")
Back to Journals » International Journal of General Medicine » Volume 14
Clinical Characteristics of Lipid Metabolism in Untreated Patients with Anti-MDA5 Antibody-Positive
Authors Huang W, Ren F, Luo L, Zhou J, Huang D, Tang L
Received 15 April 2021
Accepted for publication 24 May 2021
Published 14 June 2021 Volume 2021:14 Pages 2507—2512
DOI https://doi.org/10.2147/IJGM.S315885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Wenhan Huang, Feifeng Ren, Lei Luo, Jun Zhou, Dongmei Huang, Lin Tang
Department of Rheumatology and Immunology of the Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Lin Tang
Department of Rheumatology and Immunology of the Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
Email [email protected]
Objective: Clinical characterization of lipid metabolism in untreated patients with anti-melanoma differentiation-associated gene 5 antibodies-positive (anti-MDA5+).
Methods: Body-mass index (BMI), autoantibodies, lipid levels, and serum ferritin levels in 57 anti-MDA5+ patients were determined in the Department of Rheumatology and Immunology of the Second Affiliated Hospital of Chongqing Medical University.
Results: Plasma high-density lipoprotein (HDL) and apolipoprotein A1 (ApoA1) levels were significantly lower in deceased group than in the survival group (P < 0.05). Plasma levels of HDL and ApoA1 were significantly lower in patients who were simultaneously anti-MDA5+ and anti-Ro-52+ than in patients who were anti-MDA5+ alone (P < 0.05). Plasma levels of total cholesterol, low-density lipoprotein, HDL, and ApoA1 were significantly decreased in patients with high levels of serum ferritin compared with patients with low levels (P < 0.05). There were no significant differences in blood lipid levels between patients grouped according to BMI.
Conclusion: 1) HDL and ApoA1 levels are important indicators of poor prognosis in anti-MDA5+ patients; 2) Dysregulated lipid metabolism in anti-MDA5+ patients is closely associated with anti-Ro-52 antibody and ferritin levels but independent of BMI; 3) HDL involvement in inflammation and immune regulation merits close attention by rheumatologists.
Keywords: anti-melanoma differentiation-associated gene 5 antibodies, anti-Ro-52 antibody, lipid, high-density lipoprotein, apolipoprotein A1
Introduction
Polymyositis (PM) and dermatomyositis (DM) are severe chronic autoimmune diseases, characterized by muscle weakness and cutaneous lesions. In 2005, Sato et al1 first detected autoantibodies to a protein with a molecular weight of 140 kD in patients diagnosed with clinically amyopathic dermatomyositis. In 2009, Sato’s team further identified that this protein was anti-melanoma differentiation-associated gene 5 (MDA5) antibody.2 In addition to the typical skin lesions seen in anti-MDA5+ patients, such as V-sign, shawl sign, Gottron sign, skin ulcers,3 and subcutaneous calcification,4 rapidly progressive interstitial lung disease (RP-ILD),5,6 as well as high inflammation status7 has received increasing attention for its association with poor prognosis and high mortality.8,9
Recent studies have confirmed the close relationship between inflammation and dysregulated lipid metabolism.10 Raouf et al reported that total serum lipids were altered in patients with PM/DM compared to healthy individuals, which indicated the crucial role of lipid changes in muscle performance and inflammation.11 However, there are no studies on the characteristics of lipid metabolism in anti-MDA5+ patients. In this study, 57 anti-MDA5+ patients in our hospital were assessed. The characteristics of their lipid metabolism were explored to increase the understanding of anti-MDA5+ dermatomyositis among rheumatologists, thus providing useful scientific guidance for clinical use.
Methods
From September 2015 to September 2020, patients who were positive for anti-MDA5 antibodies of myositis-specific autoantibodies were recruited in this study. Fifty-seven anti-MDA5+ patients were all inpatients of the Second Affiliated Hospital of Chongqing Medical University (Chongqing, China) with complete clinical information. The diagnosis was based on the 2017 idiopathic inflammatory myopathies criteria.12 According to the Declaration of Helsinki, all patients were informed and consented to the publication of the data. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Chongqing Medical University.
Height, weight and body-mass index (BMI) of all 57 anti-MDA5+ patients were measured and calculated; plasma triglyceride, total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), apolipoprotein A1 (ApoA1), ApoB and ApoE levels were determined by biochemical methods; serum ferritin levels were measured by chemiluminescence; anti-MDA5 and anti-Ro-52 antibodies were measured by immunoblotting test using an OMRMUN assay kit (EUROIMMUN, Beijing, China).
The 57 anti-MDA5+ patients were divided into different groups according to disease outcome, BMI, presence of anti-Ro-52 antibody and serum ferritin level. The lipid metabolism characteristics in each group of patients were compared.
Statistical Analysis
All analyses were performed using SPSS 19.0 (IBM, Armonk, NY, USA), results are coincident with normal distribution and presented as means ± SD. Student’s t-test were used to compare two groups and P < 0.05 indicated a significant difference. Multiple comparisons were assessed by one-way ANOVA with Bonferroni correction; P < 0.05 was considered significant.
Results
Basic Information
There were 57 anti-MDA5+ patients, of whom 24 were male and 33 were female (male-to-female ratio of 1:1.375). Age of onset was 50.97 ± 12.84 years (50.96 ± 11.36 years for males and 50.97 ± 13.99 years for females).
Comparison of Blood Lipid Levels According to Outcome
The 57 anti-MDA5+ patients were comprised of 44 in the survival group and 13 in the deceased group. The results showed that HDL and ApoA1 levels were significantly lower in patients in the deceased group than in patients in the survival group, and the difference was statistically significant. The HDL levels in the deceased and survival groups were 0.70 ± 0.11 and 1.02 ± 0.26 mmol/L, respectively; the ApoA1 levels in the two groups were 0.98 ± 0.24 and 1.19 ± 0.29 g/L, respectively. The plasma levels of triglycerides, total cholesterol, LDL, ApoB and ApoE did not differ significantly between the two groups of patients (Table 1).
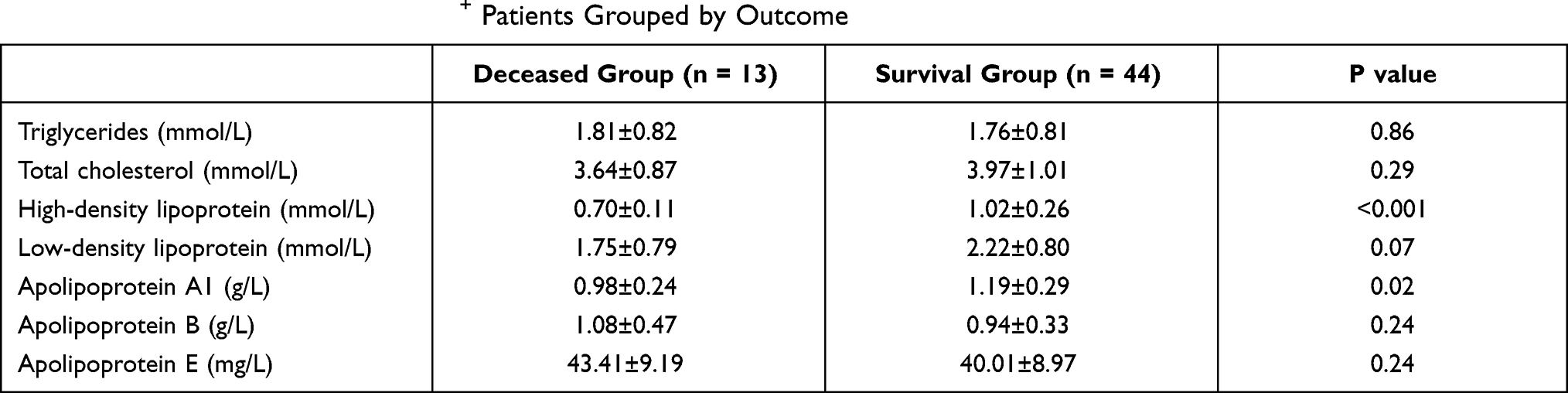 |
Table 1 Lipid Levels in 57 Anti-MDA5+ Patients Grouped by Outcome |
Comparison of Blood Lipid Levels According to BMI
The 57 anti-MDA5+ patients were divided into three groups according to BMI: <18.5 (n = 15), 18.5–24.9 (n = 35) and ≥25 (n = 7). Plasma triglycerides, total cholesterol, HDL, LDL, ApoA1, ApoB, and ApoE in the three groups of patients were compared separately. Although there was a trend for HDL, LDL, and ApoA1 to increase with increased BMI, no statistical differences were observed among the three groups of patients for all indicators (Table 2).
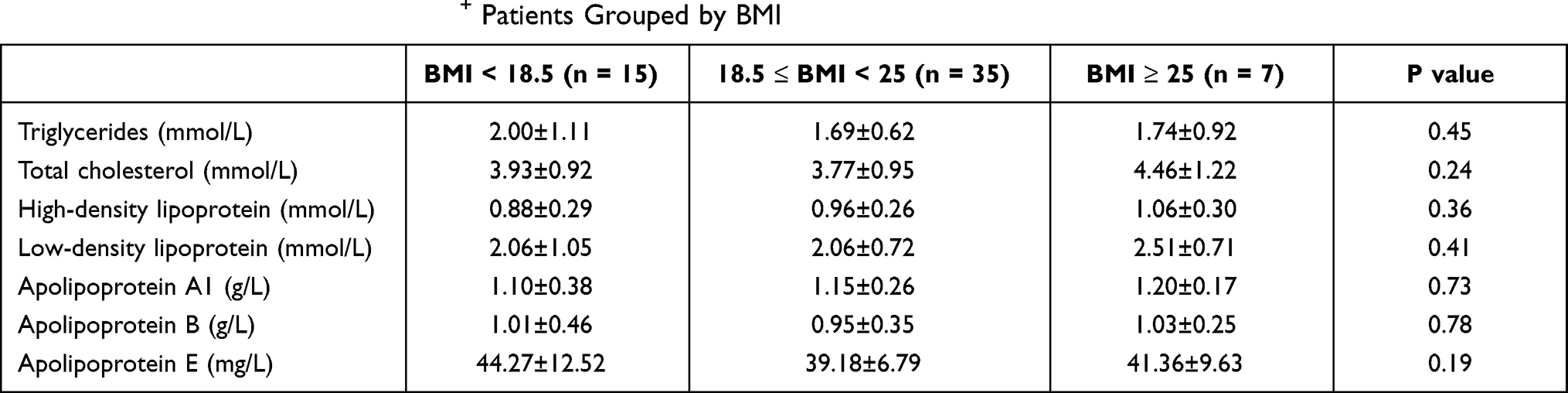 |
Table 2 Lipid Levels in 57 Anti-MDA5+ Patients Grouped by BMI |
Comparison of Blood Lipid Levels Based on Anti-Ro-52 Antibody Status
The 57 anti-MDA5+ patients included 38 anti-Ro-52+ and 19 anti-Ro-52− patients. Plasma HDL and ApoA1 levels were significantly lower in anti-MDA5+/anti-Ro-52+ patients than in anti-MDA5+ patients alone, and the differences were statistically significant. The HDL levels in anti-MDA5+/anti-Ro-52+ patients and in anti-MDA5+ patients were 0.86 ± 0.27 and 1.13 ± 0.18 mmol/L, respectively; ApoA1 levels were 1.07 ± 0.27 and 1.29 ± 0.26 g/L, respectively. Triglyceride, total cholesterol, LDL, ApoB, and ApoE levels were not significantly different between the two groups of patients (Table 3).
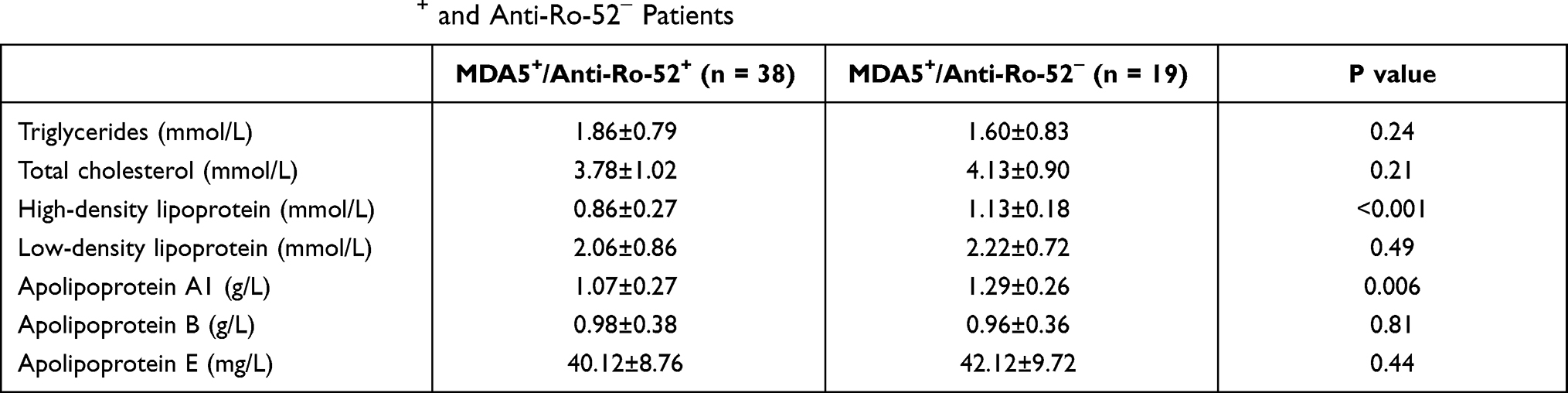 |
Table 3 Lipid Levels in Anti-Ro-52+ and Anti-Ro-52− Patients |
Comparison of Blood Lipid Levels According to Ferritin Levels
The 57 anti-MDA5+ patients were divided into three groups according to their serum ferritin levels: 0–500 ng/mL (n = 20, group 1), 500–1000 ng/mL (n = 15, group 2) and 1000–1500 ng/mL (n = 22, group 3). The total cholesterol levels in group 3 patients (3.39 ± 0.86 mmol/L) were significantly lower compared with group 1 (4.21 ± 1.04 mmol/L) and group 2 (4.21 ± 0.81 mmol/L) (Figure 1B, *P < 0.05). As serum ferritin levels increased, HDL levels decreased (group 1: 1.21 ± 0.19 mmol/L, group 2: 0.99 ± 0.15 mmol/L, group 3: 0.69 ± 0.11 mmol/L, Figure 1C, *P < 0.05). The LDL levels in group 3 patients (1.66 ± 0.69 mmol/L) were also lower than those of group 1 (2.33 ± 0.65 mmol/L) and group 2 (2.51 ± 0.91 mmol/L), and the difference was statistically significant (Figure 1D, *P < 0.05). In addition, ApoA1 levels were lowest in group 3 patients (group 1, 1.36 ± 0.24 mmol/L; group 2, 1.13 ± 0.18 mmol/L; group 3, 0.95 ± 0.25 mmol/L; Figure 1E, *P < 0.05). There were no significant differences in the levels of triglycerides (Figure 1A), ApoB (Figure 1F) or ApoE (Figure 1G) among the three groups.
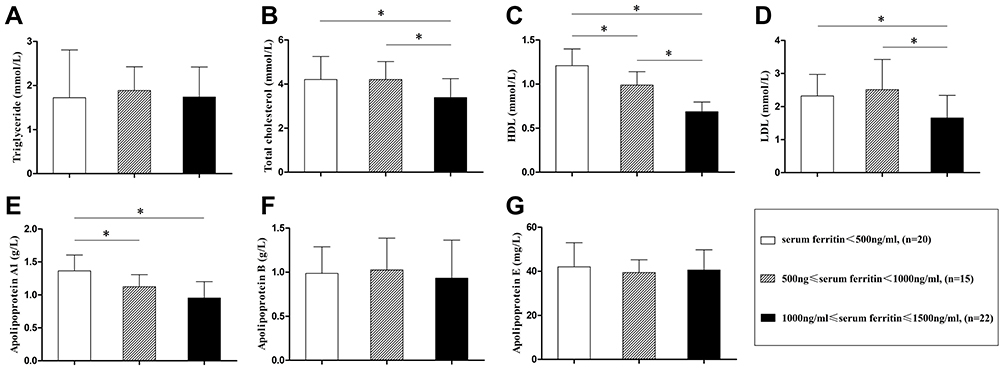 |
Figure 1 Lipid levels in patients grouped by serum ferritin levels. The levels of triglycerides (A), total cholesterol (B), high-density lipoprotein (C), low-density lipoprotein (D), apolipoprotein A1 (E), apolipoprotein B (F) and apolipoprotein E (G) were analyzed. 57 anti-MDA5+ patients were divided into three groups according to the serum ferritin levels (serum ferritin<500 ng/mL, 500≤serum ferritin<1000 ng/mL, 1000≤serum ferritin≤1500 ng/mL, respectively). *<0.05. |
Discussion
The poor outcome and high mortality of patients with anti-MDA5+ inflammatory myopathies have received increasing attention, and current research is predominantly focused on interstitial pneumonia.5,6 Autoimmune diseases often combine with disorders of lipid metabolism,13 but lipid metabolism in patients with anti-MDA5+ inflammatory myopathies has not been reported to date. In this study we set out, for the first time, to characterize lipid metabolism in anti-MDA5+ patients with the aim of deepening the understanding of this disease.
Based on a patient-by-patient comparison according to outcome, patients in the deceased group were found to be more likely to have decreased HDL and ApoA1 compared to the survival group. Our study confirmed for the first time that HDL and ApoA1 levels are strongly associated with poor prognosis in anti-MDA5+ patients, suggesting that lipid levels in these patients are an indicator that cannot be ignored by rheumatologists.
To further explore the causes of dysregulated lipid metabolism in anti-MDA5+ patients, we performed the following analyses. First of all, we grouped the 57 anti-MDA5+ patients according to their BMI and found that there were no significant differences in lipid levels among the patients. Although a large number of studies have reported14,15 that BMI correlates with lipid levels, we did not observe this in anti-MDA5+ patients.
Moreover, in our previous study,16 we found that patients who were both anti-MDA5+ and anti-Ro-52+ were more likely to develop serious complications such as RP-ILD, subcutaneous emphysema, and dysphagia, resulting in higher mortality. In addition, Bauhammer et al17 also reported a worse response to immunosuppression in patients with anti-synthetase syndrome when anti-Ro-52 antibodies were present. These studies strongly suggest an important role for anti-Ro-52 antibody in dermatomyositis. In this study, we compared patients according to whether they were also positive for anti-Ro-52 antibodies. Interestingly, HDL and ApoA1 levels were significantly reduced in patients who were both anti-MDA5+ and anti-Ro-52+ compared with patients who were anti-MDA5+ alone. We established for the first time that lipid metabolism in patients who were anti-MDA5+ was affected by anti-Ro-52 antibodies, but the specific mechanism for this effect needs more fundamental research.
Finally, our data revealed that plasma total cholesterol, LDL, HDL, and ApoA1 levels decreased to varying degrees as serum ferritin levels increased. We showed, for the first time, that lipid levels in anti-MDA5+ patients were negatively correlated with serum ferritin. Recent reports have been showed that dyslipoproteinemia is a common feature in dermatomyositis patients.11,18 Nevertheless, the underlying mechanisms of abnormal lipid profiles in untreated patients with anti-MDA5+ still remain unknown. We consider the following three reasons from limited evidence. First of all, it is well known that ferritin is an important indicator of the response to inflammation. The level of serum ferritin was increased when the body is under inflammatory circumstances. Krawczyk et al19 pointed out that iron is a potent inducer of reactive oxygen species, which have been found to increase the activity of hormone-sensitive lipase activity. Jarc et al20 also demonstrated that hormone-sensitive lipase would further promote fat mobilization and increase lipolysis, thereby providing energy to peripheral tissue cells during inflammation, this eventually resulted in dyslipidaemia. It might be an important reason why lipids were decreased in anti-MDA5+ patients. Secondly, lipid levels were affected by antibodies directly. In other rheumatic diseases, such as antiphospholipid antibody syndrome (APS), have shown the cross reactions between lipids and anti-β2G antibody. As serum lipoproteins contain phospholipids, they may become a potential target for antiphospholipid antibodies.21 We should point out that this conclusion mentioned above is based on the studies from APS patients. Further fundamental research is needed to clarify whether or not anti-MDA5 antibodies is related to lipid levels. Thirdly, in dermatomyositis and polymyositis patients, the necrotic muscle tissue would be further replaced by fat, which may affect the level of plasma lipids. However, muscle lesions were relatively mild in anti-MDA5+ patients. Therefore, the possibility of this affecting lipids is small.
Our data indicated that dyslipidemia in untreated patients with anti-MDA5+ were dominated by HDL and ApoA1 (ApoA1 is the main protein component of HDL). Intriguingly, similar studies have also been reported. In diabetic patients, poorly controlled diabetic subjects have lower HDL compared to the well-controlled diabetic patients.22 Meanwhile, HDL of the subjects with diabetic nephropathy have lower levels of HDL compared to the diabetic patients without diabetic nephropathy.23 These findings were considered to be associated with increased inflammatory burden. Besides, our study confirmed that HDL was strongly associated with poor prognosis in anti-MDA5+ patients. Current studies suggested that HDL, in addition to being associated with cardiovascular events, is also involved in immune modulation. Norata et al24 reported that HDL could affect antigen presentation functions in macrophages as well as B and T cell activation by modulating cholesterol bioavailability in the lipid rafts. Sphingosine-1 phosphate, a major active sphingolipid carried by HDL, could also modulate the function of macrophage and lymphocyte. Meanwhile, HDL is also a key modulator of inflammatory response in macrophages. Mendez et al25 mentioned that HDL could promote the efflux of free cholesterol from macrophages, which inhibiting the LPS-induced inflammatory response in macrophages. HDL replacement therapy has been a new strategy of sepsis research.26 It has been proved that the level of HDL positively correlated with survival rates in septic patients.27 Gono et al28 even proposed that anti-MDA5+ DM may be a type of macrophage activation syndrome mainly in the skin and lungs because of the increased serum ferritin, IL-1β, IL-6 and IL-18. Taking the above aspects into consideration, we believe that the low levels of HDL induced by inflammation could not reverse the activation of macrophages, resulting in the poor prognosis of anti-MDA5+ patients to some extent.
In summary, this study explores the clinical features of lipid metabolism in untreated patients with anti-MDA5 antibody-positive, deepening the understanding of this disease and providing a reliable basis for follow-up studies.
Author Contributions
Conceived and designed the manuscript: Wenhan Huang, Lin Tang.
Collected the data: Wenhan Huang, Feifeng Ren, Lei Luo, Jun Zhou, Dongmei Huang.
Analyzed the data: Wenhan Huang.
Wrote the paper: Wenhan Huang.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grant no. 81771738 from the National Natural Science Foundation of China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sato S, Hirakata M, Kuwana M, et al. Autoantibodies to a 140-kd polypeptide, CADM-140, in Japanese patients with clinically amyopathic dermatomyositis. Arthritis Rheum. 2005;52(5):1571–1576. doi:10.1002/art.21023
2. Sato S, Hoshino K, Satoh T, et al. RNA helicase encoded by melanoma differentiation-associated gene 5 is a major autoantigen in patients with clinically amyopathic dermatomyositis: association with rapidly progressive interstitial lung disease. Arthritis Rheum. 2009;60(7):2193–2200. doi:10.1002/art.24621
3. Muro Y, Sugiura K, Akiyama M. Cutaneous manifestations in dermatomyositis: key clinical and serological features-a comprehensive review. Clin Rev Allergy Immunol. 2016;51(3):
4. Huang W, Tang L. Extensive subcutaneous calcification: a rare manifestation of dermatomyositis. Rheumatology. 2019;58(6):974. doi:10.1093/rheumatology/key395
5. Abe Y, Kusaoi M, Tada K, Yamaji K, Tamura N. Successful treatment of anti-MDA5 antibody-positive refractory interstitial lung disease with plasma exchange therapy. Rheumatology. 2020;59(4):
6. Motegi SI, Sekiguchi A, Toki S, et al. Clinical features and poor prognostic factors of anti-melanoma differentiation-associated gene 5 antibody-positive dermatomyositis with rapid progressive interstitial lung disease. Eur J Dermatol. 2019;29(5):511–517. doi:10.1684/ejd.2019.3634
7. Shirakashi M, Nakashima R, Tsuji H, et al. Efficacy of plasma exchange in anti-MDA5-positive dermatomyositis with interstitial lung disease under combined immunosuppressive treatment. Rheumatology. 2020;59(11):3284–3292. doi:10.1093/rheumatology/keaa123
8. Yashiro M, Asano T, Sato S, et al. Anti-MDA5 antibody-positive hypomyopathic dermatomyositis complicated with pneumomediastinum. Fukushima J Med Sci. 2018;64(2):89–94. doi:10.5387/fms.2018-01
9. Huang K, Vinik O, Shojania K, et al. Clinical spectrum and therapeutics in Canadian patients with anti-melanoma differentiation-associated gene 5 (MDA5)-positive dermatomyositis: a case-based review. Rheumatol Int. 2019;39(11):1971–1981. doi:10.1007/s00296-019-04398-2
10. Zhang C, Wang K, Yang L, et al. Lipid metabolism in inflammation-related diseases. Analyst. 2018;143(19):4526–4536. doi:10.1039/C8AN01046C
11. Raouf J, Idborg H, Englund P, et al. Targeted lipidomics analysis identified altered serum lipid profiles in patients with polymyositis and dermatomyositis. Arthritis Res Ther. 2018;20(1):83. doi:10.1186/s13075-018-1579-y
12. Lundberg IE, Tjärnlund A, Bottai M, et al. 2017 European league against rheumatism/American college of rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Ann Rheum Dis. 2017;76(12):1955–1964. doi:10.1136/annrheumdis-2017-211468
13. Ryu H, Kim J, Kim D, Lee JE, Chung Y. Cellular and molecular links between autoimmunity and lipid metabolism. Mol Cells. 2019;42(11):747–754. doi:10.14348/molcells.2019.0196
14. Pinkas J, Bojar I, Gujski M, Bartosińska J, Owoc A, Raczkiewicz D. Serum lipid, vitamin D levels, and obesity in perimenopausal and postmenopausal women in non-manual employment. Med Sci Monit. 2017;23:5018–5026. doi:10.12659/MSM.906895
15. Wang X, Ding X, Su S, et al. Heritability of insulin sensitivity and lipid profile depend on BMI: evidence for gene-obesity interaction. Diabetologia. 2009;52(12):2578–2584. doi:10.1007/s00125-009-1524-3
16. Huang W, Ren F, Wang Q, et al. Clinical features of thirty-two patients with anti-melanoma differentiation-associated gene 5 antibodies. Clin Exp Rheumatol. 2019;37(5):803–807.
17. Bauhammer J, Blank N, Max R, et al. Rituximab in the treatment of Jo1 antibody-associated antisynthetase syndrome: anti-Ro52 positivity as a marker for severity and treatment response. J Rheumatol. 2016;43(8):1566–1574. doi:10.3899/jrheum.150844
18. Kozu KT, Silva CA, Bonfá E, et al. Dyslipidaemia in juvenile dermatomyositis: the role of disease activity. Clin Exp Rheumatol. 2013;31(4):638–644.
19. Krawczyk SA, Haller JF, Ferrante T, Zoeller RA, Corkey BE, Rishi A. Reactive oxygen species facilitate translocation of hormone sensitive lipase to the lipid droplet during lipolysis in human differentiated adipocytes. PLoS One. 2012;7(4):e34904. doi:10.1371/journal.pone.0034904
20. Jarc E, Petan T. Lipid droplets and the management of cellular stress. Yale J Biol Med. 2019;92(3):435–452.
21. Sadanand S, Paul BJ, Thachil EJ, Meletath R. Dyslipidemia and its relationship with antiphospholipid antibodies in APS patients in North Kerala. Eur J Rheumatol. 2017;3(4):161–164. doi:10.5152/eurjrheum.2016.16041
22. Aktas G, Kocak MZ, Bilgin S, Atak BM, Duman TT, Kurtkulagi O. Uric acid to HDL cholesterol ratio is a strong predictor of diabetic control in men with type 2 diabetes mellitus. Aging Male. 2020;23(5):1098–1102. doi:10.1080/13685538.2019.1678126
23. Kocak MZ, Aktas G, Duman TT, Atak BM, Savli H. Is Uric Acid elevation a random finding or a causative agent of diabetic nephropathy? Rev Assoc Med Bras. 2019;65(9):1155–1160. doi:10.1590/1806-9282.65.9.1156
24. Norata GD, Pirillo A, Ammirati E, Catapano AL. Emerging role of high density lipoproteins as a player in the immune system. Atherosclerosis. 2012;220(1):11–21. doi:10.1016/j.atherosclerosis.2011.06.045
25. Mendez AJ, Lin G, Wade DP, Lawn RM, Oram JF. Membrane lipid domains distinct from cholesterol/sphingomyelin-rich rafts are involved in the ABCA1-mediated lipid secretory pathway. J Biol Chem. 2001;276(5):3158–3166. doi:10.1074/jbc.M007717200
26. Krause BR, Remaley AT. Reconstituted HDL for the acute treatment of acute coronary syndrome. Curr Opin Lipidol. 2013;24(6):480–486. doi:10.1097/MOL.0000000000000020
27. Barlage S, Gnewuch C, Liebisch G, et al. Changes in HDL-associated apolipoproteins relate to mortality in human sepsis and correlate to monocyte and platelet activation. Intensive Care Med. 2009;35(11):1877–1885. doi:10.1007/s00134-009-1609-y
28. Gono T, Sato S, Kawaguchi Y, et al. Anti-MDA5 antibody, ferritin and IL-18 are useful for the evaluation of response to treatment in interstitial lung disease with anti-MDA5 antibody-positive dermatomyositis. Rheumatology. 2012;51(9):1563–1570. doi:10.1093/rheumatology/kes102
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.