")
Back to Journals » International Journal of General Medicine » Volume 17
Clinical Characteristics of Children Infected with SARS-CoV-2 Omicron (B.1.1.529) in China’s Shanghai
Authors Shu J, Jia L, Zhang P, Wang R, Wang M, Sun X, Peng Y, Wang P, Li X, Tang Z, Han T, Ju T, Wei Y, Pang W, Gao C, Xia Z
Received 10 July 2023
Accepted for publication 20 October 2023
Published 23 January 2024 Volume 2024:17 Pages 245—251
DOI https://doi.org/10.2147/IJGM.S429870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jiaping Shu,1,* Lili Jia,2,* Pei Zhang,2 Ren Wang,2 Meiqiu Wang,2 Xiaoyi Sun,2 Yingchao Peng,2 Peipei Wang,2 Xiaojie Li,2 Zilu Tang,3 Tingting Han,3 Tao Ju,3 Yaqin Wei,4 Wei Pang,5 Chunlin Gao,2 Zhengkun Xia1
1Department of Pediatrics, School of Medicine, Southeast University, Nanjing, Jiangsu, 210009, People’s Republic of China; 2Department of Pediatrics, Jinling Hospital, Nanjing University, Nanjing, Jiangsu, 210093, People’s Republic of China; 3Department of Pediatrics, Jinling Hospital, Nanjing Medical University, Nanjing, Jiangsu, 210093, People’s Republic of China; 4Department of Pediatrics, Jinling Hospital, The First School of Clinical Medicine, Southern Medical University, Guangzhou, Guangdong, 510000, People’s Republic of China; 5Department of Military Information, Chinese People’s Liberation Army 31102, Nanjing, Jiangsu, 210000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhengkun Xia, Department of Pediatrics, School of Medicine, Southeast University, Nanjing, Jiangsu, 210009, People’s Republic of China, Email [email protected] Chunlin Gao, Department of Pediatrics, Jinling Hospital, Nanjing University, Nanjing, Jiangsu, 210093, People’s Republic of China, Email [email protected]
Introduction: The pandemic of SARS-CoV-2 brings great challenge and threats to humans worldwide. Multiple variants of SARS-CoV-2 tend to be epidemic, among which Omicron is highly infectious within China. The aim of this study was to analyze the clinical characteristics of children infected with SARS-CoV-2 variant B.1.1.529 (Omicron) in the Shanghai, China.
Methods: We included 9378 pediatric patients diagnosed with Omicron and treated in the Shanghai International Convention and Exhibition Center between April 1, 2022 and May 31, 2022. We recorded and summarized the clinical characteristics, infectious conditions and biological features of the children infected with Omicron.
Results: A total of 9355 paediatric patients were treated in isolation since Makeshift became available, including 5564 males (59.48%) and 3791 females (40.52%). More than half (55.56%) of the affected children were identified at premises screening. The number of symptomatic or asymptomatic patients was 4530 (48.42%) and 4825 (51.58%), respectively. Initial signs or symptoms in asymptomatic patients included fatigue (3582, 38.29%), cough (560, 5.99%), fever (242, 2.59%) and other (146, 1.56%). Age and number of vaccinations in paediatric patients were negatively associated with the number of days from positive to negative nucleic acid test results.
Conclusion: Age and number of vaccinations were key factors influencing the conversion of nucleic acid test results in paediatric patients. Early childhood vaccination is encouraged to establish a complete immune barrier.
Keywords: Omicron variant, COVID-19, child patients, clinical characteristics
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has become a huge threat to global public health. Omicron, a nomenclature of the SARS-CoV-2 variant B.1.1.529, which was firstly reported by the World Health Organization on Nov 24, 2021.1 The Omicron variant presented higher transmissibility when compared with the Delta variant and other variants.2,3
Currently, BQ.1, BQ.1.1, and XBB have become the new predominant strains worldwide. Data from the official website of the Chinese Center for Disease Control and Prevention and monitoring results from Beijing Children’s Hospital affiliated to Capital Institute of Pediatrics both indicate that the prevalent strains in China are mainly BA.5.2 and its variant BF.7. Omicron infection is characterized by a shorter incubation period (1–3 days), high viral load, and rapid spread of the epidemic, making it difficult to control. With the emergence of its variants, there has been a sharp increase in children infected, often resulting in clustered infections within families and schools. According to the official report of Shanghai, a new patient was diagnosed with COVID-19 and a new asymptomatic carrier on Mar 3, 2022. What is worse, the diagnosed cases were increased to 326 in Mar 29 from 96 cases in Mar 28. Meanwhile, 5656 new asymptomatic carriers were reported. In the next half month, the curve of average daily new diagnosed cases was almost increased in 90 degrees. Sometimes, the daily new diagnosed cases were more than 20,000. According to the genetic sequencing results for virus announced by Shanghai Center for Disease Control, the current outbreak was all induced by Omicron BA.2 variant and Omicron BA.2.2 variant. To data, more than 600,000 citizens have been infected by Omicron variant in Shanghai. The sub-variant BA.2 has gradually become the new challenge in the pandemic of COVID-19 due to high transmissibility, fast spreading speed and difficulty for detection.
As a new-founded variant of COVID-19, Omicron is fast spreading in the world range. The epidemiology, pathogenic characteristics, clinical diagnosis, treatment and prevention are still being observed and concluded. Several studies have indicated that the number of child patients infected with Omicron is surpassing the number of child patients infected with Omicron in those previous waves.4,5 Although lots of reports about the Omicron variants have been made, there are few reports on the diagnosis and treatment of Chinese child patients. In the current study, we collected a total of 9378 cases (9355 cases with effective data) to analyze the clinical characteristics of child patients with mild symptoms who infected Omicron. Our findings will be conducive to providing new suggestions for prevention and treatment of child infected with Omicron variant.
Materials and Methods
Patient Recruitment
All data were obtained from 9378 child patients who were hospitalized in the Shanghai International Convention and Exhibition Center. Diagnosis was done by complying with the diagnostic standard for patients with the mild symptom based on the COVID-19 diagnosis and treatment protocols published by the National Health Commission. Patients enrolled in this study had no clinical symptom or mild symptom, and no pneumonia-related symptoms were identified in accordance with the imaging results. All child patients enrolled in this study were infected with Omicron variant but no other virus. The age of all patients was between 0 and 18. Patients did not finish data collection or had incomplete data (n = 23) were excluded from this study. The legal guardians of all patients signed the informed consent before the data collection.
Statistical Analysis
Data were analyzed using SPSS 25.0 software (IBM, USA). Group comparison was made using t test. Data that were not in normal distribution were shown as mean/median/mode±standard deviation (SD). All statistics were analyzed using two tailed test. P < 0.05 was considered statistically significant.
Results
A total of 9355 paediatric patients infected with the Omicron variant were included in this study, of whom 5564 (59.48%) were male and 3791 (40.52%) were female (Figure 1A). The mean age of all children was 11 ± 5 years, with a maximum of 18 years. All children were divided into five groups according to their age (Figure 1B), including 34 infants (babyhood, aged under 1 year), 505 toddlers (infancy stage, aged 1–3 years), 1311 preschoolers (preschool period, aged 4–6 years), 2037 schoolchildren (school period, aged 7–10 years) and 5468 adolescents (puberty, aged 11–18 years). Patients vaccinated with different numbers of doses were divided into four groups, including the 0-dose group (3106, 33.20%), the 1-dose group (560, 5.99%), the 2-dose group (5456, 58.32%) and the 3-dose group (233, 2.49%) (Figure 1C).
 |
Figure 1 Pie charts of all affected children according to different clinical variables. (A) Gender. (B) Age. (C) Vaccine. (D) Diagnostic approach. (E) Symptom. (F) Drug use. |
Diagnosis in hospitalised patients included screening in the community, school or company (5198, 55.56%), testing at nucleic acid testing sites (1704, 18.21%) and testing at fever clinics (2453, 26.22%) (Figure 1D). Of these, the number of symptomatic or asymptomatic patients was 4530 (48.42%) and 4825 (51.58%), respectively (Figure 1E). Initial signs or symptoms in asymptomatic patients included fatigue (3582, 38.29%), cough (560, 5.99%), fever (242, 2.59%) and other (146, 1.56%) (Figure 1E). In terms of treatment, 748 patients did not receive any medication, 2976 patients were treated with lianhua qingwen capsules, 2054 patients were treated with compound glycyrrhiza oral solution and 3577 patients were treated with other types of medication, most of which were treated with lianhua qingwen capsules (Figure 1F). All these data are shown in Table 1. For specific classifications of asymptomatic and symptomatic cases refer to Table 2.
 |
Table 1 Characteristics of Reported Confirmed SARS-CoV-2 Omicron (B.1.1.529) Cases in Shanghai International Convention Center Between April 1, 2022 and May 31, 2022 |
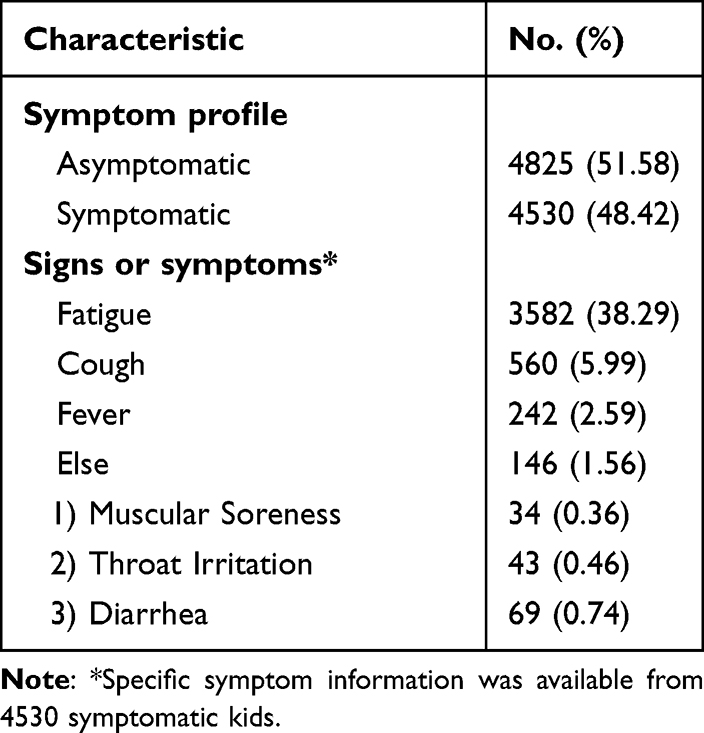 |
Table 2 Specific Classifications of Asymptomatic and Symptomatic Cases |
We recorded the number of days that a nucleic acid test result changed from positive to negative and explored the associated factors. The results showed that the number of days from positive to negative nucleic acid test results did not correlate significantly with gender (Figure 2A), diagnostic method (Figure 2B), symptoms (Figure 2E) and drug use (Figure 2F). We found that the number of vaccinations and age were significantly associated with the number of days to negative nucleic acid test results in paediatric patients, and both were negatively correlated (Figure 2C and D).
 |
Figure 2 Time to change from positive to negative nucleic acid for all affected children according to different clinical variables. (A) Gender. (B) Diagnostic approach. (C) Vaccine. (D) Age. (E) Symptom. (F) Drug use. ****P<0.001. Abbreviation: ns, non-statistical significance. |
In addition, we examined the vaccination status of patients of different ages and genders. The results showed a vaccination rate of 68% in male patients and 66% in female patients (Figure 3A). Vaccination rates tended to increase with age, with vaccination rates of 9%, 8%, 37%, 77% and 76% in patients of infancy, preschool, school age and adolescence, respectively (Figure 3B).
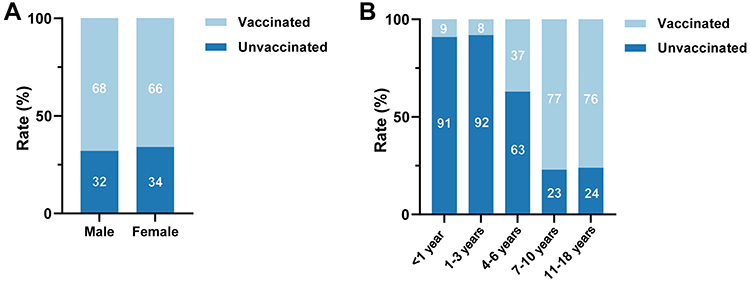 |
Figure 3 Vaccination rates for affected children of different genders and ages. (A) Gender. (B) Age. |
Discussion
The current study collected child cases in the Shanghai International Convention and Exhibition Center in China, which is the first study to reveal the details of the child patients in the current outbreak. Many studies have reported in adults or unspecified age groups.6–10 However, there are few specific studies for child patients.
In this study, we collected and analyzed 9355 valid child cases. We classified all these cases in accordance with their sex, age, diagnostic methods, symptom, therapeutic methods and building number. We found that age of child patients was negatively correlated with the number of days when the result of nucleic acid test turned into negative. These findings indicated that the elder patients had a shorter cure time than the younger patients. Therefore, self-immunity is a factor for the recovery of child patients infected with Omicron variant. Summary observation found that children are mainly light and medium, mainly manifested as fatigue, mainly in the middle and high fever, but about 2 days after the fever; The systemic symptoms were more prominent in weakness. The main respiratory symptoms, common muscular soreness, cough, sore throat (pharyngeal discomfort); cough is characterized by cough after fever and mainly dry cough with little sputum, which can be cured within 1 week. Diarrhea and other gastrointestinal symptoms were less; Severe disease is rare; Due to the young age of some children, the poor ability of private reporting leads to incomplete taste and smell recording data, and the influence of older children’s private reporting is not obvious. Because of the unique physiological and immune characteristics, the clinical phenotype of children infected with Omicron variant strains also changed. It may be because the mucosal immune system of upper respiratory tract in children is in a pre-activated state compared with adults, so interferon can be released in the early stage of SARS-Co V-2 infection and control the infection.
To date, vaccination remains the crucial way to fortify people’s immuno-barrier. Leshem and Lopman reported that population immunity could be achieved when nearly 100% of population need to be vaccinated in the absence of naturally acquired immunity.11 Clinical evidences have shown that COVID-19 vaccination protects against severe symptoms of the disease and is also an effective tool to prevent the spread of the virus and decrease the rate of infection.12,13 By Feb 7, 2022, Chinese people have received 301.0669 million shots of COVID-19 vaccination, among which, people have received two shots reach 87.10%. In the current study, patients received four different shot number of vaccination. There are 3106 patients were unvaccinated, 560 patients received 1 shot, 5456 patients received 2 shots, 233 patients received 3 shots. According to the test results for nucleic acid, the child patients received 2 or 3 shots had shorter cure time than those received 0 or 1 shot. Thus, vaccination remains an effective strategy for preventing infection. Importantly, vaccination is effective for child patients to strengthen their immuno-barrier.
Conclusions
The current study shows that self-immunity of these child patients could affect the cure time. Child patients who vaccinated with two shots or the booster shot had shorter cure time than others. Therefore, the regular and complete vaccination is conducive to establish immune-barrier.
Ethics Approval
Ethics approval was granted by the Jinling Hospital, Nanjing University Ethics Committee (JSNJ 528/2022). All studies comply with the Declaration of Helsinki.
Funding
We thank the “Jiangsu Provincial pediatric medical innovation team, Jiangsu Provincial Health and Family Planning Commission (CXTDA2017022)”.
Disclosure
The authors declare that they have no conflict interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. He X, Hong W, Pan X, Lu G, Wei X. SARS-CoV-2 Omicron variant: characteristics and prevention. MedComm. 2021;2(4):838–845. doi:10.1002/mco2.110
2. Araf Y, Akter F, Tang Y-D. Omicron variant of SARS-CoV-2: genomics, transmissibility, and responses to current COVID-19 vaccines. J Med Virol. 2022;94(5):1825–1832. doi:10.1002/jmv.27588
3. Hoffmann M, Kruger N, Schulz S, et al. The Omicron variant is highly resistant against antibody-mediated neutralization: implications for control of the COVID-19 pandemic. Cell. 2022;185(3):447–456 e411. doi:10.1016/j.cell.2021.12.032
4. Iuliano AD, Brunkard JM, Boehmer TK, et al. Trends in disease severity and health care utilization during the early Omicron variant period compared with previous SARS-CoV-2 high transmission periods - United States, December 2020–January 2022. MMWR Morb Mortal Wkly Rep. 2022;71(4):146–152. doi:10.15585/mmwr.mm7104e4
5. Abdullah F, Myers J, Basu D, et al. Decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in Tshwane, South Africa. Int J Infect Dis. 2022;116:38–42. doi:10.1016/j.ijid.2021.12.357
6. Lu L, Mok BW, Chen LL, et al. Neutralization of SARS-CoV-2 Omicron variant by sera from BNT162b2 or Coronavac vaccine recipients. Clin Infect Dis. 2021;73(11):e4012–e4019. doi:10.1093/cid/ciaa1417
7. Zhang L, Li Q, Liang Z, et al. The significant immune escape of pseudotyped SARS-CoV-2 variant Omicron. Emerg Microb Infect. 2022;11(1):1–5. doi:10.1080/22221751.2021.2017757
8. Dejnirattisai W, Shaw RH, Supasa P, et al. Reduced neutralisation of SARS-CoV-2 omicron B.1.1.529 variant by post-immunisation serum. Lancet. 2022;399(10321):234–236. doi:10.1016/S0140-6736(21)02844-0
9. Cameroni E, Bowen JE, Rosen LE. Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shift. Nature. 2022;602(7898):664–670. doi:10.1038/s41586-021-04386-2
10. Meo SA, Meo AS, Al-Jassir FF, Klonoff DC. Omicron SARS-CoV-2 new variant: global prevalence and biological and clinical characteristics. Eur Rev Med Pharmacol Sci. 2021;25(24):8012–8018. doi:10.26355/eurrev_202112_27652
11. Leshem E, Lopman BA. Population immunity and vaccine protection against infection. Lancet. 2021;397(10286):1685–1687. doi:10.1016/S0140-6736(21)00870-9
12. Vitiello A, Ferrara F, Troiano V, La Porta R. COVID-19 vaccines and decreased transmission of SARS-CoV-2. Inflammopharmacology. 2021;29(5):1357–1360. doi:10.1007/s10787-021-00847-2
13. Sreepadmanabh M, Sahu AK, Chande A. COVID-19: advances in diagnostic tools, treatment strategies, and vaccine development. J Biosci. 2020;45(1). doi:10.1007/s12038-020-00114-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.