Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 15
Clinical Characteristics, Prognostic Risk Factors, and Primary Treatment for Elderly Patients with Primary Central Nervous System Lymphoma: A Seer Database-Based Research
Authors Zhang M, Yang R, Du Y, Feng H, Liu Y, Liu H, Wu D, Niu F, He P ![]()
Received 19 March 2025
Accepted for publication 28 June 2025
Published 7 July 2025 Volume 2025:15 Pages 85—101
DOI https://doi.org/10.2147/BLCTT.S529249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Wilson Gonsalves
Mengyao Zhang,* Runyu Yang,* Yue Du,* Hui Feng, Yi Liu, Haibo Liu, Di Wu, Fan Niu, Pengcheng He
Department of Hematology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China, Xi’an, Shaanxi, 710061, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fan Niu, Department of Hematology, First Affiliated Hospital of Xi’an Jiaotong University, No. 277 Yanta West Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Email [email protected] Pengcheng He, Department of Hematology, First Affiliated Hospital of Xi’an Jiaotong University, No. 277 Yanta West Road, Xi’an, Shaanxi, 710061, People’s Republic of China, Email [email protected]
Background: Primary central nervous system lymphoma (PCNSL) is a highly aggressive extranodal non-Hodgkin’s lymphoma. Moreover, there is currently no specific prognostic model for elderly PCNSL patients.
Methods: This study retrospectively selected patients diagnosed with PCNSL between 1975 and 2016 from the National Cancer Institute Surveillance, Epidemiology, and End Results Database (SEER NCI). The COX model was used to determine the risk factors for overall survival (OS) and disease-specific survival (DSS). The prognostic prediction models for DSS and OS were developed by integrating significant covariates identified through multivariate analysis.
Results: A total of 3,554 patients with PCNSL were included in this retrospective study based on inclusion and exclusion criteria. Significant differences exist in clinical profiles between elderly (≥ 60 years) and younger (< 60 years) patients with PCNSL. The results showed that the age at diagnosis, pathological subtype, whether or not they have undergone surgical treatment, and whether or not they have received chemotherapy are independent risk factors for DSS, among elderly PCNSL patients. In addition to the risk factors, etc for DSS, human immunodeficiency virus (HIV) infection was also an independent risk factor for OS. Based on this, we developed nomograms to estimate OS and DSS for 1, 2, and 3 years.
Conclusion: This study found differences in baseline data between elderly PCNSL patients and younger PCNSL patients. Surgery and chemotherapy are associated with better OS and DSS. However, in the long run, radiotherapy is not beneficial to OS and DSS of elderly PCNSL patients.
Keywords: primary central nervous system lymphoma, elderly patients, prognostic risk factors, SEER database, primary treatment
Introduction
Primary central nervous system lymphoma (PCNSL) is a highly aggressive extranodal non-Hodgkin’s lymphoma confined to the central nervous system.1 At present, PCNSL accounts for about 1% of non-Hodgkin’s lymphoma (NHL) and 3% of all primary brain tumors.2,3 PCNSL mainly involves the brain, brainstem, eye, or spinal cord. To date, no systemic symptoms associated with PCNSL have been documented in clinical observations.4 The clinical symptoms of PCNSL mainly depend on the primary site of the lesion. The most common symptom of PCNSL is focal neurological symptoms, which are observed in approximately 70% of patients. About half of the patients have neuropsychiatric symptoms. This was followed by increased intracranial pressure signs and ocular symptoms.5 The majority of cases (over 90%) are diffuse large B-cell lymphoma (DLBCL).6
This highly aggressive disease occurs mainly in the elderly patients. Multiple European or American cohorts have reported a median onset age of 60 to 70 years in patients with PCNSL.2,7 At the same time, Eloranta et al8 conducted statistics on the incidence of PCNSL in Sweden from 2000 to 2013, and found that the incidence of PCNSL increased in the population over the age of 70. PCNSL patients usually have a poor prognosis, and the overall survival (OS) of patients without proper treatment is only 1.5 months.9 High-dose methotrexate (HD-MTX) remains the cornerstone of all therapeutic regimens. However, the best treatment currently available for patients with PCNSL is still controversial. The determination of the specific chemotherapy regimen and whether surgery and radiation contribute to the patient’s prognosis remain inconclusive.10
The International Extranodal Lymphoma Study Group 32 (IELSG32), an international randomized Phase 2 trial, addressed two key clinical questions through its dual randomizations:11 First, for PCNSL patients aged ≤70 years, the combination induction therapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) yielded significantly superior outcomes.12 Second, both WBRT and ASCT proved feasible and effective as consolidation therapies following high-dose methotrexate-based induction.13 Furthermore, with a median follow-up of 88 months,14 the trial demonstrated that MATRix was associated with excellent long-term outcomes, while WBRT and ASCT showed comparable efficacy. However, WBRT was associated with impairments in attention and executive function, whereas ASCT led to improvements in these functions, along with memory and quality of life. Over the past four decades, novel therapeutic agents—including rituximab and Bruton’s tyrosine kinase (BTK) inhibitors such as Ibrutinib15,16 —have demonstrated significant therapeutic activity in the management of relapsed/refractory central nervous system lymphoma and vitreoretinal lymphoma. Ibrutinib plays a central role in PCNSL treatment by targeting the B-cell receptor (BCR) signaling pathway. Its mechanisms encompass inducing tumor cell apoptosis, inhibiting tumor proliferation, and penetrating the blood-brain barrier, among others.16 Furthermore, although the efficacy of rituximab in PCNSL remains controversial, existing clinical evidence indicates that adding rituximab to the HD-MTX plus high-dose cytarabine (HD-AraC) regimen significantly improves the 7-year overall survival rate in newly diagnosed patients.14
Despite therapeutic advances in recent decades, significant age-based disparities in treatment outcomes persist in PCNSL.17 This is possibly due to the intolerance to HD-MTX and hematopoietic stem cell transplantation of the elderly. Unfortunately, to date there remains a lack of evidence-based consensus on optimized therapeutic protocols specifically tailored for elderly PCNSL patients. Notably, there is no optimal model available to predict the prognosis and survival of elderly patients with PCNSL, and most clinicians only rely on their own clinical experiences for treatment. Moreover, due to the stringent admission requirements of randomized controlled clinical trials, the symptoms of enrolled patients will be modest, and it is more challenging to enroll older people with PCNSL. In brief, there is rarely prospective clinical trial for PCNSL in the elderly, limiting its clinical progression.
The Surveillance, Epidemiology, and End Results (SEER) Database from the National Institutes of Health’s National Cancer Institute (NCI) contains a wealth of information about patients diagnosed with diverse cancer types, offering valuable opportunities to investigate and assess prognostic indicators for these pathological conditions. Using SEER database, we analyzed elderly (≥60 years) PCNSL patients’ clinical profiles, prognostic factors, and treatment impacts. Through multivariable Cox regression, we developed and validated a geriatric-specific prognostic model incorporating OS/DSS predictors.
Materials and Methods
Data Sources and Data Filtering
The data screening and processing procedures in this study were shown in Figure 1. Patient data included in this study were downloaded from the National Institutes of Health NCI-SEER. The “ Incidence - SEER 18 Regs Custom Data (with additional treatment fields)” data set was selected for analysis using the SEER*Stat software (version 8.9.3). PCNSL was identified using the International Classification of Tumor Diseases (ICD-O-3) histological codes (9590–9595, 9670–9699, 9700–9719, 9720–9729) and primary sites localized to the central nervous system were identified using site-specific codes (C71.0-C71.9).18 Subsequently, we excluded some unqualified cases, including incomplete baseline information (Race = “Unknown ”, marital status at diagnosis =“ unknown ”), Unclear treatment protocol (Surg Prim site (1998+) = “Blank (s)” Radiation recode =”Recommended, unknown if administered) and incomplete follow-up records (Survival months = “Unknown”; Survival months =“0”; specific death classification = “Dead (missing/unknown COD)”). Finally, we obtained the data of a total of 3,554 patients with PCNSL. Elderly patients with PCNSL (n =2146) were randomized 7:3 into a training cohort (n = 1502) and a validation cohort (n = 644) for model construction and validation. The differences of each index between the training cohort and the verification cohort were not statistically significant (Table S1).
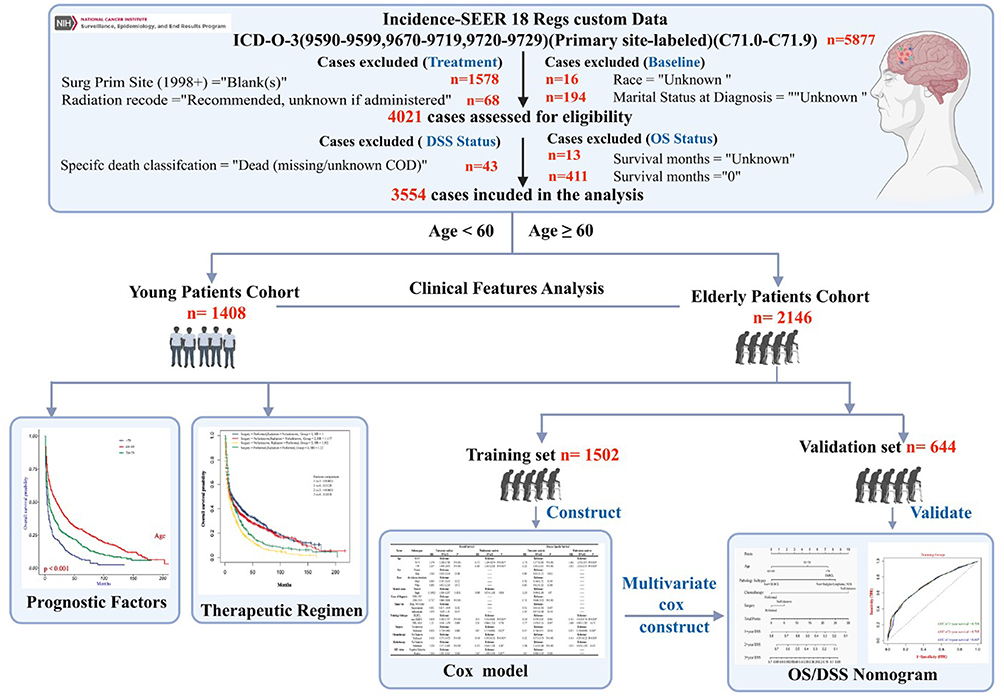 |
Figure 1 Data filtering and processing flow in SEER database. |
Variable Definition
Firstly, we collected patient baseline data and defined elderly patients as those were more than or equal to 60 years. Then we divided the age of elderly patients into three subgroups (60–69; 70–79; > 79), gender (male, female), race (the African Americans, White, other), and marital status (Married, Single). Single includes Divorced, Separated, Unmarried or Domestic Partner, and Widowed. The diagnosis included early diagnosis (1998–2007) and recent diagnosis (2008–2016). For disease-related status we collected the patient’s HIV (human immunodeficiency virus) infection status (negative, positive), the site of the tumor (Superior, infratentorial, Brain, NOS/Other), and the pathological subtypes of the tumor (Diffuse large B-cell lymphoma (DLBCL), Non-DLBCL, Non-Hodgkin lymphoma (NHL)). Non-DLBCL mainly includes Mantle cell lymphoma, Burkitt lymphoma, Follicular lymphoma, Peripheral T-cell lymphoma, NOS, Anaplastic Large Cell Lymphoma, etc. Finally, we analyzed the patient’s treatment plan, and separately marked the operation, chemotherapy, and radiotherapy as “Performed, No/unknown”.
Statistical Method
The clinical characteristics of elderly patients were compared with those of younger patients using the Pearson χ 2 tests. This study selected Overall Survival (OS) and Disease-Specific Survival (DSS) as the primary endpoints. OS is defined as the time from randomization to death due to any cause, while DSS specifically refers to deaths attributed to the studied disease (deaths from other causes were excluded). OS and DSS were analyzed using the Kaplan-Meier method via the R-package “Survival” (Version 3.2–13) and “survminer (version 0.4.9)” and compared via the Log rank test. The risk factors for OS and DSS were determined using the COX regression model in elderly PCNSL patients, and univariate and multivariate survival analyses were performed. Based on the significant results of multivariate Cox regression analysis, nomograms were constructed to predict the OS and DSS of PCNSL at 1, 2, and 3 years. The R-package “SurvivalROC” (Version 1.0.3) was used to plot the ROC curve of the prediction model for 1, 2, and 3 years. Calibration curves for nomograms were also plotted using the R-package “rms” (Version 6.3–0) to determine if the predicted survival rate was consistent with the actual survival rate. The study used R language (version 4.1.1) for data statistics and analysis. Bilateral p-values < 0.05 were considered statistically significant.
Results
Clinical Characteristics of PCNSL
This retrospective study included data of 3,554 patients with PCNSL from SEER database, according to the inclusion and exclusion criteria. We divide them into elderly patients (≥60 years old) and young patients (<60 years old) based on their ages. There are 2,146 in the elderly patient’s cohort and 1,408 in the young patient’s cohort.
Firstly, to get an overall characteristic of elderly PCNSL patients, we analyzed and compared the epidemiology and treatment plan of elderly PCNSL patient’s cohort and young patient’s cohort (Table 1). The results demonstrated that, apart from age, significant differences were observed between the elderly and younger cohorts in gender, race, marital status, year of diagnosis, pathological subtypes, receipt of chemotherapy, and HIV status. More precisely, compared with young PCNSL patients, the proportion of female, married, and white in elderly PCNSL patients was higher. Of the total PCNSL HIV-positive patients (n. 204), 5.9% were elderly and 94.1% were young (94.1%). At the same time, the pathological types of more elderly patients with PCNSL are mainly DLBCL. Compared with young patients, the treatment scheme for elderly patients seems more conservative: 74.1% of young PCNSL patients received chemotherapy, while 67.5% of elderly patients received chemotherapy (P < 0.001). In terms of radiotherapy, we observed the same phenomenon. 41.4% of young PCNSL patients received radiotherapy, while only 33.9% of elderly PCNSL patients received radiotherapy (P < 0.001). However, no statistically significant difference in surgical intervention was observed between the two age groups. In order to further analyze and show the differences between treatment methods of elderly patients with PCNSL, we further analyzed and compared the data of chemotherapy and radiotherapy among different age subgroups of elderly patients (≥60 y). Figure S1 shows a statistically significant decrease in the number of patients receiving chemotherapy as they age. At the same time, there was no significant difference in the proportion of patients receiving radiotherapy between the different age subgroups.
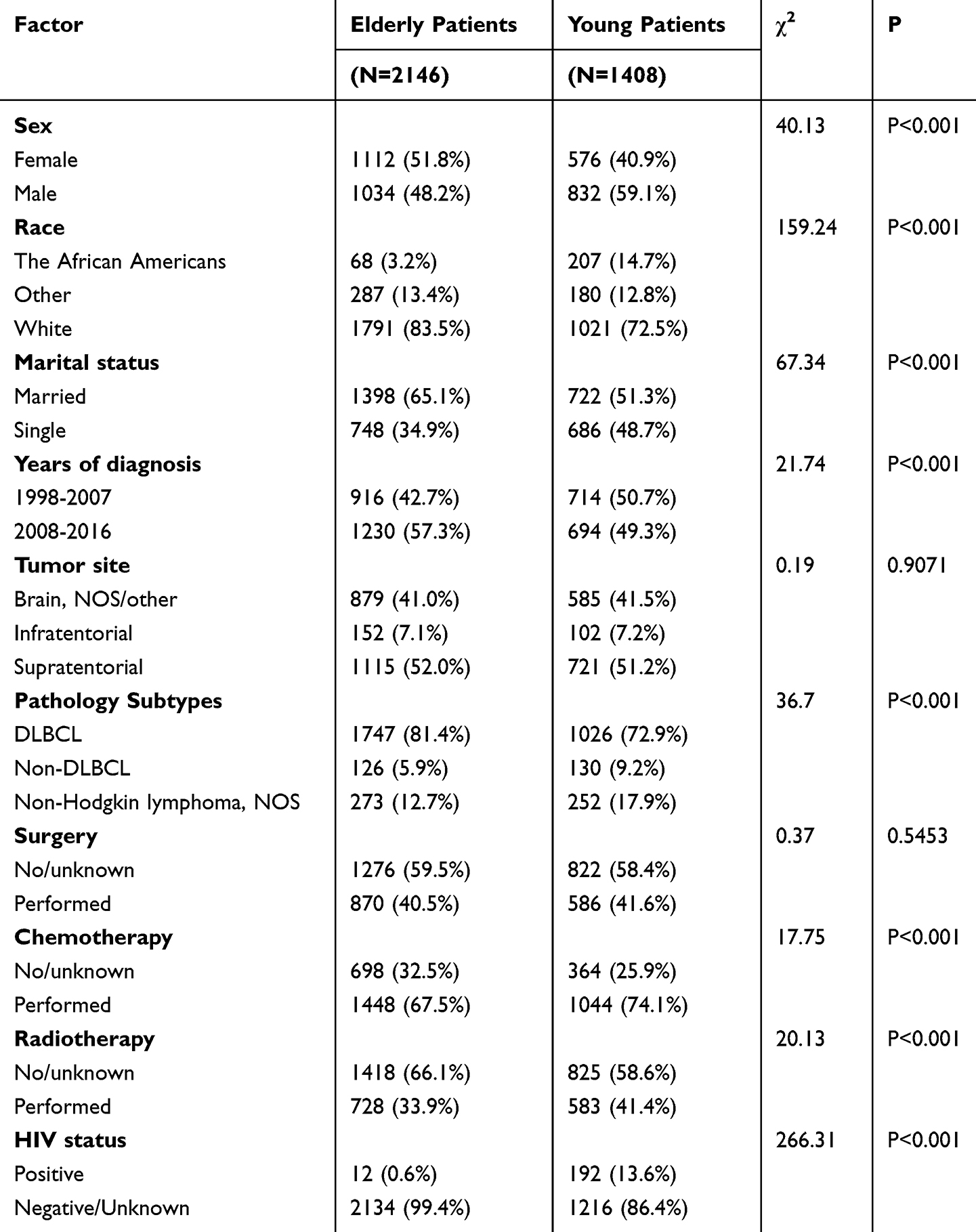 |
Table 1 Comparison of Clinical Data Between Elderly (≥60 years Old) Patients with Primary Central Nervous System Lymphoma and Young (<60 years Old) Patients with Primary Central Nervous System Lymphoma |
Prognostic Factors of Elderly Patients with PCNSL
To further investigate the survival, as well as the risk factors of elderly PCNSL patients, we subsequently analyzed the survival data of 2146 elderly patients cohort (median OS: 5 months). The results revealed a progressive decline in both OS and DSS with advancing age among elderly patients with PCNSL. And single patients at the time of diagnosis often had worse OS and DSS (P < 0.01) (Figure 2A and B). The OS and DSS of elderly patients with PCNSL diagnosed in recent years (2008–2016) were better than those diagnosed in the early years (1998–2007) (P < 0.001) (Figure 2A and B). Kaplan-Meier survival curves of disease-related factors are shown in Figure 2C and D. Results indicated that NHL patients notably DLBCL patients have a worse OS and DSS than non-DLBCL. We further classified the existing clinical data according to whether it was invasive or not. They can be divided into four categories: Aggressive B−cell NHL, indolent B−cell NHL, NHL−NOS, and T−cell NHL. To further describe the effect of detailed pathological types on prognosis, we analyzed the relationship between pathological subtypes and prognosis. Figure S2 shows that patients with pathological type of indolent B−cell NHL had better OS and DSS. Meanwhile, patients with Supratentorial tumor had poor DSS (P = 0.044), but there was no significant difference in OS (P=0.069) (Figure 2C and D). HIV-positive status is a risk factor for OS in elderly patients with PCNSL (P=0.008), but there is no significant difference for DSS (P=0.43). In addition, Figure S3 also showed there is no significant difference in terms of OS (A) and DSS (B) of elderly PCNSL patients between ethnic groups and gender.
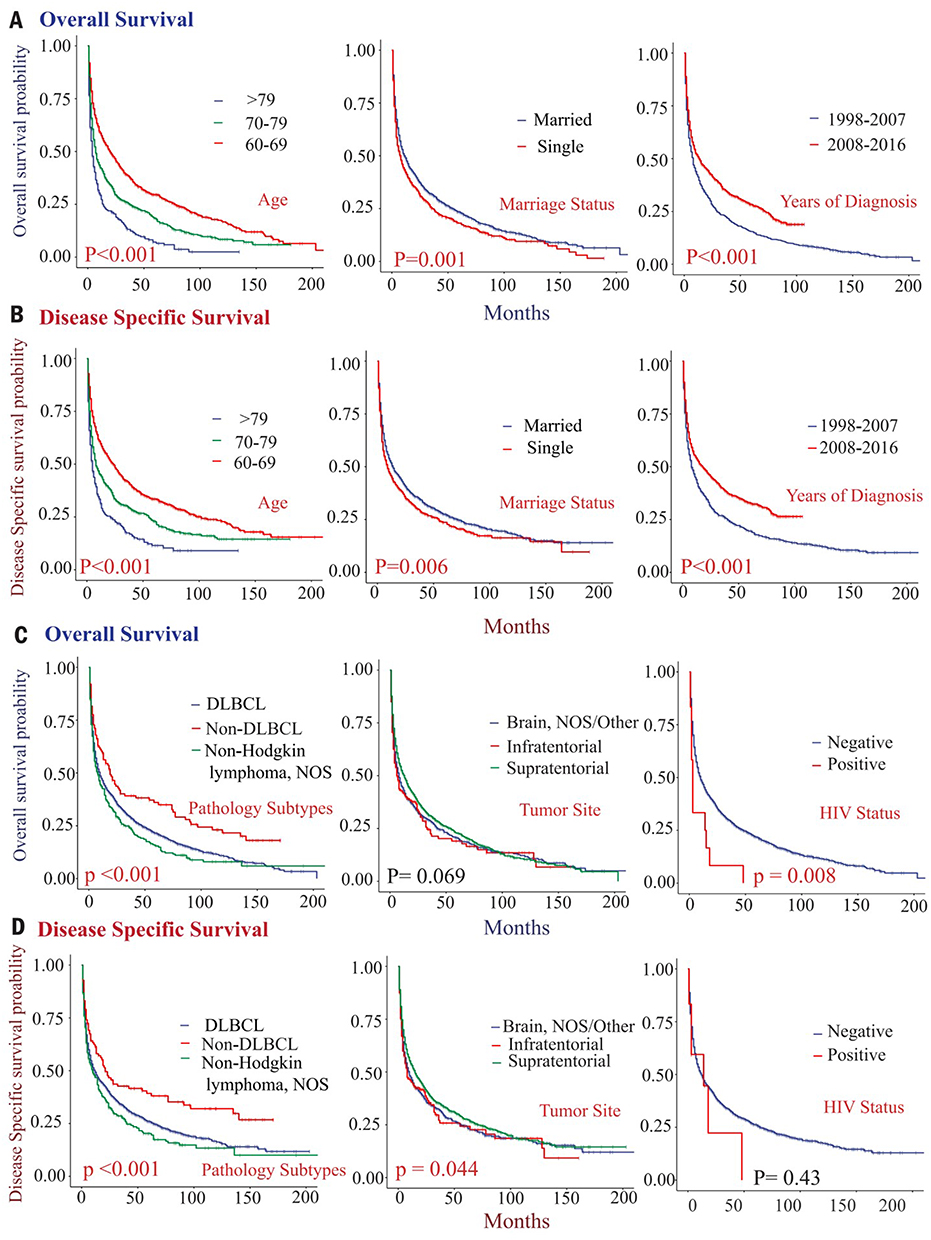 |
Figure 2 Survival analysis of elderly (≥60 years) patients with primary central nervous system lymphoma stratified by epidemiological and disease-related data. (A) Overall survival (OS) of elderly patients stratified by age (left), marital status (middle), and year of diagnosis (right); (B) Disease-specific survival (DSS) of elderly patients stratified by age (left), marital status (middle), and year of diagnosis (right); (C) Overall survival (OS) of elderly patients stratified by histological type (left), tumor location (middle), and HIV status (right); (D) Disease-specific survival (DSS) of elderly patients stratified by age (left), marital status (middle), and year of diagnosis (right). |
Effect of Therapeutic Regimen on Prognosis of Elderly Patients with PCNSL
To investigate the effect of therapeutic regimens on prognosis of elderly PCNSL patients, we subsequently compared the effects of surgery, chemotherapy and radiation on the prognosis of patients. We found that patients who received chemotherapy or surgical resection had a significant better OS and DSS than the not performed or unknown group. However, radiation resulted in worse OS and DSS (P < 0.05) (Figure 3A and B). In order to further analyze and demonstrate the impact of different surgical approaches on the prognosis of elderly patients with PCNSL, we further analyzed and compared the data between subgroups of elderly patients receiving different surgical approaches. According to the guidelines provided by the SEER database, we can further divide the surgical approach into the following 5 parts: gross total resection GTR, Lobectomy, partial lobectomy, subtotal detection STR, and No/unknown. Figure S2 shows that patients who have undergone Lobectomy have good OS and DSS.
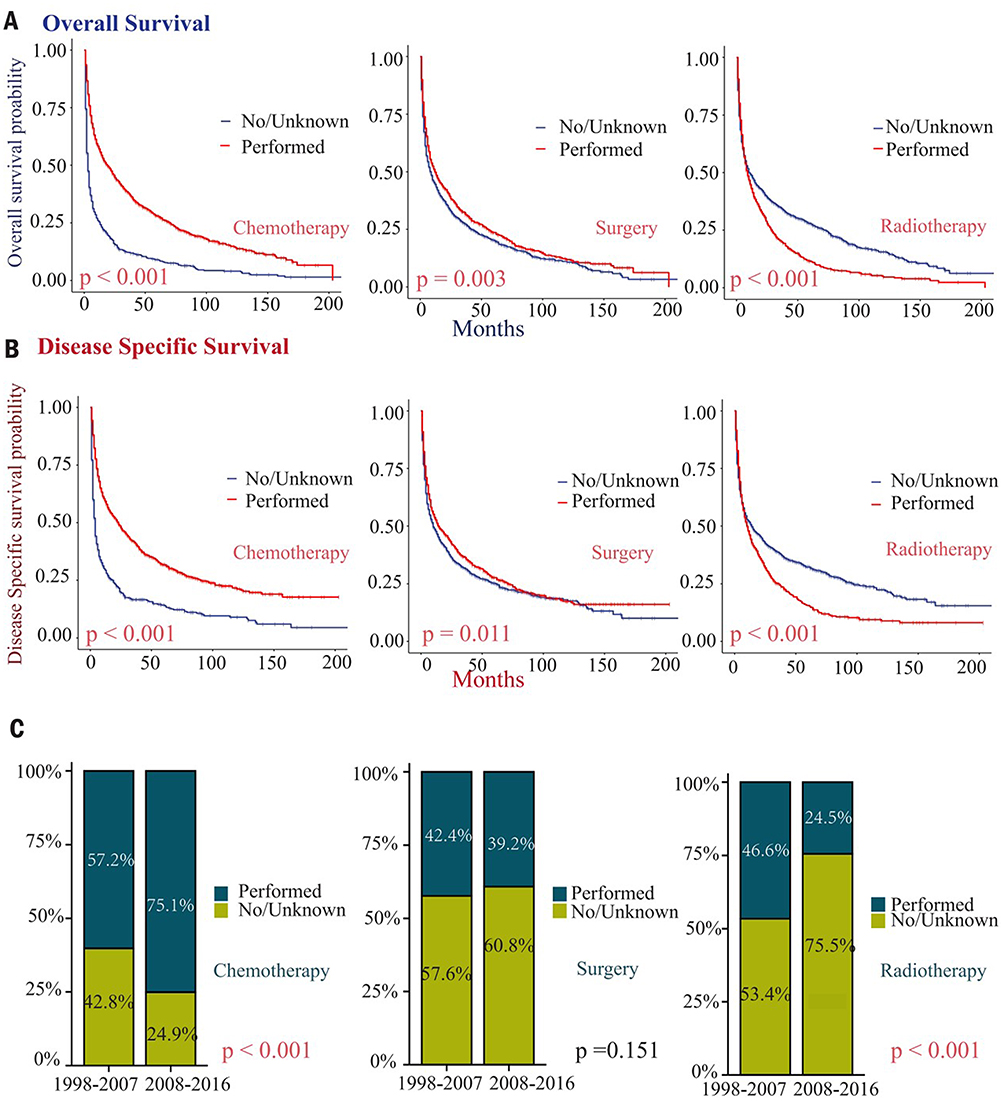 |
Figure 3 Survival analysis of treatment-stratified elderly patients (≥60 years) with primary central nervous system lymphoma. (A) Overall survival (OS) of elderly patients stratified by chemotherapy status (with vs without, left), surgical status (with vs without, middle), and radiotherapy status (with vs without, right); (B) Disease-specific survival (DSS) of elderly patients stratified by chemotherapy status (with vs without, left), surgical status (with vs without, middle), and radiotherapy status (with vs without, right); (C) The difference in the proportion of elderly patients (≥60 years old) with PCNSL between different stages and different treatment options. |
Treatment options for elderly patients with PCNSL diagnosed in early years (between 1998 and 2007) and recent years (between 2008 and 2016) were also analyzed. The results showed that the proportion of patients diagnosed in the early years receiving chemotherapy (57.2%) was significantly lower than those diagnosed in recent years (75.1%). Meanwhile, the proportion of patients diagnosed in the early years receiving radiation (46.6%) is significantly higher than that of patients diagnosed in recent years (24.5%). However, the proportion of patients diagnosed in the early years receiving surgery is not different from that of patients diagnosed in recent years (Figure 3C and Table S2).
We also explored the effects of combination therapy. The results of the chemotherapy combined with radiation or surgery group showed that chemotherapy was beneficial for the OS in elderly patients with PCNSL (Figure 4A and B). The effect of surgical resection on the patient’s OS cannot be completely determined (Figure 4B and C). However, elderly patients with PCNSL who have a radiation regimen in combination therapy tend to have poorer OS (Figure 4A–C).
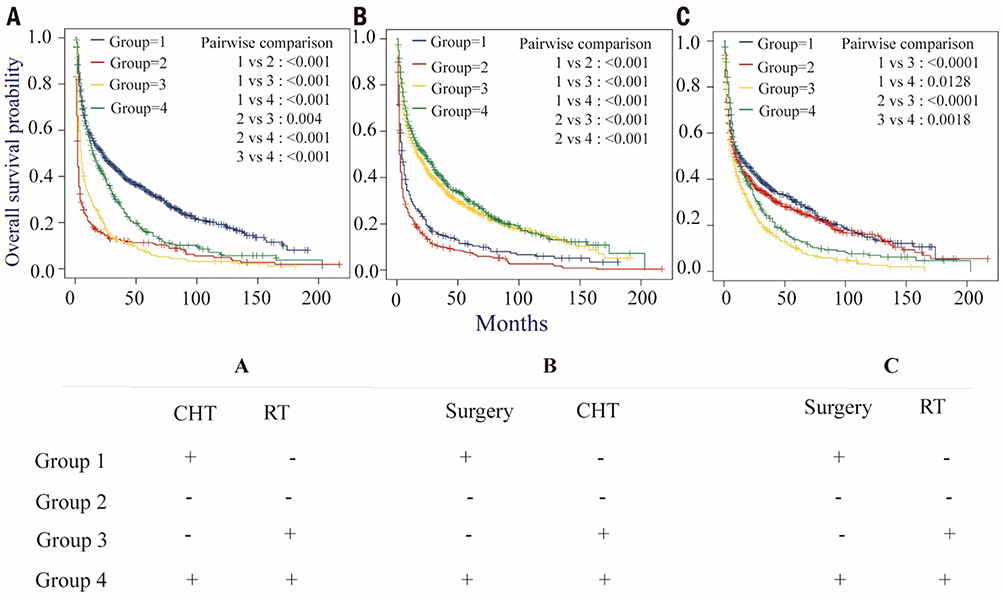 |
Figure 4 Two-factor analysis of primary central nervous system lymphoma in the elderly (≥60 years). (A) Chemotherapy and radiotherapy: Group 1 is Chemotherapy = Performed and Radiation = No/unknown, HR = 1; Group 2 is Chemotherapy = No/unknown and Radiation = No/unknown, HR = 2.883; Group 3 is Chemotherapy = No/unknown and Radiation = Performed, HR = 2.248; Group 4 is Chemotherapy = Performed and Radiation = Performed, HR = 1.305. (B) Chemotherapy and surgery: Group 1 is Surgery = Performed and Chemotherapy = No/unknown, HR = 1; Group 2 is Surgery = No/unknown and Chemotherapy = No/unknown, HR = 1.358; Group 3 is Surgery = No/unknown and Chemotherapy = Performed, HR = 0.531; Group 4 is Surgery = Performed and Chemotherapy = Performed, HR = 0.485. (C) Surgery and radiotherapy: Group 1 is Surgery = Performed and Radiation = No/unknown, HR = 1; Group 2 is Surgery = No/unknown and Radiation = No/unknown, HR = 1.117; Group 3 is Surgery = No/unknown and Radiation = Performed, HR = 1.562; Group 4 is Surgery = Performed and Radiation = Performed, HR = 1.22. |
Construction of Clinical Prognosis Prediction Model for Elderly Patients with PCNSL
To better predict the prognosis of elderly PCNSL patients, we constructed a clinical prognosis model on the basis of the SEER data. Through analysis, we definitively identified independent prognostic factors for both OS and DSS. The results showed that for the elderly patients with PCNSL, the age at the time of diagnosis, the pathological subtype, whether or not they have received surgical treatment, and whether or not they have received chemotherapy were the independent risk factors for DSS. In addition to the risk factors for DSS (Table 2), whether or not they were infected with HIV was also the independent risk factor for OS (Table 3).
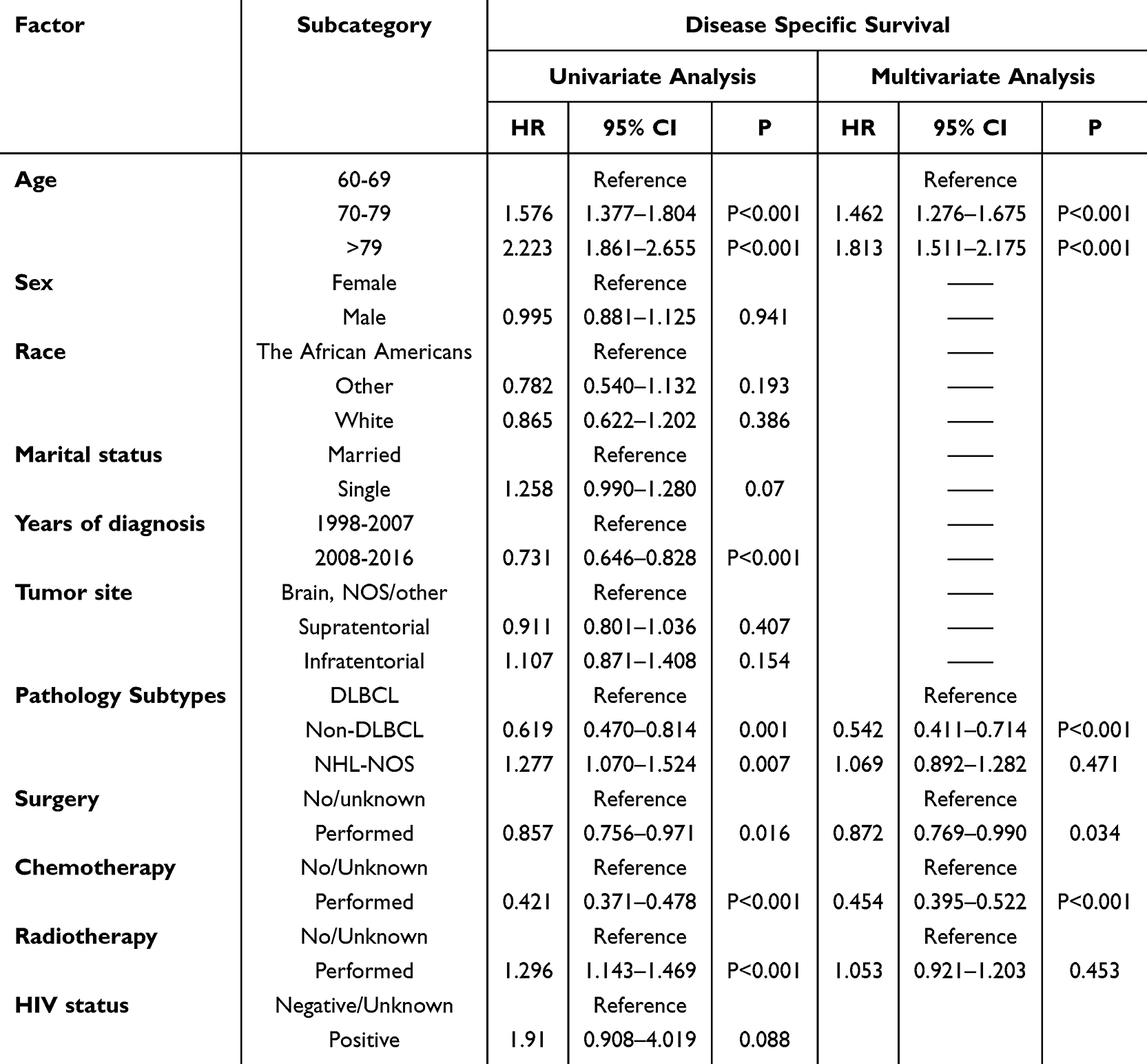 |
Table 2 Univariate and Multivariate Analysis of Clinical Data Associated with Disease-Specific Survival (DSS) in Elderly (≥60 Years) |
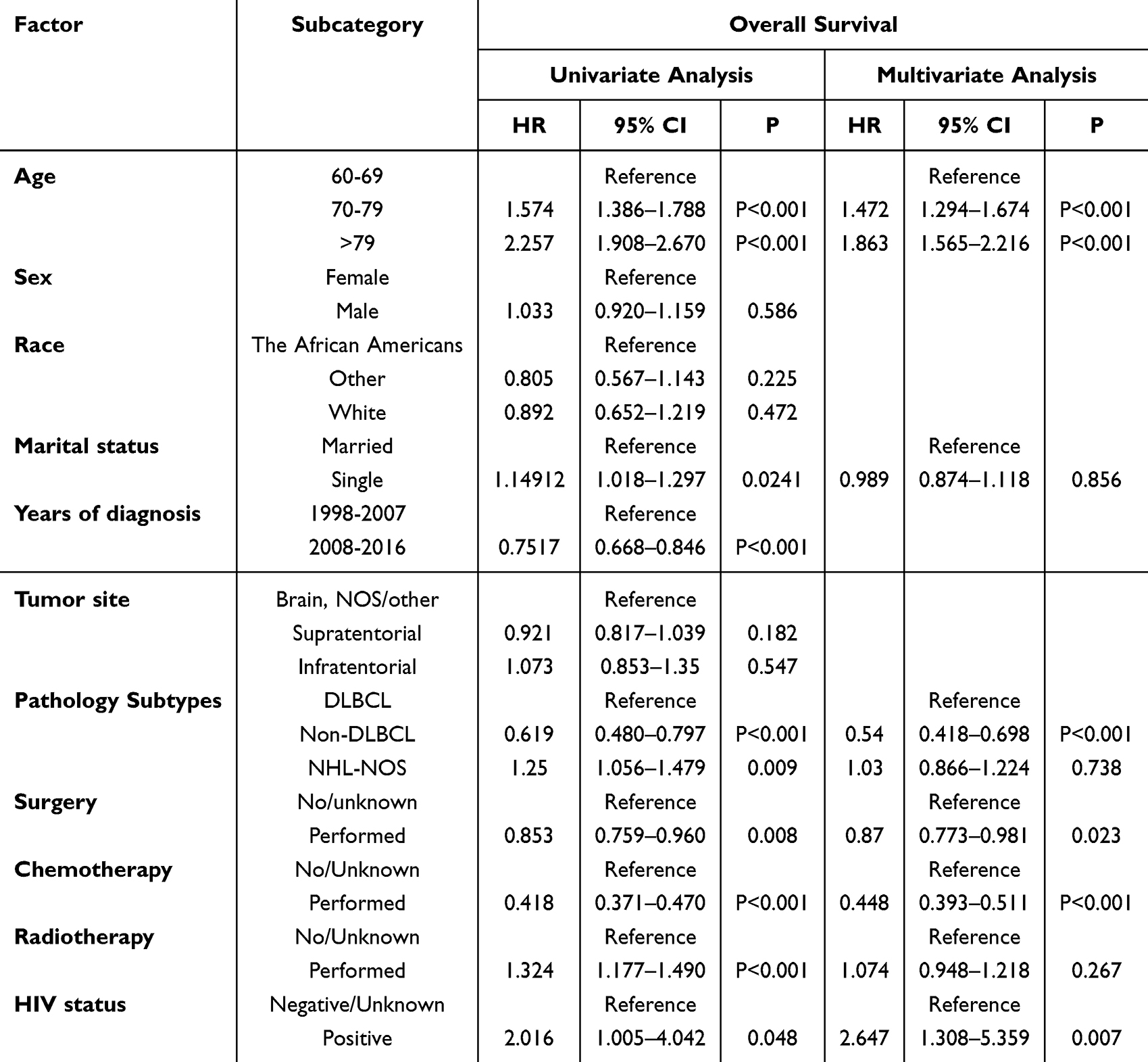 |
Table 3 Univariate and Multivariate Analysis of Clinical Data Associated with Overall Survival (OS) in Elderly (≥60 Years) |
Based on the results of multivariate Cox regression analysis, we developed a nomogram model to predict OS and DSS in elderly patients with PCNSL. As shown in Figure 5A, the 1-, 2-, and 3- years OS of elderly PCNSL patients can be predicted by integrating factors such as age, tumor pathological type, presence or absence of chemotherapy, HIV concomitant status, and presence or absence of surgery. At the same time, we tested the predictive ability and robustness of the nomogram models of OS in elderly patients with PCNSL. The time-dependent ROC curve showed that for OS prediction in elderly PCNSL, the AUC values under the ROC curve at 1-year, 2-years and 3-years survival are 0.702, 0.709 and 0.705, respectively (Figure 5B). At the same time, the calibration curve (Figure 5C) also shows a good consistency between the predicted survival rate and the actual survival rate at 1, 2, and 3 years.
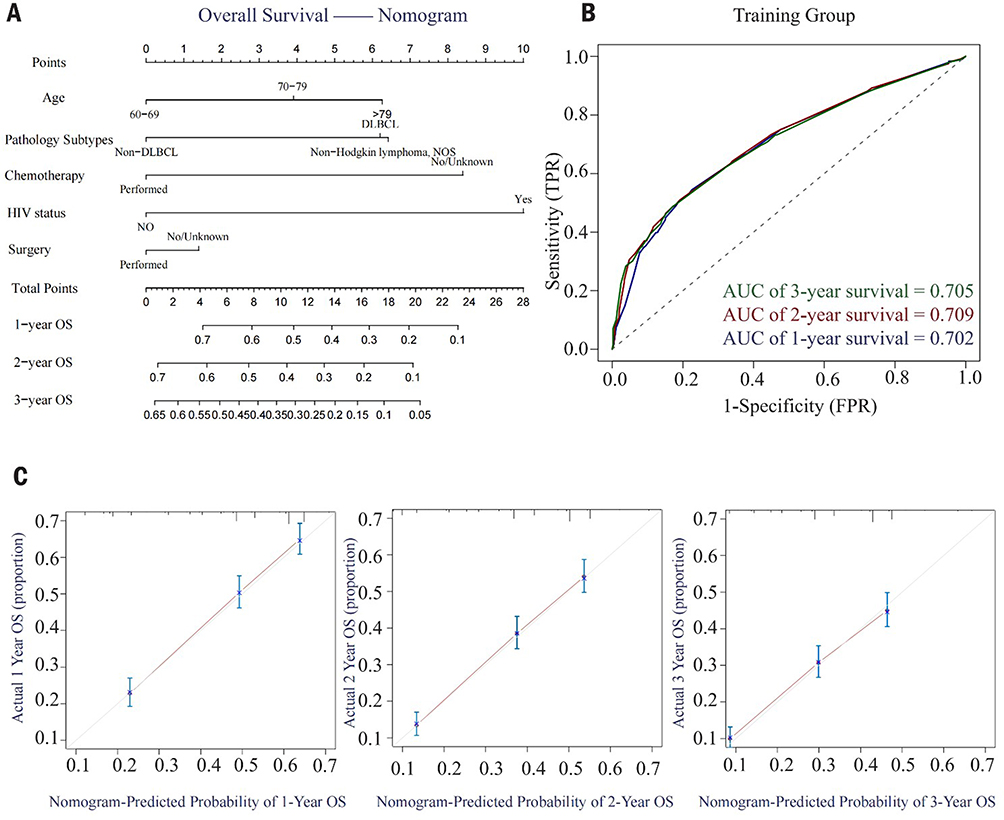 |
Figure 5 Establishment of overall survival (OS) model for the elderly (≥60 years) with primary central nervous system lymphoma. (A) The nomogram is predicting the overall survival (OS) of elderly patients (≥60 years) with primary central nervous system lymphoma at 1, 2, and 3 years; (B) Time-dependent ROC curve for total survival (OS) prognostic model: ROC curve of the 1-,2-and 3-year total survival (OS) prognostic model for elderly (≥60 years) patients with primary central nervous system lymphoma; (C) Calibration curves for the 1- (left), 2-(middle), and 3-(right) year overall survival (OS) nomograms. The abscissa represents the survival rate predicted by the nomogram, and the ordinate represents the actual survival rate. Notes: (A) is a nomogram, a tool used to visualize predictive models. It typically consists of a Variables Axis, Points Axis, Total Points Axis, and Outcome Axis. The method of reading the nomogram is as follows. First, locate the corresponding score for each predictor variable on the Points Axis. Next, sum the scores of all predictor variables to obtain the Total Points. Finally, convert the total points on the Outcome Axis to estimate the 1-, 2-, and 3-year survival rates. |
The 1-, 2, -and 3-year DSS of elderly patients with PCNSL can be predicted by integrating scores related to age, tumor pathological type, presence or absence of chemotherapy and operation, and projecting the total scores to the bottom scale (Figure 6A). For DSS prediction of elderly PCNSL patients, AUC values of 1-year, 2-years, and 3-years DSS are 0.697, 0.705, and 0.704, respectively (Figure 6B). The calibration curve (Figure 6C) also showed also a good consistency between the predicted survival rate and the actual survival rate, indicating that the prediction model has high prediction ability. Similar results are shown in the internal verification queue (Figure S4).
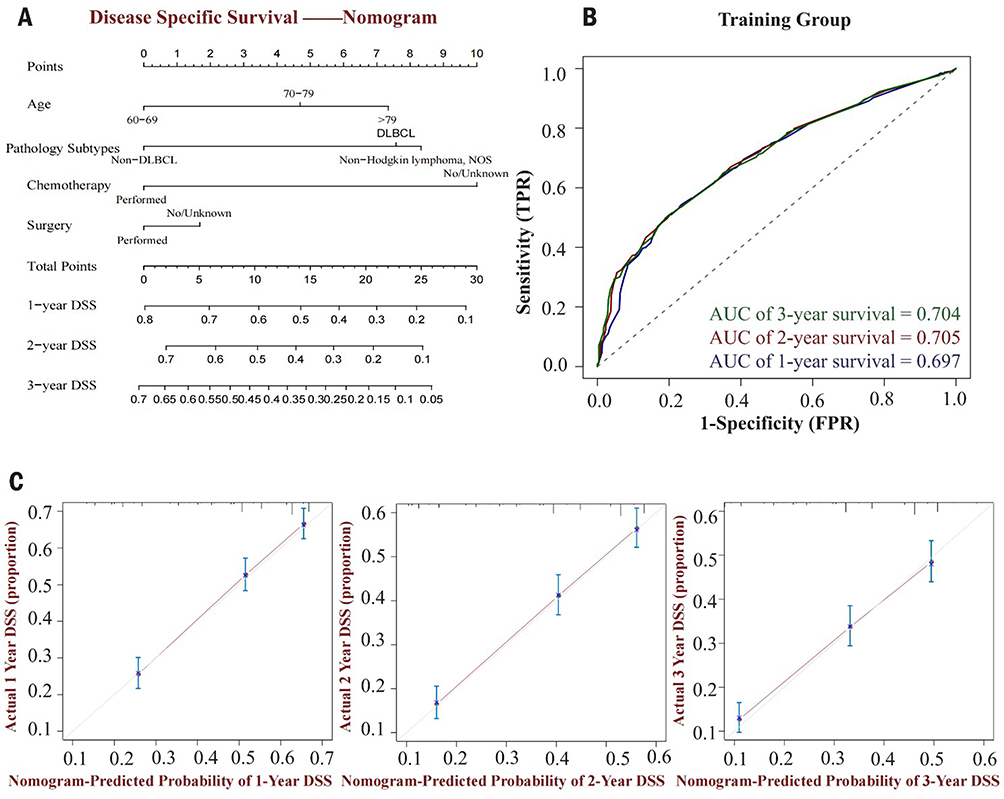 |
Figure 6 Establishment of disease-specific survival (DSS) model for predicting primary central nervous system lymphoma in the elderly (≥60 years). (A)The nomogram is predicting 1-,2-and 3-year disease-specific survival (DSS) in elderly patients (≥60 years) with primary central nervous system lymphoma; (B) Time-dependent ROC curve for disease-specific survival (DSS) prognosis model: ROC curve for the 1-,2-and 3-year disease-specific survival prognosis model for elderly (≥60 years) patients with primary central nervous system lymphoma; (C) Calibration curves for the 1- (left), 2-(middle), and 3-(right) year disease-specific survival (DSS) nomograms. The abscissa represents the survival rate predicted by the nomogram, and the ordinate represents the actual survival rate. |
Discussion
PCNSL is a highly aggressive extranodal NHL that primarily affects the elderly. Unfortunately, a retrospective review reveals that the prognosis for younger patients has considerably improved, whereas the prognosis for older patients remains inadequate.19 Multiple studies have consistently demonstrated that age and physical fitness are risk factors for PCNSL patients.10,20,21 Researchers developed a large number of prediction models for PCNSL, including the IELSG score22 developed by the International Study Group on Extranodal Lymphoma (IELSG), the MSKCC score constructed by Memorial Si Long-Kettering Cancer Center (MSKCC)23 and Nottingham/Barcelona (NB) score.24 Currently, the first two are widely used. The IELSG score identifies age (> 60 years), elevated serum lactate dehydrogenase (LDH) levels, physical status (PS) (≥2), high CSF protein concentrations and extensive deep structures involved in the brain are independent predictors of poor prognosis. The MSKCC score described the three risk groups based on age and Karnofsky performance status (KPS). Both emphasize the crucial role of age in the prognostic evaluation of PCNSL. However, none of the treatment-related information was included. At the same time, the above scoring system often cannot accurately predict the prognosis of patients with PCNSL.25 Moreover, as a distinct subgroup of the disease, the elderly lack examination of prognostic factors for large-scale data in this population. To the best of our knowledge, this work is the first to utilize the SEER database for prognostic analysis in elderly patients with PCNSL.
In this study, we investigated a total of 3,554 patients with PCNSL from the SEER database and documented the differences between elderly (≥60 years) and younger (<60 years) patients with PCNSL concerning multiple clinical variables. These findings not only illustrate the clinical differences between the two populations but also highlight the significance of the age subgroup study. In terms of clinical baseline characteristics, we discovered that the proportion of female, married, and Caucasian PCNSL patients in the elderly was greater than in the young PCNSL patient population. In disease-related aspects, the elderly patient group has a higher proportion of diffuse large B-cell subtypes and a lower HIV infection rate. This is congruent with the findings of a multi-center study conducted in the United States, which found that HIV-positive PCNSL patients are younger than HIV-negative PCNSL patients.26 Regarding therapeutic approaches, our findings align with previous studies indicating that elderly patients are more likely to receive conservative management or less intensive therapeutic regimens compared to the general patient population.27 This may be due to their physiological status and increased prevalence of comorbidities in elderly patients with PCNSL.28 More clinicians are concerned about the risk posed by treatment, and many treatment options exclude elderly individuals, contributing to the poor prognosis for elderly PCNSL patients. This urges us to pay close attention to the selection of treatment plans for elderly patients in the clinic, consider the patients’ tolerance to treatment more thoroughly, and optimize the management plans for the subgroup of elderly patients.
We also identified various independent prognostic factors in elderly patients with PCNSL. In terms of clinical baseline features, we discovered that age is a significant risk factor even in this subset of elderly PCNSL patients. Interestingly, our study reveals that PCNSL patients who are unaccompanied likely to have a poor prognosis. This is consistent with findings from previous studies.29 Multiple studies have demonstrated that marital status influences the prognosis of patients with multiple tumors (such as breast cancer, skin melanoma, and glioblastoma multiforme),30–32 which may be since married patients can receive better mental, financial support and physical care, making them more compliant with the treatment.
Concerning disease-related factors, we discovered that elderly patients with PCNSL who were infected with HIV had a poor OS, while HIV infection status was unrelated to DSS in elderly patients with PCNSL. According to a meta-analysis33 conducted in Italy, HIV infection was present in 6.1% of PCNSL patients, and Epstein-Barr virus (EBV) was discovered in the cerebrospinal fluid of the majority of HIV-infected patients. With the deepening understanding on PCNSL in recent years, researchers divided PCNSL patients into EBV-related type and EBV-negative type.34 The two subtypes exhibit distinct clinical characteristics. EBV-negative PCNSL shares features similar to the activated B-cell subtype, such as constitutive NF-ĸB activation. In contrast, EBV-associated PCNSL typically occurs in immunocompromised hosts, and these cases often have poor outcomes. In another study, some immunocompromised EBV-associated PCNSL cases were further subdivided based on the host’s HIV infection status into HIV-infected and HIV-uninfected subtypes.35 The results demonstrated that EBV-associated PCNSL without HIV infection exhibited resistance to the tumor microenvironment. Meanwhile, EBV-associated PCNSL with concurrent HIV infection showed low CD4+ T-cell counts, indicative of compromised immune function. These findings have revealed the complex clinical features of PCNSL under different disease states, which may provide a broad framework for targeted therapeutic strategies.
According to previous research, the prognosis of PCNSL patients with HIV infection is much poorer than that of PCNSL patients without HIV infection.36 We speculate that this may be due to the small number of cases included in this study, the eventual death of our patient from other diseases, and the fact that PCNSL patients with HIV-infected have taken antiretroviral therapy (ART) medications. As the majority of clinical studies on PCNSL have not provided precise data for reference on HIV infection in combination with PCNSL, large-scale prospective studies on elderly PCNSL patients with HIV infection are still required to determine the status of ART drugs in the treatment of elderly PCNSL patients with HIV infection and the impact mechanism of HIV infection on elderly PCNSL patients. In addition, we discovered that patients with supratentorial tumors and non-DLBCL tumors had a more favorable prognosis. Previous research has demonstrated the predictive significance of the primary site of PCNSL.37
The results of the study suggest that changes in treatment at different stages and the impact of treatment regimens on the prognosis of patients may explain the differences in the prognosis of elderly patients with PCNSL at different stages. In the early days, high-dose methotrexate combined with standard radiotherapy protocol was widely used in clinical practice. With a greater understanding of PCNSL, researchers discovered that although the tumor in this disease is highly sensitive to radiation, the long-term side effects of whole brain radiotherapy (WBRT), such as delayed neurotoxicity, negate the benefits of OS and DSS during radiation for elderly PCNSL patients.38 Central neurotoxicity may result in delayed progressive cognitive dysfunction, ataxia, and urinary incontinence, with typical features of leukoencephalopathy and brain atrophy on MRI scans. This central neurotoxicity tends to be more severe in older patients than in younger patients, resulting in irreversible dementia or lifelong bed rest, and previous studies indicate that this adverse effect occurs earlier in older patients than in younger patients.39 Since 2000, the classical method of whole-brain radiotherapy has been gradually phased out. The results of our research coincide with this conclusion. The results of Figure 4A clearly describe the conclusion that the prognosis of patients receiving radiotherapy alone is not as good as that of patients receiving radiotherapy and chemotherapy at the same time. However, it should be noted that the multivariate analysis results of radiotherapy as a prognostic factor are not statistically significant when establishing a prognostic model. Whether or not to receive radiotherapy still needs the support and proof of clinical data, such as large center randomized controlled trial. In our study, we also found that the proportion of patients diagnosed in early years treated with radiation was greater than that of patients diagnosed more recently. In recent years, researchers have attempted to reduce the WBRT radiation dose and frequency, but this has led to the corresponding recurrence of cancer.38
Additionally, this study reaffirms the value of chemotherapy as a long-standing first-line treatment. Higher MTX doses have been associated with improved survival outcomes.40 However, due to the poor physical function of the elderly, combined with a variety of diseases, and decreased tolerance to high-dose methotrexate, simple methotrexate treatment often cannot achieve good results. With the development of diagnosis and treatment, more elderly patients with PCNSL will choose many targeted therapies after receiving basic induction chemotherapy. Ibrutinib, as an inhibitor of BTK, has shown potent single-agent activity in relapsed/refractory CNS lymphoma. A clinical trial explored the efficacy of the combination of HD-MTX, rituximab, and Ibrutinib in patients with CNSL. The results showed that among the 9 patients with PCNSL, the CRR was 89% (8/9), and 6 of them (66.7%) achieved CR.41 As the third generation immunomodulator, pomalidomide (POM) has shown excellent permeability to the central nervous system and significant therapeutic activity against CNSL. A clinical study evaluated the efficacy of the combination of POM and dexamethasone (DEX) in the treatment of relapsed/refractory PCNSL and primary vitreoretinal lymphoma (PVRL). A total of 25 PCNSL patients were included in the trial, of which 72% were over the age of 60. The results showed that the Objective response rate (ORR) was 48% (12/25), the CR was 24% (6/25), and 11 patients finally died.42 In addition, the PD-1 inhibitor, nivolumab,43 and the mTOR selective inhibitor, Temsirolimus,44 have shown efficacy in elderly PCNSL patients. With the deepening understanding of the disease, autologous stem cell transplantation (ASCT) and targeted therapy may be a good option for elderly PCNSL patients.
The role of surgery in the treatment of elderly patients with PCNSL has always been uncertain, and various centres have frequently reached divergent conclusions. Jahr et al45 conducted a study on 79 patients with PCNSL and found that resection did not significantly improve OS or Progression-Free Survival (PFS) in patients with PCNSL. They only recommend cytoreductive surgery to improve patients’ clinical symptoms in the case of cerebral hernia. However, in a randomized controlled trial conducted in Germany among 526 PCNSL patients who received first-line treatment with HD-MTX in 2012, the PFS and OS of patients who only underwent biopsy were inferior to those who received surgical treatment.46 It should be noted that the results of this study indicated that elderly patients with PCNSL who underwent surgery had a favourable prognosis, contrary to what was previously believed about the role of surgery in elderly PCNSL. Traditionally, resection has been regarded as ineffective for significantly enhancing OS or PFS in patients with PCNSL due to the generally poorer physical condition of the elderly and the greater prevalence of other underlying diseases.45 Our study has yielded new ideas for the treatment of PCNSL in elderly patients based on the results of a study conducted on the general population. However, due to the characteristics of complex basic diseases of the elderly, a thorough evaluation of the tumor must be performed after its discovery so that the operation can be performed with a risk of postoperative defects and perioperative complications that is under control.47
Nonetheless, this study has limitations. The collection of SEER database data is restricted in some ways. First, the database only documents the incidence, mortality, and morbidity of millions of Americans with malignant tumors. Conclusions cannot provide comprehensive recommendations for the diagnosis and treatment of PCNSL patients in other countries. With such a large series, even small, clinically irrelevant differences can be statistically demonstrated. In addition, the data recorded in this database lacks numerous crucial details. For instance, the treatment plan only specifies whether or not the patient will undergo chemotherapy and radiotherapy; there is no specific chemotherapy and radiotherapy plan or dose. In particular, the term “NO” in the raw data is described together with “unkown”, which makes it impossible to distinguish between patients who have not undergone surgery/chemotherapy/radiotherapy and patients who do not know whether surgery/chemotherapy/radiotherapy has been performed. Patients’ prognosis follow-up includes only death and cause of death but no information on specific disease progression. Due to the low incidence of PCNSL, this study lacked an external, independent validation data set in addition to the database itself. Furthermore, inherent to the data collection characteristics of the SEER database, our study carries unavoidable methodological constraints in variable selection. For instance, physically frail elderly patients may demonstrate disparities in treatment regimens and clinical outcomes due to physiological intolerance - a confounding factor inherently associated with geriatric populations. However, given that this investigation specifically focuses on prognostic evaluation in elderly cohorts, certain residual confounding variables remain methodologically irreducible within the current research framework. These limitations warrant systematic evaluation in subsequent studies. Therefore, basic research and prospective trials are required for further diagnosis and treatment planning.
Conclusion
In this study, 3554 patients with PCNSL from SEER were analyzed, and it was found that there were differences in multiple baseline data between aged PCNSL patients and ordinary PCNSL patients. Surgery and chemotherapy were associated with better OS and DSS. In the long term, however, radiation was not beneficial for OS and DSS in elderly patients with PCNSL. Multivariate Cox regression analysis showed that for the elderly patients with PCNSL, the age at diagnosis, pathological subtype, whether or not they have received surgical treatment, and whether or not they have received chemotherapy are the independent risk factors for DSS. In addition to the risk factors for DSS, whether or not they are infected with HIV is also an independent risk factor for OS. Based on these findings, we developed a prognostic model to predict 1-, 2-, and 3-year OS and DSS. The model demonstrated high predictive accuracy upon validation.
Abbreviations
PCNSL, Primary central nervous system lymphoma; SEER NCI, National Cancer Institute Surveillance, Epidemiology, and End Results Database; OS, overall survival; DSS, disease-specific survival; NHL, non-Hodgkin’s lymphoma; DLBCL, diffuse large B-cell lymphoma; HD-MTX, High-dose methotrexate; BTK, Bruton Tyrosine Kinase; HIV, human immunodeficiency virus; IELSG, International Study Group on Extranodal Lymphoma; MSKCC, Memorial Sloan-Kettering Cancer Center; NB score, Nottingham/Barcelona score; LDH, lactate dehydrogenase; PS, physical status; KPS, Karnofsky performance status; EBV, Epstein-Barr virus; ART, antiretroviral therapy; WBRT, whole brain radiotherapy; POM, pomalidomide; DEX, dexamethasone; PVRL, primary vitreoretinal lymphoma.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
Based on Article 32(1)-(2) of the Ethical Review Measures for Life Sciences and Medical Research Involving Human Subjects issued by China on February 18, 2023, this study qualifies for exemption from ethical approval.
Author Contributions
Mengyao Zhang designed the research and actively wrote the manuscript. Runyu Yang performed and designed the research. Yue Du collected data. Yi Liu, Hui Feng, Haibo Liu and Di Wu assisted data analysis. Pengcheng He and Fan Niu supervised research and edited the paper. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was partially supported by the Key Research and Development Program of Shaanxi (NO. 2021ZDLSF02-17); the Key Research and Development Program in Shaanxi Province- General Projects- Social Development Field (NO.2021SF-302); the Key Research and Development Program of Shaanxi (NO.2018ZDCXL-SF-01-02-01).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. 2022;36:1720–1748. doi:10.1038/s41375-022-01620-2
2. Villano JL, Koshy M, Shaikh H, Dolecek TA, McCarthy BJ. Age, gender, and racial differences in incidence and survival in primary CNS lymphoma. Br J Cancer. 2011;105:1414–1418. doi:10.1038/bjc.2011.357
3. Hoffman S, Propp JM, McCarthy BJ. Temporal trends in incidence of primary brain tumors in the United States, 1985-1999. Neuro-Oncology. 2006;8:27–37. doi:10.1215/s1522851705000323
4. Holdhoff M, Mrugala MM, Grommes C, et al. Challenges in the treatment of newly diagnosed and recurrent primary central nervous system lymphoma. J Nat Compr Cancer Netw. 2020;18:1571–1578. doi:10.6004/jnccn.2020.7667
5. Aa M, Shah AH, Cavallo C, et al. Diagnosis of primary central nervous system lymphoma: a systematic review of the utility of CSF screening and the role of early brain biopsy. Neuro-Oncol Pract. 2019;6:415–423. doi:10.1093/nop/npz015
6. Deckert M, Engert A, Brück W, et al. Modern concepts in the biology, diagnosis, differential diagnosis and treatment of primary central nervous system lymphoma. Leukemia. 2011;25:1797–1807. doi:10.1038/leu.2011.169
7. van der Meulen M, Dinmohamed AG, Visser O, Doorduijn JK, Bromberg JEC. Improved survival in primary central nervous system lymphoma up to age 70 only: a population-based study on incidence, primary treatment and survival in the Netherlands, 1989-2015. Leukemia. 2017;31:1822–1825. doi:10.1038/leu.2017.128
8. Eloranta S, Brånvall E, Celsing F, et al. Increasing incidence of primary central nervous system lymphoma but no improvement in survival in Sweden 2000-2013. Eur J Haematol. 2018;100:61–68. doi:10.1111/ejh.12980
9. Lim T, Kim SJ, Kim K, et al. Primary CNS lymphoma other than DLBCL: a descriptive analysis of clinical features and treatment outcomes. Ann Hematol. 2011;90:1391–1398. doi:10.1007/s00277-011-1225-0
10. Grommes C, DeAngelis LM. Primary CNS Lymphoma. J Clin Oncol. 2017;35:2410–2418. doi:10.1200/jco.2017.72.7602
11. Ferreri AJ, Illerhaus G, Zucca E, Cavalli F. Flows and flaws in primary central nervous system lymphoma. Nat Rev Clin Oncol. 7. doi:10.1038/nrclinonc.2010.1039-c1031
12. Ferreri AJ, Cwynarski K, Pulczynski E, et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) phase 2 trial. Lancet Haematol. 2016;3:e217–227. doi:10.1016/s2352-3026(16)00036-3
13. Ferreri AJM, Cwynarski K, Pulczynski E, et al. Whole-brain radiotherapy or autologous stem-cell transplantation as consolidation strategies after high-dose methotrexate-based chemoimmunotherapy in patients with primary CNS lymphoma: results of the second randomisation of the international extranodal lymphoma study group-32 phase 2 trial. Lancet Haematol. 2017;4:e510–e523. doi:10.1016/s2352-3026(17)30174-6
14. Ferreri AJM, Cwynarski K, Pulczynski E, et al. Long-term efficacy, safety and neurotolerability of MATRix regimen followed by autologous transplant in primary CNS lymphoma: 7-year results of the IELSG32 randomized trial. Leukemia. 2022;36:1870–1878. doi:10.1038/s41375-022-01582-5
15. Jj K, Alhaj Moustafa M, Jiang L, et al. Long-term survival with ibrutinib therapy in elderly patients with newly diagnosed primary central nervous system lymphoma. Blood Lymphatic Cancer. 2022;12:23–29. doi:10.2147/blctt.S360442
16. Grommes C, Pastore A, Palaskas N, et al. Ibrutinib unmasks critical role of Bruton tyrosine kinase in primary CNS Lymphoma. Cancer Discovery. 2017;7:1018–1029. doi:10.1158/2159-8290.Cd-17-0613
17. Js M, Ostrom QT, Gittleman H, et al. The elderly left behind-changes in survival trends of primary central nervous system lymphoma over the past 4 decades. Neuro-Oncology. 2018;20:687–694. doi:10.1093/neuonc/nox187
18. Organization WH. International Classification of Diseases for Oncology (ICD-O), 1st Revision (ICD-O-3.2). Report No. ICD-O-3.2. 2019.
19. Kasenda B, Ferreri AJM, Marturano E, et al. First-line treatment and outcome of elderly patients with primary central nervous system lymphoma (PCNSL)--a systematic review and individual patient data meta-analysis. Ann Oncol. 2015;26:1305–1313. doi:10.1093/annonc/mdv076
20. Sinicrope K, Batchelor T. Primary central nervous system lymphoma. Neurol Clinics. 2018;36:517–532. doi:10.1016/j.ncl.2018.04.008
21. Hoang-Xuan K, Bessell E, Bromberg J, et al. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. Lancet Oncol. 2015;16:e322–332. doi:10.1016/s1470-2045(15)00076-5
22. Aj F, Blay J-Y, Reni M, et al. Prognostic scoring system for primary CNS lymphomas: the international extranodal lymphoma study group experience. J Clin Oncol. 2003;21:266–272. doi:10.1200/jco.2003.09.139
23. Le A, Ben-Porat L, Panageas KS, et al. Primary central nervous system lymphoma: the memorial sloan-kettering cancer center prognostic model. J Clin Oncol. 2006;24:5711–5715. doi:10.1200/jco.2006.08.2941
24. Em B, Graus F, Lopez-Guillermo A, et al. Primary non-Hodgkin’s lymphoma of the CNS treated with CHOD/BVAM or BVAM chemotherapy before radiotherapy: long-term survival and prognostic factors. Int J Radiat Oncol Biol Phys. 2004;59:501–508. doi:10.1016/j.ijrobp.2003.11.001
25. Liu CJ, Lin S-Y, Yang C-F, et al. A new prognostic score for disease progression and mortality in patients with newly diagnosed primary CNS lymphoma. Cancer Med. 2020;9:2134–2145. doi:10.1002/cam4.2872
26. Dandachi D, Ostrom QT, Chong I, et al. Primary central nervous system lymphoma in patients with and without HIV infection: a multicenter study and comparison with U.S national data. Cancer causes & control: CCC. Cancer Causes & Control: CCC. 2019;30:477–488. doi:10.1007/s10552-019-01144-8
27. Ney DE, Reiner AS, Panageas KS, et al. Characteristics and outcomes of elderly patients with primary central nervous system lymphoma: the memorial sloan-kettering cancer center experience. Cancer. 2010;116:4605–4612. doi:10.1002/cncr.25363
28. Morales-Martinez A, Lozano-Sanchez F, Duran-Peña A, Hoang-Xuan K, Houillier C. Primary central nervous system lymphoma in elderly patients: management and perspectives. Cancers. 2021;13:3479. doi:10.3390/cancers13143479
29. Tang D, et al. Epidemiologic characteristics, prognostic factors, and treatment outcomes in primary central nervous system lymphoma: a SEER-based study. Front Oncol. 2022;12.
30. Reyes Ortiz CA, Freeman JL, Kuo YF, Goodwin JS. The influence of marital status on stage at diagnosis and survival of older persons with melanoma. J Gerontol a Biol Sci Med Sci. 2007;62:892–898. doi:10.1093/gerona/62.8.892
31. Chang SM, Barker FG. Marital status, treatment, and survival in patients with glioblastoma multiforme: a population based study. Cancer. 2005;104:1975–1984. doi:10.1002/cncr.21399
32. Ding W, et al. Dynamic changes in marital status and survival in women with breast cancer: a population-based study. Sci Rep. 2021;11:5421. doi:10.1038/s41598-021-84996-y
33. Ra F, Travaglino A, Varricchio S, et al. HIV prevalence in primary central nervous system lymphoma: a systematic review and meta-analysis. Pathol Res Pract. 2020;216:153192. doi:10.1016/j.prp.2020.153192
34. Roschewski M, Phelan JD. Sorting biologic subtypes of primary CNS lymphoma. Blood. 2021;137:1436–1437. doi:10.1182/blood.2020009968
35. Gandhi MK, Hoang T, Law SC, et al. EBV-associated primary CNS lymphoma occurring after immunosuppression is a distinct immunobiological entity. Blood. 2021;137:1468–1477. doi:10.1182/blood.2020008520
36. Bayraktar S, Ud B, Ramos JC, Stefanovic A, Lossos IS. Primary CNS lymphoma in HIV positive and negative patients: comparison of clinical characteristics, outcome and prognostic factors. J Neuro-Oncol. 2011;101:257–265. doi:10.1007/s11060-010-0252-3
37. Tabouret E, Houillier C, Martin-Duverneuil N, et al. Patterns of response and relapse in primary CNS lymphomas after first-line chemotherapy: imaging analysis of the ANOCEF-GOELAMS prospective randomized trial. Neuro-Oncology. 2017;19:422–429. doi:10.1093/neuonc/now238
38. Adhikari N, Biswas A, Gogia A, et al. A prospective Phase II trial of response adapted whole brain radiotherapy after high dose methotrexate based chemotherapy in patients with newly diagnosed primary central nervous system lymphoma-analysis of acute toxicity profile and early clinical outcome. J Neuro-Oncol. 2018;139:153–166. doi:10.1007/s11060-018-2856-y
39. Omuro AM, Ben-Porat LS, Panageas KS, et al. Delayed neurotoxicity in primary central nervous system lymphoma. Arch Neurol. 2005;62:1595–1600. doi:10.1001/archneur.62.10.1595
40. Ab D, Abdelrashid M, Tucker Z, et al. High-dose methotrexate and rituximab induction regimen in immunocompetent patients with primary CNS lymphoma: a retrospective single-center study of survival predictors. J Neuro-Oncol. 2022;158:33–40. doi:10.1007/s11060-022-04004-9
41. Grommes C, Tang SS, Wolfe J, et al. Phase 1b trial of an ibrutinib-based combination therapy in recurrent/refractory CNS lymphoma. Blood. 2019;133:436–445. doi:10.1182/blood-2018-09-875732
42. Tun HW, Johnston PB, DeAngelis LM, et al. Phase 1 study of pomalidomide and dexamethasone for relapsed/refractory primary CNS or vitreoretinal lymphoma. Blood. 2018;132:2240–2248. doi:10.1182/blood-2018-02-835496
43. Nayak L, Iwamoto FM, LaCasce A, et al. PD-1 blockade with nivolumab in relapsed/refractory primary central nervous system and testicular lymphoma. Blood. 2017;129:3071–3073. doi:10.1182/blood-2017-01-764209
44. Korfel A, Schlegel U, Herrlinger U, et al. Phase II Trial of temsirolimus for relapsed/refractory primary CNS lymphoma. J Clin Oncol. 2016;34:1757–1763. doi:10.1200/jco.2015.64.9897
45. Jahr G, Da Broi M, Holte H, Beiske K, Meling TR. The role of surgery in intracranial PCNSL. Neurosurgical Review. 2018;41:1037–1044. doi:10.1007/s10143-018-0946-0
46. Weller M, Martus P, Roth P, Thiel E, Korfel A. Surgery for primary CNS lymphoma? Challenging a paradigm. Neuro-Oncology. 2012;14:1481–1484. doi:10.1093/neuonc/nos159
47. Roth P, Hoang-Xuan K. Challenges in the treatment of elderly patients with primary central nervous system lymphoma. Current Opinion in Neurol. 2014;27:697–701. doi:10.1097/wco.0000000000000145
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.