Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
Clinical characteristics of COPD patients with tidal expiratory flow limitation
Authors Dean J ![]() , Kolsum U
, Kolsum U ![]() , Hitchen P, Gupta V, Singh D
, Hitchen P, Gupta V, Singh D
Received 24 March 2017
Accepted for publication 13 April 2017
Published 22 May 2017 Volume 2017:12 Pages 1503—1506
DOI https://doi.org/10.2147/COPD.S137865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
James Dean,1 Umme Kolsum,1,2 Paul Hitchen,1 Vandana Gupta,1 Dave Singh1,2
1Medicines Evaluation Unit, Manchester, 2Division of Infection, Immunity and Respiratory Medicine, School of Biological Sciences, Faculty of Biology, Medicine and Health, Manchester Academic Health Science Centre, The University of Manchester and University Hospital of South Manchester NHS Foundation Trust, Manchester, UK
Abstract: We have used impulse oscillometry to identify COPD patients with tidal expiratory flow limitation (EFL), which is a measurement related to small airway disease. We report that 37.4% of COPD patients had EFL; these patients had multiple clinical characteristics of more severe disease including lower forced expiratory volume in 1 second values, greater hyperinflation, reduced exercise performance, and increased small airway impairment. We highlight that EFL can be used to identify a subgroup of COPD patients with distinct characteristics associated with small airway disease.
Keywords: COPD, expiratory flow limitation, IOS, small airway, reactance
Introduction
COPD is a heterogeneous condition, with pathophysiological abnormalities that vary in severity between patients.1 Small airway inflammation is a common feature of COPD,2 causing a reduction of the cross-sectional area of the small airway lumen. Small airway narrowing and collapse can cause gas trapping on expiration and hyperinflation.3 The presence of hyperinflation is associated with greater dyspnea and reduced exercise tolerance.4
Impulse oscillometry (IOS) measures respiratory resistance and reactance during tidal breathing using sound waves of different frequencies.5 Resistance is the loss of energy arising from friction or turbulence, while reactance is the capacity for energy storage, which is dependent on the elastic properties of the lungs. COPD patients typically have increased total airway resistance and a greater negative reactance compared to healthy subjects.6
Small airway narrowing and closure during expiration can prevent low-frequency oscillometric signals from traveling to the distal lung.6 These regional “choke points” within the airway tree are present during expiration but not during inspiration, and cause expiratory flow limitation (EFL). EFL can be detected by a marked change in reactance during tidal breathing. Dellacà et al7 used within-breath analysis to show that the difference between inspiratory and expiratory reactance at 5 Hz (known as ΔX5) identifies EFL during tidal breathing in COPD patients; ΔX5 of 0.28 kPa/L/s has a high specificity and sensitivity for detecting EFL. COPD patients with higher ΔX5 values have greater dyspnea.6
The aim of this study was to quantify the proportion of COPD patients with EFL, and to further characterize the clinical characteristics of patients with EFL. We also studied whether the presence of EFL is stable after 2 years of follow-up.
Methods
A total of 147 COPD patients were recruited (75 from the COPDMAP cohort) with 45 patients attending for follow-up at 2 years. Patients were aged >40 years, with post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio of <0.7, ≥10 pack-year smoking history, and had no history of asthma. Patients experiencing an exacerbation within the preceding 6 weeks were excluded. The study was approved by the Greater Manchester Ethics Committees (ref: 10/H1003/108) and all patients provided written informed consent.
COPD patients performed the following procedures at baseline and 2-year visit: St George’s Respiratory Questionnaire (SGRQ), COPD Assessment Test (CAT), dyspnea visual analog scale (VAS), spirometry with reversibility, IOS (MasterScreen; Erich Jaeger, Hoechberg, Germany), plethysmography, diffusing capacity of the lungs for carbon monoxide (DLCO), and the 6-minute walk test, as previously described.8 Plethysmography, DLCO, and spirometry (Vmax, CareFusion, Hoechberg, Germany) were performed according to the ATS/ERS guidelines.9–11 ΔX5 was calculated as mean inspiratory reactance at 5 Hz (X5in) minus the mean expiratory reactance at 5 Hz (X5ex). EFL was defined as ΔX5 of ≥0.28 kPa/L/s.
Statistical analysis was performed using unpaired t-tests or Mann–Whitney U tests for comparison between groups at baseline; paired t-test or Wilcoxon matched pair tests for within patient comparisons at 2 years; and chi-square tests for categorical data. Pearson’s correlation or Spearman’s rank tests were used to assess associations. Analysis was performed using Prism 5 (Graphpad, La Jolla, CA, USA); P<0.05 was considered statistically significant.
Results
In all, 55 (37.4%) of the 147 COPD patients had EFL; see Table 1 for clinical characteristics. Patients with EFL were more likely to be current smokers (P=0.01), have worse airflow obstruction (mean 42 versus 59 FEV1% predicted; P<0.0001); and have more gas trapping with a higher RV (median 166 versus 121% predicted; P<0.0001) and FRC (mean 144 versus 122% predicted; P<0.0003). The EFL group had worse SGRQ activity and symptom component scores and lower 6-minute walk distance.
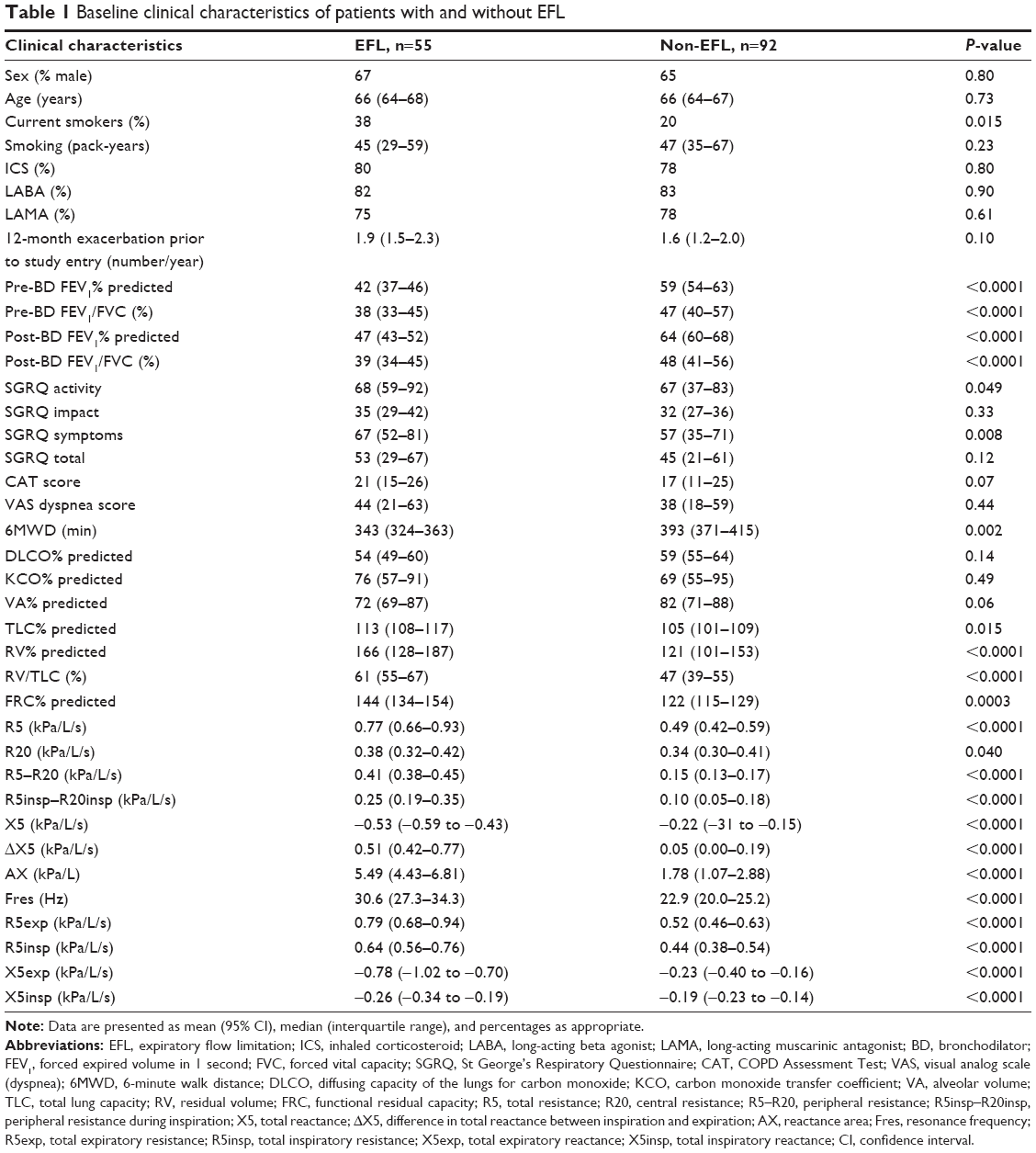 | Table 1 Baseline clinical characteristics of patients with and without EFL |
There were significant differences between groups for all IOS measurements; notably, R5–R20 was greater in the EFL group. ΔX5 was significantly associated with R5–R20 (r=0.87, P<0.0001), FEV1% predicted (r=−0.49, P<0.0001), FEV1/FVC (r=−0.27, P=0.001), hyperinflation (RV% predicted: r=0.37, P<0.0001; FRC% predicted: r=0.33, P=0.0003), CAT score (r=0.21, P=0.011), and SGRQ total score (r=0.22, P=0.009) including all the SGRQ domains (symptoms, impact, and activity). There was no association between ΔX5 and the VAS dyspnea scale (r=0.11, P=0.22).
A total of 45 patients returned at 2 years. In all, 20 patients had EFL at baseline, of which 14 (70%) had EFL at 2 years. For the remaining 6 patients without EFL at 2 years, the median ΔX5 changed from 0.44 kPa/L/s at baseline to 0.24 kPa/L/s after 2 years (P=0.031). A total of 25 patients did not have EFL at baseline; 21 (82%) remained without EFL at 2 years. Overall, there were no significant changes in ΔX5 values between baseline and 2 years for both the EFL and non-EFL groups. FEV1 decreased in both the groups (mean changes: EFL: −66.5 mL/year, P=0.003; non-EFL: −71 mL/year, P=0.0005).
Discussion
EFL was a common finding in COPD patients, being present in over a third of the cohort. EFL patients had a lower FEV1% predicted and more hyperinflation and gas trapping, with reduced exercise performance. R5–R20 is recognized as a measurement of small airway resistance5; EFL was associated with greater small airway impairment. This association is compatible with the cause of EFL, namely small airway narrowing and collapse.
Dellacà et al7 proposed the ΔX5 threshold value of 0.28 kPa/L/s for EFL using results from forced oscillometry data during individual breathing cycles. We used mean data from multiple breathing cycles during IOS, which may categorize some patients with EFL despite not all cycles reaching the EFL threshold. Nevertheless, using this method to define EFL we identified a subgroup of patients with marked small airway disease, gas trapping, and hyperinflation. Furthermore, the identification of EFL was reproducible in the majority of cases at the 2-year follow-up.
Aarli et al6 used IOS to measure EFL in COPD patients, and also found that EFL was associated with lower FEV1 values and greater hyperinflation. In common with our findings, a significant association with worse health status and symptom scores was also reported. While there were some differences in the patient-reported outcome tools used, the overall interpretation of these two studies is that the presence of EFL is associated with a greater symptom burden in COPD patients.
Aarli et al6 reported that COPD patients with ΔX5 ≥0.1 kPa/L/s experienced greater dyspnea. Healthy subjects have ΔX5 values around zero. The ΔX5 ≥0.1 kPa/L/s threshold value is obviously lower than that used in the current study, and is likely to identify patients with less severe EFL. The higher ΔX5 threshold value used in this study identified a group with greater EFL that was associated with more severe disease manifestations.
It has been reported that ΔX5 is associated with the level of symptoms and duration of hospitalization during COPD exacerbations.12 Treatment with an inhaled corticosteroid/long-acting beta-agonist combination for 3 months improved ΔX5.13 The identification of small airway disease and EFL in COPD patients using oscillometry methods may allow individualized targeting of drugs to treat these pathophysiological abnormalities. For example, inhalers with a greater proportion of extra-fine particles14 could be targeted to COPD patients with EFL.
We recruited a reasonable size cohort that was clinically characterized in detail at baseline. There was limited follow-up at 2 years, and larger cohort studies are needed to build on the observations here about the long-term clinical implications of EFL.
Conclusion
We have long recognized that small airway disease2 and EFL6,7 are features of COPD. We show that IOS can identify patients with EFL, and that EFL is associated with more severe airflow obstruction, hyperinflation, and symptoms. We suggest that EFL is a “treatable trait”,15 and may provide an opportunity for therapeutic intervention.
Disclosure
Dave Singh has received sponsorship to attend international meetings, honoraria for lecturing or attending advisory boards, and research grants from various pharmaceutical companies including Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Genentech, GlaxoSmithKline, Glenmark, Merck, NAPP, Novartis, Pfizer, Respivert, SkyePharma, Takeda, Teva, Therevance, and Verona. The other authors report no conflicts of interest in this work.
References
Singh D, Roche N, Halpin D, Agusti A, Wedzicha JA, Martinez FJ. Current controversies in the pharmacological treatment of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2016;194(5):541–549. | ||
Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. | ||
Thomas M, Decramer M, O’Donnell DE. No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J. 2013;22(1):101–111. | ||
Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:187–201. | ||
Bickel S, Popler J, Lesnick B, Eid N. Impulse oscillometry: interpretation and practical applications. Chest. 2014;146(3):841–847. | ||
Aarli BB, Calverley PM, Jensen RL, Eagan TM, Bakke PS, Hardie JA. Variability of within-breath reactance in COPD patients and its association with dyspnoea. Eur Respir J. 2015;45(3):625–634. | ||
Dellacà RL, Santus P, Aliverti A, et al. Detection of expiratory flow limitation in COPD using the forced oscillation technique. Eur Respir J. 2004;23(2):232–240. | ||
Ravi AK, Khurana S, Lemon J, et al. Increased levels of soluble interleukin-6 receptor and CCL3 in COPD sputum. Respir Res. 2014;15:103. | ||
Wanger J, Clausen JL, Coates A, et al. Standardisation of the measurement of lung volumes. Eur Respir J. 2005;26(3):511–522. | ||
Macintyre N, Crapo RO, Viegi G, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005;26(4):720–735. | ||
Miller MR, Hankinson J, Brusasco V, et al; ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. | ||
Jetmalani K, Timmins S, Brown NJ, et al. Expiratory flow limitation relates to symptoms during COPD exacerbations requiring hospital admission. Int J Chron Obstruct Pulmon Dis. 2015;10:939–945. | ||
Timmins SC, Diba C, Schoeffel RE, Salome CM, King GG, Thamrin C. Changes in oscillatory impedance and nitrogen washout with combination fluticasone/salmeterol therapy in COPD. Respir Med. 2014;108(2):344–350. | ||
Singh D, Corradi M, Spinola M, Petruzzelli S, Papi A. Extrafine beclometasone diproprionate/formoterol fumarate: a review of its effects in chronic obstructive pulmonary disease. NPJ Prim Care Respir Med. 2016;26:16030. | ||
Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.