Back to Journals » Vascular Health and Risk Management » Volume 19
Clinical and Morphological Factors for Ruptured Anterior Communicating Artery Aneurysms
Authors Rilianto B ![]() , Prasetyo BT, Kurniawan RG, Gotama KT
, Prasetyo BT, Kurniawan RG, Gotama KT ![]() , Windiani PR
, Windiani PR ![]() , Arham A, Kusdiansah M
, Arham A, Kusdiansah M
Received 21 April 2023
Accepted for publication 21 June 2023
Published 30 June 2023 Volume 2023:19 Pages 371—377
DOI https://doi.org/10.2147/VHRM.S415213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Beny Rilianto,1,2,* Bambang Tri Prasetyo,1,2,* Ricky Gusanto Kurniawan,1,2,* Kelvin Theandro Gotama,1 Pratiwi Raissa Windiani,1 Abrar Arham,2,3 Muhammad Kusdiansah2,3
1Neurointervention Division, National Brain Center Hospital Prof. Dr. dr. Mahar Mardjono, East Jakarta, Indonesia; 2Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 3Neurosurgery Department, National Brain Center Hospital Prof. Dr. dr. Mahar Mardjono, East Jakarta, Indonesia
*These authors contributed equally to this work
Correspondence: Beny Rilianto, Neurointervention Division, National Brain Center Hospital Prof. Dr. dr. Mahar Mardjono, MT Haryono St No. Kav.11, Cawang, Kramat Jati, East Jakarta, Jakarta, 13630, Indonesia, Tel +62 21 29373377, Email [email protected]
Introduction: The anterior communicating artery (ACoA) aneurysm, the most frequent cerebral aneurysm to rupture, carries a significant clinical burden, yet the factors influencing its rupture are limited in Indonesia. This study aims to determine the clinical and morphological features associated with ruptured ACoA compared to non-AcoA aneurysms among Indonesians.
Patients and Methods: We retrospectively reviewed our center’s aneurysm patient registry from January 2019 to December 2022, and compared the clinical and morphological features between ruptured ACoA aneurysms and ruptured aneurysms elsewhere with univariate and multivariate analyses.
Results: Of the 292 patients with 325 ruptured aneurysms, 89 were from ACoA. The mean age of patients was 54.99 years, with female preponderance in the non-ACoA group (non-ACoA: 73.31%, ACoA: 46.07%). On univariate analysis, ages ≥ 60 [ages 60– 69: OR = 0.311 (0.111– 0.869), p= 0.026; ages ≥ 70: OR = 0.215 (0.056– 0.819), p= 0.024], female gender [OR = 0.311 (0.182– 0.533), p< 0.001], and smoking [OR=2.069 (1.036– 4.057), p= 0.022] exhibited significant association with ruptured ACoA aneurysm. On multivariate analysis, only the female gender was independently associated with ruptured ACoA aneurysm (aOR 0.355 [0.436– 1.961], p=0.001).
Conclusion: In our study, ruptured ACoA aneurysm was inversely associated with advanced age, female gender, presence of daughter aneurysm, and directly associated with smoking. After multivariate adjustment, the female gender showed an independent association with ruptured ACoA aneurysm.
Keywords: ACoA aneurysm, ruptured, morphology, risk factor, Indonesian population
Introduction
Cerebral aneurysm is a pathological bulging of the wall of blood vessels in the brain, which, when ruptured, can lead to aneurysmal subarachnoid hemorrhage (aSAH). The estimated prevalence of cerebral aneurysm is at 0.5–6% globally and although the consequent aSAH constitutes only 5% of all stroke cases, the condition carries a significant clinical burden.1–4 Half of aSAH patients are under 55 years old, one-third of patients do not survive the first days to weeks post bleeding, and a majority of those who do have to endure lifelong cognitive and functional impairment.4 Mortality associated with the rupture of cerebral aneurysms comprises up to 25% of all deaths from cerebrovascular diseases.5
The anterior communicating artery (ACoA) remains the most common site for intracranial aneurysms, with 30–37% of all cerebral aneurysms localized here.5,6 ACoA aneurysms are also the most frequent to rupture, accounting for up to 40% of aSAH.7,8 Being adjacent to a number of important blood vessels and structures, the complex management of ACoA aneurysms – ie, surgical clipping, endovascular coiling – carries notable potential iatrogenic complications and financial burden.5,7 Accordingly, an understanding of factors that contribute to the rupture of ACoA aneurysms is of considerable value to physicians in treatment decision-making.
Multiple studies have identified several clinical – eg, age, gender, hypertension, family history of cerebral aneurysms, smoking – and morphological – eg, aneurysmal location, size, number – parameters related to the rupture of cerebral aneurysms, and scoring systems such as PHASES and the Unruptured Intracranial Aneurysm Treatment Score (UIATS) have been devised to predict rupture risk.2,5,8–12 However, in addition to displaying geographical variation, a consensus on which of these variables are consistent descriptors of rupture risk is nonexistent and, inevitably, the applicability of scoring systems in guiding treatment plans remains questionable.8,12–15
In Indonesia, where epidemiological knowledge on cerebral aneurysms remains limited, the risk factors associated with ACoA aneurysm rupture are poorly understood. Moreover, due to inadequate screening, more patients in Indonesia are only admitted to the hospital once their aneurysm has ruptured. Therefore, this study aims to determine the clinical and morphological factors associated with ruptured ACoA aneurysms among Indonesian patients, compared to cerebral aneurysms of other origin.
Materials and Methods
Ethics Approval
Our study protocol was reviewed and approved by the Committee of Research Ethics of the National Brain Center Hospital, Jakarta, Indonesia (approval number LB.02.01/KEP/102/2022). The ethics committee decided that informed consent was not required for this study, as no personal information of patients was included. This study was conducted in compliance with the Declaration of Helsinki.
Patient Selection
We retrospectively reviewed the cerebral aneurysm patient registry at the National Brain Center Hospital, Jakarta, and looked at admissions from 1 January 2019 to 31 December 2022. We excluded patients with unruptured aneurysms and/or incomplete clinical or morphological data. Data obtained for analysis included clinical variables as well as morphological parameters.
Clinical Variables
The ruptured cerebral aneurysm variable was divided into ACoA and other than ACoA. Clinical variables obtained for analysis were age and gender; personal history of hypertension, diabetes mellitus, and/or dyslipidemia; smoking; and family history of cerebrovascular disease. Hypertension was defined as systolic blood pressure of ≥140 mmHg and/or diastolic blood pressure of ≥90 mmHg preceding the onset of SAH; or regular usage of one or more antihypertensive agents. Diabetes mellitus was defined as a fasting blood glucose level of ≥126 mg/dL, random blood glucose level of ≥200 mg/dL in the presence of classic clinical manifestations (polyuria, polydipsia, polyphagia, unexplained weight loss), and/or HbA1c level of ≥6.5%; or usage of antidiabetic agents and/or insulin injection. Dyslipidemia was defined as a total cholesterol level of ≥200 mg/dL, HDL levels of ≤ 40 mg/dL, LDL levels of ≥ 100 mg/dL, and/or triglyceride levels of ≤150 mg/dL; or the use of lipid-lowering agents. Family history of cerebrovascular disease was considered relevant when concerning first- or second-degree relatives. Smoking status was considered positive for patients who were active smokers, and negative for patients who have never smoked before or were past smokers.
Morphological Parameters
The morphological parameters of interest for analysis in this study were the aneurysmal size and the presence of a daughter aneurysm. Aneurysmal size was based on the dome diameter and classified into three groups: small (<5 mm), medium (5–10 mm), and large (>10 mm). These size thresholds were based on previously established classifications seen in the IAUTS while taking into account that most aneurysms identified in the Asian population were of sizes less than 5 mm.6,16,17 Readings of morphological parameters were obtained with angiography, using the DSA-3D tool: Philips Allura Xpert FD 20 X-Ray system with 258° complex rotation scan and the XIOM Artis® C-arm (Siemens Healthcare, Erlangen, Germany) with 360° complex rotation scan.
Statistical Analysis
Data analysis was carried out using STATA statistical software version 17.0 (StataCorp, Texas, USA). Numerical variables were represented as mean and standard deviation if normally distributed, or as percentage (%) when appropriate. Categorical variables were represented as frequency and percentage (%). Univariate analysis with a Chi-square test was performed to determine differences in the occurrence of clinical and morphological variables between groups of ACoA aneurysms and aneurysms elsewhere. For variables with p<0.1 on univariate analysis, multivariate regression analysis was performed. Variables with p<0.05 on multivariate analysis were independently associated with ruptured ACoA aneurysm. For each variable, an odds ratio (OR) with a 95% confidence interval (CI) was also obtained.
Results
Between January 2019 and December 2022, our cerebral aneurysm registry recorded 369 patients with 412 cerebral aneurysms. From these, 77 patients with 80 unruptured aneurysms were excluded. From the remaining 292 patients, 7 out of 332 ruptured aneurysms had incomplete morphological data and were excluded. The final 292 patients with 325 ruptured cerebral aneurysms (322 saccular) were included in the analysis (Figure 1). The anterior communicating artery was the most common site of ruptured cerebral aneurysms (89; 27%), followed by the posterior communicating artery (82; 25%), internal carotid artery (60; 18%), middle cerebral artery (50; 15%), and anterior cerebral artery (23; 6%). Other aneurysmal sites identified among our patients were the basilar, vertebral, ophthalmic, and superior cerebellar arteries.
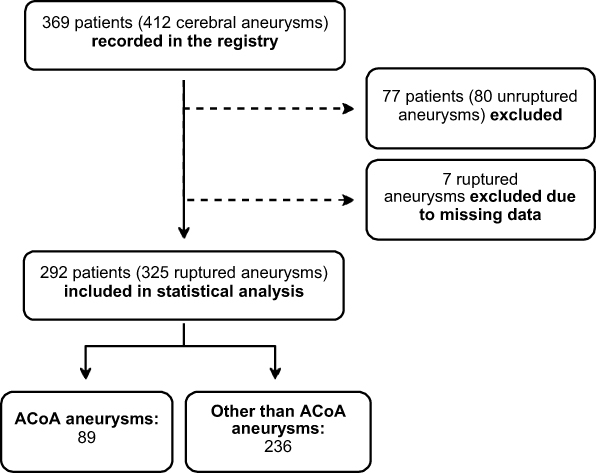 |
Figure 1 Subject selection flow chart. |
Clinical and morphological features of the subjects can be seen in Table 1. More than half of patients with ruptured aneurysms were female (65%), and the majority of them developed aneurysms in other cerebral arteries (73% of non-ACoA aneurysms). On univariate analysis, the female gender was inversely associated with ruptured ACoA aneurysms, with a significant difference between groups (OR 0.31, 95% CI [0.18–0.53], p<0.001).
 |
Table 1 Clinical and Morphological Features of Subjects |
Most patients were less than 60 years old (mean age ± SD: 54.99 ± 11.26 years), comprising the majority of those with ruptured ACoA aneurysms (81%) and ruptured aneurysms elsewhere (60%). The preponderance of younger patients was also seen on univariate analysis; there was a significant inverse association between ages 60 or older and ruptured ACoA aneurysms (age group 60–69: OR 0.31, 95% CI [0.11–0.87], p=0.026; age group ≥70: OR 0.22, 95% CI [0.06–0.82], p=0.024).
Hypertension was the most prevalent risk factor among patients across both groups of ruptured aneurysms, yet it showed no statistical significance on univariate analysis. In fact, of all clinical risk factors, smoking was the only one to exhibit a significant association with ruptured ACoA aneurysms on univariate analysis (OR 2.07, 95% CI [1.04–4.06], p=0.022).
Most of the aneurysms in our patients were smaller than 5 mm, making up 65% of ruptured ACoA aneurysms (mean size ± SD = 5.25 ± 3.53) and 59% of ruptured aneurysms elsewhere (mean size ± SD = 5.37 ± 2.88). Nevertheless, on univariate analysis, aneurysmal size was statistically insignificant. The presence of a daughter aneurysm, however, showed a significant inverse association (OR 0.36, 95% CI [0.90–1.09], p=0.057).
On multivariate analysis (Table 2), after adjustment, the female gender was independently associated with ruptured ACoA aneurysms (aOR 0.355, 95% CI [0.436–1.961], p=0.001). Other variables showed no significant difference in multivariate analysis.
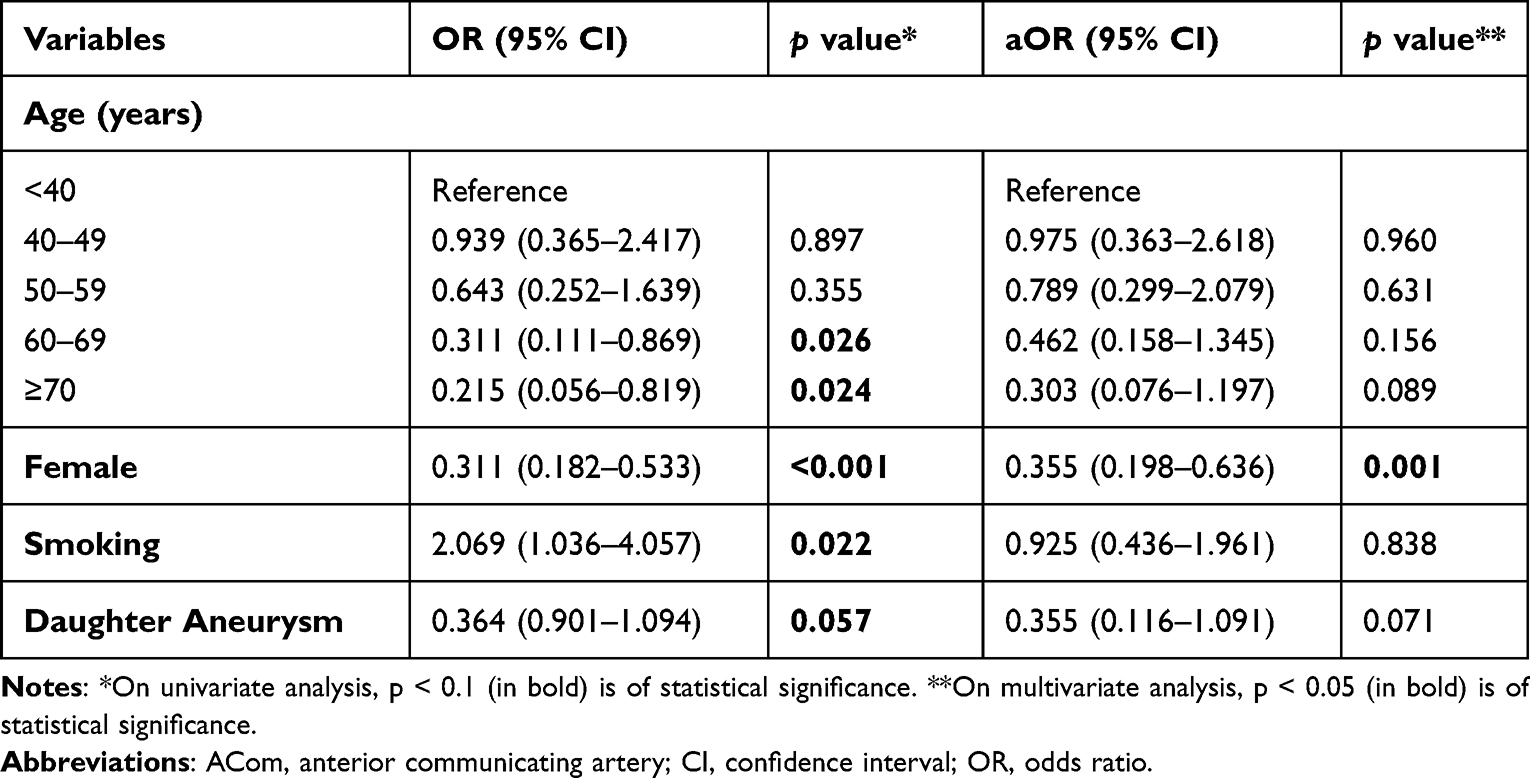 |
Table 2 Multivariate Analysis of Factors Associated with Ruptured ACoA Aneurysm |
Discussion
We found that ACoA aneurysms accounted for the majority of ruptured cerebral aneurysms among our patients, confirming previous reports that they were the most frequent to rupture.5–8 Studies have shown that patients with ACoA aneurysms are more likely to present with worse neurological deficits, have a higher likelihood of vasospasm, and have poorer outcomes, all of which are tied to ACoA aneurysms’ greater rupture risk.10 This is to be expected from ACoA’s proximity to important structures like the frontal cortex and optic chiasm.18 Thus, an understanding of factors that influence the rupture of ACoA aneurysms is of considerable clinical value.
In our study, the female displayed a significantly inverse association with ruptured ACoA aneurysms. With respect to gender—the only independent factor after multivariate adjustment—our finding agrees with previous investigations by Park et al in South Korea, Lindner et al in the Netherlands, Krzyżewski et al in Poland, and Zhang et al in the US, female was found to be a risk factor for the growth of unruptured especially in older patients and localizes preferentially in the internal carotid artery, whereas men had ruptured aneurysms at the ACoA and anterior cerebral artery more frequently.19–22 Many factors related to growth aneurysms and the risk of rupture are slightly different between males and females. In males, most of the risk factors include hypertension, atherosclerosis, and smoking, while the postmenopausal state is found as a risk factor for females.23
Older age was associated with ruptured ACoA aneurysms, results from previous studies were inconsistent; Matsukawa et al also reported that Japanese patients with ruptured ACoA aneurysms were significantly younger and the majority of them were less than 60, yet Kim et al and Zhang et al found no significant difference in age.6,10,21 Conversely, Lindner et al found that when compared to ACoA, aneurysms that ruptured in other sites were more likely to occur in younger patients.20
Based on vascular risk factors, hypertension was the most frequently encountered risk factor in both groups. However, on univariate analysis, most clinical risk factors failed to exhibit significant association with ruptured ACoA aneurysms apart from smoking. Hypertension and smoking have long been known to promote the formation as well as rupture of cerebral aneurysms, by inducing endothelial dysfunction and vascular inflammation, thus compromising vascular wall integrity.9,24,25 Thus, confirming prior studies, our findings demonstrated that no single vascular risk factor is independently associated with ruptured ACoA aneurysms.
In both ACoA and non-ACoA aneurysm groups, most aneurysms were less than 5 mm. We also found that aneurysmal size was not significantly associated with the location of aneurysm rupture. A previous Indonesian study by Swatan et al found that most ruptured aneurysms were less than 5 mm in size, with ACoA as the most frequent location.16 Similarly, Kim et al found that in South Korea, 55% of ruptured aneurysms were <4 mm in size, and Lai et al reported that most ruptured aneurysms in the Hong Kong Chinese population were 5 mm or smaller.6,17 In contrast, studies on the Japanese and Finnish populations reported bigger aneurysmal size, averaging at 7 mm.17,25 Additionally, Matsukawa et al in Japan demonstrated that a larger aneurysmal size of ≥5 mm was significantly associated with ACoA aneurysm rupture.10 It appears that among Asian populations other than Japan, aneurysms rupture at smaller sizes more frequently.
We found that the presence of a daughter aneurysm was inversely associated with ruptured ACoA aneurysms. In contrast, Chen et al found that the presence of a daughter dome was a risk factor for ACoA aneurysm rupture.26 Liu et al also found that aneurysm lobulations, including daughter sac, were significantly more frequent in ruptured than unruptured ACoA aneurysms.25 Our result shows that the presence of a daughter aneurysm may affect the rupture of aneurysms in other sites more than ACoA.
Several limitations of this study exist. This retrospective study utilized patients from a single center. Many morphological parameters of aneurysms could be potentially analyzed, like dome-neck ratio and size ratio, presence of aplastic or hypoplasia, and hemodynamics of aneurysms. Further investigations with prospective, multi-center data accrual and analysis of more morphological measurements are still needed.
Conclusion
We found that ruptured ACoA aneurysm among our patients was associated with advanced age, female, smoking, and the presence of a daughter aneurysm. Of these, only the female exhibited an independent inverse association with ruptured ACoA aneurysms. The relationship between the rupture of cerebral aneurysm and its risk factors remains complex, as evident by the variance between populations. Nevertheless, our investigation may help elucidate the clinical profile of ruptured ACoA aneurysms in Indonesia.
Data Sharing Statement
The data sets supporting the conclusions of this article are available upon reasonable request to the corresponding author.
Acknowledgments
The authors gratefully acknowledge National Brain Center Hospital Prof. Dr. dr. Mahar Mardjono for supporting this study.
Author Contributions
BR, BTP, RGK, AA, and MK contributed to the conception and design of the study. BR, BTP, and RGK collected the data utilized in the study. BR, KTG, and PRW conducted the data analysis and wrote the manuscript. All authors contributed to the manuscript revision, approved the final draft of the manuscript as well as the journal for publication, and agreed to be accountable for all aspects of the study.
Funding
This study was funded and supported by Medtronic and Balt.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Bijlenga P, Ebeling C, Jaegersberg M, et al. Risk of rupture of small anterior communicating artery aneurysms is similar to posterior circulation aneurysms. Stroke. 2013;44(11):3018–3026. doi:10.1161/STROKEAHA.113.001667
2. Zuurbier CCM, Molenberg R, Mensing LA, et al. Sex difference and rupture rate of intracranial aneurysms: an individual patient data meta-analysis. Stroke. 2022;53(2):362–369. doi:10.1161/STROKEAHA.121.035187
3. Juvela S, Poussa K, Lehto H, Porras M. Natural history of unruptured intracranial aneurysms: a long-term follow-up study. Stroke. 2013;44(9):2414–2421. doi:10.1161/STROKEAHA.113.001838
4. Etminan N, Chang HS, Hackenberg K, et al. Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region, time period, blood pressure, and smoking prevalence in the population: a systematic review and meta-analysis. JAMA Neurol. 2019;76(5):588–597. doi:10.1001/jamaneurol.2019.0006
5. Cai W, Hu C, Gong J, Lan Q. Anterior communicating artery aneurysm morphology and the risk of rupture. World Neurosurg. 2018;109:119–126. doi:10.1016/j.wneu.2017.09.118
6. Kim MC, Hwang SK. The rupture risk of aneurysm in the anterior communicating artery: a single center study. J Cerebrovasc Endovasc Neurosurg. 2017;19(1):36–43. doi:10.7461/jcen.2017.19.1.36
7. Chen J, Li M, Zhu X, et al. Anterior communicating artery aneurysms: anatomical considerations and microsurgical strategies. Front Neurol. 2020;11:1020. doi:10.3389/fneur.2020.01020
8. Xie Y, Tian H, Xiang B, Li D, Liu YZ, Xiang H. Risk factors for anterior communicating artery aneurysm rupture: a protocol for systematic review and meta-analysis. Medicine. 2021;100(48):e28088.
9. Kaspera W, Ladzinski P, Larysz P, et al. Morphological, hemodynamic, and clinical independent risk factors for anterior communicating artery aneurysms. Stroke. 2014;45(10):2906–2911. doi:10.1161/STROKEAHA.114.006055
10. Matsukawa H, Uemura A, Fujii M, Kamo M, Takahashi O, Sumiyoshi S. Morphological and clinical risk factors for the rupture of anterior communicating artery aneurysms. J Neurosurg. 2013;118(5):978–983. doi:10.3171/2012.11.JNS121210
11. Greving JP, Wermer MJ, Brown RD Jr, et al. Development of the phases score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 2014;13(1):59–66. doi:10.1016/S1474-4422(13)70263-1
12. Neulen A, Pantel T, Konig J, Brockmann MA, Ringel F, Kantelhardt SR. Comparison of unruptured intracranial aneurysm treatment score and phases score in subarachnoid hemorrhage patients with multiple intracranial aneurysms. Front Neurol. 2021;12:616497. doi:10.3389/fneur.2021.616497
13. Pagiola I, Mihalea C, Caroff J, et al. The phases score: to treat or not to treat? Retrospective evaluation of the risk of rupture of intracranial aneurysms in patients with aneurysmal subarachnoid hemorrhage. J Neuroradiol. 2020;47(5):349–352. doi:10.1016/j.neurad.2019.06.003
14. Rutledge C, Jonzzon S, Winkler EA, Raper D, Lawton MT, Abla AA. Small aneurysms with low phases scores account for most subarachnoid hemorrhage cases. World Neurosurg. 2020;139:e580–e4. doi:10.1016/j.wneu.2020.04.074
15. Neyazi B, Sandalcioglu IE, Maslehaty H. Evaluation of the risk of rupture of intracranial aneurysms in patients with aneurysmal subarachnoid hemorrhage according to the phases score. Neurosurg Rev. 2019;42(2):489–492. doi:10.1007/s10143-018-0989-2
16. Swatan JP, Sani AF, Kurniawan D, Swatan H, Husain S. What are the predictors of intracranial aneurysm rupture in Indonesian population based on angiographic findings? Insight from intracranial aneurysm registry on three comprehensive stroke centres in Indonesia. Stroke Res Treat. 2022;2022:1–6. doi:10.1155/2022/4787048
17. Lai HP, Cheng KM, Yu SC, et al. Size, location, and multiplicity of ruptured intracranial aneurysms in the Hong Kong Chinese population with subarachnoid haemorrhage. Hong Kong Med J. 2009;15(4):262–266.
18. Wang GX, Wang S, Liu LL, et al. A simple scoring model for prediction of rupture risk of anterior communicating artery aneurysms. Front Neurol. 2019;10:520. doi:10.3389/fneur.2019.00520
19. Park SK, Kim JM, Kim JH, Cheong JH, Bak KH, Kim CH. Aneurysmal subarachnoid hemorrhage in young adults: a gender comparison study. J Clin Neurosci. 2008;15(4):389–392. doi:10.1016/j.jocn.2007.04.007
20. Lindner SH, Bor AS, Rinkel GJ. Differences in risk factors according to the site of intracranial aneurysms. J Neurol Neurosurg Psychiatry. 2010;81(1):116–118. doi:10.1136/jnnp.2008.163063
21. Zhang J, Can A, Lai PMR, et al. Vascular geometry associated with anterior communicating artery aneurysm formation. World Neurosurg. 2021;146:e1318–e25. doi:10.1016/j.wneu.2020.11.160
22. Krzyzewski RM, Klis KM, Kucala R, et al. Intracranial aneurysm distribution and characteristics according to gender. Br J Neurosurg. 2018;32(5):541–543. doi:10.1080/02688697.2018.1518514
23. Fréneau M, Baron-Menguy C, Vion A-C, Loirand G. Why are women predisposed to intracranial aneurysm? Front Cardiovasc Med. 2022;9:815668. doi:10.3389/fcvm.2022.815668
24. Xia N, Liu Y, Zhong M, et al. Smoking associated with increased aneurysm size in patients with anterior communicating artery aneurysms. World Neurosurg. 2016;87:155–161. doi:10.1016/j.wneu.2015.11.094
25. Korja M, Kivisaari R, Jahromi BR, Lehto H. Size and location of ruptured intracranial aneurysms: consecutive series of 1993 hospital-admitted patients. J Neurosurg. 2017;127(4):748–753. doi:10.3171/2016.9.JNS161085
26. Chen Y, Xing H, Lin B, et al. Morphological risk model assessing anterior communicating artery aneurysm rupture: development and validation. Clin Neurol Neurosurg. 2020;197:106158. doi:10.1016/j.clineuro.2020.106158
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.