")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical Application of the Mycobacterium tuberculosis-RNA Assay of Pericardial Tissue Specimens in the Diagnosis of Tuberculous Pericarditis
Authors Zhang J, Bu C, Yao L , Xu K
Received 24 January 2023
Accepted for publication 14 March 2023
Published 30 March 2023 Volume 2023:16 Pages 1875—1883
DOI https://doi.org/10.2147/IDR.S405868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jinjuan Zhang,1 Caifang Bu,1 Liwei Yao,1,* Kan Xu2,*
1Department of Nursing, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Tuberculosis Diagnosis and Treatment Center, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liwei Yao, Department of Nursing, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, No. 208 East Huancheng Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected] Kan Xu, Zhejiang Tuberculosis Diagnosis and Treatment Center, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, No. 208 East Huancheng Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: To assess the accuracy of the Mycobacterium tuberculosis (MTB)-RNA assay using pericardial tissue specimens for tuberculous pericarditis (TBP) diagnosis.
Methods: MTB culture and MTB-RNA assay were performed for patients with suspected TBP. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC) of these two assays were analyzed.
Results: This study included 79 patients. The sensitivity, specificity, PPV, NPV, and AUC were 28.1% (18/64), 100.0% (15/15), 100.0% (18/18), 24.6% (15/61), and 0.64 for the MTB culture and 37.5% (24/64), 100.0% (15/15), 100.0% (24/24), 27.3% (15/55), and 0.69 for the MTB-RNA assay, respectively. Patients with positive pericardial tissue culture were defined as having definite TBP; in other words, culture was the gold standard for this group of patients and had a sensitivity, specificity, PPV, and NPV of 100% and an AUC of 1.00. However, these values were found to be 72.2% (13/18), 100.0% (15/15), 100.0% (13/13), 75.0% (15/20), and 0.86 for the MTB-RNA assay, respectively. Among patients with probable TBP (culture-negative patients), the sensitivity, specificity, NPV, and AUC of MTB culture were 0.0% (0/46), 100.0% (15/15), 24.6% (15/61), and 0.50, respectively, but the PPV could not be determined. These values were found to be 23.9% (11/46), 100.0% (15/15), 100.0% (11/11), 30.0% (15/50), and 0.62 for the MTB-RNA assay, respectively.
Conclusion: MTB-RNA assay using pericardial tissues had limited diagnostic efficacy for TBP. In culture-positive TBP, the diagnostic accuracy of MTB-RNA was good. In contrast, in culture-negative TBP, its diagnostic accuracy was unsatisfactory.
Keywords: tuberculous pericarditis, RNA, culture, polymerase chain reaction, accuracy
Introduction
Tuberculosis (TB), caused by Mycobacterium tuberculosis (MTB) infection, including pulmonary TB (PTB) and extrapulmonary TB (EPTB), is an ancient infectious disease that continues to pose a serious threat to human health even today.1 Tuberculous pericarditis (TBP) is a severe form of EPTB.2 Although TBP is uncommon, it can lead to serious complications, such as pericardial tamponade, pericardial constriction, and even death.3,4 Approximately 17–40% of patients with TBP die within 6 months of diagnosis.5,6 TBP is the leading cause of pericardial disease in areas with a high TB burden, particularly where human immunodeficiency virus (HIV) infection is prevalent.7,8 However, adverse events can be reduced with effective treatment, which is dependent on accurate diagnosis, which is still quite difficult in TBP.9 In early pericarditis with massive pericardial effusion, pericardial puncture can be performed to obtain a pericardial fluid specimen for adenosine deaminase (ADA) and other related tests.10 However, positive ADA test is not microbiological evidence, and septic infection or tumor can cause ADA levels to rise in the fluid, thereby leading to a misdiagnosis.11 When pericardial fluid is minimal or absent, it is difficult to identify the nature of the pericardial effusion, which makes the diagnosis more difficult. Even if pericardial fluid is obtained, conventional acid-fast bacilli (AFB) smear and culture of the fluid have limited diagnostic accuracy.12
Nucleic acid amplification tests (NAATs) are a mainstay in the diagnosis of infectious diseases, greatly improving the rate and shortening the time required for the establishment of infectious disease etiology, including TB.13,14 NAATs are also useful in TBP as they improve its diagnostic rate.15 Current NAATs are primarily tested using pericardial fluid, with few studies using pericardial tissue for testing.15,16 MTB-RNA assay is a TB detection test based on RNA detection developed by Shanghai Rendu Biotechnology Co.17 The test is widely used in China and has shown relatively satisfactory diagnostic results for PTB.18 The current applications in TBP diagnosis are all related to NAATs based on MTB-DNA detection, whereas NAATs based on RNA detection have not been reported in relevant studies. The diagnostic efficacy of MTB-RNA-based tests in TBP is unknown. Hence, this study aimed to assess the accuracy of the MTB-RNA assay using pericardial tissue specimens for TBP diagnosis.
Materials and Methods
Study Design
This retrospective study was conducted to evaluate the clinical application of the MTB-RNA assay using pericardial tissue for TBP diagnosis at the Zhejiang Province TB diagnosis and treatment center, a regional TB center in the Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine. From June 2019 to August 2022, inpatients who underwent pericardial dissection or pericardial biopsy to obtain pericardial tissue specimens were screened for suspected TBP, and MTB-RNA assay and culture were performed on the tissue specimens. Patients with hypothermia, night sweating, or other TB-related symptoms; pericardial effusion, pericardial thickening, or pericardial calcification; and positive TB-related immunological tests (such as TSPOT.TB) combined with PTB or other sites of TB were considered to have suspected TBP. Thoracoscopic pericardial biopsy was performed when the patient had pericardial effusion without pericardial constriction. We performed a pericardial biopsy by video-assisted thoracic surgery in the right lateral position, entered the thoracic cavity through the fifth intercostal space on the left side, lifted the apical pericardium and removed the apical part of the pericardium after making a small incision with scissors. Pericardial dissection was performed to obtain pericardial tissue when constrictive pericarditis developed. All patients or their guardians provided written informed consent to perform the relevant surgical procedure. Patients whose pericardial tissues were not obtained or tested or who were lost to follow-up were excluded.
The final clinical diagnosis was used as the gold standard for TBP diagnosis according to the guidelines of the European Society of Cardiology (ESC).19,20 A definite TBP was considered based on the presence of MTB in the pericardium using MTB culture. However, a probable TBP was considered when there were TB-related symptoms, pericardial calcification, a positive TB immunoassay, pericardial pathology suggesting granulomatous inflammation and caseous necrosis, positive molecular tests (such as Xpert MTB/RIF) on the pericardial tissue, and effective anti-TB treatment in areas with a high TB burden. A non-TBP was considered when there were no signs of MTB infection or definite pericardial diseases and no response to anti-TB therapy. Definite and probable TBP was considered the final clinical diagnosis of TBP.
All patients or their guardians provided written informed consent. The study protocol was approved by the Human Research Ethics Committee of the Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, and adhered to the Helsinki Declaration.
MTB Culture
MTB culture was performed on fresh pericardial tissues using solid and/or liquid culture methods. Tissue specimens were cut and ground, pretreated with N-acetyl-L-cysteine-sodium hydroxide (NaOH), 0.1 mL of the treated supernatant was taken and inoculated onto the medium, and then incubated in a thermostat at 37°C. Both solid and liquid cultures were used according to the manufacturer’s instructions.
MTB-RNA Assay
Fresh pericardial tissues were pretreated in the same way as cultured tissues. The decontaminated specimens were centrifuged at 13,000 ×g for 5 minutes, with the supernatant discarded and the sediment retained. The sediment was then mixed with 50 µL of the diluent and placed in an ultrasonic bath (Shanghai Shenyang Ultrasonic Machine, China) for 15 minutes. The treated mixture was centrifuged to obtain the supernatant, 2 μL of which was mixed with 30 μL of the reaction solution to obtain the mixed solution. It was then placed into a polymerase chain reaction (PCR) tube and incubated at 60°C for 10 minutes, followed by 42°C for 5 minutes. The incubated solution was then treated with 2000 units of T7 RNA polymerase (RD Bioscience, Inc., San Diego, CA, USA) and 2000 units of Moloney mouse leukemia virus reverse transcriptase. The final mixture was used for 16S rRNA amplification and analyzed using fluorescence quantitative real-time PCR (SLAN-96S real-time PCR system, Xiamen Zeshan Biotechnology Co., Ltd., Xiamen, China). Finally, the results were analyzed according to the product information manual.21
Data Processing and Statistical Analysis
The relevant data were recorded in Microsoft Excel 2019, and the mean, standard deviations, and proportions were calculated. The true positive (TP), false positive (FP), false negative (FN), and true negative (TN) values in the diagnostic four-compartment table were calculated using the Statistical Package for the Social Sciences, version 24.0 (IBM Corp., Armonk, NY, USA). The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the curve (AUC) with 95% confidence intervals (CIs) were calculated from the TP, FP, FN, and TN values for MTB-RNA assay and MTB culture using the MedCalc Statistical software, version 15.2.2 (MedCalc Software Bvba, Ostend, Belgium; http://www.medcalc.org). The final clinical diagnosis was the gold standard for TBP diagnosis. McNemar’s test was used to compare the differences between paired data, the chi-square test or Fisher’s exact test was used to compare the differences between proportions, and the Z-test was used to compare the differences between AUCs. A Venn diagram was created using an online interactive tool (http://www.bioinformatics.com.cn/static/others/jvenn/example.html). P-values of <0.05 were considered statistically significant.
Results
The electronic medical records of 90 patients who had undergone the relevant procedures to obtain the pericardial tissues were initially screened, and 11 patients whose pericardial tissues were not tested were excluded, leaving 79 patients in the study. Because none of the patients underwent secondary surgery, 79 pericardial tissue specimens were included. There were 50 (63.3%) men and 29 (36.7%) women in the study, ranging in age from 16 to 83 years, with a mean age of 58.8 ± 14.8 years. Only six (7.6%) patients had a positive AFB smear of pericardial tissues. There were no HIV-infected patients in the study. Twenty (25.3%) patients had concurrent PTB, and 11 (13.9%) had concurrent TB pleurisy.
Figure 1 depicts the patient screening process as well as the final diagnostic classification. Based on the final clinical diagnosis, the number of patients with definite TBP, probable TBP, and non-TBP was found to be 18 (22.8%), 46 (58.2%), and 15 (19.0%), respectively. The distribution and overlap of MTB-RNA- and culture-positive results are shown in Figure 2, with 13 (16.5%) specimens being positive for MTB-RNA assay and culture, 5 (6.3%) positive for culture only, and 11 (13.9%) positive for MTB-RNA assay only.
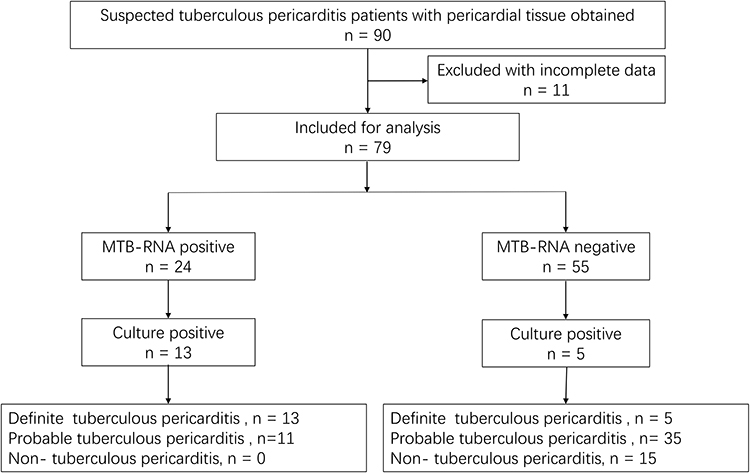 |
Figure 1 Patient screening process and the final diagnostic classification. |
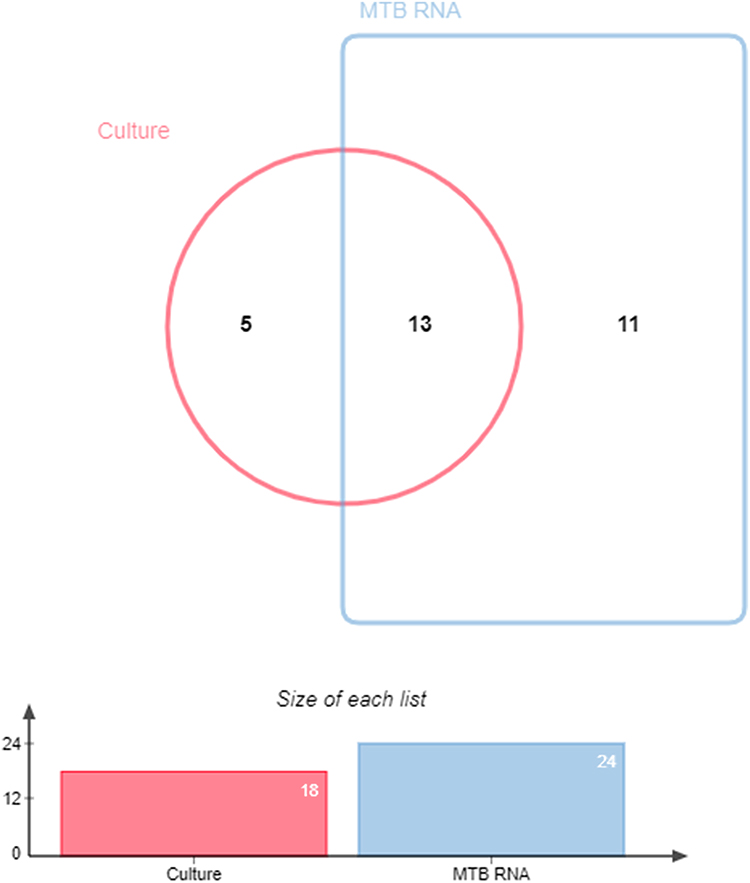 |
Figure 2 Venn diagram of MTB-RNA and culture-positive results in the included patients with tuberculous pericarditis. |
Diagnostic Accuracy of MTB Culture and MTB-RNA Assay
For all patients, the sensitivity, specificity, PPV, NPV, and AUC of the MTB culture were found to be 28.1% (18/64; 95% CI: 17.6–40.8%), 100.0% (15/15; 78.2–100.0%), 100.0% (18/18; 81.5–100.0%), 24.6% (15/61; 14.5–35.5%), and 0.64 (0.52%–0.75), respectively. The sensitivity, specificity, PPV, NPV, and AUC of the MTB-RNA assay were found to be 37.5% (24/64; 25.7–50.5%), 100.0% (15/15; 78.2–100.0%), 100.0% (24/24; 85.8–100.0%), 27.3% (15/55; 16.1–41.0%), and 0.69 (0.57–0.79), respectively. The receiver operating characteristic curve is presented in Figure 3A. In all patients, the accuracies of MTB culture and MTB-RNA assay for TBP diagnosis did not differ statistically (P > 0.05). The results are shown in Table 1.
 |
Table 1 Diagnostic Accuracy of MTB-RNA and MTB Culture for Tuberculous Pericarditis |
 |
Figure 3 The receiver operating characteristic curves for different diagnostic classifications, (A) all tuberculous pericarditis, (B) definite tuberculous pericarditis, (C) probable tuberculous pericarditis. |
In this study, patients with positive pericardial tissue culture were defined as having definite TBP; in other words, the MTB culture was the gold standard for this group of patients. Therefore, the culture had a sensitivity, specificity, PPV, and NPV of 100% and an AUC of 1.00. Accordingly, these values were found to be 72.2% (13/18; 46.5–90.3%), 100.0% (15/15; 78.2–100.0%), 100.0% (13/13; 75.3–100.0%), 75.0% (15/20; 50.9–91.3%), and 0.86 (0.70–0.96) for the MTB-RNA assay, respectively. The receiver operating characteristic curve for definite TBP is presented in Figure 3B. The accuracies of the MTB culture and MTB-RNA assay for definite TBP diagnosis differed statistically (P < 0.05; Table 1).
Among patients with probable TBP (culture-negative patients), the sensitivity, specificity, NPV, and AUC of culture were 0.0% (0/46; 0.0–7.6%), 100.0% (15/15; 78.2–100.0%), 24.6% (15/61; 14.5–37.3%), and 0.50 (0.37%–0.63), respectively, but the PPV could not be determined. Furthermore, these values were found to be 23.9% (11/46; 12.6–38.8%), 100.0% (15/15; 78.2–100.0%), 100.0% (11/11; 71.5–100.0%), 30.0% (15/50; 17.9–44.6%), and 0.62 (0.49–0.74) for the MTB-RNA assay, respectively. The receiver operating characteristic curve for probable TBP is presented in Figure 3C. The accuracies of the MTB culture and MTB-RNA assay for probable TBP diagnosis did not differ statistically (P > 0.05; Table 1).
Discussion
Because of the severity of TBP and the high incidence of adverse outcomes, clinicians have been working to improve the treatment and prognosis.22 The majority of cases with poor prognoses are due to delayed diagnosis, and effectively diagnosing TBP is the clinical focus.23,24 The diagnosis of patients without pericardial effusion is more difficult than that of patients with adequate pericardial effusion and usually necessitates invasive procedures to obtain specimens.19 The microbiological diagnosis remains the most critical aspect of TBP diagnosis, with the AFB smear and MTB culture still being the most classical microbiological tests for TB diagnosis.19,25 Although they have their own advantages, the disadvantages cannot be ignored. The AFB smear plays a limited role in EPTB diagnosis.26 In the present study, only six pericardial tissue specimens were positive for the AFB smear, which indicates the minor role of the AFB smear in TBP diagnosis. This finding is consistent with previous studies that used either pericardial effusion or pericardial tissue testing.19,25 A study using pericardial effusion to diagnose TBP found that AFB smear were negative in all 40 pericardial effusion specimens.25 Another study using pericardial tissues observed that AFB smear were positive in only 4 of 69 pericardial tissues.19 These findings suggested that the role of AFB smear in TBP diagnosis is limited. Hence, in this study, we did not compare its results with molecular assay results.
MTB culture is essential for TB diagnosis and must be performed for all patients with suspected TB.27 In this study, 18 tissue specimens were positive for MTB culture, and its sensitivity, specificity, PPV, NPV, and AUC for all TBP diagnosis were 28.1%, 100.0%, 100.0%, 24.6%, and 0.64, respectively. Notably, the sensitivity of MTB culture using pericardial tissue was unsatisfactory, which may be due to the nature of the tissue specimen. The tissue is difficult to purify adequately, and the MTB load in the dense connective tissue may be very low.19 Studies using tissue specimens for diagnostic purposes are limited, and our findings are consistent with those of previous studies.16,19 Similar results were obtained using pericardial effusion,25 which implies that culture positivity is similar between pericardial effusion and tissue. However, no head-to-head studies have been conducted to confirm this finding, and prospective large sample size studies are needed to further confirm these results. On the contrary, obtaining culture results takes several weeks, which is unsuitable for some critical patients with TBP.
The use of NAATs in TBP diagnosis is gradually increasing but remains primarily focused on pericardial effusions.28,29 The accuracy of Xpert MTB/RIF in TBP diagnosis in pericardial effusions is moderate, and it can be recommended as a method for rapid TBP diagnosis.30 In pericardial tissues, NAATs are still indicated.16 The tests currently used for TBP diagnosis are DNA-based tests,29 and there have been no studies on the role of RNA-based tests in TBP diagnosis, which is the purpose of our study. Our results revealed that the sensitivity, specificity, PPV, NPV, and AUC of the MTB-RNA assay for TBP diagnosis were 37.5%, 100%, 100%, 27.3%, and 0.69, respectively, when pericardial tissues were used for the assay. However, the sensitivity of the MTB-RNA assay for TBP diagnosis is limited and lower than that of the DNA-based assay. A previous meta-analysis found that the sensitivity, specificity, and AUC of the Xpert MTB/RIF assay using pericardial effusion were 65%, 99%, and 0.99, respectively, when compared with the composite reference standard and 75%, 99%, and 0.94, respectively, when compared with culture.31 The sensitivity of DNA-based assays for TBP diagnosis using tissue specimens ranged from 50.9% to 52.7% when compared with clinical diagnosis.19 The low sensitivity of the MTB-RNA assay may be due to the low and uneven distribution of MTB in the tissues as well as the poor stability of RNA in comparison with DNA.17 Due to the limited number of samples included in this study and the even more limited number of samples in which both MTB DNA and RNA-based assays were performed, comparisons of small samples may not accurately reflect differences between the relevant tests and therefore relevant head-to-head comparisons were not performed in this study. Relevant results will require prospective large sample studies to further confirm.
Overall, the diagnostic accuracy of the MTB-RNA assay was slightly higher than that of the culture, with no statistically significant difference. The very high PPV and very low NPV of the culture suggest that the probability of TBP is very high if these tests are positive, whereas negative results do not effectively exclude the possibility of the disease. Other relevant tests need to be performed for further clarification. The diagnostic accuracy of the MTB-RNA assay increased substantially in culture-positive patients, ie, those with definite TBP, indicating that its role in culture-positive patients is significant. However, the overall benefit is limited due to the low rate of culture positivity in the pericardial tissue. The MTB culture is limited in EPTB diagnosis because the MTB load in most EPTB specimens is very low, which limits the positive culture rate. The final clinical diagnosis combines multiple factors, including culture, and is a more appropriate reference standard for EPTB.16 Evaluation based on these two reference standards provides a more reliable interval of accuracy for the MTB-RNA assay in TBP diagnosis. In probable TBP, MTB culture has no diagnostic role, and the diagnostic role of the MTB-RNA assay is also limited, with a sensitivity of only 23.9%. In this study, the vast majority of patients had probable TBP, and more research is needed to improve the diagnostic accuracy in this group of patients. It is clear that the MTB-RNA assay may not meet these needs. Other validated tests should be developed to meet the diagnostic needs of this patient population.
This study had some limitations. First, because this is not a continuous prospective study, patient selection may be biased; for example, some patients required surgery but did not undergo it to obtain the tissue. Second, the results were not compared head-to-head with DNA-based tests, and some results might have been biased. Third, TBP is a relatively rare form of EPTB, and therefore, the overall sample size included is limited. Sample size limitations may also lead to biased results, and the associated results are still to be treated with caution. Finally, because this study was conducted in an area with a high TB burden, its relevance to other areas may be limited.
Conclusions
Overall, the sensitivity of MTB-RNA for the diagnosis of TBP using tissue specimens was relatively low, while the specificity was excellent (100.0%) and the overall diagnostic accuracy was limited. In culture-positive TBP patients, the sensitivity of MTB-RNA was satisfactory and its diagnostic accuracy was good. In culture-negative patients, the sensitivity of this test was low and its diagnostic accuracy was unsatisfactory.
Data Sharing Statement
Data will be made available on reasonable request.
Ethics Approval and Consent to Participate
All patients or their guardians gave written informed consent and the protocol of this study was approved by the Human Research Ethics Committee of Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine. This study complies with the Declaration of Helsinki.
Acknowledgments
We are grateful to all the patients and their families who were included, and also to our colleagues at the hospital for their help.
Funding
Liwei Yao, 2022ZB266, Administration of Traditional Chinese Medicine of Zhejiang Province. The funder does not have a role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2022. World Health Organization; 2022.
2. Pasipanodya JG, Mubanga M, Ntsekhe M, et al. Tuberculous pericarditis is multibacillary and bacterial burden drives high mortality. EBioMedicine. 2015;2(11):1634–1639. doi:10.1016/j.ebiom.2015.09.034
3. Wiysonge CS, Ntsekhe M, Thabane L, et al. Interventions for treating tuberculous pericarditis. Cochrane Database Syst Rev. 2017;9(9):Cd000526. doi:10.1002/14651858.CD000526.pub2
4. Naicker K, Ntsekhe M. Tuberculous pericardial disease: a focused update on diagnosis, therapy and prevention of complications. Cardiovasc Diagn Ther. 2020;10(2):289–295. doi:10.21037/cdt.2019.09.20
5. Mayosi BM, Wiysonge CS, Ntsekhe M, et al. Mortality in patients treated for tuberculous pericarditis in sub-Saharan Africa. S Afr Med J. 2008;98(1):36–40.
6. Syed FF, Mayosi BM. A modern approach to tuberculous pericarditis. Prog Cardiovasc Dis. 2007;50(3):218–236. doi:10.1016/j.pcad.2007.03.002
7. Hu X, Xing B, Wang W, et al. Diagnostic values of Xpert MTB/RIF, T-SPOT.TB and adenosine deaminase for HIV-negative tuberculous pericarditis in a high burden setting: a prospective observational study. Sci Rep. 2020;10(1):16325. doi:10.1038/s41598-020-73220-y
8. Naidoo DP, Laurence G, Sartorius B, Ponnusamy S. The effects of HIV/AIDS on the clinical profile and outcomes post pericardiectomy of patients with constrictive pericarditis: a retrospective review. Cardiovasc J Afr. 2019;30(5):251–257. doi:10.5830/CVJA-2019-015
9. Das KM, Mansoori TA, Alattar YH, et al. Tuberculosis of the heart: a diagnostic challenge. Tomography. 2022;8(4):1649–1665. doi:10.3390/tomography8040137
10. Dybowska M, Szturmowicz M, Błasińska K, et al. Large pericardial effusion-diagnostic and therapeutic options, with a special attention to the role of prolonged pericardial fluid drainage. Diagnostics. 2022;12(6):1453. doi:10.3390/diagnostics12061453
11. Ge YL, Liu CH, Zhang Q, et al. Normal tumor markers and increased adenosine deaminase in pericardial effusion misdiagnosed as tuberculous pericarditis ultimately proven as lung adenocarcinoma with pericardial metastasis: a case report and literature review. Clin Lab. 2019;65(5). doi:10.7754/Clin.Lab.2018.181036
12. Dybowska M, Błasińska K, Gątarek J, et al. Tuberculous pericarditis-own experiences and recent recommendations. Diagnostics. 2022;12(3):619. doi:10.3390/diagnostics12030619
13. Ali GA, Goravey W, Howady FS, et al. The role of post-bronchoscopy sputum examination in screening for active tuberculosis. Trop Med Infect Dis. 2022;8(1). doi:10.3390/tropicalmed8010013
14. Lee JH, Garg T, Lee J, et al. Impact of molecular diagnostic tests on diagnostic and treatment delays in tuberculosis: a systematic review and meta-analysis. BMC Infect Dis. 2022;22(1):940. doi:10.1186/s12879-022-07855-9
15. Saeed M, Ahmad M, Iram S, Riaz S, Akhtar M, Aslam M. GeneXpert technology. A breakthrough for the diagnosis of tuberculous pericarditis and pleuritis in less than 2 hours. Saudi Med J. 2017;38(7):699–705. doi:10.15537/smj.2017.7.17694
16. Yu G, Ye B, Chen D, et al. Comparison between the diagnostic validities of Xpert MTB/RIF and interferon-γ release assays for tuberculous pericarditis using pericardial tissue. PLoS One. 2017;12(12):e0188704. doi:10.1371/journal.pone.0188704
17. Yu G, Lin T, Yu Y, et al. Application of Mycobacterium tuberculosis RNA for the rapid diagnosis of lymph node tuberculosis using different specimens. Infect Drug Resist. 2023;16:179–187. doi:10.2147/IDR.S392045
18. Qiu X, Zheng S, Yang J, Yu G, Ye Y. Comparing Mycobacterium tuberculosis RNA accuracy in various respiratory specimens for the rapid diagnosis of pulmonary tuberculosis. Infect Drug Resist. 2022;15:4195–4202. doi:10.2147/IDR.S374826
19. Yu G, Zhong F, Zhao W, Ye B, Xu K, Chen G. Head-to-head comparison of the diagnostic value of five tests for constrictive tuberculous pericarditis: five tests for constrictive TBP. Int J Infect Dis. 2022;120:25–32. doi:10.1016/j.ijid.2022.04.018
20. Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) Endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921–2964. doi:10.1093/eurheartj/ehv318
21. Yan L, Xiao H, Zhang Q. Using simultaneous amplification and testing method for evaluating the treatment outcome of pulmonary tuberculosis. BMC Infect Dis. 2018;18(1):512. doi:10.1186/s12879-018-3424-y
22. Noubiap JJ, Agbor VN, Ndoadoumgue AL, et al. Epidemiology of pericardial diseases in Africa: a systematic scoping review. Heart. 2019;105(3):180–188. doi:10.1136/heartjnl-2018-313922
23. Porta-Sánchez A, Sagristà-Sauleda J, Ferreira-González I, Torrents-Fernández A, Roca-Luque I, García-Dorado D. Constrictive pericarditis: etiologic spectrum, patterns of clinical presentation, prognostic factors, and long-term follow-up. Rev Esp Cardiol. 2015;68(12):1092–1100. doi:10.1016/j.recesp.2014.12.019
24. Fang L, Yu G, Ye B, Zhong F, Chen G. The optimal duration of anti-tuberculous therapy before pericardiectomy in constrictive tuberculous pericarditis. J Cardiothorac Surg. 2021;16(1):313. doi:10.1186/s13019-021-01691-9
25. Yu G, Wang L, Shen Y, et al. Comparison of the diagnostic accuracy of Xpert MTB/RIF and CapitalBio Mycobacterium RT-PCR detection assay for tuberculous pericarditis. Infect Drug Resist. 2022;15:2127–2135. doi:10.2147/IDR.S360064
26. Nishal N, Arjun P, Arjun R, Ameer KA, Nair S, Mohan A. Diagnostic yield of CBNAAT in the diagnosis of extrapulmonary tuberculosis: a prospective observational study. Lung India. 2022;39(5):443–448. doi:10.4103/lungindia.lungindia_165_22
27. Rao PD, Devi DRG, Gouri SRM, Arjun AS, Krishnappa L, Azeem A. Evaluation of immunohistochemistry technique for diagnosis of extrapulmonary tuberculosis in biopsy tissue specimen as compared to composite diagnostic criteria. J Glob Infect Dis. 2022;14(4):136–141. doi:10.4103/jgid.jgid_112_22
28. Ullah I, Javaid A, Masud H, et al. Rapid detection of Mycobacterium tuberculosis and rifampicin resistance in extrapulmonary tuberculosis and sputum smear-negative pulmonary suspects using Xpert MTB/RIF. J Med Microbiol. 2017;66(4):412–418. doi:10.1099/jmm.0.000449
29. Yu G, Shen Y, Ye B, Chen D, Xu K. Comparison of CapitalBio™ Mycobacterium nucleic acid detection test and Xpert MTB/RIF assay for rapid diagnosis of extrapulmonary tuberculosis. J Microbiol Methods. 2020;168:105780. doi:10.1016/j.mimet.2019.105780
30. García P, Balcells ME, Castillo C, et al. Evaluación de la técnica Xpert® MTB/RIF para la detección de Mycobacterium tuberculosis complex en muestras extra-pulmonares [Evaluation of Xpert® MTB/RIF technique for Mycobacterium tuberculosis complex detection in extra-respiratory specimens]. Rev Chilena Infectol. 2017;34(4):333–339. Spanish. doi:10.4067/s0716-10182017000400333
31. Yu G, Zhong F, Shen Y, Zheng H, Quinn F. Diagnostic accuracy of the Xpert MTB/RIF assay for tuberculous pericarditis: a systematic review and meta-analysis. PLoS One. 2021;16(9):e0257220. doi:10.1371/journal.pone.0257220
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.