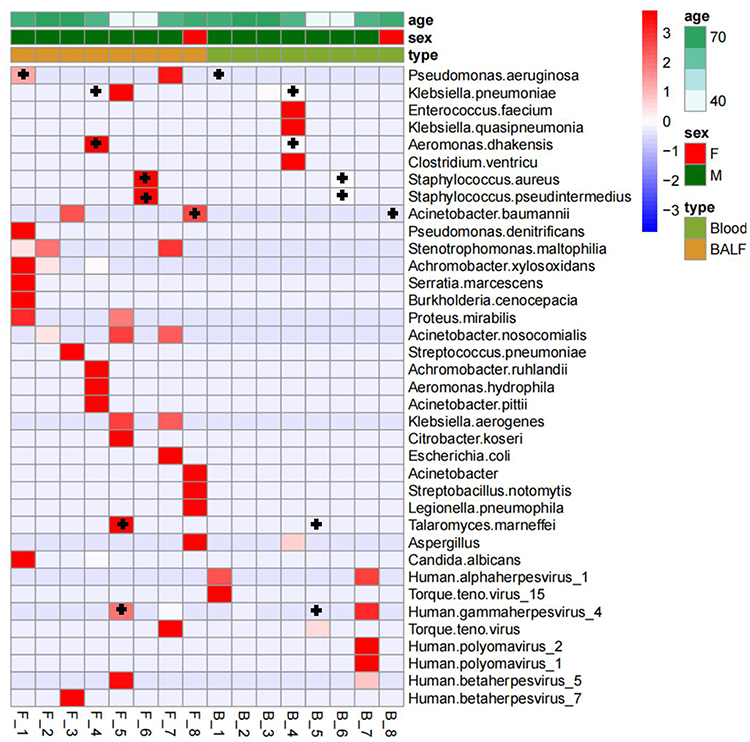 |
Figure 4 Comparison of pathogens detected by blood and BALF mNGS in patients with sepsis secondary to pulmonary infection; Each row on the vertical plane represents a sample, and each row on the horizontal plane represents potential pathogenic bacteria; The top is the clinical phenotype, and the color block on the right represents the specific value of the clinical phenotype.+, mNGS and BALF detected the same pathogenic bacteria. |
Discussion
This topic focuses on the analysis of the clinical concordance between mNGS and blood culture results from blood samples to clarify whether the pathogenic microorganisms detected by mNGS are in line with the clinical diagnosis and help with adjusting clinical treatment. Referring to other studies on this subject,22 the sensitivity of mNGS technology is higher than that of blood culture, and the true positive rate of mNGS combined with clinical information is also significantly higher than that of blood culture. At present, the etiology of sepsis is mostly bacterial and fungal infection. For the sample selection for mNGS detection technology, as sepsis is secondary to pulmonary infection, blood samples can be the best choice with a high detection rate and noninvasive, rapid sampling.
At present, mNGS technology can detect nearly all nucleic acid sequences in blood without bias, including a large number of human sequences and background mcfDNA contamination.11,23 Bacteria, fungi, and viruses can be detected by mNGS at the same time.16,24 The interpretation of the results and recognition by clinicians are the embodiment of the technical value of mNGS. In this study, according to the blood sample results from patients with suspected sepsis detected by mNGS, one or more bacteria were detected. If the bacteria belong to the same genus, clinicians generally adjust empirical medication or continue to use effective antibiotics.25 If one or more fungi are detected, which coincides with other laboratory examination results or patient conditions, clinicians will make a clearer diagnosis and effective treatment.26 If bacteria, fungi, and viruses appear in the mNGS report at the same time, it is be regarded as a clinical concordance report. If only a virus appears in the mNGS report, it is generally a false-positive since there are few cases of viral sepsis.27
The clinical concordance of viral pathogens in blood samples detected by mNGS is low. How to interpret viruses detected in blood sample with mNGS is still challenging. In a retrospective analysis, 492 clinical samples were examined for mNGS, including 384 serum samples, 92 nasopharyngeal swabs, 10 fecal samples, and 6 cerebrospinal fluid samples. Although the relevant sequences of 47 viruses belonging to 21 families were found in 93% of patients, only 13.4% of viruses are known to cause human infection.28 In combination with the doctor’s diagnosis, the patient’s clinical symptoms and treatment, and other laboratory tests for the patient, if the viral sequences detected by mNGS are few and do not conform to the above correlation, they are not considered pathogenic causes of sepsis.29 At this time, if only viruses are detected by mNGS but virus infection is not considered clinically, the pathogen of clinical infection is not truly detected by mNGS, and the mNGS detection report is not a report with clinical value. In addition, some viruses are self-limiting, and the immune function of the human body will defeat the virus within a certain period of time and restore health. Therefore, whether a large number of viruses detected in blood samples have pathogenicity or affect the prognosis of the disease also requires laboratory personnel to select whether to list pathogenic viruses according to the guidelines when interpreting the sequencing results of mNGS.30
A large cohort study in 2016 compared mNGS with the “gold standard” blood culture and found that the positive rate in blood culture combined with second-generation sequencing for the diagnosis of bacterial or fungal infection was significantly higher than that of blood culture alone.31 This conclusion was confirmed by subsequent studies, but there is still a problem with how to gain trust among clinicians. Clinicians trust the results of blood culture, and the clinical concordance of mNGS results with blood culture are important. We compared the clinical symptoms, laboratory-related inflammatory indicators, blood culture results and antibacterial treatment of patients who underwent mNGS to improve clinical concordance of mNGS results and improve clinicians’ trust in mNGS results. In recent years, an increasing number of studies have also described the relationship between mNGS results and clinical diagnosis and treatment.32
mNGS can be used to detect fungi, viruses, and some special pathogens that cannot be detected by traditional blood culture.33 To achieve early and accurate diagnosis of diseases, it is necessary not only to use a variety of detection technologies jointly but also to sample and detect more infected sites. The difference between blood mNGS and BALF mNGS pathogen examination lies in the following. First, BALF is obtained from the respiratory tract, which is typically contaminated with normal oral flora, commensal organisms, and colonizers, leading to a relatively lower purity than blood samples and more pathogens than blood samples.34 The initial infection site of a bloodstream infection is a lung infection, but not all pathogens of lung infections will enter the blood to cause sepsis. A study indicated that BALF mNGS was more sensitive than blood mNGS for bacterial and fungal pulmonary infections, which was consistent with research about the conventional test that the yield of BALF culture was higher than that of blood culture.35,36 We suggest that mNGS has potential for the diagnosis and treatment of acute and severe patients. Standardized interpretation rules and in-depth combination with clinical practice are essential for explaining mNGS results.37
There are still some limitations in this research on the interpretation of blood sample mNGS test results and the embodiment of clinical value for patients. As mentioned above, most of the viruses detected by mNGS cannot be the cause of infection. On the one hand, there is a lack of guidance in the interpretation of the report. On the other hand, the type of specimen also has a great impact on the mNGS results. There are few studies on the clinical value of mNGS test results, including shortening of the course of the disease, reducing cost, and reducing invasive operations.
Conclusion
In conclusion, compared with conventional blood culture, mNGS can rapidly detect pathogenic microorganisms, and the detection rate is higher. When interpreting the mNGS report, it is necessary to combine the clinician’s diagnostic considerations, patients’ clinical symptoms, laboratory-related inflammatory indicators and control blood culture results to improve clinical trust in the mNGS results. According to the classification of pathogens detected by mNGS and clinical experience, the pathogens that cause sepsis are mainly bacteria and fungi. If a virus sequence is detected separately, it may be a false-positive.
Data Sharing Statement
The datasets CNSA for this study can be found in the CNP0003136 [https://db.cngb.org/mycngbdb/submissions/project]. Please see the Data Availability section of the Author guidelines for more details.
Ethical Approval Information
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Medical Ethics Review Board of Taizhou Hospital of Zhejiang Province (No: K20220930; date of approval: 30 September 2022).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Taizhou Technology Project, Zhejiang Province (22ywa04) and Medical Science and Technology Project of Zhejiang Province (2023KY397).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Han D, Li Z, Li R, Tan P, Zhang R, Li J. mNGS in clinical microbiology laboratories: on the road to maturity. Crit Rev Microbiol. 2019;45(5–6):668–685. doi:10.1080/1040841X.2019.1681933
2. Jing C, Chen H, Liang Y, et al. Clinical evaluation of an improved metagenomic next-generation sequencing test for the diagnosis of bloodstream infections. Clin Chem. 2021;67(8):1133–1143. doi:10.1093/clinchem/hvab061
3. Goggin KP, Gonzalez-Pena V, Inaba Y, et al. Evaluation of plasma microbial cell-free DNA sequencing to predict bloodstream infection in pediatric patients with relapsed or refractory cancer. JAMA Oncol. 2020;6(4):552–556. doi:10.1001/jamaoncol.2019.4120
4. Huang ZD, Zhang ZJ, Yang B, et al. Pathogenic detection by metagenomic next-generation sequencing in osteoarticular infections. Front Cell Infect Microbiol. 2020;10:471. doi:10.3389/fcimb.2020.00471
5. Grumaz S, Grumaz C, Vainshtein Y, et al. Enhanced performance of next-generation sequencing diagnostics compared with standard of care microbiological diagnostics in patients suffering from septic shock. Crit Care Med. 2019;47(5):e394–e402. doi:10.1097/CCM.0000000000003658
6. Christensen MS, Heyman M, Möttönen M, Zeller B, Jonmundsson G, Hasle H. Treatment-related death in childhood acute lymphoblastic leukaemia in the Nordic countries: 1992–2001. Br J Haematol. 2005;131(1):50–58. doi:10.1111/j.1365-2141.2005.05736.x
7. Inaba H, Pei D, Wolf J, et al. Infection-related complications during treatment for childhood acute lymphoblastic leukemia. Ann Oncol. 2017;28(2):386–392. doi:10.1093/annonc/mdw557
8. Gyarmati P, Kjellander C, Aust C, Song Y, Öhrmalm L, Giske CG. Metagenomic analysis of bloodstream infections in patients with acute leukemia and therapy-induced neutropenia. Sci Rep. 2016;6:23532. doi:10.1038/srep23532
9. Han D, Li R, Shi J, Tan P, Zhang R, Li J. Liquid biopsy for infectious diseases: a focus on microbial cell-free DNA sequencing. Theranostics. 2020;10(12):5501–5513. doi:10.7150/thno.45554
10. Blauwkamp TA, Thair S, Rosen MJ, et al. Analytical and clinical validation of a microbial cell-free DNA sequencing test for infectious disease. Nat Microbiol. 2019;4(4):663–674. doi:10.1038/s41564-018-0349-6
11. Simner PJ, Miller S, Carroll KC. Understanding the promises and hurdles of metagenomic next-generation sequencing as a diagnostic tool for infectious diseases. Clin Infect Dis. 2018;66(5):778–788. doi:10.1093/cid/cix881
12. Lee RA, Al Dhaheri F, Pollock NR, Sharma TS, Dekker JP. Assessment of the clinical utility of plasma metagenomic next-generation sequencing in a pediatric hospital population. J Clin Microbiol. 2020;58(7). doi:10.1128/JCM.00419-20
13. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):80. doi:10.1001/jama.2016.0287
14. Jeon YJ, Zhou Y, Li Y, et al. The feasibility study of non-invasive fetal trisomy 18 and 21 detection with semiconductor sequencing platform. PLoS One. 2014;9(10):e110240. doi:10.1371/journal.pone.0110240
15. Li H, Durbin R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics. 2009;25(14):1754–1760. doi:10.1093/bioinformatics/btp324
16. Wilson MR, O’Donovan BD, Gelfand JM, et al. Chronic meningitis investigated via metagenomic next-generation sequencing. JAMA Neurol. 2018;75(8):947–955. doi:10.1001/jamaneurol.2018.0463
17. Chen J, Sun L, Liu X, et al. Metagenomic assessment of the pathogenic risk of microorganisms in sputum of postoperative patients with pulmonary infection. Front Cell Infect Microbiol. 2022;12:855839. doi:10.3389/fcimb.2022.855839
18. Reyes A, Carbo EC, Harinxma Thoe JSV, et al. Viral metagenomic sequencing in a cohort of international travellers returning with febrile illness. J Clin Virol. 2021;143:104940–104945. doi:10.1016/j.jcv.2021.104940
19. Liu WD, Yen TY, Liu PY. Clinical application of metagenomic next-generation sequencing in patients with hematologic malignancies suffering from sepsis. Microorganisms. 2021;9(11):2309–2319. doi:10.3390/microorganisms9112309
20. van Vught LA, Klein Klouwenberg PM, Spitoni C, et al. Incidence, risk factors, and attributable mortality of secondary infections in the intensive care unit after admission for sepsis. JAMA. 2016;315(14):1469–1479. doi:10.1001/jama.2016.2691
21. Gharbi M, Drysdale JH, Lishman H, et al. Antibiotic management of urinary tract infection in elderly patients in primary care and its association with bloodstream infections and all cause mortality: population based cohort study. BMJ. 2019;364:l525. doi:10.1136/bmj.l525
22. Gu W, Deng X, Lee M, et al. Rapid pathogen detection by metagenomic next-generation sequencing of infected body fluids. Nat Med. 2021;27(1):115–124. doi:10.1038/s41591-020-1105-z
23. Deng X, Achari A, Federman S, et al. Metagenomic sequencing with spiked primer enrichment for viral diagnostics and genomic surveillance. Nat Microbiol. 2020;5(3):443–454. doi:10.1038/s41564-019-0637-9
24. Qian YY, Wang HY, Zhou Y, et al. Improving pulmonary infection diagnosis with metagenomic next generation sequencing. Front Cell Infect Microbiol. 2020;10:567615. doi:10.3389/fcimb.2020.567615
25. Li H, Gao H, Meng H, et al. Detection of pulmonary infectious pathogens from lung biopsy tissues by metagenomic next-generation sequencing. Front Cell Infect Microbiol. 2018;8:205. doi:10.3389/fcimb.2018.00205
26. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–s240. doi:10.1093/cid/ciy693
27. Fang X, Mei Q, Fan X, et al. Diagnostic value of metagenomic next-generation sequencing for the detection of pathogens in bronchoalveolar lavage fluid in ventilator-associated pneumonia patients. Front Microbiol. 2020;11:599756. doi:10.3389/fmicb.2020.599756
28. Chau NVV, van Doorn HR, Thwaites G, Delwart E. Viruses in Vietnamese patients presenting with community-acquired sepsis of unknown cause. J Clin Microbiol. 2019;57(9):e00386–19. doi:10.1128/JCM.00386-19
29. Moustafa A, Xie C, Kirkness E, Biggs W. The blood DNA virome in 8000 humans. PLoS Pathog. 2017;13(3):e1006292. doi:10.1371/journal.ppat.1006292
30. Ebinger A, Fischer S, Höper D. A theoretical and generalized approach for the assessment of the sample-specific limit of detection for clinical metagenomics. Comput Struct Biotechnol J. 2021;19:732–742. doi:10.1016/j.csbj.2020.12.040
31. Long Y, Zhang Y, Gong Y, et al. Diagnosis of sepsis with cell-free DNA by next-generation sequencing technology in ICU patients. Arch Med Res. 2016;47(5):365–371. doi:10.1016/j.arcmed.2016.08.004
32. Zhou H, Larkin PMK, Zhao D, et al. Clinical impact of metagenomic next-generation sequencing of bronchoalveolar lavage in the diagnosis and management of pneumonia: a multicenter prospective observational study. J Mol Diagnos. 2021;23(10):1259–1268. doi:10.1016/j.jmoldx.2021.06.007
33. Armstrong AE, Rossoff J, Hollemon D, Hong DK, Muller WJ, Chaudhury S. Cell-free DNA next-generation sequencing successfully detects infectious pathogens in pediatric oncology and hematopoietic stem cell transplant patients at risk for invasive fungal disease. Pediatr Blood Cancer. 2019;66(7):e27734. doi:10.1002/pbc.27734
34. Qu Y, Ding W, Liu S, et al. Metagenomic next-generation sequencing vs traditional pathogen detection in the diagnosis of infection after allogeneic hematopoietic stem cell transplantation in children. Front Microbiol. 2022;13:868160. doi:10.3389/fmicb.2022.868160
35. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl2):S27–S72. doi:10.1086/511159
36. Chen X, Ding S, Lei C, et al. Blood and bronchoalveolar lavage fluid metagenomic next-generation sequencing in pneumonia. Can J Infect Dis Med Microbiol. 2020;2020:6839103. doi:10.1155/2020/6839103
37. Chen J, Zhao Y, Shang Y, et al. The clinical significance of simultaneous detection of pathogens from bronchoalveolar lavage fluid and blood samples by metagenomic next-generation sequencing in patients with severe pneumonia. J Med Microbiol. 2021;70(1). doi:10.1099/jmm.0.001259
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.