")
Back to Journals » International Journal of General Medicine » Volume 14
Clinical and Radiological Predictors of Early Intervention in Acute Ureteral Colic
Authors Abushamma F , Ktaifan M , Abdallah A, Alkarajeh M , Maree M , Awadghanem A , Jaradat A , Aghbar A, Zyoud SH , Keeley Jr FX
Received 4 June 2021
Accepted for publication 14 July 2021
Published 30 July 2021 Volume 2021:14 Pages 4051—4059
DOI https://doi.org/10.2147/IJGM.S322170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Faris Abushamma,1,2 Mahfouz Ktaifan,1 Abdoh Abdallah,1 Mohammad Alkarajeh,1 Mosab Maree,1,3 Ahmed Awadghanem,1,3 Ahmad Jaradat,1,2 Amir Aghbar,1,2 Sa’ed H Zyoud,4,5 Francis X Keeley Jr6
1Department of Medicine, College of Medicine and Health Sciences, An-Najah National University, Nablus, 44839, Palestine; 2Department of Urology, An-Najah National University Hospital, Nablus, 44839, Palestine; 3Department of Radiology, An-Najah National University Hospital, Nablus, 44839, Palestine; 4Department of Clinical and Community Pharmacy, College of Medicine and Health Sciences, An-Najah National University, Nablus, 44839, Palestine; 5Clinical Research Center, An-Najah National University Hospital, Nablus, 44839, Palestine; 6Bristol Urological Institute, North Bristol NHS Trust, Bristol, UK
Correspondence: Faris Abushamma
Department of Medicine, College of Medicine and Health Sciences, An-Najah National University, Nablus, 44839, Palestine
Email [email protected]
Purpose: Acute ureteric colic (AUC) is generally one of the most common reasons for emergency department attendance. Expectant management is recommended in non-complicated ureteral calculi. However, data regarding the optimal duration of observation or indications of early intervention (EI) are not well understood. This article describes the clinical and radiological factors that promote EI in AUC.
Patients and Methods: This was an observational and retrospective cohort study. Patients with AUC diagnosed based on non-contrast computerized tomography (NCCT) between 2019 and 2020 were enrolled in the study. These patients were classified into two main categories: spontaneous passage of stone (SSP) and EI. In addition, a comparative analysis was performed to identify clinical and radiological variables that promote EI.
Results: One-hundred and sixty-one patients were included. High WBCs are associated with a significant increase in EI. Forty-three percent (n=37) of patients with serum WBCs higher than 10 had an EI, while 23% had SSP (n=17;p< 0.001). High CRP level is also significantly associated with EI (n=36; 86%; p< 0.001). Upper and middle ureteral calculi are statistically associated with EI (n=54; 62%) in comparison to the SSP cohort (n=22; 30%;p< 0.001). EI is also linked to the maximal length of ureteric calculi (MCL) of 9 mm (6– 13mm), and HU density of stone of 700 (430– 990) H.U (p< 0.001). Ureteric stone volume of 0.2 (0.06– 0.3) cm3 is significantly associated with EI (p< 0.001). Ureteral wall thickness of 3 (2– 3 mm), the presence of extrarenal pelvis (n=20; 23%), and AP diameter of renal pelvis 18 (13– 28 mm) are all significantly associated with a higher rate of EI (p< 0.001). Multiple binary logistic regression analysis showed that MCL is the strongest predictor of EI.
Conclusion: MCL is an independent and robust predictor of EI in AUC. Biochemical variables and radiological characteristics can also act as an adjunct to promote EI.
Keywords: ureteral calculi, medical expulsive therapy, spontaneous stone passage, maximal length of ureteral calculi, pyonephrosis
Introduction
Acute ureteral colic (AUC) is one of the most common encounters in the emergency department, usually associated with significant pain and symptoms such as nausea and vomiting.1,2 AUC mandates prompt evaluation and management, initially by emergency physicians, in the form of resuscitation, analgesia, and ordering imaging studies to confirm the diagnosis.3 Non-contrast computerized tomography (NCCT) is currently considered the standard method of diagnosis in AUC. NCCT shows the site and size of ureteral calculi with high sensitivity and detects some variables that may influence treatment decisions, such as secondary signs of infection, degree of obstruction, and other concomitant pathologies or complications.4,5 The presence of complications in AUC such as fever, renal failure, and obstructed single kidney is a well-established indication for emergency intervention.6 The guidelines recommend observation and conservative measures in the absence of complications.7 Nevertheless, some patients do not meet the criteria for emergency intervention but need prioritisation and fast-track referral to urology for possible early intervention (EI).8 There is no consensus regarding the group of patients who require fast-tracking and may benefit from EI. A few articles were published to predict medical expulsive therapy (MET) success in AUC and others to show variables that promote emergency intervention within 24–48 hours.9 The SUSPEND trial showed no apparent benefit of MET in AUC. The MIMIC study showed that stone size and position are essential predictors for spontaneous stone passage (SSP) without real benefit from MET.10,11 Thus, the standard of care in non-complicated AUC is to wait for spontaneous passage for up to 40 days, with a high chance of possible intervention in ureteral stones larger than 5 mm regardless of the usage of MET.12 This grey zone of observation that is highly variable regarding time until stone passage, intervention rate, and risk of serious complications encouraged us to study clinical and radiological factors that promote EI. Knowing these factors allows emergency physicians, general practitioners, and urologists to identify candidates for prompt EI. Early recognition of such a cohort of patients decreases recurrent visits to the emergency department, avoids possible complications associated with the delayed intervention, and saves patients who are unlikely to pass the stone spontaneously from the unnecessary lengthy journey.
Patients and Methods
Study Design
A retrospective cohort study recruited selected patients who had presented to the emergency department with AUC.
Study Setting
This study was held at our tertiary university hospital between April 2019 and May 2020.
Study Population and Sampling
We recruited patients who presented to the emergency department complaining of AUC and had confirmatory NCCT of ureteric stone. Follow-up clinic notes at 4–6 weeks were reviewed to measure the outcome. The outcome was divided into two main groups:
- Group 1: SSP on MET at the time of follow-up clinic: this group included patients who noticed their stones passing spontaneously, had no symptoms and no visible stone on X-ray, or no hydronephrosis on ultrasonography. The medication used was Tamsulosin 0.4 mg.
- Group 2: EI prior to the follow-up clinic: this group included patients who had EI in the form of percutaneous nephrostomy, ureteroscopy or ureteral stent due to fever, progressive acute kidney injury (glomerular filtration rate (eGFR) less than 60 mL/min), or recurrent visits to the emergency department.
Inclusion and Exclusion Criteria
Inclusion Criteria
- A ureteral calculus proven by an NCCT scan.
- Follow-up clinic data available within six weeks of discharge from the emergency department.
Exclusion Criteria
- Ultrasound- or X-ray-based diagnosis of ureteral stone.
- Complicated ureteric stone such as sepsis, or eGFR less than 30 mL/min.
- Single anatomical or functional kidney.
- Age less than 18 years old.
Data Collection
Patient demographics and clinical variables: These include clinical assessment, blood tests (complete blood count [CBC], C-reactive protein (CRP), kidney function test (serum creatinine [Sr Cr] and eGFR), and urine analysis.
Radiological characteristics: Based on NCCT, radiological variables were prospectively and independently collected by two radiologists, AG and MM, who were blinded to the initial report. No training for consensus measurement between the readers was performed. The radiologists were blinded to the clinical data and the outcome.
Radiological Variables Classification
Stone Burden and Location
Location of ureteral calculi: Ureteral calculi location is classified into upper (above the sacroiliac joint), middle (overlying the sacroiliac joints), and lower (below sacroiliac joint).13,14
Maximal length of ureteral calculi (mm) (MCL): Measured by taking the longest diameter of the stone after calculating it on the three different dimensions (horizontal, axial, and sagittal) relative to the main axes of the patient's body, in a standardized bone window and using 1 mm thickness.13,14
Ureteral stone volume (cm3): Calculated using a particular program on the PACS system.
The presence of multiple ureteral calculi: Defined as the presence of more than one stone in the same ureter.
Hounsfield unit density of ureteral calculi (HU density): Using the largest possible area density of the stone on different planes.15
Radiological Signs of Potential Infection
HU density of the hydronephrotic region of the affected kidney: A value of 10 or more is considered a potential sign of infected hydronephrosis or pyonephrosis.16
Grade of perinephric stranding: Our radiologists, AG and MM, have created a novel classification of the degrees of perinephric stranding based on the level of spreading: grade 0 (no stranding), grade 1 (stranding confined to the stone area), grade 2 (stranding extending proximally along the ureter but not reaching the kidney), grade 3 (stranding extending to fat surrounding the affected kidney), grade 4 (extensive perinephric stranding involving most of Gerota’s fascia with significant thickening of perinephric bridging septa), and grade 5 (perinephric collection).
Risk of pyonephrosis: Calculated by combining HU density of renal pelvis >10 with perinephric stranding grades 4 or 5.16
Anatomical Description of Urinary Tract
Ureteral wall thickness (mm) (UWT): Measured as the point of greatest soft-tissue thickness around the circumference of the stone.17,18
Anterior–posterior diameter of the renal pelvis (AP mm), defined as the largest AP of the renal pelvis on axial NCCT, reflecting the degree of hydronephrosis.19
The extrarenal pelvis is described as a normal anatomical variant characterised by a renal pelvis that is predominantly outside the renal sinus and is larger and more distensible than an intrarenal pelvis surrounded by sinus fat.
Ethical Considerations
The Institutional Review Board (IRB) of An-Najah National University has approved this study. Because of the retrospective chart review, the IRB waived informed consent. The research was conducted in accordance with the Helsinki Declaration. There is no confidentiality risk because the analysis employed anonymized clinical data that cannot be connected to the patients who participated.
Statistical Analysis
ll analysis was performed with SPSS Statistics version 21.0 (IBM). Categorical variables were presented as absolute frequency (percentage). The Pearson’s chi-square test or Fisher’s exact test, as appropriate, were applied to assess the differences for categorical variables, and the Mann–Whitney U-test was used for continuous variables. P-values of <0.05 were considered statistically significant. Multiple logistic regression analysis was used to identify patients’ clinical and radiological characteristics associated with EI in AUC. “EI in AUC (Intervention⁄SSP)” was used as the dependent variable in the model. Variables included in the regression analysis were those with statistically significant p-values (<0.05) in the univariate analysis but we excluded the CRP because of significant missing data.
Results
Patients’ Demographics and Clinical Presentations
Two-hundred and ninety-five records for AUC were reviewed; of these, 161 patients met our inclusion criteria and 124 (77%) were male. The median age of our sample was 43 (31–59 years); 87 (54%) patients had EI (group 1), while 74 (46%) managed to pass the stone spontaneously (group 2). Diabetes was present in 13 (14.9%) patients in group 1 and 12 (16.2%) patients in group 2 with no statistical difference (p>0.05). Table 1 shows patients’ demographics and clinical presentations.
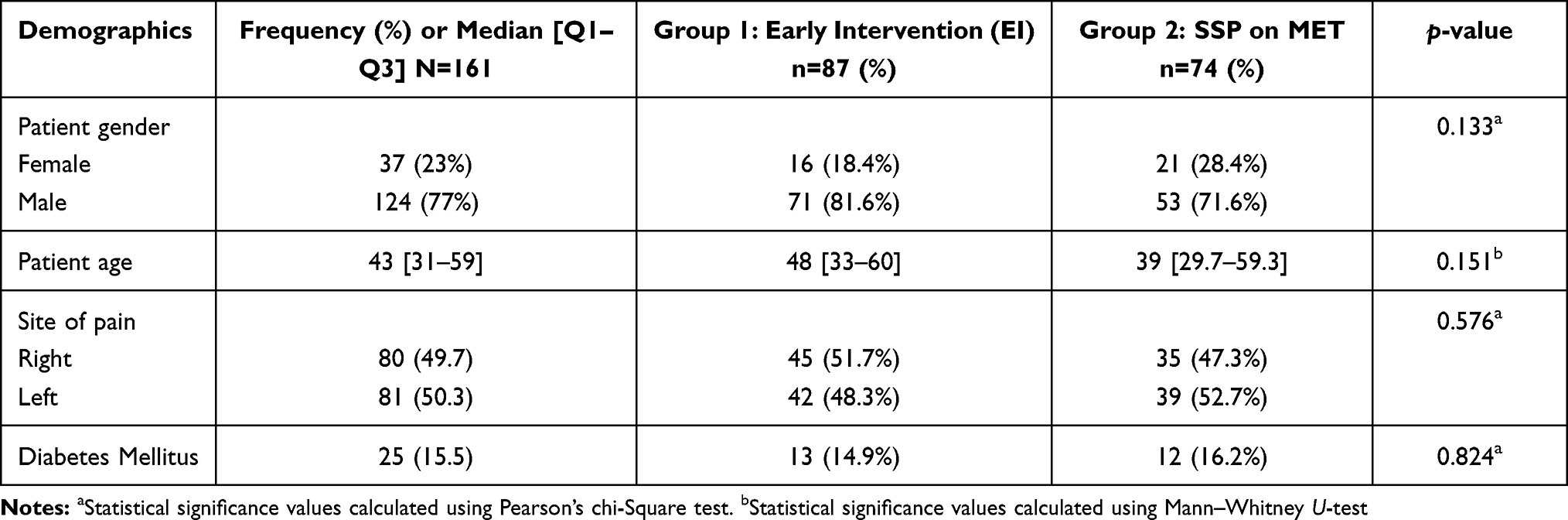 |
Table 1 Patients’ Demographics and Clinical Presentations |
Indications of EI and Mean Time to EI
The mean time of EI was 3.6 (1–37 days). Indications of EI were: developing fever (n=7; 8.04%); progressive acute kidney injury (eGFR<60) (n=26; 29.88%); and AUC refractory to standard analgesics, in addition to recurrent visits to emergency department (n=54; 62.06%).
Patients’ Clinical Characteristics for EI
High white blood cell (WBC) count and high CRP are significantly associated with EI. Thirty-seven patients (43%) with serum WBCs higher than 10 had an EI while 17 (23%) had SSP (p=0.016). High CRP levels were significantly associated with a higher rate of EI (n=36; 86%) (p=0.004). Table 2 shows different clinical variables correlated with both groups.
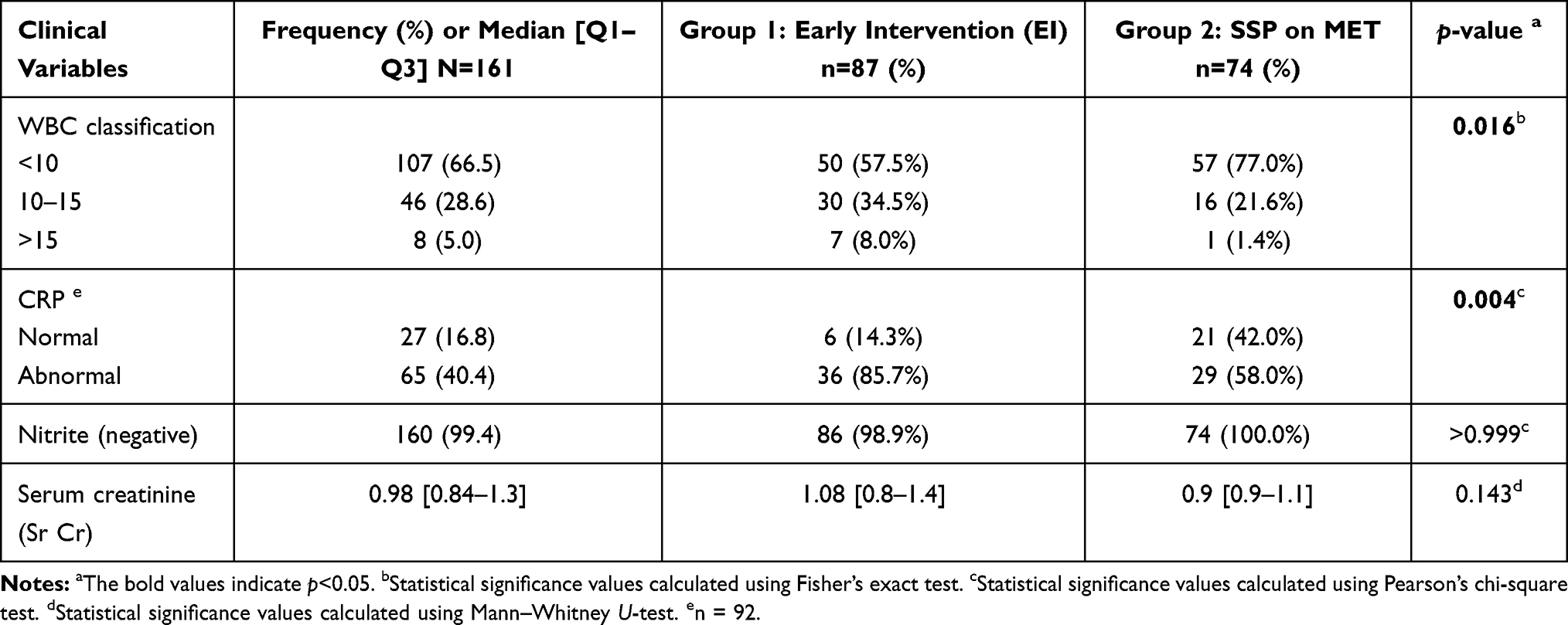 |
Table 2 Patients’ Clinical Variables Correlated to Both Groups |
Radiological Characteristics for EI
Stone Burden and Location
Location of Ureteral Calculi
Stone location was significantly associated with EI. Upper and middle ureteral calculi were statistically associated with EI (n=54; 62%) in comparison to upper and middle ureteral stones associated with SSP (n=22; 30%; p<0.001). The presence of lower ureteral calculi was significantly associated with SSP (n=52; 70%) while less likely to require EI (n=33; 38%;p<0.001). See Table 3A.
MCL)
MCL was significantly associated with EI. For example, median MCL of 9 mm (6–13 mm) was statistically associated with EI, and median MCL of 5 mm (3–6 mm) was associated with SSP (p<0.001).
Ureteral Stone Volume (cm3)
Ureteral stone volume of 0.2 [0.14–0.5] cm3 was significantly associated with EI and ureteral stone volume of 0.096 (0.04–0.2) was associated with SPP (p<0.001).
Presence of Multiple Ureteral Stones
Multiple ureteral stones were associated with EI in 22 patients (25%) and stones were less likely to pass spontaneously in 5 patients (7%) (p=0.002).
Hounsfield Unit Density of Ureteral Calculi (HU Density)
HU density of 800 [500–1100] was statistically correlated to EI, while HU density of 565 (397.5–850) was more likely to have SSP (p<0.001).
Radiological Signs of Potential Infection
HU Density of the Hydronephrotic Region of the Affected Kidney
There was no statistical difference between the two groups in the prospect of HU density of renal pelvis fluid. HU density more than 10 was found in 26 patients (30%) in group 1 (EI) and in 19 patients (26%) in group 2 (SSP), with no statistical difference (p>0.05). See Table 3B.
Grade of Perinephric Stranding
High grade of perinephric stranding (grades 3, 4 and 5) was not associated with risk of EI. Perinephric stranding (grades 3–5) was found in 48 patients (55%) in group 1 EI and in 42 patients (57%) in group 2 (SSP), with no statistical difference (p>0.05).
Risk of Pyonephrosis
The calculated potential risk of pyonephrosis was not statistically associated with an increased risk of EI. Risk of pyonephrosis was found in 10 patients (12%) in group 1 (EI) and in 11 patients (15%) in group 2 (SSP), with no statistical difference (p > 0.05).
Anatomical Description of Urinary Tract
Ureteral Wall Thickness (mm) (UWT)
Median UWT of 3 (2–3 mm) was significantly associated with EI, and UWT of 2 (2–3 mm) was associated with SSP (p=0.010). See Table 3C.
Anterior–Posterior Diameter of the Renal Pelvis (mm) (AP mm)
AP diameter of 18 (13–28 mm) was significantly associated with EI, while AP diameter of 14 (10–21 mm) was associated with SSP (p=0.001).
Presence of Extrarenal Pelvis
Extrarenal pelvis (n=20; 23%) was significantly associated with EI while absence of extrarenal pelvis was statically associated with SSP (n=66; 89%) (p=0.042).
Multivariable Logistic Regression Analysis
Table 4 shows multiple binary logistic regression analyses, using EI in AUC (with intervention versus SSP) as a dependent variable and the following factors as independent variables: the presence of multiple stones, location of ureteral calculi, MCL, ureteral stone volume, AP diameter of the renal pelvis, WBC classification, presence of extrarenal pelvis, HU density of stone, and UWT. This analysis showed that a 1 mm increase in the length of ureteral calculi was associated with a 23% increase in odds of EI in AUC (OR: 1.23, 95% CI 1.05–1.44, p=0.011).
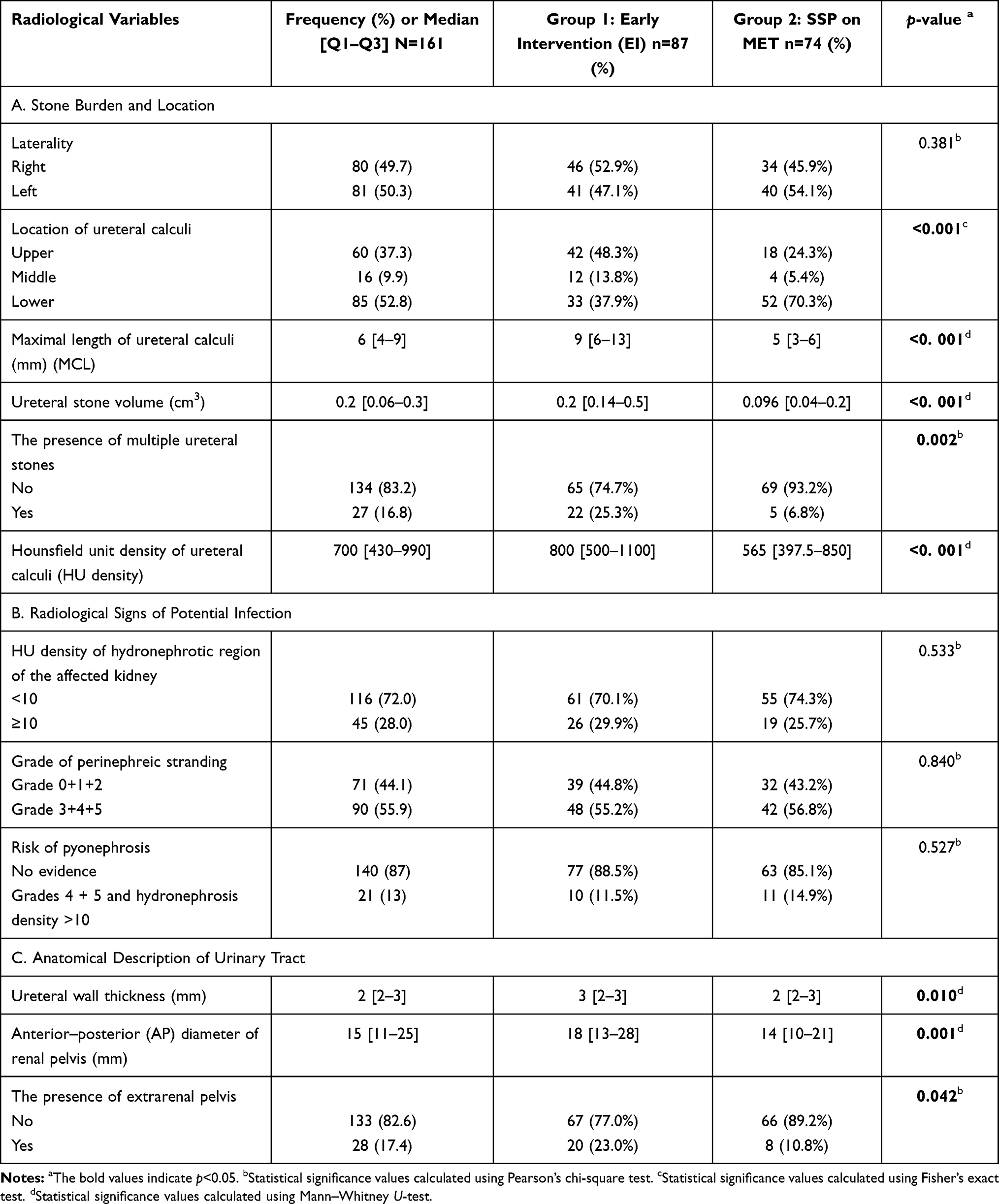 |
Table 3 Radiological Variables Classification Correlated to Both Groups |
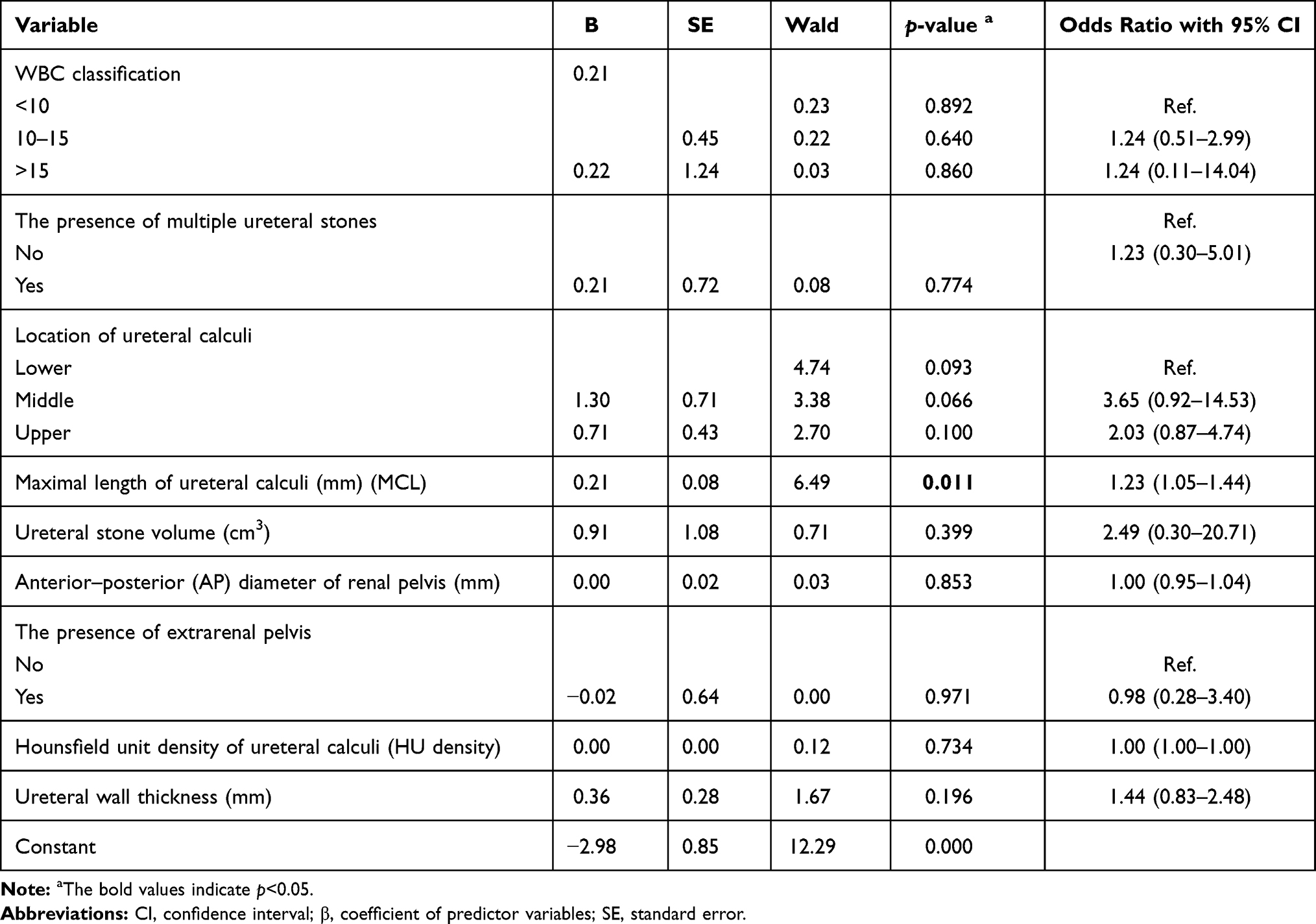 |
Table 4 Patients’ Clinical and Radiological Characteristics Associated with Early Intervention in Acute Ureteral Colic by Using Multiple Binary Logistic Regression Model |
Discussion
AUC is a common diagnosis in the emergency department, where emergency physicians usually manage such a condition according to a standard protocol of analgesia and resuscitation, followed by referral to urology services except when emergency intervention is required, such as in the case of an obstructed and infected kidney.20 There is no consensus regarding the optimal period of observation before surgical intervention. Nevertheless, it is estimated that most stones less than 5 mm will pass spontaneously within 40 days.21 Furthermore, the SUSPEND trial showed some benefits from MET in ureteral stones larger than 5 mm.11 However, EI may be required during this period of expectant management because of either failure of medical treatment or the development of complications such as sepsis or progressive kidney injury. Limited studies indicate criteria for the identification of those patients.22 There is no available tool or score for the identification of patients with stones unlikely to pass spontaneously. However, a cardiovascular risk assessment score (Framingham score) was used recently to predict SSP, and it was shown that a higher score is associated with EI.8,23 In this article, we described clinical and radiological features that may aid early recognition of patients suitable for EI, to allow prioritisation and fast-tracking to urology services for close monitoring and potential EI.
Standard biochemical workup often entails slight variation in AUC cases, including CBC, kidney function test, and CRP.24 It was previously identified that high serum WBCs at the time of AUC were associated with a higher chance of SSP.25 However, our data show that the likelihood of EI is positively correlated with the increase in WBC. For example, 43% of patients with WBC higher than 10 had EI, while 23% managed to pass their stone spontaneously.
NCCT has become the standard imaging modality to evaluate AUC.26 Emergency physicians can reliably identify ureteral calculi and some renal abnormalities based on NCCT.27 Therefore, NCCT is an essential tool used in emergency settings to highlight AUC patients who need EI. Stone size and location are well-known and established variables to predict SSP in AUC since the introduction of NCCT to diagnose kidney stones.13,28 There is consensus in the literature that lower and smaller ureteral calculi are significantly associated with high SSP.13,14 Our data agrees with the current evidence, which states that stone size and an MCL of 9 mm6–13 is more likely to require EI while stones with an MCL of 5 mm or less are more likely to pass spontaneously. Upper and middle ureteral calculi are also more likely to need EI, as 62% had EI while 29% had SSP. Surprisingly, the HU density of ureteral calculi appears to affect stone passage, as the mean attenuation of 700 [430–990] is positively related to EI. Thus, theoretically, harder stones are more likely to require EI.29 However, the HU density of stones failed to predict stone composition in vitro, and calculus radiodensity increased alongside the stone volume regardless of composition.15 Thus, this observation requires further clarification based on obtaining stone analysis for both groups and comparison with HU density.
Stone impaction markers, radiological signs of potential infection, and degree of obstruction have been a trending question in the literature since the adoption of NCCT as the modality of choice to evaluate ureteral calculi.16,22 Several published articles studied the value of such signs in the prospect of diagnosis in complicated ureteral calculi, duration of stone impaction, and the presence of underlying ureteral abnormalities such as strictures and polyps.30,31 We found that the extrarenal pelvis, AP diameter of the renal pelvis, and UWT are significantly associated with EI. A higher degree of renal pelvis distention represented by an AP diameter of 18 mm13–28 is significantly associated with EI. The significance of the dilatation of the renal pelvis and the degree of hydronephrosis has previously been studied. There is strong evidence that moderate to severe hydronephrosis is associated with a low stone-free rate even with intervention.19 UWT of 3 mm or higher, a stone impaction marker, is positively correlated with EI. This is supported by the available evidence, which showed that UWT could serve as a potential predictive factor for SSP if UWT is less than 2.3 mm and may help physicians identify patients who require EI, especially if UWT is more than 2.71 mm.17,18,22 Lastly, there is controversy in the literature regarding the role of ureteral diameter and the relation between ureteral and stone diameter in the prospect of SSP.23,32 This study supports the idea that the increase in UWT and the dilatation of the urinary tract above the level of obstruction decrease the chance of SSP and promote EI.
Multiple binary logistic regression analysis shows that MCL is an independent and robust predictor of EI in AUC. MCL of 6 mm or more is strongly associated with EI and decreased likelihood of spontaneous stone passage.33 Each 1 mm increase in the length of ureteral calculi was associated with a 23% increase in EI probability in AUC. These findings support the previously published evidence that MCL and related stone volume directly pertain to the SSP rate.14,34
Strength and Limitations
Although this is the first cohort study in the Arab world, we have encountered a few limitations. The retrospective nature of this study and the possibility of missing some patients are considered the main limitations of this study. Furthermore, the lack of a standard protocol for intervention and the concept that clinicians were not blinded to the size of the stone are also potential reasons for clinical bias as treating physicians may have a lower threshold for intervention in larger and higher stones. However, in the absence of randomized clinical trials, this article represents real-life practice. Despite having a significant correlation of EI with raised CRP, however, 43% of our cohort did not have an available CRP.35,36 Nevertheless, given these promising findings and predictors of EI in AUC, we have started a prospective, national, and multicentre trial to validate all factors with a view to developing a scoring model to predict EI in AUC.
Conclusions
Stone size is an independent and robust predictor of EI in AUC, with a noticeable increase in EI with each 1 mm increase in length. Therefore, an MCL of 6 mm or more is significantly associated with EI in the period of expectant management of non-complicated symptomatic ureteral calculi. Biochemical factors and several other radiological features based on NCCT are adjunct triage tools to identify patients suitable for EI.
Acknowledgments
Many thanks to the Clinical Research Centre of An-Najah National University Hospital for the constant support and wise advice. The authors thank Samantha Kearley from the Bristol Urological Institute, UK, for the English editing of the manuscript.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No specific grant was received from any public, commercial, or non-profit funding agency for this research.
Disclosure
All authors reported no conflicts of interest for this work.
References
1. Bultitude M, Rees J. Management of renal colic. BMJ (Clinical Research Ed). 2012;345:e5499.
2. Scales CD
3. Ramos-Fernández M, Serrano LA. Evaluation and management of renal colic in the emergency department. Bol Asoc Med P R. 2009;101(3):29–32.
4. Niall O, Russell J, MacGregor R, Duncan H, Mullins J. A comparison of noncontrast computerized tomography with excretory urography in the assessment of acute flank pain. J Urol. 1999;161(2):534–537. doi:10.1016/S0022-5347(01)61942-6
5. Fielding JR, Steele G, Fox LA, Heller H, Loughlin KR. Spiral computerized tomography in the evaluation of acute flank pain: a replacement for excretory urography. J Urol. 1997;157(6):2071–2073. doi:10.1016/S0022-5347(01)64676-7
6. Osorio L, Lima E, Autorino R, Marcelo F. Emergency management of ureteral stones: recent advances. Indian J Urol. 2008;24(4):461–466. doi:10.4103/0970-1591.44248
7. Assimos D, Krambeck A, Miller NL, et al. Surgical management of stones: american urological association/endourological society guideline, PART I. J Urol. 2016;196(4):1153–1160. doi:10.1016/j.juro.2016.05.090
8. Innes GD, Scheuermeyer FX, McRae AD, et al. Which patients should have early surgical intervention for acute ureteral colic? J Urol. 2021;205(1):152–158. doi:10.1097/JU.0000000000001318
9. Al-Terki A, El-Nahas AR. Development and validation of a score for emergency intervention in patients with acute renal colic secondary to ureteric stones. Arab J Urol. 2020;18(4):236–240.
10. Shah TT, Gao C, Peters M, et al. Factors associated with spontaneous stone passage in a contemporary cohort of patients presenting with acute ureteric colic: results from the multi-centre cohort study evaluating the role of inflammatory markers in patients presenting with acute ureteric colic (MIMIC) study. BJU Int. 2019;124(3):504–513.
11. Pickard R, Starr K, MacLennan G, et al. Medical expulsive therapy in adults with ureteric colic: a multicentre, randomised, placebo-controlled trial. Lancet. 2015;386(9991):341–349. doi:10.1016/S0140-6736(15)60933-3
12. Miller OF, Kane CJ. Time to stone passage for observed ureteral calculi: a guide for patient education. J Urol. 1999;162(3 Pt 1):
13. Jendeberg J, Geijer H, Alshamari M, Cierzniak B, Lidén M. Size matters: the width and location of a ureteral stone accurately predict the chance of spontaneous passage. Eur Radiol. 2017;27(11):4775–4785. doi:10.1007/s00330-017-4852-6
14. Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol. 2002;178(1):101–103. doi:10.2214/ajr.178.1.1780101
15. Motley G, Dalrymple N, Keesling C, Fischer J, Harmon W. Hounsfield unit density in the determination of urinary stone composition. Urology. 2001;58(2):170–173. doi:10.1016/S0090-4295(01)01115-3
16. Boeri L, Fulgheri I, Palmisano F, et al. Hounsfield unit attenuation value can differentiate pyonephrosis from hydronephrosis and predict septic complications in patients with obstructive uropathy. Sci Rep. 2020;10(1):18546. doi:10.1038/s41598-020-75672-8
17. Yoshida T, Inoue T, Taguchi M, Omura N, Kinoshita H, Matsuda T. Ureteral wall thickness as a significant factor in predicting spontaneous passage of ureteral stones of ≤ 10 mm: a preliminary report. World J Urol. 2019;37(5):913–919. doi:10.1007/s00345-018-2461-x
18. Yoshida T, Inoue T, Omura N, et al. Ureteral wall thickness as a preoperative indicator of impacted stones in patients with ureteral stones undergoing ureteroscopic lithotripsy. Urology. 2017;106:45–49. doi:10.1016/j.urology.2017.04.047
19. Hsiao HL, Huang SP, Wu WJ, et al. Impact of hydronephrosis on treatment outcome of solitary proximal ureteral stone after extracorporeal shock wave lithotripsy. Kaohsiung J Med Sci. 2008;24(10):507–513. doi:10.1016/S1607-551X(09)70009-9
20. Pearle MS, Pierce HL, Miller GL, et al. Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi. J Urol. 1998;160(4):1260–1264. doi:10.1016/S0022-5347(01)62511-4
21. Preminger GM, Tiselius HG, Assimos DG, et al. 2007 Guideline for the management of ureteral calculi. Eur Urol. 2007;52(6):1610–1631. doi:10.1016/j.eururo.2007.09.039
22. Kachroo N, Jain R, Maskal S, et al. Can CT-based stone impaction markers augment the predictive ability of spontaneous stone passage? J Endourol. 2021;35(4):429–435. doi:10.1089/end.2020.0645
23. Selvi I, Baydilli N. CT-related parameters and Framingham score as predictors of spontaneous passage of ureteral stones ≤ 10 mm: results from a prospective, observational, multicenter study. Urolithiasis. 2021;49(3):227–237.
24. Straub M, Strohmaier WL, Berg W, et al. Diagnosis and metaphylaxis of stone disease. consensus concept of the national working committee on stone disease for the upcoming german urolithiasis guideline. World J Urol. 2005;23(5):309–323. doi:10.1007/s00345-005-0029-z
25. Sfoungaristos S, Kavouras A, Katafigiotis I, Perimenis P. Role of white blood cell and neutrophil counts in predicting spontaneous stone passage in patients with renal colic. BJU Int. 2012;110(8 Pt B):E339–E345. doi:10.1111/j.1464-410X.2012.11014.x
26. Worster A, Preyra I, Weaver B, Haines T. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the diagnosis of suspected acute urolithiasis: a meta-analysis. Ann Emerg Med. 2002;40(3):280–286. doi:10.1067/mem.2002.126170
27. Holdgate A, Chan T. How accurate are emergency clinicians at interpreting noncontrast computed tomography for suspected renal colic? Acad Emergency Med. 2003;10(4):315–319. doi:10.1197/aemj.10.4.315
28. Sfoungaristos S, Kavouras A, Perimenis P. Predictors for spontaneous stone passage in patients with renal colic secondary to ureteral calculi. Int Urol Nephrol. 2012;44(1):71–79. doi:10.1007/s11255-011-9971-4
29. Ouzaid I, Al-qahtani S, Dominique S, et al. A 970 Hounsfield units (HU) threshold of kidney stone density on non-contrast computed tomography (NCCT) improves patients’ selection for extracorporeal shockwave lithotripsy (ESWL): evidence from a prospective study. BJU Int. 2012;110(11 Pt B):E438–E442. doi:10.1111/j.1464-410X.2012.10964.x
30. Smith RC, Verga M, Dalrymple N, McCarthy S, Rosenfield AT. Acute ureteral obstruction: value of secondary signs of helical unenhanced CT. AJR Am J Roentgenol. 1996;167(5):1109–1113. doi:10.2214/ajr.167.5.8911160
31. Hwang E, Kim YH, Yuk SM, Sul CK, Lim JS. Factors that predict spontaneous passage of a small distal ureteral stone <5 mm. J Endourol. 2010;24(10):1681–1685.
32. Zorba O, Ogullar S, Yazar S, Akca G. CT-based determination of ureteral stone volume: a predictor of spontaneous passage. J Endourol. 2016;30(1):32–36. doi:10.1089/end.2015.0481
33. Ahmed AF, Gabr AH, Emara AA, Ali M, Abdel-Aziz AS, Alshahrani S. Factors predicting the spontaneous passage of a ureteric calculus of ⩽10 mm. Arab J Urol. 2015;13(2):84–90. doi:10.1016/j.aju.2014.11.004
34. Demehri S, Steigner ML, Sodickson AD, Houseman EA, Rybicki FJ, Silverman SG. CT-based determination of maximum ureteral stone area: a predictor of spontaneous passage. AJR Am J Roentgenol. 2012;198(3):603–608. doi:10.2214/AJR.11.7276
35. Aldaqadossi HA. Stone expulsion rate of small distal ureteric calculi could be predicted with plasma C-reactive protein. Urolithiasis. 2013;41(3):235–239. doi:10.1007/s00240-013-0551-1
36. Park CH, Ha JY, Park CH, Kim CI, Kim KS, Kim BH. Relationship between spontaneous passage rates of ureteral stones less than 8 mm and serum c-reactive protein levels and neutrophil percentages. Korean J Urol. 2013;54(9):615–618. doi:10.4111/kju.2013.54.9.615
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.