")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Characteristics, Drug Resistance, and Risk Factors for Death of Klebsiella pneumoniae Infection in Patients with Acute Pancreatitis: A Single-Center Retrospective Study from China
Authors Jia Y, Liu Y, Huang Y, Wang J, Wang H, Tan S, Shi Y , Wang Q, Peng J
Received 4 May 2023
Accepted for publication 20 July 2023
Published 7 August 2023 Volume 2023:16 Pages 5039—5053
DOI https://doi.org/10.2147/IDR.S410397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Yan Jia,1,* Ya Liu,1,* Yilin Huang,1,* Jie Wang,1 Hanyue Wang,1 Shu Tan,2 Yuxin Shi,1 Qingxia Wang,3 Jie Peng1
1Department of Gastroenterology, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2Department of Emergency, Loudi Central Hospital, Loudi, Hunan, People’s Republic of China; 3Gastrointestinal Endoscopy Center, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Peng, Department of Gastroenterology, Xiangya Hospital, Central South University, 87 Xiangya Road, Changsha, Hunan, People’s Republic of China, Tel/Fax +86-731-89753722, Email [email protected] Qingxia Wang, Gastrointestinal Endoscopy Center, Xiangya Hospital, Central South University, 87 Xiangya Road, Changsha, Hunan, People’s Republic of China, Tel/Fax +86-15874189639, Email [email protected]
Objective: Infection is a common complication of acute pancreatitis (AP). Klebsiella pneumoniae (KP) is one of the most common pathogens associated with nosocomial infections. Our study focuses on investigating the clinical characteristics and risk factors for death of Klebsiella pneumoniae infections in AP patients, further to quantify the prognosis of the patients, and provide evidence for guiding antibiotic use and improving prognosis.
Methods: The data of epidemiology, clinical manifestations and drug resistance rate with K. pneumoniae infections in AP patients from January 1, 2012 to August 30, 2022 were retrospectively collected. Logistic regression model and Cox regression model were, respectively, used to determine the risk factors for carbapenem-resistant Klebsiella pneumoniae (CRKP) acquisition and death. The nomogram prediction model was built by RMS software package to predict the 90-day survival rate.
Results: One hundred and twenty-six AP patients combined with K. pneumoniae infections, with a mortality rate of 34.9%. The most common infection sites were pancreas and peri-pancreas (54.8%), followed by lung (20.6%) and blood stream (18.3%). The resistance rate of K. pneumoniae to commonly used antibiotics in clinical practice was high, especially CRKP, which was only sensitive to sulfamethoxazole-trimethoprim (SMZ-TMP) and tigecycline (TGC) (resistance rates were 37.57% and 17.57%, respectively). Independent risk factors for CPKP acquisition were male (OR = 1.655, 95% CI 0.642– 4.265, P = 0.017) and PICC/CVC implantation (OR = 3.157, 95% CI 1.223– 8.147, P = 0.021). Independent risk factors for mortality included carbapenem resistance (HR = 2.556, 95% CI 1.011– 6.462, P = 0.047), hemorrhage (HR = 2.392, 95% CI 1.104– 5.182, P = 0.027), septic shock (HR = 3.022, 95% CI 1.312– 6.959, P = 0.009), age > 60 years (HR = 2.977, 95% CI 1.303– 6.799, P = 0.01), creatinine > 177μmol/L (HR = 2.815, 95% CI 1.075– 7.369, P = 0.035).
Conclusion: K. pneumoniae infection has become a serious threat for AP patients, which recommends us more attention and active new strategies seeking.
Keywords: Klebsiella pneumoniae, carbapenems, drug resistance, acute pancreatitis, mortality, risk factors, nomogram
Introduction
Acute pancreatitis (AP) is the most common gastrointestinal (GI) disorder requiring emergency admission.1 The disease is characterized by local and systemic inflammatory responses and has a diverse clinical course. In most mild cases, moderate fluid resuscitation, control of pain and nausea, and early oral feeding could promise a rapid clinical improvement. The severe form accounts for about 20% to 30% of patients, which is life-threatening and with a hospital mortality rate of about 15%.2 Infection is one of the common complications of AP, and nearly one-third of AP patients develop extra-pancreatic infection.3 The patients with acute necrotizing pancreatitis who subsequently develop pancreatic infection accounted for approximately one-third of the total.4 Despite decades of basic and clinical research on secondary infections of severe acute pancreatitis (SAP), strategies to prevent and control the infection remain inadequate for effective management. Gram-negative bacilli (GNB) are common infectious pathogens in SAP, most likely due to disruption of the normal intestinal barrier and ascent through the GI tract, and their translocation increases the mortality of SAP as has been reported previously.5 Klebsiella pneumoniae (KP) is one of the most common pathogens associated with nosocomial infections such as pneumonia, urinary tract infections, bloodstream infections, and sepsis. As the most common multidrug resistant organism (MDRO), the isolated and reported rate of carbapenem-resistant Klebsiella pneumoniae (CRKP) infections has been increasing worldwide, which is prominent in Asia compared with Europe and USA.6 It is found that the detection rate of CRKP in China increased significantly from 9.2% in 2010 to 27.1% in 2021.7 Owing to the high incidence and drug-resistant rate, CRKP infection has become an important public health threat in China, with limited treatment options and unsatisfactory outcomes. The literature reports that the proportion of KP infection in SAP patients with Gram negative bacterium infection can reach to 30%. The mortality rate of AP patients with multidrug resistant Klebsiella pneumoniae (MDR-K) was 46.5%.8 Although there have been some studies on KP infection in China, few of them focusing on the clinical characteristic, antibiotic resistance, risk factors, and clinical outcomes of CRKP infection in SAP patients. We aim to depict those aspects of CRKP infection in SAP patients, provide scientific evidence for antibiotic selection, and establish a quantified model for prognosis to improve patient clinical outcomes in the future.
Materials and Methods
Study Design
This retrospective cohort study was conducted at Xiangya Hospital, Central South University, a 3500-bed tertiary teaching hospital. The clinical data of moderate and severe AP patients with KP infection who were admitted from January 1, 2012 to August 30, 2022 was collected. The main departments for AP patients were pancreatic surgery, gastroenterology and intensive care unit (ICU), and were treated with the combined treatment strategy of internal medicine and surgery method. In our cohort, AP was diagnosed and classified based on the revised Atlanta classification criteria.5 Etiological diagnostic criteria: (1) Biliary: choledocholithiasis or cholelithiasis; (2) Hypertriglyceridemia: triglyceride >1000 mg/dL; (3) Excessive drinking: alcohol consumption >50 g/day lasting for at least one year. Exclusion criteria: (1) age <18 years old; (2) patients diagnosed with pregnancy, malignant tumor and/or infection before admission; (3) hospital stay <24 hours. Samples (blood, urine, sputum, drainage fluid, etc.) were collected for the first microbial culture when the doctor considered the occurrence of infection according to symptoms and laboratory results of the patient. If there were changes in the disease course during the treatment, such as the aggravation of infection indicators and symptoms, the second culture specimen was collected at an appropriate time. The time the first positive specimen collected was observation originating point. Different types of drug-resistant bacteria in the same infected person were included in the study. When the same drug-resistant bacteria were detected in different tissues of the same patient, only the first sample submitted for examination was analyzed. The blood routine, liver and kidney function, procalcitonin and other test results synchronized with positive culture specimens were collected and analyzed. The follow-up period was 90 days or when death event occurred during hospitalization.
Clinical Data Collection
The clinical characteristics included gender, age, etiology, comorbidities, type of acute pancreatitis (recurrent acute pancreatitis (RAP), and SAP), infection site, mechanical ventilation, ICU admission, septic shock, mortality, and complications, etc. Hemoglobin, platelet count, serum creatinine, albumin, total bilirubin, and procalcitonin levels within 24 hours after the first positive culture specimen were collected. Imputation would be applied when missing data was less than 20%. Categorical variables were imputed via mode and continuous variables were imputed through K- Nearest Neighbor (KNN) algorithm.9 Clinical outcomes were divided into the mortality and the survival according to death events during hospitalization.
Definition
Identification of resistant organisms was performed using the VITEK-2 system (Biomerieux, Marcy L’etoile, France). Drug susceptibility and minimal inhibitory concentration (MIC) were determined by Kerby-Bauer disk diffusion and AGAR dilution methods, respectively. CRKP was defined as insensitive to meropenem or imipenem. The MIC was ≥2 mg/L.5 Intermediate susceptibility was classified as resistant. Infection was diagnosed based on clinical presentation and positive culture outcomes according to the criteria of the Centers for Disease Control.10 The date of the first positive sample collection was considered the start date of infection. Septic shock was defined as persistent hypotension despite adequate volume resuscitation; vasoconstrictor drugs were required to maintain the mean arterial pressure (MAP) ≥65mmHg; and a serum lactate level >2 mmol/L. The common surgical methods included percutaneous catheter drainage (PCD), minimal access retroperitoneal pancreatic necrosectomy (MARPN), and open pancreatic necrosectomy (OPN). The commonly used invasive procedures included abdominal puncture, thoracic puncture, fiberoptic bronchoscopy, deep venous catheterization (peripherally inserted central catheters (PICCs) and central venous catheters (CVCs)), tracheal intubation, and urinary catheter. Mortality was defined as death from infection within 90 days.
Construction and Validation of an Overall Survival Prediction Model
First, independent risk factors associated with death were identified by Cox univariate and multivariate analyses and included as clinical variables. The 90-day OS was used as the clinical outcome endpoint. Then, the nomogram model was constructed by using R software 3.3.0. The consistency index (C-index) was used to compare the predicted results of the nomogram with the actual observed data, and the calibration map was used to visualize the prediction model to evaluate the sensitivity and specificity of the prediction model.
Statistical Analysis
Continuous variables were presented as median and interquartile range (IQR), and comparisons between groups were performed using the Mann Whitney U-test. Categorical variables were expressed as absolute values and percentages, and the Chi-square test or Fischer exact test was used for comparison between groups. Logistic regression and Cox regression analyses were used to assess the relationship between variables and CRKP acquisition and mortality, respectively. The nomogram prediction model was built by RMS software package written in R language. The receiver operating characteristic (ROC) curve was drawn, and the area under the curve (AUC) was calculated to evaluate the prediction accuracy of the model. Kaplan–Meier analysis and Log rank test were used to compare the survival of patients with and without risk factors. P < 0.05 was considered statistically significant. IBM SPSS24.0 software was used for statistical analysis.
Results
A total of 126 AP patients developed KP infection during the 10 years, including 98 males (77.8%) and 28 females (22.2%). The average age was 47 years old, and the mortality rate was 34.9% (44/126). There were 66 cases of hyperlipidemia, 51 cases of cholelithiasis, 7 cases of alcohol, and 2 cases of other types. The most common infection sites were pancreas and peri-pancreas (54.8%), followed by lung (20.6%) and blood stream (18.3%). There were 21 patients (16.7%) with RAP and 100 patients (79.4%) with SAP. Seventy-three patients (57.9%) had multiple site infections. Thirty-four patients (27%) had fungal infection. Sixty-four patients (50.8%) had GPB infection. Eighty-eight patients had CRKP infection, and 23% patients had septic shock. Among the 126 patients, 38.1% required mechanical ventilation for respiratory failure due to infection, and the median length of ICU stay was 8 days. The demographic and clinical data of the enrolled patients are detailed in Table 1.
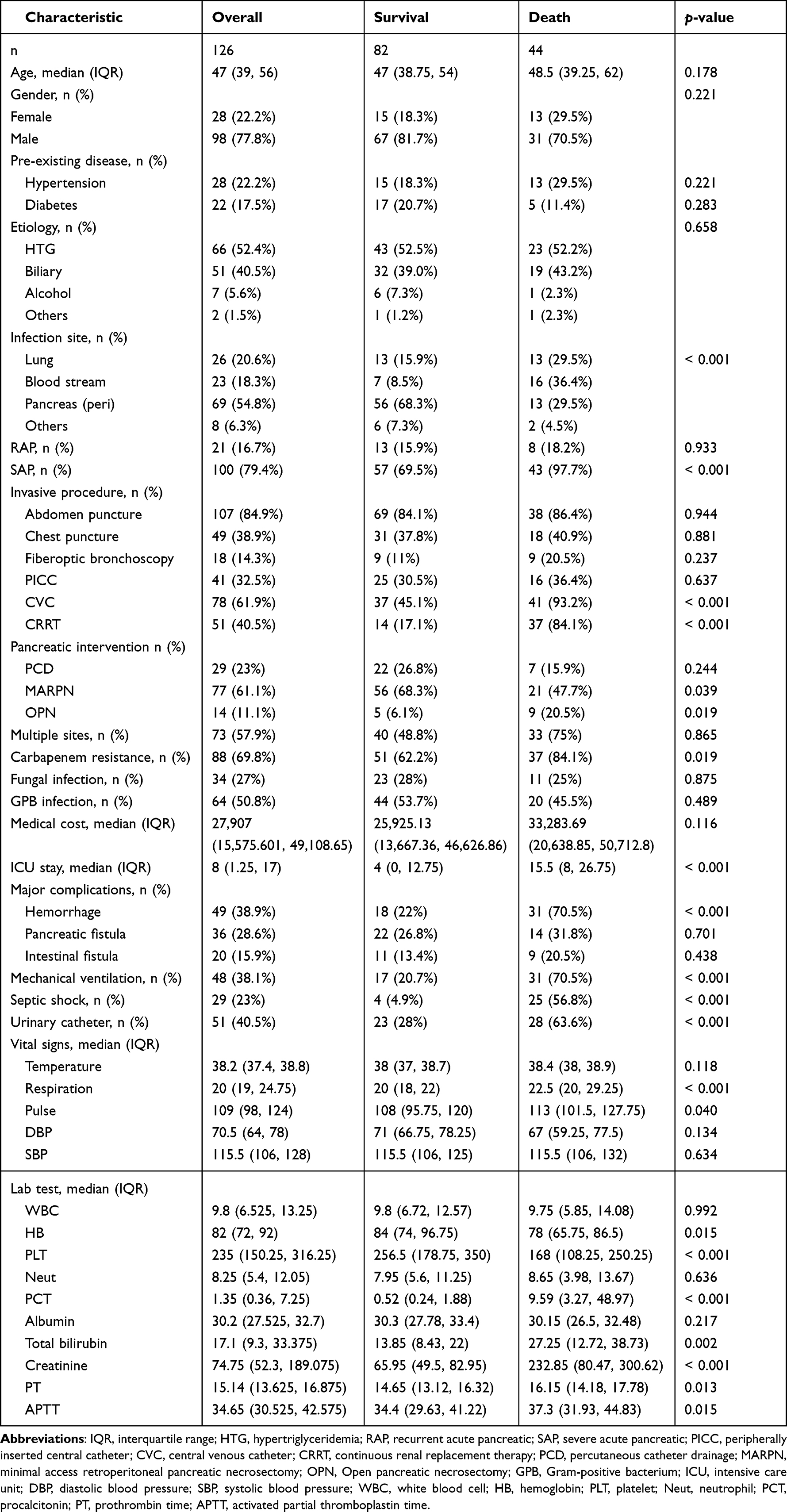 |
Table 1 Comparison of Baseline Characteristics Between Patients in Survival and Death Group |
Drug resistance rates of Klebsiella pneumoniae isolated from different sites to 16 antibiotics commonly used in clinical practice are shown in Table 2. CRKP was only sensitive to sulfamethoxazole-trimethoprim (SMZ-TMP) and tigecycline (TGC) (resistance rates were 36.6% and 17.1%, respectively) (Table 3). As Figure 1A indicates, the Sankey diagram, a specific type of flow chart in which the width of the extended branches corresponds to the size of the data flow, showed the trajectory tracking between carbapenem resistance, site of infection, and multiple drug resistance (MDR).
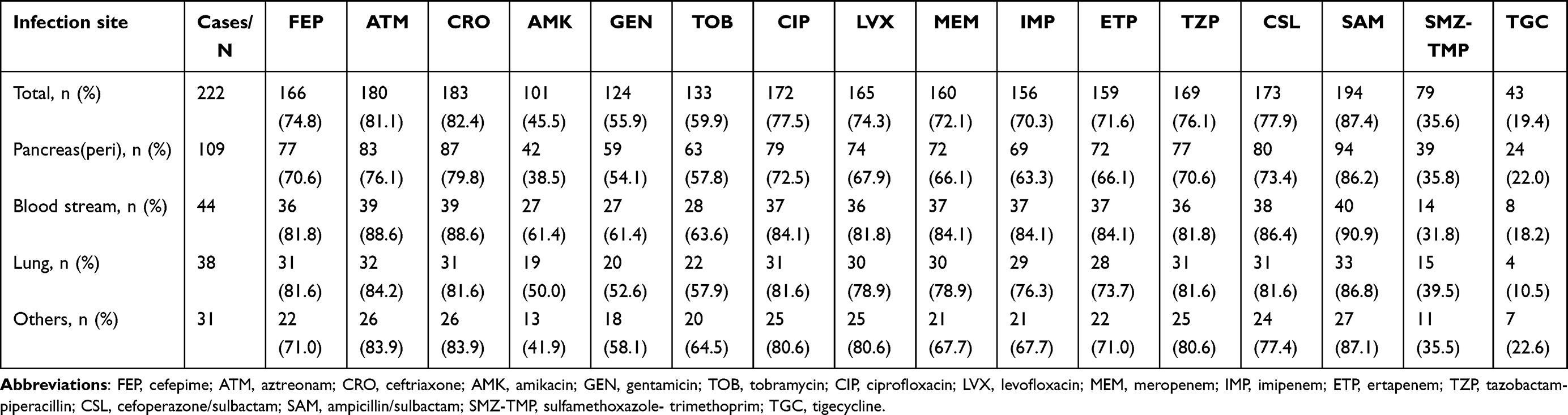 |
Table 2 Drug Resistance Rates of Klebsiella Pneumoniae Isolated from Different Sites to 16 Antibiotics Commonly Used in Clinical Practice |
 |
Table 3 Drug Resistance Rates of Carbapenem-Resistant Klebsiella Pneumoniae Isolated from Different Sites to 16 Antibiotics Commonly Used in Clinical Practice |
 |
Figure 1 (A) The trajectory tracking between carbapenem resistance, site of infection, and multiple drug resistance (MDR). |
Logistic univariate analysis showed that the factors related to CRKP acquisition included male (P = 0.037), ICU admission (P = 0.001), PICC/CVC implantation (P = 0.001), and urinary catheter implantation (P = 0.036). Logistic multivariate analysis showed that male (OR = 1.655, 95% CI 0.642–4.265, P = 0.017) and PICC/CVC implantation (OR = 3.157, 95% CI 1.223–8.147, P = 0.021) were independent risk factors for CRKP infection (Table 4).
 |
Table 4 Univariate and Multivariate Analysis of Risk Factors Associated with Carbapenem Resistance of Klebsiella Pneumoniae Infection in AP Patients |
Cox univariate analysis showed that carbapenem resistance (P = 0.013), infection site (P = 0.013), SAP (P = 0.009), hemorrhage (P = 0), mechanical ventilation (P < 0.001), septic shock (P < 0.001), multiple site infection (P = 0.01), age >60 years (P = 0.034), and platelet (PLT) count <100×109/L (P = 0.006), procalcitonin (PCT) >5 ng/mL (P < 0.001), creatinine >177 μmol/L (P < 0.001), ICU time ≥3 weeks (P = 0.015) were statistically different between the death group and the survival group. In Cox multivariate analysis, carbapenem resistance (HR = 2.556, 95% CI 1.011–6.462, P = 0.047), hemorrhage (HR = 2.392, 95% CI 1.104–5.182, P = 0.027), septic shock (HR = 3.022, 95% CI 1.312–6.959, P = 0.009), age >60 years (HR = 2.977, 95% CI 1.303–6.799, P = 0.01), creatinine >177μmol/L (HR = 2.815, 95% CI 1.075–7.369, P = 0.035) were the five independent risk factors associated with mortality (Table 5).
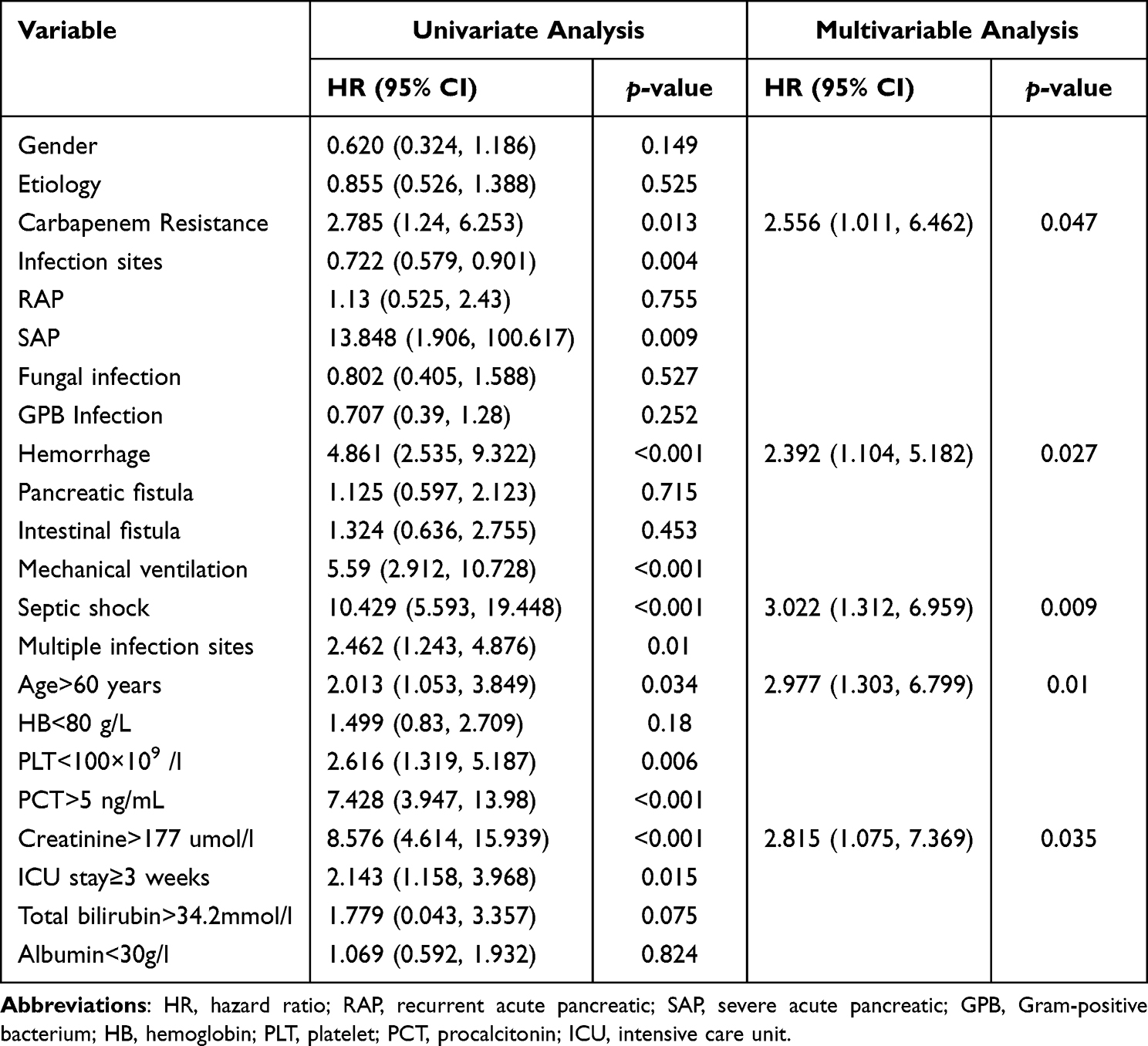 |
Table 5 Univariate Analysis and Multivariate Analysis of the Mortality Risk Factors Among the AP Patients with Klebsiella Pneumoniae Infection |
Kaplan–Meier curves for each independent risk factor are shown in Figure 2. Carbapenem resistance (18.4%vs 42% P = 0.009), hemorrhage (16.9%vs 63.3% P < 0.001), septic shock (19.6%vs 86.2% P < 0.001), age >60 years (30.7%vs 52%) P = 0.03) and Creatinine > 177 (19.1%vs 73%, P < 0.001) were significantly lower.
 |
Figure 2 Survival comparison of patients with independent risk factors (Kaplan–Meier curve). (A) Carbapenem resistance vs non-Carbapenem resistance (P = 0.009); (B)Hemorrhage vs non-Hemorrhage (P < 0.001); (C) Septic shock vs non-Septic shock (P < 0.001); (D) Age > 60 years vs ≤ 60 years (P = 0.03). (E) Creatinine >177μmol/L vs ≤177μmol/L (P < 0.001). |
To predict the 90-day survival rate of SAP patients infected with Klebsiella pneumoniae, a nomogram was established using the above independent factors (Figure 3A) with a C-index of 0.866. The nomogram proportionated regression coefficients in a multivariate logistic regression analysis to a scale of 0 to 100 points. The points among the variables were summed up respectively to gain a total point, which was transferred as predictive probabilities accordingly. Meanwhile, the calibration plot also confirmed a good consistency between the predicted value of the nomograph and the actual OS of SAP patients with KP (Figure 3B and C).
 |
Figure 3 (A) Nomogram for predicting the mortality risk in patients with AP and KP infection. (B) ROC curve for the predictive model; (C) Validity of the predictive performance of the nomogram in estimating the probabilities of 90 days survival. |
Discussion
Klebsiella pneumoniae is one of the most common pathogens causing nosocomial infection, which poses a great threat to human health, especially for patients in bad immune condition.11 After acquiring a plasmid containing the carbapenemase gene, it becomes CRKP, a super-bacterium that causes incurable or difficult-to treat infections. The incidence of CRKP has increased significantly worldwide in recent decades, making it an urgent threat to public health system.12 Due to the overuse of anti-inflammatory drugs and antibiotics in the early stage, AP patients have become a high-risk group of CRKP infection, which is associated with poor prognosis. We conducted the retrospective cohort study, with the longest time span, to describe the characteristics, risk factors, antibiotic susceptibility, and clinical outcomes of KP infection in patients with AP in China.
In this study, hyperlipidemia was the most common cause in AP patients with KP infection, which was similar to a previous study reporting it as the main etiology in AP patients infected with Carbapenem-Resistant Enterobacteriaceae.13 The lung was the second most common site of infection. Unlike previous studies in which blood flow was the most common extra-pancreatic site, this may be due to widespread empirical anti-infection therapy, which reduced the sensitivity of blood cultures.14 Besides, some patients refused repeated blood culture due to personal factors, facilitating the low positive rate of blood culture. By contrast, sputum culture samples were relatively easy to obtain. The calculated mortality of 34.9% in our cohort is similar to the 34.5% reported for SAP and secondary infections in previous studies.15 It was also noted that more than half of the patients in this cohort had multiple site infections and most had invasive procedures. The median hospitalization cost was US $27,907, which reflects the complexity and severity of the patient’s condition and presumably contributes to the poor efficacy and high mortality.6
As the data suggested, KP was sensitive to gentamicin, amikacin, and TGC, and the resistance rates to aminoglycosides, quinolones, and amidase inhibitors commonly used in clinical practice were more than 60%. And it got worse in CRKP, which owned high resistance, even more than 90%, to most antibiotics. It seemed to be merely sensitive to SMZ-TMP and TGC. This result is similar to a previous study in which TGC and SMZ-TMP were recommended for carbapenem-resistant organism (CRO) infection treatment in critical acute pancreatitis patients.16 It has been suggested that standard or high-dose TGC alone has good sensitivity to CRKP strains, but the emergence of hypervirulent CRKP, however, limits its effect.17 In addition, meta-analysis study has shown that long-term high-dose TGC use can lead to abnormal coagulation function and even the risk of bleeding, and thus increase the mortality rate of patients.18 SMZ-TMP, as an old drug, is widely used to treat infections caused by a variety of pathogens. Retrospective studies have shown that SMZ-TMP has good antibacterial activity in treating CRKP infection at a relatively low resistance rate, in both combination therapy and even as a single agent.19 For the evaluation of the efficacy of some “classical” antibiotics, a systematic review showed that the resistance rate of CRKP to colistin, polymyxin B, and fosfomycin was relatively low.20 However, we did not compare susceptibility to such antibiotics because the associated susceptibility results were not comprehensive. In recent years, the launch of new antibiotics has improved the efficacy of CRKP infection to a certain extent. Ceftazidime-avibactam, a recently approved mixture agent type, consisting of a well-known anti-Pseudomonas third-generation cephalosporin combined with a new β-lactamase inhibitor, has been reported from real-world studies to be effective in both combination and monotherapy, including in difficult-to-treat infections and critically ill patients.21,22 Plazomicin is a new generation semisynthetic aminoglycoside with dose-dependent bactericidal activity and synergistic effects with meropenem, colistin and fosfomycin. An in vitro study confirmed that plazomicin has good activity compared with other antibiotics. Only one ndm-1 producing Klebsiella pneumoniae was resistant to plazomicin.23,24 It should be emphasized that due to the actual medical conditions in different regions, including the time of drug launch, medical insurance policy, price and other factors, it is currently unable to make a detailed comparison with the efficacy of some new antibiotics. Overall, the results suggest that CRKP infections, especially those caused by resistant strains, remain challenging to treat clinically and thus, there is a great need for the development of effective drugs with safe therapeutic window.
Carbapenem resistance, hemorrhage, septic shock, age > 60 years, creatinine > 177μmol/L are independent risk factors for the death of KP infection. Carbapenems are considered the most effective drugs against MDR Gram-negative pathogens, for the relative resistance to hydrolysis of most β-lactamases.25 However, inappropriate use of antimicrobial agents has led to an increase in drug-resistant pathogens. As the overuse rate of antibiotics in China ranks first in the world, Chinese AP patients are more susceptible to infection with drug-resistant pathogens.6 In a previous study, the adverse effects of carbapenem resistance was described.26 A systematic review analysis showed that the overall gross mortality rate of CRKP patients was 42.14%, significantly higher than that of carbapenem-sensitive Klebsiella pneumoniae (CSKP) infection patients, especially for the critically ill group.27 Therefore, CRKP infection should be taken with caution. Rational and strict infection control measures and new antibiotics selection should be adopted as well as more targeted treatment. Hemorrhage is a serious complication of AP, although gastrointestinal bleeding is not considered organ failure in the revised Atlanta classification.28 The consequences associated with it are sometimes fatal.29,30 Hemorrhage can arise secondary to erosion of the vascular wall, formation of pseudoaneurysms or microvascular ischaemic complications, oesophagogastric varices caused by spleno-porto-mesenteric venous thrombosis,29,31 and surgical debridement.29,32–34 Severe inflammation and activated enzymes which leak into the retroperitoneum in SAP can digest the viscus and vascular structure, thus lead to acute erosion, disruption, wall weakening, pseudoaneurysm formation, and eventually rupture and bleed.29,31,32,34,35 Pancreatic necrosis, abscess and pseudocysts may produce similar damage to the vasculature. In addition to pancreatic debridement, timing of surgery and surgical technique have also been identified as risk factors for the occurrence of hemorrhage.29,32,34 One study found that the incidence of hemorrhage in the presence of infected necrosis was 29.5%, and infected necrosis and sepsis may be risk factors for hemorrhage.36 In this study, bleeding was observed in 38.9% of the cases, which was higher than that in previous studies. The higher incidence of severe type of infection might explain the higher hemorrhage rate. Mortality from bleeding directly related to the pancreas was as high as 50%.32 Hemorrhage can cause death in a short period, though it is rare in clinical practice. Given the high risk, early intervention in patients with bleeding is warranted. Immunosuppression in the early stage of AP can lead to systemic hyperinflammatory response syndrome and induce intestinal barrier dysfunction, thereby increasing intestinal mucosal permeability. Intestinal bacterial translocation can cause extra-intestinal organ damage, leading to secondary multiple organ failure and eventually sepsis.37 Septic shock is defined as a subset of sepsis in which circulatory, cellular or metabolic abnormalities occur and increase risk of mortality.38 In this study, septic shock was found to be an independent predictive risk factor for death in patients with KP infection. Indeed, previous reports of septic shock have been reported to be associated with higher mortality in patients with AP and MDR KP infection and CRO infection.8,39 This is consistent with our results. Taken together with previous studies and our findings, samples for microbial culture should be collected before antibiotic administration in patients with suspected sepsis or septic shock, as antimicrobial therapy can alter culture results.38 Patients presenting with septic shock should be treated and resuscitated early, especially with anti-infection therapy, since clear guidelines for early initiation of antimicrobial therapy in septic shock are available.40 Creatinine is a key indicator of renal function, and renal failure has been one of the main driving factors of multiple organ failure in SAP.41 The increase in creatinine level of SAP patients may be attributed to body tissues damaging by releasing pancreatic, activation of a large number of inflammatory cytokines, and insufficient renal perfusion or prerenal dysfunction.42 Previous studies have reported that impaired leukocyte chemotaxis, lymphopenia and dysfunction further lead to impaired immune function, which may be the mechanism of increasing the degree of infection when renal insufficiency occurs.43 In addition, some studies have reported that serum creatinine level is related to the severity of AP disease.44 Although our observation is preliminary, the current study suggests the significance of monitoring renal function.
Carbapenem resistance, hemorrhage, septic shock, old age, and high creatinine level were risk factors of death, while in order to quantify the role of these five risk factors in the pathology development of the disease, to translate them into clinical practice, and to provide the clinical doctor with more accurate and scientific guidance in diagnosis and treatment decision-making, a prediction model was established accordingly. The calibration curve shows that the model has good predictive performance. The model will be validated and upgraded in larger clinical cohorts.
Our study has a number of limitations that must be acknowledged. This is a single-center retrospective cohort study, so the results may be different from those in other regions due to sample size, accuracy of medical records, data completeness, selection bias, etc. Multi-center data or prospective studies are needed to make up for the above shortcomings. Second, as mentioned above, clinical data and efficacy assessments for some of the new antibiotics are not available at this time. Third, this study did not involve CRKP colonization, antibiotic combination, surgical treatment and other factors, which may be the risk factors for the occurrence or mortality of KP in AP patients.
Conclusions
Klebsiella pneumoniae is one of the most common pathogens causing nosocomial infection, with increasing rates of drug resistance and mortality. CRKP was sensitive to SMZ-TMP and TGC to some extent. Carbapenem resistance, hemorrhage, septic shock, age >60 years, creatinine >177μmol/L are independent risk factors for the death of KP infection. It is necessary to make a comprehensive judgment based on local epidemiology and actual medical condition in different regions.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
This was a retrospective cohort analysis and all data were obtained anonymously through an electronic medical record information system. The institutional review board of Xiangya Hospital endorsed this project and approved the waiver of informed consent from patients (no. 202105092). This study was in compliance with the Declaration of Helsinki.
Funding
This work was supported by grants from the Scientific research project of Hunan Provincial Health Commission (B2019198), and National Natural Science Foundation of China (Grant No. 82170661).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Xiao AY, Tan ML, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi:10.1016/S2468-1253(16)30004-8
2. van Santvoort HC, Bakker OJ, Bollen TL, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology. 2011;141(4):1254–1263. doi:10.1053/j.gastro.2011.06.073
3. Brown LA, Hore TA, Phillips AR, Windsor JA, Petrov MS. A systematic review of the extra-pancreatic infectious complications in acute pancreatitis. Pancreatology. 2014;14(6):436–443. doi:10.1016/j.pan.2014.09.010
4. van Brunschot S, Bakker OJ, Besselink MG, et al. Treatment of necrotizing pancreatitis. Clin Gastroenterol Hepatol. 2012;10(11):1190–1201. doi:10.1016/j.cgh.2012.05.005
5. Schmidt PN, Roug S, Hansen EF, Knudsen JD, Novovic S. Spectrum of microorganisms in infected walled-off pancreatic necrosis - impact on organ failure and mortality. Pancreatology. 2014;14(6):444–449. doi:10.1016/j.pan.2014.09.001
6. Ning C, Huang G, Shen D, et al. Adverse clinical outcomes associated with multidrug-resistant organisms in patients with infected pancreatic necrosis. Pancreatology. 2019;19(7):935–940. doi:10.1016/j.pan.2019.09.008
7. Effah CY, Sun T, Liu S, Wu Y. Klebsiella pneumoniae: an increasing threat to public health. Ann Clin Microbiol Antimicrob. 2020;19(1):1. doi:10.1186/s12941-019-0343-8
8. Wu D, Ding J, Jia Y, Liu H, Xiao J, Peng J. Predictors of mortality in acute pancreatitis complicated with multidrug-resistant Klebsiella pneumoniae infection. BMC Infect Dis. 2021;21(1):977. doi:10.1186/s12879-021-06709-0
9. Meinel T, Lerch C, Fischer U, et al. Multivariable prediction model for futile recanalization therapies in patients with acute ischemic stroke. Neurology. 2022;99(10):e1009–1018. doi:10.1212/WNL.0000000000200815
10. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
11. Qin X, Wu S, Hao M, et al. The colonization of carbapenem-resistant Klebsiella pneumoniae: epidemiology, resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. 2020;221(Suppl 2):S206–s214. doi:10.1093/infdis/jiz622
12. Yang X, Sun Q, Li J, et al. Molecular epidemiology of carbapenem-resistant hypervirulent Klebsiella pneumoniae in China. Emerg Microbes Infect. 2022;11(1):841–849. doi:10.1080/22221751.2022.2049458
13. Wu D, Xiao J, Ding J, et al. Predictors of mortality and drug resistance among carbapenem-resistant enterobacteriaceae-infected pancreatic necrosis patients. Infect Dis Ther. 2021;10(3):1665–1676. doi:10.1007/s40121-021-00489-5
14. Cheng MP, Stenstrom R, Paquette K, et al. Blood culture results before and after antimicrobial administration in patients with severe manifestations of sepsis: a diagnostic study. Ann Intern Med. 2019;171(8):547–554. doi:10.7326/M19-1696
15. Tian H, Chen L, Wu X, et al. Infectious complications in severe acute pancreatitis: pathogens, drug resistance, and status of nosocomial infection in a university-affiliated teaching hospital. Dig Dis Sci. 2020;65(7):2079–2088. doi:10.1007/s10620-019-05924-9
16. Wu D, Huang Y, Xiao J, Qin G, Liu H, Peng J. Risk factors for mortality among critical acute pancreatitis patients with carbapenem-resistant organism infections and drug resistance of causative pathogens. Infect Dis Ther. 2022;11(3):1089–1101. doi:10.1007/s40121-022-00624-w
17. Jin X, Chen Q, Shen F, et al. Resistance evolution of hypervirulent carbapenem-resistant Klebsiella pneumoniae ST11 during treatment with tigecycline and polymyxin. Emerg Microbes Infect. 2021;10(1):1129–1136. doi:10.1080/22221751.2021.1937327
18. Cui N, Cai H, Li Z, Lu Y, Wang G, Lu A. Tigecycline-induced coagulopathy: a literature review. Int J Clin Pharm. 2019;41(6):1408–1413. doi:10.1007/s11096-019-00912-5
19. Murri R, Fiori B, Spanu T, et al. Trimethoprim-sulfamethoxazole therapy for patients with carbapenemase-producing Klebsiella pneumoniae infections: retrospective single-center case series. Infection. 2017;45(2):209–213. doi:10.1007/s15010-016-0968-x
20. Bassetti M, Righi E, Carnelutti A, Graziano E, Russo A. Multidrug-resistant Klebsiella pneumoniae: challenges for treatment, prevention and infection control. Expert Rev Anti Infect Ther. 2018;16(10):749–761. doi:10.1080/14787210.2018.1522249
21. Jayol A, Nordmann P, Poirel L, Dubois V. Ceftazidime/avibactam alone or in combination with aztreonam against colistin-resistant and carbapenemase-producing Klebsiella pneumoniae. J Antimicrob Chemother. 2018;73(2):542–544. doi:10.1093/jac/dkx393
22. García-Castillo M, García-Fernández S, Gómez-Gil R, et al. Activity of ceftazidime-avibactam against carbapenemase-producing Enterobacteriaceae from urine specimens obtained during the infection-carbapenem resistance evaluation surveillance trial (iCREST) in Spain. Int J Antimicrob Agents. 2018;51(3):511–515. doi:10.1016/j.ijantimicag.2018.01.011
23. Rodríguez-Avial I, Pena I, Picazo JJ, Rodríguez-Avial C, Culebras E. In vitro activity of the next-generation aminoglycoside plazomicin alone and in combination with colistin, meropenem, fosfomycin or tigecycline against carbapenemase-producing Enterobacteriaceae strains. Int J Antimicrob Agents. 2015;46(6):616–621. doi:10.1016/j.ijantimicag.2015.07.021
24. Denervaud-Tendon V, Poirel L, Connolly LE, Krause KM, Nordmann P. Plazomicin activity against polymyxin-resistant Enterobacteriaceae, including MCR-1-producing isolates. J Antimicrob Chemother. 2017;72(10):2787–2791. doi:10.1093/jac/dkx239
25. Guo D, Dai W, Shen J, et al. Assessment of prophylactic carbapenem antibiotics administration for severe acute pancreatitis: an updated systematic review and meta-analysis. Digestion. 2022;103(3):183–191. doi:10.1159/000520892
26. Yan J, Yilin H, Di W, et al. A nomogram for predicting the risk of mortality in patients with acute pancreatitis and Gram-negative bacilli infection. Front Cell Infect Microbiol. 2022;12:1032375. doi:10.3389/fcimb.2022.1032375
27. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16(1):18. doi:10.1186/s12941-017-0191-3
28. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013;62(1):102–111. doi:10.1136/gutjnl-2012-302779
29. Evans RP, Mourad MM, Pall G, Fisher SG, Bramhall SR. Pancreatitis: preventing catastrophic haemorrhage. World J Gastroenterol. 2017;23(30):5460–5468. doi:10.3748/wjg.v23.i30.5460
30. Wei AL, Guo Q, Wang MJ, Hu WM, Zhang ZD. Early complications after interventions in patients with acute pancreatitis. World J Gastroenterol. 2016;22(9):2828–2836. doi:10.3748/wjg.v22.i9.2828
31. Andersson E, Ansari D, Andersson R. Major haemorrhagic complications of acute pancreatitis. Br J Surg. 2010;97(9):1379–1384. doi:10.1002/bjs.7113
32. Ammori BJ, Madan M, Alexander DJ. Haemorrhagic complications of pancreatitis: presentation, diagnosis and management. Ann R Coll Surg Engl. 1998;80(5):316–325.
33. Balthazar EJ, Fisher LA. Hemorrhagic complications of pancreatitis: radiologic evaluation with emphasis on CT imaging. Pancreatology. 2001;1(4):306–313. doi:10.1159/000055829
34. Labarca E, Zubia F, Maraví-Poma E, Martinez F. Early predictors of abdominal hemorrhage among critically Ill patients with pancreatitis: a prospective cohort study. Pancreas. 2018;47(8):1027–1032. doi:10.1097/MPA.0000000000001135
35. Flati G, Andrén-Sandberg A, La Pinta M, Porowska B, Carboni M. Potentially fatal bleeding in acute pancreatitis: pathophysiology, prevention, and treatment. Pancreas. 2003;26(1):8–14. doi:10.1097/00006676-200301000-00002
36. Gupta V, Krishna P, Kochhar R, et al. Hemorrhage complicating the course of severe acute pancreatitis. Ann Hepatobiliary Pancreat Surg. 2020;24(3):292–300. doi:10.14701/ahbps.2020.24.3.292
37. Li X, Li L, Liu L, et al. Risk factors of multidrug resistant pathogens induced infection in severe acute pancreatitis. Shock. 2020;53(3):293–298. doi:10.1097/SHK.0000000000001371
38. Esposito S, De Simone G, Boccia G, De Caro F, Pagliano P. Sepsis and septic shock: new definitions, new diagnostic and therapeutic approaches. J Glob Antimicrob Resist. 2017;10:204–212. doi:10.1016/j.jgar.2017.06.013
39. Jia Y, Li Y, Liu Y, Yang Z, Chen X, Liu Y. Epidemiology, antimicrobial resistance, and mortality risk factors of carbapenem resistant gram-negative bacteria in hematopoietic stem cell transplantation recipients. Front Cell Infect Microbiol. 2022;12:1098856. doi:10.3389/fcimb.2022.1098856
40. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/S1473-3099(17)30753-3
41. Pupelis G. Renal failure in acute pancreatitis. Timing of dialysis and surgery. Przegl Lek. 2000;57 Suppl 5:29–31.
42. Cao X, Wang HM, Lu R, et al. Establishment and verification of a nomogram for predicting severe acute pancreatitis. Eur Rev Med Pharmacol Sci. 2021;25(3):1455–1461. doi:10.26355/eurrev_202102_24853
43. Zou C, Lu Z, Zhang Z, et al. Factors associated with pancreatic infection in patients with severe acute pancreatisis. Int J Clin Exp Med. 2015;8(8):14100–14104.
44. Engoren M, Maile MD, Heung M, et al. The association between urine output, creatinine elevation, and death. Ann Thorac Surg. 2017;103(4):1229–1237. doi:10.1016/j.athoracsur.2016.07.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.