Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Characteristics and Risk Factors Analysis of Nontuberculous Mycobacterial Pulmonary Disease Complicated with Bronchiectasis
Authors Li J ![]() , Zeng P, Mu X, Cai C
, Zeng P, Mu X, Cai C ![]()
Received 14 November 2025
Accepted for publication 4 February 2026
Published 23 February 2026 Volume 2026:19 483326
DOI https://doi.org/10.2147/IDR.S483326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Jun Li, Pu Zeng, Xiangdong Mu, Cunliang Cai
Department of Respiratory and Critical Care Medicine, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, 102218, People’s Republic of China
Correspondence: Cunliang Cai, Email [email protected] Xiangdong Mu, Email [email protected]
Background: Nontuberculous mycobacteria pulmonary disease (NTM-PD) frequently coexists with bronchiectasis. This study aimed to compare clinical profiles and identify risk factors between NTM-PD patients with/without bronchiectasis and explore differences between rapid- vs slow-growing non-tuberculous mycobacteria (NTM) species.
Methods: A retrospective analysis was conducted on patients diagnosed with NTM-PD and admitted to Beijing Tsinghua Changgung Hospital between April 2021 and April 2025. Among 496 inpatients with pulmonary diseases who underwent metagenomic next-generation sequencing (mNGS) analysis of bronchoalveolar lavage fluid, NTM were identified in 57 patients. Ultimately, 43 of these cases were confirmed and diagnosed as having NTM-PD. Relevant clinical data were collected, and the association between each variable and adverse outcomes was assessed using univariate and multivariate logistic regression analyses.
Results: Among the 43 confirmed NTM-PD patients, 24 had concurrent bronchiectasis (NTM-PD with bronchiectasis group) and 19 did not (NTM-PD group). In terms of baseline characteristics, the NTM-PD with bronchiectasis had a significantly higher proportion of females (79.17% vs 31.57%, P=0.002) and lower BMI (19.46 vs 22.46, P=0.023). Slow-growing NTM (SGM, mainly Mycobacterium avium complex [MAC]) was more common in the NTM-PD with bronchiectasis group (70.83% vs 31.58%, P=0.010); rapid-growing NTM (RGM, mainly M. abscessus) was more prevalent in the NTM-PD group (57.89% vs 20.83%, P=0.013). The positive rate of T-SPOT.TB in the NTM-PD group was higher than that in the NTM-PD with bronchiectasis group (47.37% vs 8.33%, P=0.010). Multivariate logistic regression identified female sex as an independent risk factor for NTM-PD complicated with bronchiectasis (OR=17.784, 95% CI: 1.103– 286.857, P=0.042), while T-SPOT.TB was not (OR=0.047, 95% CI: 0.002– 1.341, P=0.074).
Conclusion: Female sex is an independent risk factor for NTM-PD complicated with bronchiectasis. NTM-PD patients with bronchiectasis are more likely to be infected with SGM (especially MAC), while those without bronchiectasis tend to have RGM (especially M. abscessus) infection.
Keywords: nontuberculous mycobacteria, bronchiectasis, rapid-growing mycobacteria, slow-growing mycobacteria, risk factors
Introduction
Nontuberculous mycobacterial pulmonary disease (NTM-PD) has emerged as a growing global health concern, with increasing incidence and prevalence reported in both immunocompetent and immunocompromised populations over recent decades.1 Unlike tuberculosis, NTM-PD is characterized by chronic, often indolent infections caused by ubiquitous environmental mycobacteria, such as Mycobacterium avium complex (MAC) and Mycobacterium abscessus, which pose significant diagnostic and therapeutic challenges.2,3 Among the diverse clinical manifestations of NTM-PD, its association with structural lung diseases-particularly bronchiectasis-has garnered substantial attention.4 Bronchiectasis is a chronic respiratory syndrome characterized by permanent, abnormal dilation of the bronchi, leading to impaired mucus clearance, persistent airway inflammation, and recurrent bacterial infections. Its clinical significance lies not only in structural damage but also in a constellation of distinct symptoms, including chronic productive cough, daily purulent sputum production, hemoptysis, dyspnea, and constitutional symptoms such as fatigue and weight loss.5,6 These symptoms collectively contribute to frequent exacerbations, reduced quality of life, and accelerated lung function decline.7 Bronchiectasis is increasingly recognized as both a predisposing factor and a consequence of NTM-PD, creating a vicious cycle of inflammation, infection, and progressive lung damage.8,9 The bidirectional relationship between NTM-PD and bronchiectasis remains incompletely understood.
Current evidence suggests that the co-occurrence of NTM-PD and bronchiectasis is associated with worse clinical outcomes, such as a more rapid decline in lung function, increased frequency of exacerbations, and elevated mortality rates.10 Moreover, the superimposition of NTM infection in bronchiectasis patients may alter or amplify the typical symptomatology-for instance, by increasing sputum volume, altering its characteristics, or leading to more systemic inflammatory responses-which in turn complicates clinical management and prognostic assessment.7 While bronchiectasis is widely acknowledged as a risk factor for NTM colonization and infection,11,12 specific clinical characteristics and independent predictors that distinguish NTM-PD patients with concurrent bronchiectasis from those without are poorly defined.
This study aims to address these knowledge gaps by conducting a retrospective cohort analysis to systematically delineate the clinical and radiological features of NTM-PD patients complicated with bronchiectasis. Additionally, we seek to identify independent risk factors associated with the coexistence of these conditions, with a focus on demographic variables, comorbidities, microbiological profiles, and imaging findings. By elucidating these associations, our findings may inform early risk stratification, optimize multidisciplinary management, and ultimately improve prognostication for this vulnerable patient population.
Materials and Methods
Study Population and Design
A retrospective observational study was undertaken involving adult patients diagnosed with NTM-PD who were admitted to Beijing Tsinghua Changgung Hospital between April 2021 and April 2025. Patients who met the criteria were enrolled in the study: (1) Patients present with respiratory symptoms and/or systemic symptoms. (2) Chest imaging examinations reveal cavitary shadows, multifocal bronchiectasis, and multiple small nodular lesions. (3) Meet one of the following criteria: a. Two distinct sputum specimens test positive for NTM culture and are identified as the same pathogenic species, and/or molecular biological testing confirms the presence of the same causative agent; b. A single positive NTM culture and/or molecular biological test (eg, metagenomic next-generation sequencing [mNGS]) performed on bronchoalveolar lavage fluid (BALF) or bronchial wash fluid; c. Characteristic histopathological findings of mycobacterial disease-such as granulomatous inflammation or positive acid-fast staining-identified via bronchoscopy or other lung biopsy methods, accompanied by either: (i) a positive NTM culture and/or molecular biological test result or (ii) a positive NTM culture and/or molecular detection in one or more sputum specimens, bronchial wash fluid, or bronchoalveolar lavage fluid. (4) Other lung diseases have been excluded.13,14 The process of patient enrollment and screening is presented in Figure 1. Among the 496 patients who underwent mNGS testing, NTM was detected in 57 cases; after excluding 14 cases, a total of 43 patients were confirmed to have NTM-PD. The study was approval by the Ethics Committee of the Beijing Tsinghua Changgung Hospital (No. 22447-6-01).
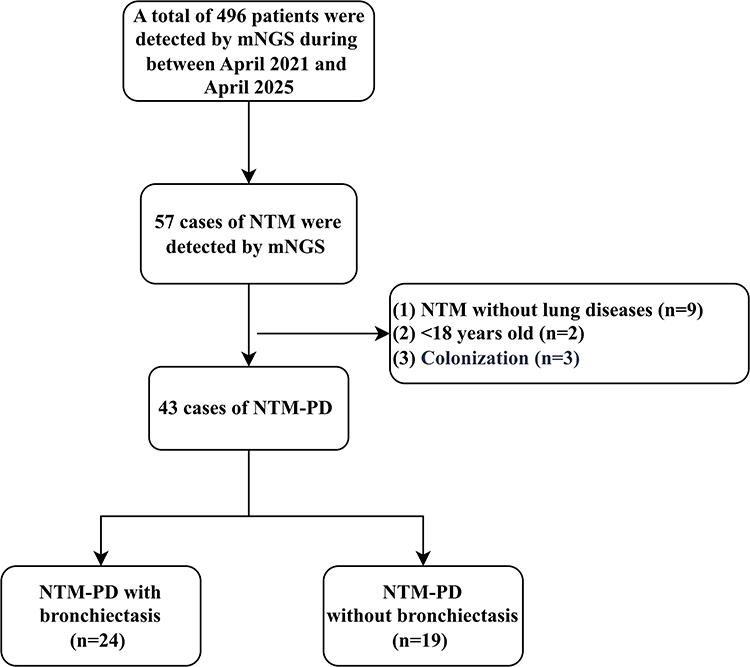 |
Figure 1 Flow chart of patient enrollment. |
Data Collection
Cases were identified through the hospital’s electronic medical record system. Data were systematically collected across multiple domains, including baseline demographic characteristics (age, sex, smoking history, etc), comorbidities, symptoms, microbiological profiles, and imaging features, etc. Additionally, pulmonary function tests and laboratory findings during clinical stability were documented, along with therapeutic regimens and longitudinal outcomes (encompassing survival status) over a 36-month observation period.
All participants underwent high-resolution computed tomography (HRCT) examinations. The diagnosis of bronchiectasis was independently verified by two specialists: a board-certified radiologist with 15 years of HRCT interpretation experience and a pulmonologist specializing in bronchiectasis research.
mNGS Testing
Nucleic Acid Extraction and mNGS Detection
BALF and sputum sample DNA was extracted using the TIANamp Magnetic DNA Kit (Tiangen, Beijing, China) according to the manufacturer’s protocols. Sputum was liquefied by 0.1% DTT (dithiothreitol) for 20 minutes at 56°C before extraction. The quantity and quality of DNA was assessed with the Qubit 2.0 (Thermo Fisher Scientific, USA) and NanoDrop 8000 (Thermo Fisher Scientific, USA), respectively. DNA library construction was performed using the Hieff NGS C130P2 OnePot II DNA Library Prep Kit (Yeasen Biotechnology, Shanghai, China), adhering to the manufacturer’s guidelines. Agilent 2100 system was used for quality control of the DNA libraries, and sequencing was carried out on the DIFESEQ-200 platform (Dinfectome, Nanjing, China) employing a 50-base single-end, approach yielding approximately 20 million reads for the metagenomic workflow.
Bio-Informatics Analysis
Pathogen identification was conducted through bioinformatics analysis utilizing an internally developed pipeline.15 This pipeline facilitated the generation of high-quality sequencing data by removing low-quality reads, adapter contamination, duplicate reads, and reads with a sequence length of less than 36 base pairs. The sequences derived from the human host were aligned to the human reference genome (hs37d5) using Bowtie2 software (version 2.2.6) to ascertain the human host sequences. Reads that could not be mapped to the human genome were retained and subsequently compared against a microbial genome database to identify potential pathogens. This microbial genome database encompasses sequences from bacteria, fungi, viruses, and parasites, and is available for download at https://www.ncbi.nlm.nih.gov/.
Interpretation and Reporting
The elucidation and documentation of the positive outcomes of mNGS are based on the following criteria, which have been previously outlined in the literature.15,16 The criteria for positive detection are as follows: 1) For the identification of Mycobacteria, Nocardia, and Legionella pneumophila, a minimum of one species-specific read is required; 2) For the detection of other bacteria, fungi, viruses, and parasites, a minimum of three specific reads is necessary; 3) Pathogens are excluded if the ratio of microbial reads per million to the negative control (NTC) in the given sample is less than 10.
Statistical Analysis
For continuous variables, non-normally distributed data were summarized as the median with interquartile range (IQR), while normally distributed data were presented as the mean ± standard deviation (SD). Between-group comparisons for continuous variables were performed using the Student’s t-test for normally distributed data or the Mann–Whitney U-test for non-normally distributed data. Categorical variables were described as percentages (%), and group differences were evaluated using the Chi-square test or Fisher’s exact test, depending on sample size and expected frequency assumptions. Statistical significance was defined as a two-tailed P-value <0.05. In univariate analyses, covariates with P <0.05 were selected for inclusion in the final multivariable logistic regression model to identify independent predictors while controlling for confounding factors. All statistical analyses were conducted using IBM SPSS Statistics Version 29.0 (IBM Corp. USA).
Results
Patient Enrollment and Baseline Characteristics
A total of 496 inpatients with pulmonary diseases who underwent BALF mNGS at Beijing Tsinghua Changgung Hospital from April 2021 to April 2025 were screened. Among them, 57 tested positive for NTM; after excluding 9 cases of NTM without lung diseases, 2 cases under 18 years old, and 3 cases of NTM colonization, 43 patients were confirmed as NTM-PD. These patients were divided into two groups: NTM-PD with bronchiectasis (n=24) and NTM-PD without bronchiectasis (NTM-PD group, n=19) (Figure 1).
As shown in Table 1, there was no significant difference in age between the NTM-PD with bronchiectasis group (64.83±14.16 years) and the NTM-PD group (60.7±15.08 years) (P=0.365). However, the proportion of females in the NTM-PD with bronchiectasis group (79.17%, 19/24) was significantly higher than that in the NTM-PD group (31.57%, 6/19) (P=0.002). The body mass index (BMI) of the NTM-PD with bronchiectasis group was significantly lower than that of the NTM-PD group (19.46 vs 22.46, P=0.023). There was no significant difference in smoking history or previous medical history (including chronic obstructive pulmonary disease, pulmonary interstitial fibrosis, tuberculosis, sinusitis, hypertension, diabetes, autoimmune diseases, and tumor) between the two groups.
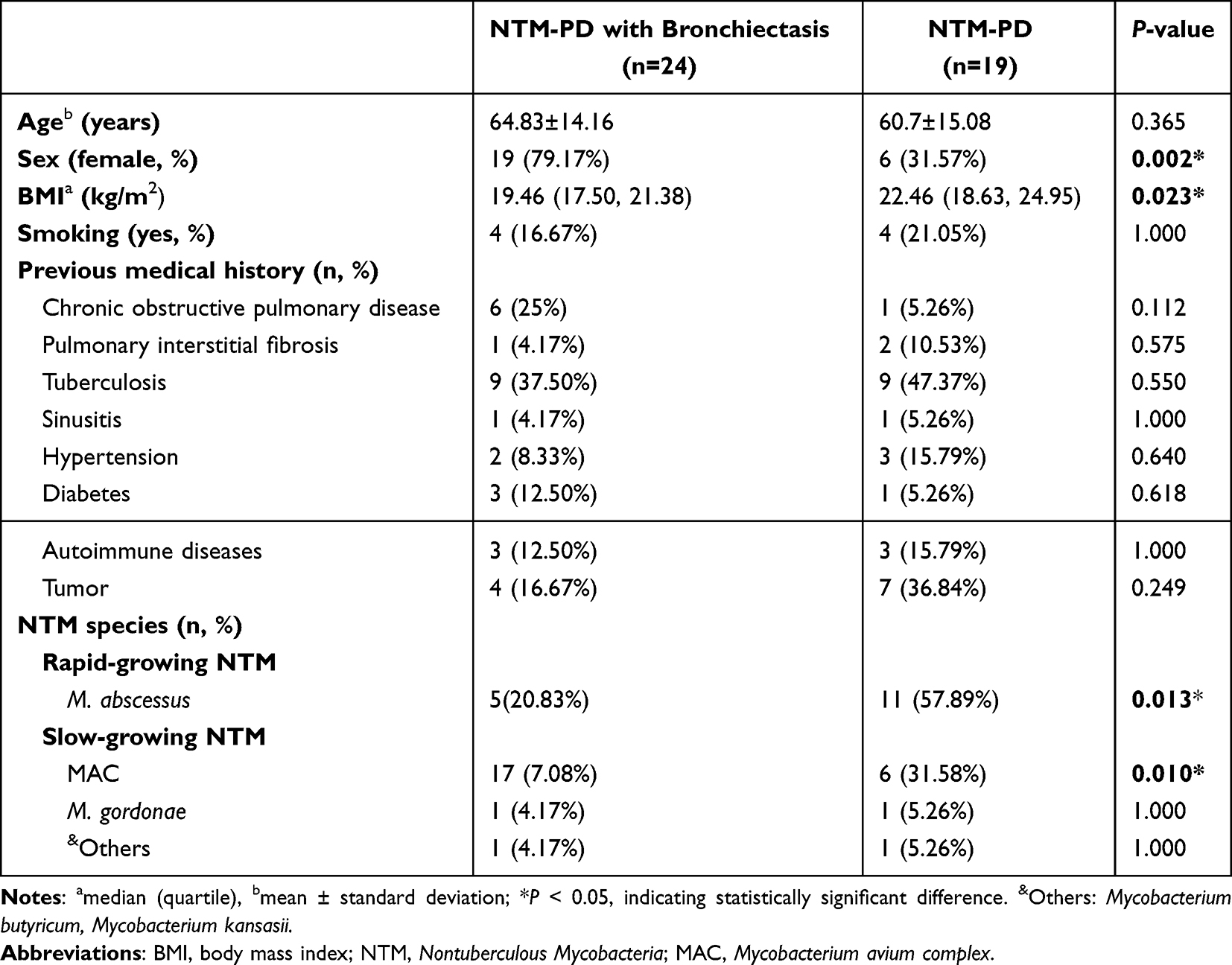 |
Table 1 Baseline Characteristics of NTM-PD Accompanied by Bronchiectasis |
Distribution of NTM Species
As presented in Table 1 and Figure 2A, the distribution of NTM species differed significantly between the two groups. In the NTM-PD with bronchiectasis group, 70.83% (17/24) of patients were infected with slow-growing NTM (SGM) (mainly MAC), while only 31.58% (6/19) in the NTM-PD group had SGM infection (P=0.010). In contrast, the proportion of rapid-growing NTM (RGM) infection (mainly M. abscessus) in the NTM-PD with bronchiectasis group (20.83%, 5/24) was significantly lower than that in the NTM-PD group (57.89%, 11/19) (P=0.013) (Figure 2B). No significant differences were found in other NTM species (eg, M. xenopi, M. kansasii, M. gordonae) between the two groups (all P>0.05).
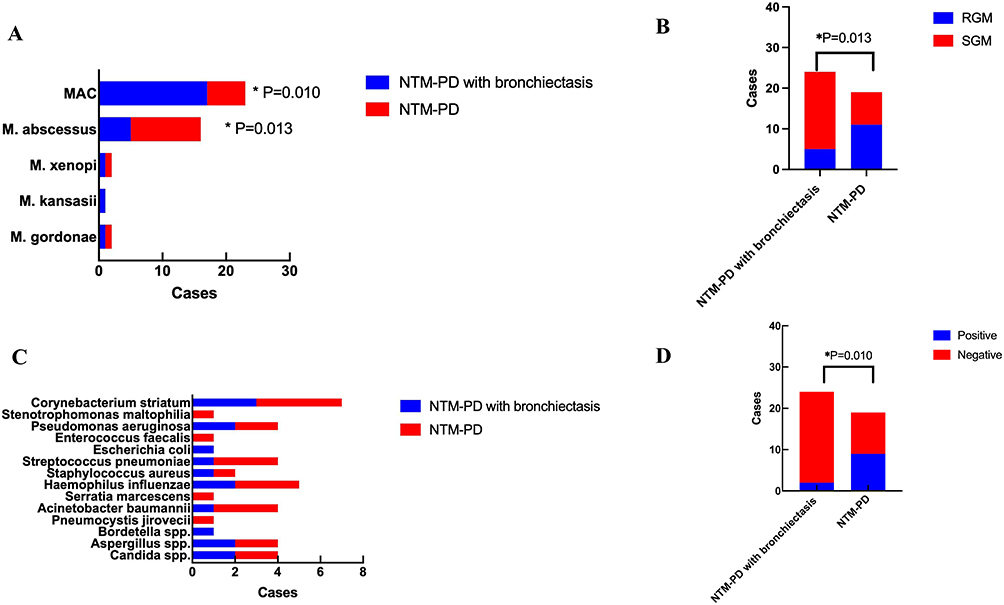 |
Figure 2 (A) Comparison of NTM species between patients with NTM-PD and those with NTM-PD with bronchiectasis. (B) Comparison of rapid-growing mycobacteria (RGM) and slow-growing mycobacteria (SGM) between patients with NTM-PD and those with NTM-PD with bronchiectasis. (C) Comparison of etiological components between patients with NTM-PD and those with NTM-PD with bronchiectasis. (D) Comparison of the T-SPOT.TB positive rates between patients with NTM-PD and those with NTM-PD with bronchiectasis. *P < 0.05, the difference was statistically significant. |
In Figure 2C and Table S1, Mycobacterium tuberculosis (MTB) was not identified among the pathogenic microorganisms assessed. In patients diagnosed with NTM-PD and bronchiectasis, the most prevalent co-occurring bacterial infections were identified as Corynebacterium striatum (n=3), Haemophilus influenzae (n=2), and Pseudomonas aeruginosa (n=2). There was no statistically significant difference in the etiological components between patients with NTM-PD and those with NTM-PD combined with bronchiectasis.
T-SPOT.TB Positive Rate
As shown in Figure 2D and Table 2, the T-SPOT.TB positive rate in the NTM-PD group (n=9, 47.37%) was significantly higher than that in the NTM-PD with bronchiectasis group (n=2, 8.33%), and the difference was statistically significant (P=0.010).
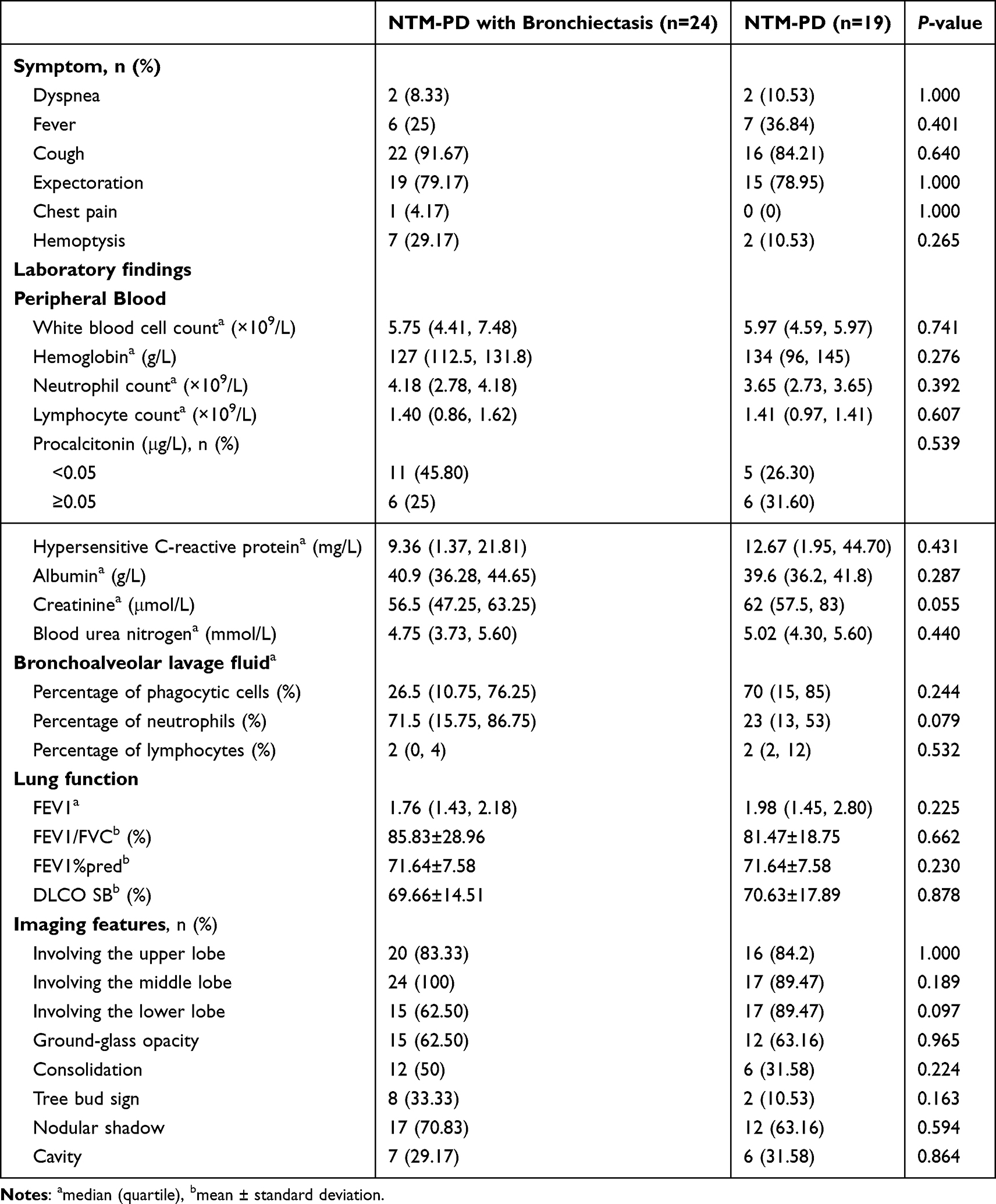 |
Table 2 Clinical Features of NTM-PD with Bronchiectasis Patients |
Comparison of Clinical Characteristics Between the Two Groups of Patients
Table 2 displays the comparison of clinical symptoms between the two groups. The main symptoms included cough, expectoration, fever, dyspnea, chest pain, and hemoptysis. The incidence of cough was the highest in both groups (91.67% in NTM-PD with bronchiectasis group vs 84.21% in NTM-PD group), but there were no significant differences in the incidence of all symptoms between the two groups.
There were no significant differences in peripheral blood indicators (white blood cell count, hemoglobin, neutrophil count, lymphocyte count), inflammatory/nutritional markers (procalcitonin, hypersensitive C-reactive protein, albumin), or renal function indicators (creatinine, blood urea nitrogen) between the two groups. No significant differences were observed in the proportions of phagocytic cells, neutrophils, and lymphocytes in BALF between the two groups. Parameters including FEV1, FEV1/FVC, FEV1%pred, and DLCO SB showed no significant differences between the NTM-PD with bronchiectasis group and the NTM-PD group. There were no significant differences in the involvement of upper, middle, and lower lung lobes, or the presence of ground-glass opacity, consolidation, tree bud sign, nodular shadow, and cavity between the two groups.
Multivariate Analysis of Risk Factors
The results of the multivariate logistic regression analysis are presented in Table 3. After adjusting for potential confounding factors, female sex was identified as an independent risk factor for NTM-PD complicated with bronchiectasis (OR=17.784, 95% CI: 1.103–286.857, P=0.042). Notably, despite the significant difference in T-SPOT.TB positive rate in univariate analysis, T-SPOT.TB was not an independent risk factor for NTM-PD concurrent with bronchiectasis (OR=0.047, 95% CI: 0.002–1.341, P=0.074). Additionally, BMI, infection with RGM- (mainly M. abscessus), infection with SGM (mainly MAC), BALF neutrophil proportion, and sputum/BALF acid-fast bacillus smear/culture positivity were not independent risk factors.
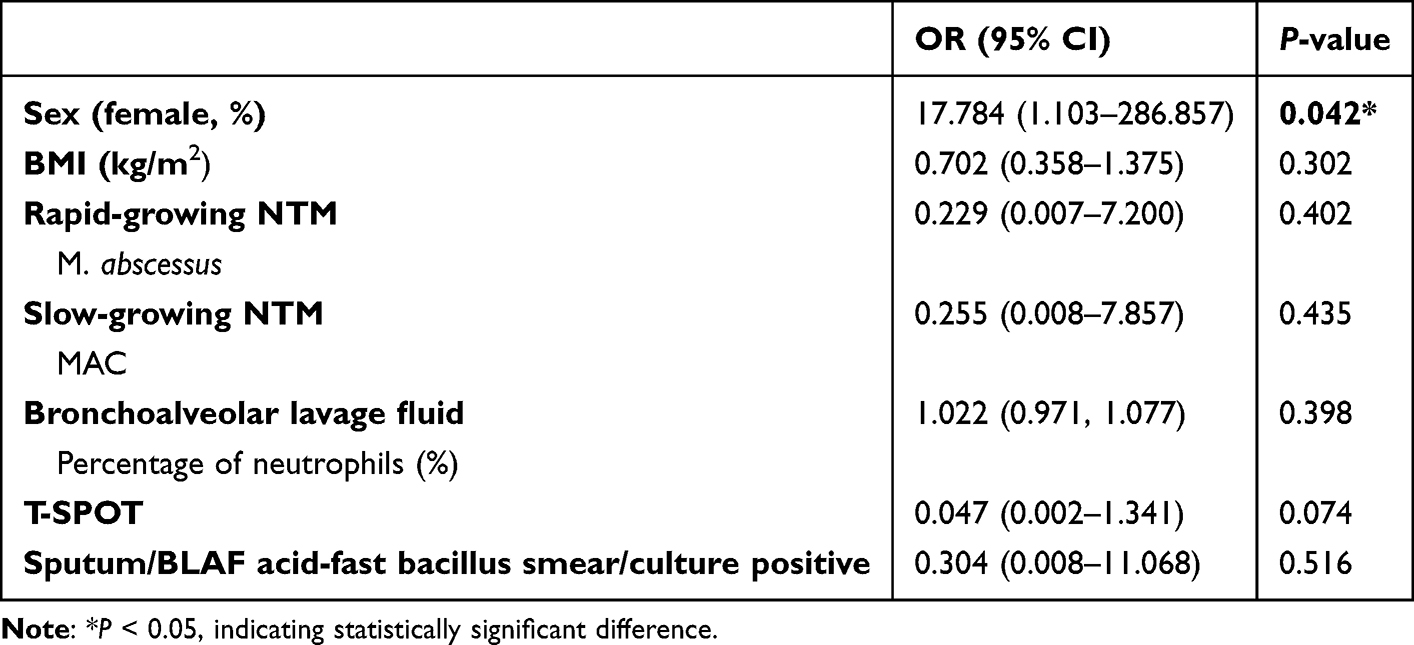 |
Table 3 Multivariate Analysis of NTM-PD with Bronchiectasis Patients |
Clinical Characteristics of Patients with SGM Complicated with Bronchiectasis
There were 17 patients with SGM (mainly MAC) complicated with bronchiectasis (Table 4). Among them, 14 were females and 3 were males, with an age range of 53–87 years. Most patients had a BMI below the normal range. Two patients were T-SPOT.TB positive, 7 had positive sputum/BALF culture and 8 had positive sputum/BALF smear. Lung lesions were mostly distributed in both lungs, and some patients were lost to follow-up during the 36-months follow-up period. No recurrence of the disease was observed in the patients during the follow-up.
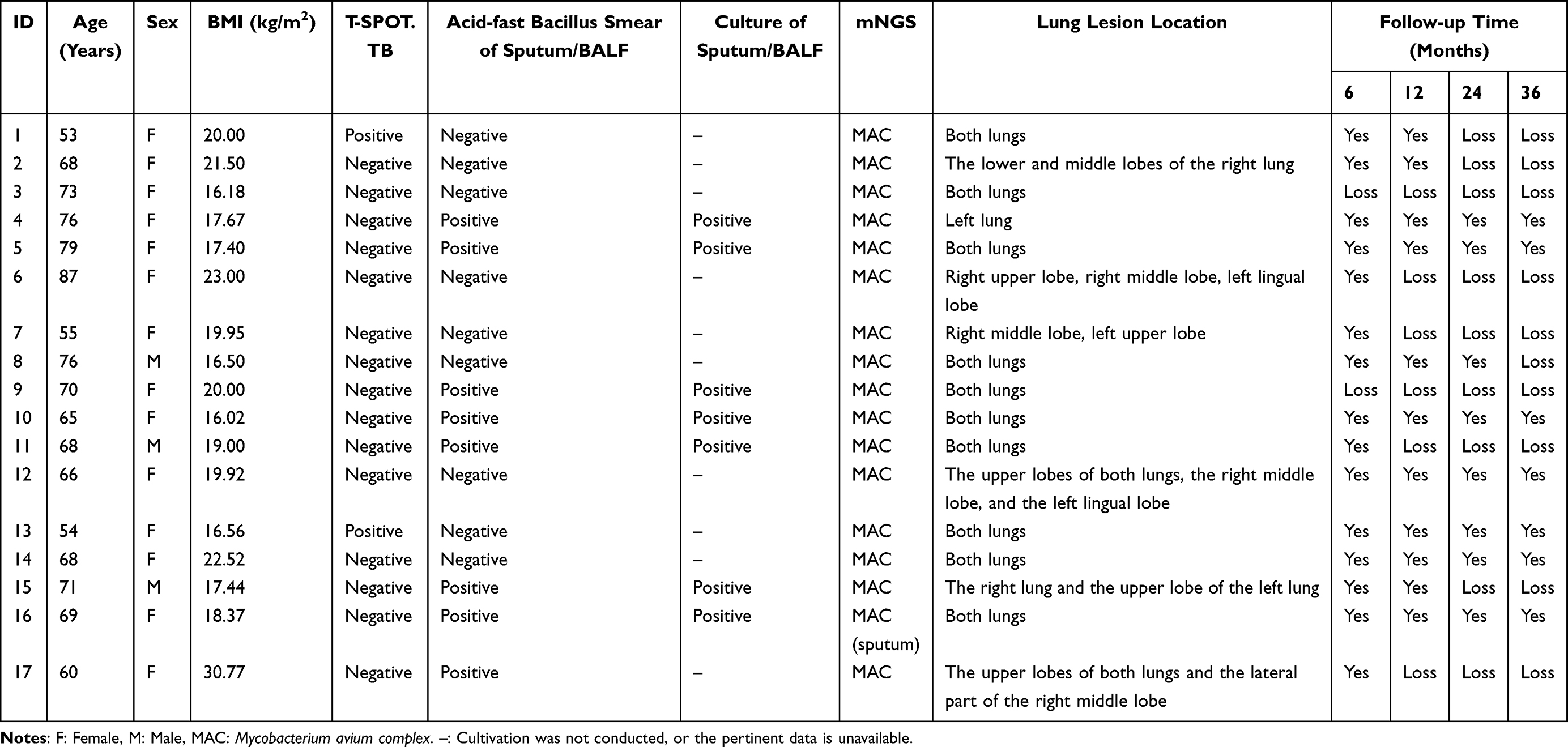 |
Table 4 Clinical Characteristics of Patients with Slow-Growing Mycobacteria Complicated with Bronchiectasis |
Discussion
The global burden of NTM-PD has risen sharply over three decades, with bronchiectasis as its most common comorbidity.4 This bidirectional relationship-bronchiectasis impairs mucociliary clearance to facilitate NTM colonization; NTM infection exacerbates airway damage to perpetuate bronchiectasis-creates a therapeutic dilemma unaddressed by current guidelines.17 The retrospective cohort study of 43 patients with NTM-PD analyzed species distribution, identified sex-based differences in susceptibility, and evaluated the role of T-SPOT.TB in differential diagnosis. The resulting findings offer targeted insights to inform clinical screening, etiological diagnosis, and risk stratification for NTM-PD patients with concurrent bronchiectasis.
Multivariate analysis identified female sex as an independent risk factor for NTM-PD with bronchiectasis (OR=17.784, 95% CI: 1.103–286.857, P=0.042), consistent with population-based studies reporting female predominance in NTM-PD, especially postmenopausal women.18–20 This disparity may reflect two linked mechanisms: hormonal modulation of airway physiology and anatomical differences. Estrogen maintains bronchial epithelial integrity and mucociliary clearance; postmenopausal deficiency disrupts ENaC and CFTR expression, reducing airway surface liquid and slowing ciliary beat frequency,21,22 creating a stagnant microenvironment favorable for NTM biofilm formation. Additionally, women have narrower airways relative to lung volume, increasing airflow resistance and mucus stasis even in health.23 Combined with estrogen-driven epithelial dysfunction, this trait amplifies bronchiectasis risk after NTM infection.
Notably, the NTM-PD with bronchiectasis group had a lower BMI [19.46 (17.50, 21.38) kg/m2] than the NTM-PD group [22.46 (18.63, 24.95) kg/m2] (P=0.023), though BMI was not an independent risk factor (P=0.302). Previous studies reported an inverse correlation between BMI and NTM infection risk;24,25 underweight individuals and those with weight loss during follow-up face higher risk. Proposed mechanisms include altered adipokine levels (eg, leptin, resistin) in low-BMI individuals;26 mouse models show fat tissue removal exacerbates mycobacterial lung pathology27 and leptin-deficient mice have higher MTB loads.28 However, the precise role of adipokines in human NTM host defense remains unclear.26
No intergroup differences were observed in lung function (FEV1, DLCO) or radiological severity. This may reflect NTM’s indolent nature, which causes slow progression on pre-existing bronchiectatic airways rather than acute destruction-contrasting with tuberculosis, which drives rapid cavity formation. Furthermore, the cross-sectional design may have captured a disease plateau phase, and standardized management may have masked intergroup differences. Thus, NTM impact may be more evident in symptom burden and exacerbation frequency than single time-point lung function measurements.
A key finding was divergent species distribution: 70.83% of NTM-PD with bronchiectasis patients had SGM (predominantly MAC), versus 31.58% in the NTM-PD group (P=0.010). Conversely, RGM (mainly M. abscessus) accounted for 57.89% of infections in non-bronchiectatic patients versus 20.83% in the bronchiectatic group (P=0.013). This tropism has critical implications for pathogenesis and treatment. MAC adapts to hypoxic, nutrient-poor bronchiectatic airways by forming biofilms (to evade antibiotics/immunity)29–31 and producing siderophores to scavenge iron from airway secretions.32,33 In contrast, M. abscessus invades intact airway epithelium via CFTR receptors, enabling intracellular replication34-a phenotype distinct from MAC’s colonization of damaged airways,35 explaining its higher prevalence in non-bronchiectatic patients and association with acute presentations.36
Univariate analysis showed a higher T-SPOT.TB positive rate in the NTM-PD group (47.37%) than the bronchiectasis group (8.33%, P=0.010), though T-SPOT.TB was not an independent risk factor (OR=0.047, 95% CI: 0.002–1.341, P=0.074). This discrepancy highlights that T-SPOT.TB results must be interpreted alongside NTM species and structural lung disease, not as a standalone indicator. The assay detects IFN-γ release by memory T cells stimulated with MTB-specific antigens (ESAT-6, CFP-10);37 these antigens are absent in MAC (the dominant species in the bronchiectasis group) but present in some NTM.38 Thus, T-SPOT.TB reactivity differences likely reflect NTM species immunogenicity and bronchiectasis-related immune microenvironment changes, rather than MTB co-infection.
This study has limitations: its retrospective, single-center design with small sample size (n=43) may introduce selection bias and limit generalizability. Standardized mycobacterial load measurements were inconsistently available, precluding analysis of bacterial burden-clinical severity relationships. The 36-month follow-up period was insufficient to evaluate long-term outcomes, such as disease progression and mortality. Furthermore, data completeness may have been affected by loss to follow-up, which primarily resulted from patients transferring care to local hospitals, death from non-respiratory causes, and attrition among those who were clinically stable Future multi-center, prospective studies with larger samples, longer follow-up, and protocol-driven microbiological assessments are needed to validate these findings.
Conclusion
Our study demonstrates that female sex is an independent risk factor for NTM-PD complicated with bronchiectasis, with SGM (predominantly MAC) being the dominant pathogen in this subgroup. While T-SPOT.TB positivity differs between groups in univariate analysis, it is not an independent risk factor, likely due to species-specific immune modulation. Our findings provide targeted clinical insights for the screening, etiological diagnosis, and risk stratification of NTM-PD patients with bronchiectasis.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the two corresponding authors on reasonable request.
Ethics Approval and Informed Consent
This study was performed in line with the principles of the Declaration of Helsinki. The study was approval by the Ethics Committee of the Beijing Tsinghua Changgung Hospital (No. 22447-6-01). Data confidentiality and participant anonymity were strictly maintained throughout the study.
Consent for Publication
This manuscript does not contain any individual person’s data in any form (including individual details, images, or videos) that would require consent for publication. As this was a retrospective study, the requirement for informed consent was waived by the ethics committee. All patient data were de-identified and processed confidentially to ensure privacy protection.
Acknowledgments
We sincerely thank Dinfectome Inc., Nanjing, China, for providing the help in mNGS sequencing and results interpretation.
Funding
This work was supported by the Beijing Clinical Key Specialty Project (XKB2022B1002) and Beijing Hospitals Authority Clinical Medicine Development of Special Funding Support (ZLRK202323).
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Ingen J, Obradovic M, Hassan M, et al. Nontuberculous mycobacterial lung disease caused by Mycobacterium avium complex - disease burden, unmet needs, and advances in treatment developments. Expert Rev Respir Med. 2021;15(11):1387–12.
2. Cowman S, van Ingen J, Griffith DE, Loebinger MR. Non-tuberculous mycobacterial pulmonary disease. Eur Respir J. 2019;54(1):1900250.
3. Zweijpfenning SMH, van Ingen J, Hoefsloot W. Geographic distribution of nontuberculous mycobacteria isolated from clinical specimens: a systematic review. Semin Respir Crit Care Med. 2018;39(3):336–342. doi:10.1055/s-0038-1660864
4. Loebinger MR, Quint JK, van der Laan R, et al. Risk factors for nontuberculous mycobacterial pulmonary disease: a systematic literature review and meta-analysis. Chest. 2023;164(5):1115–1124. doi:10.1016/j.chest.2023.06.014
5. Chalmers JD, Aliberti S, Blasi F. Management of bronchiectasis in adults. Eur Respir J. 2015;45(5):1446–1462. doi:10.1183/09031936.00119114
6. Aliberti S, Goeminne PC, O’Donnell AE, et al. Criteria and definitions for the radiological and clinical diagnosis of bronchiectasis in adults for use in clinical trials: international consensus recommendations. Lancet Respir Med. 2022;10(3):298–306.
7. Fujita M. Pulmonary nontuberculous mycobacteria infection in bronchiectasis: a narrative review of current status and future. Health Sci Rep. 2025;8(4):e70749. doi:10.1002/hsr2.70749
8. O’Donnell AE. Bronchiectasis - A Clinical Review. N Engl J Med. 2022;387(6):533–545. doi:10.1056/NEJMra2202819
9. Mirsaeidi M, Hadid W, Ericsoussi B, Rodgers D, Sadikot RT. Non-tuberculous mycobacterial disease is common in patients with non-cystic fibrosis bronchiectasis. Int J Infect Dis. 2013;17(11):e1000–1004. doi:10.1016/j.ijid.2013.03.018
10. Chinese Medical Association Tuberculosis Branch, Chinese Medical Association Respiratory Branch. Expert consensus on diagnosis and treatment of comorbid nontuberculous mycobacterial pulmonary disease and bronchiectasis. Chin J Tubercul Respirat Dis. 2025;48(2):101–115.
11. Zhou Y, Mu W, Zhang J, Wen SW, Pakhale S. Global prevalence of non-tuberculous mycobacteria in adults with non-cystic fibrosis bronchiectasis 2006–2021: a systematic review and meta-analysis. BMJ Open. 2022;12(8):e055672. doi:10.1136/bmjopen-2021-055672
12. Henkle E, Novosad SA, Shafer S, et al. Long-term outcomes in a population-based cohort with respiratory nontuberculous mycobacteria isolation. Ann Am Thorac Soc. 2017;14(7):1120–1128. doi:10.1513/AnnalsATS.201610-801OC
13. Chinese Medical Association Tuberculosis Branch. Guidelines for the diagnosis and treatment of nontuberculous mycobacteriosis (2020 edition). Chin J Tubercul Respirat Dis. 2020;43(11):918–946.
14. Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J. 2020;56(1):2000535. doi:10.1183/13993003.00535-2020
15. Lv H, Liao S, Shi Z, et al. Application of metagenomic next-generation sequencing for rapid molecular identification in spinal infection diagnosis. Front Cell Infect Microbiol. 2024;14:1382635.
16. Xu J, Zhou P, Liu J, et al. Utilizing Metagenomic Next-Generation Sequencing (mNGS) for rapid pathogen identification and to inform clinical decision-making: results from a large real-world cohort. Infect Dis Ther. 2023;12(4):1175–1187.
17. McShane PJ. Investigation and management of bronchiectasis in nontuberculous mycobacterial pulmonary disease. Clin Chest Med. 2023;44(4):731–742. doi:10.1016/j.ccm.2023.07.005
18. Lim SY, Lee YJ, Park JS, et al. Association of low fat mass with nontuberculous mycobacterial infection in patients with bronchiectasis. Medicine. 2021;100(14):e25193. doi:10.1097/MD.0000000000025193
19. Xu J-F, Zheng H-Z, Lu H-W, et al. Baseline characteristics of patients in the Chinese Bronchiectasis Registry (BE-China): a multicentre prospective cohort study. Lancet Respir Med. 2025;13(2):166–176. doi:10.1016/S2213-2600(24)00364-3
20. Yang B, Ryu J, Kim T, et al. Impact of bronchiectasis on incident nontuberculous mycobacterial pulmonary disease: a 10-year national cohort study. Chest. 2021;159(5):1807–1811. doi:10.1016/j.chest.2020.12.020
21. Han XY, Tarrand JJ, Infante R, Jacobson KL, Truong M. Clinical significance and epidemiologic analyses of Mycobacterium avium and Mycobacterium intracellulare among patients without AIDS. J Clin Microbiol. 2005;43(9):4407–4412. doi:10.1128/JCM.43.9.4407-4412.2005
22. Saint-Criq V, Rapetti-Mauss R, Yusef YR, Harvey BJ. Estrogen regulation of epithelial ion transport: implications in health and disease. Steroids. 2012;77(10):918–923. doi:10.1016/j.steroids.2012.02.017
23. Mann LM, Angus SA, Doherty CJ, Dominelli PB. Evaluation of sex-based differences in airway size and the physiological implications. Eur J Appl Physiol. 2021;121(11):2957–2966. doi:10.1007/s00421-021-04778-2
24. Blakney RA, Ricotta EE, Frankland TB, et al. Incidence of nontuberculous mycobacterial pulmonary infection, by ethnic group, Hawaii, USA, 2005–2019. Emerg Infect Dis. 2022;28(8):1543–1550. doi:10.3201/eid2808.212375
25. Song JH, Kim BS, Kwak N, Han K, Yim -J-J. Impact of body mass index on development of nontuberculous mycobacterial pulmonary disease. Eur Respir J. 2021;57(2):2000454.
26. Chan ED, Iseman MD. Underlying host risk factors for nontuberculous mycobacterial lung disease. Semin Respir Crit Care Med. 2013;34(1):110–123. doi:10.1055/s-0033-1333573
27. Ayyappan JP, Ganapathi U, Lizardo K, et al. Adipose tissue regulates pulmonary pathology during TB infection. mBio. 2019;10(2):e02771–18. doi:10.1128/mBio.02771-18
28. Wieland CW, Florquin S, Chan ED, et al. Pulmonary Mycobacterium tuberculosis infection in leptin-deficient ob/ob mice. Int Immunol. 2005;17(11):1399–1408. doi:10.1093/intimm/dxh317
29. De Beer D, Srinivasan R, Stewart PS. Direct measurement of chlorine penetration into biofilms during disinfection. Appl Environ Microbiol. 1994;60(12):4339–4344. doi:10.1128/aem.60.12.4339-4344.1994
30. Ojha A, Anand M, Bhatt A, Kremer L, Jacobs WR, Hatfull GF. GroEL1: a dedicated chaperone involved in mycolic acid biosynthesis during biofilm formation in mycobacteria. Cell. 2005;123(5):861–873. doi:10.1016/j.cell.2005.09.012
31. Falkinham JO. Mycobacterium avium complex: adherence as a way of life. AIMS Microbiol. 2018;4(3):428–438. doi:10.3934/microbiol.2018.3.428
32. Ratledge C. Iron, mycobacteria and tuberculosis. Tuberculosis. 2004;84(1–2):110–130.
33. De Voss JJ, Rutter K, Schroeder BG, Su H, Zhu Y, Barry CE. The salicylate-derived mycobactin siderophores of Mycobacterium tuberculosis are essential for growth in macrophages. Proc Natl Acad Sci U S A. 2000;97(3):1252–1257.
34. Bernut A, Dupont C, Ogryzko NV, et al. CFTR protects against Mycobacterium abscessus infection by fine-tuning host oxidative defenses. Cell Rep. 2019;26(7):1828–1840.e4.
35. Jönsson BE, Gilljam M, Lindblad A, Ridell M, Wold AE, Welinder-Olsson C. Molecular epidemiology of Mycobacterium abscessus, with focus on cystic fibrosis. J Clin Microbiol. 2007;45(5):1497–1504. doi:10.1128/JCM.02592-06
36. Johansen MD, Herrmann J-L, Kremer L. Non-tuberculous mycobacteria and the rise of Mycobacterium abscessus. Nat Rev Microbiol. 2020;18(7):392–407. doi:10.1038/s41579-020-0331-1
37. Richeldi L. An update on the diagnosis of tuberculosis infection. Am J Respir Crit Care Med. 2006;174(7):736–742. doi:10.1164/rccm.200509-1516PP
38. Shao JB, Wang XD, Xia R, Shao Y, Xu CH, Yan H. Value of T-SPOT.TB, TB-Ab and TB-DNA in the differential diagnosis of pulmonary tuberculosis and nontuberculous mycobacterial pulmonary disease. Mod Med Lab J. 2018;33(4):104–106.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Detection of Mycobacterium avium-intracellulare Complex (MAC) by Bronchial Lavage and the Relationship with Titers of Anti-Glycopeptidolipid-Core IgA Antibodies to MAC in Patients with Pulmonary MAC Disease
Shimada D, Sagawa M, Seki M
Infection and Drug Resistance 2023, 16:977-984
Published Date: 17 February 2023