")
Back to Journals » International Journal of Women's Health » Volume 13
Clinical Care of Victims of Interpersonal Violence and Rape in Tanzania: A Qualitative Investigation
Authors Mgopa LR , Rosser BRS, Ross MW , Mohammed I, Lukumay GG , Massae AF, Mushy SE , Mwakawanga DL , Mkonyi E, Trent M, Bonilla ZE, Wadley J, Leshabari S
Received 13 January 2021
Accepted for publication 23 June 2021
Published 24 July 2021 Volume 2021:13 Pages 727—741
DOI https://doi.org/10.2147/IJWH.S301804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Lucy R Mgopa,1 B R Simon Rosser,2 Michael W Ross,3 Inari Mohammed,2 Gift Gadiel Lukumay,4 Agnes F Massae,4 Stella E Mushy,4 Dorkasi L Mwakawanga,4 Ever Mkonyi,2 Maria Trent,5 Zobeida E Bonilla,2 James Wadley,6 Sebalda Leshabari4, †
1Department of Psychiatry and Mental Health, School of Medicine, Muhimbili University of Health and Allied Sciences (MUHAS), Dar Es Salaam, Tanzania; 2Department of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, MN, USA; 3Program in Human Sexuality, Department of Family Medicine, University of Minnesota, Minneapolis, MN, USA; 4Department of Community Health Nursing, School of Nursing, Muhimbili University of Health and Allied Sciences, Dar Es Salaam, Tanzania; 5Department of Adolescent and Young Adult Medicine, Johns Hopkins University Schools of Medicine and Public Health, Baltimore, MD, USA; 6Department of Counseling and Health Services, Lincoln University, Philadelphia, PA, USA
†Dr. Leshabari passed away on October 16th, 2020.
Correspondence: B R Simon Rosser
University of Minnesota, 1300 S. 2 nd St. #300, Minneapolis, 55454, MN Tel +1 612- 624-0358
Email [email protected]
Introduction: Africa has high rates of interpersonal violence and rape, although little is known about how these cases are handled in the clinical setting.
Methods: We enrolled 121 health care professionals and students in Tanzania from the fields of midwifery, nursing and medicine, and conducted 18 focus group discussions stratified by both professional and clinical experience. Two clinical scenarios were presented across all groups and participants were asked to give their opinions on how the hospital they worked in would manage the cases. Case 1 focused on how to address a case of an injured woman beaten by her husband (and whether the perpetrator would be reported to the police). Case 2 focused on how to handle a rape victim who is brought to the hospital by the police.
Results: Participants considered both cases as emergencies. There was a similarity in the clinical care procedures across both scenarios. This included building rapport with the patient, prioritization of the medical care, history taking, and referring to other specialties for follow-up. Participants differed in how they would handle the legal aspects of both cases, including whether and how to best follow mandated reporting policies. Providers wondered if they should report the husband in case study 1, the criteria for reporting, and where to report. Providers displayed a lack of knowledge about resources needed for sexual violence victim and the availability of resources.
Conclusion: These findings indicate that cases of intimate partner violence and rape are likely to be under-reported within hospitals and clinics in Tanzania. Health care providers lack training in their required obligations and procedures that need to be followed to ensure victim’s safety. The findings confirm that there is a need for health care students in Tanzania (and possibly Africa) to receive comprehensive training in how to handle such cases.
Keywords: IPV, violence, rape, GBV, health provider, Tanzania
Introduction
Sexual health is fundamental to an individual’s physical and emotional health, between couples, within families and to the socioeconomic development of a country.1 Key sexual health challenges across Africa include unintended pregnancy and abortion, sexual orientation and gender identity concerns, HIV/AIDS, sexually transmitted infections (STIs) and reproductive tract infections, mental health issues related to sexual health, sexual dysfunction, and violence related to gender and sexuality, including female genital mutilation.1,2
Violence related to gender and sexuality is both a violation of human rights and a health concern.1 According to the World Health Organization (WHO), violence can occur through physical, sexual, and psychological harm, or through deprivation and neglect, resulting in serious health complications up to and including death.3 Despite its multiple forms and typology, violence towards women is most commonly perpetrated by men, especially intimate partners, family members and to a lesser extent, strangers.1 Globally, estimates of physical and/or sexual violence among all ever-partnered women were reported to be 30%, with highest prevalence of 37% in the Mediterranean and African regions, followed by the Americas (30%), and other high-income regions including some European countries (23%).4 Sexual violence among non-partnered women was estimated to be 7% worldwide; however, 12% of non-partnered women reported to have ever experienced sexual violence in sub-Saharan Africa.4 A WHO multi-country study on women’s health reported the prevalence of physical and sexual violence among ever-partnered women in Tanzania being 41% and 23%, respectively.5 One in 10 women reported non-partnered sexual violence from the age of 15, while 19% of non-partnered women reported having experienced physical violence in their lifetime.4,5
Violence has both direct and indirect effects on sexual health outcomes. Sexual violence can be an important factor in HIV/STI transmission, unwanted pregnancy, and spontaneous abortion.1 Moreover, its documented psychological effects include lack of confidence, low self-esteem, inability to make safer sexual choices, and an inability to negotiate discussions about sexual intercourse with sexual partners.1 These associations show the importance of providing sexual health care services to individuals. Such services should be available and accessible at all levels of health facilities (ie, from primary level to tertiary/referral level) and equipped with trained staff so that comprehensive care is provided to those in need.1,6
The majority of health care professionals from sub-Saharan Africa are socio-culturally conservative and lack adequate training in either sexual health or in addressing victims of violence. Negative attitudes, stigma and discrimination are high among health care providers towards the populations most likely to be victimized especially young people, women, and key populations, including men who have sex with men, transgender people and sex workers.1,7,8 The negative attitudes of some health care providers reflect cultural and societal norms that tolerate violent acts, prefer violence to be resolved discretely within the extended family system, reflect patriarchal attitudes that blame the victim, and promote solutions that favor victims remaining within the family unit.1,9 In many African countries, health care providers are unaware of their legal obligations towards issues related to violence and may be unwilling or cautious about reporting gender-based violence (GBV) and its related cases. Providers lack confidence and comfort in addressing cases involving violence, and indeed in addressing sexual health–related problems in general.7,8,10
Across Africa, victims of GBV including rape victims face enormous challenges when receiving health services.11,12 Providers’ misconceptions, judgements, unaccepting attitudes, and stereotypes around various forms of violence acts may increase the risk of patients not disclosing about their health status and violence experiences.13,14 Given the lack of training, the health providers’ responses towards victims may reflect their own personal experiences, values and sociocultural beliefs.13–15
The Tanzania government, through its Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC), developed a training curriculum for health care workers to educate providers on GBV screening protocols, mandated requirements, and management to expand knowledge and awareness. Despite these efforts, survivors of abuse to date still face inadequate care at the hospitals due to limited resources including the unavailability of forensic kits, and inadequate continuing education training to health professionals.16
Delayed and/or inadequate care of assault victims in Tanzania occurs when care providers are uncertain about their legal responsibilities and lack information regarding appropriate or mandated referral of victims to other related services including community agencies, the police and the legal system.17 Mandatory reporting is the legal standard that requires specific individuals including all licensed health care providers to report actual or suspected abuse to a legal or government agency.18,19
Under Tanzania law, all assault cases, including those that involve rape and intimate partner violence, require police involvement and investigation.9 The way the law is written, health providers are mandated reporters for all violence of minors and adults to police, with the proviso that reporting of assault against an adult must be made with the victim’s consent. In practice, victims are asked by health care providers to first report and provide a statement to the nearest “Gender and Children’s Desk” at the local police station, a unit that deals with women and children protection against gender-based violence. After this, the police will provide the victim with a police-issued medical examination form, commonly known as police form three (PF3).9,20 Armed with this form, the victim can then go to the health facility where the health provider is required to record any evidence of assault including physical examination findings and collection of forensic evidence (with a rape kit), that will be used by police for further investigations and court proceedings.9
In Tanzania, the PF3 is the critical document during legal proceedings, especially in cases where the victim decides to press charges, or when the police have captured the perpetrator (rapist) and decide to transfer the case to court. Legally, victims do not need to have a PF3 in hand before they can receive treatment. A PF3 form can also be obtained while the victim is receiving emergency care. The current GBV and forensic guidelines used in Tanzania instruct health care providers to provide life-saving interventions, timely management, to collect evidence and samples, as well as instructions on both proper preservation of evidence and filling in all the required forms including PF3.21 The PF3 usually consists of four parts: (i) Request for medical examination (must be completed by the police officer); (ii) Medical details of the alleged case to be completed by the medical practitioner carrying out the examination; (iii) Assault, accident and other cases (where the provider summarizes the presenting information, any relevant history and evidence collected); and (iv) Sexual assault cases (history/s of sexual assault, physical findings, evidences and sexual health presentation, eg, HIV, STI’s and pregnancy outcomes). Parts iii and iv are completed by a medical practitioner and a subsection under part iv provides a space for medical practitioners to add any additional remarks.21
As compared to hospitals and clinics in high-income countries, the context of providing clinical care in Tanzania, even to assault victims and particularly in publicly funded facilities, is more challenging.22 Provider–patient ratio is low in both urban and rural areas, requiring providers to be efficient with each patient.22,23 There are challenges in ensuring confidentiality in care settings where multiple patients may be present, equipment shortages include lack of rape kits at clinics, and staff lack the requisite training. These factors provide additional barriers to providers following the legal guidelines for assessing and treating victims.22–24
The aim of this study was 1) to assess the clinical practice of experienced health care providers and those in training (health students) towards intimate partner violence and rape victims, and 2) to explore providers’ experiences and challenges during clinical care provision and examine their legal understanding and practices related to cases of assault. The information obtained was used to inform an Afrocentric, comprehensive sexual health training curriculum for midwifery, nursing and medical students.
Materials and Methods
Study Design
This qualitative study was part of a larger mixed methods research study entitled Training for Health Professionals that sought to inform the development of a comprehensive sexual health curriculum for health care students attending an urban medical university known as Muhimbili University of Health and Allied Sciences in Dar es Salaam, Tanzania. The qualitative portion of the study investigated the experiences of health professionals and students across the different professions (ie, midwifery, nursing and medicine) and by experience (providers versus students) when providing sexual health care, in order to understand, compare and identify gaps in clinical practice, and to obtain information needed for the training of future health professionals.
Focus group interviews were conducted to examine the perspectives of both practicing professionals and students in each healthcare profession regarding the provision of sexual health in Tanzania. This study was a collaboration between two major universities: The University of Minnesota in the US and Muhimbili University of Health and Allied Sciences (MUHAS) in Tanzania. Ethical clearance was approved by the institutional review boards of both universities and the Tanzania National Institute of Medical Research (NIMR). Permission to conduct the study was also obtained from the involved study sites. The study was exempted from human subject’s review because its focus was on studying clinical procedures in health care settings.
Study Participants and Recruitment
Midwifery, nursing, and medical experienced health care providers were recruited from three public and private hospitals in Ilala District, Dar es Salaam: Muhimbili National Hospital, Mnazi Mmoja Hospital and Aga Khan Hospital. Midwifery, nursing and medical students were recruited from MUHAS and were in their fourth year (final year for nurses and midwives and penultimate year for medical students). Recruitment staff posted announcement fliers around the MUHAS campus noticeboards. These fliers had the study contact address and phone number whereby interested students could sign up to participate. Providers were recruited by profession and from different specialties to allow diversity. If there was more than one provider who met the criteria from the same professional unit, purposive sampling was used to enroll the one with most experience and expertise.
Study Procedures
We conducted a total of 18 focus group discussions in June 2019 in Dar es Salaam, Tanzania, with 121 health care providers and students from fields of nursing, midwifery and medicine. We collected a purposive sample stratified by health profession and experience (18 focus groups in total; see Figure 1). Each group had five to eight participants and took 60–90 minutes. To enhance diverse opinions and experiences, we recruited participants with different demographic characteristics.25 To ensure comfort and confidentiality, the focus groups were held in private rooms within the hospital or university premises. Sessions began by a moderator welcoming the participants, making them comfortable with some refreshments and then reviewing a set of ground rules for the discussion. Ground rules for each group included that participation was voluntary, that participants could withdraw from the interview at any time, or say pass to any question, that confidentiality was encouraged (and that no individually identifiable information would be reported) and that the session was being audio recorded and would be transcribed. All participants provided informed consent for participation and publication of anonymized responses provided during discussions. Each group was led by a moderator assisted by a co-moderator who took notes and observed non-verbal expressions of the participants. Participants were instructed that they could communicate in either Kiswahili or English. The questions were asked in Kiswahili and most of the discussion was in Kiswahili.
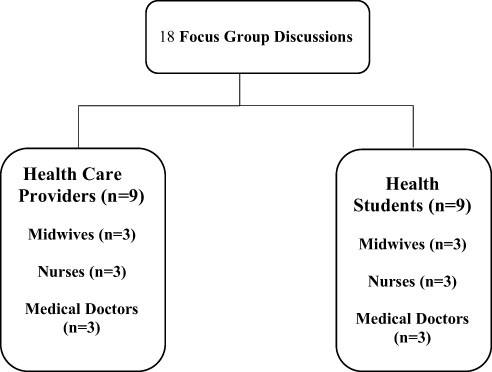 |
Figure 1 Distribution of focus groups among students and health professionals. |
At the end of the session, each participant was reimbursed with a token of 60,000 Tanzania Shillings (about US$25) for transport and other encountered costs. Participants were asked to complete a brief demographic form (ie, age, gender, years of experience or clinical rotation, department) on a paper, which was collected prior to initiating the focus group interview. Participants were asked to write their first names or nicknames on a table card.
A team-based approach was employed throughout all stages of the research, including data analysis.26 The team developed and tested a semi-structured interview protocol that contained key questions and probes, about current health practices in the clinics or hospitals or for student’s, most recent rotation in the clinics or hospitals. First, we asked participants to identify the most common sexual health challenges in Tanzania, and among their own patients. The next set of questions asked participants how seven clinical cases “would be treated or not treated in Tanzania” The cases were, in order of presentation, male erectile dysfunction, interpersonal violence (IPV), vaginal pain, child sexual abuse, rectal gonorrhea, rape, and masturbation. In this paper, we present the results of the interpersonal violence and rape case studies. The questions were asked as follows: Case 1: “A woman who comes in bruised with a broken arm and says her husband beats her. How would this be handled?” The follow-up probe was, “How many of you would report the husband to police?” Case 2: “A police officer brings a rape victim to the clinic. How would this be handled?” The follow-up probe was, “What about collecting the rape kit from the victim?”
Data Management and Analysis
All data, including audio files, flipcharts and written notes, were stored in locked filing cabinets or electronically in password-protected files. The audio files were transcribed verbatim in Kiswahili then translated into English. A team-based coding approach was utilized.26
Codebook development followed procedures adapted from published literature for team-based codebook development.26,27 The initial list of codes was generated from the focus group interview guide, the literature that informed the protocol, and emerging ideas provided by the interview team. While most codes on the codebook were deductive, inductive codes emerge as the coding progressed. Both deductive and inductive codes derived during the coding process were added to the final codebook. Codebook development was an iterative process involving revisions and refinements of codes and their definitions during all coding steps.
Thematic analysis was conducted to identify, organize, and describe the findings of this study.28 The analysis was not guided by a predetermined theoretical framework granting the team greater flexibility during the coding process, and enabling team members with different backgrounds and levels of experience in qualitative research to engage in the data analysis process.26
The six Tanzanian moderators and co-moderators, who led the focus groups, also conducted the thematic analysis. The team was divided into pairs of two coders who had the most relevant clinical and/or research experience for each case study. Thematic analysis was conducted following a series of steps beginning with 1) discovery of the themes and emerging ideas during open coding, 2) application of codes to all transcripts, and 3) final identification and description of categories and themes. During open coding, each coder individually read and re-read the transcripts and manually coded an initial set of transcripts to identify codes and early ideas. The team of coders met to compare codes and their meaning, reconcile any coding discrepancies, and establish code definitions. These codes were entered into the codebook and shared with the larger research team for another layer of verification and validation. Following this initial meeting, the teams continued coding their respective sections and held regular meetings throughout the coding period. The peer debriefing method was used as another layer of verification, confirmation and codebook refinement.29
This process of code development, refinement and verification continued throughout all stages of the coding process. During the final coding steps, each team reviewed the codes and emerging themes, clustered them based on similarities, and developed categories to capture codes with shared meanings. These categories were applied to the transcripts and representative quotes were identified to report the themes that emerged during data analysis. The final categories and themes were shared with the larger research team for a final verification and validation. This iterative process was aided by the use of an online Google document containing the codebook annotated with memos and weekly team meetings to discuss the codes and coding procedures.29
Results
The demographic data of the study participants, stratified by profession and experience, are detailed in Table 1. Half of the sample were experienced health providers (n=60) and another half, students (n=61). The experienced providers were mainly female, middle aged, and on average had 14.6 years of clinical experience. The student sample were mainly male, younger (on average 25.5 years old), and all in their fourth year of training.
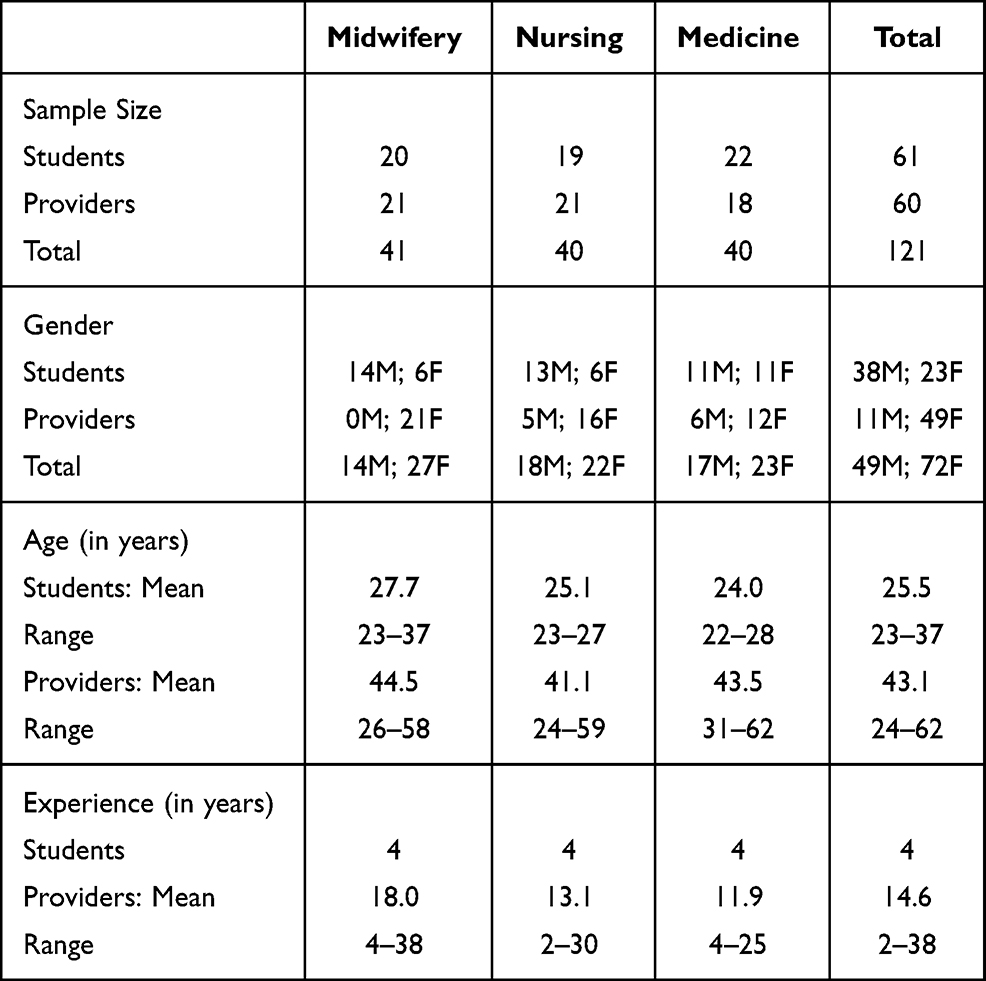 |
Table 1 Demographic Characteristics of Health Care Students and Providers Stratified by Experience and Profession, Tanzania (N=121) |
Each case was analyzed individually and each had one central theme with two main categories (see Tables 2 and 3).
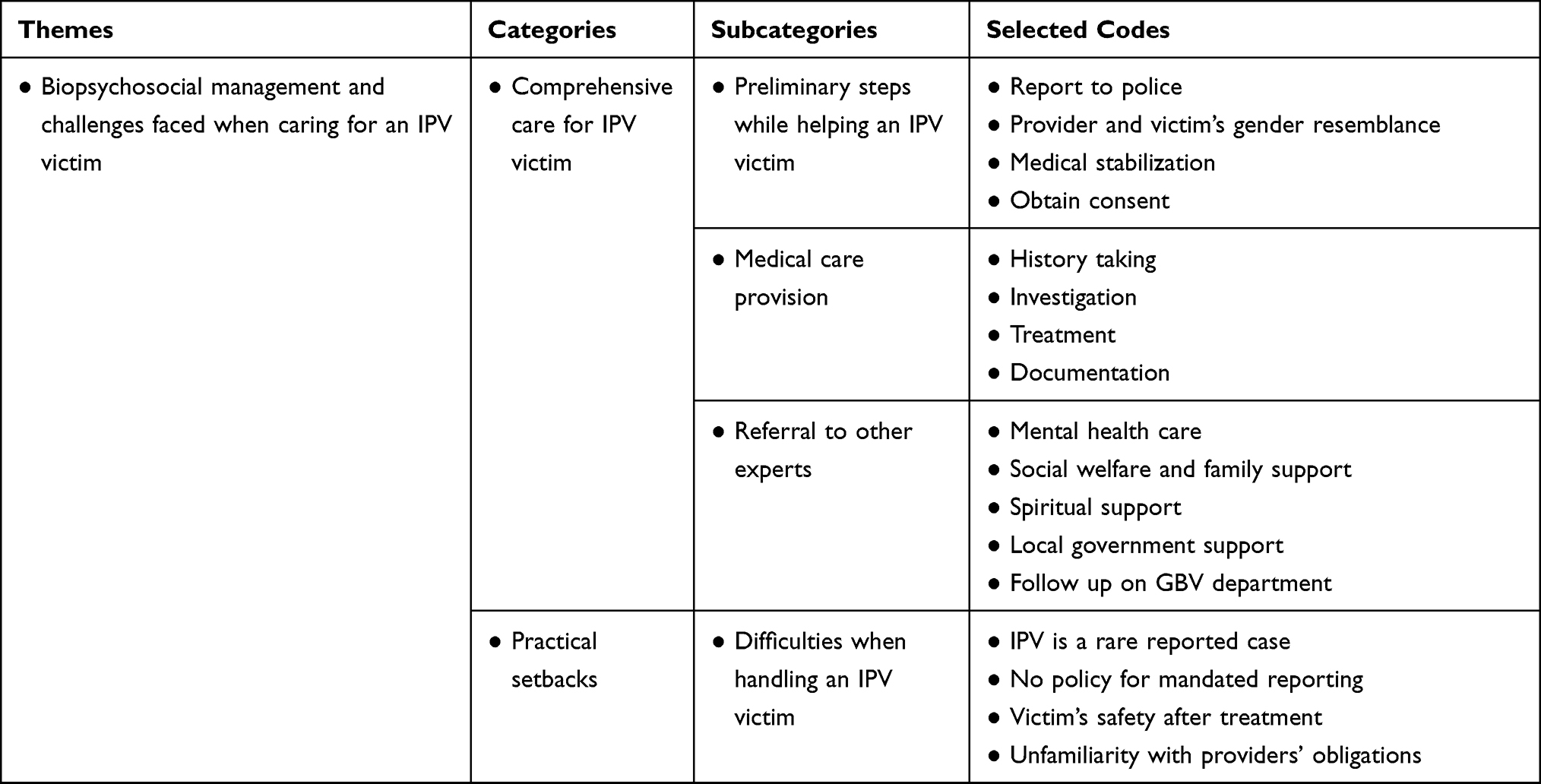 |
Table 2 Biopsychosocial Management and Challenges Faced When Caring for an IPV Victim |
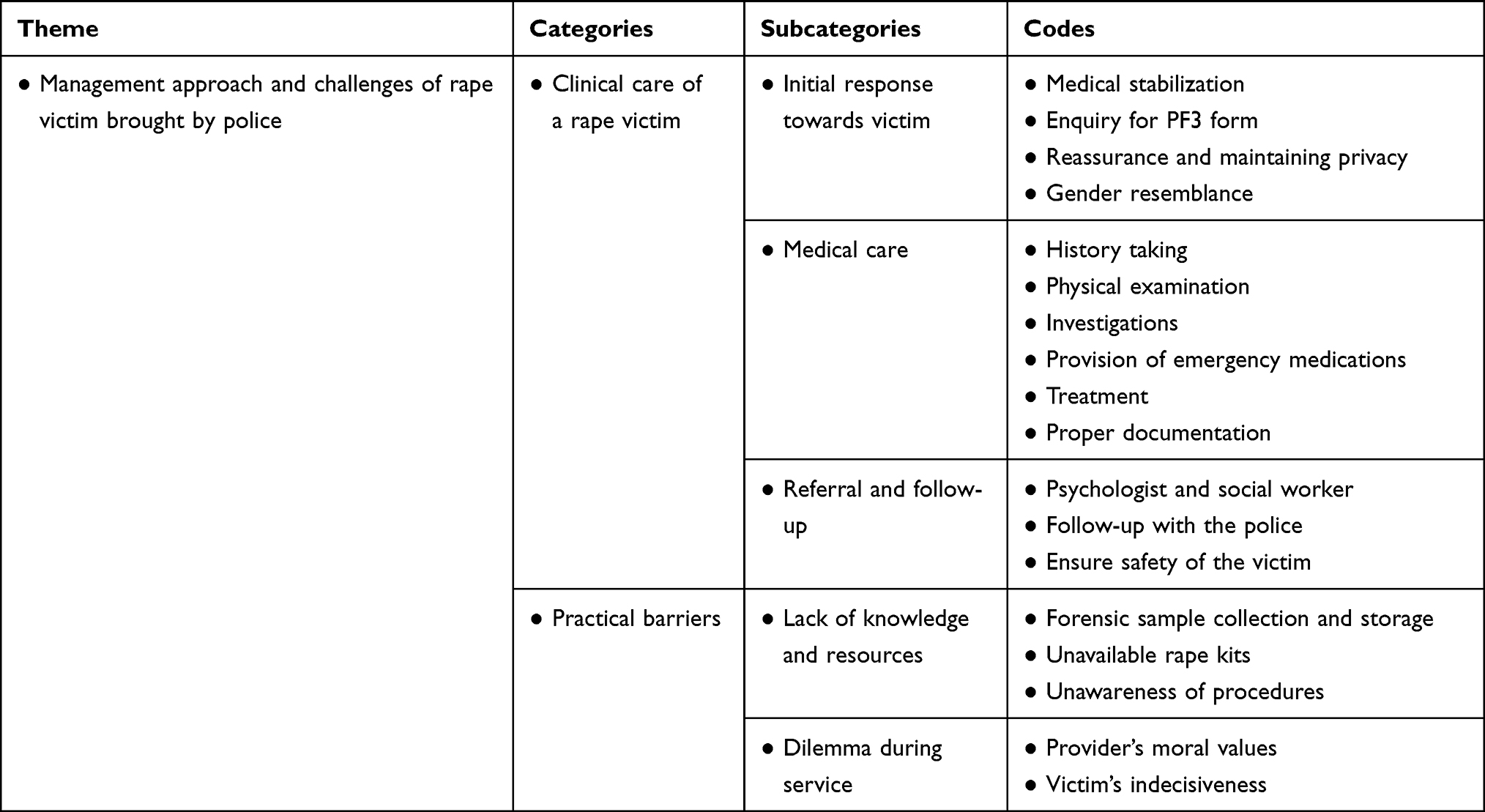 |
Table 3 Management Approach and Challenges of a Rape Victim Brought by Police |
Case 1: Biopsychosocial Management and Challenges When Caring for a Victim of Interpersonal Violence
Participants shared their experiences on how they would handle a person who has been abused from the time the victim arrived at the hospital to the point of discharge or being referred to other health colleagues and authorities.
Comprehensive Care for IPV Victim
The participants said that any victim of IPV deserves comprehensive care including both physical and mental health management. Both students and health care providers mentioned that among the first things they would consider is whether or not to involve the police. Participants recognized that violence is considered to be a police case in Tanzania. Participants explained, the patient should either come to the hospital with a police form (PF3) that shows the victim has already filed her complaint; or if not, then she would be required to go back after her initial treatment or send a relative to the police station to obtain it. Participants stated that observing the patient’s state is critical during this process because if the victim requires immediate medical attention then she will need to be cared for and stabilized first to save her life. For example, if she came in with fractures, bleeding, or any other injuries, they would attend to these. Moreover, while attending the patient, they said care providers should make the patient comfortable Strategies participants mentioned to facilitate comfort included having a provider of the same gender attend the victim, asking for and obtaining informed consent to attend to any injuries, and explaining any necessary clinical procedures prior to performing them. Most participants acknowledged the need to involve the law and suggested that the perpetrator (husband) should be taken into custody.
Depending on the situation and condition she presents with, for example, if she came in bleeding or anything that is life threatening, we must handle that first.… Then, she goes for PF3; when she gets it then she can return and get other services. (Nurse professional)
However, a few participants (especially students) disagreed about reporting the husband to the police as long as the victim did not have life-threatening injuries. They explained that they saw this domestic violence as a family or marital matter, better handled by the extended family. In Tanzania, most families are extended meaning a typical family includes both parents of the couple, uncles, aunties, grandparents, and other elders; all of whom may participate in resolving a marital conflict.
“Yes … ! We will not report. And if it does not involve critical injuries, I will also not report to the police.” (Medical Student)
Some students added that they might have the victim call her husband to the hospital during the treatment process as they felt that it was important.
For me, after treating her and making her stable, I will take history and ask her to call her husband … not only her husband, I will even call the patient’s relatives and family so they can discuss and know what to do. If you call the husband alone, they might go out and keep on fighting each other again. (Nursing student)
Once the patient is out of immediate danger, participants stated they would take a proper history, clarifying it should contain current complaints, any previous history of assault, family and social history, medical history and any surgical history in the past, a mental health history and a thorough mental status evaluation. Participants mentioned that in addition to the physical examination, laboratory tests could be significant. They said, by doing so, a provider would able to assess clinical status and avoid consequences to the victim. Discussion included the collection of evidence of sexual violence, sexually transmitted infection testing including HIV, and/or initiating post-exposure HIV prophylaxis, and imaging for any signs of possible fractures.
I will attend to her by first asking some questions, what happened to a broken arm or those bruises or if she had confronted her husband or [if] it’s about sex, maybe she was not prepared [unwilling to have sex]. Then, after taking her to appropriate room for x-ray or to a doctor, for issues of bruises, I will start medication immediately. (Nursing student)
Participants stressed that all information, procedures performed on the patient and treatment given should be well documented in a patient file. Potential treatments discussed included medications, psychological and social interventions (eg, to explore the victim’s home environment and social life). Participants also emphasized counseling for both the victim and the husband, individually at first, and later on as a couple. Participants reasoned that this could be helpful to minimize future conflicts once the couple returned home. Couple counselling was emphasized by all participants (across profession and experience).
Lastly, once treatment has commenced, you can call her husband and give counseling together so that you can get to understand the source of the problem and advise them. (Medical student)
For me … I would call her husband and, together with her, we will find solution of the problem. The husband would be called [in] to resolve the problem. Since it is a family issue, they will have to come together for solution by themselves. (Midwife professional)
“Better to talk to each person, separately at first, then keeping them in one meeting and then decide if doing for both of them.” (Nurse professional)
During the discussion, some participants appeared to raise the possibility that the victims may have caused or deserved the abuse.
On my side … I should know first why she has been beaten by the husband? … Sometimes, she might be the cause. Hence, I will meet them (victim and husband) and discuss on how we will solve the issue together. (Nursing student)
Participants mentioned several referrals that they would consider: the mental health department of their hospital for a thorough mental status and psychological evaluation as well as treatment in case she presents with mental illness such as post-traumatic stress symptoms. The hospital’s social welfare department was raised also, where social workers specialize in social investigations and practical management such as finding a safe house. Social welfare in Tanzania can also involve local government or community leaders, as well as the victim’s family for family intervention. Religious leaders were a third referral mentioned mainly by the experienced professionals. Religious leaders were seen as an appropriate referral for victims seeking marital reconciliation. Finally, the gender-based violence desk (either at the hospital or at the police station) was raised by most groups, which is where a victim can initiate legal proceedings.
You will refer her to a psychologist for further management, but sometime abused women who come with violence or rape cases, normally may start at the police so they come to you already stated everything legally. Therefore, you manage your part and refer her to psychiatrist/psychologist. (Medical doctor)
What we usually do is referring her to a social worker. The social worker will deal with that aspect … and lead her to a proper channel. Social worker can also link her to local government or police to allow her (to report through) proper channels. (Medical doctor)
You know these things of GBV [gender-based violence] have processes. Although I will encourage her to go by my side, I will do my duties as a nurse. Then, I will take her to social worker who will take her to local leaders to which they will write a file and take her to police. I think, those are the processes. (Nurse professional)
Practical Setbacks
Regardless of having some knowledge about what to do when caring for an IPV victim, participants did raise concerns about challenges during service provision. Some participants reported that despite the sensitivity of gender-based violence in Tanzania, there is no clear policy in our country that allows health professionals to report adult cases to the required authorities as part of mandated reporting. As such, many participants were unsure of their professional obligations and legal duty. The health professionals, more than students, emphasized they lacked knowledge concerning their obligations when dealing with an adult IPV case. Others did not know what to do with the victim after they had treated the injuries or once they discharged the victim. Most participants stated that IPV cases in practice are rarely reported in most hospitals. They saw IPV as clinically uncommon. They also opined that frequently violence victims deny or minimize the causes of their injuries or trauma due to fear of additional abuse or other negative consequences from the perpetrator.
It is a very uncommon scenario for a woman to come and say her husband has beaten her. It is really uncommon; I have never seen [it]. … I do not have an obligation to take up her case. (Midwife professional)
You know even policy does not give us the mandate to report. As far as I know, there is no policy which allows us as health professionals to go and report these cases.… So, where do I take her so that she can be safe? Our hospital, they do not have a department of some form or unit where you can report. Should I call the police? (Medical doctor)
Other[s] come when badly injured, and when you ask her, she hides the truth, telling you that she has fallen down and then her husband will start yelling. Later, when you separate them, the woman reveals, “Sister(nurse), this man has beaten me. (Midwife professional)
Comparisons by Profession and Experience
There were several key differences we observed across participants. First, on the issue of reporting the husband to the police, most experienced professionals stated they would report. However, most students disagreed about reporting the husband to the police. First, they stated they were unsure about whether a husband meets the legal definition of a perpetrator. Second, they feared reporting him might cause further marital discord. Third, when participants talked of the challenges encountered when handling an IPV case, students were less aware of mandated reporting and less informed about a health care provider’s obligation in violence-related cases. Fourth, more responses came from the health professionals than the students, presumably because they had more experience with such cases. Finally, compared to the midwives and nurses, the medical doctors were the professionals who raised the most concerns about the inadequacy of policies and absence of mandated reporting. This observation may be due to the frequent role medical doctors have in writing and/or signing off on the medical reports, forensic reports and any other medical documentation associated with legal issues. This role necessitates the doctors’ knowledge about policies and principles for optimal management of special cases including those involving violence and victimization.
Case 2: Management Approach and Challenges of a Rape Victim Brought in by Police
Clinical Care of the Rape Victim
All participants said, upon the victim’s arrival, a thorough assessment must be conducted to ensure that the victim does not have any impending signs of danger (ie, checking for injuries and/or bleeding). If there were any signs and symptoms of emergency, then participants stated their first duty was immediate assistance to medically stabilize the patient. While doing so, they stated the provider must maintain privacy, provide assurance to the victim of their safety during treatment, and establish rapport using effective communication.
“First of all, we carry out assessment and we shall manage if there is any risk of infection and bleeding. We stabilize the victim … ” (Nursing student)
Most participants agreed that once the victim is stabilized, a proper history should be taken detailing the event and previous medical history of the victim. A thorough physical examination must be performed and during this process it is important to consider gender equivalence between the victim and the health care provider to further enhance perceived safety by the patient. Thereafter, participants reported that the victim should undergo laboratory testing to diagnose any sexually transmitted infections, and possible pregnancy. Prior to testing, participants stated they would initiate pre-test counselling for HIV/STIs. Frequently, participants emphasized the collection of samples for forensic evidence including vaginal swab, DNA, sperm, pubic hair and clothes in order to have proof of penetration and to determine the identity of the perpetrator.
“So, the first thing is to take the victim’s information and if the patient’s condition is good then you just work on the forensic evidence.” (Midwife student)
As usual, start with history taking if brought by police then there is a PF3 already. You need to complete history and physical examination. If you do an examination and saw bruises and fluid there, you will probably tell maybe it is evidence … you do something called the rape kit am not sure if [Name of Hospital] has it but we are supposed to collect samples for rape kit. (Medical doctor)
Once the investigation is complete, participants stated that the victim should be provided with post-exposure prophylaxis to prevent HIV infection and emergency contraception for unwanted pregnancy if the patient is female. Then, they would proceed with medical treatment, depending on the physical findings as well as investigation results. In talking about treatment, participants included both medication and psychological intervention including initial counselling to the victim and provision of health education. Participants emphasized proper documentation in the victim file as important and that the file should contain copies of any forms from the police.
For me, like he has said, if she has everything, the first thing she will get is contraceptive but she would also get PEP [post-exposure prophylaxis to prevent HIV infection] but after, testing and counselling for HIV. (Midwife professional)
It depends on the time of the act. If time allows, we will give her PEP and emergency contraceptives. This will help to protect the victim from pregnancy and HIV. (Nursing student)
Participants mentioned three kinds of referral. First, participants emphasized the need to have a PF3 form brought in with the victim, or else the providers are required to follow up the case with the police and by involving the hospital’s Gender-Based Violence Desk so that the victim can be supported legally. However, if the victim was not brought in by the police, then the first referral participants emphasized was to the police station. Second, participants mentioned referral to a psychologist given the mental health consequences associated with the trauma of sexual violence for the victim. Third, participants mentioned referral to a social worker should be considered in order to facilitate the safety of the patient within her living environment.
A rape case and coming with police, it means it will be a GBV case, so after treatment and filling of PF3, we will be done with our work and refer back to police to find those responsible and also to social workers so that they take her to safety. (Midwife professional)
And this person, you may not discharge her home, you may have to refer her to the psychologist. This is the person that can help her to be stable so that she cannot get more effects. (Medical student)
Sometimes psychological treatment is important because the victim can undergo depression because of what happened. … I will refer to the psychologist. (Nurse student)
She was brought by the police so we must know the environment she comes from. Maybe there are groups of women who suffer or where will she go after treatment? … Then, social welfare will get involved to that case. (Nurse professional)
Practical Barriers
Participants described the obstacles they faced when handling a rape victim case. Several mentioned that rape kits were not available in their hospitals. While these kits were widely mentioned as scarce, health care providers also reported not knowing how to use them. Lack of knowledge included not knowing how to collect the sample, storage of the samples until their transfer to the required authorities, and which authorities ultimately stored the forensic evidence. Specifically, they wondered whether it was at the police or the Government Chemist Laboratory Agency.
We do not have those rape kits in our setting. We don’t know how to preserve them. They are not available, no training or where to bring them after you have collected. (Medical Doctor)
Participants reported that sometimes they are faced with additional dilemmas. The most difficult was when the rape victim conceives following a sexual assault. Participants stated caveats that referred to their personal morals and/or religious backgrounds. In such a scenario, participants reported they would find it difficult to decide how to help the victim considering that the victim may be very ambivalent regarding the pregnancy.
Also, in case of rape, sometime it might happen that the victim is pregnant. So, after the examination and you have confirmed that she has conceived, now I don’t know if she will decide to remain with it or otherwise. I am in dilemma. I would not know what to advise because abortion is not good, it is sinful. (Nursing Student)
Comparisons by Profession and Experience
The contributions made by the participants regarding the management of the rape case did not differ greatly from their management of the IPV case. Students appeared less familiar with the collection of forensic evidence and its processing. Students would offer comments that reflected what they thought should be done, but they had no idea whether rape kits were actually available in most health facilities, nor what to do after collecting the samples. Some professionals, particularly the medical doctors, appeared less aware about such resources being unavailable and the logistical difficulties around the whole process of handling forensic evidence.
Discussion
The aim of this qualitative study was to gain an in-depth understanding of health care providers’ knowledge and their clinical practices in relation to violence cases. Overall, while we had an equal distribution of provider and student participants, there were more female participants in the provider groups (likely due to midwifery and nursing being traditionally female-dominant professions) and more males in the student groups. Three core findings emerged from our study results: 1) Clinical care of IPV and rape victims, including initial and/or emergency responses, medical care and channels for referrals as primary; 2) Existing barriers to clinical practices when managing IPV or rape victims; and 3) Practical and clinical knowledge comparisons by profession and experience.
In this study, we wanted to examine current clinical practices of health care professionals in Tanzania when they encounter assault victims in their health care settings. Across both case studies, participants emphasized the importance of initial assessment and stabilizing the patient, in case of any medical emergency in order to save the life of a victim. Moreover, they recognized that any emergency care must be performed ethically and professionally by first obtaining informed consent or as soon as the victim is out of danger and is able to respond. These findings are similar to the published recommendations in Tanzania and with practices in addressing domestic violence in primary care setting in a Middle Eastern country.21,30 Usta et al described how to identify the survivor, initiate medical response, provide interim care and document the victim’s case notes.30
The participants in our study stressed the significance of the police form 3 (PF3) during the victim’s medical care. Tanzania currently uses the National Guideline for Gender-Based Violence and Violence Against Children Forensic Evidence Management which instructs medical practitioners, law enforcers, social welfare officers and prosecutors on the usefulness of the PF3 for assault cases. Participants emphasized handling the medical emergency first, then reporting and obtaining the PF3 from the police which is to be filled by the examining doctor, if it was not brought by or with the victim at the initial visit.21 According to Tanzanian GBV guidelines, the medical examination and sample collection from a victim of IPV and/or sexual violence must be done by a trained medical practitioner in forensics or a forensic expert, with the support of a police investigator who is also a custodian of forensic evidence at every step of the investigation and prosecution.21
Our study identified several similarities in the medical management of the two cases. These included assessment procedures, investigations, treatment and importance of gender resemblance between the provider and the victim. However, there were also some differences noted. One was the provision of preventive medications and collection of forensic evidence from the rape victim. Participants emphasized the need to provide emergency contraception and post-exposure prophylaxis for prevention of pregnancy and acquisition of HIV for those with negative baseline HIV testing respectively, within the recommended time frame after the assault. (Post-exposure prophylaxis is only medically recommended if taken within 72 hours of an exposure). This should also be offered to an IPV victim, whenever there is evidence of sexual assault. With respect to the rape victim, most participants discussed the importance of forensic investigation. They recognized their role includes to look for evidence and prove that a rape was committed so that it could facilitate capturing the perpetrator (or their exoneration). Examples of critical data mentioned by participants included evidence of penetration on clinical examination such as a torn hymen, bruises and tears around genitalia, physical evidence such as blood or semen stained clothes or objects, used condoms, scratches, DNA evidence and eye witness testimony. Overall, the practices participants raised were consistent with several of the recommended procedures from the national guidelines and WHO guidelines,21,31,32 and are similar to those reported in other parts of Africa and other low-income countries such as Papua New Guinea.33,34
Second, in discussing the IPV case, couple’s counselling was favored over individual counselling of the victim and/or the perpetrator. A meta-analysis shows couple’s counselling or therapy can be an effective treatment in certain situations among partners experiencing IPV.35 In other countries (eg, Papua New Guinea), individual counselling instead of couple’s counselling was recommended and having multiple sessions was found to be helpful.34 In Tanzania, our participants defaulted to couples’ counseling on the assumption that it was essential to preserve the couple’s relationship. Some participants expressed concern that involving the husband in couples’ counseling had the potential to exacerbate the violence in some cases.
The referrals participants considered were similar to those found in other low-income countries including Uganda, Ghana and Sri Lanka.11,33,36 The participants stressed the importance of making referrals to social, health, and legal services in order to provide comprehensive care to the victims. In addition, participants identified referral to extended family for support, involvement of spiritual/religious leaders for counseling and assistance from local government agencies as additional resources to referrals. Considering the strong cultural and religious backgrounds held by the majority of the population in Tanzania,37 most cases of IPV or rape where the perpetrator is a family member will be resolved at the family level. This is to avoid destroying the family’s reputation and to protect its honor.37 Others will seek pastoral counselling, perceiving the interpersonal violence or rape as more of a marital issue than a violence issue.11,38
This study identified several barriers and challenges faced by practitioners while attending to assault victims. System barriers included inadequate resources, insufficient training, as well as inadequate regulations and policies. At the individual level, some participants expressed statements showing personal conflict or potentially unprofessional conduct when approaching such cases. This included imposing their own personal values, for example cultural values that tolerate or normalize violence to women, judgmental assessment of some victims as being sinful or deserving of violence, and religious precepts against contraception that may narrow the options that are supposed to be offered to the victim seeking help. Other barriers such as delays by the victim in seeking help may impact both forensic evidence collection and what treatments can be offered (eg, HIV post-exposure prophylaxis). Studies in Brazil, Ghana, Angola and Tanzania11,15,37,39–41 report some of these same challenges, and the need for health care providers to adhere to professionalism and to evaluate their own feelings and beliefs towards these acts, in order to provide quality care to the survivors. Cultural beliefs of health care professionals should not impinge the medical care of IPV and/or rape victims. Additionally, in Tanzania, widespread social acceptance and normalization of IPV and/or non-partnered violence is commonly linked to cultural norms that promote male dominance and control over women. This and the fear that reporting the violence will lead to violence escalation or retaliation among the victims are the two reasons most survivors opt not to seek for help.37,42
The qualitative data from our study indicate that most health care providers have no or insufficient training on the clinical management for victims of rape and/or interpersonal violence. Most providers, and especially the students, were unclear about their ethical and legal responsibilities to these victims. This lack of training may be a regional problem as evidenced in studies from other parts of sub-Saharan Africa,11,12,33,43 and elsewhere.15,36,44,45 Across Africa, providers need training in how to treat both rape and IPV victims, when and how to refer, and the procedures in the collection and handling of forensic evidence. The existing national GBV protocols will have a significant impact on health care providers once they have received sufficient training.20,21
Collection of forensic evidence is a crucial procedure while managing a rape victim. It confirms the occurrence of the crime, exonerates possible suspects and establishes a link between the alleged perpetrator and the assault, for example using DNA evidence.21 In our case study, some experienced providers appeared unaware about the availability of rape kits, collection procedures including sample contamination, and its transportation. Studies in other parts of Africa have also reported poor healthcare provider knowledge of forensic evidence protocols including evidence collection11,12,15,33,43 and a shortage of specialized units for rape victims with reference to studies done in Kenya, Ghana and South Africa.11,46,47 These units act as “one stop centers” in managing assault survivors in a holistic approach, catering for victims’ physical and mental health as well as judicial and welfare needs.46,47 Therefore, such comprehensive training in the treatment of gender-based violence appears beneficial.16 Training programs should include the proper handling of forensic evidence, challenge negative attitudes and myths, improve knowledge on screening and identification of victims, optimize clinical care, referral and how to interact with other authorities involved in handling current victims or survivors.
Tanzania lacks a clear policy regarding mandated reporting of adult cases affected by violence, which may be why most participants in our study were unsure of their legal duties towards the victims. Other studies from Kenya and outside Africa report similar results.12,44 This law increases the chances of victim safety and it allows earlier detection of victims, providing necessary intervention and referral to other required services.18 However, such laws may also present some challenges for survivors, including a fear of seeking medical help if the information might be used by legal authorities to prosecute the perpetrator. An associated fear is that reporting will make the situation worse for the victim, either through increased aggression from the perpetrator, community stigma, or making other circumstances worse.19 Such policies can be beneficial to victims especially in the developing world, with caution that they do not result in violence retaliation or reduce help seeking efforts among victims.
In both case studies, student participants demonstrated little or inaccurate knowledge regarding the appropriate management of assault victims compared to the experienced providers. This confirms the need for such training to be included in health curriculums in Tanzania. In such training, students need to be taught both their legal duties and clinical protocols for management of violence-related cases.12,20,21 Such policies and guidelines should also be part of continuing education to experienced health professionals in order to reduce uncertainties when providing care to victims.
Our study had several limitations. Recruitment of professionals was limited to three hospitals all located in Dar es Salaam. These hospitals are not representative of healthcare across the whole nation. The victims presenting at these hospitals and hospital resources may differ from those in rural areas. Indeed, because service provision is likely to be much better in a large urban hospital, our results may represent a best-case scenario. Second, our study utilized a qualitative methodology so the results are not designed to be generalizable. Third, our study only collected information from health care providers and not the victims/survivors. Capturing information from the survivors would be important to confirm the patients’ experiences, services received, practitioners’ practices and the challenges the victims encounter in health settings. Fourth, because the experienced providers and students differed by gender, it is possible that differences attributed to experience may be explained, at least in part, by gender differences.
Conclusion
Intimate partner violence and rape are common in developing countries including Tanzania. This study identified barriers in clinical practice that may result in challenges or suboptimal health care for gender-based violence cases. Moreover, sociocultural dynamics may have a contribution towards escalation of IPV acts and rape. The key finding of this study was that many health providers and students are uncertain about how to manage cases of IPV and rape. Structural barriers identified included access to rape kits and lack of provider knowledge of proper procedures in collecting and preserving evidence. Based on these findings, we recommend support for the Tanzanian guidelines with interdisciplinary training for health professional students and continuing education opportunities for providers in practice. Such education will also benefit non-forensic health care professionals when managing patients from various levels of health care. Training in best clinical practice should address screening for abuse, clinical history taking, developing rapport through effective communication, cultural competence so the provider can effectively explore and address African-centric community norms, and training in how to use a rape kit. Moreover, it is necessary to have well-trained forensic experts including physicians and nurses within health facilities. Structurally, it is critical that resources including rape kits, medication for prevention of HIV acquisition and unwanted pregnancies are readily available. The national GBV guidelines and related policies should be implemented in order to avoid uncertainties among health care providers during clinical care provision and also by other stakeholders such as police, legal aids and social welfare. Further studies focusing on the victims’ experience of health care services might identify other gaps in care that need to be addressed for optimal treatment for GBV and rape.
Acknowledgments
We acknowledge, with thanks, the assistance of Muhimbili National Hospital, Mnazi Mmoja Hospital and Aga Khan Hospital in Dar es Salaam for help in recruiting the providers and on-site space to conduct the provider focus groups. We warmly acknowledge our beloved late colleague, Dr Sebalda Leshabari, PhD, who was a principal investigator on this study until her death on October 16, 2020.
Funding
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number R01HD092655. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Dr Maria Trent reports grants from the National Institutes of Health, during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. Organization WH. Developing sexual health programmes: a framework for action. World Health Organization; 2010. Available from: https://apps.who.int/iris/handle/10665/70501.
2. Organization WH. Sexual health and its linkages to reproductive health: an operational approach; 2017. Available from: https://www.who.int/reproductivehealth/publications/sexual_health/sh-linkages-rh/en/.
3. Organization WH. “World report on violence and health: summary”, Geneva (2002). World Health Organization, p v; 2002. Available from: https://www.who.int/violence_injury_prevention/violence/world_report/en/summary_en.pdf.
4. Organization WH. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and non-partner sexual violence. World Health Organization. 2013. Available from: https://apps.who.int/iris/handle/10665/85239.
5. García-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C WHO multi-country study on women’s health and domestic violence against women. World Health Organization. 2005. Available from: https://www.who.int/reproductivehealth/publications/violence/24159358X/en/.
6. Meek J, Brittain D, Dunnett K. The role of the HCA in sexual health services. Br J Healthcare Assist. 2014;8(10):489–495.
7. Müller A, Röhrs S, Hoffman-Wanderer Y, Moult K. “You have to make a judgment call”.--Morals, judgments and the provision of quality sexual and reproductive health services for adolescents in South Africa. Soc Sci Med. 2016;148:71–78. doi:10.1016/j.socscimed.2015.11.048
8. Ross MW, Leshabari S, Rosser BRS, et al. Evaluation of an assessment instrument for a sexual health curriculum for nurses and midwifery students in Tanzania: the sexual health education for professionals scale (SHEPS). Appl Nurs Res. 2018;40:152–156. doi:10.1016/j.apnr.2018.01.005
9. Canada CIaRBo. Tanzania: situation of female victims of domestic violence, including legislation and availability of state protection and support services (2012- July 2015); 26 August 2015. Available from: https://www.refworld.org/docid/55ffaa004.html.
10. Alli F, Maharaj P, Vawda MY. Interpersonal relations between health care workers and young clients: barriers to accessing sexual and reproductive health care. J Community Health. 2013;38(1):150–155. doi:10.1007/s10900-012-9595-3
11. Cannon LM, Sheridan-Fulton EC, Dankyi R, et al. Understanding the healthcare provider response to sexual violence in Ghana: a situational analysis. PLoS One. 2020;15(4):e0231644. doi:10.1371/journal.pone.0231644
12. Gatuguta A, Merrill KG, Colombini M, et al. Missed treatment opportunities and barriers to comprehensive treatment for sexual violence survivors in Kenya: a mixed methods study. BMC Public Health. 2018;18(1):769. doi:10.1186/s12889-018-5681-5
13. Zorjan S, Smrke U, Šprah L. The role of attitudes to, and the frequency of, domestic violence encounters in the healthcare professionals’ handling of domestic violence cases. Zdr Varst. 2017;56(3):166–171.
14. Laisser R, Nyström L, Emmelin M. Health-care workers’ attitudes and perceptions of intimate partner violence against women in Tanzania. Af J Midwifery Womens Health. 2014;8(1):28–35. doi:10.12968/ajmw.2014.8.1.28
15. Colombini M, Mayhew S, Ali SH, Shuib R, Watts C. “I feel it is not enough” Health providers’ perspectives on services for victims of intimate partner violence in Malaysia. BMC Health Serv Res. 2013;13(1):65. doi:10.1186/1472-6963-13-65
16. Abeid M, Muganyizi P, Mpembeni R, Darj E, Axemo P. Evaluation of a training program for health care workers to improve the quality of care for rape survivors: a quasi-experimental design study in Morogoro, Tanzania. Glob Health Action. 2016;9(1):31735. doi:10.3402/gha.v9.31735
17. Welfare TURoT-MoHaS. National policy guideline for the health sector prevention and response to gender – based violence (GBV). Welfare TURoT-MoHaS; September 2011. Available from: http://www.healthpolicyplus.com/archive/ns/pubs/hpi/Documents/1529_1_NATIONAL_POLICY_GUIDELINE.pdf.
18. Sachs CJ. Mandatory reporting of injuries inflicted by intimate partner violence. AMA J Ethics. 2007;9(12):842–845.
19. Lippy C, Jumarali SN, Nnawulezi NA, Williams EP, Burk C. The impact of mandatory reporting laws on survivors of intimate partner violence: intersectionality, help-seeking and the need for change. J Fam Violence. 2019;1–13.
20. Betron M Gender-based violence in Tanzania: an assessment of policies, services, and promising interventions. Health Policy Initiative, Task Order 1, Futures Group International. 2008; Retrieved from Library of Congress. Available from: https://www.loc.gov/item/2019352551.
21. The United Republic of Tanzania; Ministry of Health CD, Gender, Elderly and Children and Ministry of Home Affairs. National guideline for gender based violence and violence against children forensic evidence management: for medical practitioners, law enforcers, social welfare officers and prosecutors;2015.
22. Mamdani M, Bangser M. Poor people’s experiences of health services in Tanzania: a literature review. Reprod Health Matters. 2004;12(24):138–153. doi:10.1016/S0968-8080(04)24135-0
23. Kwesigabo G, Mwangu MA, Kakoko DC, et al. Tanzania’s health system and workforce crisis. J Public Health Policy. 2012;33(Suppl 1):S35–44. doi:10.1057/jphp.2012.55
24. Juma D, Manongi R. Users’ perceptions of outpatient quality of care in Kilosa District Hospital in central Tanzania. Tanzan J Health Res. 2009;11(4):196–204.
25. Krueger RA. Focus Groups: A Practical Guide for Applied Research. Sage publications; 2009.
26. Saldaña J The coding manual for qualitative researchers; 2009.
27. MacQueen KM, McLellan E, Kay K, Milstein B. Codebook development for team-based qualitative analysis. CAM J. 1998;10(2):31–36. doi:10.1177/1525822X980100020301
28. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
29. Given LM. The Sage Encyclopedia of Qualitative Research Methods. Sage publications; 2008.
30. Usta J, Taleb R. Addressing domestic violence in primary care: what the physician needs to know. Libyan J Med. 2014;9(1):23527. doi:10.3402/ljm.v9.23527
31. Organization WH. Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. World Health Organization; 2013. Available from: https://apps.who.int/iris/bitstream/handle/10665/85240/9789241548595_eng.pdf;jsessionid=7EB2D2007FA0E63C8F8BC4A4B7241497?sequence=1.
32. Organization WH. Clinical management of rape and intimate partner violence survivors: developing protocols for use in humanitarian settings; 2020. Available from: https://apps.who.int/iris/bitstream/handle/10665/331535/9789240001411-eng.pdf?ua=1.
33. Henttonen M, Watts C, Roberts B, Kaducu F, Borchert M. Health services for survivors of gender-based violence in northern Uganda: a qualitative study. Reprod Health Matters. 2008;16(31):122–131. doi:10.1016/S0968-8080(08)31353-6
34. Lokuge K, Verputten M, Ajakali M, et al. Health services for gender-based violence: médecins sans frontières experience caring for survivors in Urban Papua New Guinea. PLoS One. 2016;11(6):e0156813. doi:10.1371/journal.pone.0156813
35. Karakurt G, Whiting K, van Esch C, Bolen SD, Calabrese JR. Couples therapy for intimate partner violence: a systematic review and meta-analysis. J Marital Fam Ther. 2016;42(4):567–583. doi:10.1111/jmft.12178
36. Guruge S. Nurses’ role in caring for women experiencing intimate partner violence in the Sri Lankan context. Int Sch Res Notices. 2012;2012.
37. Abeid M, Muganyizi P, Olsson P, Darj E, Axemo P. Community perceptions of rape and child sexual abuse: a qualitative study in rural Tanzania. BMC Int Health Hum Rights. 2014;14(1):23. doi:10.1186/1472-698X-14-23
38. Sigalla GN, Mushi D, Gammeltoft T. “Staying for the children”: the role of natal relatives in supporting women experiencing intimate partner violence during pregnancy in northern Tanzania–A qualitative study. PLoS One. 2018;13(6):e0198098. doi:10.1371/journal.pone.0198098
39. Barros Lde A, Albuquerque MC, Gomes NP, Riscado JL, Araújo BR, Magalhães JR. [The (un)receptive experiences of female rape victims who seek healthcare services]. Rev Esc Enferm USP. 2015;49(2):193–200. doi:10.1590/S0080-623420150000200002. [Portugese]
40. Nascimento Ede F, Ribeiro AP, Souza ER. Perceptions and practices of Angolan health care professionals concerning intimate partner violence against women. Cad Saude Publica. 2014;30(6):1229–1238. doi:10.1590/0102-311X00103613
41. Muganyizi PS, Nyström L, Axemo P, Emmelin M. Managing in the contemporary world: rape victims’ and supporters’ experiences of barriers within the police and the health care system in Tanzania. J Interpers Violence. 2011;26(16):3187–3209. doi:10.1177/0886260510393006
42. McCleary-Sills J, Namy S, Nyoni J, et al. Stigma, shame and women’s limited agency in help-seeking for intimate partner violence. Glob Public Health. 2016;11(1–2):224–235. doi:10.1080/17441692.2015.1047391
43. Fouche L, Bezuidenhout J, Liebenberg C, Adefuye AO. Medico-legal documentation of rape or sexual assault: are community-service doctors equipped for the task? S Afr Fam Pract. 2018;60(1):46. doi:10.4102/safp.v60i1.4680
44. Acosta DF, Gomes VL, Oliveira DC, Gomes GC, Fonseca AD. Aspectos éticos e legais no cuidado de enfermagem às vítimas de violência doméstica. Texto Contexto-Enferm. 2017;26(3). doi:10.1590/0104-07072017006770015
45. Alshammari KF, McGarry J, Higginbottom GMA. Nurse education and understanding related to domestic violence and abuse against women: an integrative review of the literature. Nurs Open. 2018;5(3):237–253. doi:10.1002/nop2.133
46. Martin LJ. Forensic evidence collection for sexual assault: a South African perspective. Int J Gynaecol Obstet. 2002;78(Suppl 1):S105–110. doi:10.1016/S0020-7292(02)00054-1
47. Shako K, Kalsi M. Forensic observations and recommendations on sexual and gender based violence in Kenya. Forensic Sci Int Synerg. 2019;1:185–203. doi:10.1016/j.fsisyn.2019.06.001
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.