")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Clinical Application of Metformin Use in Anhui Province, China: A Cross-Sectional Study
Authors Chen L , Chen Q, Chen X, Zhu P, Chen M, Wang W, Ye S, Zheng M
Received 22 November 2022
Accepted for publication 9 January 2023
Published 6 February 2023 Volume 2023:16 Pages 345—354
DOI https://doi.org/10.2147/JMDH.S397061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Li Chen,1,* Qin Chen,2 Xueping Chen,3,4 Pengli Zhu,5 Meinan Chen,6 Wei Wang,7,8 Shandong Ye,7,8 Mao Zheng7,8,*
1Department of Endocrinology, The Third Affiliated Hospital of Anhui Medical University (The First People’s Hospital of Hefei City), Hefei, People’s Republic of China; 2Department of Pharmacy, Taihe County People’s Hospital, Taihe, People’s Republic of China; 3Department of Pharmacy, Hefei Fourth People’s Hospital, Hefei, People’s Republic of China; 4Psychopharmacology Research Laboratory, Anhui Mental Health Center and Department of Pharmacy, Affiliated Psychological Hospital of Anhui Medical University, Hefei, People’s Republic of China; 5Department of Pharmacy, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China; 6Ethics Committee on Medical Research, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China; 7Department of Endocrinology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China; 8Laboratory of Diabetes, Department of Endocrinology, The First Affiliated Hospital of USTC, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shandong Ye; Mao Zheng, Department of Endocrinology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, Anhui, 230001, People’s Republic of China, Tel +86 189 6378 9135 ; +86 13215603125, Fax +86 0551-62283524, Email [email protected]; [email protected]
Purpose: Given the importance of metformin, reasonable utilization is essential. We designed a cross-sectional survey on physicians’ attitude and clinical application of metformin in Anhui Province, China.
Methods: The survey was distributed via an electronic questionnaire among endocrinologists and general practitioners. Seven representative questions were used to evaluate professional levels.
Results: Among the 477 valid responses, 72.75% of the respondents preferred to prescribe metformin extended-release, while only 34.38% of them would prescribe metformin extended-release at the correct frequency. More than half of the respondents thought that estimated glomerular filtration rate ˂ 45 mL/min/1.73 m² should be the contraindication of metformin prescription. Less than 10% of the physicians selected correct responses for two questions regarding metformin usage and contrast agent. Physicians with higher levels of hospital grades, education background and professional titles as well as working in general hospitals and in the Department of Endocrinology achieved high scores (P˂0.05). Logistic regression showed that department was an independent predictor for high scores.
Conclusion: Physicians, especially non-endocrinologists, are not at a professional level for prescribing metformin. Physicians should be highly vigilant in terms of standardized prescription for metformin. The guidelines or consensuses about diabetes care for physicians should be promoted.
Keywords: metformin, professional knowledge, clinical application, diabetes mellitus, physicians
Introduction
Prevention and control of diabetes mellitus (DM) is becoming a serious challenge for doctors worldwide due to the rapid and sustained growth of DM prevalence in recent decades. According to the latest International Diabetes Federation Diabetes Atlas, an estimated 537 million people were diagnosed with DM worldwide in 2021, and if the current trends continue, 783 million adults are predicted to have DM by 2045.1 At present, although many new hypoglycemic agents, such as dipeptidyl peptidase-4 inhibitors, sodium glucose cotransporter 2 inhibitors and glucagon like peptide-1 (GLP-1) agonists, have been emerging in the medical market, metformin (Met) is considered the first-line therapy in patients with type 2 diabetes mellitus (T2DM).2,3 Recent studies reported that Met was still commonly used as antidiabetic drugs in patients with T2DM both among inpatients and outpatients.4–7The National Diabetes Prevention Program (DPP) recommended Met to be used for prevention of T2DM, and Met use has substantially increased in patients with prediabetes.8–10 Therefore, the full understanding of Met is essential for a clinician to provide appropriate prescription and instruction. We tried to search the relevant literature of Met’s application in PubMed database and only a few surveys have been performed to investigate the attitudes toward Met use in clinical practice among clinicians. An investigation of the knowledge, attitude and practice (KAP) of Met extended-release (Met-XR) among clinicians in Sichuan Province was conducted by the team of Professor Sheyu LI from West China Hospital.11 They concluded that the clinicians needed sufficient knowledge to assist their clinical decision-making when prescribing metformin XR. Tamkeen et al reported less than half of medical students had correct answers on the item measuring effectiveness of Met in a lifestyle change program.12 However, to the best of our knowledge, there was no survey in the available literature, which fully investigated the clinical practice of different pharmaceutical dosage forms of Met used for patients with various comorbidities (eg: dysfunction of major organs, tumors) as well as special populations (eg: children or adolescents, pregnant women, elderly people) among the clinicians. Here, a cross-sectional survey was conducted to evaluate the attitude and clinical application of physicians regarding Met use in Anhui Province, China. We tried to get more knowledge of clinicians’ attitudes toward and application of Met use, and also to evaluate the expertise levels of all the respondents.
Methods
Respondents and Sample Size Calculation
The cross-sectional survey was conducted via an electronic questionnaire between June 8 and September 23, 2021. All eligible participants were required to meet the following conditions: 1) obtained qualification for practicing doctors of P.R. China; 2) currently practicing in different levels of registered health care institutes in Anhui Province; 3) diagnosed and treated at least 10 patients with DM per month in the past 6 months; and 4) volunteered to take part in the survey.
A formula sample size calculator was used to calculate the sample size (https://www.calculator.net/sample-size-calculator.html).11 More than 385 respondents were needed for the present study, and 496 respondents were included at the end of the survey with an estimated margin of error of 4.4% and a confidence level of 95%.
Survey Development and Distribution
The questionnaire was designed by a multidisciplinary team, including clinical endocrinologists, clinical pharmacists and statisticians. Survey questions were developed for this study by researchers based on guidelines or expert consensuses of diabetic care and clinical use of Met both in China and abroad.2,3,13–15 An online version of the questionnaire was created using the WJX.cn survey platform. The questionnaire was sent using a two-dimensional code, and WeChat social media was used for dissemination of the survey and to invite physicians from all grades of hospitals in Anhui Province to complete the survey. All respondents filled in the questionnaire anonymously, and the results were collected by the WJX.cn background.
The questionnaire consisted of 27 questions and required approximately 10 min to complete. The questionnaire comprised the following three parts: 1) demographic information of all the respondents, including gender, years of practice, education background, professional titles, hospital grades, hospital categories and departments; 2) assessment of the attitude and clinical application of the physicians regarding Met using multiple-choice or true/false questions (see Appendix 1); and 3) evaluation of the professional level of the respondents prescribing Met in their clinical work. Seven representative questions were determined by the researchers (see Appendix 2), and the total scores of correct responses were calculated (1 point score for each question). Respondents with high scores (≥5 points) were considered to have good professional knowledge.
Ethics
All the respondents were informed about the intention of this research and that their personal information would be collected and used with confidential protection. The respondents were also informed how their responses would be analyzed. Informed consent from the respondent was obtained through checking a box at the beginning of the questionnaire. This investigation adhered to the tenets of the Declaration of Helsinki. Because no medications were prescribed and no interventions were performed, ethical approval was not required, and exemption was granted by Ethics Committee of the The First Affiliated Hospital of USTC (No. 2022-ky393).
Data Analysis
Qualitative data are presented as frequencies and percentages. Subgroup analysis for the professional level in the third part included gender, professional titles, education background, departments, hospital grades, hospital categories and years of practice. The differences between the two subgroups were compared by the Chi-square test. The independent factors that impacted the scores of correct responses were evaluated by multivariate logistic regression. P˂0.05 was considered statistically significant. SPSS statistical software version 21.0 was used for all statistical analyses.
Results
Response Rate and Demographic Information of Respondents
There were 496 respondents who volunteered to participate in the survey, and 19 respondents who never prescribed Met were not included in the final analysis, resulting in 477 valid respondents with an estimated response rate of 96.17%. Table 1 shows the demographic characteristics of respondents. Among the respondents, 66.25% had a professional title of Primary or Intermediate, and 33.75% were senior physicians. In addition, 36.48% of the respondents had a Master’s degree or above, while 63.52% of the respondents had a Bachelor’s degree or below. Most of the participants (85.53%) practiced in general hospitals, and 59.33% of the physicians served in tertiary hospitals.
 |
Table 1 Demographic Characteristics of the Survey Respondents (n=477) |
Attitudes Toward Met
The physicians’ attitudes toward Met are described and summarized in Table 2. The particular concerns, such as the indications of Met, special populations, considerations of prescription, supplementation of vitamin B12 (VitB12) and gastrointestinal (GI) reaction, were investigated among all the respondents.
 |
Table 2 Physicians’ Attitude toward Met |
Pharmaceutical Dosage Form, Frequency and Dose of Met Use
As shown in Table 3, the preference of pharmaceutical dosage form, the frequency of prescription, the initial dose, maintenance dose as well as the maximum dose of Met use were investigated. More than 70% of the respondents preferred to prescribe Met-XR, while only 34.38% of the respondents prescribed Met-XR quaque die (QD). Among the physicians, 78.20% considered 500–1000 mg/d as the initial dose of Met, 66.25% considered 1000–1500 mg/d as the maintenance dose, and 69.18% considered 1500–2000 mg/d as the maximum dose in their daily work.
 |
Table 3 Pharmaceutical Dosage Form, Frequency and Dose of Met |
Application of Met in Different Comorbidities
As shown in Figure 1, 70.86%, 48.22%, and 19.50% of the physicians prescribed Met for patients with cancer, chronic obstructive pulmonary disease and severe infections, respectively. Approximately 80% of the respondents considered that Met should not be used in patients undergoing major surgery.
 |
Figure 1 Application of Met in different comorbidities. |
Professional Knowledge Toward Met
The correct responses of seven representative questions (Appendix 2) were calculated to evaluate the professional knowledge of the respondents regarding Met prescription. As shown in Figure 2, most of the respondents considered that long-term use of Met does not cause impaired renal function (86.16%), hepatic function (85.95%) or heart failure (91.19%). Only half of the participants had good knowledge of the contraindications of Met. For the question, “To which extent of renal damage is Met prescription contraindicated?”, 53.88% of participants thought that glomerular filtration rate (eGFR) of 45 mL/min/1.73 m² should be the upper limit of Met usage. For the question, “To which extent of hepatic impairment is Met prescription contraindicated?”, 42.98% of participants selected “serum transaminase reaching more than 3 times the normal upper limit” as the correct answer. Most participants were unclear how to prescribe Met before using contrast agent. Only 8.18% participants indicated that they would discontinue Met just before using contrast agent, at the time of the scan when the eGFR was ˃60 mL/min/1.73 m2 or 48 h before using contrast agent when the eGFR was 45–59 mL/min/1.73 m2. Over half of the physicians (58.70%) considered that Met should be continued 48 h after using contrast agent if there is no exacerbation of renal function.
 |
Figure 2 The accuracy of answers to 7 representative questions. |
Participants’ Characteristics Associated with Professional Knowledge Toward Met
The demographic characteristics associated with professional knowledge toward Met were analyzed (Table 4). The respondents were stratified into different groups based on gender, professional titles, departments, hospital categories, education background, years of practice, and hospital grades. The physicians with senior professional titles or highly educated, or those serving in general hospitals, or in tertiary hospitals, as well as those in the Department of Endocrinology achieved high scores.
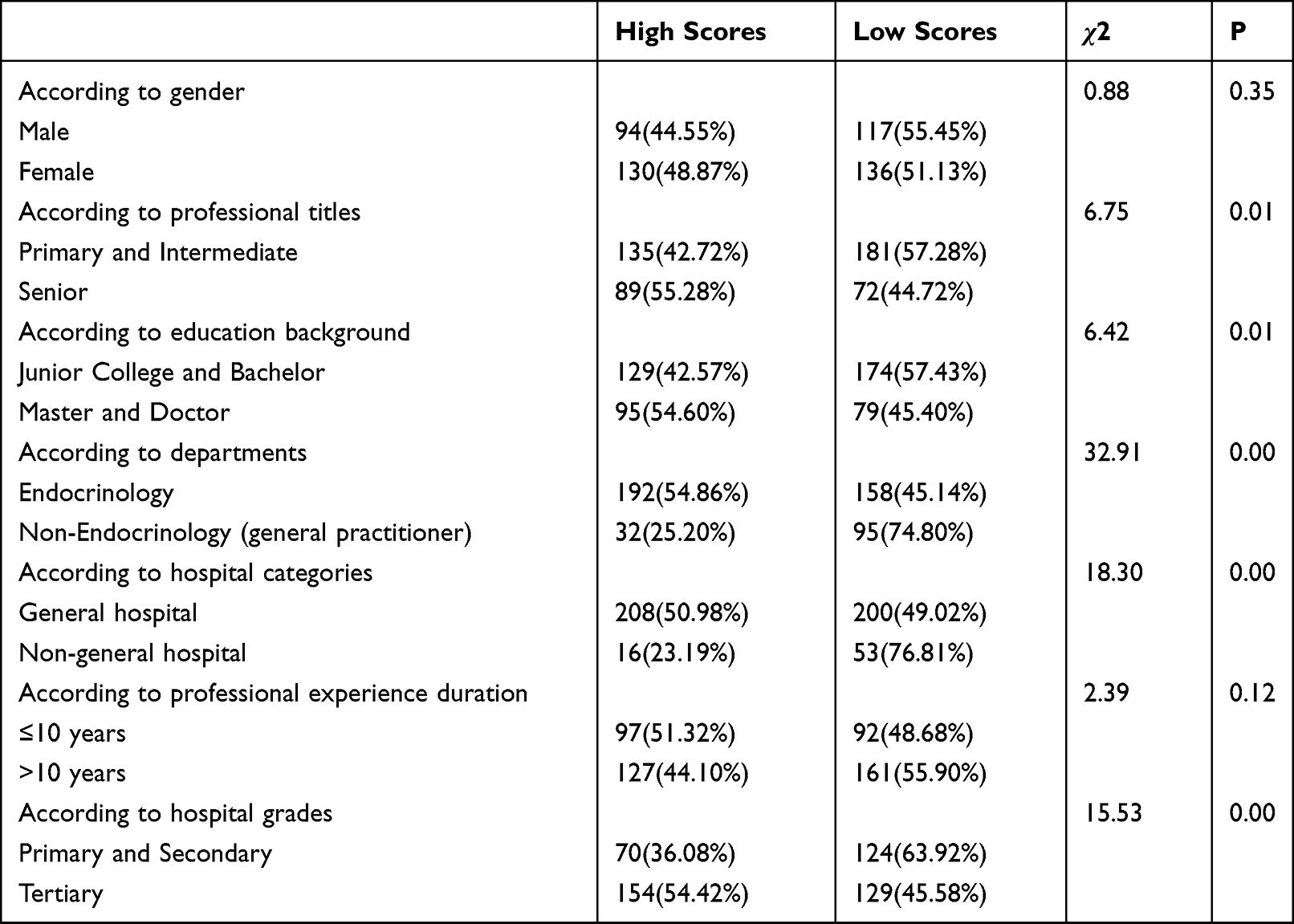 |
Table 4 Comparison of Correct Responses of the Physicians According to Different Grouping Methods |
Whether the respondents received high scores and the relevant single factors were input into a logistic regression equation as dependent and independent variables, respectively. The result showed that working in Department of Endocrinology was the independent predictor for high expertise level (OR=2.64, 95% confidence interval (CI) 1.53–4.57, P=0.00) (Figure 3).
 |
Figure 3 Logistic regression results of variables that affect the scores of respondents. |
Discussion
Most surveys of Met were conducted among patients diagnosed with T2DM or clinical pharmacists,16–18 only a few surveys were performed to get knowledge of the KAP regarding Met in clinicians.11 At present, clinicians mainly discharge the prescription in China healthcare industry. Therefore, in view of the first-line status of Met, being fully aware of the KAP of Met among clinicians is essential. Liu et al designed a complete questionnaire of KAP among clinicians in Sichuan Province regarding Met-XR.11 However, so far there has been no survey in the available literature reporting the complicated application situation of Met (including the different dosage forms, special populations, various comorbidities, etc.) among physicians. The present survey provided insights regarding the attitudes toward and clinical applications of Met of physicians from different departments and institutes in Anhui Province, China. The analysis of the survey showed that the physicians are not professional with regard to prescribing Met and should be highly vigilant in terms of standardized prescription for Met.
Met has been prescribed to diabetic patients for more than 60 years, and some guidelines or consensuses have been already released to standardize the prescription of Met.2,13,15 As the most widely used glucose-lowering drug, Met is mainly prescribed for patients with T2DM. Both guidelines in China and abroad recommend adding Met for type 1 diabetes mellitus (T1DM) in overweight or obese populations as a supplementary treatment of insulin therapy.19,20 Met has been demonstrated to improve insulin resistance, minimize insulin dose, reduce body weight and provide cardiovascular protection in patients with T1DM.19–21 In the present survey, only less than 15% of the respondents considered T1DM as an indication for Met, while most of the respondents did not consider the use of Met in combination with insulin. For the special population of pregnant women, Met is not recommended as a first-line agent because it can cross the placenta to the fetus. However, neonatal hypoglycemia incidence and maternal weight gain occur less in pregnant women using Met when compared to those using insulin.2,22 Some follow-up studies reported that the offspring of pregnant patients who used Met during pregnancy due to diagnosis of polycystic ovary syndrome (PCOS) or gestational diabetes (GDM) have higher BMI, increased obesity, increased waist and slightly increased fat mass.23–25 Our survey showed that a minority of the physicians (1.05%) indicated that they would prescribe Met for pregnant women. In the present study, over half of the respondents indicated that they have previously selected Met as a treatment alternative for patients with hyperinsulinemia, obesity or PCOS. So, an increasing number of physicians are aware of the pleiotropic effects of Met and use Met widely in different populations and not just to treat adult T2DM. In addition, Met also has beneficial effects on other diseases such as aging and cancers.26
It is concerning that our survey found that different forms, dosages and frequency use of Met were reported by the respondents. Met-XR, which is recommended to be administered once daily and provides an alternative for Met-IR intolerance, has a lower rate of GI response and a similar hypoglycemia effect.27,28 If cost is not an issue, it is recommended that physicians start treatment with Met-XR as the first choice to avoid switching or discontinuing due to GI adverse effects (AEs). In our survey, 72.75% of physicians selected Met-XR, but only one third of the physicians selected the correct frequency (Met-XR QD). These findings indicated that most of the physicians are unfamiliar with the pharmacokinetics and correct frequency of the extended-release dosage form. About 69% of the physicians selected 1500–2000 mg/d as the maximum dose in their daily work. Liu et al reported that 60.8% of the respondents selected the correct dose range of 500–2000 mg for Met-XR and that 62.0% of the respondents selected the correct frequency (once daily),11 which disagree with our results and may be related to the differences in the knowledge and region.
GI AEs are typical problems frequently encountered with the use of Met, especially the dosage form of conventional immediate-release (Met-IR). The side effects do not show a complete dose-response relationship and may disappear after cessation.29 Although some patients are unable to tolerate Met at all after initiating at a low dose or titrating slowly, pharmacology and endocrinology specialists suggest not to diagnose Met intolerance too quickly to avoid depriving the patients of the benefits of Met.13,30 Physicians should set a proper dose to weigh the glucose-lowering benefits against GI reaction when AE occurs. Once started, Met therapy is suggested to be sustained as long as possible if the patients can tolerate the GI reaction.3 In the present study, 38.16% of the physicians indicated that they would stop Met treatment when AEs emerge, and more than half of the physicians (61.84%) responded that they would withhold the medication and adopt at least one of the following approaches to mitigate the GI reaction to Met: 1) start with a low dose and gradually titrate up according to the patients’ response (86.44%); 2) change to Met extended-release (Met-XR) or enteric-coated tablets (53.56%); and 3) suggest that Met-IR be taken with meals or immediately after meals (71.19%).
The safety of antidiabetic drugs for patients with DM and chronic kidney disease remains the center of attention. In 2020, the FDA revised the instructions for Met use and suggested expanded use of Met for diabetic patients with chronic kidney disease (CKD).31 In view of the apparent mortality reduction and safety in DM patients with mild to moderate impairment of renal function,32 it is recommended that Met can be safely used when the eGFR decreases to 45 mL/min/1.73 m2 or even below 30 mL/min/1.73 m2.33,34 Once the eGFR decreases to 45 mL/min/1.73 m2, it is necessary for physicians to weigh the risks against the benefits of ongoing use of Met. When the eGFR is lower than 30 mL/min/1.73 m2, patients should not be treated with Met.31 According to the consensus of clinical use of Met in China (2018), Met prescription is also contraindicated when eGFR decreases to less than 45 mL/min/1.73 m2.15 Our questionnaire showed that 13.84% of the respondents had incorrect viewpoints that long-term use of Met may impair renal function, and nearly half of the respondents did not know the contraindications of Met prescription in patients with renal damage. Additionally, the association between radiocontrast agents and Met use was also surveyed by two multiple-choice questions about clinical practice in the real world. The results showed that only 8.18% of the respondents correctly answered the following question:” When would you suggest stopping Met prescription before using a contrast agent?”. Around half of the participants selected the correct options for the following question: “Which do you select after using a contrast agent?”.
Evidence has shown that Met is safe in diabetic patients with liver cirrhosis and that it decreases the related risk of death and the incidence of hepatocellular carcinoma35 as well as preventing the development of fatty liver disease.36,37 In our survey, most respondents had the correct viewpoint that long-term use of Met will not impair hepatic function. However, more than half of the physicians selected the wrong options regarding hepatic contraindication of Met prescription. There have been no Cardiovascular Outcomes Trials performed to evaluate the safety of Met in cardiovascular disease (CVD). Nevertheless, many retrospective or observational studies have demonstrated consistent beneficial effects of Met in diabetic patients with CVDs, such as coronary heart disease and heart failure.38–41 Most of the respondents (91.19%) in our survey considered that long-term use of Met would not exacerbate heart failure.
We analyzed the accuracy of reponses to seven professional questions in the questionnaire. The degrees of scores showed that the physicians with higher levels of hospital grades or categories, education background, professional titles as well as physicians working in Endocrinology Department tended to achieve high scores. However, further statistical analysis demonstrated that department was the only independent risk factor of the professional levels. Therefore, professional knowledge should be enhanced among non-endocrinology physicians, mainly referring to general practitioners both in comprehensive hospitals and community health centers. In the background of the COVID-19 global pandemic, online training may provide an appropriate form of continuing training.
The present study had several limitations. First, a limited number of clinicians participated in our survey, and all of the respondents were from Anhui Province, China. The circumstances in other provinces may be different. Second, our survey covered physicians from all institution levels, but more than half of them were from higher level hospitals, which may have introduced a bias.
Conclusion
Based on the present findings, some physicians have an unclear understanding of Met pharmaceutical dosage, side effects, indications and contraindications, indicating that physicians should be highly vigilant in terms of standardized prescription for Met. We recommended the physicians take continuous professional development training course. Self-learning of guidelines or expert consensuses of diabetic care should be insisted on. Endocrinologists serving in general hospitals or in tertiary hospitals have the responsibility to improve the professional skills and understanding of grass-roots medical staff according to the current medical situation in China.
Acknowledgments
This study was supported by the Fundamental Research Funds for the Central Universities (NO.WK9110000194) and the Research Fund of Anhui Medical University (NO. 2020xkj239).
Disclosure
The authors report no conflicts of interest in this work.
References
1. IDF_Atlas_10th_Edition_2021; 2021. Available from: https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf.
2. Society CD. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellit. 2021;13(4):315–409.
3. Draznin B, Aroda VR, Bakris G, et al.; American Diabetes Association Professional Practice Committee. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl1):S125–125S143. doi:10.2337/dc22-S009
4. Pasquel FJ, Lansang MC, Dhatariya K, Umpierrez GE. Management of diabetes and hyperglycaemia in the hospital. Lancet Diabetes Endocrinol. 2021;9(3):174–188. doi:10.1016/S2213-8587(20)30381-8
5. Le S, Lee GC. Emerging trends in metformin prescribing in the United States from 2000 to 2015. Clin Drug Investig. 2019;39(8):757–763. doi:10.1007/s40261-019-00799-0
6. Haymana C, Sonmez A, Demirci I, et al. Patterns and preferences of antidiabetic drug use in Turkish patients with type 2 diabetes - A nationwide cross-sectional study (TEMD treatment study). Diabetes Res Clin Pract. 2021;171:108556. doi:10.1016/j.diabres.2020.108556
7. Yang A, Wu H, Lau E, et al. Trends in glucose-lowering drug use, glycemic control, and severe hypoglycemia in adults with diabetes in Hong Kong, 2002–2016. Diabetes Care. 2020;43(12):2967–2974. doi:10.2337/dc20-0260
8. McEwen LN, Hurst TE, Joiner KL, Herman WH. Health beliefs associated with metformin use among insured adults with prediabetes. Diabetes Care. 2022;45(10):2282–2288. doi:10.2337/dc21-2316
9. Tseng E, Greer RC, O’Rourke P, et al. National survey of primary care physicians’ knowledge, practices, and perceptions of prediabetes. J Gen Intern Med. 2019;34(11):2475–2481. doi:10.1007/s11606-019-05245-7
10. Liu C, Foti K, Grams ME, Shin JI, Selvin E. Trends in self-reported prediabetes and metformin use in the USA: NHANES 2005–2014. J Gen Intern Med. 2020;35(1):95–101. doi:10.1007/s11606-019-05398-5
11. Liu C, Tang S, An K, et al. Knowledge, attitude, and practice of metformin extended-release tablets among clinicians in China: a cross-sectional survey. Front Pharmacol. 2021;12:634561. doi:10.3389/fphar.2021.634561
12. Khan T, Wozniak GD, Kirley K. An assessment of medical students’ knowledge of prediabetes and diabetes prevention. BMC Med Educ. 2019;19(1):285. doi:10.1186/s12909-019-1721-9
13. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes, 2015: a patient-centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia. 2015;58(3):429–442. doi:10.1007/s00125-014-3460-0
14. Seferović PM, Petrie MC, Filippatos GS, et al. Type 2 diabetes mellitus and heart failure: a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2018;20(5):853–872. doi:10.1002/ejhf.1170
15. Mu YM; Expert Group of Metformin in Clinical Practice. Expert consensus on clinical use of metformin (2018 edition). Chin J Diabetes. 2019;27(3):161–173. doi:10.3969/j.issn.1006-6187.2019.03.001
16. Gu XC, Men P, Zhai SD. Questionnaire survey on pharmacists’s attitude to safety and efficacy of original patented drug and generic drug of metformin. China Acad J. 2017;37(13):1292–1294+1301.
17. Liu C, Zhou YL, Wang Y, et al. Knowledge, attitude and practice of metformin hydrochloride sustained release tablets in outpatients with type 2 diabetes mellitus. Chin Gen Pract. 2021;24(36):4593–4598.
18. Hashimoto Y, Yasuzawa H, Ishida T, Miyazaki Y, Fukui M. A survey on consciousness towards the proper use of metformin and medical cost in Japanese patients with type 2 diabetes. J Clin Biochem Nutr. 2021;69(3):286–293. doi:10.3164/jcbn.21-5
19. Guo T, Guo LX, Weng JP and Zhou ZG. Chinese guidelines for insulin treatment of type 1 diabetes mellitus. Chin J Diabetes Mellit. 2016;8:591–597.
20. Amiel SA, Pursey N, Higgins B, Dawoud D. Type 1 Diabetes in Adults: Diagnosis and Management. London: National Institute for Health and Care Excellence (NICE); 2022.
21. Bjornstad P, Schäfer M, Truong U, et al. Metformin improves insulin sensitivity and vascular health in youth with type 1 diabetes mellitus. Circulation. 2018;138(25):2895–2907. doi:10.1161/CIRCULATIONAHA.118.035525
22. Draznin B; American Diabetes Association Professional Practice Committee, American Diabetes Association Professional Practice Committee. Management of diabetes in pregnancy: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl1):S232–232S243. doi:10.2337/dc22-S015
23. Hanem L, Stridsklev S, Júlíusson PB, et al. Metformin use in PCOS pregnancies increases the risk of offspring overweight at 4 years of age: follow-up of two RCTs. J Clin Endocrinol Metab. 2018;103(4):1612–1621. doi:10.1210/jc.2017-02419
24. Hanem L, Salvesen Ø, Juliusson PB, et al. Intrauterine metformin exposure and offspring cardiometabolic risk factors (PedMet study): a 5–10 year follow-up of the PregMet randomised controlled trial. Lancet Child Adolesc Health. 2019;3(3):166–174. doi:10.1016/S2352-4642(18)30385-7
25. Tarry-Adkins JL, Aiken CE, Ozanne SE. Neonatal, infant, and childhood growth following metformin versus insulin treatment for gestational diabetes: a systematic review and meta-analysis. PLoS Med. 2019;16(8):e1002848. doi:10.1371/journal.pmed.1002848
26. Lv Z, Guo Y. Metformin and its benefits for various diseases. Front Endocrinol. 2020;11:191. doi:10.3389/fendo.2020.00191
27. NICE guideline. Type 2 diabetes in adults: management. Available from: https://www.nice.org.uk/guidance/ng28/chapter/Recommendations.; 2022
28. Tan J, Wang Y, Liu S, et al. Long-acting metformin vs. metformin immediate release in patients with type 2 diabetes: a systematic review. Front Pharmacol. 2021;12:669814. doi:10.3389/fphar.2021.669814
29. Guo L, Guo X, Li Y, et al. Effects of body mass index or dosage on gastrointestinal disorders associated with extended-release metformin in type 2 diabetes: sub-analysis of a Phase IV open-label trial in Chinese patients. Diabetes Metab Syndr. 2016;10(3):137–142. doi:10.1016/j.dsx.2016.01.004
30. Bonnet F, Scheen A. Understanding and overcoming metformin gastrointestinal intolerance. Diabetes Obes Metab. 2017;19(4):473–481. doi:10.1111/dom.12854
31. U.S. FaDA. FDA Drug Safety Communication: FDA revises warnings regarding use of the diabetes medicine metformin in certain patients with reduced kidney function; 2016.
32. Ekström N, Schiöler L, Svensson AM, et al. Effectiveness and safety of metformin in 51 675 patients with type 2 diabetes and different levels of renal function: a cohort study from the Swedish National Diabetes Register. BMJ Open. 2012;2:4. doi:10.1136/bmjopen-2012-001076
33. Dissanayake AM, Wheldon MC, Ahmed J, Hood CJ. Extending metformin use in diabetic kidney disease: a pharmacokinetic study in stage 4 diabetic nephropathy. Kidney Int Rep. 2017;2(4):705–712. doi:10.1016/j.ekir.2017.03.005
34. Lalau JD, Kajbaf F, Bennis Y, Hurtel-Lemaire AS, Belpaire F, De Broe ME. Metformin treatment in patients with type 2 diabetes and chronic kidney disease stages 3A, 3B, or 4. Diabetes Care. 2018;41(3):547–553. doi:10.2337/dc17-2231
35. Singh S, Singh PP, Singh AG, Murad MH, Sanchez W. Anti-diabetic medications and the risk of hepatocellular cancer: a systematic review and meta-analysis. Am J Gastroenterol. 2013;108(6):881–891; quiz 892. doi:10.1038/ajg.2013.5
36. Pinyopornpanish K, Leerapun A, Pinyopornpanish K, Chattipakorn N. Effects of metformin on hepatic steatosis in adults with nonalcoholic fatty liver disease and diabetes: insights from the cellular to patient levels. Gut Liver. 2021;15(6):827–840. doi:10.5009/gnl20367
37. Huang Y, Wang X, Yan C, et al. Effect of metformin on nonalcoholic fatty liver based on meta-analysis and network pharmacology. Medicine. 2022;101(43):e31437. doi:10.1097/MD.0000000000031437
38. Orloff J, Min JY, Mushlin A, Flory J. Safety and effectiveness of metformin in patients with reduced renal function: a systematic review. Diabetes Obes Metab. 2021;23(9):2035–2047. doi:10.1111/dom.14440
39. Bergmark BA, Bhatt DL, McGuire DK, et al. Metformin use and clinical outcomes among patients with diabetes mellitus with or without heart failure or kidney dysfunction: observations from the SAVOR-TIMI 53 Trial. Circulation. 2019;140(12):1004–1014. doi:10.1161/CIRCULATIONAHA.119.040144
40. Han Y, Xie H, Liu Y, Gao P, Yang X, Shen Z. Effect of metformin on all-cause and cardiovascular mortality in patients with coronary artery diseases: a systematic review and an updated meta-analysis. Cardiovasc Diabetol. 2019;18(1):96. doi:10.1186/s12933-019-0900-7
41. Tseng CH. Metformin use is associated with a lower risk of hospitalization for heart failure in patients with type 2 diabetes mellitus: a retrospective cohort analysis. J Am Heart Assoc. 2019;8(21):e011640. doi:10.1161/JAHA.118.011640
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.