Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Clinical Concepts for Triple Therapy Use in Patients with COPD: A Delphi Consensus
Authors Miravitlles M ![]() , Acharya S, Aggarwal B
, Acharya S, Aggarwal B ![]() , Fernandes FL, Dreyse J, Jardim JR
, Fernandes FL, Dreyse J, Jardim JR ![]() , Juthong S, Levy G, Sivori M
, Juthong S, Levy G, Sivori M ![]()
Received 2 June 2023
Accepted for publication 15 August 2023
Published 28 August 2023 Volume 2023:18 Pages 1853—1866
DOI https://doi.org/10.2147/COPD.S424128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Marc Miravitlles,1 Sudeep Acharya,2 Bhumika Aggarwal,2 Frederico LA Fernandes,3 Jorge Dreyse,4 José R Jardim,5 Siwasak Juthong,6 Gur Levy,7 Martin Sivori8
1Pneumology Department, Hospital Universitari Vall d’Hebron/Vall d’Hebron Institut de Recerca (VHIR), Vall d’Hebron Barcelona Hospital Campus; CIBER de Enfermedades Respiratorias (CIBERES), Barcelona, Spain; 2Emerging Markets, GlaxoSmithKline, Singapore; 3Hospital das Clinicas HCFMUSP, Faculdade de Medicina, Universidade de Sao Paulo, Sao Paulo, SP, Brazil; 4Internal Medicine and Critical Care Center Departments, Clínica Las Condes and School of Medicine, Universidad Finis Terrae, Santiago, Chile; 5Respiratory Division, Escola Paulista de Medicina, Federal University of São Paulo, Sao Paulo, Brazil; 6Division of Respiratory and Respiratory Critical Care Medicine, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand; 7Emerging Markets, GlaxoSmithKline, Panama City, Panama; 8Pneumonology University Center, School of Medicine, University of Buenos Aires, Argentina, Unit of Pneumonology Hospital “Dr.J.M. Ramos Mejia”, Buenos Aires, Argentina
Correspondence: Marc Miravitlles, Pneumology Department, Hospital Universitari Vall d’Hebron, Pg. Vall d’Hebron 119-129, Barcelona, 08035, Spain, Tel/Fax +34 932746083, Email [email protected]
Purpose: Role of triple therapy in chronic obstructive pulmonary disease (COPD) management is supported by growing evidence, but consensus is lacking on various aspects. We conducted a Delphi survey in respiratory experts on the effects of triple therapy on exacerbation reduction, early optimization, pneumonia risk, and mortality benefits in COPD management.
Methods: The study comprised 2-round online surveys and a participant meeting with 21 respiratory experts from 10 countries. The 31-statement questionnaire was prepared using Decipher software after literature review. Responses were recorded using Likert scale ranging from 1 (disagreement) to 9 (agreement) with a consensus threshold of 75%.
Results: All experts participated in both surveys and 14/21 attended participant meeting. Consensus was reached on 13/31 questions in first survey and 4/14 in second survey on: mortality benefits of triple therapy; comparable pneumonia risk between single inhaler triple therapy (SITT) and multiple inhaler triple therapy (81%); preference of SITT for patients with high eosinophil count (95%); exacerbation risk reduction and healthcare cost benefits with early initiation of SITT post exacerbation-related hospitalization (< 30 days) (86%). No consensus was reached on first line SITT use after first exacerbation resulting in COPD diagnosis (62%).
Conclusion: This study demonstrated that there is consensus among experts regarding many of the key concepts about appropriate clinical use and benefits of triple therapy in COPD. More evidence is required for evaluating the benefits of early optimisation of triple therapy.
Keywords: SITT, MITT, triple inhaled therapy, Delphi procedure, COPD exacerbations, COPD mortality
Introduction
Chronic obstructive pulmonary disease (COPD) treatment strategies call for a tailored approach to patient needs, in which therapies are introduced to relieve symptoms, improve health status and exercise tolerance, and reduce future risk and severity of exacerbations (including prevent disease progression, prevent and treat exacerbations and reduce mortality).1 Bronchodilator therapy with long-acting muscarinic antagonist (LAMA) and/or long-acting β2-agonist (LABA) is the recommended initial treatment regimen for COPD management.1,2 However, for certain patients with COPD who are at a higher risk of exacerbation while on dual bronchodilator therapy, triple therapy with an inhaled corticosteroid (ICS), LAMA, and LABA is recommended by the Global Initiative for Chronic Obstructive Lung Disease (GOLD).1 Similarly, the Spanish chronic obstructive pulmonary disease guidelines (GesEPOC) 2021 recommend using triple therapy in high-risk patients whose exacerbations are not controlled with dual bronchodilator or ICS/LABA combination and with blood eosinophils ≥100 cells/µL.3 In addition, GOLD 2023 strategy recommends use of triple therapy as initial management in patients with two or more moderate exacerbations or one severe exacerbation and with blood eosinophils ≥300 cells/µL.1
Data from randomized controlled multi-country studies such as IMPACT and ETHOS have shown that triple therapy reduced the risk of exacerbation and decreased the risk of mortality compared to dual bronchodilator therapy in patients with history of exacerbations.4,5 Triple inhaler therapy in patients with COPD can be prescribed through multiple inhaler triple therapy (MITT) or single inhaler triple therapy (SITT). MITT, such as fluticasone propionate/salmeterol plus tiotropium or budesonide/formoterol added to tiotropium, was commonly prescribed in patients with COPD who required triple therapy prior to the development and availability of a SITT combination.6–9 MITT requires the use of at least two inhalers more than once a day in majority of patients with COPD who require triple therapy, which is potentially associated with poor compliance and adherence and an increased potential for inhaler technique errors due to patients having to learn multiple devices.10–13 Considering these reasons, SITT can be an optimal option to simplify therapy, potentially improve adherence and compliance with treatments for patients with COPD.12,13
Currently, the triple therapies available in a single inhaler device are: fluticasone furoate/vilanterol/umeclidinium for once daily administration (OD), beclomethasone dipropionate/formoterol fumarate/glycopyrronium bromide for twice a day administration (BID), and budesonide/glycopyrronium bromide/formoterol fumarate (BGF) for BID administration.6 A real-world retrospective cohort study conducted by Alcázar-Navarrete et al reported that patients initiating SITT experienced a clinically meaningful improvement in treatment persistence during a 12-month follow-up, which resulted in significant reductions in the risk of all-cause mortality and frequency of exacerbations compared with patients initiating MITT.14
There is, however, a lack of consensus and dichotomous evidence regarding selection of appropriate patients for triple therapy and treatment outcomes including mortality reduction benefit, risk of exacerbation, early optimization, and pneumonia risk associated with the use of triple therapy in patients with COPD.15–17
The aim of this Delphi study was to understand and measure the level of consensus (agreement or disagreement) on concepts, such as exacerbation reduction, early optimization, pneumonia risk, and mortality benefits related to triple therapy use in patients with COPD among a group of respiratory experts in the field of COPD.
Materials and Methods
Study Design
This study used a Delphi technique, which included a two-round Delphi survey and an online participant meeting to assess the level of consensus among the respiratory experts for the management of COPD with triple therapy.18 The cross-sectional surveys were conducted between September and November 2022 among respiratory experts with expertise in COPD management. The Delphi survey was developed by a scientific committee and was run by an independent external vendor. The team developed the questionnaires, hosted the online surveys using Decipher software (version compat=’153’), and analyzed the data. All information provided by participants was kept confidential and anonymous. The research complied with UK Data Protection law (UK General Data Protection Regulation; GDPR), with the British Healthcare Business Intelligence Association’s (BHBIA) Legal & Ethical Guidelines, and with the European Pharmaceutical Market Research Association’s (EphMRA) code of conduct. No formal ethical approval was required because this was a non-interventional physician survey.
Participants
Twenty-one respiratory experts were invited to participate in the surveys. The respiratory experts were from 10 countries (Argentina, Brazil, Chile, Colombia, India, Kuwait, Mexico, Oman, Saudi Arabia, and Thailand) where both SITT and MITT treatment options for managing patients with COPD are available. The participants were chosen in a non-random manner, based on their expert knowledge of COPD and its management and their years of expertise in the field. The selected participants represented geographic diversity, had experience in the use of triple therapies (both SITT and MITT) and fulfilled three or more of the following criteria: (a) tier one experts or key opinion leaders in representative countries, (b) involved in a wide range of scientific activities related to COPD or inhaled medication, such as speaker at a congress, (c) membership in a respiratory society, (d) membership of an international and/or national guideline committee and (e) having an interest in improving patient outcomes in COPD.
Stages of the Delphi Procedure
The Delphi Procedure Comprised Three Stages
Survey Questionnaire Development
The first questionnaire was developed using a comprehensive targeted literature review on the management of COPD in patients prescribed triple therapy. Topics with dichotomous evidence were identified and a questionnaire was formulated on these topics. A subsequent questionnaire was developed for the second survey with questions which did not achieve consensus in the first round. The questions for the second round were modified based on participants’ feedback, for clarification purposes. The questionnaire was validated by a non-participating respiratory expert for both rounds of survey.
Delphi Surveys and Participant Meeting
The first round of the Delphi survey was conducted in September 2022 and was completed before the participants’ meeting. The survey was emailed to the participants and consisted of 31 questions. Participants from the first round of survey were invited for an online, virtual meeting to discuss the results from the first survey and to understand their views on scientific and clinical data for new concepts in COPD management with triple therapy. The participant meeting was arranged and facilitated by the sponsor, but the sponsor did not participate in the Delphi surveys. Following the participant meeting, the second Delphi survey link was emailed to the participants. The second round was open from October to November 2022.
Development of Consensus Statements
A 1-to-9-point Likert scale was used to phrase questions and rate the responses in accordance with previous Delphi surveys.18–22 The participants anonymously assessed their level of agreement with each statement, ranging from 1 (completely disagree with the statement) to 9 (completely agree with the statement). These scores were divided into three groups: agree (7–9 points), neither agree nor disagree (4–6 points) and disagree (1–3 points). Four open-ended questions were also included in the first round of survey. See complete questionnaire in Supplementary Table S1.
Data Analysis
All questionnaires were fully completed and were taken into consideration for the descriptive analysis of all data. Data were presented as the mean, standard deviation (SD), median, and range. Using a deductive approach, analysis of the first survey results and the participant meeting was conducted to identify commonalities in the panel’s overall opinion to create a second survey. A consensus was deemed to have been reached when 75% of the respondents scored within the agreement range (7–9 points) or disagree range (1–3) for negative consensus. This was consistent with previous studies that have employed the Delphi method.19–21,23 All responses were examined for accuracy and consistency by an external reviewer for data quality checks. The research team collected all the responses, and analysis was performed using Microsoft Office Excel (ver. 2019).
Results
Participants
In the first round of the survey, all 21 participating respiratory experts completed the survey (response rate of 100%). Fourteen experts attended the participant meeting (66.7%). All the original participants completed the post-meeting second survey conducted in October–November 2022 (response rate of 100%). The participating experts had an average age of 50.7 years and managed an average of 161 patients in a month. All participants had advanced medical degrees, with particular interest in COPD research and had an average working experience of 20 years in the respiratory field and met the selection criteria.
Delphi First Survey Results
In the first survey, there was consensus on 13 of the 27 closed ended questions. Theme-wise results for each of the four concepts are presented below.
Exacerbation Reduction
All participants (100% participants) reached consensus that a history of exacerbations is an important predictor of future exacerbations and can help identify patients appropriate to receive triple therapy. No consensus was reached (62% of participants agreed) on the statement that SITT is more effective than MITT for reducing the risk of exacerbations. Only 29% of participants agreed that patients with COPD identify and report exacerbations in a timely manner to doctors, failing to reach consensus (Figure 1a). Sixteen of the 21 participants and 20 of 21 participants were of the opinion that triple therapy can be initiated in patients with COPD who have had one severe exacerbation and 1–2 moderate exacerbations in the past 12 months, respectively (Figure 1b).
 |
Figure 1 Survey 1 responses on exacerbation reduction concept and number of exacerbations for triple therapy initiation. Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. Notes: (a) Overall responses on exacerbation reduction concept (Survey 1). (b) Number of moderate and severe exacerbation for initiation of triple therapy (Survey 1). |
Early Optimization
SITT was considered a treatment option for patients with COPD with a high blood eosinophil count by 95% of participants. Furthermore, 86% of participants agreed that initiating SITT within 30 days of hospital discharge post an exacerbation of COPD can help reduce healthcare costs and the risk of future exacerbations. The participants did not agree that SITT can be considered treatment of choice for symptomatic patients without history of previous exacerbations (only 33% participants agreed) (Figure 2a); 48% participants believed that a blood eosinophil count of 150 cells/µL was high, while 29% believed a count of 300 cells/µL to be high (Figure 2b). All participants agreed that patients with COPD experiencing frequent exacerbations in the previous year would benefit from early treatment with SITT. The experts did not agree that elderly population (38% participants agreed), and patients with a higher degree of dyspnea with cough and sputum (62% participants agreed) were target population for early initiation of triple therapy (Figure 2c).
 |
Figure 2 Survey 1 responses on early optimization concept, blood eosinophil count and benefits of early triple therapy initiation. Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. Notes: (a) Overall responses on early optimization concept (Survey 1). (b) Responses on blood eosinophil count threshold (Survey 1). (c): Responses on patient population likely to benefit from early initiation of triple therapy (Survey 1). |
Pneumonia Risk
Eighty-one percent of participants agreed that there is similar degree of pneumonia risk while using SITT vs MITT and that the risk of pneumonia is ICS dose-dependent (Figure 3a). The participants also agreed regarding current smoking history (86% participants), history of prior exacerbation or pneumonia (90% participants), and severe airflow limitation (86% participants), as factors that increase and contribute to the risk of pneumonia. A consensus was not reached with respect to older age (≥55 years), body mass index (BMI) <25 kg/m2 and poor Medical Research Council (MRC) dyspnea grade being factors that contributed to risk of pneumonia. No consensus was reached on female gender (14% participants agreed) and concurrent statin therapy (10% participants agreed), as factors that contribute to the risk of pneumonia (Figure 3b).
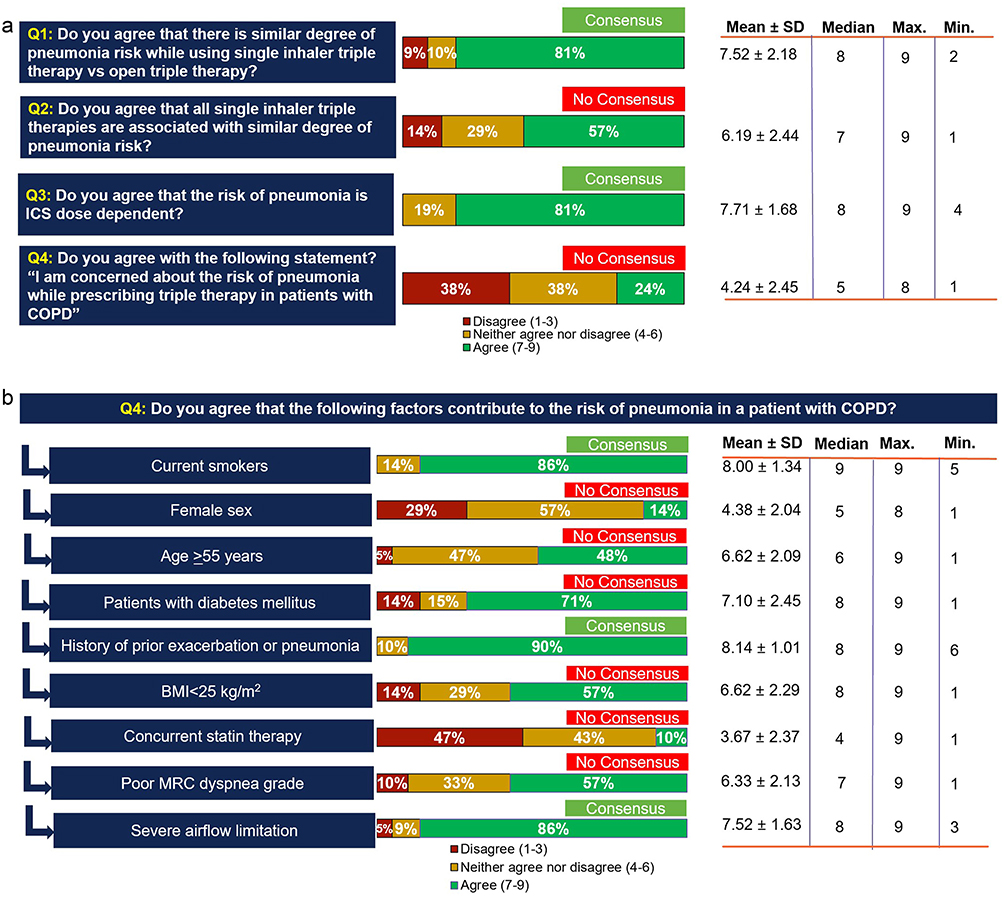 |
Figure 3 Survey 1 responses on pneumonia risk concept and risk factors for pneumonia. Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. Notes: (a) Overall responses on pneumonia risk concept (Survey 1). (b) Responses on factors contributing to risk of pneumonia (Survey 1). |
Mortality Benefits
A consensus was reached on all four questions related to mortality benefit statements with the use of triple therapy in patients with COPD. The most important risk factors for increased mortality in patients with COPD considered by experts were exacerbations, followed by COPD severity, behavioral, and pulmonary treatable traits (Table 1). There was agreement among the participants that SITT improves the survival of patients with COPD in comparison to LABA/LAMA based dual bronchodilator therapy (76% participants agreed). The importance of reducing the risk of mortality in clinical treatment decision-making achieved a consensus on consideration of the prescription of triple therapy (86% participants agreed). In addition, 76% of participants agreed that improvement in all-cause mortality described in the clinical studies was also seen in their real-life practice (Figure 4).
 |
Table 1 Baseline Characteristics of the COPD Patients That May Be the Risk Factors for Mortality (Mortality Benefit – Q5: What Baseline Characteristics of the COPD Patients Do You Think May Be the Risk Factors for Increased Mortality?) |
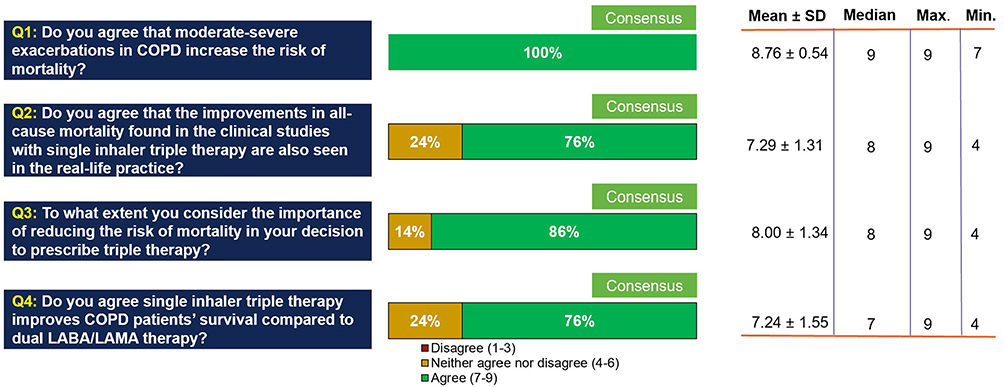 |
Figure 4 Overall responses on questions on mortality benefits concept (Survey 1). Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. |
Delphi Second Survey Results
Of the 27 questions, 14 questions that did not achieve consensus in the first survey were revisited in the second survey. In the second survey, four of the 14 questions reached consensus. Seventy-six percent of participants agreed that SITT is more effective than MITT in reducing the risk of exacerbations in patients with COPD. No consensus was reached where only 14% participants agreed that COPD patients identify and report exacerbations on time (Figure 5).
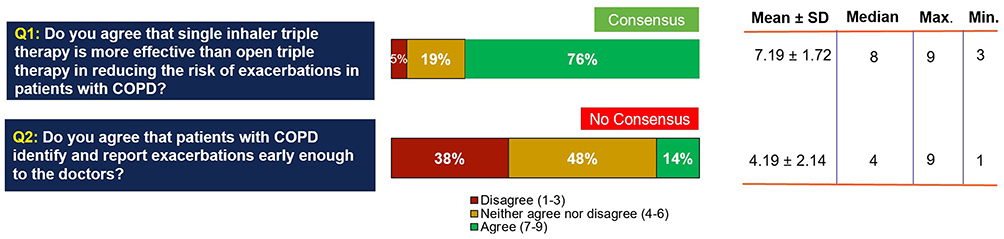 |
Figure 5 Overall responses on questions on exacerbation reduction concept (Survey 2). Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. |
No consensus was reached on the initiation of SITT as a first-line therapy in patients with COPD hospitalization due to exacerbation (62% participants agreed). The use of SITT as the treatment of choice for symptomatic COPD without an exacerbation history (19% participants agreed) did not achieve a consensus (Figure 6a). No consensus was reached on which patient population would benefit the most from early treatment with SITT instead of bronchodilators alone, with 33% participants reporting most benefit from SITT in elderly patients, and 62% participants reporting that patients with higher degree of dyspnea plus cough and sputum would benefit the most (Figure 6b).
 |
Figure 6 Survey 2 responses on early optimization concept and benefits of early triple therapy initiation. Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. Notes: (a): Overall responses on questions on early optimization concept (Survey 2). (b) Responses on patient population likely to benefit from early initiation of triple therapy (Survey 2). |
Nine percent of participants voted that they do not prescribe SITT due to the risk of pneumonia in patients with COPD, not reaching a consensus. The participants did not reach a consensus regarding the statement that all SITT are associated with a similar degree of pneumonia (67% participants agreed) (Figure 7a). There was agreement among the participants on the factors that contribute to the risk of pneumonia: diabetes mellitus (76% participants), older age (90% participants) and lower BMI (76% participants). No consensus was achieved on female gender and concurrent statin therapy as factors that contribute to the risk of pneumonia in the second round as well. Higher levels of dyspnea as a factor for early initiation of triple therapy (57% participants) failed to achieve consensus in this round of survey as well (Figure 7b).
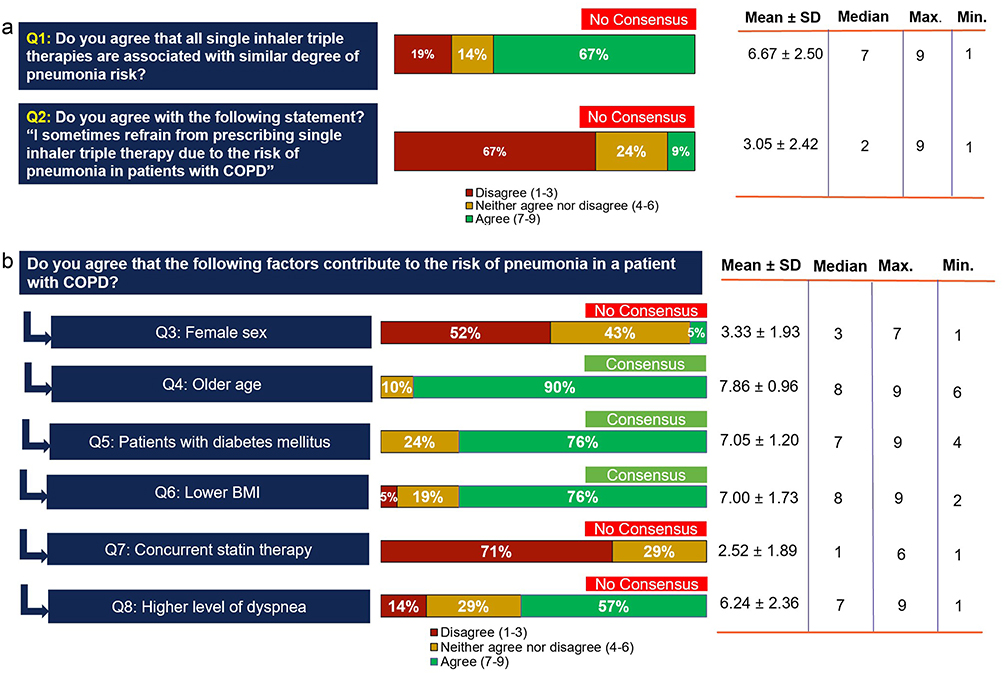 |
Figure 7 Survey 2 responses on pneumonia risk concept and risk factors for pneumonia. Abbreviations: COPD, chronic obstructive pulmonary disease; SD, standard deviation; Max, maximum; Min, minimum. Notes: (a) Overall responses on questions on pneumonia risk concept (Survey 2). (b) Responses on factors contributing to risk of pneumonia (Survey 2). |
Discussion
The aim of this Delphi study was to understand the consensus among respiratory experts regarding use of triple therapy for the management of patients with COPD with respect to exacerbation reduction, early optimization, pneumonia risk, and mortality benefits. The expert panel agreed on the benefits of triple therapy on mortality and exacerbation risk reduction, while further discussion is warranted on identifying the patient population most appropriate for triple therapy.
Exacerbations of COPD are under-reported by patients. According to studies conducted by Seemungal et al and Jones et al, almost half of all the exacerbations experienced by a patient are not reported to the doctor and have a negative impact on the health status of the patients with COPD similar to that of the exacerbation events that are reported.25,26 In this Delphi study, the respiratory experts were aligned that the patients are not always able to identify and report the exacerbations to the doctor on time. However, previous clinical and population-based studies have shown that a significant proportion of COPD patients initiating triple therapy do not meet the criteria regarding exacerbation history and prior maintenance therapy as per the GOLD recommendations.24,27,28 Based on the above discussion, one of the reasons for this could be the underreporting of exacerbations by patients with COPD. Early reporting of exacerbations may be influenced by factors such as age, and disease or exacerbation severity.29
A previous exacerbation is the strongest predictor of future occurrences.30,31 The experts in the current Delphi study agreed that exacerbation history is an important factor while considering a patient for triple therapy and that a previous history of exacerbation is a predictor for future exacerbations. According to data from the randomized controlled ETHOS trial and from a cohort study by Suissa et al, triple therapy is most beneficial in patients with more than one exacerbation in the past year, as compared with dual therapy.4,32 Two previous randomized trials showed comparable efficacy of SITT and MITT in reducing the risk of exacerbations.33,34 A recent Delphi study by Lopez-Campos et al also noted the agreement on triple therapy resulting in improvement in lung function and reduction in exacerbation risk in patients with COPD.35 A consensus was reached in the current Delphi study regarding triple therapy being more beneficial compared to dual therapy in frequent exacerbators and with SITT being considered more effective than MITT in reducing exacerbations.
In a retrospective study, Bogart et al reported that prompt use of triple therapy may reduce subsequent exacerbations and future costs compared with delaying the initiation of triple therapy in patients with COPD, who experienced a severe exacerbation.36 Mannino et al also reported that a lower rate of exacerbations was observed in the patients who received prompt triple therapy after being discharged from a severe exacerbation, compared with delayed initiation of triple therapy.37 Consistent with the evidence, the participants in the current study agreed that initiation of SITT within 30 days of exacerbation related hospitalization can reduce health care costs and future exacerbation risk. Initiation of ICS based triple therapy was found to be dependent on multiple factors, such as exacerbations (frequency and severity), blood eosinophil count, and a history of asthma or pneumonia as noted by Miravitlles et al.38 Pascoe et al showed that regimens containing ICS (dual or triple therapy) can more effectively control COPD exacerbations in patients with higher blood eosinophil counts. Blood eosinophil counts can be an important biomarker for identifying patients who can benefit from early optimization to triple therapy. There is a continuous gradation of the preventive effect of ICS in patients with eosinophil values between 100 and 300 cells/µL, so some patients are likely to get benefit from adding ICS.39 Most of the experts in the current Delphi study agreed that a blood eosinophil count of ≥150 cells/µL can be considered high in patients with COPD. There was no agreement among the participants regarding the population most likely to benefit from SITT instead of bronchodilator alone especially for use of SITT as a first-line therapy after hospitalization or a hospital visit due to an exacerbation resulting in first diagnosis of COPD.
According to a Cochrane review and an assessment report published by the European Medicines Agency, pneumonia is likely an ICS-related condition.40,41 This correlation of ICS dose and pneumonia risk was agreed by the participants of this study. The current study further highlights that risk of pneumonia is perceived as similar when using SITT vs MITT and that all SITT combinations have similar pneumonia risk since this is an ICS-class effect. Participants also confirmed that they do not refrain from prescribing SITT in the appropriate patients with COPD due to the fear of a risk of pneumonia. Hartley et al and Williams et al have noted that in addition to ICS use, the risk of pneumonia is increased by multiple factors, such as low BMI, a history of exacerbations, worsening lung function, and comorbidities such as ischemic heart disease.42,43 Bourbeau et al note that the benefits of SITT outweigh the pneumonia risk attributable to ICS component of triple therapy.44 Experts were in agreement that current smoking history, older age, history of diabetes mellitus, a history of previous exacerbations or pneumonia, lower BMI and severe airflow obstruction contribute to the risk of pneumonia in a patient with COPD.
Mortality benefit was deemed to be one of the most important outcomes for new initiation or stepping up to triple therapy for an appropriate patient profile, as noted in the consensus achieved in the first survey. The consensus is consistent with the data from the IMPACT study where a statistically significant reduction in the risk of all-cause mortality in patients treated with fluticasone furoate/umeclidinium bromide/vilanterol versus umeclidinium bromide/vilanterol was reported.5 The ETHOS study found that BGF 320 microgram was associated with a decreased risk of death when compared to glycopyrrolate/formoterol fumarate (GFF) dual therapy.4 SITT was also associated with significant reductions in the risk of 12-month all-cause mortality rate when compared to MITT in a real-world observational study (2.9% vs 4.4%, respectively).14 It is important to note that studies showing a survival effect with triple therapy were conducted in severe patients with frequent exacerbations, but no significant effect on mortality of triple versus dual bronchodilation has been observed in milder or non-exacerbating patients.45 The GOLD 2023 strategy recommends triple therapy to reduce the risk of mortality.1 The expert consensus aligns with the recommendation, even though the surveys were conducted prior to the release of the 2023 version.
The Delphi method has been frequently used for reaching consensus through expert opinions in scenarios of uncertainty or dichotomous evidence or situations with a lack of adequate evidence or standard guidelines.19,20,46–48 Strengths of this study include the high response rates of the expert panel and their engagement in the topic, demonstrated by high participant meeting attendance and 100% response to both the surveys with no dropouts in the second survey. Another strength of this study is the diverse scientific expertise in COPD management brought by 21 experts from 10 countries who were recruited for the study. Previous Delphi studies conducted in asthma and COPD suggest that a panel of 12 experts or more is sufficient to reach a meaningful consensus.19,49 The use of an independent facilitator and anonymous supervised feedback ensured the robustness of the process.
There are certain limitations to our study. The study focused on opinions of respiratory experts specializing in COPD management who have a certain leadership role and may not be representative of non-specialist physicians involved in COPD treatment. Another limitation is that the results of the Delphi study can be considered expert opinions; and other expert panels may not reach the same conclusions. Additionally, the participating experts involved in the present study were from countries in Near East and South America where both SITT and MITT were available at the time of the study, providing geographic validity but also room for bias in the findings of this Delphi. Further, the result obtained from this study has a temporal validity as it may change over time, and participant views were not unanimous on all questions. As a result, these findings should be interpreted rationally, and recommendations need to be further complemented to clarify the areas of uncertainty detected in the results.
Conclusion
Consensus was reached on many of the key concepts related to triple therapy use in COPD such as reduction in risk of COPD exacerbations, benefits of early optimization in appropriate patients and pneumonia risks associated with it and the mortality benefits. This shows the robustness of the clinical data of triple therapy in these aspects and the consistency seen in clinical experience. Overall, it appears that SITT is rapidly becoming an important treatment modality for the treatment of patients with COPD as it reduces exacerbation rate, improves all-cause mortality, and potentially could result in improved adherence. Many of the outcomes of this study are in line with the recent GOLD 2023 report update, even though the study was conducted prior to the release of the strategy document. Further research is required to address the questions where there was no consensus reached but that are equally clinically important for appropriate decision making in the management of patients with COPD.
Abbreviations
COPD, chronic obstructive pulmonary disease; SITT, single inhaler triple therapy; LAMA, long-acting muscarinic antagonist; LABA, long-acting β2-agonist; ICS, inhaled corticosteroid; GOLD, global initiative for chronic obstructive lung disease; GeSPOC, Spanish Chronic Obstructive Pulmonary Disease Guidelines; MITT, multiple inhaler triple therapy; OD, once daily; BID, twice daily; BGF, budesonide/glycopyrronium bromide/formoterol fumarate; GDPR, General Data Protection Regulation; BHBIA, British Healthcare Business Intelligence Association; EPhMRA, European Pharmaceutical Market Research Association; MRC, Medical Research Council; BMI, body mass index; GFF, glycopyrrolate/formoterol fumarate; BFF, budesonide/formoterol fumarate.
Data Sharing Statement
All relevant data underlying this article are available in the article and in its online Supplementary Materials.
Acknowledgments
The authors would like to thank the experts who participated in the Delphi process to express their degree of agreement with the statements: Al Busaidi N, Alejandro Casas, Andrea Colli Dominguez, Arjun Khanna, Arturo Cortes, Carlos Andrés Celis Preciado, Diego Litewka, Irma de Godoy, Karen Czischke, Mahmoud Mokhtar, Mohamed Alghobain, Naparat Amornputtisathaporn, Olga Milena García Morales, Rafael Hernandez Centeno, Sana S Almutairi, Tomás Alvarez.
Editorial support was provided by EVERSANA and was funded by GSK.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GSK. Meetings, data analysis, and medical writing assistance were funded by GSK.
Disclosure
Marc Miravitlles has received speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GSK, Menarini, Kamada, Takeda, Zambon, CSL Behring, Specialty Therapeutics, Janssen, Grifols and Novartis, consulting fees from AstraZeneca, Atriva Therapeutics, Boehringer Ingelheim, Chiesi, GSK, CSL Behring, Inhibrx, Ferrer, Menarini, Mereo Biopharma, Spin Therapeutics, Specialty Therapeutics, ONO Pharma, Palobiofarma SL, Takeda, Novartis, Novo Nordisk, Sanofi, Zambon and Grifols and research grants from Grifols. Sudeep Acharya is an employee of GSK and holds shares in GSK. Bhumika Aggarwal is an employee of GSK and holds shares in GSK. Frederico LA Fernandes has received consulting fees from GSK, Chiesi, AstraZeneca, Zambon, Abbott and Boehringer Ingelheim and speaker fees from Abbott, GSK, ACHE, AstraZeneca, Novartis, Zambon and Boehringer Ingelheim. Jorge Dreyse Dañobeitía has received grants from Boehringer Ingelheim and AstraZeneca and consulting and speaker fees from GSK. José R. Jardim has received grants from GSK and speaker fees from Zambon, Grifols and GSK. Siwasak Juthong declares no conflicts of interest in this work. Gur Levy is an employee of GSK and holds shares in GSK. Martin Sivori has received speaker fees from AstraZeneca, TEVA, ELEA and GSK. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis and management of COPD: 2023 report. Global Initiative for Chronic Obstructive Lung Disease; 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
2. Miravitlles M, Kawayama T, Dreher M. LABA/LAMA as first-line therapy for COPD: a summary of the evidence and guideline recommendations. J Clin Med. 2022;11(22):6623. doi:10.3390/jcm11226623
3. Miravitlles M, Calle M, Molina J, et al. Spanish COPD Guidelines (GesEPOC) 2021: updated pharmacological treatment of stable COPD. Arch Bronconeumol. 2022;58(1):69–81. doi:10.1016/j.arbres.2021.03.005
4. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. A randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/rccm.202006-2618OC
5. Lipson DA, Crim C, Criner GJ, et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. doi:10.1164/rccm.201911-2207OC
6. Lai CC, Chen CH, Chen KH, et al. The impact of 52-week single inhaler device triple therapy versus dual therapy on the mortality of COPD patients: a systematic review and meta-analysis of randomized controlled trials. Life. 2022;12(2):173. doi:10.3390/life12020173
7. Maltais F, Mahler DA, Pepin V, et al. Effect of fluticasone propionate/salmeterol plus tiotropium versus tiotropium on walking endurance in COPD. Eur Respir J. 2013;42(2):539–541. doi:10.1183/09031936.00074113
8. Lee SD, Xie CM, Yunus F, et al. Efficacy and tolerability of budesonide/formoterol added to tiotropium compared with tiotropium alone in patients with severe or very severe COPD: a randomized, multicentre study in East Asia. Respirology. 2016;21(1):119–127. doi:10.1111/resp.12646
9. Jung KS, Park HY, Park SY, et al. Korean academy of tuberculosis and respiratory diseases study group; Korea chronic obstructive pulmonary disease study group. Comparison of tiotropium plus fluticasone propionate/salmeterol with tiotropium in COPD: a randomized controlled study. Respir Med. 2012;106(3):382–389. doi:10.1016/j.rmed.2011.09.004
10. Miravitlles M, Marín A, Huerta A, Carcedo D, Villacampa A, Puig-Junoy J. Estimation of the clinical and economic impact of an improvement in adherence based on the use of once-daily single-inhaler triple therapy in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:1643–1654. doi:10.2147/COPD.S253567
11. Yu AP, Guérin A, Ponce de Leon D, et al. Therapy persistence and adherence in patients with chronic obstructive pulmonary disease: multiple versus single long-acting maintenance inhalers. J Med Econ. 2011;14(4):486–496. doi:10.3111/13696998.2011.594123
12. Zhang S, King D, Rosen VM, Ismaila AS. Impact of single combination inhaler versus multiple inhalers to deliver the same medications for patients with asthma or COPD: a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:417–438. doi:10.2147/COPD.S234823
13. Malerba M, Nardin M, Santini G, Mores N, Radaeli A, Montuschi P. Single-inhaler triple therapy utilizing the once-daily combination of fluticasone furoate, umeclidinium and vilanterol in the management of COPD: the current evidence base and future prospects. Ther Adv Respir Dis. 2018;12:1753466618760779. doi:10.1177/1753466618760779
14. Alcázar-Navarrete B, Jamart L, Sánchez-Covisa J, Juárez M, Graefenhain R, Sicras-Mainar A. Clinical characteristics, treatment persistence, and outcomes among patients with COPD treated with single- or multiple-inhaler triple therapy: a retrospective analysis in Spain. Chest. 2022;162(5):1017–1029. doi:10.1016/j.chest.2022.06.033
15. Calverley PMA, Magnussen H, Miravitlles M, Wedzicha JA. Triple therapy in COPD: what we know and what we don’t. COPD. 2017;14(6):648–662. doi:10.1080/15412555.2017.1389875
16. Cazzola M, Rogliani P, Laitano R, Calzetta L, Matera MG. Beyond dual bronchodilation - triple therapy, when and why. Int J Chron Obstruct Pulmon Dis. 2022;17:165–180. doi:10.2147/COPD.S345263
17. Suissa S, Dell’Aniello S, Ernst P. Triple inhaler versus dual bronchodilator therapy in COPD: real-world effectiveness on mortality. COPD. 2022;19(1):1–9. doi:10.1080/15412555.2021.1977789
18. Sriprasart T, Siasoco MB, Aggarwal B, et al. The role of modeling studies in asthma management and clinical decision-making: a Delphi survey of physician knowledge and perceptions. J Asthma. 2023;7:1–15. doi:10.1080/02770903.2023.2180748
19. Domingo C, Garcia G, Gemicioglu B, et al. Consensus on mild asthma management: results of a modified Delphi study. J Asthma. 2023;60(1):145–157. doi:10.1080/02770903.2022.2034850
20. Miravitlles M, Soler-Cataluña JJ, Alcázar B, Viejo JL, García-Río F. Factors affecting the selection of an inhaler device for COPD and the ideal device for different patient profiles. Results of EPOCA Delphi consensus. Pulm Pharmacol Ther. 2018;48:97–103. doi:10.1016/j.pupt.2017.10.006
21. Beiderbeck D, Frevel N, von der Gracht HA, Schmidt SL, Schweitzer VM. Preparing, conducting, and analyzing Delphi surveys: cross-disciplinary practices, new directions, and advancements. MethodsX. 2021;8:101401. doi:10.1016/j.mex.2021.101401
22. Alcázar Navarrete B, Casanova C, Miravitlles M, de Lucas P, Riesco JA, Rodríguez González-Moro JM; Working Group “Consensus document on the appropriate use of inhaled corticosteroids in COPD”. ”Correct use of inhaled corticosteroids in chronic obstructive pulmonary disease”: a consensus document. Arch Bronconeumol. 2015;51(4):193–198. doi:10.1016/j.arbres.2014.11.001
23. Traversi L, Miravitlles M, Martinez-Garcia MA, et al. ROSE: radiology, obstruction, symptoms, and exposure - A Delphi consensus definition of the association of COPD and bronchiectasis by the EMBARC airways working group. ERJ Open Res. 2021;7(4):00399–2021. doi:10.1183/23120541.00399-2021
24. Monteagudo M, Barrecheguren M, Solntseva I, et al. Clinical characteristics, and factors associated with triple therapy use in newly diagnosed patients with COPD. NPJ Prim Care Respir Med. 2021;31(1):16. doi:10.1038/s41533-021-00227-x
25. Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. doi:10.1164/ajrccm.157.5.9709032
26. Jones PW, Lamarca R, Chuecos F, et al. Characterisation, and impact of reported and unreported exacerbations: results from ATTAIN. Eur Respir J. 2014;44(5):1156–1165. doi:10.1183/09031936.00038814
27. Bhatt SP, Blauer-Peterson C, Buysman EK, Bengtson LGS, Paine Iii SR. Trends and characteristics of global initiative for chronic obstructive lung disease guidelines-Discordant prescribing of triple therapy among patients with COPD. Chronic Obstr Pulm Dis. 2022;9(2):135–153. doi:10.15326/jcopdf.2021.0256
28. Monteagudo M, Nuñez A, Solntseva I, et al. Treatment pathways before and after triple therapy in COPD: a population-based study in primary care in Spain. Arch Bronconeumol. 2021;57(3):205–213. doi:10.1016/j.arbres.2020.07.032
29. Langsetmo L, Platt RW, Ernst P, Bourbeau J. Underreporting exacerbation of chronic obstructive pulmonary disease in a longitudinal cohort. Am J Respir Crit Care Med. 2008;177(4):396–401. doi:10.1164/rccm.200708-1290OC
30. Hurst JR, Han MK, Singh B, et al. Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: a systematic literature review. Respir Res. 2022;23(1):213. doi:10.1186/s12931-022-02123-5
31. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
32. Suissa S, Dell’Aniello S, Ernst P. Comparative effects of LAMA-LABA-ICS vs LAMA-LABA for COPD: cohort study in real-world clinical practice. Chest. 2020;157(4):846–855. doi:10.1016/j.chest.2019.11.007
33. Vestbo J, Papi A, Corradi M, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet. 2017;389(10082):1919–1929. doi:10.1016/S0140-6736(17)30188-5
34. Salvi S, Balki A, Krishnamurthy S, et al. Efficacy, and safety of single-inhaler triple therapy of glycopyrronium, formoterol and fluticasone in patients with COPD: a double-blind, randomised controlled trial. ERJ Open Res. 2021;7(3):00255–2021. doi:10.1183/23120541.00255-2021
35. López-Campos JL, Alcázar Navarrete B, Riesco Miranda JA, et al. A Delphi consensus document on the use of single-inhaler fixed-dose triple therapies in COPD patients. Int J Chron Obstruct Pulmon Dis. 2020;15:1801–1811. doi:10.2147/COPD.S258818
36. Bogart M, Glassberg MB, Reinsch T, Stanford RH. Impact of prompt versus delayed initiation of triple therapy post COPD exacerbation in a US-managed care setting. Respir Med. 2018;145:138–144. doi:10.1016/j.rmed.2018.10.013
37. Mannino D, Bogart M, Germain G, et al. Benefit of prompt versus delayed use of single-inhaler fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) following a COPD exacerbation. Int J Chron Obstruct Pulmon Dis. 2022;17:491–504. doi:10.2147/COPD.S337668
38. Miravitlles M, González-Torralba F, Represas-Represas C, et al. Pulmonologists’ opinion on the use of inhaled corticosteroids in chronic obstructive pulmonary disease patients in Spain: a cross-sectional survey. Int J Chron Obstruct Pulmon Dis. 2022;17:1577–1587. doi:10.2147/COPD.S369118
39. Pascoe S, Barnes N, Brusselle G, et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med. 2019;7(9):745–756. doi:10.1016/S2213-2600(19)30190-0
40. Kew KM, Seniukovich A. Inhaled steroids, and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;2014(3):CD010115. doi:10.1002/14651858.CD010115.pub2
41. European Medicines Agency; Pharmacovigilance Risk Assessment Committee (PRAC). Inhaled corticosteroids (ICS) containing medicinal products indicated in the treatment of chronic obstructive pulmonary disease (COPD) assessment report. London, UK: European Medicines Agency; 2016. Available from: https://www.ema.europa.eu/documents/referral/inhaled-corticosteroids-article-31-referral-ema-completes-review-inhaled-corticosteroids-chronic_en.pdf.
42. Hartley BF, Barnes NC, Lettis S, Compton CH, Papi A, Jones P. Risk factors for exacerbations and pneumonia in patients with chronic obstructive pulmonary disease: a pooled analysis. Respir Res. 2020;21(1):5. doi:10.1186/s12931-019-1262-0
43. Williams NP, Coombs NA, Johnson MJ, et al. Seasonality, risk factors and burden of community-acquired pneumonia in COPD patients: a population database study using linked health care records. Int J Chron Obstruct Pulmon Dis. 2017;12:313–322. doi:10.2147/COPD.S121389
44. Bourbeau J, Bafadhel M, Barnes NC, et al. Benefit/risk profile of single-inhaler triple therapy in COPD. Int J Chron Obstruct Pulmon Dis. 2021;16:499–517. doi:10.2147/COPD.S291967
45. Miravitlles M, Verhamme K, Calverley PMA, et al. A pooled analysis of mortality in patients with COPD receiving dual bronchodilation with and without additional inhaled corticosteroid. Int J Chron Obstruct Pulmon Dis. 2022;17:545–558. doi:10.2147/COPD.S350167
46. Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One. 2011;6(6):e20476. doi:10.1371/journal.pone.0020476
47. Thompson M. Considering the implication of variations within Delphi research. Fam Pract. 2009;26(5):420–424. doi:10.1093/fampra/cmp051
48. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32(4):1008–1015.
49. Harding G, Leidy NK, Meddis D, Kleinman L, Wagner S, O’Brien CD. Interpreting clinical trial results of patient-perceived onset of effect in asthma: methods and results of a Delphi panel. Curr Med Res Opin. 2009;25(6):1563–1571. doi:10.1185/03007990902914403
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Adherence and Persistence of Single- and Multiple-Inhaler Triple Therapies Among Patients with Chronic Obstructive Pulmonary Disease in an English Real-World Primary Care Setting
Halpin DM, Rothnie KJ, Banks V, Czira A, Compton C, Wood R, Tritton T, Massey O, Wild R, Snowise N, Nikitin K, Sharma R, Ismaila AS, Vogelmeier CF
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2417-2429
Published Date: 24 September 2022
Characteristics of Users and New Initiators of Single- and Multiple-Inhaler Triple Therapy for Chronic Obstructive Pulmonary Disease in Germany
Beeh KM, Rothnie KJ, Claussen J, Hardtstock F, Knapp RK, Wilke T, Czira A, Compton C, Ismaila AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:945-956
Published Date: 17 April 2024
Preserved Ratio Impaired Spirometry in US Primary Care Patients Diagnosed with Chronic Obstructive Pulmonary Disease
Evans A, Tarabichi Y, Pace WD, Make B, Bushell N, Carter V, Chang KL, Fox C, Han MK, Kaplan A, Kocks JWH, Le Lievre C, Roussos A, Skolnik N, Soriano JB, Yawn BP, Price D
Pragmatic and Observational Research 2024, 15:221-232
Published Date: 13 December 2024