")
Back to Journals » International Journal of General Medicine » Volume 17
Clinical and Radiological Outcomes of Halo Vest Application for Type II and III Odontoid Fractures
Authors Hashem M, Surur S, Hamad AS
Received 25 September 2023
Accepted for publication 25 January 2024
Published 5 February 2024 Volume 2024:17 Pages 457—469
DOI https://doi.org/10.2147/IJGM.S440126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Majdi Hashem,1 Saad Surur,2 Abdullah Soliman Hamad2
1Department of Surgery, Faculty of Medicine, imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia; 2Department of Orthopedic, king Saud Medical City, Riyadh, Saudi Arabia
Correspondence: Majdi Hashem, Assistant professor of Orthopedic, consultant Spine Surgeon, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia, Tel +966507739919, Email [email protected]
Objective: To assess halo vest applications for type II and III odontoid fractures and to ascertain the radiological and clinical outcomes of this approach.
Methods: A cross-sectional retrospective study was conducted by reviewing the medical charts of selected patients having type II and III odontoid fractures who underwent halo vest treatment at the King Saud Medical City Orthopaedic Department. Radiographic evaluations for the cervical spine (anterior-posterior, lateral, and open-mouth views) were used. Computed tomography scans were used to delineate the extent of the fracture and to measure the magnitude of displacement, the degree of the angulation, the vertebrae involved, and the fracture type.
Results: A total of 45 patients with odontoid fractures (55.6% of the patients with type II odontoid fractures and 44.4% of patients with type III) received halo vest treatment. In the present study, in type II odontoid fractures, union was achieved in 15.6% of patients, 28.9% of patients had malunion and 11.1% had nonunion. In type III odontoid fractures, union cases comprised 15.6% of patients, while malunion cases accounted for 28.9% of patients and nonunion cases were found in 4.4% of the patients.
Conclusion: The halo vest management for type II and III odontoid fracture requires a prolonged course of cervical immobilisation. Multiple factors contribute to the alteration of the management protocol, patient adherence, and difficulties related to HV, and a significant rate of reduction loss ultimately results in malunion or nonunion.
Keywords: halo vest, type II and III odontoid fractures, cervical spine, malunion, nonunion
Introduction
Despite being rare, cervical spine injuries can cause serious and protracted impairment. Seven vertebrae make up the cervical spine, which contains and protects the spinal cord.1–3 Due to its structure and flexibility, the cervical spine is the part of the spine that is most prone to injury. The most frequent sites of injury in the cervical spine are close to the second cervical vertebra C2 (the axis) or in the region of C5, C6, and C7. The most frequent cause of cervical injuries is trauma, which can result from sports-related or diving accidents, falls, penetrating or blunt trauma, or car accidents.4–8
The most frequent cervical spine fractures in the senior population, especially in individuals over 70 years, are traumatic odontoid fractures.9 Despite the rare incidence of spinal cord injury, more than 50% of patients who receive halo vest immobilisation (HVI) for type II odontoid fractures have unstable fractures that are worsened by nonunion.10 Avulsion fractures at the base have a higher rate of nonunion with nonsurgical therapy, while fractures of the tip are less frequent but more stable.11 Posterior displacement of the odontoid process is more commonly associated with spinal cord injury and is likely to result in nonunion.12,13 However, the ideal treatment for type II odontoid fractures is still controversial and debatable Recent recommendations suggest that surgical intervention should be the main treatment in such cases.14
Perry and Nickel originally developed the halo cast in 1959 to treat cervical instability and other spinal abnormalities.15 Thereafter, Blount modified it to the halo vest (HV).16,17 Although the HV has been conventionally used in the treatment of type II odontoid fractures, a high number of complications from its use have been noticed.14,18 Limited studies have explored the radiological parameters of type II and III odontoid fractures and their affection in union rate with HV treatment. In this study, we present the outcomes of HV management for type II and III odontoid fractures in young individuals to ascertain the radiological and clinical outcomes of this approach. Furthermore, this study aims to identify whether the displaced odontoid fractures are good candidates for the use of HV as a definitive treatment method. We also seek to determine the main causes of acute and long-term complications.
Methods
Study Design
A cross-sectional retrospective study was conducted after evaluating the medical records of a sample of patients with type II and type III odontoid fractures who had HV therapy in the King Saud Medical City Orthopaedic Department from January 2014 to October 2017.
Inclusion and Exclusion Criteria
The inclusion criteria for this study comprised patients aged between 15 and 44 years with a diagnosis of type II or type III odontoid fractures in which the traumatic mechanism of injury was caused by road traffic accidents or falls and which were initially treated conservatively using an HV. A minimum of 12 months of follow-up was required and all the patients included in the study attended follow-up in the orthopaedic clinic every two weeks after the surgery until the HV was removed. Exclusion criteria included patients below 14 and above 45 years of age, patients who presented with osteolytic lesions, a compression fracture, those who had a history of rheumatoid arthritis or any other inflammatory disease that may lead to odontoid fractures, and patients who had undergone previous cervical spine fixation with a lack of full postoperative follow-up and a lack of computed tomography (CT) scan evaluations of their results.
To allocate the patients to pretreated angulation or displacement groups, we conducted the analysis based on two main domains, displacement type and angulation type, with three subcategories (union, malunion and nonunion), to see which factors offered less stability during HV treatment and had a greater impact on union rate at the fracture level, leading to malunion or nonunion (malunion means the fracture healed crookedly and nonunion means the fracture did not heal and unite the bones).
Radiological Evaluation
None of the selected subjects in this study presented with neurological deficits. All the patients underwent an initial radiographic evaluation of the cervical spine (anterior-posterior, lateral, and open-mouth view). Further evaluation using CT scans was conducted to delineate the extent of the fracture, measure the magnitude of displacement, the degree of the angulation, the vertebrae involved, and the fracture type.
The radiographic evaluation was made for all patients at scheduled follow-up appointments every two weeks for six weeks to monitor the alignment of the odontoid process with the body of C2. Then, at 12 weeks, a CT scan was requested to assess the union status. This series of follow-up X-ray and CT scan evaluations for a few cases from the periphery were obtained at four, eight and 12 weeks. Results are archived on the institution’s system. Through follow-up and radiograph results, we monitored the progress of the treatment by comparing pretreatment angulation and displacement to the latest findings. All measurements were taken by two spine surgeons and were based on a CT scan mid-sagittal view (see Figures 1–4).
 |
Figure 1 Type II odontoid fracture showing 37-degree posterior angulation. |
 |
Figure 2 Type II odontoid fracture showing 4.4 mm anterior displacement. |
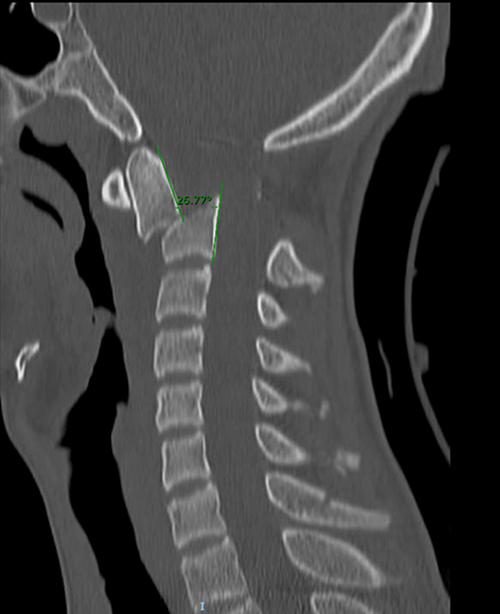 |
Figure 3 Before HV application. Type III odontoid fracture showing 27-degree anterior angulation. |
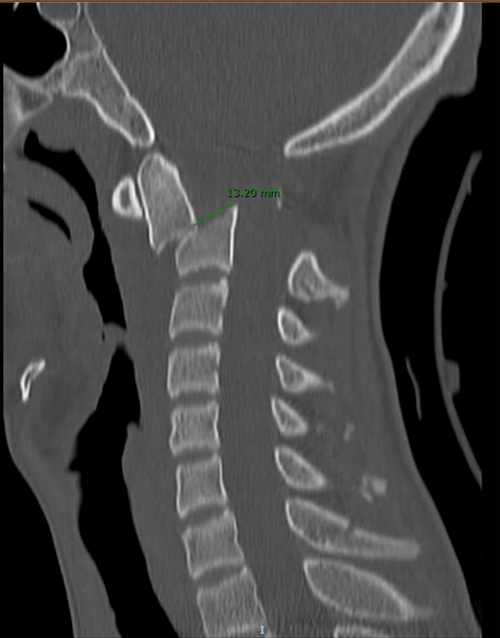 |
Figure 4 Before HV application. Type III odontoid fracture showing 13 mm anterior displacement. |
We used the Smiley-Webster scale through structured telephone interviews to assess the clinical outcome as a subjective response of the patient to grade their functional outcomes. Complications encountered during the treatment period were ascertained from the patients’ hospital charts. Union status was assessed using a CT scan. The union criteria were callus bridging without sclerotic edges or lysis at the centre and integrity of the anterior and posterior cortices. Malunion was defined as odontoid fractures that ended with a complete union in angulation of more than 5 degrees and/or displacement of more than 2 mm.19 The anterior translation of the odontoid fracture fragment concerning the C2 or C3 vertebral body was referred to as displacement. Surgery to fuse the bones was advised whenever alignment or displacement significantly deteriorated.
Ethics Approval
This research has been approved by the institutional review board of the authors’ affiliated institutions (HAPO-01-R-011/05-02-2019), which follows the rules of the National Committee of Bio-Ethics.
Statistical Analysis
Statistical Package for Social Science software, version 27, was used to analyse the data (IBM Corp, Armonk, NY, USA). The patients’ characteristics were described using descriptive statistics. The frequencies and percentages for categorical variables were presented. A Chi-squared test and Fisher’s test and their non-parametric equivalent tests were used to compare proportions for categorical variables.
Results
A total of 45 patients with odontoid fractures were included in this study, of which 55.6% (n = 25) had type II odontoid fractures and 44.4% (n = 20) had type III odontoid fractures. Gender and nationality were included in the data but were not significant in the study. The vast majority of the participants (95.6%) were males. The vast majority (97.8%) of the odontoid fractures among the study participants were caused by road traffic accidents, and only 2.2% were fall-related incidents. More than half of the patients (55.6%) were between 15 and 24 years old. The mean follow-up period ranged from one year to 28 months. Anterior pretreatment displacement contributed to around two-thirds (66.7%) of the cases. Anterior and posterior pretreatment angulation contributed similarly, with 46.7% for each. For further details on the baseline characteristics of the study participants, refer to Table 1.
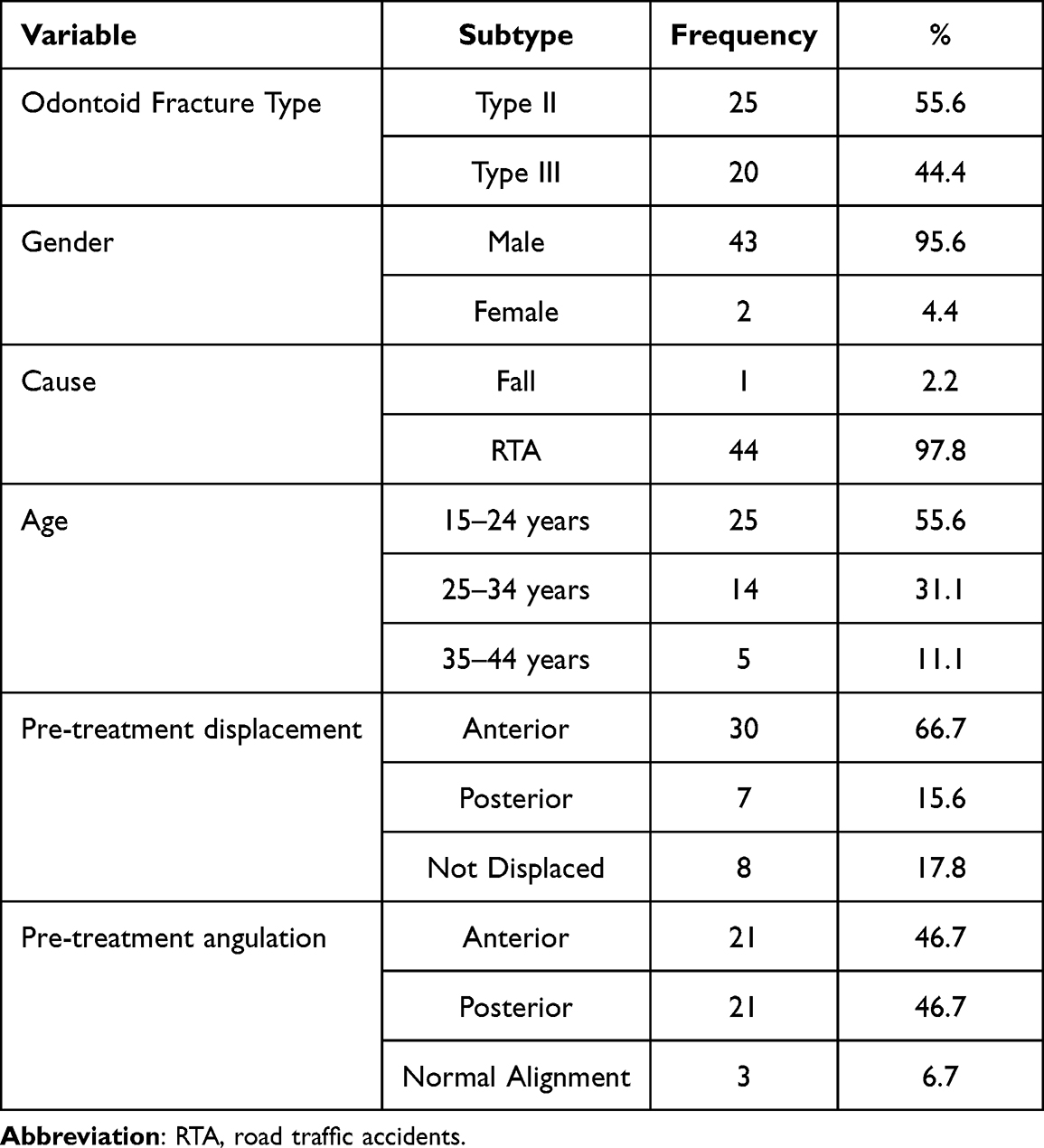 |
Table 1 Characteristics of the Study Participants |
Union Status
In the present study, union was achieved in seven patients (15.56%) with type II odontoid fractures, while 13 patients (28.89%) were malunion and five patients (11.11%) were nonunion. Among patients with type III odontoid fractures, there were seven union cases (15.56%), 11 malunion cases (28.86%), and two nonunion cases (4.44%)(Table 2).
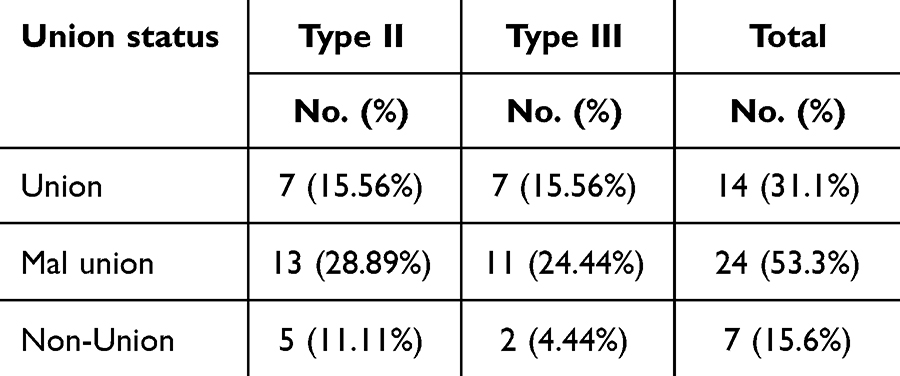 |
Table 2 Distribution of the Studied Cases According to Union Status (n=45) |
Displacement Type
Pretreatment, there was a statistically nonsignificant difference between groups. Posttreatment, there was a statistically significant difference between groups. In the union group, during pretreatment, 42.9% (n = 6) showed anterior displacement, 14.3% (n = 2) had posterior displacement and 42.9% (n = 6) were without displacement. In posttreatment, 21.4% (n = 3) showed anterior displacement, 7.1% (n = 1) had posterior displacement and 71.4% (n = 10) were without displacement. Anterior and posterior displacement decreased by 50%. The number of patients without displacement increased by 67%. Regarding malunion, in pretreatment, 75.% (n = 18) showed anterior displacement, 16.7% (n = 4) had posterior displacement, and 8.3% (n = 2) were without displacement. Posttreatment, 58.3% (n = 14) showed anterior displacement, 12.5% (n = 3) had posterior displacement, and 29.2% (n = 7) were without displacement. Anterior displacement decreased by 22.%. Posterior displacement decreased by 25.%. The number of patients without displacement increased by 250%. Regarding nonunion, in pretreatment, 85.7% (n = 6) showed anterior displacement, 14.3% (n =1) had posterior displacement, and no patients were without displacement. Posttreatment, 85.7% (n =6) showed anterior displacement, 14.3% (n = 1) had posterior displacement, and no patients were without displacement. No change was observed (Table 3).
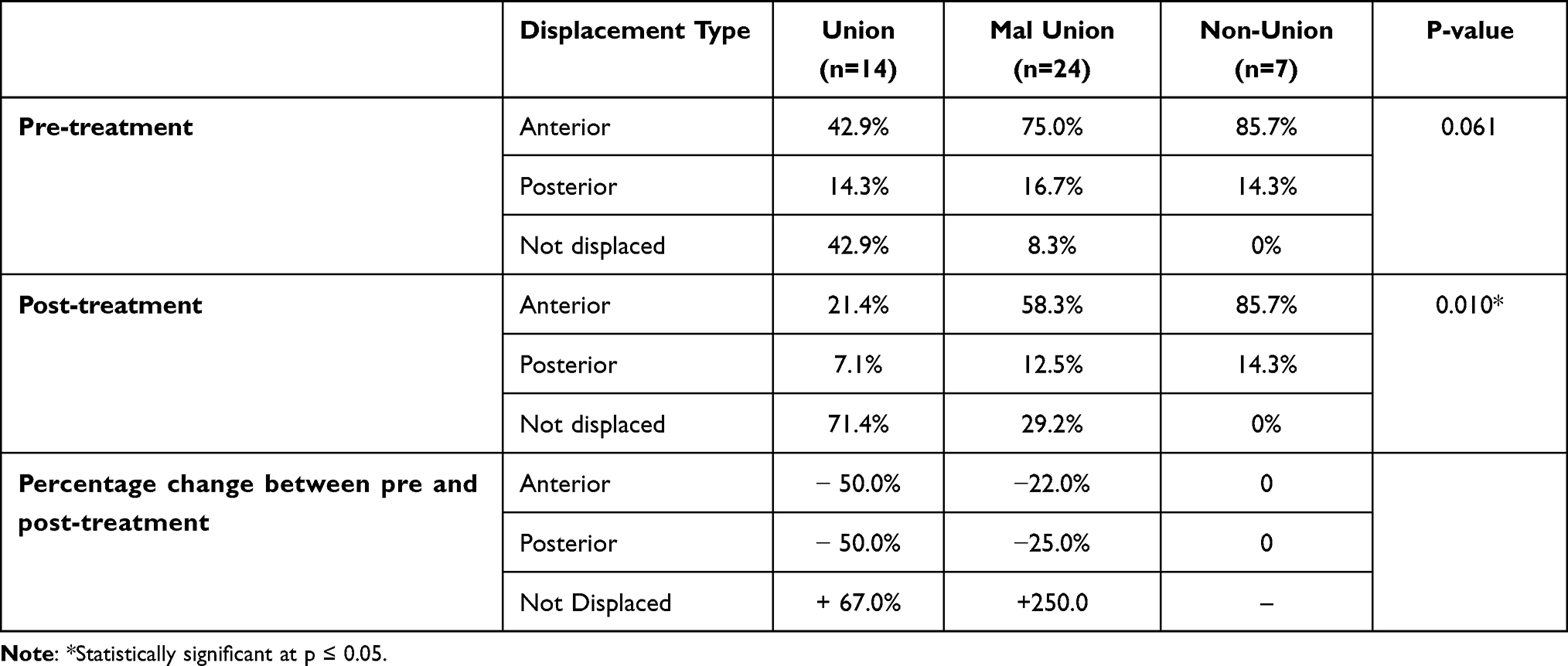 |
Table 3 Comparison Between the Three Studied Groups According to Sub Displacement Type (n=45) |
Thirty patients (66.6%) presented with anterior displacement and seven patients (15.6%) presented with posterior displacement, while the remaining eight patients (17.8%) presented with no displacement. There were 21 cases each of anterior (46.7%) and posterior angulation (46.7%), while the angulation direction varied between anterior (46.7%) and posterior angulation (46.7%) in 21 cases each. Only three cases (6.6%) showed normal angulation.
In the anterior displacement group (66.6%), 20 cases (66.7%) showed anterior angulation on top of the anterior displacement, while the other 10 cases (33.3%) showed posterior angulation on top of the anterior displacement. However, the seven cases (15.6%) that were presented with posterior displacement showed posterior angulation. The magnitude of the displacement and angulation changed after the application of the HV, as shown in Table 2 and Table 3. The fracture angulation tends to shift posteriorly after the application of an HV (Table 3).
Angulation Type
Of the 45 cases, 25 (55.6%) had their angulation altered or forced posteriorly, nine (20%) shifted anteriorly, and the other eight stayed in the posterior angulation zone, except for 11, the angulation of which remained unchanged. We found no evident impact or association between displacement direction and angulation correction following the installation of an HV. We found that a displacement of more than 4 mm is associated with malunion or nonunion in 85.7% of cases. During pretreatment, there was a statistically nonsignificant difference between groups. Posttreatment, there was a statistically significant difference between groups. In the union group, during pretreatment, 42.9% (n = 6) showed anterior angulation, 35.7% (n = 5) had posterior angulation, and 21.4% (n = 3) were without angulation. Posttreatment, 14.3% (n = 2) showed anterior displacement, 28.6% (n = 4) had posterior angulation and 57.1% (n = 8) were without angulation. Anterior angulation decreased by 67.%. Posterior angulation decreased by 20%. The number of patients without angulation increased by 167%. Regarding malunion, during pretreatment, 45.8% (n = 11) showed anterior angulation, 54.2% (n = 13) had posterior angulation, and no cases were without angulation. Posttreatment, 33.3% (n = 8) showed anterior displacement, 66.7% (n = 16) had posterior displacement, and no cases were without displacement. Anterior angulation decreased by 28.% while posterior angulation increased by 23%. Regarding nonunion, during pretreatment, 57.1% (n = 4) showed anterior angulation, 42.9% (n = 3) had posterior displacement, and no cases were without angulation. Posttreatment, 28.6% (n = 2) showed anterior angulation, 71.4% (n = 5) had posterior angulation, and no cases were without angulation. Anterior angulation decreased by 50% and posterior angulation increased by 67% (Table 4).
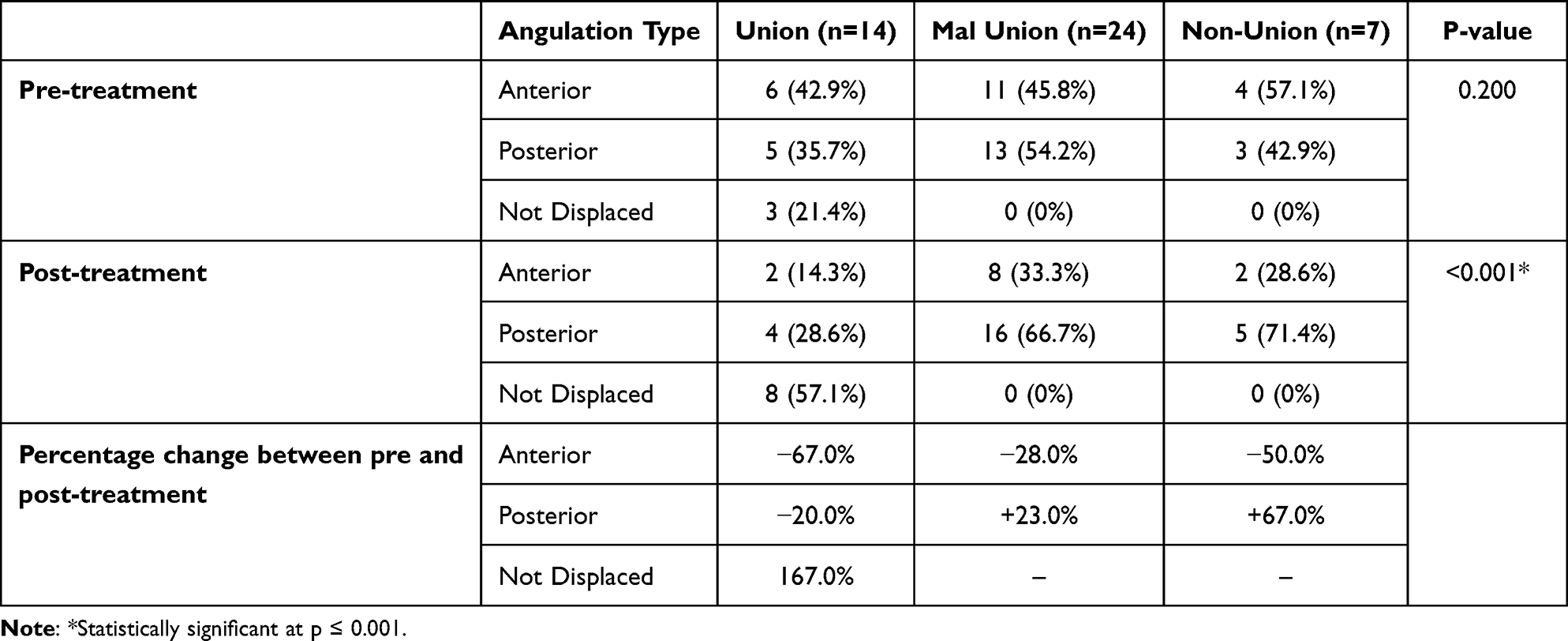 |
Table 4 Comparison Between the Three Studied Groups According to Angulation Type (n=45) |
Based on the outcomes, we divided the patients into three main groups: union, malunion, and nonunion. We tested the effect of displacement and angulation on the union status and found that regardless of age and the level of fracture (type II or III), the worst combination was anterior displacement followed by posterior angulation (58.3%), and ending with malunion, while (33.3%) resulted in nonunion (Table 5). Table 5 presents odontoid fracture posttreatment angulation and displacement outcomes stratified by union type.
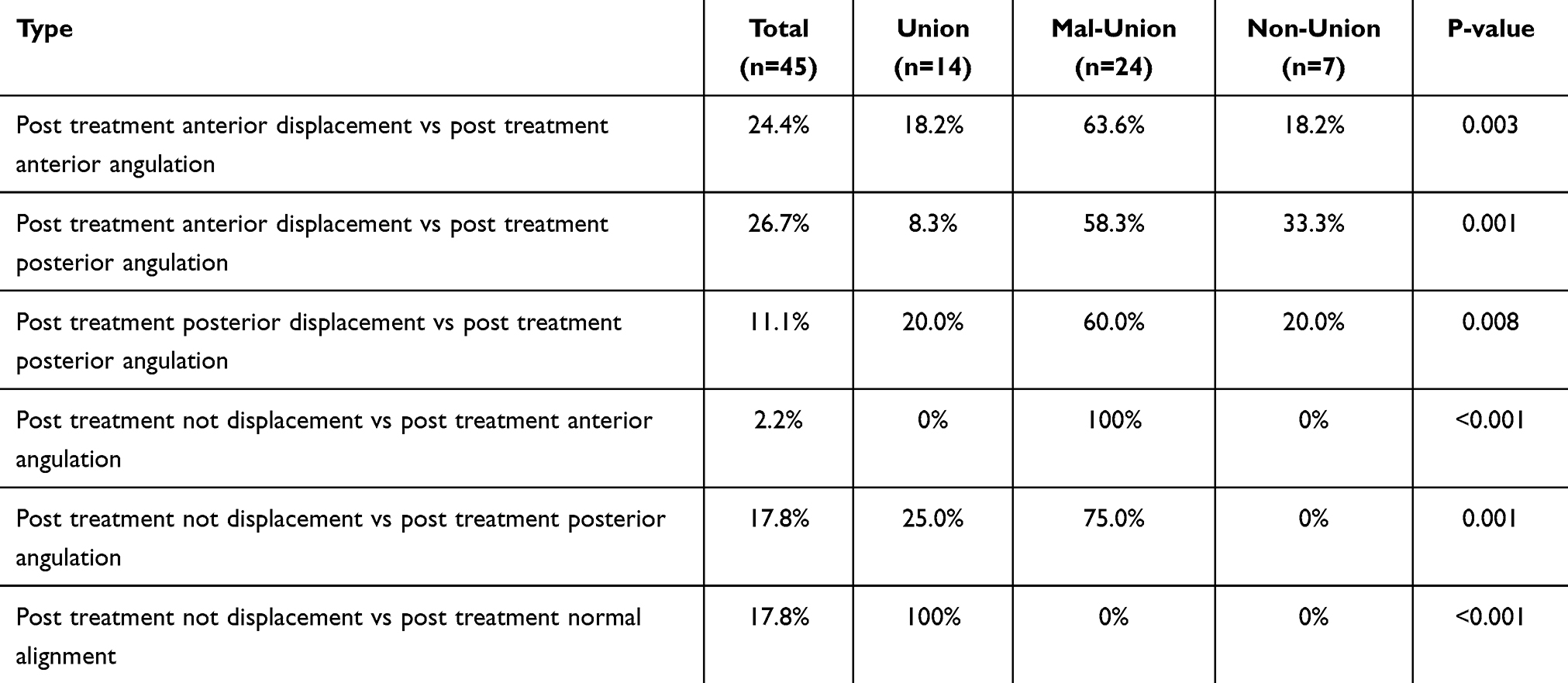 |
Table 5 Comparison Between the Three Studied Groups According to Type (n=45) |
The clinical outcome for 85.7% of the union group was excellent and good for 14.3%. The malunion and nonunion groups had less favourable outcomes; the poor functional outcomes were 16.7% and 42.8%, respectively (Table 6). Figures 5 and 6 present those showing union status four months after the HV application.
 |
Table 6 Comparison Between the Three Studied Groups According to Smiley Webster Scale (n=45) % from Total |
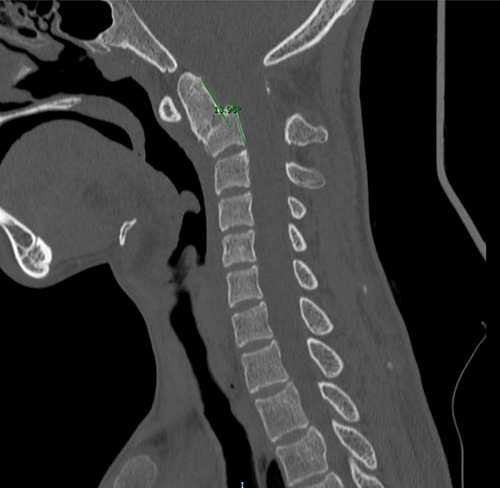 |
Figure 5 Four months after HV application. Type III odontoid fracture showing good union with 14-degree anterior angulation. |
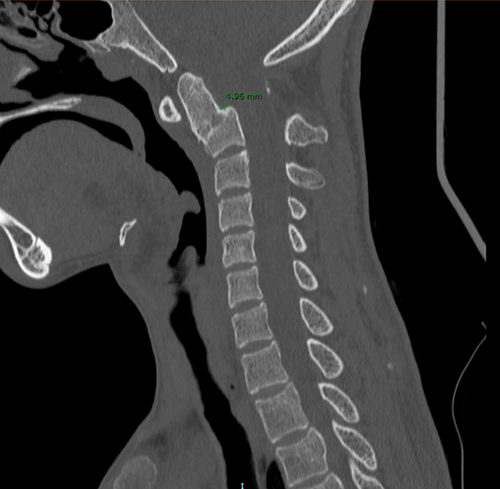 |
Figure 6 Four months after HV application. Type III odontoid fracture showing good union with 5 mm anterior displacement. |
Discussion
The odontoid process is a protrusion of the second cervical vertebra (C2, or the axis). The first cervical vertebra (atlas) rotates around the odontoid process to give the biggest component of the cervical spine’s lateral rotation. Depending on the position and shape of the fracture, fractures of the odontoid process are categorised as type I, type II, or type III fractures.20 A cervical spine injury might result in odontoid fractures. These often originate from high-energy trauma in younger individuals.19 Elderly people may experience trauma after lower-energy impacts, like falls from a standing position. Hyperextension of the cervical spine, which forces the head and C1 vertebrae backward, is the most frequent mechanism of injury. The odontoid fracture with varied displacement and degrees of comminution occurs if the energy mechanism and consequent force are high enough or if the patient’s bone density is reduced as a consequence of osteopenia/osteoporosis.19
Type I and type III odontoid fractures based on the Anderson and D Alonzo classification21 heal well with external immobilisation (with a 100% healing rate for type I and 84% to 88% for type III).11,17 Some studies report nonunion rates between 35% and 85% in nonsurgical management.17,18,22 In the present study, union was achieved in seven patients (15.56%), while 13 patients (28.89%) had malunion and five patients (11.11%) had nonunion in type II odontoid fractures. Type III odontoid fractures had seven cases of union (15.56%), 11 cases of poor union (28.86%), and two cases of nonunion (4.44%). In this study, we tested the effect of displacement and angulation on union status and found that regardless of age and the level of fracture (type II or III), the worst combination was anterior displacement with posterior angulation (58.3%), ending with malunion, while 33.3% resulted in nonunion. The nonunion group was associated with anterior displacement (85.7%) and was divided based on angulation into the anterior angulation subgroup (33.3%), in which the cause of nonunion was the high level of displacement (5–7 mm), and the posterior angulation subgroup (66.7%), in which the amount of displacement was at 1.75 mm but the magnitude of angulation increased dramatically (10–25 degrees) while the displacement remained the same. Due to thin bone trabeculae and a watershed zone at the base of dens, the nonunion rate after conservative care may be as high as 90%.23 Nonsurgical management of odontoid fractures might lead to solid fusion, unstable nonunion, or fibrous nonunion.24 Fusion is influenced by patterns of damage, fracture subclass, the inclination of a fracture line, angulation (more than or equal to 11 degrees), displacement (more or less than 5 mm), life support, bone quality, and the patient’s and fracture’s ages.25 The benefits of employing HVI for odontoid fractures rather than surgery are that it offers stiff immobilisation and a high level of stability for atlantoaxial segments. This is crucial to achieving union because it is less invasive than posterior cervical C1–2 fusion, is well-tolerated by the majority of patients (saving the patients from needless surgery) and preserves axial rotation at C1–2 compared to C1–2 fusion.
The malunion rate in this study was high for two main reasons: The first is the definition of any healed fracture with an angulation of more than 5 degrees and a displacement of more than 2 mm as malunion. Second, micromotion and relative stability at the fracture line provided by the HV, as reported by Kim et al26 and Anderson et al,21 have a great impact on the increased degree of angulation and, eventually, nonunion. We believe that the cases of low nonunion rates are due to the young age group in this study. Clinical outcomes were excellent in 85.7% of patients and good in 14.3% of patients for the union group. The group of malunion and nonunion cases had a less favourable result; the poor functional result was 16.7% and 42.8%, respectively. Kim et al (2011)26 found that 93.3% of patients who had HVI treatment had good or excellent clinical outcomes, as measured on the Smiley-Webster scale. Unfortunately, a high risk of insufficient bone fusion is coupled with external immobilisation, which is also poorly tolerated.26 It has been shown that the HV produced fusion rates of approximately 55% in type II and 50% to 60% in type III injuries.27 According to several studies, surgical treatment has a greater recovery rate for odontoid fractures than nonsurgical treatment.9,28 Clark and White28 documented a 96% recovery rate following posterior surgery and a 68% recovery rate after HVI. Few studies have examined how different treatment approaches affect individuals with odontoid fractures in terms of the healing duration. In this study, the mean bone-healing time was 20 weeks (with a range between 12 and 28 weeks), and the high overall fusion rate (union and malunion group) was 84.4%. Kim et al (2011)26 evaluated the clinical effects of surgical fixation followed by immobilisation using an HV for the treatment of odontoid fractures. They concluded that the overall healing rate after HVI was 60%, and following surgical management, it was 93.8% (see Table 2).
Posterior angulation tends to deteriorate after HV application, while anterior angulation tends to correct to normal or further to the posterior. Apuzzo et al29 reported that the total nonunion rate in undisplaced fractures was 16%, whereas 60% of displaced fractures failed to unite and 88% of fractures displaced more than 4 mm failed to unite. They concluded that the treatment of undisplaced odontoid fractures is appropriate for external immobilisation. Candidates for primary fusion are fractures that have a displacement greater than 4 mm. Kim et al 201126 found that the nonunion rate for a fracture that was displaced by more than 4 mm was 20%. The combination of anterior displacement and posterior angulation was evident in this study in 26.7% of cases; 58.3% of the patients had malunion, and 33.3% had nonunion. Ryken et al and Fujii et al have suggested surgical treatment for fractures with a displacement > 5 mm.30,31 Niemeier et al32 support conservative management of type III odontoid fractures, regardless of their nature or location. A tiny fraction of fractures require fusion surgery since external immobilisation is ineffective for treating the majority of cases.33 If instability is noted or the patient moves to nonunion, delayed surgery can be performed with effective results.34
Obtaining fracture stability is the cornerstone of management.25 The fibrous union may offer sufficient support.35,36 In the absence of instability on flexion/extension views or ligamentous damage on an MRI scan, a stiff brace or HV may be used to facilitate fracture repair, which may occur in 12 weeks.35 A conservative strategy may be justifiable for patients with excellent alignment, no dynamic instability, and no impairments.24 For fracture types I and III in the majority of cases, halo fixation, cervical traction, and a stiff cervical collar result in the fusion of 100% of type 1 fractures, 90% of type III fractures, and 60% of type II fractures.37 Biomechanically, a cervical collar is preferable to halo orthoses, while the risk of concomitant device-related problems is negligible.25 Soft collars provide the same advantages to elderly patients as stiff collars.38 The use of an HV was not linked to an increase in mortality.39 The in-hospital mortality rates for both conservative therapy and surgery were identical.
The clinical and radiological results of this study have justified changes in the treatment protocol for type II odontoid fractures from nonsurgical to surgical treatment that started in October 2018 for all of these fractures. Kim et al26 made significant changes in the treatment protocol in their introduction to surgical treatment based on the correlated increase in nonunion and the complications of this nonsurgical (HV) treatment for odontoid fractures.
Comprehending the biomechanics of odontoid fractures is crucial as it directly impacts the decisions made regarding therapy, and the subsequent results. Biomechanical parameters are also important in predicting future issues, such as a failure of bone-healing or improper bone alignment, and in comprehending the elements that affect the process of tissue repair. The stability of a fracture in the odontoid process is vital in selecting the most suitable approach for treatment. Unstable fractures are frequently treated with surgical fixation to restore stability and alignment. The selection of implants for fixing is determined by the biomechanical characteristics of the fracture and the surgeon’s personal preference. Comprehending the ability of the odontoid process and its surrounding structures to bear weight is crucial for developing efficient treatment strategies.
This study has limitations. The small sample size is one of the main limitations. It restricted our ability to do further inferential analysis. The cross-sectional nature of the study prevented us from examining causality among the study variables.
Conclusion
The HV management for type II and III odontoid fracture requires a prolonged course of cervical immobilisation. We are in an era of surgical intervention for all type II odontoid fractures, in which most cases are treated by HV. Several factors play a role in changing the management protocol: patient compliance, complications associated with HV, and a high rate of reduction loss may eventually lead to malunion or nonunion. Based on our findings, the efficacy of HV treatment for odorous fracture type II and III should be considered for non-displaced fractures.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Ethics Approval
This research has been approved by the IRB at Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia (HAPO-01-R-011/05-02-2019), which follows the rules of the National Committee of Bio-Ethics. All subjects provided written informed consent to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No fund was received for this study.
Disclosure
The authors declare no conflict of interest.
References
1. Whyte T, Stuart CA, Mallory A, et al. A review of impact testing methods for headgear in sports: considerations for improved prevention of head injury through research and standards. J Biomech Eng. 2019;141(7). doi:10.1115/1.4043140
2. Kong T, Lee JW, Park YA, et al. Clinical features of fracture versus concussion of the temporal bone after head trauma. J Audiol Otol. 2019;23(2):96–102. doi:10.7874/jao.2018.00339
3. Hale A. Traumatic occipitocervical distraction injuries in children: a systematic review. Pediatr Neurosurg. 2019;54(2):75–84. doi:10.1159/000496832
4. Goldberg W, Mueller C, Panacek E, et al. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med. 2001;38(1):17–21. doi:10.1067/mem.2001.116150
5. Hsu WK, Anderson PA. Odontoid fractures: update on management. J Am Acad Orthop Surg. 2010;18(7):383–394. doi:10.5435/00124635-201007000-00001
6. Pepin JW, Bourne RB, Hawkins RJ. Odontoid fractures, with special reference to the elderly patient. Clin Orthop Relat Res. 1985;193:178–183. doi:10.1097/00003086-198503000-00025
7. Rief M, Zoidl P, Zajic P, et al. Atlanto-occipital dislocation in a patient presenting with out-of-hospital cardiac arrest: a case report and literature review. J Med Case Rep. 2019;13(1):1–6. doi:10.1186/s13256-018-1926-2
8. Shafafy R, Valsamis EM, Luck J, et al. Predictors of mortality in the elderly patient with a fracture of the odontoid process. Bone Joint J. 2019;101(3):253–259. doi:10.1302/0301-620X.101B3.BJJ-2018-1004.R1
9. Frangen TM, Zilkens C, Muhr G, et al. Odontoid fractures in the elderly: dorsal C1/C2 fusion is superior to halo-vest immobilization. J Trauma. 2007;63(1):83–89. doi:10.1097/TA.0b013e318060d2b9
10. Koivikko MP, Kiuru MJ, Koskinen SK, et al. Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br. 2004;86(8):1146–1151. doi:10.1302/0301-620X.86B8.14839
11. Maak TG, Grauer JN. The contemporary treatment of odontoid injuries. Spine. 2006;31(11S):S53–60. doi:10.1097/01.brs.0000217941.55817.52
12. Ekong CE, Schwartz ML, Tator CH, et al. Odontoid fracture: management with early mobilization using the halo device. Neurosurgery. 1981;9(6):631–637. doi:10.1227/00006123-198112000-00004
13. Lewis E, Liew S, Dowrick A. Risk factors for non‐union in the non‐operative management of type II dens fractures. ANZ J Surg. 2011;81(9):604–607. doi:10.1111/j.1445-2197.2010.05586.x
14. Perry J, Nickel VL. Total cervical-spine fusion for neck paralysis. J Bone Joint Surg. 1959;41(1):37–60. doi:10.2106/00004623-195941010-00006
15. Blount W. Early recognition and prompt evaluation of spinal deformity. J Sch Health. 1970;40(9):514–515.
16. Johnson RM, Owen JR, Hart DL, et al. Cervical orthoses: a guide to their selection and use. Clin Orthop Relat Res. 1981;154:34–45. doi:10.1097/00003086-198101000-00008
17. Sasso R. C2 dens fractures: treatment options. J Spinal Disord. 2001;14(5):455–463. doi:10.1097/00002517-200110000-00015
18. Shin J, Kim SJ, Kim TH, et al. Optimal use of the halo-vest orthosis for upper cervical spine injuries. Yonsei Med J. 2010;51(5):648–652. doi:10.3349/ymj.2010.51.5.648
19. Tenny S, Munakomi S, Varacallo M. Odontoid Fractures; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441956/.
20. Robinson AL, Möller A, Robinson Y, Olerud C. C2 fracture subtypes, incidence, and treatment allocation change with age: a retrospective cohort study of 233 consecutive cases. Biomed Res Int. 2017;2017:1–7.
21. Anderson L, D’Alonzo R. Fractures of the odontoid process of the axis. J Bone Joint Surg Am. 1974;56(8):1663–1674. doi:10.2106/00004623-197456080-00017
22. Tashjian R, Majercik S, Biffl WL, et al. Halo-vest immobilization increases early morbidity and mortality in elderly odontoid fractures. J Trauma. 2006;60(1):199–203. doi:10.1097/01.ta.0000197426.72261.17
23. Sommer F, Kirnaz S, Goldberg J, et al. Treatment of odontoid fractures in elderly patients using C1/C2 instrumented fusion supplemented with bilateral atlantoaxial joint spacers: a case series. Int J Spine Surg. 2022;16(3):442–449. doi:10.14444/8250
24. Florman JE, Gerstl JVE, Kilgallon JL, Riesenburger RI. Fibrous nonunion of odontoid fractures: is it safe to accept nonoperative management? A systematic review. World Neurosurg. 2022;164:298–304. doi:10.1016/j.wneu.2022.05.116
25. Deluca A, Wichlas F, Deininger C, Traweger A, Mueller EJ. Reevaluation of a classification system: stable and unstable odontoid fractures in geriatric patients-a radiological outcome measurement. Euro J Trauma Emerg Surg. 2022;48(4):2967–2976. doi:10.1007/s00068-022-01985-0
26. Kim S, Shin JJ, Kim TH, et al. Clinical outcomes of halo-vest immobilization and surgical fusion of odontoid fractures. J Korean Neurosurg Soc. 2011;50(1):17–22. doi:10.3340/jkns.2011.50.1.17
27. Hadley M, Dickman CA, Browner CM, et al. Acute axis fractures: a review of 229 cases. J Neurosurg. 1989;71(5 Pt 1):642–647. doi:10.3171/jns.1989.71.5.0642
28. Clark C, White A. Fractures of the dens. A multicenter study. J Bone Joint Surg Am. 1985;67(9):1340–1348. doi:10.2106/00004623-198567090-00006
29. Apuzzo M. Acute fractures of the odontoid process. An analysis of 45 cases. J Neurosurg. 1978;48(1):85–91. doi:10.3171/jns.1978.48.1.0085
30. Fujii E, Kobayashi K, Hirabayashi K. Treatment in fractures of the odontoid process. Spine. 1988;13(6):604–609. doi:10.1097/00007632-198813060-00002
31. Ryken T, Hadley MN, Aarabi B, et al. Management of isolated fractures of the axis in adults. Neurosurgery. 2013;72(Suppl 2):132–150. doi:10.1227/NEU.0b013e318276ee40
32. Niemeier T, Dyas A, Manoharan S, et al. Type III odontoid fractures: a subgroup analysis of complex, high-energy fractures treated with external immobilization. J Craniovertebr Junction Spine. 2018;9(1):63–67. doi:10.4103/jcvjs.JCVJS_152_17
33. Goel A, Jain S, Shah A, et al. Atlantoaxial fixation for odontoid fracture: analysis of 124 surgically treated cases. World Neurosurg. 2018;110:558–567. doi:10.1016/j.wneu.2017.08.192
34. Smith J, Kepler CK, Kopjar B, et al. Effect of type II odontoid fracture nonunion on outcome among elderly patients treated without surgery: based on the AOSpine North America geriatric odontoid fracture study. Spine. 2013;38(26):2240–2246. doi:10.1097/BRS.0000000000000009
35. Wilson C, Hoyos M, Huh A, et al. Institutional review of the management of type II odontoid fractures: associations and outcomes with fibrous union. J Neurosurg Spine. 2021;34(4):623–631. doi:10.3171/2020.8.SPINE20860
36. Sucu HK. A true percutaneous anterior odontoid screw fixation: the results of 42 cases by a single surgeon. World Neurosurg. 2022;166:e892–e904. doi:10.1016/j.wneu.2022.07.125
37. Apfelbaum R, Rao G. Odontoid screw fixation for fresh and remote fractures. Neurol India. 2005;53(4):416–423. doi:10.4103/0028-3886.22607
38. Coleman N, Chan HH, Gibbons V, Baker JF. Comparison of hard and soft cervical collars for the management of odontoid peg fractures in the elderly. Geriat Orthopa Surg Rehabil. 2022;13:1–9. doi:10.1177/21514593211070263
39. Honda A, Michihata N, Iizuka Y, et al. Clinical features and early post-operative complications of isolated C2 odontoid fractures: a retrospective analysis using a national inpatient database in Japan. Euro Spine J. 2021;30(12):3631–3638. doi:10.1007/s00586-021-06862-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.