")
Back to Journals » Cancer Management and Research » Volume 14
Clinical Characteristics and Image Manifestations of a Rare Retinoblastoma with a Bone Metastasis
Authors Gu H , Wang Y, Huang D, Ji X, Zhang Y, Ma J, Li M, Zhang W , Hu H , Li J, Zhang P
Received 27 January 2022
Accepted for publication 12 April 2022
Published 26 April 2022 Volume 2022:14 Pages 1565—1575
DOI https://doi.org/10.2147/CMAR.S360180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sanjeev K. Srivastava
Huali Gu,1 Yizhuo Wang,1 Dongsheng Huang,1 Xunda Ji,2 Yi Zhang,1 Jianmin Ma,3 Mei Li,4 Weiling Zhang,1 Huimin Hu,1 Jing Li,1 Pinwei Zhang1
1Department of Pediatrics, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Ophthalmology, Xinhua Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Ophthalmic Oncology, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Department of Nuclear Medicine, Beijing Tongren Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Dongsheng Huang, Department of Pediatrics, Beijing Tongren Hospital, Capital Medical University, West South Road 2, Yizhuang Economic and Technological Development Zone, Daxing District, Beijing, 100176, People’s Republic of China, Tel +86 01058266032, Email [email protected] Xunda Ji, Department of Ophthalmology, Xinhua Hospital, Shanghai Jiao Tong University School of Medicine, Kong Jiang Road 1665, Shanghai, 200092, People’s Republic of China, Tel +86 15921670980, Email [email protected]
Purpose: Retinoblastoma (RB) is the most common intraocular malignancy in infancy and childhood. This study evaluated the clinical and imaging features, treatment, and prognosis of patients with recurrent RB with limb bone metastases and without central nervous system involvement.
Patients and Methods: The clinical data of five patients with RB with limb bone metastases who were diagnosed at the Department of Pediatrics in Beijing Tongren Hospital between January 2015 and January 2021 were analyzed retrospectively.
Results: Three males and two females were included (seven eyes: four group E and one each of group D, C, and B). The most common symptom was pain. Three patients had bone marrow and lymph node metastases. Three patients had single and two had multiple skeletal lesions. The main bones that were involved were the femur, humerus, talus, and ulna. The simultaneous involvement of the bone marrow and cortex was also observed. Serum neuron-specific enolase (NSE) levels were significantly elevated in four cases and slightly elevated in one case; primary intravenous chemotherapy resulted in a decrease in NSE levels and the gradual resolution of the bone lesions. Two patients died at the time of follow-up and three were in complete remission. The results of the statistical analysis showed that anterior chamber invasion was correlated with prognosis, and there was significant difference in the decrease in the serum NSE levels after intravenous chemotherapy.
Conclusion: Regular lifelong follow-up of patients with RB is warranted to identify bone metastases earlier. Anterior chamber invasion may be a risk factor. The simultaneous involvement of the bone marrow and cortex is characteristic manifestations in images of RB with bone metastases. Multidisciplinary treatment especially intravenous chemotherapy is useful, at least at the beginning.
Keywords: recurrent, NSE, SRE, pathological fracture, pamidronate, osteoclast inhibitors
Introduction
Retinoblastoma (RB) is the most common intraocular malignancy in infancy and childhood. It accounts for 3% of all pediatric cancers and has a reported incidence of one per 15,000–20,000 live births.1,2 The overall survival rate in patients with an early diagnosis of localized intraocular disease exceeds 95%;3,4 however, delayed diagnoses and treatment, which are common in developing countries, may lead to extra-ocular and distant metastases. The sites of distant RB metastases include the central nervous system (CNS), bone, bone marrow, lymph nodes, and other organs.5–8 CNS metastasis is the most common, and it is usually fatal. Therefore, attention has been focused on the CNS metastasis of RB, andCNS invasion has been regarded as an independent group in the M1B in American Joint Committee on Cancer (AJCC) staging system. However, there is no authoritative study on RB patients with bone metastases in the M1a stage. Bone metastases usually involves the skull and axial bones with distant limb bone metastases being rare. Bone metastases can be confused with second primary tumors, such as osteosarcomas and Ewing’s sarcomas. Therefore, we aimed to evaluate and summarize the clinical characteristics, imaging features, treatment, and prognosis of RB patients with limb bone metastases and without CNS metastases.
Materials and Methods
Patients
A total of 1032 patients with RB were treated at the Department of Pediatrics in Beijing Tongren Hospital, Beijing, China, between January 2015 and January 2021. Of these RB patients, 671 underwent enucleation and their diagnoses were provenhistopathologically, while 361 were diagnosed clinically. In total, five patients who were diagnosed with limb bone metastasis without CNS involvement were eligible for inclusion in this study, and their clinical data were analyzed retrospectively. The initial assessment of all the patients included serum biochemistry, neuron-specific enolase (NSE) evaluation, bone marrow cytology, cerebrospinal fluid cytology, superficial lymph nodes ultrasound, computed tomography (CT)/magnetic resonance imaging (MRI) of the diseased limb, orbital enhanced MRI, cranio-cerebral MRI, and 18F-deoxyglucose positron emission tomography (PET/CT). The lactate dehydrogenase (LDH) levels were was determined using the lactic acid substrate method with a Beckman AU5800 biochemical analyzer. The NSE was determined using electrochemiluminescence with a Roche E801 instrument and supporting reagents.
Treatment Protocols
Multi-drug combination chemotherapy including carboplatin/cisplatin, cyclophosphamide/ifosfamide, vincristine, and etoposide was administered. Pamidronate was used in patients with hypercalcemia and obvious bone pain. Patients with an involvement of the weight-bearing limbs and who were prone to pathological fractures underwent surgical interventions. After chemotherapy, the patients were scheduled for radiotherapy and autologous peripheral blood stem cell transplantation (APBSCT). The adverse reactions to radiotherapy and chemotherapy were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0.
Follow-Up Analysis
Out-patient or telephonic interviews were conducted until March 20, 2022, or until the patient’s time of death.
Statistical Method
The statistical analyses were performed using the SPSS 21.0 software. The numerical data were expressed as percentages or rates. A Kaplan-Meier survival analysis was performed with survival time as the outcome. The statistical significance was set at P <0.05.
Ethics and Empowerment
This study was conducted in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki), and the research protocol was approved by the Medical Ethics Committee of the Beijing Tongren Hospital [ethics number: 2016–1116]. The parents of all participants provided written informed consent for the publication of this report and associated images.
Results
Clinical Characteristics
General Condition
The final analysis included five patients (seven eyes), with three being male (60.0%), and two being female (40.0%). All the patients were older than three years of age at the time of the diagnosis of the metastatic bone disease. In all the cases, the bone metastases occurred at the time of tumor relapse or progression. The interval between the RB diagnosis and the bone metastasis was 12–102 months. There were three (60.0%) cases of unilateral RB (two left and one right) and two (40.0%) cases with bilateral involvement. According to the International Intraocular Retinoblastoma Classification, four eyes (57.1%) were classified as group E and one eye as each of group D (14.3%), C (14.3%), and B (14.3%). None of the patients had a CNS metastasis, while three patients (60.0%) had both bone marrow and lymph node metastases. The detailed clinical characteristics are provided in Table 1. Although the retinoblastoma stage varied from groups B to E in the studied eyes, all the patients had advanced retinoblastoma in at least one eye (group D or E). After recurrence, all the patients were stage IV, according to AJCC stage system.
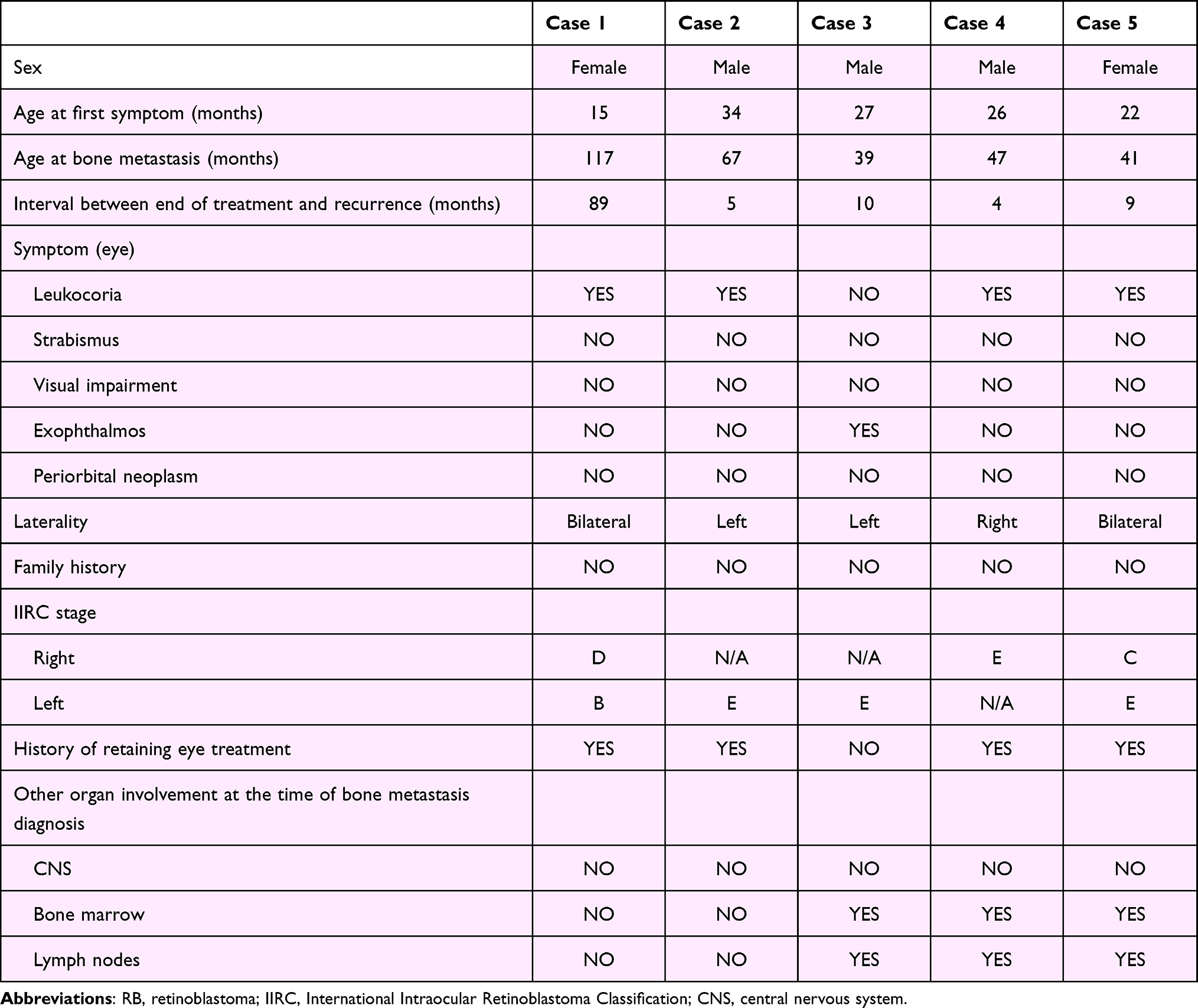 |
Table 1 Clinical Characteristics of Recurrent RB Patients with a Bone Metastasis |
Bone Metastasis
Single and multiple bone involvement were present in three (60.0%) and two (40.0%) patients, respectively. The single involvement sites were the femur and humerus. The multiple involvement sites included the talus, vertebrae, iliac, ulna, and ribs. The details of the bone metastases are shown in Table 2. Figures 1–4 show representative image results of cases 1, 2, 3, and 4, respectively. These images show the simultaneous involvement of the bone marrow and cortex.
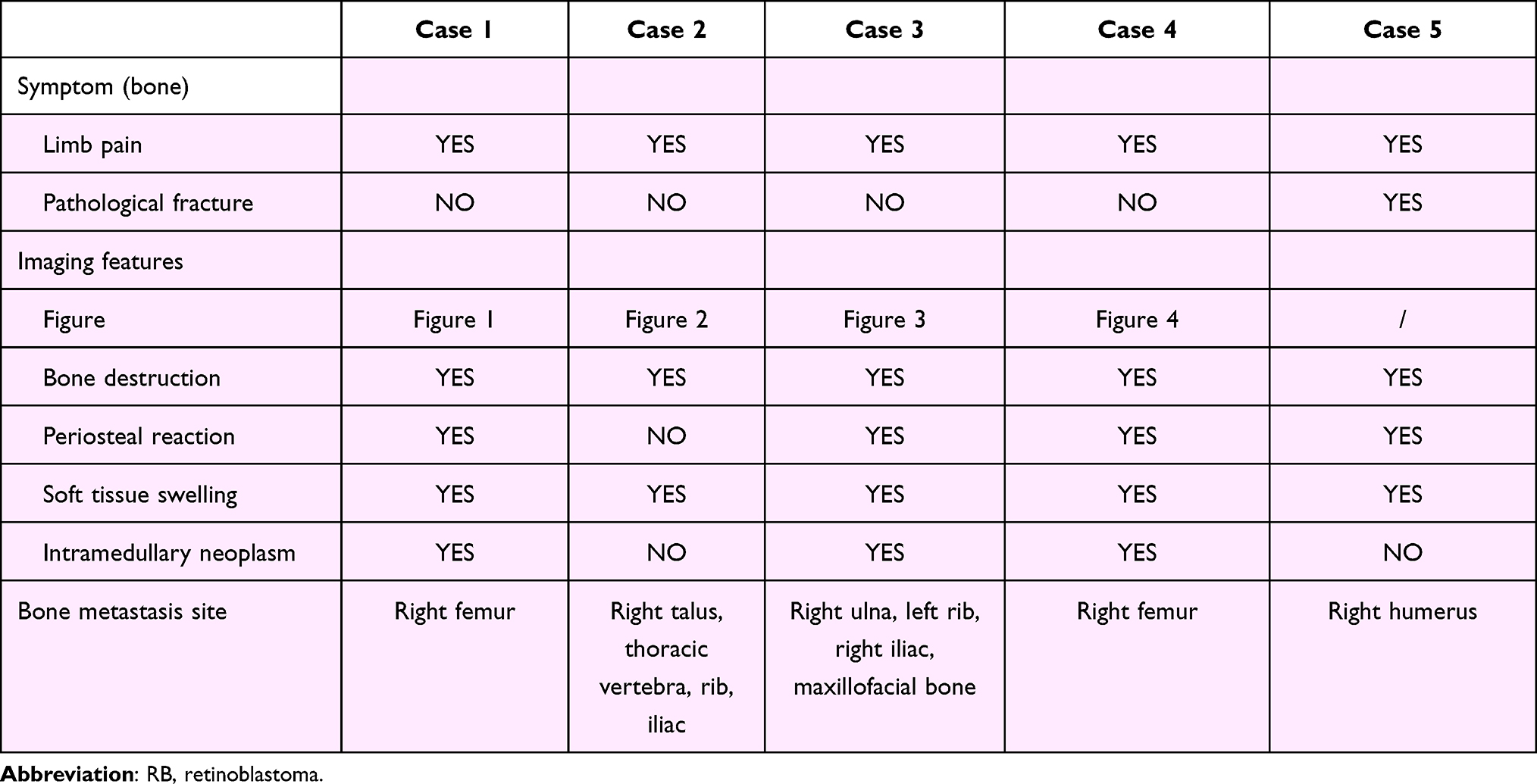 |
Table 2 Details of the Bone Metastases of Recurrent RB Patients |
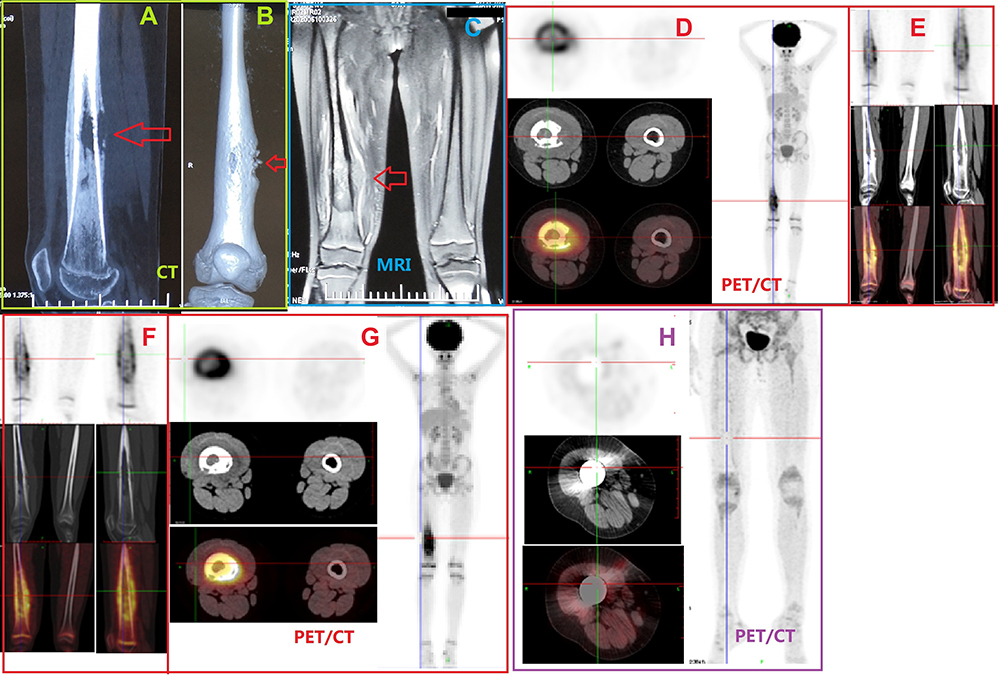 |
Figure 1 Representative imaging results from the patient with metastatic retinoblastoma to the bone in case 1 in Table 1. (A and B) CT scans showing significant bone destruction, soft tissue swelling, and intramedullary neoplasm. The red arrow showing obvious bone destruction. (C) Simultaneous magnetic resonance images showing serious bone destruction and soft tissue swelling. The red arrow showing obvious swelling of soft tissue around the diseased bone. (D–G) Positron emission tomography/CT scans showing visible thickening in the middle and distal shaft of the right femur, the soft tissue in the medullary cavity, discontinuous bone cortex, bite-like bone destruction with diffuse periosteal reaction, an uneven increase of radiation uptake, and soft tissue swelling around the lesion. Maximum standardized uptake value: 8.42. (H) Postoperative PET/CT. Abbreviation: PET/CT, positron emission tomography/CT. |
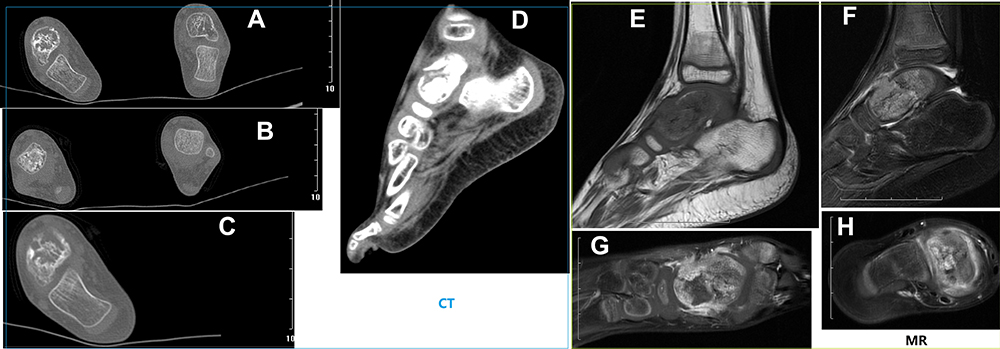 |
Figure 2 Representative imaging results of case 2 in Table 1. (A–C) CT scans showing significant bone destruction, and intramedullary neoplasm. The white arrow showing bone destruction and intramedullary masses. (D–H) Simultaneous magnetic resonance images showing serious bone destruction and soft tissue swelling. The white arrow showing obvious bone destruction and soft tissue swelling. |
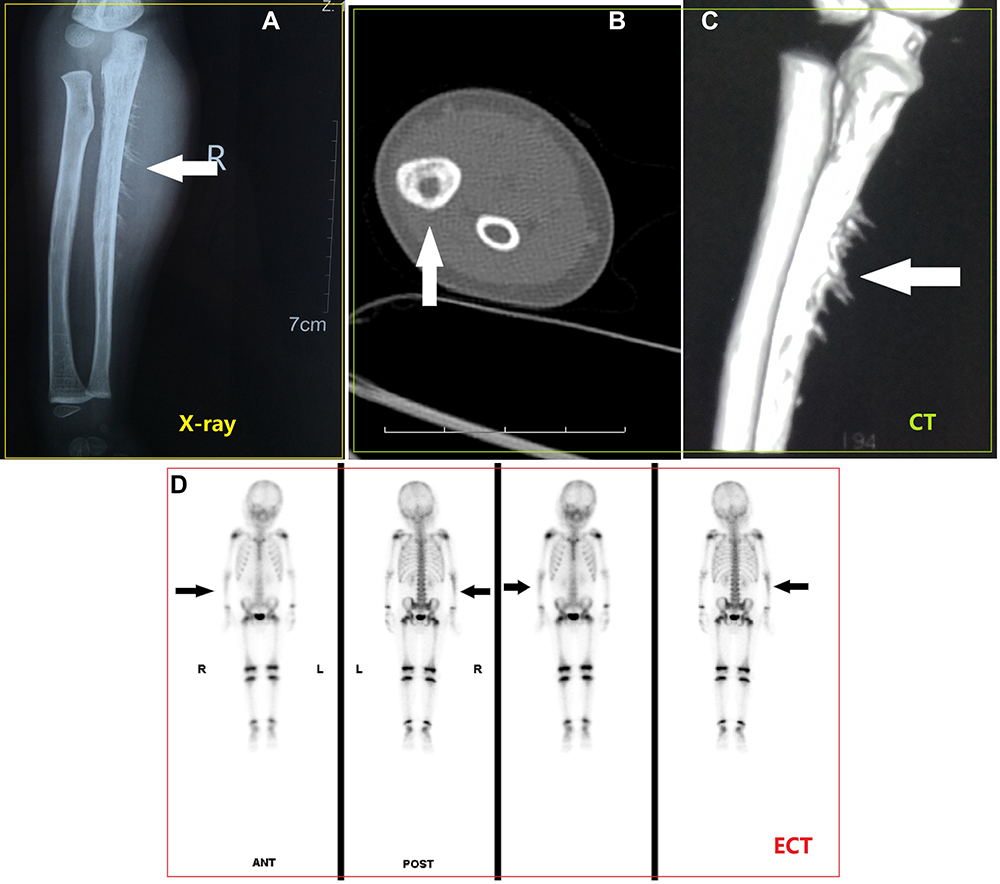 |
Figure 3 Representative imaging results of case 3 in Table 1. (A) X-ray showed “sun-ray” manifestation. The white arrow indicates the “sun-ray” sign. (B and C) CT showed significant bone destruction. The white arrow indicates bone destruction. (D) Emission computed tomography showed radioactive concentration zone of right ulna. The black arrow shows the radioactive concentration area, indicating the possibility of metastasis. |
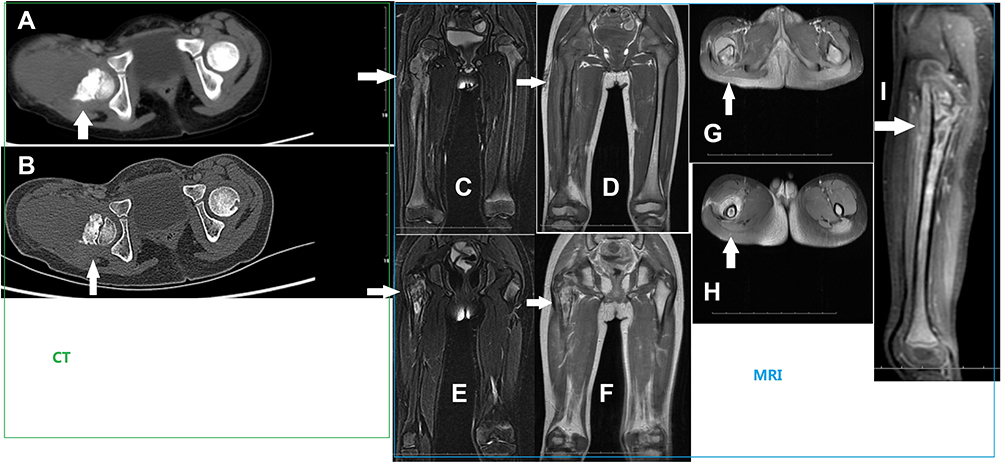 |
Figure 4 Representative imaging results from case 4 in Table 1. (A and B) CT scans showing significant bone destruction. The white arrow indicates obvious bone destruction in the upper femur. (C–I) Simultaneous magnetic resonance images showing serious bone destruction and soft tissue swelling. The white arrow indicates bone destruction and soft tissue swelling in the upper femur. |
Laboratory Examinations
The results of the laboratory examinations are presented in Table 3. Four patients had significantly elevated serum NSE and lactate dehydrogenase (LDH) levels with normal serum phosphorus (P) and normal or slightly elevated serum calcium (Ca) levels. One patient had slightly elevated serum NSE and alkaline phosphatase (ALP) levels with normal Ca, P, and LDH levels.
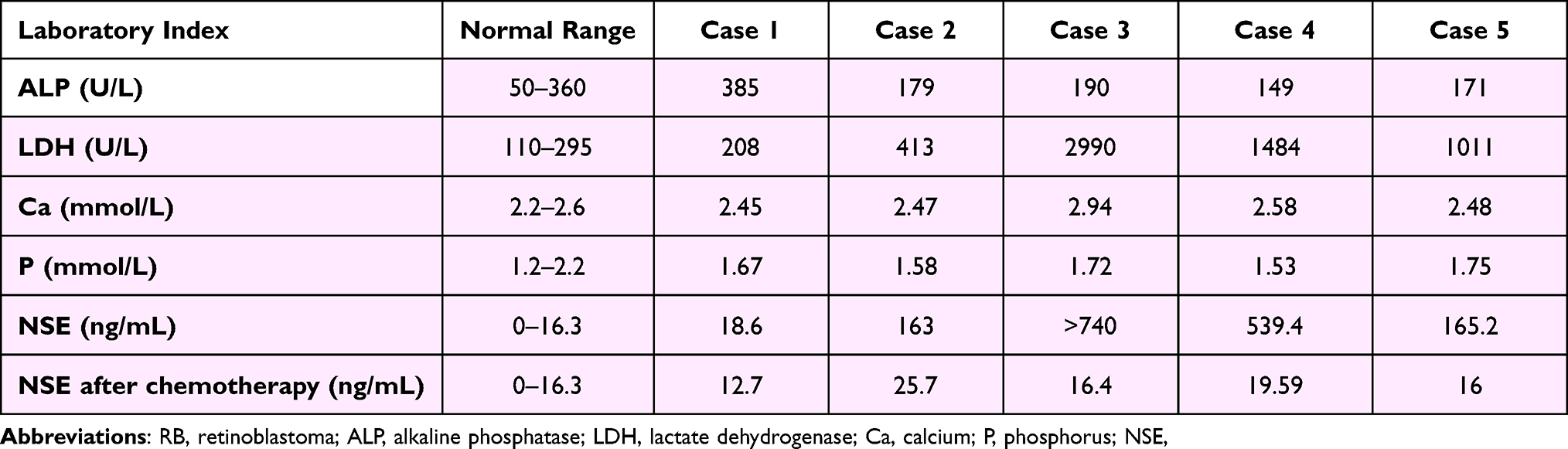 |
Table 3 Laboratory Results of Recurrent RB Patients with Bone Metastases |
Pathological Findings
Of the 1032 RB patients, 671 underwent enucleation and were provenhistopathologically. Of the 671 patients, 368 had a high risk factor. However, not all of the five patients that were studied had a high risk factor. The details of the pathology are shown in Table 4. One patient showed high simultaneous pathological risk in the anterior chamber, choroid and sclera, and one patient a high pathological risk in the anterior chamber.
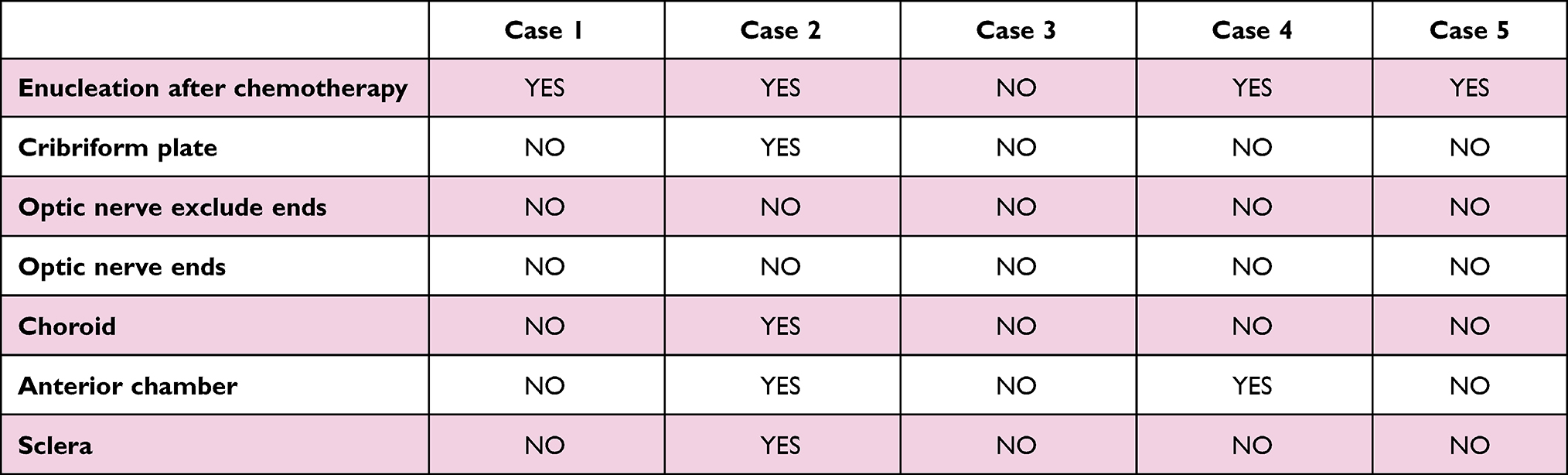 |
Table 4 Pathological Findings of Recurrent RB Patients with Bone Metastases |
Treatments
All five patients underwent enucleation either immediately after the RB diagnosis (one patient) or after failure of eye-preserving treatments including intraocular local treatment, ophthalmologic artery interventional therapy, and intravenous chemotherapy (four patients). The treatment methods used in these patients after the initial diagnosis of RB is shown in Table 5.
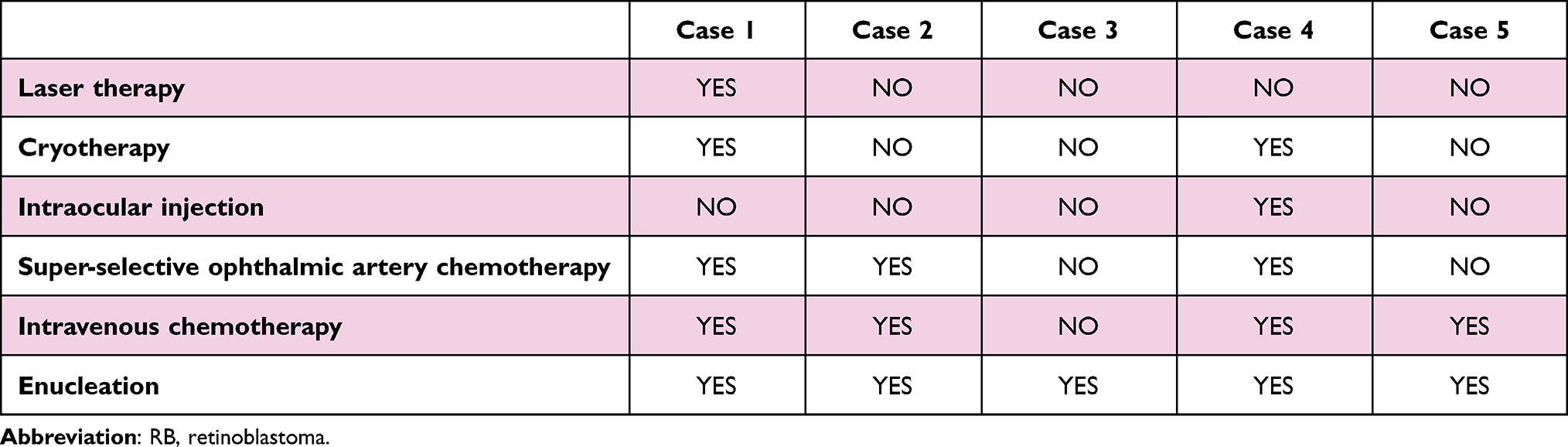 |
Table 5 Treatment for Retinoblastoma Provided in Each Case After the Initial Diagnosis of RB |
One patient underwent resection of the diseased bone and had an artificial bone insertion. One patient with bone marrow and lymph node metastases underwent APBSCT. Two patients underwent radiotherapy for the bone lesions.
The complications of the chemoradiotherapy were evaluated, and these included primarily headache, vomiting, fever, and myelosuppression, which improved after treatment. There were no cases of hemorrhagic cystitis or peripheral nervous system damage.
In all five patients, the serum NSE levels decreased, and the bone tumor regressed gradually after intravenous chemotherapy.
Prognosis
Two patients died at the time of follow-up and three were in complete remission. The survival times after the diagnoses of bone metastases of the two deceased patients who died of tumor progression, was seven and 14 months. The three patients who survived completed their treatment and were in complete remission at the time of follow-up, with r disease-free times of 23, 29, 36 months after the diagnoses of bone metastases.
Statistical Results
The statistical analyses indicated that the pathological risk factor for the anterior chamber was related to prognosis, and that there was a statistically significant difference in the decrease in the serum NSE levels after treatment. However, combined with the fact that the sample size was small, this maybe a bit of a lack of convincing. In the future, more cases will be accumulated in order to expand the sample size for to obtain statistical evidence with greater power.
Discussion
Although the long-term survival of patients with RB is improving, the prognosis of patients with distant metastases, especially CNS metastases, remains poor.8 Therefore, attention has been focused on the CNS metastasis of RB, but there is no authoritative study on RB patients with bone metastases. Bone metastases usually occur in the skull and axial bones.5,9 This study described a series of rare cases of RB with limb metastases without CNS involvement. Our findings will contribute to a greater understanding of the diversity of RB, and help pediatricians and ophthalmic oncologists formulate a more comprehensive evaluation of the patients with RB.
Distant metastases can be identified either at the time of RB diagnosis or at illness recurrence. Distant metastases usually occur within one year of RB diagnosis, and patients without evidence of metastatic disease for more than five years after diagnosis have usually been considered to be completely cured.10 In this study, while all the patients were diagnosed with bone metastases at the time of RB recurrence, the interval between the RB diagnosis and recurrence varied between 12–102 months. Based on this observation, and the inconsistencies with the intervals reported in the literature, we recommend that all patients with RB should receive regular lifelong follow-up, including local eye examinations, serum tests, and imaging. Furthermore, patients with a history of RB who present with symptoms such as limb pain and masses should undergo a detailed assessment to exclude possible bone metastases.
High-risk pathological factors for distant metastases include invasion of the optic nerve to involve the ethmoid plate, choroid, sclera, anterior chamber, iris, or ciliary body.9,11,12 However, some studies have suggested that the anterior chamber invasion is not a pathological high-risk factor.13,14 Two patients in this study had anterior chamber involvement, and both died at follow-up. The other three had no pathological high-risk factors. The results of the statistical analysis, showed that the anterior chamber invasion was correlated with prognosis. These findings suggested that the anterior chamber involvement is a high-risk pathological factor of RBand it is related to prognosis. However, the other three patients without high-risk pathological factors still developed bone metastases, which demonstrated the importance of clinical vigilance in identifying bone metastases during treatment and follow-up.
It has been unclear whether intravenous chemotherapy before enucleation can change the risk of disease progression. Some studies have proposed that preoperative chemotherapy may reduce the risk grade and affect the postoperative treatment plan,15 while, others have reported that, although chemotherapy changed the high-risk pathological factors, it did not affect the overall survival rate of patients with intraocular RB.16 Four of the patients in this study underwent enucleation after intravenous chemotherapy, and two had high-risk pathological factors. Therefore, patients with early RB may have distant metastases without obvious symptoms, and chemotherapy may result in micro-metastasis dormancy or conceal high-risk pathological factors, which may then led to suboptimal postoperative treatment. These observations demonstrated the importance of thorough assessments to rule out bone metastases before eye-conserving treatment.
Bone metastases includes osteolytic, osteogenic, and mixed lesions. Skeleton-related events (SRE) include pain, pathological fractures, hypercalcemia, and spinal cord compression. Pain is the most common SRE caused by tumor-related intimal nerve compression, injury, or pathological fractures. Pathological fractures tend to occur in osteolytic lesions, and hypercalcemia only occurs in osteolytic lesions. Our findings were consistent with those of previous reports, with all patients having either pain symptoms, pathological fracture, or hypercalcemia.
The most common sites of bone metastases have been found to be the spine, sacrum, pelvis, and proximal femur,17–19 with the involved bone structure being mainly the red bone marrow area. Cortical involvement is rare, but can be a feature of appendicular bone metastases. All five patients had evidence of the simultaneous involvement of the bone marrow and bone cortex in this study.
This study suggested that the bone marrow and bone cortex involvement are features of appendicular bone metastases. However, there is no standard method for the early detection and diagnosis of an appendicular bone metastasis. Although plain radiographs of the lesions are useful for preliminary evaluation, the sensitivity of this imaging modality is not high because obvious lesions can be seen on radiographs only when the bone density is reduced by 30–75%.20 Therefore, CT and MRI were used for a more detailed evaluation of the lesions, including lesion size and extent of invasion, and of the adjacent soft tissue. In addition, a radionuclide bone scan or PET/CT has been used to screen for bone metastasis.21 In this study, we chose primarily radiographs for the primary examination, radionuclide bone scanning or PET/CT for the systemic evaluation, and MRI for the local examination.
NSE is an important marker of neurogenic tumors. Therefore, it is valuable as a tumor marker for RB, especially for evaluating distant metastases.22 Indices of bone metabolism such as Ca, P, and ALP are also invaluable in evaluating bone metastases. In this study, the NSE levels showed a significant increase in four patients which decreased significantly after treatment. The decrease in the NSE levels were statistically significant, indicating that intravenous chemotherapy in the early stage of recurrence was effective. However, elevated NSE levels were associated with non-specific changes in markers of bone metabolism. Although the elevated NSE levels could be related to the heavy tumor burden, its low specificity precluded its use as a diagnostic marker of RB bone metastasis. Therefore, clinicians should analyze imaging findings and laboratory results comprehensively to facilitate the diagnoses.
Multidisciplinary treatment, including intravenous chemotherapy, radiotherapy, surgery, and APBSCT, is recommended for metastatic RB. Osteoclast inhibitors are used to reduce the frequency of SRE in patients with bone metastases. Treatment with pamidronate and intravenous chemotherapy have resulted in an improvement in local symptoms and a reduction in the tumor burden, confirming their efficacy in the treatment of RB bone metastases. After primary comprehensive treatment, all five patients achieved complete or partial remission. Therefore, patients with RB and bone metastasis should be treated actively. Considering the poor prognosis of RB patients with CNS involvement, we excluded patients with CNS involvement to allow us better understand the prognosis of bone metastasis. Two patients died of tumor progression during the follow-up, and three patients survived for more than one year. At present, the overall survival of RB with bone metastases is acceptable, and is significantly better than that of the CNS metastatic RB, which was consistent with the literature. However, further studies are required to improve our understanding of the pathogenesis of RB, identify high-risk factors, and ultimately improve patient outcomes.
Differential diagnosis must be made between aRB bone metastasis and an osteosarcoma and Ewing’s sarcoma. Especially for patients with hereditary RB, if radiotherapy is conducted, the probability of secondary primary tumor is higher. The supplementary examinations included histopathological examination, immunohistochemistry, molecular pathology and so on. For example, results of cone rod homeobox positive, FLI1 negative, CD99 negative, cytokinin negative, or EWSR1 fluorescence in situ hybridization negative, support the diagnosis of bone metastasis rather than sarcoma.23 At present, the PCR detection of the RB1 gene mutation is an important tool in RB diagnosis. For RB bone metastases, it is more important to identify similar diseases. Relevant gene detection methodsincludingBCOR, CIC-DUX4, SS18, EWSR, and FUS-POU5F1 have been used in the differential diagnosis of RB bone metastases.23 However, the patients involved in this study did not undergo relevant gene testing, which is also the deficiency of our research.
Conclusion
Regular lifelong follow-up of patients with RB is warranted to identify bone metastases earlier. Anterior chamber invasion may be a risk factor. The simultaneous involvement of the bone marrow and cortex are characteristic manifestations in images of RB with bone metastases. Multidisciplinary treatment, especially intravenous chemotherapy is useful, at least at the beginning.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank Editage, a division of Cactus Communication China, for editing the English text of a draft of this manuscript.
Funding
This work was supported by Beijing Hospitals Authority’ Ascent Plan (DFL20190201 and DFL20180201).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kivelä T. The epidemiological challenge of the most frequent eye cancer: retinoblastoma, an issue of birth and death. Br J Ophthalmol. 2009;93(9):1129–1131. doi:10.1136/bjo.2008.150292
2. Aerts I, Lumbroso-le Rouic L, Gauthier-Villars M, Brisse H, Doz F. Retinoblastoma update. Arch Pediatr. 2016;23(1):112–116. doi:10.1016/j.arcped.2015.09.025
3. Temming P, Lohmann D, Bornfeld N, Sauerwein W, Goericke SL, Eggert A. Current concepts for diagnosis and treatment of retinoblastoma in Germany: aiming for safe tumor control and vision preservation. KlinPaediatr. 2012;224(6):339–347.
4. Huang D, Zhang Y, Zhang W, et al. Study on clinical therapeutic effect including symptoms, eye preservation rate, and follow-up of 684 children with retinoblastoma. Eur J Ophthalmol. 2013;23(4):532–538. doi:10.5301/ejo.5000245
5. Gündüz K, Müftüoglu O, Günalp I, Unal E, Taçyildiz N. Metastatic retinoblastoma clinical features, treatment, and prognosis. Ophthalmology. 2006;113(9):1558–1566. doi:10.1016/j.ophtha.2006.03.039
6. Hu HM, Zhang WL, Wang YZ, et al. Clinical features, treatment and prognosis of retinoblastoma in distant metastasis stage. Zhonghua Yan KeZaZhi. 2017;53(2):121–127.
7. Dunkel IJ, Khakoo Y, Kernan NA, et al. Intensive multimodality therapy for patients with stage 4a metastatic retinoblastoma. Pediatr Blood Cancer. 2010;55(1):55–59. doi:10.1002/pbc.22504
8. Dunkel IJ, Chan HSL, Jubran R, et al. High-dose chemotherapy with autologous hematopoietic stem cell rescue for stage 4B retinoblastoma. Pediatr Blood Cancer. 2010;55(1):149–152. doi:10.1002/pbc.22491
9. Haik BG, Dunleavy SA, Cooke C, et al. Retinoblastoma with anterior chamber extension. Ophthalmology. 1987;94(4):367–370. doi:10.1016/S0161-6420(87)33437-2
10. Kopelman JE, McLean IW, Rosenberg SH. Multivariate analysis of risk factors for metastasis in retinoblastoma treated by enucleation. Ophthalmology. 1987;94(4):371–377. doi:10.1016/S0161-6420(87)33436-0
11. Shields CL, Shields JA, Baez K, Cater JR, De Potter P. Optic nerve invasion of retinoblastoma. Metastatic potential and clinical risk factors. Cancer. 1994;73(3):692–698. doi:10.1002/1097-0142(19940201)73:3<692::AID-CNCR2820730331>3.0.CO;2-8
12. Finger PT, Harbour JW, Karcioglu ZA. Risk factors for metastasis in retinoblastoma. SurvOphthalmol. 2002;47(1):1–16.
13. Baroni LV, Sampor C, Fandiño A, et al. Anterior segment invasion in retinoblastoma: is it a risk factor for extraocular relapse? J Edatrexate lOncol. 2014;36(8):e509–e512.
14. Sreelakshmi KV, Chandra A, Krishnakumar S, Natarajan V, Khetan V. Anterior Chamber invasion in retinoblastoma: not an indication for adjuvant chemotherapy. Invest Ophthalmol Vis Sci. 2017;58(11):4654–4661. doi:10.1167/iovs.17-22111
15. Zhao J, Dimaras H, Massey C, et al. Pre-enucleation chemotherapy for eyes severely affected by retinoblastoma masks risk of tumor extension and increases death from metastasis. J ClinOncol. 2011;29(7):845–851. doi:10.1200/JCO.2010.32.5332
16. Wang YZ, Huang DS, Shi JT, et al. Effects of pre-enucleation chemotherapy on pathological stage and prognosis of patients with intraocular retinoblastoma. J China Pediatr Blood Cancer. 2016;21:269–274.
17. Choi J, Raghavan M. Diagnostic imaging and image-guided therapy of skeletal metastases. Cancer Control. 2012;19(2):102–112. doi:10.1177/107327481201900204
18. Tubiana-Hulin M. Incidence, prevalence and distribution of bone metastases. Bone. 1991;12(suppl 1):S9–S10. doi:10.1016/8756-3282(91)90059-R
19. Krishnamurthy GT, Tubis M, Hiss J, Blahd WH. Distribution pattern of metastatic bone disease. A need for total body skeletal image. JAMA. 1977;237(23):2504–2506. doi:10.1001/jama.1977.03270500056025
20. Even–Sapir E. Imaging of malignant bone involvement by morphologic, scintigraphic, and hybrid modalities. J Nucl Med. 2005;46(8):1356–1367.
21. Chang CY, Gill CM, Joseph Simeone FJ, et al. Comparison of the diagnostic accuracy of 99 m-Tc-MDP bone scintigraphy and 18 F-FDG PET/CT for the detection of skeletal metastases. ActaRadiol. 2016;57(1):58–65.
22. Liu ZP, Zhou KY, Chen LL, Xiao ZH, Chen YZ. A preliminary study of retinoblastoma-related serum tumor markers. Zhongguo Dang Dai ErKeZaZhi. 2017;19(3):318–321.
23. Ting SC, Kiefer T, Ehlert K, et al. Bone metastasis of retinoblastoma five years after primary treatment. Am J Ophthalmol Case Rep. 2020;19:100834. doi:10.1016/j.ajoc.2020.100834
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.