")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Clinical Characteristics and Predictive Factors of Invasive Fungal Disease in Pediatric Oncology Patients with Febrile Neutropenia in a Country with Limited Resources
Authors Monsereenusorn C , Sricharoen T, Rujkijyanont P , Suwanpakdee D, Photia A , Lertvivatpong N, Traivaree C
Received 6 January 2021
Accepted for publication 27 March 2021
Published 12 July 2021 Volume 2021:12 Pages 335—345
DOI https://doi.org/10.2147/PHMT.S299965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Roosy Aulakh
Chalinee Monsereenusorn,1 Thitiyaporn Sricharoen,2 Piya Rujkijyanont,1 Detchvijitr Suwanpakdee,3 Apichat Photia,1 Nawachai Lertvivatpong,1 Chanchai Traivaree1
1Division of Hematology/Oncology, Department of Pediatrics, Phramongkutklao Hospital and Phramongkutklao College of Medicine, Bangkok, Thailand; 2Buayai Hospital, Nakhon Ratchasima, Thailand; 3Division of Infectious Disease, Department of Pediatrics, Phramongkutklao Hospital and Phramongkutklao College of Medicine, Bangkok, Thailand
Correspondence: Chalinee Monsereenusorn
Division of Hematology/Oncology, Department of Pediatrics, Phramongkutklao Hospital and Phramongkutklao College of Medicine, 315 Ratchawithi Road, Ratchathewi, Bangkok, 10400, Thailand
Email [email protected]
Background: The most common complication among pediatric oncology patients is febrile neutropenia (FN). Invasive fungal disease (IFD) is suspected when fever persists > 4– 7 days after empirical antibiotics. Its clinical characteristics and predictive factors associated with IFD among pediatric oncology patients with FN were thus explored.
Methods: Pediatric oncology patients with FN between January 1, 2012 and December 31, 2016 were enrolled in this study. Clinical characteristics, including laboratory investigations, treatment modalities, and final outcomes of IFD were retrospectively reviewed and analyzed.
Results: In all, 73 patients with 180 episodes of confirmed diagnosis of FN were studied. Median age at diagnosis was 6.2 years, with equal sex distribution. The most common diagnosis was acute lymphoblastic leukemia (n=91, 51%), followed by acute myeloid leukemia (n=47, 26%), Burkitt’s lymphoma (n=7, 4%) and neuroblastoma (n=7, 4%). Median absolute neutrophil count at FN diagnosis was 0 (0– 806) cells/mm3. IFD was diagnosed for 25 (14%) episodes. Mortality rates for FN and IFD were 4% and 20%, respectively. Respiratory compromise, oxygen requirement, hypotension, prolonged hospitalization, duration of fever and neutropenia, bacteremia, bacteriuria, funguria, abnormal liver-function results, and prolonged broad-spectrum antibiotic administration were factors associated with IFD (P< 0.05). Prolonged duration between initiation of fever and antifungal administration for nearly 10 days was an independent factor in prediction of IFD occurrence (P= 0.014).
Conclusion: Respiratory compromise, oxygen requirement, hypotension, prolonged hospitalization, duration of fever and neutropenia, bacteremia, bacteriuria, funguria, abnormal liver-function results and prolonged broad-spectrum antibiotic administration were factors associated with IFD. Duration between initiation of fever and antifungal administration of nearly 10 days were considered a risk factors of IFD among patients with FN.
IRB Reference Number: IRBRTA 825/2560.
Keywords: febrile neutropenia, invasive fungal disease, pediatric oncology, risk factors, mortality
Background
The most common complication among pediatric oncology patients is febrile neutropenia (FN). FN is mostly caused by mucocutaneous infection in the gastrointestinal tract, pulmonary system, and skin from bacteria and fungi. Occult bacteremia is found in 20%–30% of patients with FN1 and related to neutropenia of <100 cells/mm3.2 Patients hospitalized for fever and neutropenia are often treated with empirical antibiotics. Investigations and treatment of invasive fungal infection with antifungals is initiated when fever persists >4–7 days or when the patient exhibits illness. A third of these patients are at risk of fungal coinfection, ie, candidiasis or aspergillosis. Clinical symptoms, such as respiratory distress, sinonasal symptoms, and abdominal pain with laboratory such findings as bacteremia or fungemia or funguria,3 may warrant further workup for invasive fungal disease (IFD).
Patients receiving high-intensity chemotherapy regimens are at increased risk of developing IFD. Only 5.8% of patients with FN were ultimately diagnosed with IFD in one high-income country,4 while higher rates up to 23% were found in a country with limited resources.5 Related studies have shown increasing risk of developing IFD correlate with prolonged duration of neutropenia after initiation of fever, treatment of acute myeloid leukemia,6 high-risk (or relapsed) acute lymphoblastic leukemia,7 high-dose steroid exposure,8 prolonged use of empirical antibiotics,9 and pre-existing sites of fungal colonization.10,11 Patients who develop fever during the induction phase of treatment (compared with the maintenance phase) and patients with early fever onset, ie, fever occurring within 5 days of becoming neutropenic appeared to be at higher risk of IFD.12
The mortality rate of FN due to Gram-negative septicemia is 10%–30%,13 while that of Gram positive septicemia is 28%.14 Similarly, the mortality rate of overall IFD is 48.2%.9 Specifically invasive aspergillosis has a mortality rate as high as 30%.15
Most publications had defined IFD using clinical criteria, along with culture or biopsy of involved tissue. However, few of these reports have detailed whether the clinical characteristics, signs and symptoms, laboratory findings, or previous treatment are associated with IFD occurrence.4 Moreover, studies have been conducted in different geographical areas and populations, such as South America4 or adult patients.16 Accordingly, these findings in a pediatric population might be considered as specific guidelines to create greater awareness in center with limited resources, such as in Southeast Asia.
This study primarily aimed to explore clinical characteristics, including investigational and treatment approaches, and associated prognostic factors of IFD, specifically in a pediatric oncology population presenting FN.
Methods
Patient Selection
Medical records of 85 pediatric oncology patients, newly diagnosed and treated for FN primarily at the Division of Hematology and Oncology, Department of Pediatrics, Phramongkutklao Hospital, from January 1, 2012 to December 31, 2016 were retrospectively reviewed.
Inclusion criteria were oncology patients aged 0–21 years whose diagnosis of FN had been confirmed by FN definitions in the 2010 Infectious Disease Society of America clinical practice guidelines.17 Patients with incomplete diagnosis criteria, undergoing hematopoietic stem–cell transplantation (HSCT), or with a previous diagnosis IFD were excluded from the study.
This study was approved by the Institutional Review Board, Royal Thai Army Medical Department according to the ethics principles of the Declaration of Helsinki (1975) and its revisions (IRBRTA 825/2560).
Laboratory Procedure
Galactomannan was detected in serum by direct double-sandwich ELISA, with an index value ≥0.5 considered positive.
Operational Definition of Febrile Neutropenia
Patients had to meet two criteria: fever defined as a single oral temperature measurement >38.3°C (101°F) or >38°C (100.4°F) sustained over 1 hour, and neutropenia defined as an absolute neutrophil count (ANC) <500 cells/mm3 or expected to decline to this level.17
Institutional Definition of Fungal Infections
IFD definition was adapted from the European Organization for Research and Treatment of Cancer (EORTC)–Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (MSG) Consensus Group.18,19
Proven IFD was defined as documented constitutional symptoms with evidence of fungus isolated from normally sterile body fluid or confirmed by histopathology.
Probable IFD was defined as documented constitutional symptoms in appropriate host factors with radiological findings confirmed by a radiologist, ie, computed tomography scan showing dense, well-circumscribed lesions with or without a halo or air-crescent sign, cavities, and evidence of fungus isolated from nonsterile body fluid or laboratory evidence of galactomannan antigen or β-D-glucan detected in serum.
Possible IFD was defined as documented constitutional symptoms in appropriate host factors with no laboratory support in a nonendemic mycosis area.
Mucosal fungal disease was defined as documented symptoms and confirmed histopathology or positive culture of specifically nonsterile mucosa, ie, the skin or esophagus.
Diagnostic Definitions
Respiratory compromise was defined as any symptoms addressing deterioration in respiratory function, ie, use of accessory muscle, and increased or decreased respiratory rate according to age.
Oxygen requirement was defined as abnormal cardiopulmonary conditions causing respiratory compromise that required oxygen therapy to maintain target oxygen saturation >94% in room air.
Hypotension was defined as blood pressure less than the fifth percentile according to age and/or 90/50 mmHg.
Abnormal liver-function test (LFT) results were defined as at least one of increased alanine aminotransferase (ALT), increased aspartate aminotransferase (AST) at least double the upper normal limit, increased total bilirubin concentration, or decreased serum albumin.
Treatment of Febrile Neutropenia
Ceftazidime and amikacin were given to pediatric oncology patients with FN as a first-line empirical antibiotic regimen after blood cultures had been collected. Meropenem would be substituted due to unresponsive treatment. Additionally, vancomycin was considered for patients who were clinically unstable, with possible skin infection or suspected catheter-related infection. Amphotericin B was given as an empirical antifungal if fever had persisted >4–7 days.
Statistical Analysis
Baseline values of demographic data, clinical manifestations, laboratory studies, treatment strategies, and outcomes from all participating patients were analyzed using descriptive statistics and are presented as means ± SD (normal distribution) or medians with range (abnormal distribution) for continuous variables and calculated using frequency and percentage for categorical variables. Categorical and continuous variables were compared using Fisher’s exact and Mann–Whitney U tests, respectively. Univariate and multivariate binary logistic regression analyses were performed to analyze the impact of possible factors on defined outcomes. Five to ten potential risk factors on defined outcomes from observational experience were chosen and analyzed in the univariate analytic model. In addition, all factors that were statistically significant on univariate analysis were also analyzed with multivariate analysis and affirmed interrelationships among several variables. The number of patients was sufficient for an acceptable level of statistical power to perform the multivariate analysis. Statistical analysis was performed using IBM SPSS 23.0, and P<0.05 was considered statistically significant.
Results
Patient Characteristics
Among 85 oncology patients who presented with fever and neutropenia, 12 were excluded due to previously diagnosed confirmation of IFD and inability to confirm clinical criteria of FN. As such, 73 patients with a confirmed diagnosis of FN for a total of 180 FN episodes were subsequently studied, as shown in Figure 1. Patient age, sex, diagnosis, status of disease, and complete blood–count parameters, including initial white blood cell (WBC) count and ANC, at diagnosis of FN are summarized in Table 1.
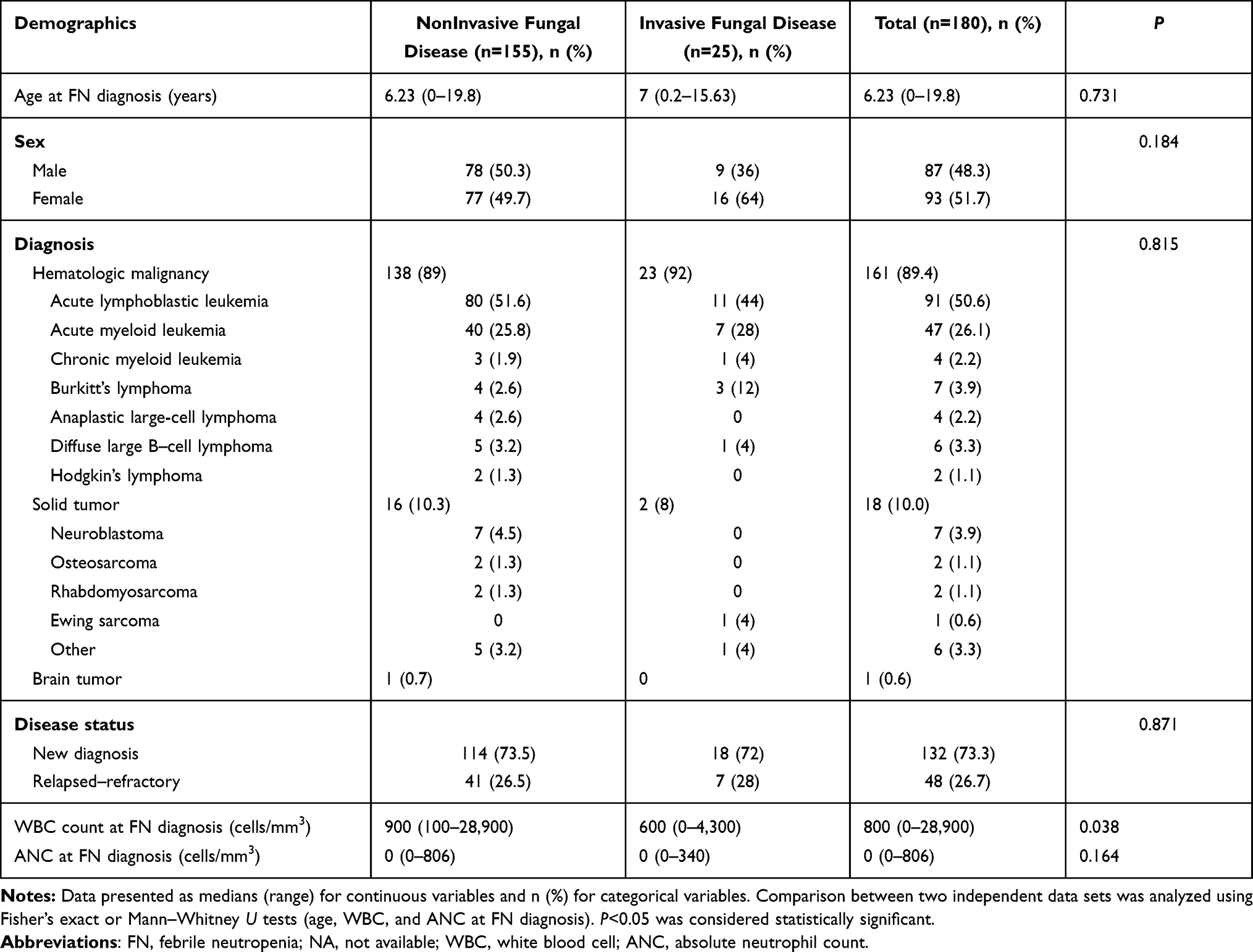 |
Table 1 Characteristics of Febrile Neutropenia Patients (n=180) |
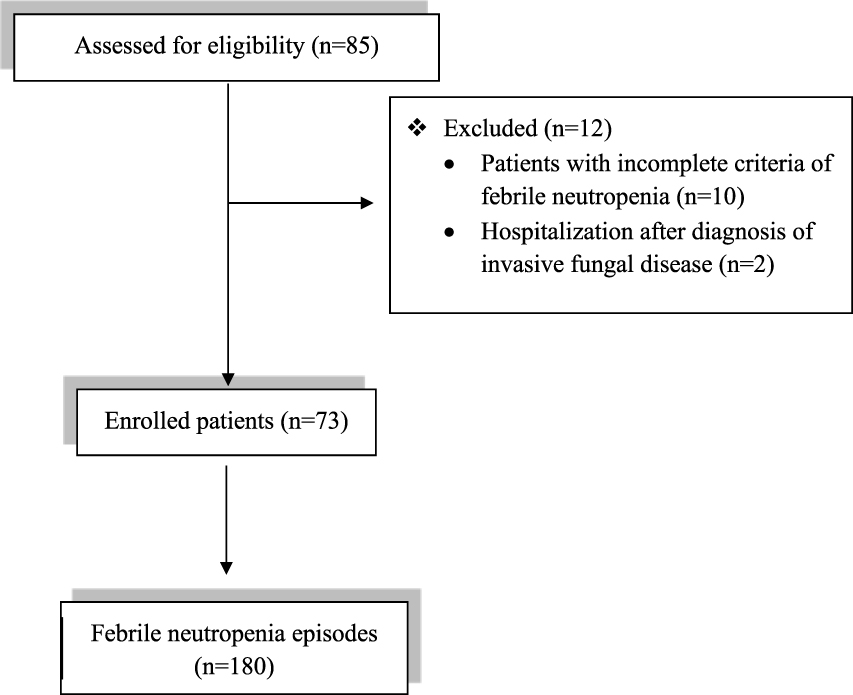 |
Figure 1 Study flowchart. |
Among the 180 FN episodes, IFD was diagnosed in 25 (13.9%). Median duration between initiation of fever until diagnosis of IFD was 10 (0–53) days. Overall median age was approximately 6.23 (range, 0–19.8) years, and the male:female ratio was 1:1. The most common diagnosis was hematologic malignancy, totaling 161 (89.4%) FN episodes. A majority were acute lymphoblastic leukemia, followed by acute myeloid leukemia, Burkitt’s lymphoma, diffuse large B–cell lymphoma, chronic myeloid leukemia, anaplastic large-cell lymphoma and Hodgkin’s lymphoma. Solid tumors for 18 (10%) episodes involved neuroblastoma followed by osteosarcoma, rhabdomyosarcoma, and Ewing’s sarcoma.
Disease status was divided into newly diagnosed (132, 73.3%) and relapsed or refractory disease 48 (26.7%).
Median WBC count and ANC at diagnosis of FN were 800 cells/mm3 and 0 cells/mm3, respectively.
Only median initial WBC count at FN diagnosis in patients with IFD (600, range 0–4,300 cells/mm3) was significantly lower than those without (900, range 100–28,900 cells/mm3; P=0.038). Age, sex, diagnosis, disease status, and ANC at FN diagnosis between the non-IFD and IFD groups did not significantly differ.
Pathogens Causing Febrile Neutropenia
Among the 180 FN episodes, pathogens causing FN were identified by histopathology, microbiology, or meeting institutional definition of fungal infections in 71 (39.4%) episodes. The most common organisms were bacteria (39, 54.9%), followed by fungus (31, 43.7%) and virus (one, 1.4%; Supplementary Table 1).
IFD was identified in 25 (13.9%) of the FN episodes, (Supplementary Table 2). Proven IFD totaled seven (28%) episodes, candidemia four (57.1%), invasive aspergillosis two (28.6%), and combined candidemia and cryptococcal skin infection one (14.3%). Probable and possible IFD were identified for 14 (56%) and four (16%) episodes, respectively. For IFD, six (24%) episodes showed IFD concomitant with bacteremia and eleven (44%) with bacterial infection.
Treatment Outcomes
Over 96% (173 episodes) of patients with FN survived, as shown in Figure 2. Seven (4%) patients died. Five (71.4%) had IFD concomitant with bacterial septicemia and/or hemodynamic instability (septic or spinal shock) causing multiorgan failure. One (14.3%) patient had Neisseria meningitidis encephalitis, and one (14.3%) an unidentified pathogen.
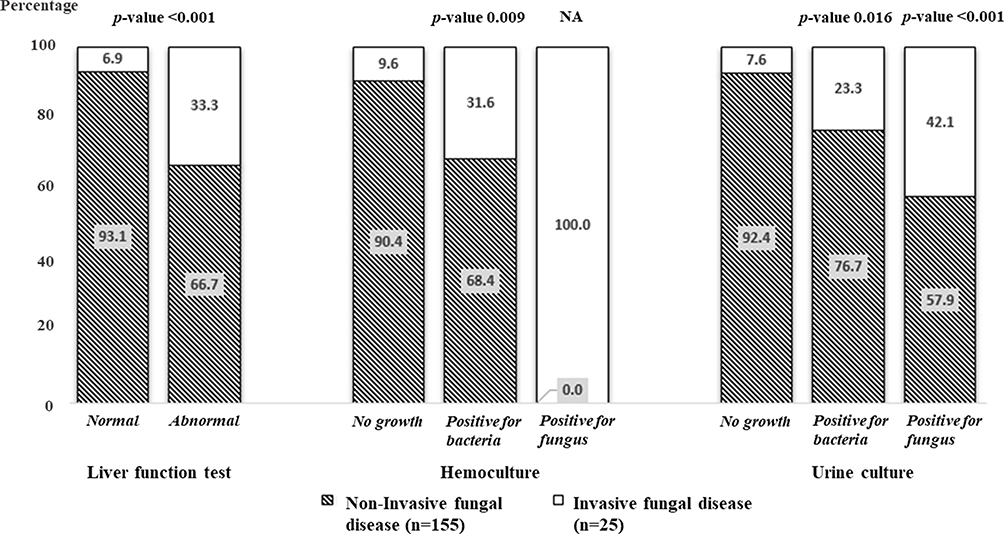 |
Figure 2 Outcomes of patients with febrile neutropenia associated with invasive fungal disease (n=180). Notes: Data are presented as n (%) for categorical variables. Univariate analysis was calculated using logistic regression. P<0.05 was considered statistically significant. |
The overall mortality rate among patients with FN was 4%. Patients with IFD had significantly higher mortality (20%, five of 25) than non-IFD (1.3%, two of 155); (OR 19.125, 95% CI 3.477–105.189; P=0.001).
Clinical and Laboratory Factors Associated with IFD
Signs and symptoms, including compromised respiratory symptoms requiring oxygen therapy, hypotension, prolonged hospitalization and duration of fever, neutropenia, and broad-spectrum antibiotics were influential factors associated with IFD on univariate analysis (P<0.05).Multivariate analysis was subsequently performed, and none was an independent risk factors of IFD (Table 2).
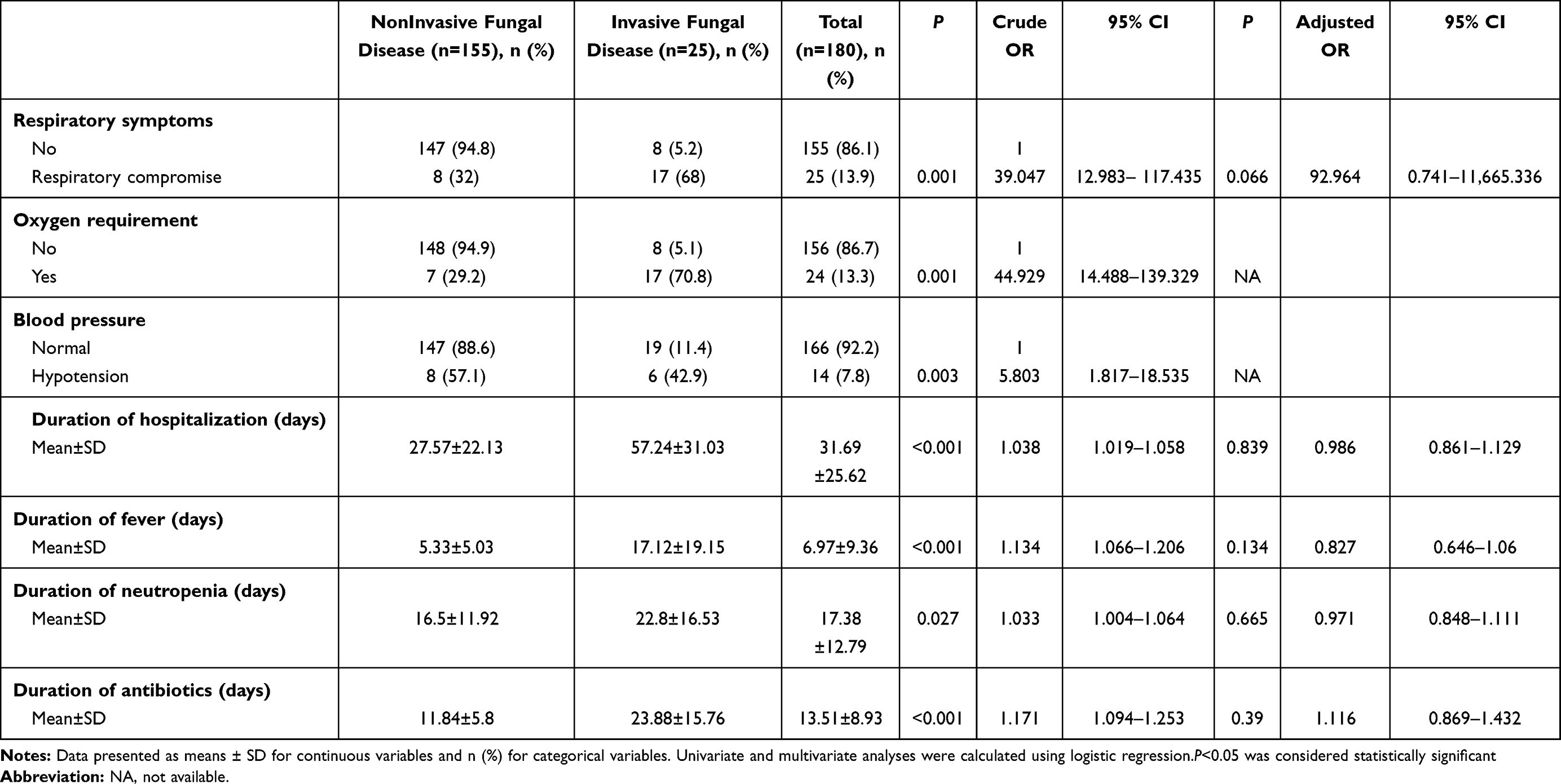 |
Table 2 Clinical Factors Affecting Clinical Outcomes of Invasive Fungal Disease in Febrile Neutropenia Patients (n=180) |
Abnormal LFT results, bacteremia, bacteriuria, and funguria were statistically significantly associated with occurrence of IFD on univariate analysis (P<0.05, Figure 3), but were not independent risk factors of IFD on multivariate analysis.
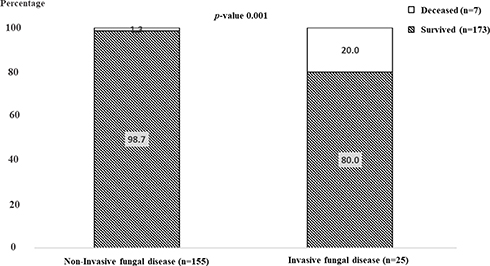 |
Figure 3 Laboratory factors affecting clinical outcomes of invasive fungal disease in febrile neutropenia patients (n=180). Abbreviation: NA, not available. Notes: Data are presented as n (%) for categorical variables. Univariate analysis was calculated using logistic regression. P<0.05 was considered statistically significant. |
Antibiotics Associated with IFD
All patients received antibiotics for FN treatment. Meropenem and vancomycin were associated with the occurrence of IFD. Patients receiving meropenem were associated with IFD (OR 5.338, 95% CI 2.201–12.947; P<0.001). Similarly, vancomycin was also associated with IFD (OR 9.297, 95% CI 3.568–24.225; P<0.001) as shown in Supplementary Table 3.
Influential Factors Associated with Clinical Outcomes among Patients Receiving Antifungal Treatment
Among 61 (34%) FN cases receiving antifungal treatment, 36 (59%) episodes were non-IFD and 25 (41%) IFD. WBC count and ANC at diagnosis of FN, fever, and neutropenia duration were not significant predictive factors of IFD. Occurrence of IFD among patients with FN presenting abnormal LFT results was significantly higher on univariate analysis(OR 3.556, 95% CI 1.218–10.376; P=0.02). Moreover, longer duration between initiation of fever and antifungal administration was a risk factor associated with IFD. Multivariate analysis was subsequently performed, and affirmed that longer duration (nearly 10 days) between onset of fever and antifungal administration remained an independent risk factor of IFD (adjusted OR 1.201, 95% CI 1.038–1.389; P=0.014), as shown in Table 3.
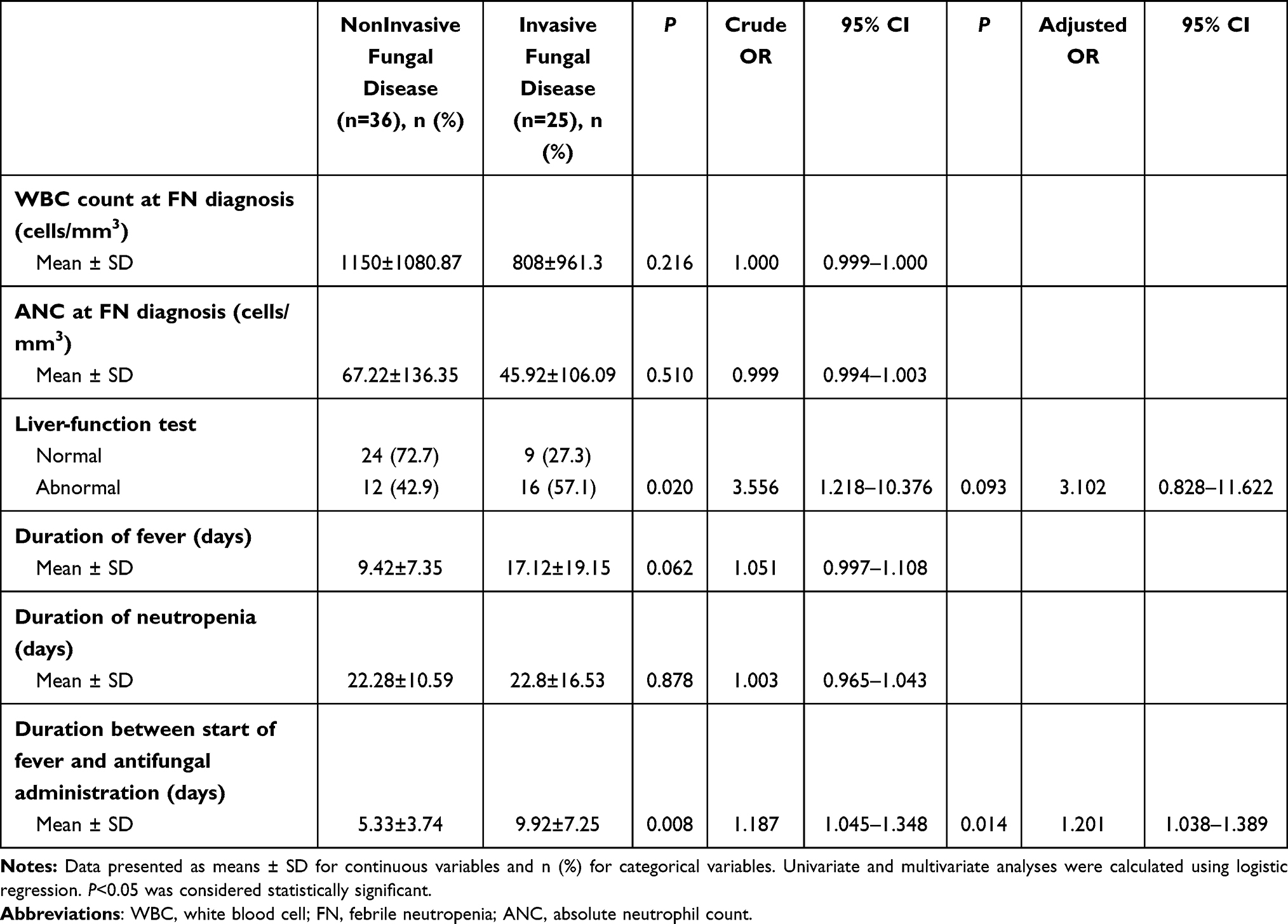 |
Table 3 Clinical and Laboratory Factors Associated with Clinical Outcomes of Invasive Fungal Disease in Febrile Neutropenia Patients Who Received Antifungal Treatment (n=61) |
Discussion
The most common serious complication following pediatric hematology/oncology treatment is FN. It causes high fatality, unnecessarily consumed resources, and prolonged hospitalization. Mortality from FN was higher in low- and middle-income countries — 4% in our study and 5.5% in India20 — than high-income countries, eg, 0.6% in the US.21
Pathogens related to FN are bacteria causing bacteremia and fungal infections. IFD is the crucial cause of morbidity and mortality.22 However, FN is sometimes remains unidentified or labeled “fever of unknown origin”.
The epidemiology of FN-causative organisms depends on the country. Fever of unknown origin in countries with limited resources, as in our study, has been reported as 60% compared to 45% in a developed country.22 In addition, Gram-positive bacteremia dominates in countries widely using central venous catheters23 compared to countries with limited resources, which have a higher percentage of occult Gram-negative bacteremia.20
Risk factors of FN in literature reviews have included type of cancer, intensity of chemotherapy, associated comorbidities,24 duration of neutropenia, length of hospital stay, and previous bacteremia.25
Nevertheless, fungal infection remained the leading cause of mortality, especially among immunocompromised patients experiencing FN. IFD represents one of the serious complications among patients undergoing immunosuppressive therapy or HSCT. IFD occurred at 13.9% in our study. This is similar to a recent finding in Siriraj Hospital, Bangkok, Thailand,16 but higher than studies in South America 8.8%22 and the US (4.9%).26 This higher incidence was possibly affected by the lower use of antifungal prophylaxis in a center with limited resources.
Clinical presentations associated with IFD include sinusitis and abdominal discomfort.5 However, abdominal pain and pneumonia predominated in our study. Nevertheless, respiratory distress, oxygen requirement, and hypotension have been documented as high risk factors of FN in developing serious morbidity.25,27,28 In our study, these factors were associated with IFD on univariate analysis, but not as independent risk factors on multivariate analysis.
The most common pathogens causing IFD in pediatric oncology populations were Candida and Aspergillus infection,7,24 which was likewise found in our study.
The definition of IFD is divided into proven, probable, and possible, as described by the EORTC/MSG Consensus Group.18,19 In countries with limited resources, most IFD cases are classified as probable or possible, rather than proven.6,9 In our study, probable IFD totaled 56%, possible IFD 16%, and proven IFD 28%. The low IFD figure might be due to inaccessibility of tissue biopsies and unidentified fungal cultures in a country with limited resources, such as Thailand.
Risk factors associated with IFD in pediatric oncology previously reported include age, cancer type, duration of fever,4 prolonged neutropenia,8 ANC <500 cells/mm3, and prolonged using of broad-spectrum antimicrobial agents.9,28 These are usually reported among patients with mostly hematologic malignancies in most studies.5,9 In addition, most previous studies on pediatric oncology populations have included nonfever or nonneutropenic cases.26 In our study, cancer types were not associated with IFD. However, our study is one of the few to report both hematologic (90%) and solid malignancies (10%) among children with fever and neutropenia. This variation affected the results differently. In our study, ANC at diagnosis of FN was not associated with IFD. This was because average ANC was 0 cells/mm3 in our study population, regardless of IFD occurrence. ANC in our report was much <500 cells/mm3 which has been documented as an IFD risk in most published data.
We identified bacteremia concomitant with IFD in 24% of patients with IFD. This was possibly because most patients with IFD received multiple and prolonged administration of broad-spectrum antibiotics, such as meropenem and vancomycin, for prolonged fever and neutropenia.29 Antifungal therapy is considered for patients presenting persistent or recurrent fever after 4–7 days of receiving broad-spectrum antibiotics according to Infectious Disease Society of America clinical practice guidelines.17 Therefore, this group of patients is more susceptible to developing multidrug-resistant bacteremia,30 which often leads to the development of systemic coinfection such as bacterial septicemia, urinary tract infection, or enteritis.
Interestingly, abnormal LFT results associated with IFD were found in this study, though not an independent risk factor. Abnormal LFT results might represent an early sign of organ compromise or septicemia, which are risks factors of developing IFD.
In summary, the abnormal LFT results, bacteremia,3,29,31 bacteriuria, and funguria found in our study were associated with IFD.
On multivariate analysis, patients with IFD had significantly longer duration, nearly 10 days, between initiation of fever and antifungal administration than patients without IFD. This presumably prolonged waiting period for antifungal administration was associated with developing IFD. Earlier administration of antifungal treatment could be a potential factor in suppressing IFD manifestation in patients with FN. As such, this finding was not truly an independent predictive factor of IFD. However, if patients experience symptoms suspected to be IFD and fever >4–7 days after empirical antibiotics, antifungal treatment should be considered promptly and not postponed >10 days.
The mortality rate of IFD was 20% in our study, similar to 25% in Taiwan15 and 14%–29% in US studies,26,32 whereas antifungal prophylaxis was widely used. The causes of death are associated with concomitant bacterial septicemia causing multiorgan failure.
To our knowledge, this study is the first to identify predictive factors of IFD in a Southeast Asian pediatric oncology population with FN.
Limitations
This was a retrospective study on IFD that was mostly “probable” or “possible” by definition, and thus does not represent a study of an entire group of IFD cases that should otherwise be diagnosed by proven IFD. Moreover, all patients with IFD in our study were in fever and neutropenic settings. We excluded patients with IFD undergoing HSCT and presenting nonfever and nonneutropenic IFD,7 which would have represented an entire population of patients with IFD.
Conclusion
This study affirmed that IFD was the main factor contributing to the high mortality rate among pediatric hematology/oncology patients with FN. IFD definitions often meet “probable” or “possible” rather than “proven” cases in countries with limited resources. Addressing the factors associated with IFD is warranted in order to decrease disease mortality and complications. Respiratory compromise, oxygen requirement, hypotension, prolonged hospitalization, duration of fever and neutropenia, bacteremia, bacteriuria, funguria, abnormal LFT results, and broad-spectrum antibiotic administration were factors associated with IFD. ANC was not associated with IFD when <100 cells/mm3. In addition, duration between initiation of fever and antifungal administration of nearly 10 days was a potential influential factor to predict occurrence of IFD, though, earlier administration of antifungal treatment would be a confounding factor suppressing IFD manifestation among pediatric oncology patients with FN.
Abbreviations
ALT, alanine aminotransferase; ANC, absolute neutrophil count; AST, aspartate aminotransferase; EORTC–MSG, European Organization for Research and Treatment of Cancer–Invasive Fungal Infections Cooperative Group–National Institute of Allergy and Infectious Diseases Mycoses Study Group; FN, febrile neutropenia; HSCT, hematopoietic stem–-cell transplantation; IFD, invasive fungal disease; LFT, liver-function test; WBC, white blood cell.
Data Sharing Statement
The data sets generated and/or analyzed during the current study are not publicly available, since they are being used in another ongoing study; however, data are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate and for Publication
Written informed consent and assent forms were waived due to the anonymous, retrospective nature of this study. This study was approved by the Institutional Review Board, Royal Thai Army Medical Department (IRBRTA 825/2560) in accordance with the ethical principles of the Declaration of Helsinki (1975), including revisions.
Acknowledgments
The authors gratefully acknowledge Mrs Supak Cae-Ngow, Office of Research and Development, Phramongkutklao Hospital and Phramongkutklao College of Medicine for statistical analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval toof the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
Funding from the Phramongkutklao College of Medicine, Royal Thai Army was used to conduct the study, analyze and interpret the study results, and submit the study for publication.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Misch EA, Andes DR. Bacterial infections in the stem cell transplant recipient and hematologic malignancy patient. Infect Dis Clin North Am. 2019;33(2):399–445. doi:10.1016/j.idc.2019.02.011
2. Kara SS, Tezer H, Polat M, et al. Risk factors for bacteremia in children with febrile neutropenia. Turk J Med Sci. 2019;49(4):1198–1205. doi:10.3906/sag-1901-90
3. Sano H, Kobayashi R, Suzuki D, Kishimoto K, Yasuda K, Kobayashi K. Bacteremia during neutropenia is a predictive factor for invasive fungal infection in children. Pediatr Int. 2013;55(2):145–150. doi:10.1111/ped.12031
4. Villarroel M, Aviles CL, Silva P, et al. Risk factors associated with invasive fungal disease in children with cancer and febrile neutropenia: a prospective multicenter evaluation. Pediatr Infect Dis J. 2010;29(9):816–821. doi:10.1097/INF.0b013e3181e7db7f
5. Kumar J, Singh A, Seth R, Xess I, Jana M, Kabra SK. Prevalence and predictors of invasive fungal infections in children with persistent febrile neutropenia treated for acute leukemia - a Prospective Study. Indian J Pediatr. 2018;85(12):1090–1095. doi:10.1007/s12098-018-2722-0
6. Nganthavee V, Phutthasakda W, Atipas K, et al. High incidence of invasive fungal infection during acute myeloid leukemia treatment in a resource-limited country: clinical risk factors and treatment outcomes. Support Care Cancer. 2019;27(9):3613–3622. doi:10.1007/s00520-019-04720-5
7. King J, Pana ZD, Lehrnbecher T, Steinbach WJ, Warris A. Recognition and clinical presentation of invasive fungal disease in neonates and children. J Pediatric Infect Dis Soc. 2017;6(suppl_1):S12–S21. doi:10.1093/jpids/pix053
8. Fisher BT, Robinson PD, Lehrnbecher T, et al. Risk factors for invasive fungal disease in pediatric cancer and hematopoietic stem cell transplantation: a Systematic Review. J Pediatric Infect Dis Soc. 2018;7(3):191–198. doi:10.1093/jpids/pix030
9. Kobayashi R, Kaneda M, Sato T, Ichikawa M, Suzuki D, Ariga T. The clinical feature of invasive fungal infection in pediatric patients with hematologic and malignant diseases: a 10-year analysis at a single institution at Japan. J Pediatr Hematol Oncol. 2008;30(12):886–890. doi:10.1097/MPH.0b013e3181864a80
10. Pizzo PA, Robichaud KJ, Wesley R, Commers JR. Fever in the pediatric and young adult patient with cancer. A prospective study of 1001 episodes. Medicine (Baltimore). 1982;61(3):153–165. doi:10.1097/00005792-198205000-00003
11. Schwartz RS, Mackintosh FR, Schrier SL, Greenberg PL. Multivariate analysis of factors associated with invasive fungal disease during remission induction therapy for acute myelogenous leukemia. Cancer. 1984;53(3):411–419. doi:10.1002/1097-0142(19840201)53:3<411::AID-CNCR2820530308>3.0.CO;2-E
12. Wiley JM, Smith N, Leventhal BG, et al. Invasive fungal disease in pediatric acute leukemia patients with fever and neutropenia during induction chemotherapy: a multivariate analysis of risk factors. J Clin Oncol. 1990;8(2):280–286. doi:10.1200/JCO.1990.8.2.280
13. Kang CI, Kim SH, Park WB, et al. Bloodstream infections caused by antibiotic-resistant gram-negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother. 2005;49(2):760–766. doi:10.1128/AAC.49.2.760-766.2005
14. Alexandraki I, Palacio C. Gram-negative versus Gram-positive bacteremia: what is more alarmin(g)? Crit Care. 2010;14(3):161. doi:10.1186/cc9013
15. Sun KS, Tsai CF, Chen SC, Huang WC. Clinical outcome and prognostic factors associated with invasive pulmonary aspergillosis: an 11-year follow-up report from Taiwan. PLoS One. 2017;12(10):e0186422. doi:10.1371/journal.pone.0186422
16. Phikulsod P, Suwannawiboon B, Chayakulkeeree M. Invasive fungal infection among febrile patients with chemotherapy-induced neutropenia in Thailand. Southeast Asian J Trop Med Public Health. 2017;48(1):159–169.
17. Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin Infect Dis. 2011;52(4):e56–93.
18. De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008;46(12):1813–1821. doi:10.1086/588660
19. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. 2020;71(6):1367–1376. doi:10.1093/cid/ciz1008
20. Noronha V, Joshi A, Patil VM, et al. Pattern of infection, therapy, outcome and risk stratification of patients with febrile neutropenia in a tertiary care oncology hospital in India. Indian J Cancer. 2014;51(4):470–474. doi:10.4103/0019-509X.175306
21. Hakim H, Flynn PM, Knapp KM, Srivastava DK, Gaur AH. Etiology and clinical course of febrile neutropenia in children with cancer. J Pediatr Hematol Oncol. 2009;31(9):623–629. doi:10.1097/MPH.0b013e3181b1edc6
22. Nicolato A, Nouer SA, Garnica M, Portugal R, Maiolino A, Nucci M. Invasive fungal diseases in patients with acute lymphoid leukemia. Leuk Lymphoma. 2016;57(9):2084–2089. doi:10.3109/10428194.2016.1154957
23. Agyeman P, Aebi C, Hirt A, et al. Predicting bacteremia in children with cancer and fever in chemotherapy-induced neutropenia: results of the prospective multicenter SPOG 2003 FN study. Pediatr Infect Dis J. 2011;30(7):e114–119. doi:10.1097/INF.0b013e318215a290
24. Davis K, Wilson S. Febrile neutropenia in paediatric oncology. Paediatr Child Health (Oxford). 2020;30(3):93–97. doi:10.1016/j.paed.2019.12.002
25. Alexander SW, Wade KC, Hibberd PL, Parsons SK. Evaluation of risk prediction criteria for episodes of febrile neutropenia in children with cancer. J Pediatr Hematol Oncol. 2002;24(1):38–42. doi:10.1097/00043426-200201000-00011
26. Rosen GP, Nielsen K, Glenn S, Abelson J, Deville J, Moore TB. Invasive fungal infections in pediatric oncology patients: 11-year experience at a single institution. J Pediatr Hematol Oncol. 2005;27(3):135–140. doi:10.1097/01.mph.0000155861.38641.ca
27. Lehrnbecher T, Robinson P, Fisher B, et al. Guideline for the management of fever and neutropenia in children with cancer and hematopoietic stem-cell transplantation recipients: 2017 update. J Clin Oncol. 2017;35(18):2082–2094. doi:10.1200/JCO.2016.71.7017
28. Lehrnbecher T, Phillips R, Alexander S, et al. Guideline for the management of fever and neutropenia in children with cancer and/or undergoing hematopoietic stem-cell transplantation. J Clin Oncol. 2012;30(35):4427–4438. doi:10.1200/JCO.2012.42.7161
29. Richet HM, Andremont A, Tancrede C, Pico JL, Jarvis WR. Risk factors for candidemia in patients with acute lymphocytic leukemia. Rev Infect Dis. 1991;13(2):211–215. doi:10.1093/clinids/13.2.211
30. Barton CD, Waugh LK, Nielsen MJ, Paulus S. Febrile neutropenia in children treated for malignancy. J Infect. 2015;71(Suppl 1):S27–35. doi:10.1016/j.jinf.2015.04.026
31. Haeusler GM, Thursky KA, Mechinaud F, et al. Predicting infectious complications in children with cancer: an external validation study. Br J Cancer. 2017;117(2):171–178. doi:10.1038/bjc.2017.154
32. Pana ZD, Roilides E, Warris A, Groll AH, Zaoutis T. Epidemiology of invasive fungal disease in children. J Pediatric Infect Dis Soc. 2017;6(suppl_1):S3–S11. doi:10.1093/jpids/pix046
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.