Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Characteristics of Necrotizing Pneumonia Caused by Different Pathogens
Received 29 April 2023
Accepted for publication 2 June 2023
Published 14 June 2023 Volume 2023:16 Pages 3777—3786
DOI https://doi.org/10.2147/IDR.S419294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yonghan Luo, Yanchun Wang
Second Department of Infectious Disease, Kunming Children’s Hospital, Kunming, Yunnan, People’s Republic of China
Correspondence: Yanchun Wang, Second Department of Infectious Disease, Kunming Children’s Hospital, Kunming, Yunnan, 650000, People’s Republic of China, Email [email protected]
Objective: To explore the clinical characteristics of necrotizing pneumonia (NP) caused by different pathogens.
Methods: A total of 282 children with NP admitted to Kunming Children’s Hospital from January 2014 to November 2022 were enrolled. The clinical data of all children was collected. According to the different pathogens causing NP, the children were divided into three groups: the Mycoplasma pneumoniae necrotizing pneumonia (MPNP) group, the bacterial necrotizing pneumonia (BNP) group, and necrotizing pneumonia with no pathogen detected (NNP) group. The basic information, symptoms, signs, laboratory tests, radiological features, treatment, and prognosis of the three groups were compared.
Results: Among the 282 cases of NP, there were 62 (22.0%) cases of MPNP, 98 (34.75%) cases of BNP, and 142 (50.35%) cases of NNP. The most common bacteria causing NP were Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, and Acinetobacter baumannii, respectively. Most clinical features of the three groups were statistically significant. The area under the concentration curve of white blood cell, C-reactive protein, albumin, neutrophil percentage, and fibrinogen in differentiating MPNP from BNP were 0.743 (0.638– 0.849), 0.797 (0.711– 0.883), 0.766 (0.671– 0.861), 0.616 (0.509– 0.724), and 0.634 (0.523– 0.744), respectively. The decision curve showed that white blood cells, albumin, and C-reactive protein had good clinical application in differentiating MPNP from BNP. All patients were improved and discharged without death.
Conclusion: Bacteria are the most common cause of NP, and the most common bacteria are Streptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenzae. NP with no pathogen detected accounted for a large proportion. white blood, C-reactive protein, and albumin can identify the pathogens of NP. Patients with BNP were more severe, had a longer hospital stay, and were more likely to undergo closed drainage and surgery.
Keywords: pathogen, children, necrotizing pneumonia, clinical features
Introduction
Necrotizing pneumonia (NP) is an uncommon but serious complication of community-acquired pneumonia (CAP) in children.1 It has been reported in many areas since the 20th century, accounting for about 0.8–7% of the total CAP hospitalized patients.2 The primary clinical manifestations of NP are similar to those of other severe pneumonias.2 But children with NP have significantly longer fever duration, hospital stays, and anti-infection courses and about 10% of children need to be hospitalized again.2,3 Some critically ill children require ventilator-assisted ventilation or even ECMO to maintain oxygenation.4–6
NP refers to the liquefaction and necrosis of lung parenchyma caused by various factors, resulting in the formation of multiple cysts or cavities. On the enhanced CT of the lung, there was no obvious enhancement at the edge of the cavity, and there could be gas-liquid flatness in the cavity.7 At present, it is reported that the most common pathogens of NP are Streptococcus pneumoniae, Staphylococcus aureus, and Mycoplasma pneumoniae (MP).8–10 But these single-center studies tend to have small sample sizes, mostly only dozens of cases. In addition, a large proportion of NP cases have no detectable pathogen and can only be treated empirically. There is no study on the clinical characteristics of “pathogen-free” NP. In our previous study,11 we explored predictors of massive NP and developed a predictive model but did not analyze the clinical characteristics of NP caused by different pathogens. Considering the above reasons, we reviewed all the cases of NP in our hospital since the establishment of the electronic medical record system, and analyzed the clinical characteristics of NP according to the types of pathogens, in order to provide an evidence-based basis for the treatment of NP.
Study Variables and Data Extraction
Data Source
The retrospective study was conducted at the Children’s Hospital affiliated with Kunming Medical University. The hospitalized children with NP from January 2014 to November 2022 were analyzed retrospectively. This study complied with the Declaration of Helsinki and approved by the Ethics Review Committee of the Children’s Hospital affiliated with Kunming Medical University (2023–03-049-k01). Written informed consent was obtained from the guardian of each patient.
Study Population
The inclusion criteria for NP were as follows: 1) being under the age of 18; 2) a definite diagnosis of community-acquired pneumonia;12 3) the chest CT showed large consolidation with multiple liquefaction and necrosis lesions, some of which had air-fluid level. Exclusion criteria for NP:1) patients with a history of chronic lung disease, immunodeficiency disease, connective tissue disease, or hematological disease; 2) cavitary lung diseases such as pulmonary cysts and tuberculosis;
The inclusion criteria for MP infection were as follows: 1) cough, fever, and other symptoms and signs of pulmonary infection; 2) MP-IgM positive in serum and MP-DNA positive in sputum and bronchoalveolar lavage fluid by PCR fluorescent probe method. Inclusion criteria for bacterial infection: 1) Pathogenic bacteria were cultured from body fluids, including blood, alveolar lavage fluid, and pleural puncture fluid.
According to the different pathogens causing NP, the children were divided into three groups: the Mycoplasma pneumoniae necrotizing pneumonia (MPNP) group, the bacterial necrotizing pneumonia (BNP) group, and the necrotizing pneumonia with no pathogen detected group (NNP).
Study Variables and Data Extraction
All clinical data were collected through the medical case system of the Children’s Hospital of Kunming Medical University. Including general information, clinical features, radiological features, complications, laboratory tests, treatment, and outcome.
Treatment
The MPNP group received azithromycin 10 mg/kg/day via intravenous infusion therapy, infusion for three days, withdrawal for four days, 2–3 courses of treatment, and 4 courses in severe cases. Patients over 8 years old who failed to respond to azithromycin were given doxycycline 2 mg/kg orally, q12h, for 10 days. The treatment of BNP and NNP: vancomycin, azithromycin, or β-lactam antibiotics were given or combined when the etiology was not clear. Effective antibiotics were selected according to drug sensitivity when the pathogen was confirmed, and the course of treatment was 3–4 weeks. Methylprednisolone sodium succinate, 1–2 mg/kg, was given to children with persistent high fever, once every 12 hours, and the dose was gradually reduced for 5–10 days after the condition was stable. Intravenous gamma globulin was used in severe cases such as septic shock, persistent fever, and large area of lung necrosis. Patients with a large amount of pleural effusion or a diagnosis of empyema were treated with closed thoracic drainage. After 2–4 weeks of medical anti-infection treatment, the clinical symptoms were not significantly improved, and the imaging showed no obvious absorption or aggravation of the lesion, lobectomy was performed.
Definition
Hematogenous spread is defined as the pathogen that causes NP not through direct respiratory infection but through blood flow from other parts of the body to the lungs. Patients who complain not of respiratory symptoms but of other systemic symptoms such as bone pain and have specific pathogenic bacteria in their blood cultures will be considered to have hematogenous spread.
Statistical Analysis
R software 4.2.2 was used for statistical analysis. t test was used for comparison of continuous variables with normal distribution between the two groups, and analysis of variance was used for comparison of continuous variables with normal distribution between the three groups, which were expressed as x±s. the Mann–Whitney U-test was used to analyze the non-normal distribution of continuous variables between the two groups, and the Kruskal–Wallis H-test was used to analyze the non-normal distribution of continuous variables among the three groups, expressed as M (P25, P75). Categorical variables were compared between groups using the chi-square test or Fisher exact probability method, and were expressed as frequency (%). Univariate analysis of the variables showed that the three groups had differences in the laboratory values. We created a box chart of data visualization to compare the differences between the groups more intuitively. The receiver operating characteristic (ROC) curve was used to analyze the predictive accuracy of differential indicators, and the decision curve was used to analyze the clinical practicability of differential indicators. P value of less than 0.05 was considered statistically significant.
Outcome
Etiological Analysis
A total of 282 cases of NP were included. There were 62 (22.0%) cases of MPNP, 98 (34.75%) cases of BNP, and 142 (50.35%) cases of NNP (Figure 1A). The most common bacteria causing NP were Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, and Acinetobacter Baumannii, respectively Figure 1B. Other pathogens included Legionella pneumophila (3 cases), Klebsiella pneumoniae (2 cases), Pseudomonas aeruginosa (1 case), Staphylococcus epidermidis (1 case), and Moraxella catarrhalis (1 case).
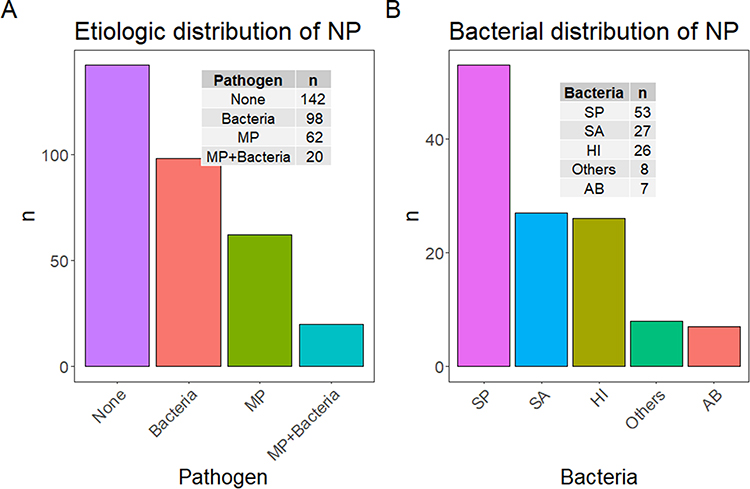 |
Figure 1 (A) Etiologic distribution of NP. (B) Bacterial distribution of NP. Abbreviations: MP, Mycoplasma pneumoniae; SP, Streptococcus pneumoniae; SA, Staphylococcus aureus; HI, Haemophilus influenzae; AB, Acinetobacter baumannii. |
Baseline Information
To compare the clinical features of NP caused by different pathogens. We excluded a total of 20 cases with both bacterial and MP infections. A total of 262 cases were divided into three groups according to the different pathogens. The comparison of variable clinical characteristics between the three groups was shown in Table 1. In general, NP was common in preschool and school-age children (5.06 ±3.97y), and there was no significant difference in age or gender among the three groups. However, children in the None group weighed less than those in the other two groups (p < 0.05).
 |
Table 1 The Clinical Characteristic in MPNP, BNP, and NNP |
Clinical Features
The majority of MPNP had cough (95.2%), but the proportion of cough in BNP was significantly lower (79.5%, P < 0.05). The median fever of NNP was 10.00 (6.25, 15.00) d, higher than that of MPNP and BNP groups (P < 0.05). In addition, rales (38.1%) and haematogenous spread (10.3%) were more common in the BNP group than in the other two groups. There was no significant difference in the incidence of other symptoms between the two groups.
Radiological Features and Complications
BNP had a higher proportion of complications in the digestive system, circulatory system, and blood system. The remaining complications and imaging lesions were not statistically different among the three groups.
Laboratory Values
There were significant differences in laboratory values among the three groups. In order to intuitively compare the differences between the groups, we plotted box plots for data visualization. Figure 2 showed the continuous variables with statistically significant differences among the three groups, and these variables were mainly some laboratory values.
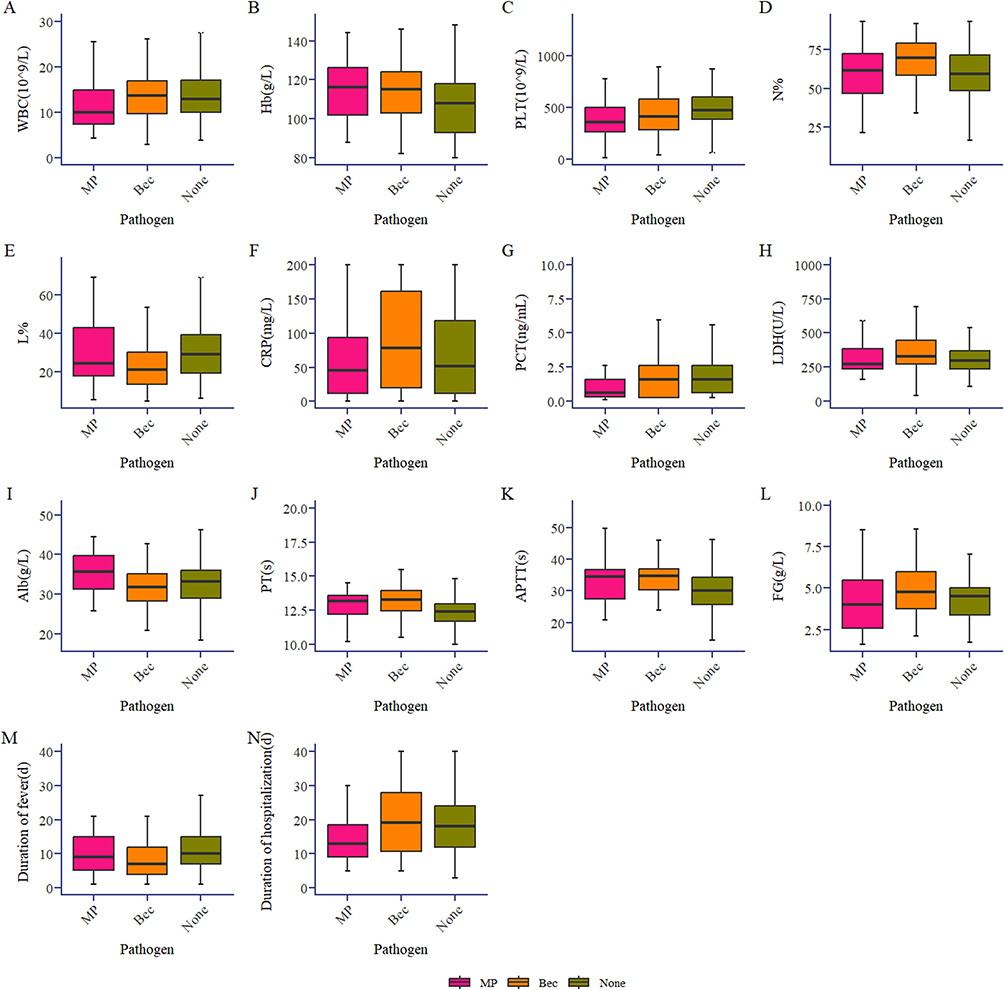 |
Figure 2 Comparison of continuous clinical characteristics variables among MPNP, BNP and NNP. Abbreviations: WBC, white blood cell; Hb, hemoglobin; PLT, platelet; N%, Percentage of neutrophils; L%, Percentage of lymphocytes; CRP, C -reactive protein; PCT, procalcitonin; LDH, lactate dehydrogenase; Alb, albumin; PT, Prothrombin time; APTT, activated partial thromboplastin time; FG, fibrinogen. |
Identification of BNP and MPNP
Univariate analysis showed that length of hospital stays, cough, shortness of breath, rales, WBC, percentage of neutrophils, CRP, ALB, FG, chest drainage, surge, hospitalization expenses, and blood system complications were statistically significant between the two groups. ROC curve was used to analyze the accuracy of each continuous variable with statistical significance in distinguishing NP caused by different pathogens. The results showed that the AUC of WBC, CRP, ALB, percentage of neutrophils, and FG in differentiating MPNP from BNP were 0.743 (0.638–0.849), 0.797 (0.711–0.883), 0.766 (0.671–0.861), 0.616 (0.509–0.724), and 0.634 (0.523–0.744), respectively, as shown in Figure 3. The results of the decision curve analysis showed that when the threshold probability was between 0.4 and 0.8, the net benefit rate of the identification index was greater than 0, showing good clinical application value, as shown in Figure 4.
 |
Figure 3 ROC curve of various indicators for differentiating MPNP from NNP. Abbreviations: WBC, white blood cell; N%, percentage of neutrophils; CRP, C-reactive protein; Alb, albumin; FG, fibrinogen. |
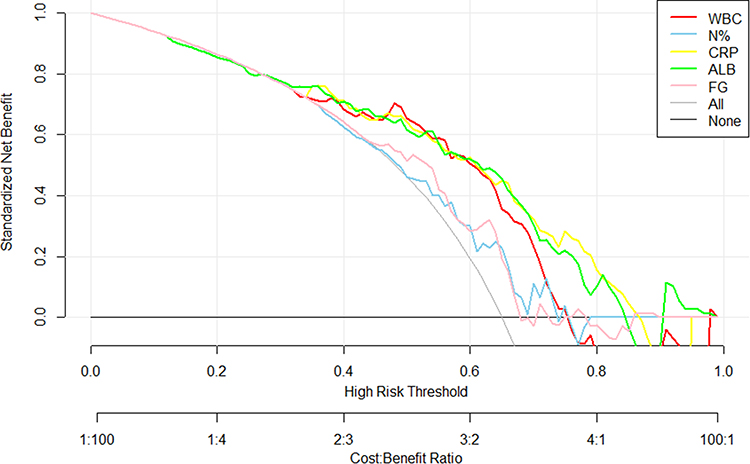 |
Figure 4 Decision curve analysis (DCA) of various indicators for differentiating MPNP from NNP. Abbreviations: WBC, white blood cell; N%, percentage of neutrophils; CRP, C-reactive protein; Alb, albumin; FG, fibrinogen. |
Discussion
In this study, we summarized 282 cases of NP and analyzed the clinical, laboratory, and imaging characteristics of NP according to its etiological results. We also analyzed the clinical indicators used to distinguish MPNP from BNP and their practical clinical value. We believe that this large sample size study analyzing NP clinical characteristics will aid in early detection and treatment.
It is very important to determine the distribution of pathogens for the diagnosis and treatment of NP. If we can find a specific pathogen and its drug sensitivity test results, it will have a double effect with half the effort. However, due to inappropriate specimen collection and the use of antibiotics before admission, no pathogen was detected in many cases. Clinicians will use empirical treatment based on the common pathogens of NP. In the past, it was considered that Staphylococcus aureus and Streptococcus pneumoniae were the most common pathogens causing NP.1,13,14 However, NP caused by MP has gradually increased in recent years,15–19 especially in many studies in China. The most common pathogens in our study were bacteria, but in terms of absolute numbers, MP was the first. In addition, our study also found that a large proportion of children with NP cannot identify a specific pathogen, but we know that NP is mostly caused by infection, so how do we choose antibiotics in the absence of a pathogen? As can be seen from Figure 2, the median of WBC in the NNP group was > 10*109/L, neutrophils were the dominant cell type, CRP was > 50 mg/L, and PCT was >1.5 ng/mL, which was more consistent with the blood picture of BNP than MPNP. Moreover, the visualized Figure 2 also showed that indicators of NNP were closer to those of BNP. Similar to the BNP, about 70% of children with NNP were discharged after antibiotic treatment covering common pathogens of NP such as Staphylococcus aureus or Streptococcus pneumoniae, which could provide evidence-based guidance for the treatment of NNP.
In terms of clinical symptoms, the MPNP group had a higher proportion of cough, while the BNP had a higher proportion of rales and hematogenous spread. After adhering to host cells, MP causes lung injury through the synthesis and secretion of hydrogen peroxide and an excessive inflammatory response.20 The high proportion of cough in MPNP is mainly due to repeated stimulation of MP adhesion to the respiratory tract. The adhesion of MP and its tendency to cause consolidation (35% in our study) and atelectasis could lead to a decrease in lung rales. In this study, the duration of fever was longer in NNP, which was related to the disease delay caused by empirical anti-infection. Although NP caused by osteomyelitis has been reported in a case report,21 NP caused by hematogenous infection had been generally ignored in previous retrospective studies. In our study, eleven cases of BNP were caused by hematogenous infection. Among these 11 cases, 8 cases complained of bone pain, 3 cases complained of abdominal pain and diarrhea rather than respiratory symptoms, and all of them were concentrated in the non-MPNP group. The relatively high proportion of hematogenous infections (4.2%) suggests that NP secondary to osteomyelitis should be considered when other non-respiratory symptoms, especially bone pain, appear with the progression of the disease. An active chest CT and blood culture should be performed to identify the disease and pathogen as soon as possible.
The pathogenesis of NP is still not very clear, and the invasiveness of pathogenic microorganisms and cytokine-mediated immune response play a key role in the pathogenesis.20,22 Current studies suggest that the main causes of pulmonary cavity are abnormal coagulation function, vascular occlusion, and thrombosis caused by infection-induced vasculitis. This study suggested that BNP is associated with a higher rate of systemic complications, a higher rate of admission to the ICU, a longer length of hospital stay, and higher hospital costs than MPNP, which suggests that BNP is more severe. In this study, the levels of WBC, neutrophil percentage, CRP, and PCT in the BNP group were significantly higher than those in the MPNP group. It was suggested that BNP is related to a more serious systemic inflammatory response, and monitoring the changes in inflammatory indicators can help clinicians distinguish BNP from MPNP. The ROC curve showed that the AUC of WBC, CRP, and ALB were 0.743, 0.797, and 0.766, respectively, which had good discrimination accuracy. The prediction accuracy of WBC and CRP was consistent with that of Yang and Zhang’s study.23,24 ALB is often used as a negative inflammatory marker to predict the severity of pneumonia.25 Because of increased protein consumption caused by more severe inflammation and protein exudation caused by increased vascular permeability, Alb was lower in the BNP. In addition, we evaluated the clinical utility of WBC, CRP, and ALB in differentiating MPNP from BNP using the decision curve, which showed that there was a clinical benefit when the high-risk threshold was between 0.4 and 0.8.
Lobectomy was performed in 13% of the cases in this study, which was higher than other studies.20,23 First, Yunnan Province, where the hospital is located, is a relatively developed region in western China. Patients referred from districts and counties took longer to be diagnosed, had less standard anti-infection treatment, and were more likely to have prolonged disease. Second, the proportion of non-MPNP was higher in this study. In general, MPNP has a better effect on anti-infective treatment, while lung abscesses caused by bacteria are more likely to be treated with puncture drainage and surgical intervention. Third, our data were collected over a longer period (up to 8 years). With advances in the understanding of NP, the proportion of surgical lobectomy for NP has decreased in recent retrospective studies.20,23 It is worth mentioning that whether severe MPNP should be treated by lobectomy is controversial. “Guideline for diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2023 version)” clearly states that MPNP does not need to be treated by lobectomy. However, there were still many cases of MPNP with poor efficacy of anti-infection treatment, and the disease was prolonged and finally surgery was still performed. At present, there is a lack of clinical research on the comparison of the effect of surgery and anti-infection treatment on MPNP, and prospective studies with large samples are needed to provide evidence-based support.
In general, the outcome of NP was good, and all patients improved and were discharged from the hospital except for five children who were withdrawn from treatment by their parents.
The advantage of this study is that the clinical characteristics of NP were analyzed with a large sample size, the characteristics of NNP were analyzed for the first time, the differences among the three groups were visually analyzed, and the differential indicators with clinical practical value were found. However, there are still some limitations to this study. Firstly, the retrospective study inevitably has some selection bias. Second, some indicators that reflect the characteristics of NP, such as tumor necrosis factor, interleukin, and ferritin, have to be excluded because of the lack of data. Finally, this study lacks long-term follow-up data.
Conclusions
Bacteria are the most common cause of NP, and the most common bacteria are Streptococcus pneumoniae, Staphylococcus aureus, and Haemophilus influenzae. NP with no pathogen detected accounted for a large proportion. WBC, CRP, and ALB can identify the pathogens of NP. Patients with BNP were more severe, had a longer hospital stay, and were more likely to undergo closed drainage and surgery.
Funding
This work was supported by the Joint project of Yunnan Science and Technology Department Kunming Medical University (202101AY070001—217); Kunming Health Science and technology personnel training project (2020(Province)-21); Yunnan key specialty of pediatric infection(Training and education program/Kunming key specialty of pediatric infection; Key Science and Technology Program of Yunnan Province (No.202102AA100019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sawicki GS, Lu FL, Valim C, Cleveland RH, Colin AA. Necrotising pneumonia is an increasingly detected complication of pneumonia in children. Eur Respir J. 2008;31(6):1285–1291. doi:10.1183/09031936.00099807
2. Masters IB, Isles AF, Grimwood K. Necrotizing pneumonia: an emerging problem in children? Pneumonia. 2017;9:11. doi:10.1186/s41479-017-0035-0
3. Lai SH, Wong KS, Liao SL. Value of Lung Ultrasonography in the Diagnosis and Outcome Prediction of Pediatric Community-Acquired Pneumonia with Necrotizing Change. PLoS One. 2015;10(6):e0130082. doi:10.1371/journal.pone.0130082
4. Cortina G, Niederwanger C, Klingkowski U, Velik-Salchner C, Neu N. Prolonged extracorporeal membrane oxygenation for pediatric necrotizing pneumonia due to Streptococcus pneumonia and influenza H1N1 co-infection: how long should we wait for native lung recovery? J Artif Organs. 2018;21(3):367–370. doi:10.1007/s10047-018-1024-7
5. Gerdung CA, Ross BC, Dicken BJ, Bjornson CL. Pneumonectomy in a Child with Multilobar Pneumatocele Secondary to Necrotizing Pneumonia: case Report and Review of the Literature. Case Rep Pediatr. 2019;2019:2464390. doi:10.1155/2019/2464390
6. Ashkenazi S, Ben-Nun A, Pessach I, Rubinshtein M, Paret G. Lobectomy on ECMO as a Life-Saving Procedure following Necrotizing Pneumonia in a Toddler: a Case Study. J Pediatr Intensive Care. 2018;7(4):207–209. doi:10.1055/s-0038-1636507
7. Chatha N, Fortin D, Bosma KJ. Management of necrotizing pneumonia and pulmonary gangrene: a case series and review of the literature. Can Respir J. 2014;21(4):239–245. doi:10.1155/2014/864159
8. Byington CL, Hulten KG, Ampofo K, et al. Molecular epidemiology of pediatric pneumococcal empyema from 2001 to 2007 in Utah. J Clin Microbiol. 2010;48(2):520–525. doi:10.1128/JCM.01200-09
9. San Martin I, Zarikian SE, Herranz M, Moreno-Galarraga L. Necrotizing pneumonia due to Mycoplasma in children: an uncommon presentation of a common disease. Adv Respir Med. 2018;86(6):305–309. doi:10.5603/ARM.a2018.0049
10. Blanco-Iglesias E, Oñoro G, Almodovar-Martín JL, et al. Retrospective Study in Children With Necrotizing Pneumonia: nine Years of Intensive Care Experience. Pediatr Infect Dis J. 2020;39(7):571–575. doi:10.1097/INF.0000000000002633
11. Luo Y, Wang Y. Development of a Nomogram for Predicting Massive Necrotizing Pneumonia in Children. Infect Drug Resist. 2023;16:1829–1838. doi:10.2147/IDR.S408198
12. Board CM. 儿童社区获得性肺炎管理指南(2013修订)[Guidelines for management of community acquired pneumonia in children(the revised edition of 2013) (II)]. Zhonghua Er Ke Za Zhi. 2013;51(11):856–862. Chinese.
13. Krenke K, Sanocki M, Urbankowska E, et al. Necrotizing Pneumonia and Its Complications in Children. Adv Exp Med Biol. 2015;857:9–17.
14. Ness-Cochinwala M, Kobaitri K, Totapally BR. Characteristics and Outcomes of Children With Necrotizing Pneumonia. Pediatr Crit Care Med. 2021;22(12):e640–e643. doi:10.1097/PCC.0000000000002793
15. Zhou Y, Hu M, Ye B, Chen Z, Zhang Y. Early prediction of necrotizing pneumonia from mycoplasma pneumoniae pneumonia with large pulmonary lesions in children. Sci Rep. 2020;10(1):19061. doi:10.1038/s41598-020-76083-5
16. Wang X, Zhong LJ, Chen ZM, Zhou YL, Ye B, Zhang YY. Necrotizing pneumonia caused by refractory Mycoplasma pneumonia pneumonia in children. World J Pediatr. 2018;14(4):344–349. doi:10.1007/s12519-018-0162-6
17. Chiu CY, Chiang LM, Chen TP. Mycoplasma pneumoniae infection complicated by necrotizing pneumonitis with massive pleural effusion. Eur J Pediatr. 2006;165(4):275–277. doi:10.1007/s00431-005-0058-z
18. Pellan M, Bastian C, Gaudelus J, Delacourt C, de Pontual L. Pulmonary necrotizing cavity caused by Mycoplasma pneumoniae infection. Arch Pediatr. 2013;20(10):1158–1159. doi:10.1016/j.arcped.2013.06.031
19. Zhou YL, Liu JR, Yi QW, et al. A multicenter retrospective study on the etiology of necrotizing pneumonia in children. Zhonghua Er Ke Za Zhi. 2021;59(8):658–664. doi:10.3760/cma.j.cn112140-20210126-00072
20. Qian J, Wei YJ, Cheng YJ, Zhang Y, Peng B, Zhu CM. Analysis of clinical features and risk factors of necrotizing pneumonia in children. Beijing Da Xue Xue Bao Yi Xue Ban. 2022;54(3):541–547. doi:10.19723/j.issn.1671-167X.2022.03.021
21. Li P, Dai L, Yuan K, et al. Necrotizing pneumonia and purulent meningitis caused by bloodstream infection of CA-MRSA in a child: a rare case report. Front Pediatr. 2022;10:1045774. doi:10.3389/fped.2022.1045774
22. Wang RS, Wang SY, Hsieh KS, et al. Necrotizing pneumonitis caused by Mycoplasma pneumoniae in pediatric patients: report of five cases and review of literature. Pediatr Infect Dis J. 2004;23(6):564–567. doi:10.1097/01.inf.0000130074.56368.4b
23. Yang B, Zhang W, Gu W, et al. Differences of clinical features and prognosis between Mycoplasma pneumoniae necrotizing pneumonia and non-Mycoplasma pneumoniae necrotizing pneumonia in children. BMC Infect Dis. 2021;21(1):797. doi:10.1186/s12879-021-06469-x
24. Zhang YY, Dai LM, Zhou YL, Yang DH, Tang LF, Chen ZM. Comparative analysis of clinical characteristics and prognosis between bacterial necrotizing pneumonia and Mycoplasma pneumoniae necrotizing pneumonia in children. Zhonghua Er Ke Za Zhi. 2019;57(8):625–630. doi:10.3760/cma.j.issn.0578-1310.2019.08.011
25. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of a Nomogram for Predicting Massive Necrotizing Pneumonia in Children
Luo Y, Wang Y
Infection and Drug Resistance 2023, 16:1829-1838
Published Date: 29 March 2023
The Impact of mNGS Technology in the Etiological Diagnosis of Severe Pneumonia in Children During the Epidemic of COVID-19
Yu C, Guo W, Zhang Z, Ma Y, Cao X, Sun N, Cui Y, Wang Y, Cui W, Xu Y, Zhan J
Infection and Drug Resistance 2023, 16:2395-2402
Published Date: 21 April 2023
Surge in Mycoplasma Pneumoniae infection and Respiratory Viruses Co-infection in Children With Community-Acquired Pneumonia in the Post-Pandemic
Chi J, Tang H, Wang F, Wang Y, Chen Z
Pediatric Health, Medicine and Therapeutics 2024, 15:279-288
Published Date: 7 September 2024
Clinical Characteristics of Mycoplasma pneumoniae Pneumonia in Children and Analysis of the Risk Factors for Severe Mycoplasma pneumoniae Pneumonia
Yang G, Qiao Y, Sun X, Yang T, Lv A, Deng M, Yu Q
Infection and Drug Resistance 2026, 19:412506
Published Date: 13 February 2026
Etiology and Epidemiology of Acute Lower Respiratory Infections Among Hospitalized Pediatric Patients in Northeastern China: A Retrospective Study from 2023 to 2025
Zhao HY, Zhang SY, Wang R, Zhang XY, Wang XF
Infection and Drug Resistance 2026, 19:591898
Published Date: 8 June 2026