")
Back to Journals » Infection and Drug Resistance » Volume 17
Clinical and Genomic Characteristics of a Clinical Listeria Monocytogenes ST120 Isolate Recovered from a Pregnant Woman
Authors Zhang J, Liu Z, Li Z , Xu C, Wang H, Yang R, Liu L
Received 10 November 2023
Accepted for publication 18 January 2024
Published 23 January 2024 Volume 2024:17 Pages 229—237
DOI https://doi.org/10.2147/IDR.S446860
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi Ruan
Jingrui Zhang,1,* Zengbin Liu,2,* Zhirong Li,2 Caihong Xu,1 Hongbin Wang,3 Rugang Yang,1 Li Liu1
1Department of Clinical Laboratory, The Fourth Hospital of Shijiazhuang, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Clinical Laboratory, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 3Department of Gynecology and Obstetrics, The Fourth Hospital of Shijiazhuang, Shijiazhuang, Hebei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingrui Zhang; Li Liu, The Fourth Hospital of Shijiazhuang, Shijiazhuang, 050000, People’s Republic of China, Email [email protected]; [email protected]
Background: Maternal–fetal listeriosis, caused by Listeria monocytogenes, is a rare but serious infection. Herein, we report the clinical and genomic characteristics of a clinical L. monocytogenes ST120 isolate recovered from a pregnant woman.
Methods: The clinical symptoms and treatment in pregnant woman were described in detail. Whole genome sequencing (WGS) was performed on the L. monocytogenes isolate SJZ_LM001, and the genomic characterization of the isolate was deeply analyzed.
Results: The clinical symptoms in pregnant women were mainly fever, and the placenta experienced severe inflammation. The pregnant woman was treated with ampicillin for effective anti-infective therapy. Genomic analysis showed that isolate SJZ_LM001 is sequence type (ST) 120, belong to clonal complex (CC)8 and lineage II of L. monocytogenes. Additionally, the isolates SJZ_LM001 harbored a novel plasmid pSJZ_LM001, which carried arsenical resistance genes (arsACD and acr3), and cadmium resistance genes (cadAC). Drug susceptibility testing showed that the isolate SJZ-LM001 was susceptible to ampicillin, meropenem, penicillin, and cotrimoxazole.
Conclusion: This is the first to identify a clinical case of infection in a pregnant woman caused by ST120 L. monocytogenes in China. These findings could benefit our understanding of the genomic characteristics of L. monocytogenes, and the pregnancy-related listeriosis and providing early diagnosis and effective targeted treatment.
Keywords: Listeria monocytogenes, whole genome sequence, ST120, plasmid
Introduction
Listeriosis, caused by Listeria monocytogenes, is a rare but particularly severe foodborne disease.1 Human listeriosis remains one of the top three foodborne illnesses that result in hospital admissions in North America and Europe.2 Invasive L. monocytogenes infections manifests three main clinical forms: pregnancy-related and neonatal listeriosis, bacteremia or septicemic listeriosis, and central nervous system (CNS) infection.2
Pregnancy-related listeriosis continues to be one of the illnesses with the highest fetal and newborn morbidity, causing a fetal disseminated disease with a high mortality of 27%–33%,3 and severe neonatal infections or preterm.4 Pregnancy-related listeriosis accounts for approximately 43% of all listeria infections, of which about 14% occur during the third trimester of pregnancy.3,5 The most recent outbreak in South Africa, which is the largest outbreak to date, involved around 1000 cases, of which 50% were associated with pregnancy6. Moreover, 41.1–62.8% of listeriosis cases in China were associated with pregnancies, highlighting the nationwide pressure of this disease.7,8
Currently, L. monocytogenes can be categorized into four lineages, with 15 serotypes comprising six PCR serogroups, and a variety of clonal complexes (CCs), multi-locus sequence types (STs), and sublineages (SLs).9 While all L. monocytogenes strains are potentially pathogenic, epidemiological and experimental evidence showed that the virulence is varied. Previous study showed that the serotype 4b was prevalent among pregnancy-related isolates.10,11 CC1, CC2, CC4, and CC6 were overrepresented in maternal-neonatal infected isolates in France, accounting for more than two-thirds of cases.12 In China, CC87, CC5, and CC8 were the most abundant CCs for pregnancy-related cases in the national listeriosis special surveillance program.8
To date, ST120 L. monocytogenes strains have caused several cases of human listeriosis in Canada and New Zealand,13 but have rarely been reported in China. In this study, we describe a clinical case of infection in a pregnant woman caused by ST120 L. monocytogenes in China. Furthermore, we have profiled the ST120 strain using whole-genome sequencing (WGS) to help understand the genomic characteristics of the strain.
Methods
The Patient and Isolates
A 32-year-old pregnant woman (second child) was admitted to the Fourth Hospital of Shijiazhuang at 17+5 weeks’ gestation with a 2-day fever and a temperature of 39.1°C. Ultrasonography revealed a gestational week of 18+6 and intrauterine fetal demise, and the patient was immediately admitted to the obstetrics department for hospitalization. Meanwhile, the blood and cervical secretions of the pregnant were collected for bacterial culture and identification. Subsequently, clinicians provided timely treatment based on the patient’s clinical symptoms and clinical examination results.
Bacteriological culture showed blood plate growth of smooth, moist, grayish-white colonies with narrow beta hemolytic rings. The result of the test showed it is Gram positive and finally diagnosed with L. monocytogenes by VITEK2 Compact bacterial identification system (bioMérieux, Marcy-l’Étoile, France). We examined pathological sections of the placental tissue and preserved the L. monocytogenes isolate (SJZ_LM001) from the blood cultures of for further analysis.
Antimicrobial Susceptibility Testing
The antibiotic susceptibility profile of the isolate SJZ_LM001 against ampicillin (AMP), penicillin, meropenem, trimethoprim-sulfamethoxazole, and erythromycin was performed by broth dilution method, according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.14 Staphylococcus aureus ATCCTM29213 was used as a quality control in each batch of drug susceptibility testing.
DNA Extraction and Sequencing
The isolate SJZ_LM001 was collected and cultured at 37°C in brain heart infusion (BHI) broth. The DNA genome was extracted using Wizard® Genomic DNA Purification Kit (Promega, United States) according to the manufacturer’s instructions. WGS was performed on Illumina NovaSeq and Pacbio Sequel platform by Personalbio (Shanghai, China). The Pacbio reads were assembled. The PacBio sequence reads were assembled into a high-quality genome using HGAP, CANU, and corrected by Illumina MiSeq with pilon (v1.22). Then, the complete genome sequence of SJZ_LM001 was assembled. The annotation of the whole-genome sequence was performed using Prokka (v1.14.6.)
Whole Genome Sequence Analysis
The Serogroup and MLST identification of the isolates was performed in silico on BIGSdb-Lm platform (https://bigsdb.pasteur.fr/listeria). The core SNPs were generated by a snippy pipeline with the reference genome EGD-e (NZ_CP023861.1). The minimum spanning tree of the isolates was constructed by Grapetree. The replicon genes of plasmid were determined by ABRicate (v1.0.1) with PlasmidFinder database, and the group plasmid was identified by the previous reported.15
Identification of Stress Resistance, Virulence, and Antibiotic Resistance Genes
According to the BIGSdb-Lm database, the BLASTN method was used to find genes encoding determinants for virulence, stress resistance, and antibiotic resistance with a minimum of 80% coverage and 80% identity.
Results
Clinical Characteristics and Treatment
In this study, the pregnant patient exhibited clinical symptoms mainly fever (39.1°C), and laboratory tests showed that the white blood cell (WBC) count was as follows: 17.4×109 /L, lymphocytes accounted for 7.6%, neutrophils accounted for 84.3%, and monocytes accounted for 7.9%, and the C-reactive protein (CRP) was 91.35 mg/L (the normal value < 10 mg/L). In addition, mycoplasma pneumoniae antibody, respiratory syncytial virus antibody, parainfluenza virus antibody, and coxsackievirus antibody were all negative. After hospitalization, the doctor promptly provided appropriate treatment according to the clinical symptoms and examination indicators of the pregnant patient (Figure 1). Of note, anti-infective treatment with ampicillin instead of cefoperazone/sulbactam sodium was administered immediately after the diagnosis of L. monocytogenes infection, as L. monocytogenes is naturally resistant to cefoperazone (a cephalosporin). The isolate SJZ-LM001 was also tested for drug susceptibility testing, and the results showed that the isolate was susceptible to ampicillin, meropenem, penicillin, and cotrimoxazole, and thus treatment was continued with ampicillin. Additionally, we questioned the pregnant patient about her diet prior to hospitalization, and the patient recalled that the infection might be suspected to have been caused by eating kimchi purchased in the market.
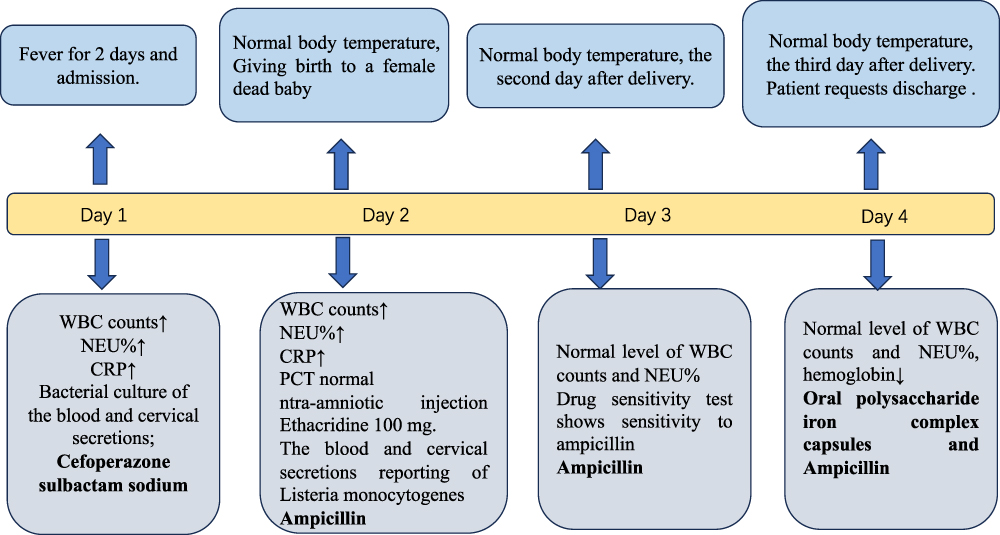 |
Figure 1 The timeline of the clinical presentations, assessment, and treatment of the pregnant women. |
Pathologic sections of the placenta showed mid-stage immature placental tissue, severe inflammation of the blood vessels and subplates, severe inflammation of the chorionic villous space, multifocal chorionic villitis, some interchorionic fibrosis, some perichorionic fibrin deposition visible, focal chorionic villous space siltation, ecchymotic membrane plethysmography, and no visible fetal membranes or umbilical cord (Figure 2).
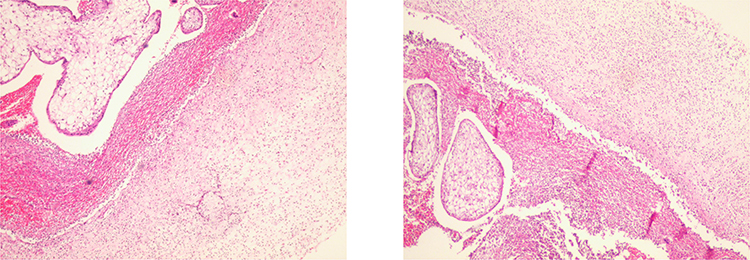 |
Figure 2 Pathologic sections of placental tissue in pregnant patient from in different fields of view. |
The General Genomic Features
The isolate SJZ-LM001 has a 2,954,308 bp single chromosome with a GC content of 38% (Figure S1). The chromosome genome contained 2930 coding sequences (CDS), six 16S-5S-23S operons, 67 tRNA genes, and 108 ncRNA. In addition, the isolates SJZ-LM001 carried a 92,088 bp plasmid, named pSHJ-LM001, with 37% GC content (Figure S1). The plasmid pSJZ-LM001 genome contains 93 CDS and only contained 2 ncRNA. All protein-coding genes were functionally annotated using the eggNOG database (Table S1), and the results showed that the top three known functional categories were Carbohydrate transport and metabolism (G), Transcription (K), and Amino acid transport and metabolism (E), which is in line with the ST87 LM reported.16
Serotype and MLST Identification
The serotype of the isolate SJZ-LM001 belong to 1/2a according to the differentiation of L. monocytogenes serovars (https://bigsdb.pasteur.fr/listeria/).17 Based on seven-genes MLST sachem, the isolate SJZ-LM001 was ST120, which belong to CC8 and lineage II of the L. monocytogenes classification.
Single Nucleotide Polymorphism (SNP) Analysis and Phylogenetic Analysis
To determine the relationship between the isolates SJZ-LM001 and those ST120 isolates from other countries, a total of 99 publicly accessible genomes of ST120 L. monocytogenes were selected for comparison analysis (Table S2). A maximum likelihood phylogenetic tree is constructed based on the core-SNPs of isolates (Figure 3A). Minimum spanning tree shows the relationship between the 100 ST120 isolates (Figure 3B). We found that the isolates were isolated from various geographical locations and isolation years were clustered on the same branches of the phylogenetic tree, but no epidemiologically specific clustering was observed.
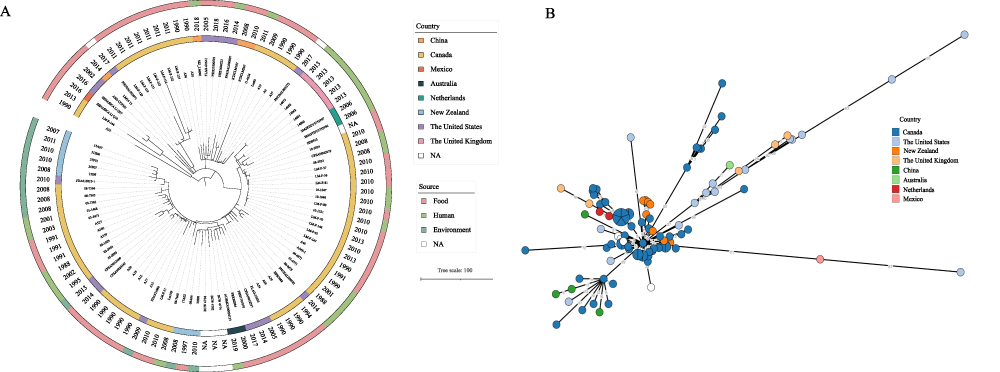 |
Figure 3 The core-SNP phylogenetic tree of 100 ST120 L. monocytogenes isolates. (A) The maximum likelihood phylogenetic tree was constructed by Raxml. The geographic location, date of isolation, and isolation source are shown on the tree (from inner to outer circles). (B) Minimum spanning tree show the relationship between the 100 ST120 isolates. |
The Plasmid Analysis
Comparing with reported plasmids of L. monocytogenes, the plasmid pSJZ-LM001 was found to be most similar to the previously reported plasmid pLM1686,18 with 99.75% identity in alignments covering 83% of pLM1686. According to the grouping of plasmids based on the plasmid replication protein RepA, the plasmid pSJZ-LM001 belongs to group 2, which is in line with pLM1686.18 The plasmid pSJZ-LM001 genome contained arsenical resistance arsACD and acr3 genes, cadmium resistance cadAC genes, copper transporter gene copB, and multicopper oxidase mco gene, Zinc-transporting ATPase zosA gene, but no genes associated with antimicrobial resistance and virulence (Figure 4).
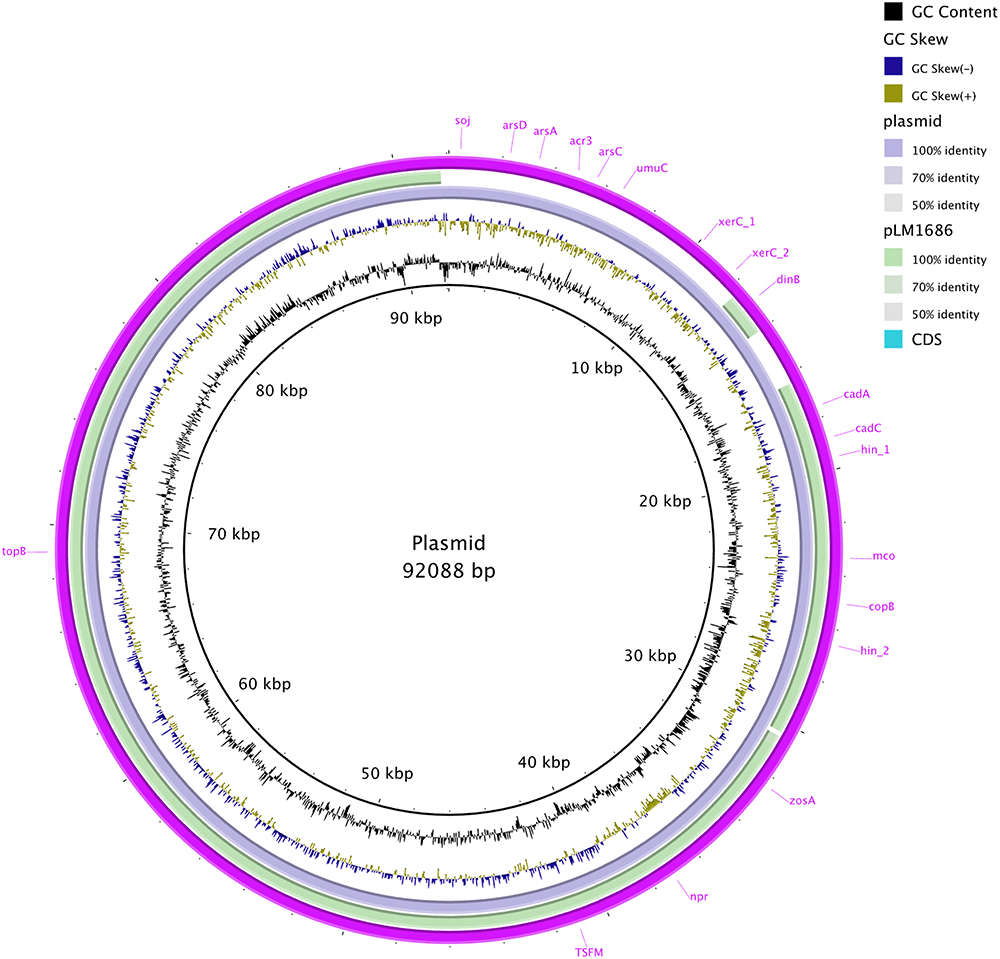 |
Figure 4 The plasmid comparison using BRIG with the plasmid pLM1686. |
Virulence Factors and Other Genetic Elements
All well-known virulence factors, including the Listeria pathogenicity island (LIPI)-1, multiple internalins (internalin A, B, C, E, F, G, H, J, and K) were found in SJZ-LM001 isolate. In addition, the internalin InlA is no premature stop codon (PMSC) in SJZ-LM001 isolate. PMSCs in InlA are frequently found in LM isolated from food, especially in ST9 L. monocytogenes, but are rare in human cases.15 As expected, the isolates SJZ-LM001 does not contain virulence LIPI- IV, which is mostly present in the isolates of lineage I.19
The isolate SJZ-LM001 was screened for the presence of stress adaptation associated element. The results showed that the isolate harbored stress survival islet 1 (SSI-1), which contributes to L. monocytogenes isolates adapting to low pH and high salt concentration.20 But not SSI-2, which is involved in the alkaline and oxidative stress response.20
The Antibiotic Resistance Genes
Four intrinsic antibiotic resistance genes were identified in the isolates SHJ-LM001, including fosX (fosfomycin), lmo0919 (lincosamides), mprF (cationic antimicrobial peptides), and norB (quinolones), which were present in all 322 foodborne L. monocytogenes isolates in China.21 However, no acquired antibiotic resistance gene was identified in the isolate SJZ-LM001 and the plasmid pSJZ-LM001.
Discussion
Maternal–fetal listeriosis is a rare but serious infection. L. monocytogenes is one of the few foodborne pathogens that can be transmitted vertically to the fetus via the placenta.22 In this case, the infection acquired by the mother resulted in an intrauterine fetal death. According to a retrospective study, miscarriage or fetal death/stillbirth caused a fatality rate of 42% among maternal/neonatal cases of listeriosis in China.23 Therefore, it is crucial to precisely and rapidly diagnose L. monocytogenes infection and administer the proper care. Most often, pregnant women who have been infected with L. monocytogenes exhibit non-specific clinical symptoms, such as headache, fever, diarrhea, or other digestive-related symptoms.4 Maternal listeriosis is frequently ignored until the mother exhibits obstetric symptoms or the fetus develops listeriosis. In this study, the pregnant mother exhibited vaginal discharge and blood cultures positive for L. monocytogenes. Maternal blood cultures were positive for L. monocytogenes in only 55% of samples in a large national prospective cohort study in France.24 A recent study reported that genital swab culture for L. monocytogenes had been informative in the diagnosis of maternal listeriosis, although blood culture was negative.25 This highlights the fact that for suspected maternal listeriosis, non-invasive cervical/genital swab cultures for L. monocytogenes may be useful in the diagnosis of maternal-neonatal listeriosis.
Antibiotics such as ampicillin, amoxicillin, and penicillin are recommended for L. monocytogenes infections as early as possible in clinical. Macrolide antibiotics are recommended for women who are allergic to penicillin.2,26 In this study, anti-infective treatment with ampicillin instead of cefoperazone/sulbactam sodium was administered immediately after the diagnosis of L. monocytogenes infection, which is an accurate and effective treatment for pregnant women.7 The intrinsic antibiotic resistance genes identified in the isolate SJZ-LM001 were consistent with foodborne L. monocytogenes isolates in China.21 Although low antibiotic resistance has been found in L. monocytogenes clinical isolates,27,28 horizontal transfer of transposons and plasmids from other Gram-positive bacteria to L. monocytogenes and thus acquisition of drug resistance has been observed.27 At the same time, L. monocytogenes is naturally resistant to the natural resistance of to cefoperazone, which is one of the most routinely used in clinical practice. Therefore, timely and accurate drug susceptibility testing can help to target treatment in the clinic.
To date, a number of goods, including meat, fruits and vegetables, mixed commodities, and unexplained sources have been reported to contain the clonal complex 8 (CC8) of L. monocytogenes12. CC87, CC5, and CC8 were the most abundant CCs for pregnancy-related cases in the national listeriosis special surveillance program of China. In the classification of L. monocytogenes, ST8 and ST120 all belong to CC8, but ST8 was one of the predominant types in pregnancy-associated listeriosis,29 and ST120 has been implicated in several cases of foodborne illness outbreaks.30 This is the first case of ST120 L. monocytogenes causing infection during pregnancy in China, suggesting the need for further increased surveillance of clinical isolates. In addition, previous study has reported that ST120 L. monocytogenes isolates are resistant to benzalkonium chloride,31 which can be well adapted to and persist in the factory environment.32 In this study, the pregnant woman was suspected to have consumed infections caused by kimchi purchased in the market, but the remaining kimchi has been discarded and the exact route of transmission has not been confirmed. Therefore, people, notably pregnant women, should be counseled on appropriate preventative strategies including eating cooked food and avoiding foods commonly contaminated with L. monocytogenes, such as soft ripened cheeses and pate.
Plasmids are commonly present in L. monocytogenes isolates from food products and environment, particularly in persistent strains. Previous studies showed that plasmid could benefit the isolate to adapt to selective environmental conditions, such as oxidation, salinity, and benzalkonium bromide.18 Interestingly, we found a novel complete plasmid pSJZ-LM001 in ST120 isolate. The plasmid pSJZ-LM001 was most closely related to pLM1686, which was found in the prevalent ST87 L. monocytogenes and improved the salinity tolerance, cell invasion, and cytotoxicity of the isolates.18 In addition to the gene for cadmium resistance, the plasmid pSHJ-LM001 also carried the arsenic-resistance gene, which could influence the environment fitness of the host isolates or have additional cellular functions. Previous study showed that 16 ST120 L. monocytogenes from Canada and New Zealand harbored a 77k bp plasmid with highly similar to pLM5578 (>99% coverage and >99.8% nucleotide identity). And pLM1686 also was identified in ST120 isolates in China.33 Thus, the conjugation, distribution, and function of the plasmid pSHJ-LM001 need to be further studied.
There are several limitations. Firstly, we performed an in-depth analysis of strains from blood sample sources only, lacking strains from placental and vaginal sources. Secondly, since the remaining food from the pregnant woman had been discarded, no further investigations could be conducted to trace the source and confirm the exact route of transmission. In addition, only one ST120 isolate was available in this study, and its genome was not analyzed in depth enough. Further analysis of strains from the population structure of the ST120 L. monocytogenes is needed.
Conclusion
Maternal-neonatal listeriosis is a rare but severe vertical transmissible disease, which could lead to fetal loss and neonatal infection. This study is the first to report a clinical case of infection in a pregnant woman caused by ST120 L. monocytogenes in China, which suggests the importance of understanding the distribution of molecular profiles in this particular category of invasive listeriosis cases. Furthermore, the discovery of novel plasmids pSJZ-LM001 illustrates the need for genomic profiling of the isolate, which contributes to further understanding of the adaptations of L. monocytogenes.
Ethical Approval
The study received ethical approval from the Ethics Committee of the Fourth Hospital of Shijiazhuang (20210024), which complies with the Declaration of Helsinki. The clinical information was collected from the patient after written informed consent.
Consent for Publication
Written informed consent was obtained from the patient to publish this article and clinical information including the use of images.
Funding
This work was supported by grants from Shijiazhuang science and technology research and development plan item (211460593).
Disclosure
The authors declare that they have no competing interests.
References
1. Radoshevich L, Cossart P. Listeria monocytogenes: towards a complete picture of its physiology and pathogenesis. Nat Rev Microbiol. 2018;16(1):32–46. doi:10.1038/nrmicro.2017.126
2. Koopmans MM, Brouwer MC, Vázquez-Boland JA, van de Beek D. Human Listeriosis. Clin Microbiol Rev. 2023;36(1):e0006019. doi:10.1128/cmr.00060-19
3. Elinav H, Hershko-Klement A, Valinsky L, et al. Pregnancy-associated listeriosis: clinical characteristics and geospatial analysis of a 10-year period in Israel. Clin Infect Dis. 2014;59(7):953–961. doi:10.1093/cid/ciu504
4. Charlier C, Disson O, Lecuit M. Maternal-neonatal listeriosis. Virulence. 2020;11(1):391–397. doi:10.1080/21505594.2020.1759287
5. Soni DK, Singh DV, Dubey SK. Pregnancy - associated human listeriosis: virulence and genotypic analysis of Listeria monocytogenes from clinical samples. J Microbiol. 2015;53(9):653–660. doi:10.1007/s12275-015-5243-9
6. Thomas J, Govender N, McCarthy KM, et al. Outbreak of listeriosis in South Africa associated with processed meat. N Engl J Med. 2020;382(7):632–643. doi:10.1056/NEJMoa1907462
7. Wang Z, Tao X, Liu S, Zhao Y, Yang X. An update review on listeria infection in pregnancy. Infect Drug Resist. 2021;14:1967–1978. doi:10.2147/idr.S313675
8. Li W, Guo Y, Cui Q, et al. Whole-genome sequencing-based characterization of clinical listeria monocytogenes isolates in China, 2013–2019. Foodborne Pathog Dis. 2023;20(4):158–168. doi:10.1089/fpd.2022.0040
9. Moura A, Criscuolo A, Pouseele H, et al. Whole genome-based population biology and epidemiological surveillance of Listeria monocytogenes. Nat Microbiol. 2016;2:16185. doi:10.1038/nmicrobiol.2016.185
10. Filipello V, Amato E, Gori M, et al. Epidemiology and molecular typing of pregnancy-associated listeriosis cases in Lombardy, Italy, over a 10-Year Period (2005–2014). Infect Dis Obstet Gynecol. 2017;2017:6479121. doi:10.1155/2017/6479121
11. Zahirnia Z, Mansouri S, Saffari F. [Pregnancy-related listeriosis: frequency and genotypic characteristics of L. monocytogenes from human specimens in Kerman, Iran] Listeriose in der Schwangerschaft: häufigkeit und genotypische Eigenschaften von L. monocytogenes in menschlichen Proben aus Kerman, Iran. Wien Med Wochenschr. 2019;169(9–10):226–231. doi:10.1007/s10354-018-0648-9
12. Maury MM, Bracq-Dieye H, Huang L, et al. Hypervirulent Listeria monocytogenes clones’ adaption to mammalian gut accounts for their association with dairy products. Nat Commun. 2019;10(1):2488. doi:10.1038/s41467-019-10380-0
13. Rivas L, Paine S, Dupont PY, et al. Genome typing and epidemiology of human Listeriosis in New Zealand, 1999 to 2018. J Clin Microbiol. 2021;59(11):e0084921. doi:10.1128/jcm.00849-21
14. CaLS Institute. Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria.
15. Song Z, Ji S, Wang Y, et al. The population structure and genetic diversity of Listeria monocytogenes ST9 strains based on genomic analysis. Front Microbiol. 2022;13:982220. doi:10.3389/fmicb.2022.982220
16. Wang Y, Luo L, Li Q, et al. Genomic dissection of the most prevalent Listeria monocytogenes clone, sequence type ST87, in China. BMC Genomics. 2019;20(1):1014. doi:10.1186/s12864-019-6399-1
17. Doumith M, Buchrieser C, Glaser P, Jacquet C, Martin P. Differentiation of the major Listeria monocytogenes serovars by multiplex PCR. J Clin Microbiol. 2004;42(8):3819–3822. doi:10.1128/jcm.42.8.3819-3822.2004
18. Mao P, Wang Y, Gan L, et al. Function and distribution of the conjugative plasmid pLM1686 in foodborne Listeria monocytogenes in China. Int J Food Microbiol. 2021;352:109261. doi:10.1016/j.ijfoodmicro.2021.109261
19. Maury MM, Tsai YH, Charlier C, et al. Uncovering Listeria monocytogenes hypervirulence by harnessing its biodiversity. Nat Genet. 2016;48(3):308–313. doi:10.1038/ng.3501
20. Pasquali F, Palma F, Guillier L, Lucchi A, De Cesare A, Manfreda G. Listeria monocytogenes sequence types 121 and 14 repeatedly isolated within one year of sampling in a rabbit meat processing plant: persistence and ecophysiology. Front Microbiol. 2018;9:596. doi:10.3389/fmicb.2018.00596
21. Ji S, Song Z, Luo L, et al. Whole-genome sequencing reveals genomic characterization of Listeria monocytogenes from food in China. Front Microbiol. 2022;13:1049843. doi:10.3389/fmicb.2022.1049843
22. Charlier C, Kermorvant-Duchemin E, Perrodeau E, et al. Neonatal listeriosis presentation and outcome: a prospective study of 189 cases. Clin Infect Dis. 2022;74(1):8–16. doi:10.1093/cid/ciab337
23. Chen S, Meng F, Sun X, et al. Epidemiology of human listeriosis in china during 2008–2017. Foodborne Pathog Dis. 2020;17(2):119–125. doi:10.1089/fpd.2019.2683
24. Delesalle S, Delesalle C, Delhoustal L, et al. Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study. Lancet Infect Dis. 2017;17(5):510–519. doi:10.1016/s1473-3099(16)30521-7
25. Luo L, Chen X, Payne M, et al. Case report: whole genome sequencing based investigation of maternal-neonatal listeriosis in Sichuan, China. BMC Infect Dis. 2019;19(1). doi:10.1186/s12879-019-4551-9
26. Grayo S, Join-Lambert O, Desroches MC, Le Monnier A. Comparison of the in vitro efficacies of moxifloxacin and amoxicillin against Listeria monocytogenes. Antimicrob Agents Chemother. 2008;52(5):1697–1702. doi:10.1128/aac.01211-07
27. Yan S, Li M, Luque-Sastre L, et al. Susceptibility (re)-testing of a large collection of Listeria monocytogenes from foods in China from 2012 to 2015 and WGS characterization of resistant isolates. J Antimicrob Chemother. 2019;74(7):1786–1794. doi:10.1093/jac/dkz126
28. Reis CM, Barbosa AV, Rusak LA, Vallim DC, Hofer E. Antimicrobial susceptibilities of Listeria monocytogenes human strains isolated from 1970 to 2008 in Brazil. Rev Soc Bras Med Trop. 2011;44(2):173–176. doi:10.1590/s0037-86822011005000019
29. Li W, Bai L, Ma X, et al. Sentinel Listeriosis surveillance in selected hospitals, China, 2013–2017. Emerg Infect Dis. 2019;25(12):2274–2277. doi:10.3201/eid2512.180892
30. Knabel SJ, Reimer A, Verghese B, et al. Sequence typing confirms that a predominant Listeria monocytogenes clone caused human listeriosis cases and outbreaks in Canada from 1988 to 2010. J Clin Microbiol. 2012;50(5):1748–1751. doi:10.1128/jcm.06185-11
31. Meier AB, Guldimann C, Markkula A, Pöntinen A, Korkeala H, Tasara T. Comparative phenotypic and genotypic analysis of Swiss and Finnish Listeria monocytogenes isolates with respect to benzalkonium chloride resistance. Front Microbiol. 2017;8:397. doi:10.3389/fmicb.2017.00397
32. Mohan V, Cruz CD, van Vliet AHM, et al. Genomic diversity of Listeria monocytogenes isolates from seafood, horticulture and factory environments in New Zealand. Int J Food Microbiol. 2021;347:109166. doi:10.1016/j.ijfoodmicro.2021.109166
33. Parsons C, Lee S, Kathariou S. Dissemination and conservation of cadmium and arsenic resistance determinants in Listeria and other Gram-positive bacteria. Mol Microbiol. 2020;113(3):560–569. doi:10.1111/mmi.14470
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.