")
Back to Journals » International Journal of General Medicine » Volume 16
Clinical Characteristics and Risk Factors of Neonatal Hypoxic-Ischaemic Encephalopathy and Its Associated Neurodevelopmental Outcomes During the First Two Years of Life: A Retrospective Study in Saudi Arabia
Authors AlMuqbil M, Alanazi J, Alsaif N, Baarmah D , Altwaijri W, Alrumayyan A, Alrifai MT, Othman F, Al-shehri H , Alsaif S
Received 16 December 2022
Accepted for publication 1 February 2023
Published 11 February 2023 Volume 2023:16 Pages 525—536
DOI https://doi.org/10.2147/IJGM.S401803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammed AlMuqbil,1– 3 Jawaher Alanazi,2 Nada Alsaif,1 Duaa Baarmah,2 Waleed Altwaijri,1,2 Ahmad Alrumayyan,1,2 Muhammad Talal Alrifai,1,2 Fatmah Othman,3,4 Hassan Al-shehri,5 Saif Alsaif1,3
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Saudi Arabia; 2Division of Pediatric Neurology, King Abdullah Specialist Children’s Hospital (KASCH), National Guard Health Affairs (NGHA), Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center (KAIMRC), Ministry of National Guard, Riyadh, Saudi Arabia; 4Department of Epidemiology and Biostatistics, College of Public Health and Health Informatics, King Saud bin Abdulaziz University for Health-Science, Riyadh, Saudi Arabia; 5Department of Pediatrics, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia
Correspondence: Mohammed AlMuqbil, College of Medicine, King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, 11481, Saudi Arabia, Tel +966 50533 7752, Email [email protected]
Objective: This study aimed to determine the clinical characteristics and factors associated with neonatal hypoxic-ischaemic encephalopathy (HIE) and its neurodevelopmental outcomes.
Methods: We conducted retrospective case-control research to investigate the clinical and labour-related risk factors for HIE. In addition, a single-centre cohort study was conducted on infants with HIE to describe their neurodevelopment from birth to 24 months. For this investigation, cases with a diagnosis of HIE who were born at King Abdullah Children’s Specialist Hospital (KASCH), Riyadh, Saudi Arabia, between 2015 and 2019 were identified and matched with controls from the same facility (1:4). Each case’s clinical information was extracted using electronic medical records. In addition, 24-month follow-up HIE cases were included in a cohort study to describe their neurodevelopmental outcomes.
Results: The sample includes 60 infants diagnosed with HIE and 234 infants serving as controls, with a mean gestational age of 38.8 weeks (SD 1.6) and a predominance of males (56.4%). Around one-third of the HIE cases (36.6%) had moderate HIE (stage 2), whereas 35.1% of infants had severe HIE (stage 3), according to Sarnat staging. Compared to the control group, children with HIE were twice as likely to be born to mothers with maternal comorbidities and more likely to have prepartum and intrapartum complications. A 24-month follow-up of neurodevelopmental outcomes for HIE babies revealed that approximately 24% exhibited delays in gross motor skill development, 22% in fine motor skill development, 33% in language skill development, and 22% in social skill development.
Conclusion: In the HIE group, maternal comorbidities and prepartum or intrapartum complications were more common. The severity grade of HIE can be used to predict neurodevelopmental consequences. Enhancing patient care and rehabilitation requires a minimum of 24 months of neurodevelopmental follow-up.
Keywords: hypoxic-ischaemic encephalopathy, seizure, perinatal asphyxia
Introduction
Hypoxic-ischaemic encephalopathy (HIE) is a combination of clinical and biochemical signs of immediate or subacute brain injury in term or near-term newborns associated with asphyxia.1,2 HIE affects approximately one to eight per 1000 live newborns worldwide.3 It is regarded as one of the most prevalent causes of persistent injury to the central nervous system, leading to newborn mortality or neurodevelopmental impairment.4 Infants with moderate HIE have a 10% chance of death, while those who survive have a 30% chance of developing impairments.5 Infants with severe HIE have a 60% chance of death, and nearly all survivors suffer from epilepsy and neurodevelopmental damage, such as cerebral palsy and intellectual incapacity.6
The conventional treatment for newborns of ≥ 36 weeks’ gestational age (GA) with moderate to severe HIE is therapeutic hypothermia.7–10 The first injury generally creates reactive oxygen species, neurotransmitters, inflammatory mediators, and apoptosis.11 Hypothermia mitigates this toxicity. Erythropoietin has also been provided to newborns with prenatal HIE to minimise the risk of brain injury, cerebral palsy, and cognitive impairment; however, there is limited evidence to support its role as an adjuvant to hypothermia.1,12
Numerous studies have been undertaken to investigate the risk factors associated with HIE and its consequences.13–16 Although these studies have identified peripartum monitoring patterns and acute obstetric emergency events associated with neonatal HIE morbidity and mortality,13–15 they have not identified risk factors for HIE in the absence of a sentinel event, other than nulliparity and infection (not identified before delivery), with comparable morbidity and mortality between cases of unexplained HIE and those with a sentinel event. Most commonly reported risk factors for HIE included meconium-stained amniotic fluid, a prolonged second stage of labour, the occurrence of a sentinel or acute event, signs indicated by electronic fetal monitoring such as an indeterminate baseline heart rate, bradycardia, low variability, rupture of a previous uterine caesarean scar and placental abruption, nulliparity, infection, clinical chorioamnionitis, a maternal age of ≥35 years, and a urinary tract infection during pregnancy.13–16
Given the significance of sentinel events, research continues to emphasise the significance of developing improved mechanisms for prediction and prevention, with a focus on reducing other complications, such as clinical chorioamnionitis and/or maternal pyrexia, to improve the ability to prevent HIE.15
Few local studies have sought to investigate the characteristics of HIE in Saudi Arabia. Al-Shehri et al described the risk factors for the development of HIE in 57 cases and a comparable number of controls.17 Identified HIE risk variables included a non-cephalic presentation, antepartum haemorrhage, instrumental delivery, and a prolonged second stage of labour.17
Although previous research has examined the epidemiological characteristics of newborns with HIE, there is limited evidence regarding the neurodevelopmental outcomes of these children. Using clinical and imaging biomarkers, this research aimed to identify predictors of HIE and neurodevelopmental outcomes in newborns. This research may facilitate the identification of novel risk factors for HIE among newborns in Saudi Arabia, as well as the identification of important elements to predict potential severe neurodevelopmental consequences, hence facilitating the use of HIE severity as a predictive tool.
Methods
Study Type and Population
We conducted a retrospective case-control study to identify clinical and labour-related HIE risk factors. In addition, a retrospective cohort study was undertaken on infants with HIE to describe their neurodevelopmental outcomes over their first two years. Initially, the study group comprised all live-born newborns at KACSH, Riyadh, Saudi Arabia, between 2015 and 2019. Then, for the case-control study, the study case group comprised newborns who had been admitted to the neonatal intensive care unit (NICU – Level IV) with a final diagnosis of HIE, either as a primary diagnosis or a secondary diagnosis attributed to other causes of encephalopathy, such as major congenital anomalies or metabolic disorders. The diagnosis of HIE was confirmed based on the operational definition outlined in the hospital’s developmental policies and procedures (DPP 7610–2009) as a clinical syndrome characterised by abnormal consciousness, tone, reflexes, feeding, and respiration (and occasionally seizures) in full-term or near-term newborns. This syndrome is a subtype of neonatal encephalopathy, which can occur for a variety of reasons, including HIE,18 and is characterised by significant oxygen and blood flow restriction near the time of delivery. As it was difficult to follow their neurodevelopmental-outcome data, we excluded neonates who were born in other facilities or who had been moved to another hospital after birth. For each case of HIE, up to four controls were selected at random from all hospital deliveries during the same calendar year and matched to the HIE cases in terms of gestational age (±2 weeks) and maternal age (±5 years).
Study Variables for HIE Cases and Control
Clinical data for each HIE case and control were extracted from the hospital’s electronic medical record (ie, maternal obstetric history and delivery details). The following data were extracted: antepartum-associated risk factors, intrapartum-associated risk factors, and infant characteristics. The antepartum-associated risk factors included maternal age at delivery, maternal comorbidities (eg, gestational diabetes, hypertension, thyroid disease), and maternal mortality during the delivery. For the intrapartum-associated risk factors, we collected data on the gestational age, mode of delivery (vaginal or C-section), and intrapartum complications and events, including malpresentation, abnormal cardiotocographic findings, the presence of peripartum decelerations, positive screening for a group B streptococcus test (GBS), meconium-stained amniotic fluid, abruption placentae, uterine rupture, and abnormality of amniotic fluid. For the neonatal data, the following variables were collected: sex, birth weight, Apgar score (at 1, 5, and 10 minutes), the need for and method of resuscitation (including the use of non-invasive or invasive ventilation), the presence of congenital anomalies, and the length of stay in NICU for those admitted to NICU.
Classification of HIE Cases and Description of Their Clinical Variables
Clinical and radiological investigation information was extracted from the HIE patients’ medical records. This was performed exclusively for HIE cases to offer a descriptive analysis of this group of patients. Thus, information regarding the severity of HIE, mortality, abnormalities in imaging modalities, documentation of neonatal seizures, cerebral palsy, and intellectual and learning deficits were retrieved. A trained neonatology expert evaluated the severity of HIE as normal, mild (stage 1), moderate (stage 2), and severe (stage 3) based on the modified Sarnat Staging System.19 In addition, information was collected on the treatment and utilisation of therapeutic hypothermia for mild and severe HIE. Data on various clinical investigations conducted on HIE cases, such as audiology tests, autism spectrum disorder, attention deficit hyperactivity, diagnosis of epilepsy, and EEG information, were obtained. The hospital followed a set of diagnostic criteria and a precise definition for diagnosing these conditions.
Neurodevelopmental Outcomes of the HIE Cases
Only the HIE cases were monitored retrospectively for 24 months using medical records to describe the neurodevelopmental outcomes of this cohort concerning gross motor, fine motor, language, and social skills development. Thus, the HIE case’s medical records were reviewed up to 24 months following delivery. Those who were lost to follow-up within this time frame were excluded. The neurodevelopmental assessment was standardised using the third edition of the Baily Scales of Infant and Toddler Development.20 For infants and toddlers younger than five years of age, the Baily scales were used, whereas neuropsychology was utilised for older children. The neurodevelopment testing was standardised following the hospital policy that governs healthcare delivery and service management in terms of clinical visits, referrals, follow-up tests, and evaluation procedures.
Statistical Analysis
In the case-control study, the baseline characteristics of HIE cases and controls were reported as numbers and percentages for categorical variables and as mean and standard deviation (SD) for normally distributed continuous variables. Histogram and the Shapiro–Wilk test were employed to determine the data’s normality. Using a Chi-square or Fisher’s exact test for categorical variables and two-sample t-tests for continuous variables, we compared the maternal intrapartum factors and the neonatal features of the HIE patients (case group) with the control group. The risk factors of interest were estimated using conditional logistic regression models, the odds ratio (OR), a 95% confidence interval (CI), and p-values. We divided the characteristics that were substantially linked with HIE into three categories: maternal comorbidities, prepartum, and intrapartum. If p<0.05, the variable was maintained in the final multivariable model.
For the cohort study analysis of HIE patients, we described the clinical outcome 24 months after birth for those patients who survived and for those whose clinical follow-up data were available. This included intellectual and learning disabilities, cerebral palsy, epilepsy, radiological findings, and treatment received. Using the Chi-square test or Fisher’s exact test for categorical data, the difference between the proportion of patients stratified by HIE stage and their neurodevelopmental outcomes was analysed. The p-value threshold for statistical significance was set at 0<0.05. The statistical analyses were conducted using version 15 of the STATA® software (StataCorp, College Station, TX, USA).
Results
Description of the Cases and Control
Initially, 79 infants with HIE were identified; however, after analysing the medical records of these infants, 19 infants were excluded from the case group (incomplete data), leaving 60 infants with an HIE diagnosis for analysis (which formed the study cases group). Of these cases, 234 infants (the control group) were matched, bringing the total number of infants included in the final case-control analysis to 294 (Figure 1). Then, the case group was retrospectively followed through their medical records for the neurodevelopmental outcome, which was available for 55 HIE cases, and these were included in the cohort analysis. Table 1 displays the maternal and labour characteristics of the HIE cases analysed and the control cases. The average maternal age for the study sample was 30.6 (5.6) years. The average maternal age was comparable across children with and without HIE (p≥0.05). The proportion of women with gestational diabetes was considerably greater among children with HIE compared to the control group (26.9% vs 13.6%) (p-value = 0.010), and the occurrence of polyhydramnios was significantly higher among HIE cases compared to controls (3.1% vs 0.4%) (p-value = 0.041). The prevalence of peripartum distress during childbirth was considerably greater among children with HIE (case group) compared to infants in the control group compared to the case group (1.2% vs 78.3%) (p-value < 0.001).
 |
Table 1 Maternal and Labor Characteristics for the Hypoxic-Ischemic Encephalopathy Cases and Their Matched Controls |
 |
Figure 1 Flow chart describing the enrollment of the hypoxic-ischemic encephalopathy (HIE) cases and controls. |
The majority of HIE patients and controls were male (56.4%), with a mean gestational age of 38.8 weeks (SD = 1.6) (Table 2). Children with HIE were much more likely to be born to mothers who suffered maternal uterine rupture, and showed considerably higher rates of meconium-stained amniotic fluid and nuchal cord compared to controls (Table 2). Similarly, the Apgar scores for 1, 5, and 10 minutes were significantly lower among HIE cases than among controls, with HIE cases significantly more likely to have 5- and 10-min Apgar scores below 7 on average. Of the HIE patients that required resuscitation, 77.0% were intubated. In addition, congenital abnormalities were more prevalent among HIE cases than among the control group; (p-value<0.001).
 |
Table 2 Intrapartum-, Postpartum-, and Neonatal-Related Characteristics for the Hypoxic-Ischemic Encephalopathy Cases and Their Matched Controls |
Factors Associated with HIE Cases Compared to Controls
Table 3 presents the results of a univariate logistic regression study of clinical and labour characteristics linked with HIE. Compared to infants in the control group, infants with HIE were twice as likely to be born to mothers with maternal comorbidities (OR 2.68, 95% CI 1.45–4.96, p≤0.05), and this remained unchanged after controlling for other variables. Similarly, infants with HIE were more likely than infants in the control group to experience prepartum and intrapartum complications (p≤0.05).
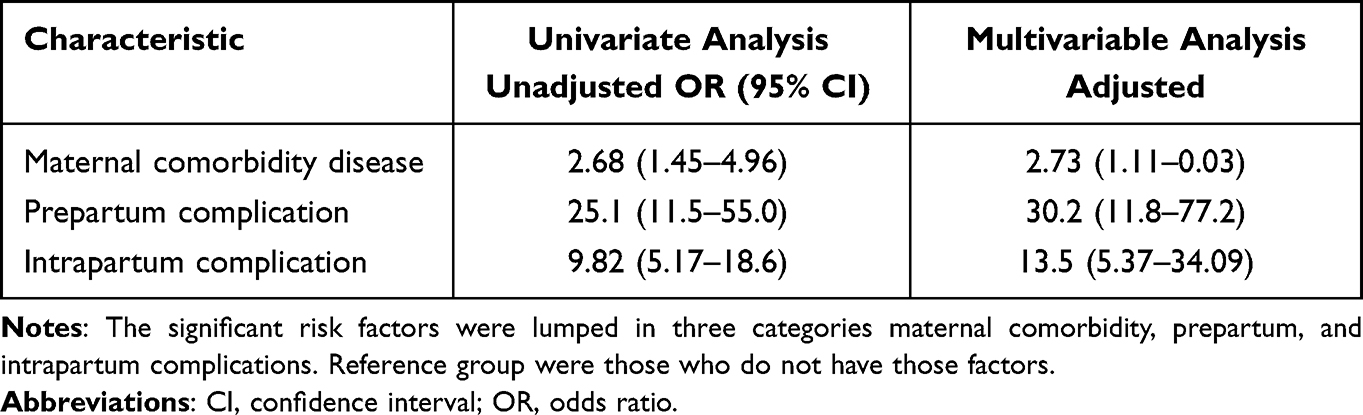 |
Table 3 Clinical and Labor Characteristics and Factors Associated with Hypoxic-Ischemic Encephalopathy Cases Compared to Control Cases |
Description of the Clinical Characteristics of HIE Cases
The clinical outcomes and complications of HIE patients are detailed in Table 4. Sixty infants with HIE (case group) were included in this investigation. Of these, 28.3% had mild HIE (ie, stage 1), 36.6% had moderate HIE (ie, stage 2), and 35.1% of infants had severe HIE (ie, stage 3). Table 4 presents the clinical outcomes and neurological complications of the HIE cases, stratified by HIE severity stage, for all HIE cases. The most prevalent characteristic among HIE cases was hypotonia (60%), followed by normal muscular tone (29.3%) and hypertonia (10%). Seventy-five percent of all HIE cases and 89% of HIE stage 2 cases were treated with therapeutic hypothermia. Only patients with moderate to severe HIE are administered therapeutic hypothermia, per centre policy. Imaging abnormalities on magnetic resonance imaging (MRI) were more common in HIE stage 3 patients than in HIE stages 2 or 1. Around 44.8% of HIE cases had neonatal seizures, of which 82% had simple seizures (defined as seizures in which the patient maintains consciousness) and 17% were intractable. At hospital discharge following the diagnosis of HIE, phenobarbital was the most commonly recommended drug for 37 cases (62%). In eight patients (13.3%) with HIE, audiology tests were abnormal, autism spectrum disorder was present in two patients (3.3%), and attention deficit hyperactivity disorder was present in two individuals (3.3%).
 |
Table 4 Clinical Outcomes and Complication of the Patients with Hypoxic-Ischemic Encephalopathy |
Epilepsy was identified in 6.6% of HIE cases, and of those with epilepsy, three (75%) patients had uncomplicated epilepsy (two patients received levetiracetam and the other received valproic acid) and one patient had intractable epilepsy (and therefore received levetiracetam and topiramate). Around 28% of HIE patients had first EEG background information in their medical file; of these, 56% had a normal first EEG background and 40% had an abnormal one. Nine (30%) of these individuals showed epileptiform activity on their initial EEG, while five (16%) had a burst suppression pattern. Seven individuals (41%) exhibited a final EEG pattern, of which four (23%) exhibited aberrant epileptiform activity and none exhibited a burst suppression pattern.
Neurodevelopmental Outcome of HIE Cases During 24 Months After Delivery
A total of 55 HIE infants out of the original 60 HIE infant cases were included in the study and had a complete follow-up over 24 months. Table 5 displays the neurodevelopmental outcomes at 24 months for the 55 HIE infants whose records were complete. In total, 42 infants (76.3%) had no delay in gross motor skills development, whereas 3.5%, 9.1%, and 10.9% had mild, moderate, or severe delays in gross motor skills development, respectively. The majority of individuals with a moderate to severe delay in gross motor development had HIE stage 3. Similarly, 78.1% of the 55 infants with HIE had no delay in the development of their fine motor skills, whereas 12.7% had a severe delay in the development of their fine motor skills, and all of them had HIE stage 3. A total of 67.6% of all HIE cases exhibited no delay in language skills, while 9% exhibited mild delay, 10.9% exhibited moderate delay, and 12.7% exhibited a severe delay. Around 78.1% of HIE cases exhibited no delay in the development of social skills, while 1.8% and 5.4% of cases exhibited mild and moderately severe delays, respectively. Approximately 14.5% of individuals exhibited severe social developmental deficits, and 40% had HIE stage 3 (Table 5).
 |
Table 5 Neurodevelopmental Outcome After 24-Months Follow-Up According to the HIE Staging |
Discussion
The objectives of this study were to identify risk factors for HIE and to describe the clinical and neurological characteristics of infants diagnosed with HIE. Intrapartum risk factors, such as placenta abruption, uterine rupture, meconium-stained amniotic fluid, and nuchal cord, were substantially more prevalent among HIE cases. Two-thirds of the HIE cases exhibited a mild delay in gross motor skills development at the age of 24 months, but the majority had no delay in fine motor, language, or social skills development, respectively.
Previous studies have investigated the maternal and neonatal factors associated with an elevated risk of HIE.3,13–15,21 Consistent with previous research, maternal comorbidities such as gestational diabetes were prevalent in our study among mothers who had a child with HIE compared to the control group. Newborns whose mothers had comorbidities were twice as likely to have HIE compared to infants whose mothers did not have comorbidities.21 Previous research indicated maternal hypertension as a frequent risk factor for HIE; however, our study failed to reveal a significant link (p = 0.42).1
Compared to the control group, the HIE cases were shown to have a considerable risk for the prepartum complication/event of peripartum distress during labour (78% vs 1.2%), such as polyhydramnios (3.1% vs.0.4%). Regarding other prenatal complications/events, such as GBS screening positivity, breech presentation, and oligohydramnios, the HIE cases did not demonstrate statistical significance (p > 0.05) when compared to the controls. Surprisingly, our analysis found no connection between non-cephalic presentation and the incidence of HIE (5% vs 2.5%). This contradicts the conclusions of the Abha City (southwest Saudi Arabia) study conducted in 2005.17 Multiple factors could have contributed to the difference between the two studies’ findings. High-risk pregnancies, including obesity, the presence of diabetes mellitus, high blood pressure, intrauterine growth restriction, multiple pregnancy (twins, triplets, or more), the presence of autoimmune disorders, smoking status, maternal age (a mother who is under 20 or over 35) and a history of complications in previous pregnancies are important factors that might have increased the risk of HIE and may account for the differences between our current study and the previous study in Abha.22 Unfortunately, however, we did not have information on these variables to explore the difference in the maternal profiles between the two studies.
The majority of HIE cases were male, which was substantially different from the control group (p=0.03), and the incidence of acute intrapartum events was likewise higher in HIE cases than in controls. The incidence of placenta abruption, uterine rupture, meconium-stained amniotic fluid, and nuchal cord was substantially higher among HIE cases (p≤0.05). Similarly, the Apgar ratings for 1, 5, and 10 minutes were considerably lower for HIE cases than for controls. Significantly more HIE cases had average 5- and 10-minute Apgar scores below 7 than non-HIE cases. These findings are comparable to those of a 2005 local study that identified the following risk variables as significant: mode of delivery, antepartum haemorrhage, low Apgar score, and low birth weight.23 In the HIE group, congenital abnormalities and dysmorphism were more prevalent than in the control group (p<0.001): 17% vs 3.4% and 13% vs 0%, respectively. This confirms the findings of previous studies that identified HIE risk factors, which defined meconium-stained amniotic fluid as a risk factor that increases the risk of HIE by 12-fold.16 Both antepartum and intrapartum conditions are considered to be potential risk factors for the development of HIE. Antepartum factors, including gestation above 41 weeks, and intrapartum factors, including prolonged membrane rupture, thick meconium, abnormal cardiotocography, sentinel event, shoulder dystocia, tight nuchal cord, and failed suction, are significant risk factors for HIE.24
Around 77% of all HIE patients who had resuscitation were intubated; 95% required bag valve mask ventilation and positive pressure breathing; only nine individuals had a cardiac massage, and two patients were administered epinephrine.
Magnetic resonance imaging (MRI) is the most sensitive and specific imaging method for assessing infants suspected of having hypoxic-ischaemic brain injury.25,26 Brain MRI was categorised as the final HIE-recommended pattern in this study.27 MRI abnormalities were more prevalent in cases of severe HIE (stage 3) than in cases of moderate and mild HIE (stages 2 and 1). Watershed prominent lesions were the most numerous, followed by global, white matter, and basal ganglia or thalamus lesions (p<0.001). Although HIE cases were more likely to have abnormal brain CT scans than controls, we were unable to demonstrate a significant link (p=0.17). Imaging plays a crucial role in the diagnosis and treatment of HIE, guiding case management in the acute setting and providing significant prognostic information for the long term.28 To make an accurate radiologic diagnosis of HIE, one must be conversant with the numerous imaging symptoms of this injury. Brain maturity, the duration and severity of the injury, and the type and timing of imaging examinations all influence the findings in HIE.28 Severe hypoxia-ischaemia preferentially affects the deep grey matter in both preterm and term infants, with perirolandic involvement being detected more commonly in the latter age group. Less severe injuries cause periventricular white matter injury and intraventricular haemorrhages in preterm infants, and infarcts in the parasagittal watershed territory in term neonates. In the neonatal period, acute injuries result in diffuse damage to grey matter, but the perirolandic cortex and structures supplied by the posterior circulation are mostly spared.28
In our study, around 75% of all HIE cases and 89% of severe HIE (stage 3) cases were treated with therapeutic hypothermia. In the majority of these patients, erythropoietin was also administered. This includes 84% of patients with severe HIE (stage 3) and 72% of patients with moderate HIE (stage 2). In a non-human animal model of prenatal hypoxia, a previous study found that therapy with erythropoietin and hypothermia decreased cerebral palsy. In addition, the efficacy of combining moderate hypothermia and erythropoietin for the treatment of neonatal HIE was promising.29
Neurodevelopmental outcomes are more prevalent in cases of severe HIE (stage 3) than in mild and moderate cases (stages 1 and 2). These include intellectual disability, learning disabilities, autism spectrum disorder, attention deficit hyperactivity disorder, cerebral palsy, and epilepsy. Cerebral palsy and epilepsy were significantly associated with severe HIE (stage 3) (p<0.02). Cerebral palsy cases accounted for 6.3% of all severe HIE (grade 3) cases, with the majority being quadriplegia, one case being diplegia, and other forms (hemiplegia or monoplegia) not noted in any patients. A total of 42 newborns with HIE had abnormal muscle tone, with the majority (60%) having hypotonia. At the 24-month follow-up, concerning the neurodevelopmental outcomes, which comprise gross motor, fine motor, language, and social skills, only 24% of HIE cases exhibited gross motor skills development delays, while 22%, 33%, and 22% had delays in fine motor, language, and social skills, respectively. The majority of severe HIE (stage 3) cases exhibited substantial delays in all four neurodevelopmental-outcome domains, with language skills development being notably affected (p<0.05). However, all developmental skills indicated a significant connection with the severity of HIE. The previous literature reported that the spectrum of developmental outcomes associated with HIE includes motor delays, learning difficulties, cognitive impairment, neurodevelopmental disorders, and visual and hearing impairments.30
In over half of the HIE cases, a neonatal seizure was identified, with the majority being a simple seizure that was most frequently treated with phenobarbital. Around 38% of HIE patients with neonatal seizures were discharged without antiepileptic therapy. In 6.6% of HIE cases, epilepsy was identified, with the majority having uncomplicated seizures that required only one drug. In HIE cases with epilepsy, levetriacetam was the most frequently prescribed medicine, followed by valporic acid. An electroencephalogram (EEG) was performed in only 28% of HIE cases, and aberrant background was frequently noted in the initial EEG. In addition, in the initial EEG, epileptiform activity was detected in nine patients, although the burst suppression pattern (shown in Figure 2) was detected in only five individuals. In the previous EEG, only 23% of patients had aberrant results, which included abnormal epileptiform activity. In the 2005 study conducted in Abha City (southwest Saudi Arabia),17 moderate or severe HIE occurred in approximately 63% of all HIE cases, with seizures occurring in 67% of these cases. Seizures are common in infants with hypoxic-ischaemic encephalopathy and are strongly associated with neurodevelopmental outcomes that are detrimental. Preclinical research suggests that the majority of anticonvulsants are associated with detrimental effects on the developing brain.31 Levetiracetam appears to have fewer possible neurotoxic effects than other anticonvulsants; yet, it may not be more effective. Small clinical trials suggest that prophylactic administration of phenobarbital may improve neurodevelopmental outcomes in comparison to delayed treatment; however, additional, high-quality research is needed to validate this.31
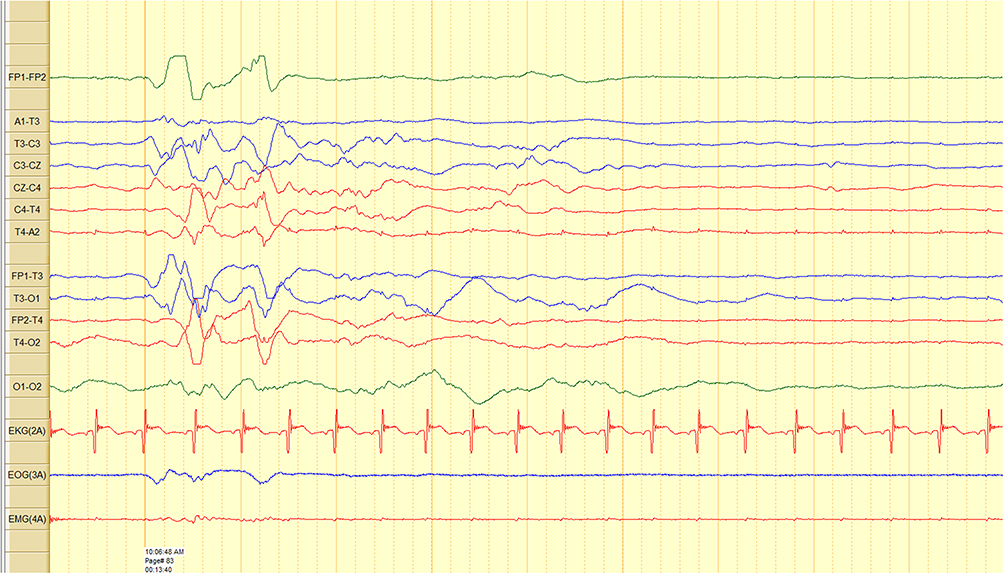 |
Figure 2 EEG in neonate with Hypoxic ischemic encephalopathy showing burst suppression pattern. |
This study was able to uncover prenatal/antenatal and perinatal variables related to HIE that were more thorough and precise than those discovered in other Western Asian studies, particularly local studies conducted in Saudi Arabia. This study had limitations. First, the data were gathered from a single centre, limiting the generalisability of this study’s findings and emphasising the need for a nationwide register of HIE cases. By identifying risk variables and analysing the most effective management strategies, such a registry would greatly assist the care of newborns with HIE by identifying risk factors and assessing the most effective management plans. The second limitation of this investigation was the potential effect of the presence of unmeasured or uncollected confounders between cases and controls, which could either underestimate or overstate the associated risk. Our study sample size was relatively small and additional research with a larger sample size is necessary to improve the accuracy of our estimates. Lastly, the completeness of the obstetric, neonatal, and neurologists’ records from which the study data were retrieved or obtained may have an impact on the validity of the findings. In light of these limitations, it is recommended to interpret the results with caution.
Conclusion
In neonates diagnosed with HIE, maternal comorbidities such as gestational diabetes, fetal deceleration, and polyhydramnios were more prevalent. These results demonstrate the need to implement stringent preventative measures, especially for high-risk pregnancies. The severity grade of HIE can be utilised as a predictor of neurodevelopmental outcomes, particularly gross motor skills. A minimum of 24 months of neurodevelopmental follow-up is required to improve the care and rehabilitation of patients. Further research is needed to explore the role of HIE severity in predicting infants’ neurodevelopmental outcomes.
Abbreviations
HIE, hypoxic-ischemic encephalopathy; GA, gestational age; NICU, neonatal intensive care unit; DPP, developmental policies and procedures; GBS, group B streptococcus test; OR, odds ratio; CI, confidence interval; MRI, magnetic resonance imaging; EEG, electroencephalography.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval
This study has been approved by research ethics committee, Institutional Review Board (IRB), King Abdullah International Medical Research Centre (KAIMRC), Riyadh, Saudi Arabia (reference number RC19/302/R). All methods were carried out in accordance with relevant guidelines and regulations or declaration of Helsinki. The need for informed consent was waived by the ethics committee/Institutional Review Board of King Abdullah International Medical Research Center (KAIMRC), because of the retrospective nature of the study and based on the fact that patients gave their consent upon admission to hospital. All patients’ data were kept anonymized in a password secured external driver by the primary investigator.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interests.
References
1. Dhillon SK, Wassink G, Lear CA, et al. The effect of size, maturation, global asphyxia, cerebral ischemia, and therapeutic hypothermia on the pharmacokinetics of high-dose recombinant erythropoietin in fetal sheep. Int J Mol Sci. 2020;21(9):1–20. doi:10.3390/ijms21093042
2. Finer NN, Robertson CM, Richards RT, Pinnell LE, Peters KL. Hypoxic-ischemic encephalopathy in term neonates: perinatal factors and outcome. J Pediatr. 1981;98(1):112–117. doi:10.1016/S0022-3476(81)80555-0
3. Lee AC, Kozuki N, Blencowe H, et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr Res. 2013;74(1):50–72. doi:10.1038/pr.2013.206
4. Ferriero DM. Neonatal brain injury. N Engl J Med. 2004;351(19):1985–1995. doi:10.1056/NEJMra041996
5. Shankaran S, Laptook AR, Ehrenkranz RA, et al.; National Institute of Child Health and Human Development Neonatal Research Network. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005;353(15):1574–1584. doi:10.1056/NEJMcps050929
6. Long M, Brandon DH. Induced hypothermia for neonates with hypoxic-ischemic encephalopathy. J Obstet Gynecol Neonat Nurs. 2007;36(3):293–298. doi:10.1111/j.1552-6909.2007.00150.x
7. Busl KM, Greer DM, Arciniegas DB. Hypoxic-ischemic brain injury: pathophysiology, neuropathology and mechanisms. NeuroRehabilitation. 2010;26(1):5–13. doi:10.3233/NRE-2010-0531
8. Cotten CM, Shankaran S. Hypothermia for hypoxic-ischemic encephalopathy. Expert Rev Obstet Gynecol. 2010;5(2):227–239. doi:10.1586/eog.10.7
9. Silveira RC, Procianoy RS. Hypothermia therapy for newborns with hypoxic ischemic encephalopathy. J Pediatr. 2015;91(1):S78–S83. doi:10.1016/j.jped.2015.07.004
10. Tagin MA, Woolcott CG, Vincer MJ, Whyte RK, Stinson DA. Hypothermia for neonatal hypoxic ischemic encephalopathy: an updated systematic review and meta-analysis. Arch Pediatr Adolesc Med. 2012;166(6):558–566. doi:10.1001/archpediatrics.2011.1772
11. Ma H, Sinha B, Pandya RS, et al. Therapeutic hypothermia as a neuroprotective strategy in neonatal hypoxic-ischemic brain injury and traumatic brain injury. Curr Mol Med. 2012;12(10):1282–1296. doi:10.2174/156652412803833517
12. Malla RR, Asimi R, Teli MA, Shaheen F, Bhat MA. Erythropoietin monotherapy in perinatal asphyxia with moderate to severe encephalopathy: a randomized placebo-controlled trial. J Perinatol. 2017;37(5):596–601. doi:10.1038/jp.2017.17
13. Michaeli J, Srebnik N, Zilberstein Z, Rotem R, Bin-Nun A, Grisaru-Granovsky S. Intrapartum fetal monitoring and perinatal risk factors of neonatal hypoxic-ischemic encephalopathy. Arch Gynecol Obstet. 2021;303(2):409–417. doi:10.1007/s00404-020-05757-2
14. Novak CM, Eke AC, Ozen M, Burd I, Graham EM. Risk factors for neonatal hypoxic-ischemic encephalopathy in the absence of sentinel events. Am J Perinatol. 2019;36(1):27–33. doi:10.1055/s-0038-1639356
15. Parker SJ, Kuzniewicz M, Niki H, Wu YW. Antenatal and intrapartum risk factors for hypoxic-ischemic encephalopathy in a US birth cohort. J Pediatr. 2018;203:163–169. doi:10.1016/j.jpeds.2018.08.028
16. Torbenson VE, Tolcher MC, Nesbitt KM, et al. Intrapartum factors associated with neonatal hypoxic ischemic encephalopathy: a case-controlled study. BMC Pregnancy Childbirth. 2017;17(1):1–7. doi:10.1186/s12884-017-1610-3
17. AlShehri M, Eid WA. Risk factors for development of hypoxic-ischemic encephalopathy in Abha City-southwestern Saudi Arabia. Afr J Med Med Sci. 2005;34(3):207–212.
18. American College of Obstetricians and Gynecologists and The American Academy of Pediatrics, Neonatal Encephalopathy Committee Opinion. Neonatal Encephalopathy and Cerebral Palsy: Defining the Pathogenesis and Pathophysiology. Washington, DC: American College of Obstetricians and Gynecologists and The American Academy of Pediatrics; 2003.
19. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol. 1976;33(10):696–705. doi:10.1001/archneur.1976.00500100030012
20. Michalec D. Encyclopedia of child behavior and development. In: Goldstein S, Naglieri JA, editors. Bayley Scales of Infant Development.
21. Pálsdóttir K, Thórkelsson T, Hardardóttir H, Dagbjartsson A. Fósturköfnun og heilakvilli--áhaettuthaettir og afleidingar fyrir nýbura [Birth asphyxia, neonatal risk factors for hypoxic ischemic encephalopathy]. Laeknabladid. 2007;93(10):669–673.
22. Lorain P, Bower A, Gottardi E, et al. Risk factors for hypoxic-ischemic encephalopathy in cases of severe acidosis: a case-control study. Acta Obstet Gynecol Scand. 2022;101(4):471–478. doi:10.1111/aogs.14326
23. Itoo BA, Al-Hawsawi ZM, Khan AH. Hypoxic ischemic encephalopathy. Incidence and risk factors in North Western Saudi Arabia. Saudi Med J. 2003;24(2):147–153.
24. Martinez-Biarge M, Diez-Sebastian J, Wusthoff CJ, Mercuri E, Cowan FM. Antepartum and intrapartum factors preceding neonatal hypoxic-ischemic encephalopathy. Pediatrics. 2013;132(4):e952–9. doi:10.1542/peds.2013-0511
25. Chao CP, Zaleski CG, Patton AC. Neonatal hypoxic-ischemic encephalopathy: multimodality imaging findings. Radiographics. 2006;26(1):S159–S172. doi:10.1148/rg.26si065504
26. Trivedi SB, Vesoulis ZA, Rao R, et al. A validated clinical MRI injury scoring system in neonatal hypoxic-ischemic encephalopathy. Pediatr Radiol. 2017;47(11):1491–1499. doi:10.1007/s00247-017-3893-y
27. Mao J. Patterns of brain injury in neonatal hypoxic-ischemic encephalopathy on magnetic resonance imaging: recommendations on classification. Zhongguo dang dai er ke za zhi. 2017;19(12):1225–1233. doi:10.7499/j.issn.1008-8830.2017.12.001
28. Huang BY, Castillo M. Hypoxic-ischemic brain injury: imaging findings from birth to adulthood. Radiographics. 2008;28(2):417–617. doi:10.1148/rg.282075066
29. Oorschot DE, Sizemore RJ, Amer AR. Treatment of neonatal hypoxic-ischemic encephalopathy with erythropoietin alone, and erythropoietin combined with hypothermia: history, current status, and future research. Int J Mol Sci. 2020;21(4):1–27. doi:10.3390/ijms21041487
30. Mbatha S, Nakwa FL, Thandrayen K, Velaphi S. Neurodevelopmental outcome in neonates with hypoxic-ischaemic encephalopathy managed with therapeutic hypothermia in a tertiary-level public hospital outside an intensive care unit setting. Paediatr Int Child Health. 2021;41(3):171–176. doi:10.1080/20469047.2021.1967625
31. Zhou KQ, McDouall A, Drury PP, et al. Treating seizures after hypoxic-ischemic encephalopathy-current controversies and future directions. Int J Mol Sci. 2021;22(13):1–14.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.