")
Back to Journals » Infection and Drug Resistance » Volume 16
Clinical and Microbiological Characteristics of Candidemia Cases in Saudi Arabia
Authors Alkhalifa W , Alhawaj H, Alamri A , Alturki F, Alshahrani M , Alnimr A
Received 18 April 2023
Accepted for publication 21 June 2023
Published 10 July 2023 Volume 2023:16 Pages 4489—4503
DOI https://doi.org/10.2147/IDR.S411865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Wala Alkhalifa,1 Hassan Alhawaj,1 Aisha Alamri,2 Fatimah Alturki,1 Mohammed Alshahrani,3 Amani Alnimr1
1Department of Microbiology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Department of Clinical Laboratory Sciences, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Emergency and Critical Care Department, King Fahad Hospital of the University - Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Wala Alkhalifa, 2722 Al Jouri Street, Saihat, Saudi Arabia, Tel +966 551873892, Email [email protected]
Purpose: Candidemia and antifungal resistance are major healthcare challenges. The aim of this study is to describe the frequency of candidemia cases, distribution of Candida spp., and the associated risk factors for mortality in an academic institution in Saudi Arabia over an 18-month period. We also evaluated the susceptibility patterns of Candida blood isolates.
Methods: Candidemia cases were collected from King Fahad Hospital of the University over the period between July 1st, 2020 through December 31st, 2021. They were prospectively reviewed for the preceding risk factors and antifungal (AF) susceptibility, testing results to fluconazole (FL), voriconazole (VO), itraconazole (IT), posaconazole (PO), caspofungin (CASP), anidulafungin (AND), micafungin (MYC), flucytosine (FLC) and amphotericin B (AMPB) using a broth microdilution kit (Sensititre™ YeastOne).
Results: A total of 48 candidemia isolates were included that were isolated from 43 patients. The median age of cases was 62 ± 23.3 years (60.4% males and 83% ICU patients). Independent risk factors for mortality at 30 days in candidemia patients were age, COVID-19 co-infection, and use of tocilizumab. The most commonly isolated species were C. glabrata and C. parapsilosis (22.9% each) followed by C. albicans (18.75%). AF resistance for ≥ 1 antifungal was detected in 39.3% of 33 cases tested, with no cross-resistance identified. Resistance rates for each AF were as follows: FL (18%), VO (6%), IT (6%), PO (9%) and AMPB (3%). No resistance was seen for echinocandins apart from one C. krusei strain showing an intermediate result for CASP.
Conclusion: The study showed an overall high rate of non-albicans Candida, with the predominance of C. parapsilosis and C. glabrata, representing a therapeutic challenge. AF resistance rate was high which emphasizes the importance of continuing surveillance and providing accurate and reliable tools in the laboratories for rapid speciation and susceptibility testing.
Keywords: Candida, candidemia, invasive candidiasis, risk factors, epidemiology, antifungal susceptibility testing
Introduction
The prevalence of Candida as a nosocomial bloodstream pathogen is increasing.1 Candidemia is a devastating disease with high morbidity and mortality rates.2 Candida species (spp.) distribution in bloodstream infections varies across geographical areas. Until recently, Candida albicans has been the most commonly isolated species. However, a recent shift toward non-albicans Candida (NAC) is described.3 A meta-analysis in 2019 by Koehler et al demonstrated variability among Candida species in European countries, with an overall predominance of non-albicans strains.4 In contrast, two global SENTRY surveillance studies conducted during different periods (1997–1999 and 2017–2019) concluded that C. albicans was the most common species, followed by C. glabrata.5,6 In Saudi Arabia (SA), it is becoming increasingly evident that NAC and C. albicans contribute differently to bloodstream infections in various regions with C. albicans being still the most common in all regions followed in most studies by C. tropicalis.7–10 In the Eastern Region of SA, Al-Tawfiq et al observed that the annual incidence of candidemia fluctuated between 0.2–0.76 cases/1000 hospital discharges, with C. albicans being the predominant species.11 A subsequent seven-year surveillance study conducted in our institution demonstrated an increasing trend of NAC (69.2%), whereas C. albicans (38%) remained the single predominant species.12
The risk factors for candidemia have been discussed in several studies, highlighting the role of age (>60 years), as well as underlying conditions, such as diabetes mellitus, acute renal failure (ARF), being on hemodialysis (HD), burns, and having malignancies.3,11,13–15 Additional risk factors include previous Candida colonization, complicated abdominal surgeries, the presence of central venous lines, total parenteral nutrition, the use of corticosteroids and broad-spectrum antibiotics, and immunosuppressive therapy. The coronavirus disease 2019 (COVID-19) is a recently identified risk factor for candidemia. A study in Turkey found an increased rate of COVID-19-associated candidemia (CAC), with a higher incidence rate of 2.16-fold, as well as earlier onset (two weeks) and a higher mortality rate (92% vs 79%) compared to patients without COVID-19.16 Corticosteroids and tocilizumab (TZ), two known immunomodulatory agents, have been used to treat severe COVID-19 infections and have been studied as a possible cause of this trend with discrepant results.17,18
Mortality rates of candidemia cases worldwide are highly variable, ranging from 28.6–70%.13,19,20 Many predictors of mortality in candidemia have been proposed in the literature including the timing of initiation of effective antifungal treatment,21,22 the time to positivity (TTP),23,24 bacterial co-infection14,25 and the adherence to order follow-up cultures of candidemia cases, as recommended by the guidelines.26–28 With the incremental use of systemic antifungal (AF) (empirically or prophylactically), breakthrough candidemia (BTC) has been found to increase in high-risk patient groups.29,30 BTC is defined as any invasive candidiasis developing while the patient is on an antifungal drug, including those outside the antifungal coverage, taking into consideration the pharmacokinetics and pharmacodynamics of the drug.31 Multiple causes of BTC have been addressed, including infection with resistant species, poor source control, biofilm formation, and AF tolerance. Studies investigating BTC have reported variable rates for different antifungal drugs.29,30 However, data are lacking in SA, with only one report of small sample size (n = 32) in KFHU reporting BTC in two cases (6%), corresponding to patients undergoing fluconazole therapy.13
Antifungal resistance is a global concern owing to reports of increasing rates worldwide.5 A global SENTRY antimicrobial surveillance system involving 22 nations from 1997–1999 found that fluconazole continued to exert action against most Candida spp. (98–100%). However, this was not the case for C. glabrata, for which sensitivity to fluconazole ranged between 48–83%.6 A subsequent study from 2017–2019 found increased fluconazole resistance in C. parapsilosis (11.4%) and the emergence of echinocandin resistance.5 A study in Finland compared resistance rates over two time periods (2007–2011 and 2012–2016) and found an increasing trend of fluconazole resistance (from 13.4–19.2%), whereas anidulafungin resistance rate was found to be 2.1% in the later period.20 The current study aimed to describe candidemia frequency, Candida spp. distribution and the associated risk factors, and clinical outcome. Also, we aimed to evaluate the resistance profiles of candidemia strains based on antifungal susceptibility testing (AFST) using Sensititre™ YeastOne (SYO).
Materials and Methods
Study Settings, Population, and Data Collection
The study was conducted in the microbiology laboratory of King Fahad Hospital of the University (KFHU), a 550-bed secondary care and training center. Non-replicate positive blood cultures (BCx) for yeasts at direct Gram staining were collected as part of routine hospital care during the period between July 1st, 2020–December 31st, 2021. All flagging positive BCx bottles belonging to neonates, pediatrics and adult cases from in- and outpatient services were included. For each case, only the first BCx positive for yeasts on Gram-staining was included in the study, unless a strain was isolated later than 28 days from the previous set with negative BCx in between the episodes, or another Candida spp. was identified. Mixed cultures containing yeasts and bacteria, patients with breakthrough candidemia were included for subsequent batch testing from purely grown cultures. Candida strains originating from sites other than blood or sterile body fluids were excluded as they were unlikely to represent a pathogenic status. Patients’ medical records were reviewed to collect demographics, underlying medical conditions, COVID-19 status, antimicrobial therapy, and routine laboratory testing results. A three-month review was done for the period prior to the onset of candidemia to identify risk factors.3 The sample size was calculated based on a power of 95% using this formula  .32
.32
Definitions
Candida colonization counted by any growth of Candida in non-invasive samples and it was considered colonizer clinically with no subsequent therapeutic intervention eg sputum cultures. Corticosteroid use was defined as exposure to more than or equal to 20 mg prednisone or equivalent daily for more than or equal to 10 days before candidemia.14 Any use of chemotherapy or immunosuppressant was also reported as a risk factor. COVID-19 was considered as positive if a patient had a documented polymerase chain reaction (PCR) result in the same admission. Concomitant bacteremia was defined as any significant bacteremia two days before or within seven days after candidemia onset. Any usual blood contaminant such as Coagulase negative staphylococci or Gram-positive bacilli were considered insignificant and thus not recorded if antibiotic regimen was not changed accordingly, and vancomycin was not initiated after detecting the organism, or if vancomycin started for 4 or less days for the reason of turnaround time in our institution from BC until IDC and decision making. The length of stay was calculated from the first day of current admission until the day of candidemia. Antibiotic exposure was defined as at least 3 days of any antibiotic treatment administered within 3 months prior to the onset of candidemia. Neutropenia was defined as an absolute neutrophil count of less than 500 cells/μL. Co-morbidities were evaluated using the Charlson comorbidity index.33 Antifungal use was classified based on the initial use into four groups: on the same day of candidemia or before, within 24 hours of blood collection, within 48 hours, and after 48 hours. The time to positivity of the blood bottle was also documented and classified into three groups: within 24 hours of blood collection, within 48 hours, and after 48 hours. The cases were grouped into survivors versus non-survivors with a cut-off of 30 days’ mortality. Follow-up and sterility cultures were investigated; the latter was defined as the first negative follow up culture after previous positive blood culture with Candida spp. The debatable cases (defined as those with regrowth of Candida or that have bacterial growth in the first negative follow up culture) were not included in the median calculations of sterility culture. Compliance with the guidelines was determined based on a 96-hour interval instead of 48 hours considering the turnaround time in our institution from BC until IDC that enhanced decision-making. BTC was investigated considering days of exposure for each class as previously described.31 If a patient had exposure to more than one AF in the preceding three months, the one with the longer duration was considered. Outcomes were measured at 4 points of time: 14, 30, 60 and 90 days from the first laboratory detection of candidemia.
Blood Culture Processing
Once received, blood culture bottles for patients suspected to have bloodstream infections were loaded into the Bact/alert (bioMe ́rieux, USA) or Virtuo instruments (bioMe ́rieux, USA) for a maximum of 5 days, unless a signal is detected earlier. Following a positive signal, bottles were processed according to the laboratory’s standard policy. Gram stain was performed and a sample from the bottle was sub-cultured to a blood agar plate (BAP), a chocolate agar plate, and McConkey agar. If yeasts were visualized on microscopy, an additional Sabouraud dextrose agar (SDA) plate is streaked. The plates were aerobically incubated at 35 °C for 24–48 hours and checked every 8 hours for visible colonies. When the growth was sufficient, yeast identification and susceptibility testing were carried out. Isolates from pure plate were stored in glycerol at −80 °C throughout the study for SYO batch testing.
Microbial Identification
The VITEK MS (bioMe ́rieux, Durham, NC, USA) was used for yeast identification based on Matrix Assisted Laser Desorption/Ionization-Transfer for Flight (MALDI-TOF) technology following the manufacturer’s recommendations.34 For quality control purposes, target plates were calibrated and quality controlled using E. coli ATCC 8739. If MALDI-TOF could not identify the strain or there was any doubt about the species, the strain was further identified by VITEK 2 system (bioMe ́rieux, Durham, NC, USA) as per our routine lab policy. The system was set according to the manufacturer’s instructions including running the quality control (QC) strains (C. parapsilosis ATCC 22019TM and C. krusei ATCC 6258TM).
Antifungal Susceptibility Testing (Sensititre™ YeastOne)
The test was performed and read according to the manufacture instructions (Thermo Fisher Scientific, Waltham, MA, USA).35 The susceptibility results were interpreted manually at 24 hours. C. parapsilosis ATCC 22019TM and C. krusei ATCC 6258TM were used for quality control. During the optimization phase, both C. parapsilosis ATCC 22019TM and C. krusei ATCC 6258TM were tested to each antifungal following the CLSI and manufacturer’s instructions. Due to limitations in the SYO stock, only C. parapsilosis ATCC 22019TM was chosen as the weekly QC subsequently, and cohort isolates were thawed and batch-tested, all QC and clinical isolates were performed in duplicate. Colony count on SDA and purity plates on BAP were also checked as per the research protocol. QC was considered as passing if either one of the readings fall in the accepted range of either CLSI or SYO recommended breakpoints, with an acceptable colony count.
MIC Interpretation
MIC Interpretation was done using the CLSI breakpoints (M-60).36,37 If not available, the following references were referred to in sequence; epidemiologic cut off values (ECVs) in the CLSI M59 document,38 European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoints and EUCAST ECVs. If all were not available, interpretation was documented as not available (NA). For C. auris, the Centers of Disease Control (CDC) tentative MICs were used for interpretation.39,40 Discrepant MIC results between the duplicate readings could not be repeated due to limited SYO kit number. As all MIC tests were done in duplicate, the two MIC readings were interpreted and data were checked for normality using the SPSS (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.) and the median was calculated for the two readings for each strain unless 1 reading failed the other reading was accepted to be used as the median. Categorical classifications for any reading between two breakpoints sensitive (S) or resistant (R) was considered intermediate (I) or susceptible dose-dependent (SDD) based on the species.
Ethical Approval
This study was approved by Imam Abdulrahman Bin Faisal University Institutional Review Board (IRB-PGS-2020-01-396). No additional consent was needed for this observational, lab-based non-interventional study. The institution operates in accordance with the 1964 Helsinki Declaration and its later amendments.
Statistical Analysis
The statistical analysis was performed using Excel and SPSS software. Data were analyzed as non-parametric after being checked for normality using the Shapiro–Wilk Test. The GraphPad Prism software version 9.3.1 was used for the risk factor analysis by Kruskal–Wallis one-way analysis of variance for multiple groups of non-parametric data. A two-tailed p-value < 0.05 was considered to represent statistical significance for all tests. The MIC50 and MIC90 were calculated for the available results for each antifungal using Microsoft excel.
Results
Demographic and Clinical Characteristics
A total of 49 isolates belonging to 48 episodes of infection (1 episode with poly-fungal blood stream infection involving 2 different Candida spp.) was collected from 43 patients with candidemia. Risk factors and demographic data were calculated according to the episodes of candidemia (n = 48). The median age of candidemia cases was 62 ± 26 (± IQR) years and those aged 45–74 years were the most commonly affected age group (58.3%). We had only 5 pediatric cases during this study. Males were more frequently affected (60.4%) than females (39.6%), with a male to female ratio of (1.6:1). Patients were distributed between intensive care units (ICUs) and non-ICU wards, the most common was surgical ICU (37.5%), and followed by medical ICU (33.3%), other ICUs (14.5%) and non-ICUs (14.5%). Candidemia occurred after a median of 16 days of hospital stay (± IQR of 15) with 93% of cases developing it after 48 hours of hospital admission (a hospital acquired infection). Most cases were admitted initially with a primary diagnosis of respiratory diseases including COVID-19 pneumonia (41%), while gastrointestinal tract (GIT) diseases were the reason of admission in 20%. Other morbidities including renal diseases or multiple pathologies, were leading for admission in 39% of cases.
Risk Factors for Candidemia
A summary of the risk factors for candidemia is shown in Table 1. COVID-19 was confirmed in 30.6% of cases, all of them aged between 45 to 74 years which is the most affected age group by candidemia. Antibiotics administration was noticed in the majority of cases (88%) with a median number of (4± IQR of 3.75). The most commonly used antibiotics in order were carbapenems (69%), glycopeptides (53%), and macrolides (37%).
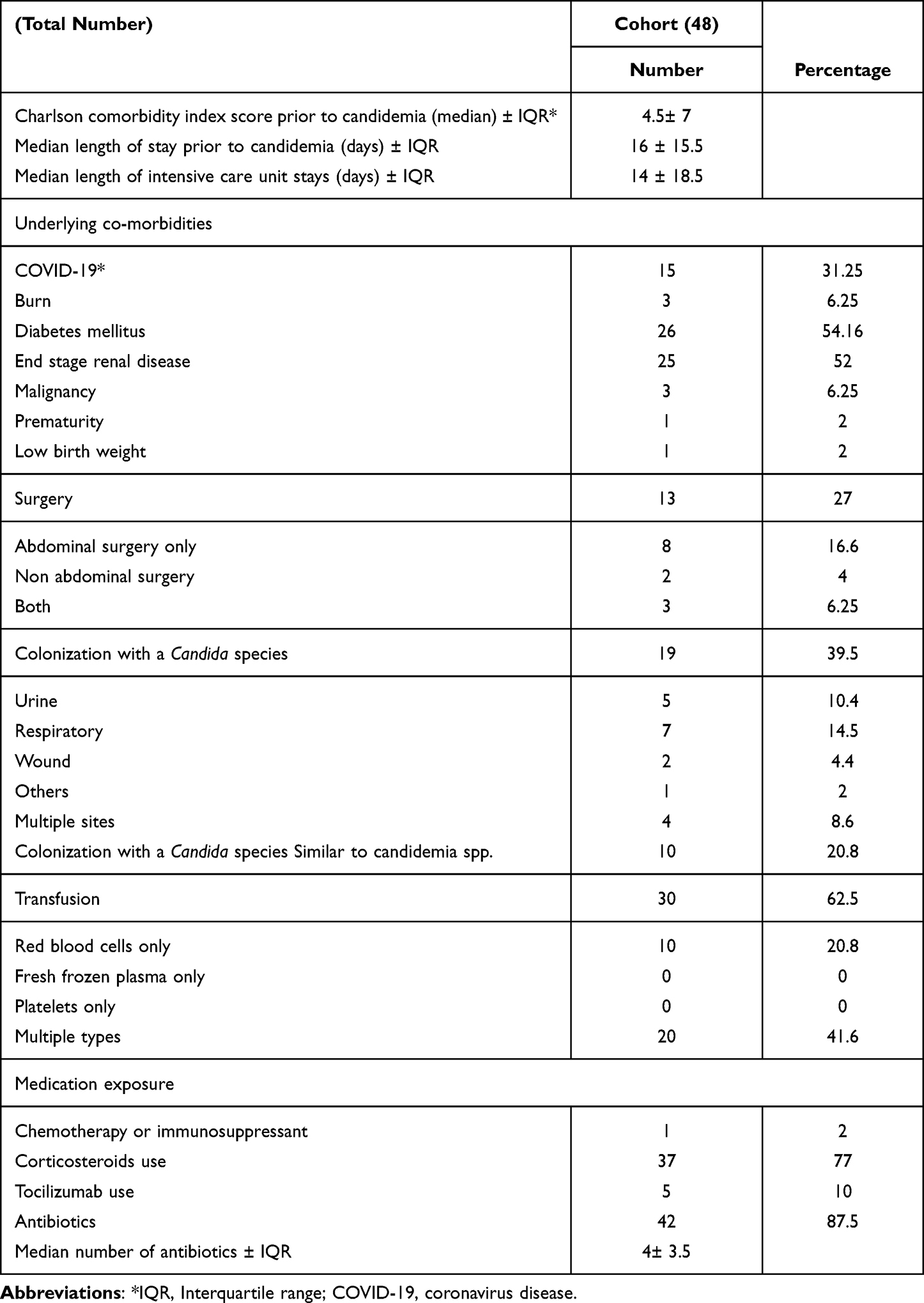 |
Table 1 Risk Factors for Candidemia in the Preceding 3 Months of the 48 episodes |
Microbiological Findings
Species Distribution, Time to Positivity, Bacterial Co-Infection, and Previous Bacteremia
C. glabrata and C. parapsilosis were the most frequent species isolated with each representing (22.9%), followed by C. albicans (18.75%), C. tropicalis (18.75%), C. auris (6.25%), C. orthopsilosis (4.16%) and other Candida spp. (including C. dublinensis, C. famata and C. krusei) each represent (2%).
88% of the Candida strains were isolated from aerobic bottles only, while 6% were isolated from anaerobic bottles only, and 4% were cultivated from both bottle types. The median TTP for candidemia cases was 38.5 hours ± IQR of 20.33 with the fastest being C. tropicalis of 7 hours and the latest being C. glabrata of 90 hours. More than half of the BCx flagged within 48 hours (53%). Those that flagged after 48 hours accounted for 29%; of them 57% were C. glabrata (n=8 out of 14), and the least number of cases flagged within 24 hours (18%).
Previous bacteremia in the 3 months prior to onset of candidemia was observed in 56% of the cases. 11 patients (22.9%) had bacteremic episodes due to multidrug resistant (MDR) or extensively drug resistant (XDR) Gram-negative bacilli (GNB), including K. pneumoniae with a carbapenems resistant Enterobacterales (CRE) genotype and/or phenotype in 3 patients (27%), MDR or XDR.
A. baumannii in 4 patients (36%), while both organisms were isolated from 2 cases (18%) and 1 had ESBL K. pneumonia (11%). On the other hand, concomitant bacteremia was seen in 12 (25%) of the total patients (31% among survivors and 22% among non survivors) and were mostly GNBs (n = 7, 58%), followed by Gram positive bacilli (n = 4, 33%), and one had anaerobic concomitant bacteremia (8%).
Follow Up and Sterility Cultures
This study found inconsistency in ordering the follow-up cultures (fu cxs) for candidemia cases. 15 cases died within 4 days of blood collection for which they were not recorded as non-compliant nor included in the calculations. The total expected fu cxs at 4 days is 33 after subtracting the deceased cases. However, we received only 29 fu cxs (88%). The median time to send the first follow-up culture was 4th day after diagnosis, of those 19 cases (57.6%) showed compliance ie, the first fu cx was sent within 4 days of BC. The non-compliant cases (42.4%) included 10 cases for which the 1st fu cx was sent after 4 days with a period ranging between 5 to 18 days and 4 cases who survived more than 4 days after BC but with no fu cx sent. Sterility culture was achieved in 63% of cases from the first BCx sent. It is noted that six cases had negative follow-up cultures for Candida, but positive for bacteria which might have masked the growth of Candida competitively. Another debatable group of cases were those who showed negative initial follow-up cultures at a certain point, but with regrowth of Candida at a following period. These cases are illustrated in Table 2 and Table 3
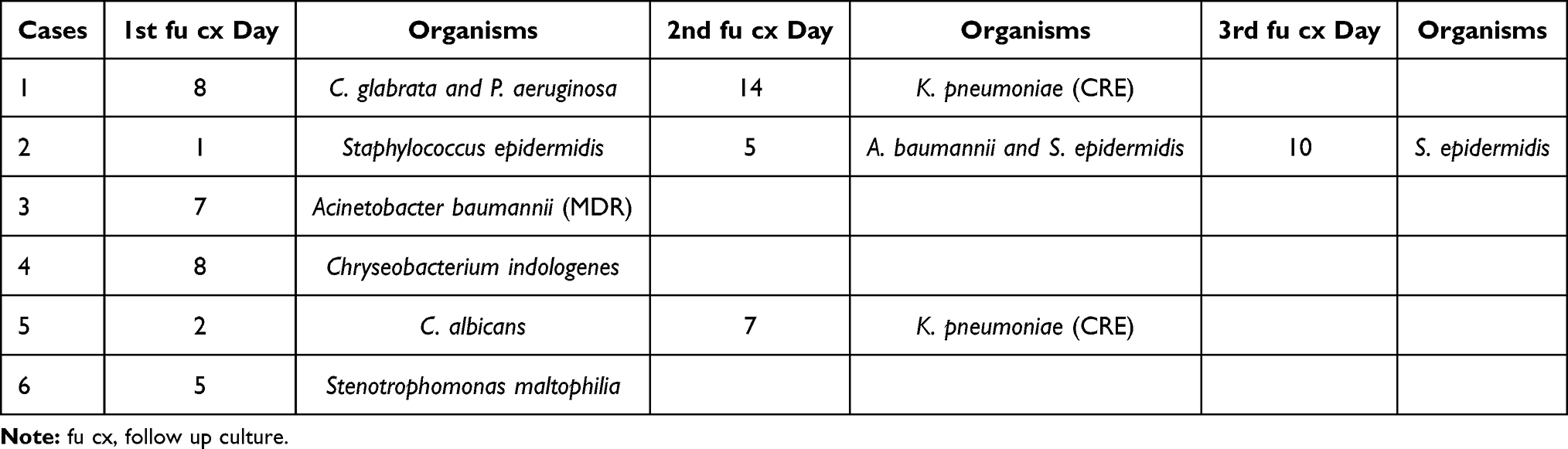 |
Table 2 Cases with Bacterial Growth in the Follow Up Cultures without Candida (Candidemia Date Considered as 0) |
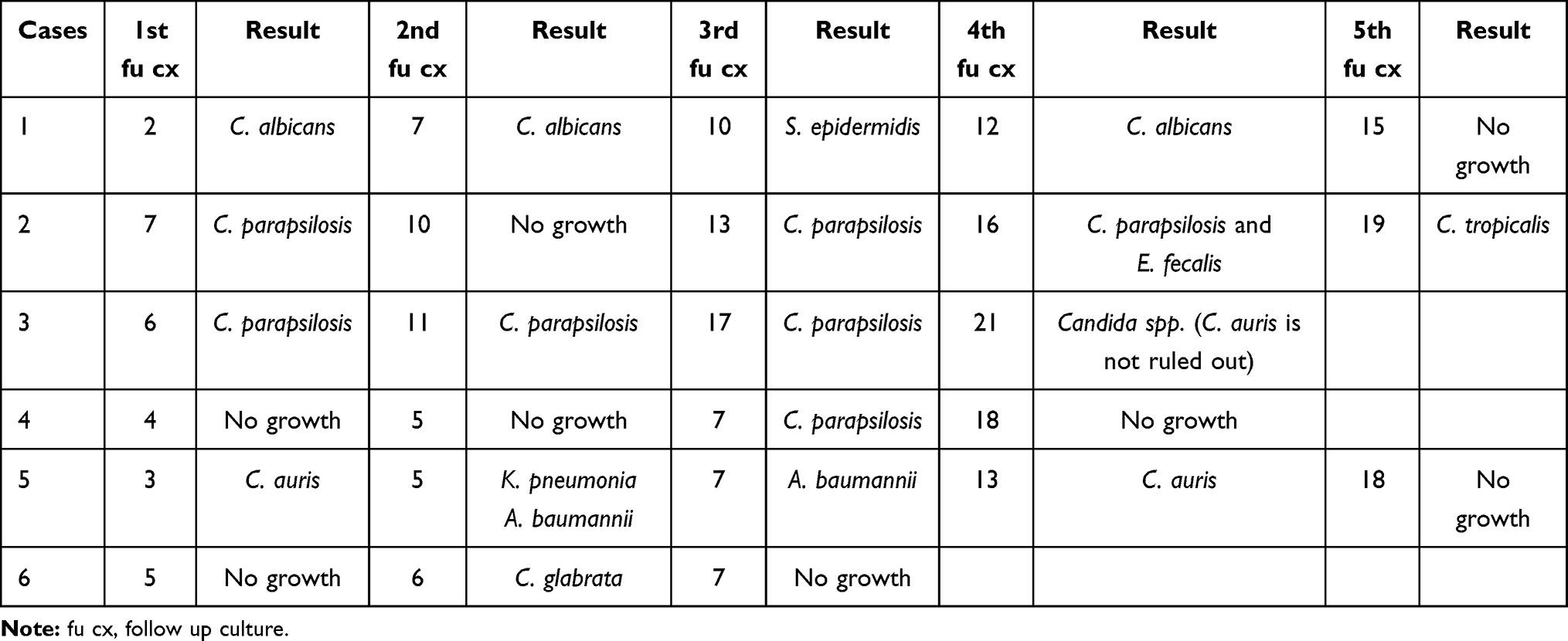 |
Table 3 Cases with Regrowth of Candida After Negative Follow Up Culture (Candidemia Date Considered as 0) |
Prior Antifungal Exposure and Breakthrough Candidemia
Twenty-one patients (43.75%) had prior antifungal exposure with a median duration of 8 days. Eight patients developed candidemia after stopping AF by a median of 19.5 days ± IQR of 18.25. Thirteen patients (27.1%) had BTC of whom seven (53%) cases were receiving an echinocandin, while an azole (n = 3, 23%) or amphotericin B (n = 3, 23%) was administered in the other cases.
Predictors of Mortality at 30 Days and Mortality Outcomes
Mortality at 30 days was significantly higher in older age, COVID-19 patients and those who were exposed to tocilizumab (Table 4). There were 44%, 71%, 77% and 77% of candidemia patients’ deaths at 14, 30, 60 and 90 days respectively, as shown in Figure 1. The 30 days’ mortality point was designated to compare the impact of risk factors on mortality.
 |
Table 4 Clinical and Microbiological Profiles of 16 Survivors and 32 Non-Survivor Candidemia Cases |
 |
Figure 1 Mortality rates at different time frames of candidemia in relation to age. |
Initial Antifungal Therapy and Antifungal Susceptibility Testing results
Initial AF therapy used in most cases was from echinocandins (73%) followed by amphotericin B in (18%) of cases. The Timing of initiation was mostly before or at the day of BC (59.3%), but initiation of antifungal therapy happened after 48 hours of BC in 29% of cases.
A total of 48 candidemia episodes were identified in the study. SYO was performed only on 33 strains due to limited kit number. For the whole 33 strains for which SYO was performed, voriconazole and itraconazole were more potent than fluconazole (MIC90 of 0.5, 0.5, and 57.6 µg/mL) respectively. Caspofungin on the other hand was slightly more potent (MIC90= 0.5) than the other two echinocandins (MIC90= 1.0). Detailed MIC distribution depending antifungal and Candida spp. is shown in Table 5. To be noted that we had flucytosine multiple failures due to multiple skip wells seen which led to reading failure and repeating was not feasible due to limited kit numbers.
 |
Table 5 MIC Distribution of Candidemia Cases Based on Candida Species and Antifungal Drug by Sensititre™ YeastOne |
Antifungal Resistance
Resistance to one antifungal in each strain was seen in 13 isolates (39.3%) further details illustrated in Table 5. The one isolate that showed an intermediate result to caspofungin was C. krusei and that which showed resistance to amphotericin B was C. auris. Fluconazole non-sensitive strains (48%) were either (R/NWT) 18% (n = 6) or (SDD) 30.3% (n = 10). Resistance was seen in three C. auris, two C. parapsilosis and one C. orthopsilosis, while SDD strains were mostly C. glabrata (n = 8). The remainder were one C. parapsilosis and one C. tropicalis. Out of the cohort tested, 39.3% of the isolates were resistant but none exhibited cross-resistance. However, once resistance was detected in one azole, it was associated with higher MICs for other azoles but not crossing the breakpoints. For example, fluconazole resistant isolates MICs were ranging between 4–256 µg/mL. Of those, none documented resistance to the other azoles rather they had higher MICs. In 2 isolates, both C. parapsilosis, out of the 6 that were resistant to fluconazole, voriconazole MICs were in intermediate range (0.5, 0.25 µg/mL). Similarly, voriconazole NWT isolates have higher MICs of fluconazole reaching to SDD range (12, 16 µg/mL) and both were C. glabrata. Posaconazole and itraconazole MICs were still within the sensitive range in all those cases.
Discussion
In the present study, NAC strains were the most frequently isolated species, representing 79.5%, with a predominance of C. parapsilosis and C. glabrata (22% each). These findings are in contrast to the global SENTRY program surveillance, which consistently observed a predominance of C. albicans.5,6 In Saudi Arabia (SA), geographical areas demonstrated different distributions of Candida species, which could be attributed to the population and their co-morbidities, as well as the different treatment strategies used in each region, similar to reports in Europe.41 Studies from the central region of SA demonstrated that C. albicans was the most frequent species, accounting for 50.3%, 50.7%, and 38.7% of candidemia cases.8–10 In the western region, although C. albicans was the predominating spp. (71% and 46%, respectively);7,42 a more recent study demonstrated a predominance of C. glabrata,3 which is in line with our findings. In the eastern region of SA, Bukharie et al observed that C. parapsilosis (44%) was the most frequently isolated species, followed by C. tropicalis (25%) and C. albicans (19%).13 While Al-Musawi et al, observed that most common was C. albicans but most isolates were NAC species (69.2%), which is similar to our findings (79.5%).12
C. parapsilosis and C. glabrata isolates have elevated MICs for echinocandins and fluconazole, respectively. This shift toward these two species may be related to the selective pressure of echinocandins and fluconazole when used empirically or prophylactically. This is supported by the fact that 42.9% of our cases had prior antifungal exposure, with two cases of BTC caused by C. parapsilosis who were already on an echinocandin. However, the echinocandins MIC90 of C. parapsilosis isolates in the cohort demonstrated no significant difference from other NAC (see Table 5). This phenomenon raises the debate of whether the clinical response is correlated to such in vitro MIC results.43 Another explanation for the predominance of C. parapsilosis is that most of our cases were CVC (82%), which could have led to C. parapsilosis being a common isolate since it can produce biofilms and central line-associated BSI (CLABSI). However, this has not been proven since we have only four cases with documented CLBSI. The emergence of rare species, such as C. famata and C. auris, as a cause of BSI in our study compared to previous studies in the same region is worth noting. When comparing our findings with a large-scale surveillance study, the C. auris BSI rate was relatively higher in our setting (<0.1% and 6%, respectively).
In regard to risk factors of candidemia, as reported previously men were affected more than women, with a ratio of (1.6:1).14,20 Also, similar patterns of underlying co-morbidities and predisposing risk factors were observed.14,20 Age was directly related to increased candidemia cases (age >60, 51%), with those aged 45–74 years being the most frequently affected age group (59%), in line with a previous study.5 The association between a higher incidence of candidemia and age can be explained by the changes in mucosal colonization that occur with age, which favours yeast colonization, especially C. glabrata, as proposed by Lockhart et al.44 In contrast, ARF or being on dialysis was not a significant risk factor in our cohort, nor was being on corticosteroid therapy. COVID-19 co-infection was associated with a higher mortality rate (p = 0.02), similar to the results of a study performed in Turkey, which found a mortality rate of 92% vs 79% (p = 0.005) for patients with CAC vs non-COVID, respectively.16 Omrani et al observed a similar increase in the rate of mortality in CAC vs non-COVID candidemia cases (60% vs 18.19%; p < 0.001, respectively); however, tocilizumab administration was not a significant risk factor for mortality contrary to our findings. This may be related to the small number of cases with TZ use in our study (n = 5) compared to Omrani et al's study (n = 104).18
As a microbiological finding, the TTP was not observed to impact the mortality rate.23,24 A previous study attributed this relationship to a subsequent delay in AF initiation,24 whereas another study highlighted the association of TTP with the source of candidemia. For instance, CLABSI with less TTP compared to non-CLABSI Candida spp. C. glabrata was found to have longer incubation times and higher mortality rates.23 Although none of the previously mentioned findings were confirmed, this contradicts our findings. In addition, a longer TTP can reflect a lower load on an organism. Thus, evidence is still lacking regarding the role of this microbiological parameter in predicting prognosis and reflecting species variability. Another microbiological finding we observed was the concomitant bacteremia rate reported in our study (24%). Similarly, a previous study performed in a teaching hospital in China between 2013 and 2018 focused on the risk factors for mixed C. albicans and found a rate of bacterial infection of 20.5%,25 while a local study reported a higher rate of (41.8%)3 with no specific bacterial identification. In our study, most concomitant bacteria were GNB (58%) compared to GPC (33.3%). In comparison, previous candidemia reports with larger sample sizes have identified a great abundance of Gram-positive organisms (63% and 52%). These differences may reflect different epidemiological situations across centers, as Gram-negative organisms demonstrated a decreasing trend in one study (26%).45 In contrast, another study suggested that both Gram-positive and Gram-negative organisms were equal.25,45 While one study observed concomitant bacteremia as a significant risk factor for mortality, we did not find any association.14
Despite its importance in candidemia guidelines, local data on follow-up cultures are largely lacking. Two studies from the United States reported 85.4% and 95% compliance rates, with the high adherence in one study being attributed to IDC. In contrast, the other was attributed to a comprehensive care bundle of candidemia implementation.46,47 Notably, both studies used an even stricter definition of compliance (every 48 hours) in follow-up cultures than the definition used in the present study.26–28 Although we preferred to use four days as an interval to indicate compliance for reasons explained in methods. This was found to be suboptimal (55.8%), highlighting the need for an effective antimicrobial stewardship program for managing such cases.
Empirical antifungal use was higher in the present study (26.5%) compared to a previous study (6%; n = 2) at the same institution (1995–2000), however, this did not affect the mortality rates.13 Although the mortality endpoint was not defined by days, we compared it against the 14 days’ all-cause mortality and found that it was comparable (44% vs 47%). Conversely, the BTC rate increased (from 6% to 26.5%) as these cases developed candidemia while on antifungal therapy. To the best of our knowledge, no other recent data is available in the study region. However, several studies have documented BTC worldwide. A study done in southern Brazil by Breda et al reported a rate of 18%, with 44% of patients receiving micafungin.30 Multiple causes have been attributed to the occurrence of BTC, including caspofungin tolerance,48 biofilm production, and AF resistance.31,49
In a recent meta-analysis, the mortality rates in patients with candidemia were highly variable, ranging from 28.6–70.0%.19 In the present study, an increasing trend of early mortality (43%, 71%, 78%, and 78% at 14, 30, 60, and 90 days, respectively) was observed in comparison with a previously performed surveillance study in our institution (29.3%, 47.9%, 56.4%, and 58.0% at 14, 30, 60, and 90 days, respectively).12 This could be explained by predominance of NAC with a high frequency of C. glabrata (21%) and the COVID-19 co-infection which is supported by a mortality rate of 86% observed for patients with CAC compared to 61% for those without COVID-19. Notably, the age distribution in both studies (median 49.5 vs 62) may also explain the higher mortality in the present study since candidemia is fatal in older age groups.5,20 However, the mortality rates were similar at both 60 and 90 days.
A lack of data regarding the frequency of antifungal resistance rates and MIC distribution exists in SA, as addressed in this study. Voriconazole and itraconazole were more effective in vitro than fluconazole (median MIC90 of 0.5, 0.5, and 58 µg/mL, respectively). Similar findings were reported by Pfaller et al in their SENTRY program study (1997–1999), where voriconazole and ravuconazole were found to be more potent than fluconazole.6 Our study presents higher resistance rates (39.3%) than previously reported by Aldardeer et al (21%) using a similar AFST method.3 We have previously reported fluconazole mono-resistance in 14.8% of candidemia cases using VITEK 2.12 In the present study, a consistent fluconazole resistance rate (18%) was observed. In Finland, a study that compared cases of candidemia during two time periods (2007–2011 and 2012–2016) reported a similar trend of fluconazole resistance (13.4–19.2%) as in our institution (14–18%).12,20 No resistance to echinocandins was detected in this study among Candida species while other studies in different geographical areas detected an anidulafungin resistance rate of 2.1% among patients with candidemia20 and 1.5% for NWT Candida spp. to one or more echinocandins during a recent SENTRY surveillance program.5 All C. auris isolates in our cohort (n = 3) were fluconazole-resistant, similar to reports in the Gulf Cooperation Council (GCC) region and worldwide.50 In the present study, one strain of C. auris (33%) out of three isolates exhibited resistance to amphotericin B compared to 42% of C. auris isolates in Kuwait.50,51 No difference in the breakpoints was introduced in the CLSI M 60 2nd edition to reflect the resistance rates when comparing older and new studies.36,52 Among fluconazole-resistant isolates, none exhibited cross-resistance to other azoles, in contrast to a previous study (n = 21) performed in Jeddah, Saudi Arabia3 where cross-resistance was found in seven strains out of the total resistant isolates (33.3%).
Limitations
The present study has several limitations. First, the risk factors for patients transferred from other hospitals were difficult to retrieve, and only clinical data available for the current admissions were included. Although the calculated sample size was powered for the primary objectives, the small size of AFST results due to limited resources may have contributed to the differences in findings concerning larger studies, along with other possible confounders. Expanding the study to include more representative strains will confirm some of our findings.
Conclusion
This study demonstrated the local endemicity of Candida spp. with a high frequency of NAC isolated from BSI. The role of three risk factors, namely old age, COVID-19 infection, and tocilizumab use, was evident and will need to be considered in the clinical evaluation when initiating an empirical antifungal therapy in susceptible patient populations. In the present study, the AF resistance rate was alarmingly high compared to that in previous local studies, excluding echinocandins, which emphasizes the importance of continuing surveillance and providing accurate and rapidly reliable tools for speciation and susceptibility testing. An effective antimicrobial stewardship program is needed to optimize the diagnostic and management phases of candidemia, including revisiting adherence to follow-up cultures when deciding the duration of therapy. Further research is needed to address polyfungal infections, concomitant bacteremia, and the effect of routine follow-up cultures, and TTP on the mortality rates of candidemia cases.
Abbreviations
AF, antifungal; AFST, antifungal susceptibility testing; AMPB, amphotericin B; AND, anidulafungin; ARF, acute renal failure; ATCC, American type culture collection; BAP, blood agar plate; BC, blood collection; BCx, blood culture; BSI, blood stream infection; BSI, blood stream infection; BTC, breakthrough candidemia; CAC, coronavirus associated candidemia; CASP, caspofungin; CCU, cardiac care unit; CDC, center of disease control; CLSI, clinical and laboratory standards institute; COVID-19, coronavirus disease; CRE, Carbapenems resistant Enterobacterales; CVC, central venous catheter; DM, diabetes mellitus; ECMM, European confederation of medical mycology; ECV, epidemiologic cut off value; ESCMID, the European society of clinical microbiology & infectious diseases; EUCAST, European committee on antimicrobial susceptibility testing; FFP, fresh frozen plasma; FL, fluconazole; FLC, flucytosine; FU cx, follow up cultures; GIT, gastrointestinal tract; GNB, Gram negative bacilli; GPC, Gram positive cocci; HD, hemodialysis; hr., hours; I, intermediate; ICU, intensive care unit; IDC, infectious diseases consultation; IDSA, Infectious Diseases Society of America; IFI, invasive fungal infection; IQR, interquartile range; IT, itraconazole; KFHU, King Fahad University Hospital; LOS, length of stay; MALDI-TOF, matrix assisted laser desorption/ionization-transfer for flight; MDR, multidrug resistant; MIC, minimum inhibitory concentration; MICU, medical intensive care unit; MSG-ERC, mycoses study group education and research consortium; MYC, micafungin; NA, not available; NAC, non-albicans Candida; NCCLS, national committee for clinical laboratory standards; NICU, neonates intensive care unit; NWT, non-wild type; PCR, polymerase chain reaction; PICU, paediatric intensive care unit; PO, posaconazole; QC, quality control; R, resistant; RBCs, red blood cells; S, sensitive; SA, Saudi Arabia; SDA, sabouraud dextrose agar; SDD, susceptible dose dependent; SICU, surgical intensive care unit; Spp, species; SYO, Sensititre™ YeastOne; TPN, total parenteral nutrition; TTP, time to positivity; TZ, tocilizumab; USA, United States of America; VO, voriconazole; WT, wild type; XDR, extensively drug resistant; yr, years.
Data Sharing Statement
Data are available upon reasonable request to the corresponding author.
Acknowledgments
Special thanks for Dr. Tariq Almusawi from Dr. Sulaiman Alhabib hospital for his critical review of the work. Many thanks for the Clinical Microbiology Department, at King Fahad Hospital of the University for their support and for Mr. Omar AlKhasawneh for his marvelous technical assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was partially funded by the Deanship of Scientific Research at Imam Abdulrahman University, Dammam, Saudi Arabia (project number 2020-288-Med).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bassetti M, Righi E, Costa A, et al. Epidemiological trends in nosocomial candidemia in intensive care. BMC Infect Dis. 2006;6. doi:10.1186/1471-2334-6-21
2. Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB. Cases from a prospective nationwide surveillance study. BSI US Hosp CID. 2004;309:1.
3. Aldardeer NF, Albar H, Al-Attas M, et al. Antifungal resistance in patients with Candidaemia: a retrospective cohort study. BMC Infect Dis. 2020;20(1). doi:10.1186/s12879-019-4710-z
4. Koehler P, Stecher M, Cornely OA, et al. Morbidity and mortality of candidaemia in Europe: an epidemiologic meta-analysis. Clin Microbiol Infect. 2019;25(10):1200–1212. doi:10.1016/j.cmi.2019.04.024
5. Pfaller MA, Carvalhaes CG, DeVries S, Huband MD, Castanheira M. Elderly versus nonelderly patients with invasive fungal infections: species distribution and antifungal resistance, SENTRY antifungal surveillance program 2017–2019. Diagn Microbiol Infect Dis. 2022;102(4):115627. doi:10.1016/j.diagmicrobio.2021.115627
6. Pfaller MA, Diekema DJ, Jones RN, et al. International surveillance of bloodstream infections due to Candida species: frequency of occurrence and in vitro susceptibilities to fluconazole, ravuconazole, and voriconazole of isolates collected from 1997 through 1999 in the SENTRY antimicrobial surveillance program. J Clin Microbiol. 2001;39(9):3254–3259. doi:10.1128/JCM.39.9.3254-3259.2001
7. Akbar DH, Tahawi AT. Candidemia at a university hospital: epidemiology, risk factors and predictors of mortality. Ann Saudi Med. 2001;21(3–4):178–182. doi:10.5144/0256-4947.2001.178
8. Al-Jasser AM, Elkhizzi NA. Distribution of Candida species among bloodstream isolates. Saudi Med J. 2004;25(5):566–569.
9. Al-Hedaithy SSA. The yeast species causing fungemia at a university Hospital in Riyadh, Saudi Arabia, during a 10-year period. Mycoses. 2003;46(8):275–280. doi:10.1046/j.1439-0507.2003.00893.x
10. Omrani AS, Makkawy EA, Baig K, et al. Ten-year review of invasive Candida infections in a tertiary care center in Saudi Arabia. Saudi Med J. 2014;35(8):821–826.
11. Al-Tawfiq JA. Distribution and epidemiology of Candida species causing fungemia at a Saudi Arabian hospital, 1996–2004. Int J Infect Dis. 2007;11(3):239–244. doi:10.1016/j.ijid.2006.03.003
12. Al-Musawi TS, Alkhalifa WA, Alasaker NA, Rahman JU, Alnimr AM. A seven-year surveillance of Candida bloodstream infection at a university hospital in KSA. J Taibah Univ Med Sci. 2021;16(2):184–190. doi:10.1016/j.jtumed.2020.12.002
13. Bukharie HA. Nosocomial Candidemia in a tertiary care hospital in Saudi Arabia. Mycopathologia. 2001;153:1.
14. Poissy J, Damonti L, Bignon A, et al. Risk factors for candidemia: a prospective matched case-control study. Crit Care. 2020;24(1). doi:10.1186/s13054-020-2766-1
15. Rodríguez D, Almirante B, Cuenca-Estrella M, et al. Predictors of candidaemia caused by non-albicans Candida species: results of a population-based surveillance in Barcelona, Spain. Clin Microbiol Infect. 2010;16(11):1676–1682. doi:10.1111/j.1469-0691.2010.03208.x
16. Kayaaslan B, Eser F, Kaya Kalem A, et al. Characteristics of candidemia in COVID-19 patients; increased incidence, earlier occurrence and higher mortality rates compared to non-COVID-19 patients. Mycoses. 2021;64(9):1083–1091. doi:10.1111/myc.13332
17. Riche CVW, Cassol R, Pasqualotto AC. Is the frequency of candidemia increasing in covid-19 patients receiving corticosteroids? J Fungus. 2020;6(4):1–4. doi:10.3390/jof6040286
18. Omrani AS, Koleri J, Ben Abid F, et al. Clinical characteristics and risk factors for COVID-19-associated Candidemia. Med Mycol. 2021;59(12):1262–1266. doi:10.1093/mmy/myab056
19. Zhang Z, Zhu R, Luan Z, Ma X. Risk of invasive candidiasis with prolonged duration of ICU stay: a systematic review and meta-analysis. BMJ Open. 2020;10(7):e036452. doi:10.1136/bmjopen-2019-036452
20. Ala-Houhala M, Valkonen M, Kolho E, Friberg N, Anttila VJ. Clinical and microbiological factors associated with mortality in candidemia in adult patients 2007–2016. Infect Dis. 2019;51(11–12):824–830. doi:10.1080/23744235.2019.1662941
21. Morrell M, Fraser VJ, Kollef MH. Delaying the empiric treatment of Candida bloodstream infection until positive blood culture results are obtained: a potential risk factor for hospital mortality. Antimicrob Agents Chemother. 2005;49(9):3640–3645. doi:10.1128/AAC.49.9.3640-3645.2005
22. Garey KW, Rege M, Pai MP, et al. Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study; 2006. Available from: https://academic.oup.com/cid/article/43/1/25/308688.
23. Taur Y, Cohen N, Dubnow S, Paskovaty A, Seo SK. Effect of antifungal therapy timing on mortality in cancer patients with candidemia. Antimicrob Agents Chemother. 2010;54(1):184–190. doi:10.1128/AAC.00945-09
24. Nunes CZ, Marra AR, Edmond MB, da Silva Victor E, Pereira CAP. Time to blood culture positivity as a predictor of clinical outcome in patients with Candida albicans bloodstream infection. BMC Infect Dis. 2013;13(1). doi:10.1186/1471-2334-13-486
25. Zhong L, Zhang S, Tang K, et al. Clinical characteristics, risk factors and outcomes of mixed Candida albicans/bacterial bloodstream infections. BMC Infect Dis. 2020;20(1). doi:10.1186/s12879-020-05536-z
26. Pappas PG, Kauffman CA, Andes DR, et al. Clinical Practice guideline for the management of Candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2015;62(4):e1–e50. doi:10.1093/cid/civ933
27. Cornely OA, Bassetti M, Calandra T, et al. ESCMID guideline for the diagnosis and management of Candida diseases 2012: non-neutropenic adult patients. Clin Microbiol Infect. 2012;18(SUPPL.7):19–37. doi:10.1111/1469-0691.12039
28. Alothman AF, Al-Musawi T, Al-Abdely HM, et al. Clinical practice guidelines for the management of invasive Candida infections in adults in the Middle East region: expert panel recommendations. J Infect Public Health. 2014;7(1):6–19. doi:10.1016/j.jiph.2013.08.002
29. Nucci M, Colombo A. Risk factors for breakthrough candidemia. Eur J Clin Microbiol Infect Dis. 2002;21(3):209–211. doi:10.1007/s10096-002-0697-1
30. Breda GL, Tuon FF, Meis JF, et al. Breakthrough candidemia after the introduction of broad spectrum antifungal agents: a 5-year retrospective study. Med Mycol. 2018;56(4):406–415. doi:10.1093/mmy/myx077
31. Cornely OA, Hoenigl M, Lass-Flörl C, et al. Defining breakthrough invasive fungal infection–Position paper of the mycoses study group education and research consortium and the European Confederation of medical mycology. Mycoses. 2019;62(9):716–729. doi:10.1111/myc.12960
32. Calculator.net. Sample size calculator; 2022. Available from: https://www.calculator.net.
33. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
34. Biomerieux SA. Instrument User Manual VITEK® MS Clinical Use-EN; 2019. Available from: www.biomerieux.com.
35. Instructions for use thermo scientific sensititre yeastone susceptibility plate’s 029-YEAST-ROW-IVD CID8962; 2015. Available from: www.trekds.com/techinfo.
36. Procop GW; Clinical and Laboratory Standards Institute. Performance Standards for Antifungal Susceptibility Testing of Yeasts. Clinical and Laboratory Standards Institute; 2017.
37. Alexander BD; Clinical and Laboratory Standards Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts. Clinical and Laboratory Standards Institute; 2017.
38. Procop GW; Clinical and Laboratory Standards Institute. Epidemiological Cutoff Values for Antifungal Susceptibility Testing. Clinical and Laboratory Standards Institute; 2017.
39. EUCAST. European committee on antimicrobial susceptibility testing breakpoint tables for interpretation of mics for antifungal agents; 2020.
40. EUCAST. General changes clinical breakpoints and ECOFFs for yeasts clinical breakpoints and ECOFFs for moulds clinical breakpoints and ECOFFs for dermatophytes 8 European committee on antimicrobial susceptibility testing. Available from: http://www.eucast.org.
41. Lass-Flörl C. The changing face of epidemiology of invasive fungal disease in Europe. Mycoses. 2009;52(3):197–205. doi:10.1111/j.1439-0507.2009.01691.x
42. Osoba AO, Amaw MDE, McAlear DE, Hussein BA. Candidemia and the susceptibility pattern of Candida isolates in blood. Saudi Med J. 2003;24(10):1060–1063.
43. Reboli AC. Editorial commentary: is the debate about treatment of Candida parapsilosis complex infections with echinocandins much ado about nothing? Clin Infect Dis. 2014;58(10):1422–1423. doi:10.1093/cid/ciu160
44. Lockhart’ SR, Joly S, Vargas K, Swails-Wengerl J, Engerl L, Solll DR. Natural defenses against Candida colonization breakdown in the oral cavities of the elderly. J Dent Res. 1999;78(4):857–868. doi:10.1177/00220345990780040601
45. Bouza E, Burillo A, Muñoz P, Guinea J, Marín M, Rodríguez-Créixems M. Mixed bloodstream infections involving bacteria and Candida spp. J Antimicrob Chemother. 2013;68(8):1881–1888. doi:10.1093/jac/dkt099
46. Antworth A, Collins CD, Kunapuli A, et al. Impact of an antimicrobial stewardship program comprehensive care bundle on management of candidemia. Pharmacotherapy. 2013;33(2):137–143. doi:10.1002/phar.1186
47. Lee RA, Zurko JC, Camins BC, et al. Impact of infectious disease consultation on clinical management and mortality in patients with candidemia. Clin Infect Dis. 2019;68(9):1585–1587. doi:10.1093/cid/ciy849
48. Yang F, Zhang L, Wakabayashi H, et al. Tolerance to caspofungin in Candida albicans is associated with at least three distinctive mechanisms that govern expression of FKS genes and cell wall remodeling. Antimicrob Agents Chemother. 2017;61(5). doi:10.1128/AAC.00071-17
49. Jenks JD, Cornely OA, Chen SCA, Thompson GR, Hoenigl M. Breakthrough invasive fungal infections: who is at risk? Mycoses. 2020;63(10):1021–1032. doi:10.1111/myc.13148
50. Khan Z, Ahmad S, Al-Sweih N, Joseph L, Alfouzan W, Asadzadeh M. Increasing prevalence, molecular characterization and antifungal drug susceptibility of serial Candida auris isolates in Kuwait. PLoS One. 2018;13(4). doi:10.1371/journal.pone.0195743
51. Aljindan R, Aleraky DM, Mahmoud N, et al. Drug resistance-associated mutations in erg11 of multidrug-resistant candida auris in a tertiary care hospital of eastern Saudi Arabia. J Fungus. 2021;7(1):1–9. doi:10.3390/jof7010018
52. Alexander BD, Espinel-Ingroff A, Pemán J; Clinical and Laboratory Standards Institute. Performance standards for antifungal susceptibility testing of yeasts. Expert Rev Anti Infect Ther. 2009;7(1):107–119. doi:10.1586/14787210.7.1.107
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.