")
Back to Journals » International Journal of General Medicine » Volume 16
Clinical Characteristics Profile of COVID-19 Patients with Omicron Variant Admitted in a Tertiary Hospital, Central China
Received 9 March 2023
Accepted for publication 31 May 2023
Published 9 June 2023 Volume 2023:16 Pages 2365—2371
DOI https://doi.org/10.2147/IJGM.S409478
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Yi Miao,1 Yi Ren,2 Tongwei Ren2
1Nanyang Central Hospital, Nanyang City, Henan Province, People’s Republic of China; 2Nanyang Zhang Zhongjing Hospital, Nanyang City, Henan Province, People’s Republic of China
Correspondence: Tongwei Ren, Tel +86-377-83976176, Email [email protected]
Purpose: Omicron, a variant of COVID-19, is becoming a major issue of global concern. Its high transmissibility may bring challenges to the distribution of health care in a large population country like China. Investigating the behavior of the virus in the Chinese population will certainly help to plan for the upcoming surge of Omicron. Therefore, we made a preliminary analysis of the clinical and epidemiological characteristics of suspected cases of Omicron at the early stage of the surge.
Patients and Methods: The study was conducted in Nanyang Central Hospital, a tertiary hospital, from 21st December, 2022 to 8th January, 2023. A total of 210 patients underwent demographic characteristics and clinical symptom collection from their medical records. Moreover, sputum culture was also conducted to explore the types of bacterial or fungal infections.
Results: Our results showed that 5 patients (4.1%) were aged 16– 49, 40 patients (32.5%) were aged 50– 70, and 78 patients (63.4%) were aged 70 or more in the severe group. The proportion of male patients with severe diseases infected with Omicron is higher than that of female patients and the proportion of severe cases increases with age. The main symptoms of patients infected with Omicron are cough (91, 74.0%), fever (90, 73.2%), and asthma (73, 59.3%). The pathogens Streptococcus pneumoniae (71, 31.0%), Staphylococcus aureus (46, 20.1%), Mycoplasma pneumoniae (26, 11.4%), Klebsiella pneumoniae (18, 7.9%), Acinetobacter baumannii (13, 5.7%), and Haemophilus influenzae were detected in lower respiratory tract.
Conclusion: This study suggests that age > 70 is a risk factor for severe COVID-19 and that patients often have bacterial or fungal infections. Our research results may help to provide effective treatment for patients with Omicron infection and also contribute to health economic analysis and research to assist future public health decision-making.
Keywords: COVID-19, Omicron variant, epidemiological characteristics, infections
Introduction
Coronavirus disease 2019 (COVID-19) is an acute infectious disease of the respiratory system caused by novel coronavirus infection, which is mainly transmitted through droplets and contact.1 COVID-19 has the characteristics of strong infectivity, rapid transmission, and general susceptibility among people.2 Since the outbreak of COVID-19, it has evolved and mutated in the process of transmission, and has formed multiple variants including Alpha, Beta, Gamma, Delta and Omicron.3 South Africa first detected a COVID-19 variant (B.1.1.529) from case samples, and the World Health Organization named it Omicron variant on 25th November 2021.4 Since January 2022, Omicron has surpassed all previous mutants in its super transmissibility and replaced Delta as the main transmission strain in the world.5
The Omicron (B.1.1.529) variant is from the B.1.1 lineage and belongs to the same lineage as Alpha (B.1.1.7), which is one of the evolutionary branches of SARS-CoV-2.5 The researchers analyzed the variant sequences of Omicron variant and 3590 other COVID-19 strains, and found that Omicron is likely to be isolated from other strains in the middle of 2020 for parallel evolution.6 Compared with wild strains or other variant of concern (VOC), Omicron variant has more mutations, which is likely to exhibit stronger infectivity and immune escape ability than Delta mutant. The risk ratio of re-infection and primary infection of Omicron variant is 2.39, which is 3 times that of Beta and Delta variants.7 Moreover, the immune escape characteristics of Omicron variant are obvious, and the proportion of symptomatic cases is smaller, and the infection interval is shorter, indicating that the immune response can protect the human body from symptomatic reinfection, but this protection tends to weaken with time.8 The neutralizing activity of Omicron variant to most monoclonal antibodies was completely or substantially lost.9 The super-transmission ability and immune escape ability of Omicron variant have increased the pressure of epidemic prevention and control, bringing new challenges to the development of vaccine and antibody-related drugs for Omicron variant.
Although some studies claim that the clinical severity of omicron patients is slight in nature, several reports show that the infection caused by Omicron may be no less than that caused by Delta.4,10 Since December 2022, the Chinese government’s epidemic prevention and control policy has been adjusted, and the number of people infected with Omicron has soared. Considering China’s large population, how the surge is going in the large number of infected people will be a matter of huge concern. At present, few studies in China have recorded the course of COVID-19 patients infected by Omicron. In this context, we carried out a study to record the clinical and epidemiological characteristics of the suspected Omicron patients. The information provided in this study will help to plan medical resources and formulate appropriate policies to properly respond to the potential surge in Omicron.
Methods
Study Population
The 210 samples selected for this study are the suspected cases of Omicron (BA.5.2) admitted by Nanyang Central Hospital, a tertiary hospital, from 21st December, 2022 to 8th January, 2023 (This period was the time when the number of infected people with Omicron increased sharply in Nanyang City, China).
Data Collection and Analysis
The relevant information of this study was obtained by reading the electronic medical record file, collecting the general situation of the case (age, sex, etc.), basic clinical characteristics, laboratory examination results and treatment measures within 48 hours after admission. BMI < 18.5 is considered underweight, 18.5 ≤ BMI < 25 is considered normal-weight, and BMI ≥ 25 is considered overweight. The data were shown as mean ± standard deviation. SPSS 25.0 software was used for statistical analysis of the data. The counting data was expressed in (%), and the inter-group comparison was performed by a two-tailed Student’s t-test. In all cases, p-values <0.05 were considered significant.
Ethical Approval
This research was approved by the Nanyang Central Hospital medical ethics committee. This study was conducted conforming to the Helsinki declaration of 1975, as revised in 2000 and 2008 concerning human and animal rights. In this study, the informed consent form of the father of a patient under the age of 18 has been obtained.
Results
Demographics and Baseline Characteristics
A total of 210 cases were included in the present study. The severe group comprised 123 patients (58.6%) and the non-severe group 87 (41.4%). The sample consisted of 131 males (62.4%) and 79 females (37.6%) with a sex ratio of 1.7. In the severe group, there were 80 males (65.0%) and 43 females (35.0%), with a sex ratio of 1.9 (Figure 1A). There were 51 males (58.6%) and 36 females (41.4%) in the non-severe group, with a sex ratio of 1.4 (Figure 1B). The mean age of all cases was 67.6 years (±13.7). In the severe group, 5 patients (4.1%) were aged 16–49, 40 patients (32.5%) were aged 50–70, and 78 patients (63.4%) were aged 70 or more. In the non-severe group, 15 patients (17.2%) were aged 16–49, 41 patients (47.1%) were aged 50–70, and 31 patients (35.6%) were aged 70 or more. The mean BMI of all cases was 24.1 ± 3.5 (Figure 1C). In the severe group, there were 8 (6.5%) underweight (BMI < 18.5) patients, 73 (59.3%) normal-weight (18.5 ≤ BMI < 25) patients and 42 (34.1%) overweight (BMI ≥ 25) patients. In the non-severe group, there were 4 (4.6%) underweight (BMI < 18.5) patients, 44 (50.6%) normal-weight (18.5 ≤ BMI < 25) patients and 39 (44.8%) overweight (BMI ≥ 25) patients.
 |
Figure 1 Demography of study participants. (A) severe and non-severe case counts by sex; (B) severe and non-severe case counts by age; (C) severe and non-severe case counts by BMI. BMI (Body Mass Index) = weight/height2; weight (kg), height (m). |
Clinical Manifestations of Patients
Clinical symptoms of all patients are summarized in Table 1. All the symptomatic patients had one or more of the twelve symptoms including cough, fever, asthma, expectoration, dyspnea, chest tightness, weakness, chest pain, hiccup, ambiguity of consciousness, nasal congestion, and palpitation. In the severe group, 91 (74.0%) patients had cough, 90 (73.2%) patients had fever, 73 (59.3%) patients had asthma, 32 (26.0%) patients had expectoration, and 13 (10.6%) patients had chest tightness. In the non-severe group, 66 (75.9%) patients had cough, 55 (63.2%) patients had fever, 35 (40.2%) patients had asthma, 29 (33.3%) patients had expectoration, and 13 (10.6%) patients had chest tightness. In the severe group, 15 patients exhibited dyspnea, while in the non-severe group, only 1 patient exhibited dyspnea. Other symptoms including weakness, chest pain, hiccup, ambiguity of consciousness, nasal congestion, and palpitation occurred less frequently in both groups.
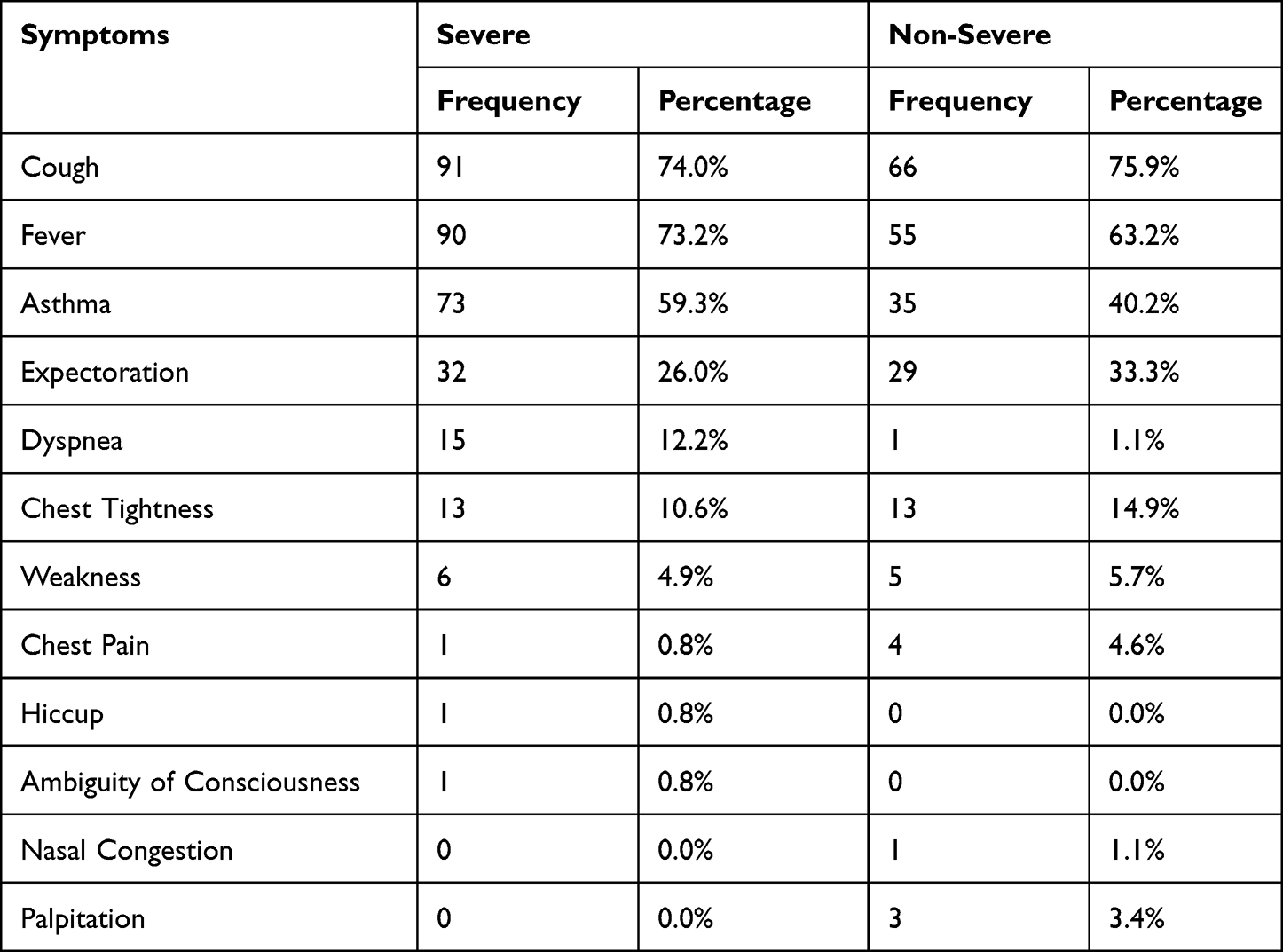 |
Table 1 Symptoms of Patients in This Study |
Laboratory Findings
Laboratory parameters were tested and recorded for all patients on the day of admission (Table 2). The average leukocyte count in severe group was 9.3×109/L, and that in non-severe group was 6.5×109/L. The average cell counts of lymphocyte had an average of 1.1×109/L in the severe group vs 1.6×109/L in the non-severe group. The average cell count of neutrophils was 7.6×109/L in the severe group vs 4.3×109/L in the non-severe group. The average content of ESR in the severe group is 121.4 pg/mL, which is 2.98 times that of the non-severe group (40.8 pg/mL). The average content of IL-6 in the severe group is 147 pg/mL, which is 4.6 times that of the non-severe group (32.1 pg/mL). The average CRP in severe group was 38.2 mg/L and that in non-severe group was 15.3 mg/L. The average PCT had an average of 5.8 ng/mL in the severe group vs 5.3 ng/mL in the non-severe group. The average content of ferritin in the severe group is 656.9 μg/L, which is 2.53 times that of the non-severe group (260.1 μg/L). The average content of D-Dimer in the severe group is 5193.3 μg/L, which is 3.9-fold higher than that of the non-severe group (1059.1 μg/L). The average ALB had an average of 31.3 g/L in the severe group vs 37.7 g/L in the non-severe group. The average content of AST in the severe group is 44.4 U/L, which is 1.9 times that of the non-severe group (23.5 U/L). The average ALTU in severe group was 44.5 U/L and that in non-severe group was 25.0 U/L. The content of leukocyte, neutrophils, ESR, IL-6, CRP, ferritin, D-Dimer, AST and ALT in the severe group is significantly higher than that of the non-severe group (p<0.001). The content of lymphocyte and ALB in the severe group is significantly lower than that of the non-severe group (p<0.001). There is no significant difference in PCT content between severe group and non-severe group (p=0.829).
 |
Table 2 Laboratory Parameters of Patients in This Study |
Distribution of Pathogens in Lower Respiratory Tract Infections
A total of 229 pathogens were detected in these patients (Figure 2). Among them, 204 strains (89.1%) were bacteria and 25 strains (10.9%) were fungi. As shown in Figure 2A, the pathogens with high detection rate are Streptococcus pneumoniae (71, 31.0%), Staphylococcus aureus (46, 20.1%), Mycoplasma pneumoniae (26, 11.4%), Klebsiella pneumoniae (18, 7.9%), Acinetobacter baumannii (13, 5.7%), and Haemophilus influenzae (11, 4.8%). As shown in Figure 2B, the sex ratio of infection with S. pneumoniae, S. aureus, M. pneumoniae, K. pneumoniae, A. baumannii, H. influenzae, Aflatoxin, Aspergillus, and Escherichia coli are 1.4, 1.9, 1.4, 1.6, 1.8, 1.7, 1.7, and 1.5, which are similar with the all sample sex ratio. This result suggests that there is no clear correlation between the type of the main infectious pathogens and sex of patients.
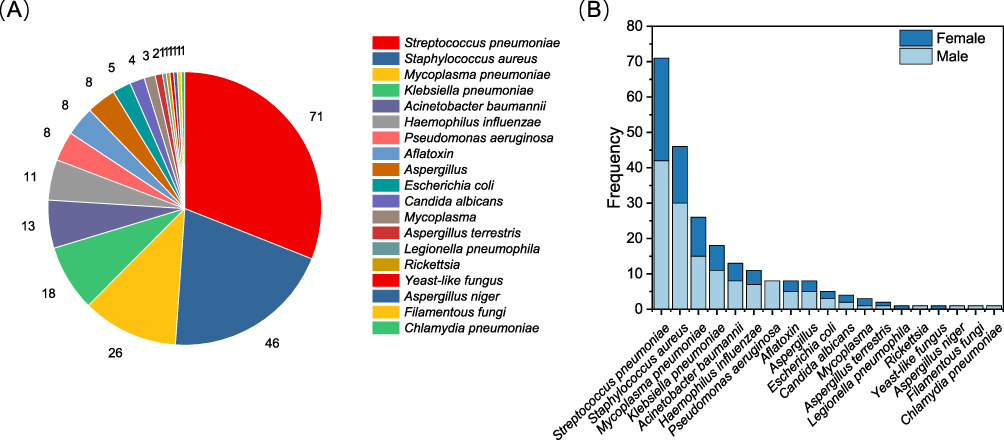 |
Figure 2 (A) Bacterial and fungal frequency of infection in patients with Omicron; (B) bacterial and fungal frequency of infection in male and female patients with Omicron. |
Discussion
The study investigated the clinical and laboratory findings of 210 Omicron patients who were admitted to a tertiary hospital for medical observation after the adjustment of the Chinese government’s epidemic prevention and control policies. Our results show that in the severe group, there were 80 males (65.0%) and 43 females (35.0%), with a sex ratio of 1.9, while the overall sample sex ratio was 1.7. This result suggests that the proportion of male patients with severe diseases infected with Omicron is higher than that of female patients. This phenomenon is consistent with the result that the hospital admission rate and mortality rate of men were higher than that of women during the COVID-19 pandemic in China (2020).11 A recent study evaluated the role of androgens in the severity and mortality of COVID-19 and reported that the androgen-mediated mechanism could explain this gender difference.12 Androgen increased the expression of type II transmembrane serine protease (TMPRSS2) and angiotensin converting enzyme 2 (ACE2), which made the new coronavirus enter the host cell, and the expression in young men was higher than that in women.12
This study shows that 5 patients (4.1%) were aged 16–49, 40 patients (32.5%) were aged 50–70, and 78 patients (63.4%) were aged 70 or more in the severe group (Figure 1B). It can be found that the proportion of severe cases increases with age. Previous clinical studies have exhibited that in the COVID-2 pandemic, age is positively correlated with the disease severity and mortality after COVID-19 infection and is the strongest risk factor.13 A recent study showed that the response of aging mice to COVID-19 infected interferon and adaptive antibody was significantly lower than that of young mice.14 The results of this study indicate that there is no obvious relationship between BMI and the proportion of severe cases. The size of BMI not only affects the changes of other functional and quality indicators of the human body but also directly affects the health status. In addition, excessive BMI index may have a negative impact on the relevant functions of the human body. Overweight or obesity may increase the probability of adults suffering from cardiovascular and cerebrovascular diseases, hypertension, diabetes, and endocrine system diseases. At present, there is no report proving the relationship between BMI and the probability of infection with COVID-19, but too high BMI may aggravate the symptoms after infection.15
Our results reveal that all the symptomatic patients had one or more of the twelve symptoms including cough, fever, asthma, expectoration, dyspnea, chest tightness, weakness, chest pain, hiccup, ambiguity of consciousness, nasal congestion, and palpitation (Table 1). The main symptoms are cough (91, 74.0%), fever (90, 73.2%), and asthma (73, 59.3%). Few people in our patients have been recorded with myalgia, runny nose, headache, cold, fatigue and night sweats, which are reported to be new symptoms of western counterparts.16 The laboratory test results reveal that the content of leukocyte, neutrophils, ESR, IL-6, CRP, ferritin, D-Dimer, AST and ALT in the severe group is significantly higher than that of the non-severe group (p<0.001). In addition, the pathogens S. pneumoniae, S. aureus, M. pneumoniae, K. pneumoniae, A. baumannii, and H. influenzae were detected in lower respiratory tract. Omicron infection may precede the previous microbial infection, or co-infection or overlapping infection.17 The risk of microbial co-infection increased significantly, and the risk of death and severe disease increased significantly.18,19 However, the mechanism of co-infection is not clear and needs further study.
Several limitations should be mentioned in this study. Our study only includes Omicron patients in a hospital in Nanyang City, which does not fully represent the overall population of Omicron infected patients. Due to the adjustment of the epidemic prevention and control policy and the hospital reception plan, it is impossible to carry out laboratory and radiological examinations for all patients.
Our study describes in detail the clinical characteristics of severe and non-severe patients infected with Omicron. We found that the proportion of male patients with severe diseases infected with Omicron is higher than that of female patients and the proportion of severe cases increases with age. The main symptoms of patients infected with Omicron are cough (91, 74.0%), fever (90, 73.2%), and asthma (73, 59.3%). The laboratory test results reveal that the content of leukocyte, neutrophils, ESR, IL-6, CRP, ferritin, D-Dimer, AST and ALT in the severe group is significantly higher than that of the non-severe group (p<0.001). In addition, the pathogens S. pneumoniae, S. aureus, M. pneumoniae, K. pneumoniae, A. baumannii, and H. influenzae were detected in lower respiratory tract. Our research results may help to provide effective treatment for patients with Omicron infection. It will also contribute to health economic analysis and research to assist future public health decision-making.
Ethical Approval
This research was approved by the Nanyang Central Hospital medical ethics committee and all patients signed an informed consent (the informed consent form of the father of a patient under the age of 18 was obtained).
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mehraeen E, Salehi MA, Behnezhad F, et al. Transmission modes of COVID-19: a systematic review. Infect Disord Drug Targets. 2021;21(6):e1077503845. doi:10.2174/22123989MTExjNTEn0
2. Awad M, Al-Hussaniy HA, Alburghaif AH, et al. The role of COVID-19 in myopathy: incidence, causes, treatment, and prevention. J Med Life. 2022;15(12):1458–1463. doi:10.25122/jml-2022-0167
3. Focosi D, Quiroga R, McConnell S, et al. Convergent evolution in SARS-CoV-2 spike creates a variant soup from which new COVID-19 waves emerge. Int J Mol Sci. 2023;24(3):2264. doi:10.3390/ijms24032264
4. Ethirajan T, Natarajan G, Velayudham R, et al. Clinico-epidemiological profile of COVID-19 patients with Omicron variant admitted in a tertiary care center, South India. Int J Gen Med. 2023;16:185–191. doi:10.2147/IJGM.S365207
5. Migueres M, Dimeglio C, Tremeaux P, et al. Influence of immune escape and nasopharyngeal virus load on the spread of SARS-CoV-2 Omicron variant. J Infect. 2022;84(4):e7–e9. doi:10.1016/j.jinf.2022.01.036
6. Kupferschmidt K. Where did ‘weird’ Omicron come from? Science. 2021;374(6572):1179. doi:10.1126/science.acx9738
7. Pulliam J, van Schalkwyk C, Govender N, et al. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science. 2022;376(6593):n4947. doi:10.1126/science.abn4947
8. Bastard J, Taisne B, Figoni J, et al. Impact of the Omicron variant on SARS-CoV-2 reinfections in France, March 2021 to February 2022. Euro Surveill. 2022;27(13). doi:10.2807/1560-7917.ES.2022.27.13.2200247
9. Ai J, Wang X, He X, et al. Antibody evasion of SARS-CoV-2 Omicron BA.1, BA.1.1, BA.2, and BA.3 sub-lineages. Cell Host Microbe. 2022;30(8):1077–1083. doi:10.1016/j.chom.2022.05.001
10. Wolter N, Jassat W, Walaza S, et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet. 2022;399(10323):437–446. doi:10.1016/S0140-6736(22)00017-4
11. CDC Weekly C. The epidemiological characteristics of an outbreak of 2019 Novel Coronavirus Diseases (COVID-19) - China, 2020. China CDC Wkly. 2020;2(8):113–122. doi:10.46234/ccdcw2020.032
12. Ataei A, Derakhshan MM, Razmjooie M, et al. Androgens’ role in severity and mortality rates of COVID-19. Horm Metab Res. 2022;54(12):813–826. doi:10.1055/a-1954-5605
13. Borgoni S, Kudryashova KS, Burka K, et al. Targeting immune dysfunction in aging. Ageing Res Rev. 2021;70:101410. doi:10.1016/j.arr.2021.101410
14. Chen Y, Li C, Liu F, et al. Age-associated SARS-CoV-2 breakthrough infection and changes in immune response in a mouse model. Emerg Microbes Infect. 2022;11(1):368–383. doi:10.1080/22221751.2022.2026741
15. DeSantis SM, Yaseen A, Hao T, et al. Incidence and predictors of breakthrough and severe breakthrough infections of SARS-CoV-2 after primary series vaccination in adults: a population-based survey of 22,575 participants. J Infect Dis. 2023;227:1164–1172. doi:10.1093/infdis/jiad020
16. Jansen L, Tegomoh B, Lange K, et al. Investigation of a SARS-CoV-2 B.1.1.529 (Omicron) variant cluster - Nebraska, November-December 2021. MMWR Morb Mortal Wkly Rep. 2021;70(5152):1782–1784. doi:10.15585/mmwr.mm705152e3
17. Zhu X, Ge Y, Wu T, et al. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res. 2020;285:198005. doi:10.1016/j.virusres.2020.198005
18. Hughes S, Troise O, Donaldson H, et al. Bacterial and fungal coinfection among hospitalized patients with COVID-19: a retrospective cohort study in a UK secondary-care setting. Clin Microbiol Infect. 2020;26(10):1395–1399. doi:10.1016/j.cmi.2020.06.025
19. Nowak MD, Sordillo EM, Gitman MR, et al. Coinfection in SARS-CoV-2 infected patients: where are influenza virus and rhinovirus/enterovirus? J Med Virol. 2020;92(10):1699–1700. doi:10.1002/jmv.25953
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.