Back to Journals » International Journal of General Medicine » Volume 19
CLEC4D as an Effective Indicator for Assessing Severity of Illness in Critically Ill Patients: A Prospective Study
Authors Wang G, Li Z, Zhao X, Wang X, Lian H, Liu Y
Received 10 December 2025
Accepted for publication 22 April 2026
Published 30 April 2026 Volume 2026:19 587855
DOI https://doi.org/10.2147/IJGM.S587855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Guangjian Wang,1,* Zhimao Li,2,* Xinyue Zhao,1 Xiaoru Wang,3 Hui Lian,1 Yecheng Liu2
1Department of Health Care, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Emergency Department, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Critical Care Medicine, The Second Hospital of Shanxi Medical University, Shanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hui Lian; Yecheng Liu, Email [email protected]; [email protected]
Background: Accurate assessment of illness severity is crucial in critically ill patients. The APACHE II score is widely used but complex and fails to reflect underlying immune-inflammatory dysregulation. C-type lectin domain family 4 member D (CLEC4D), a pattern recognition receptor on myeloid cells, is pivotal in immune responses. We investigated whether circulating CLEC4D levels could serve as a novel biomarker for severity of illness.
Methods: 368 adult ICU patients were enrolled. Serum CLEC4D levels, APACHE II scores, and immune-inflammatory parameters were measured within 24 hours of admission. Associations were analyzed using generalized additive models and multiple linear regression.
Results: Patients with high APACHE II scores (≥ 16) exhibited significantly elevated CLEC4D levels compared with those with lower scores (344.20 ± 65.75 pg/mL vs. 321.28 ± 73.31 pg/mL, P = 0.002). Multiple linear regression demonstrated a robust positive association between CLEC4D and APACHE II scores, with each 1 pg/mL increase in CLEC4D corresponding to a 0.016-point rise in APACHE II (P < 0.05). CLEC4D was inversely correlated with lymphocyte (β = − 0.028, P < 0.001) and IL-6 (β = − 1.404, P = 0.021) but positively correlated with PCT (β = 0.022, P = 0.031). Subgroup analyses confirmed the stability of this correlation across tumor and non-tumor cohorts and revealed a markedly stronger association among patients with sepsis (β = 0.030, P < 0.001).
Conclusion: Circulating CLEC4D levels positively correlate with APACHE II scores in critically ill patients, potentially associated with dynamic shifts in immune-inflammatory markers. CLEC4D represents a promising biomarker for assessing illness severity, especially in sepsis.
Keywords: CLEC4D, APACHE II, critically ill patients, severity of illness, biomarker, immune-inflammation
Introduction
The assessment of severity of illness (SOI) represents a fundamental aspect of clinical management in the intensive care unit (ICU). Accurate evaluation of SOI is crucial for prognostication, risk stratification, therapeutic decision-making, and resource allocation. Comprehensive scoring systems such as the Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) are widely applied to quantify disease severity and predict mortality by integrating a range of physiological and biochemical parameters.1 However, despite their widespread use, these systems are limited by their computational complexity and by their reliance on clinical and physiological endpoints, which do not adequately capture the underlying molecular and immunological mechanisms driving disease progression. In particular, they fail to reflect the profound immune and inflammatory dysregulation that characterizes critical illness.
Pathophysiological insults such as severe infection, trauma, or major surgery can precipitate a dysregulated immune-inflammatory cascade. This process is typically initiated by a hyperinflammatory state marked by excessive cytokine release, followed by an adaptive phase of immunosuppression that predisposes patients to secondary infections and organ dysfunction. The transition between these phases plays a decisive role in determining clinical outcomes.2 Accordingly, the identification of reliable molecular biomarkers that reflect immune imbalance and correlate with established SOI indices holds considerable clinical value. Such biomarkers could enhance the precision of disease assessment, facilitate individualized management, and provide mechanistic insights into immune regulation in critical illness.
C-type lectin domain family 4 member D (CLEC4D) is a pattern recognition receptor predominantly expressed on myeloid cells, including neutrophils, monocytes, and macrophages, where it mediates pathogen recognition and inflammatory signaling.3 Experimental evidence indicates that CLEC4D binds pathogen-associated molecular patterns and modulates the expression of inflammatory cytokines and chemokines that orchestrate immune cell activation and migration.4 In animal models, CLEC4D deficiency has been associated with excessive inflammatory responses, impaired bacterial clearance, and dysregulated cytokine profiles,5 underscoring its pivotal role in maintaining immune homeostasis. Despite these findings, research on CLEC4D has largely been confined to preclinical studies, and its clinical relevance in critical illness remains poorly understood.
To address this gap, we hypothesized that circulating CLEC4D levels are closely associated with the SOI in critically ill patients. In this prospective study, we aimed to systematically examine (1) the relationship between serum CLEC4D concentrations and APACHE II scores; (2) the robustness of this association across different clinical subgroups, including patients with sepsis or malignancy; and (3) the potential mechanistic links between CLEC4D and key immune-inflammatory biomarkers, such as lymphocytes, interleukin-6 (IL-6), and procalcitonin (PCT). This study seeks to elucidate the potential role of CLEC4D as an immune-inflammatory biomarker for SOI assessment and to provide new insights into the molecular mechanisms underlying critical illness.
Methods and Materials
Study Design and Patient Population
This prospective, single-center observational study was conducted at Peking Union Medical College Hospital (PUMCH), a tertiary referral center in China. Adult patients (≥18 years) admitted to the ICU between November 2024 and August 2025 were consecutively screened for eligibility. Written informed consent was obtained from all participants or their legally authorized representatives. Exclusion criteria were as follows: (1) absence of either CLEC4D measurements or APACHE II scores; (2) pregnancy or postpartum status; (3) recent cardiopulmonary bypass (eg, post-cardiac surgery); (4) corticosteroid or immunosuppressant use within the preceding month; and (5) refusal to provide written informed consent. A total of 368 critically ill patients met the inclusion criteria and were enrolled in the final analysis (Figure 1). The study protocol was approved by the Ethics Committee of PUMCH (I-24PJ2082).
 |
Figure 1 Flowchart of the study. Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CLEC4D, C-type lectin domain family 4 member D. |
Data Collection
Electronic Data
Clinical, demographic, and laboratory data were extracted from the institutional electronic medical record system. Demographic and medical history data included information on age, sex, comorbidities (eg, diabetes, autoimmune disease, and cancer), surgical history, and the presence of sepsis. ICU parameters collected included APACHE II and SOFA scores, mean arterial pressure (MAP), heart rate (HR), perfusion index (PI), and duration of mechanical ventilation. Laboratory variables obtained within 24 hours of ICU admission comprised complete blood counts (white blood cell [WBC], neutrophil [N], and lymphocyte [L] counts), inflammatory markers (IL-6, IL-10, and PCT), and serum lactate. APACHE II scores and routine clinical parameters were calculated and extracted from the electronic medical records. Data extraction was performed independently by two investigators (Guangjian Wang and Zhimao Li), and all data were cross-verified and confirmed by a third investigator (Hui Lian).
Measurement of CLEC4D
Peripheral venous blood samples were collected within 24 hours of ICU admission. Samples were centrifuged to isolate serum, which was immediately stored at −80°C until analysis. Serum CLEC4D concentrations were determined using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Zhichaobio Biotechnology Co., ZC-157656, Beijing, China) in accordance with the manufacturer’s protocol. All measurements were performed in duplicate by technicians blinded to the patients’ clinical data. The serum samples were thawed strictly once to prevent freeze-thaw degradation. Currently, the CLEC4D test is not a routine laboratory test performed in clinical practice at our study site. The measurements of CLEC4D for this study were exclusively conducted by the research team using commercially available ELISA kits for academic purposes.
Endpoints
The primary endpoint was the correlation between serum CLEC4D concentration and the APACHE II score. Secondary endpoints included the associations between CLEC4D and WBC, N, L, IL-6, IL-10, and PCT.
Statistical Analysis
The distribution of continuous variables was assessed using the Kolmogorov–Smirnov test. Normally distributed data are expressed as mean ± standard deviation (SD), whereas non-normally distributed data are presented as median (interquartile range, IQR). Categorical variables are expressed as frequencies and percentages. Patients were dichotomized into a low APACHE II group (<16) and a high APACHE II group (≥16) based on the cohort’s median score. Between-group comparisons were performed using the chi-square test for categorical variables and the Mann–Whitney U-test for continuous variables. Generalized additive models (GAMs) were used for both univariate and multivariate analyses to explore linear and nonlinear relationships between CLEC4D and clinical parameters. To minimize the potential risk of multicollinearity between APACHE II and SOFA scores, variance inflation factors were monitored in multivariable models. Confounders were selected based on their associations with the outcomes of interest or if their inclusion altered the effect estimate by more than 10%. Both linear and nonlinear relationships were examined using generalized linear models, with inflection points automatically identified through principal curve algorithms within the boundaries of the 95% confidence interval. Slight fluctuations in inflection points were anticipated given the modest sample size. The estimated effect size was derived by approximating the linear segments on either side of the inflection point. All statistical analyses were two-sided, with P < 0.05 considered statistically significant. Analyses were performed using EmpowerStats (http://www.empowerstats.com) and R software (version 4.2.0, http://www.R-project.org/). Figure 1 was created using WPS Office (Kingsoft, Beijing, China).
Results
A total of 368 critically ill ICU patients were enrolled during the study period (Figure 1). Based on the cohort’s median APACHE II score of 16, patients were stratified into a low APACHE II group (<16) and a high APACHE II group (≥16). The baseline clinical and demographic characteristics of the overall cohort and the two subgroups are summarized in Table 1. The median age of the entire population was 63 years, with patients in the high APACHE II group being significantly older than those in the low-score group (67 vs. 60 years, P < 0.001). The sex distribution was balanced in the low APACHE II group, whereas the high APACHE II group demonstrated a significantly greater proportion of male patients. The prevalence of sepsis increased markedly from 28.16% in the low APACHE II group to 57.73% in the high APACHE II group. Overall, 81.25% of patients underwent surgical procedures; notably, the surgical rate was significantly higher among those with lower APACHE II scores (88.51% vs. 74.74%, P < 0.001). Approximately half of the study population had malignancies, while the majority did not have diabetes mellitus, and only a small proportion presented with autoimmune diseases (AID). The prevalence of diabetes, malignancy, and AID did not differ significantly between groups.
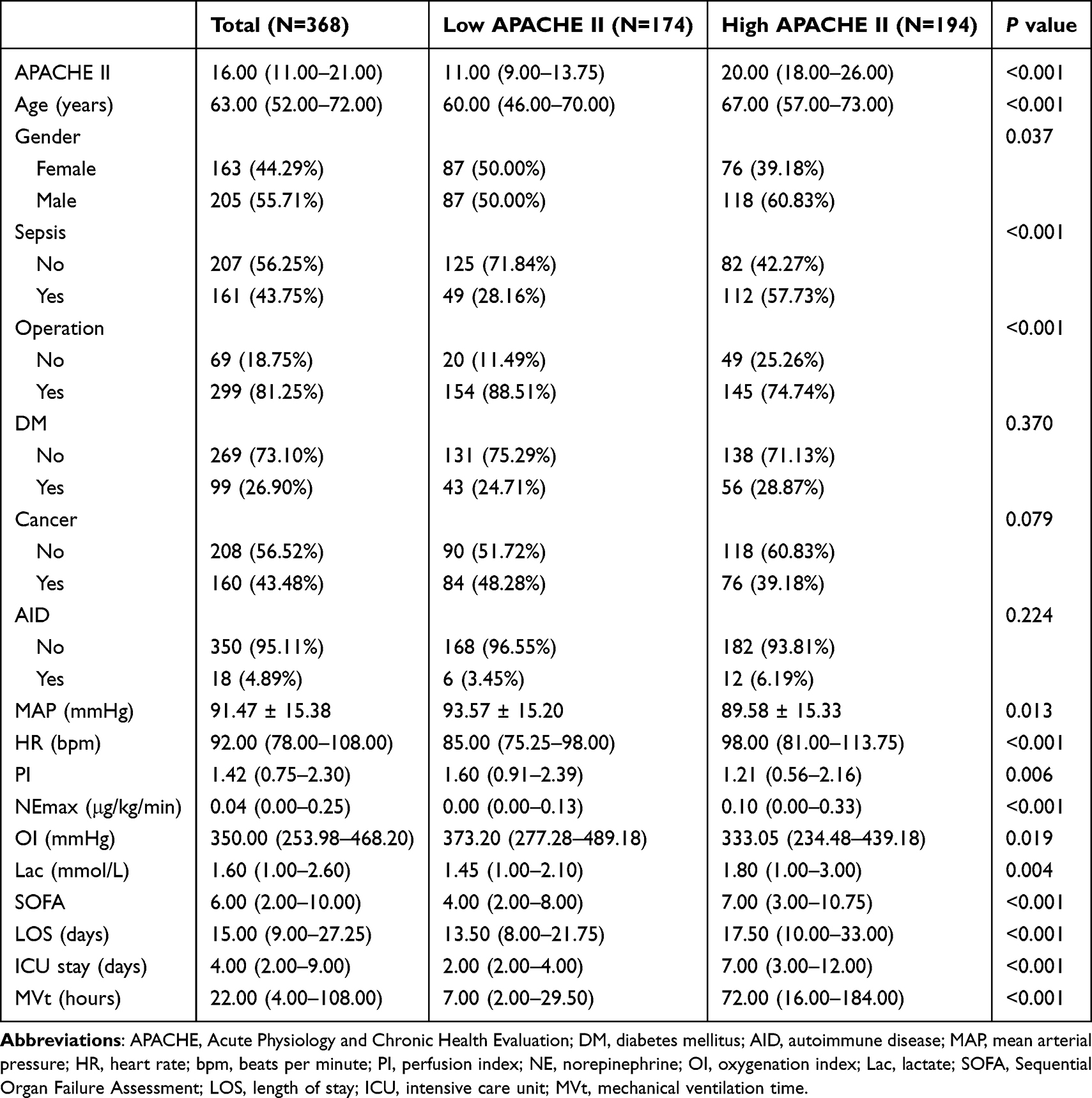 |
Table 1 Clinical Characteristics of the Study Population |
Hemodynamic and physiological parameters revealed marked distinctions between groups. Compared with patients in the low APACHE II group, patients with higher scores exhibited significantly lower MAP, PI, and oxygenation index (OI), alongside significantly higher HR, maximum norepinephrine (NEmax), lactic acid (Lac), and SOFA scores. These findings collectively reflect greater disease severity in the high APACHE II cohort. Regarding clinical outcomes, the median hospital length of stay (LOS) for the entire cohort was 15 days, with a median ICU stay of 4 days and a median mechanical ventilation time (MVt) of 22 hours. Patients in the high APACHE II group demonstrated significantly longer LOS (17.50 vs. 13.50 days), ICU stay (7.00 vs. 2.00 days), and MVt (72.00 vs. 7.00 hours) compared with those in the low APACHE II group (all P < 0.001), indicating more severe illness and prolonged treatment requirements.
Analysis of immune and inflammatory markers further revealed that serum CLEC4D levels were significantly elevated in the high APACHE II group compared with those in the low APACHE II group (344.20 ± 65.75 pg/mL vs. 321.28 ± 73.31 pg/mL; P = 0.002) (Table 2). A smooth curve fitting analysis demonstrated a clear linear increase in CLEC4D concentration with rising APACHE II scores (Figure S1). Patients in the high APACHE II group also exhibited significantly higher IL-10 levels (138.25 vs. 129.4 pg/mL, P = 0.002) and PCT (1.70 vs. 0.34 ng/mL, P = 0.007). In contrast, L was significantly lower among patients with higher APACHE II scores (1.27 vs. 2.80 ×109/L, P = 0.003), although still within the normal range. No significant between-group differences were observed in WBC count, N, or IL-6 levels; however, the median values of these markers in both groups exceeded their respective upper limits of normal.
 |
Table 2 Immune-Inflammation-Related Indicators of the Study Population |
The significantly elevated CLEC4D levels observed in patients with high APACHE II scores suggested a potential correlation between these two indicators. To further characterize this relationship, a smooth curve fitting analysis was performed using a GAM (Figure 2). The model revealed a clear linear association between CLEC4D concentration and APACHE II score. In the graphical output, the solid red line represents the fitted curve between variables, while the shaded blue bands denote the 95% confidence intervals. All models were adjusted for potential confounders, including age, sex, SOFA score, diabetes mellitus, surgical history, and sepsis status. Both univariate and multivariate regression analyses demonstrated that CLEC4D was significantly and positively correlated with APACHE II scores (Table S1). In the fully adjusted multivariate model, each 1 pg/mL increase in serum CLEC4D corresponded to a 0.016-point increase in the APACHE II score (P < 0.05). These findings indicate a robust linear association between circulating CLEC4D levels and the severity of illness in critically ill patients, supporting its potential utility as a quantitative biomarker for SOI assessment.
 |
Figure 2 Association between CLEC4D and APACHE II. Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CLEC4D, C-type lectin domain family 4 member D; SOFA, Sequential Organ Failure Assessment. Note: The smooth fitting curve was adjusted for age, gender, diabetes mellitus, surgery, sepsis, and SOFA score. |
To elucidate the potential mechanisms underlying this association, we further examined the relationships between CLEC4D and key immune-inflammatory markers (Figure 3A–F). Smooth curve fitting analyses revealed generally positive linear relationships between CLEC4D and several markers, including WBC count, N count, IL-10, and PCT, as well as negative linear relationships with L and IL-6. Subsequent regression analyses confirmed that CLEC4D was significantly and inversely correlated with L and IL-6, while demonstrating a significant positive correlation with PCT (Table 3). Although the relationship between CLEC4D and WBC count appeared to be non-linear, threshold and saturation effect analyses identified an inflection point at 356.3 pg/mL. However, no statistically significant association was observed on either side of this threshold (<356.3 pg/mL or ≥356.3 pg/mL). A log-likelihood ratio test comparing linear and non-linear models yielded a non-significant P-value, confirming the absence of a meaningful correlation between CLEC4D and WBC count (Table S2). In the multivariate model, each 1 pg/mL increase in CLEC4D was associated with a 0.028 × 109/L decrease in L (P < 0.001), a 1.405 pg/mL decrease in IL-6 (P = 0.021), and a 0.022 ng/mL increase in PCT (P = 0.031). Taken together, these findings suggest that the observed positive association between CLEC4D and APACHE II score may be associated with dynamic shifts in pathways involving lymphocyte depletion, suppression of IL-6–driven inflammation, and increased PCT production.
 |
Table 3 Regression Models Between CLEC4D and Immune-Inflammatory Indicators |
 |
Figure 3 Smooth fitting curves of CLEC4D and immune-inflammatory indicators. (A) Association with WBC; (B) Association with N; (C) Association with L; (D) Association with IL-6; (E) Association with IL-10; (F) Association with PCT. Abbreviations: CLEC4D, C-type lectin domain family 4 member D; WBC, white blood cell; N, neutrophil; L, lymphocyte; IL, interleukin; PCT, procalcitonin. Note: The smooth fitting curve was adjusted for: (A) age, gender, AID, tumor, surgery, sepsis, and SOFA; (B) tumor, sepsis, and SOFA; (C) SOFA; (D) AID, sepsis, and SOFA; (E) gender, sepsis, and SOFA; (F) gender, tumor, sepsis, and SOFA. |
The robustness of the linear relationship between CLEC4D and APACHE II score was further evaluated through subgroup sensitivity analyses stratified by tumor status and sepsis. As illustrated in Figure 4A, CLEC4D demonstrated a consistent positive linear correlation with APACHE II score in both tumor and non-tumor patients. Similarly, this positive association remained stable regardless of sepsis status (Figure 4B). Multivariate regression models were subsequently applied to refine these observations. All models were adjusted for age, sex, DM, surgical status, sepsis, and SOFA score. In both tumor and non-tumor subgroups, CLEC4D levels were significantly and positively correlated with APACHE II scores, with β values (95% CIs) of 0.018 (0.003, 0.033) and 0.017 (0.002, 0.031), respectively. Among non-tumor patients, CLEC4D exhibited a significant negative correlation with L but no significant relationship with IL-6 or PCT. In contrast, within the tumor subgroup, CLEC4D was significantly and inversely associated with both IL-6 and L, while demonstrating a significant positive correlation with PCT (Table 4). As shown in Table 4, when patients were stratified by sepsis status, the relationship between CLEC4D and APACHE II score was not statistically significant among non-septic patients, although a positive trend was evident (P = 0.070). Conversely, in patients with sepsis, the association was both significant and stronger, with a β value of 0.030 (95% CI: 0.013–0.046). Furthermore, within the septic subgroup, CLEC4D was significantly and negatively correlated with both L and IL-6.
 |
Table 4 Regression Models Between CLEC4D and APACHE II in Different Subgroups |
 |
Figure 4 Smooth fitting curves of CLEC4D and APACHE II in different subgroups. (A) Tumor and non-tumor subgroups; (B) Sepsis and non-sepsis subgroups. Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CLEC4D, C-type lectin domain family 4 member D; SOFA, Sequential Organ Failure Assessment. Note: Smooth fitting curves were adjusted for age, gender, diabetes mellitus, surgery, sepsis, and SOFA. |
Discussion
This prospective study is the first to systematically investigate the relationship between CLEC4D and APACHE II scores in the context of assessing SOI among critically ill patients. Our findings revealed a significant, independent, and positive linear correlation between circulating CLEC4D levels and APACHE II scores, establishing CLEC4D as a promising candidate biomarker for evaluating disease severity. This relationship remained robust across multiple clinical subgroups, particularly among patients with sepsis and those with tumors, reinforcing the consistency and reliability of the observed association. Moreover, mechanistic analyses demonstrated that CLEC4D was significantly correlated with key immune-inflammatory markers, including L, IL-6, and PCT, suggesting that immune-inflammatory pathways may mediate the link between CLEC4D expression and SOI.
Relationship Between CLEC4D and APACHE II Scores and Its Clinical Implications
The principal finding of this study is that the positive linear association between CLEC4D and APACHE II score persisted even after rigorous adjustment for potential confounders, including age, sex, SOFA score, DM, surgical history, and sepsis status. The observation that higher CLEC4D concentrations corresponded to increased APACHE II scores indicates that elevated CLEC4D levels reflect more severe physiological derangement and greater illness burden.
As a pattern recognition receptor predominantly expressed on myeloid cells, CLEC4D functions as a key sentinel in immune and inflammatory signaling.5 Upon exposure to systemic insults such as severe infection or trauma, the immune system initiates a cascade of inflammatory responses. Through recognition of pathogen-associated molecular patterns (PAMPs), CLEC4D contributes to the amplification and modulation of these early immune responses.6 Consequently, elevated CLEC4D levels may serve as an indirect indicator of heightened immune-inflammatory activation, paralleling the systemic dysfunction captured by higher APACHE II scores. Collectively, these findings suggest that CLEC4D represents a novel, quantifiable molecular marker of SOI in critically ill patients. Furthermore, given its integral role in immune regulation, the observed relationship between CLEC4D and APACHE II not only supports its diagnostic value but also provides deeper insight into the immunopathophysiological processes underpinning disease progression in critical illness.
Currently, the CLEC4D test is predominantly utilized in preclinical research settings and is not yet widely available or affordable in routine clinical laboratories. The cost of commercial ELISA kits limits its large-scale clinical application. However, as our study demonstrates, existing scoring systems like APACHE II rely heavily on physiological metrics and may overlook underlying immune-inflammatory derangements. CLEC4D acts as a supplementary immunological window. If future automated and cost-effective assays are developed, adding CLEC4D to existing clinical evaluations could significantly enhance the precision of assessing immune dysregulation and illness severity.
Immune-Inflammation Response: A Potential Mechanism Linking CLEC4D to SOI
To elucidate the potential biological mechanisms underlying the association between CLEC4D and APACHE II score, we further investigated the association between CLEC4D and a panel of representative immune-inflammatory markers. The analyses revealed that CLEC4D was significantly negatively correlated with L and IL-6, and positively correlated with PCT. This distinct “immune-inflammation signature” provides mechanistic insight into the immunopathological role of CLEC4D in critically ill patients.
CLEC4D and Lymphocyte Depletion
A significant negative correlation was observed between CLEC4D and L, a hallmark finding consistent with the immunosuppressive phenotype frequently observed in critically ill and septic patients. Lymphopenia is a well-established indicator of immune exhaustion and poor prognosis in critical illness.7 CLEC4D, an immunomodulatory receptor expressed on myeloid cells, may indirectly influence lymphocyte homeostasis by regulating T cell activity and apoptosis. Experimental studies have demonstrated that CLEC4D-deficient mice exhibit dysregulated inflammatory responses and excessive immune cell infiltration in infectious models,8 underscoring the essential role of CLEC4D in maintaining balanced immune cell activation and turnover. Therefore, elevated CLEC4D levels in critically ill patients may represent a compensatory response to systemic inflammation, yet concurrently indicate intensified lymphocyte depletion and immunosuppression—both of which align with the greater SOI reflected by higher APACHE II scores.
CLEC4D and Negative-Feedback Regulation of IL-6
Another key observation was the inverse relationship between CLEC4D and IL-6. Previous studies have reported that CLEC4D deficiency leads to dysregulated IL-6 production and exacerbated pulmonary inflammation in experimental models.9 IL-6 is a key pro-inflammatory cytokine central to the cytokine storm and organ dysfunction that characterize severe systemic inflammation. Although IL-6 levels typically rise during acute inflammation, the negative correlation observed in our study may indicate an adaptive regulatory mechanism. Specifically, CLEC4D may participate in a negative-feedback loop that modulates excessive cytokine activity. In the early inflammatory phase, an initial surge of pro-inflammatory mediators, including IL-6, may induce CLEC4D expression. Subsequently, increased CLEC4D signaling—potentially through interactions with inhibitory receptors or induction of anti-inflammatory mediators—acts to suppress further IL-6 production and downstream inflammatory amplification. Therefore, elevated CLEC4D levels may reflect an activated endogenous anti-inflammatory response designed to counterbalance cytokine overproduction, although this compensatory mechanism may ultimately contribute to immune dysregulation and severe disease manifestation.
CLEC4D and PCT: Insights into Bacterial Infection and Systemic Inflammation
PCT serves as a well-established biomarker of bacterial infection and systemic inflammatory activation. The significant positive correlation between CLEC4D and PCT observed in our study further supports the involvement of CLEC4D in infection-associated immune responses. During bacterial infection, PAMPs can directly or indirectly stimulate CLEC4D expression on myeloid cells, either through pathogen recognition or cytokine-mediated signaling cascades.8,10 Concurrently, bacterial invasion triggers robust PCT synthesis, reflecting systemic inflammatory burden.11 The parallel elevation of CLEC4D and PCT thus delineates a coordinated host response to severe bacterial infection, highlighting CLEC4D as a key participant in the immune-inflammatory network. These findings suggest that CLEC4D may hold particular clinical relevance in the evaluation of infectious critical illnesses such as sepsis, where immune activation and dysregulation coexist as major determinants of disease severity.
CLEC4D Was Not Significantly Correlated with N and IL-10
Interestingly, no significant correlations were identified between CLEC4D and either N or IL-10 level in the present study. Although CLEC4D is expressed on neutrophils, previous studies8 have reported that CLEC4D deficiency enhances neutrophil infiltration at sites of inflammation, such as the lungs. This phenomenon, however, appears to be predominantly related to localized processes—including chemotaxis, migration, and tissue retention—rather than changes in the circulating neutrophil pool. Furthermore, CLEC4D has not been shown to directly influence neutrophil phagocytic or bactericidal functions, which may explain the absence of a measurable association between serum CLEC4D levels and total neutrophil count.12 Future investigations incorporating tissue-level functional analyses of neutrophils are warranted to clarify the mechanistic interactions between CLEC4D expression and neutrophil behavior in critical illness.
IL-10, a pivotal anti-inflammatory cytokine that undergoes substantial fluctuations in critically ill patients, also demonstrated no significant relationship with CLEC4D in this study.13 Although animal experiments have reported altered IL-10 expression in CLEC4D-deficient models, such findings were not recapitulated in our clinical cohort. Several factors may account for this discrepancy, including (1) species-specific differences in immune regulation, (2) heterogeneity among experimental disease models, and (3) the multifactorial regulation of IL-10 through numerous signaling cascades, among which the CLEC4D-mediated pathway may not exert a dominant or discernible influence in the systemic circulation.
In-Depth Subgroup Analysis: Robustness and Specificity
Subgroup analyses further reinforced the robustness of our primary findings while highlighting potential context-specific differences in CLEC4D’s immunological behavior. In both tumor and non-tumor subgroups, CLEC4D maintained a significant positive correlation with APACHE II score, indicating that its association with SOI was not confounded by the presence of malignancy and suggesting broad clinical applicability. A more striking pattern emerged in the sepsis subgroup, where CLEC4D exhibited the strongest positive correlation with APACHE II score, alongside the most pronounced negative correlations with IL-6 and L. This observation implies that during sepsis—a syndrome characterized by profound immune dysregulation—the CLEC4D pathway is more robustly activated, underscoring its potential as a biomarker particularly relevant to infectious critical illness.14 Conversely, among non-sepsis patients, the association between CLEC4D and APACHE II score, though directionally positive, did not reach statistical significance. This attenuation may reflect distinct immunopathological mechanisms in non-septic critical illness (eg, following major surgery or trauma), in which CLEC4D likely plays a secondary role. Additionally, the smaller sample size in the non-sepsis cohort may have reduced statistical power, limiting the ability to detect a modest association.
The differential correlation profiles of CLEC4D with L, IL-6, and PCT across clinical subgroups—for instance, the relatively stronger positive association with PCT in tumor-bearing and non-septic patients—further emphasize the context-dependent nature of CLEC4D’s immunoregulatory function. These findings suggest that CLEC4D may act as a dynamic modulator within distinct branches of the inflammatory network, fine-tuning downstream signaling pathways in response to specific pathological stimuli. Collectively, this evidence highlights the potential of CLEC4D as a foundation for developing personalized immune assessment strategies tailored to the heterogeneous pathophysiological states encountered in critical illness.
Limitations
The study has several limitations that should be acknowledged. First, as a single-center investigation, the generalizability of our findings is limited and warrants validation in future multicenter studies with larger and more diverse populations. Second, owing to its observational design, causal inferences regarding the relationship between CLEC4D and SOI cannot be definitively established. Experimental studies are therefore required to clarify the mechanistic pathways underlying this association. Third, biomarker measurements were obtained only once—within 24 hours of ICU admission—precluding evaluation of temporal fluctuations and their potential prognostic relevance. Future research should incorporate serial monitoring of CLEC4D levels and integrate these data with dynamic clinical outcomes. Additionally, complementary in vitro and in vivo studies are necessary to delineate the molecular mechanisms through which CLEC4D regulates immune responses in critical illness, particularly its interactions with lymphocyte apoptosis and IL-6 signaling crosstalk. Fourth, while our primary endpoint focused on the correlation between CLEC4D and the APACHE II score, we recognize that APACHE II is a composite physiological score rather than a direct clinical outcome. Although we provided basic clinical outcome data (eg, length of stay, mechanical ventilation time), our study did not evaluate the incremental benefit of CLEC4D using clinical endpoints such as 28-day mortality. Future studies should incorporate these rigorous prognostic evaluations.
Conclusions
Elevated circulating CLEC4D levels in critically ill patients demonstrate a significant positive correlation with APACHE II scores, an association that is particularly pronounced in patients with sepsis. This robust correlation appears to be intrinsically linked to key immune-inflammatory shifts, such as lymphocyte depletion and altered cytokine profiles (such as IL-6 and PCT). As an indicator of underlying immune dysregulation, CLEC4D provides an important biological dimension that complements traditional physiological scoring systems. These findings highlight its potential as an immunological biomarker for assessing disease severity and pave the way for future exploration of CLEC4D-targeted interventions in critical care.
Data Sharing Statement
All datasets used and analyzed during the current study are available from the corresponding author, Hui Lian ([email protected]), on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Peking Union Medical College Hospital, Beijing, China (Approval No. I-24PJ2082). Written informed consent was obtained from all participating patients prior to enrollment. For patients who were unconscious or otherwise lacked the capacity to provide direct consent due to the severity of their illness, written informed consent was obtained from their legally authorized representatives or next of kin. This study strictly complies with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Guangjian Wang and Zhimao Li contributed equally to this work.
Funding
Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0517200); Peking Union Medical College Hospital Talent Cultivation Program Category D (UHB11894); National High Level Hospital Clinical Research Funding (2025-PUMCH-A-001); Beijing Natural Science Foundation (7264312); Scientific Research Project of Shanxi Provincial Health Commission (2022060).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Pellathy TP, Pinsky MR, Hravnak M. Intensive care unit scoring systems. Crit Care Nurse. 2021;41(4):54–12. doi:10.4037/ccn2021613
2. Cavaillon JM. During sepsis and COVID-19, the pro-inflammatory and anti-inflammatory responses are concomitant. Clin Rev Allergy Immunol. 2023;65(2):183–187. doi:10.1007/s12016-023-08965-1
3. Yang Y, Zhang M, Cai F, et al. CLEC4D as a novel prognostic marker boosts the proliferation and migration of gastric cancer via the NF-kappaB/AKT signaling pathway. Int J Gen Med. 2024;17:1923–1935. doi:10.2147/IJGM.S458228
4. Zhang Y, Wei H, Fan L, et al. CLEC4s as potential therapeutic targets in hepatocellular carcinoma microenvironment. Front Cell Dev Biol. 2021;9:681372. doi:10.3389/fcell.2021.681372
5. Graham LM, Gupta V, Schafer G, et al. The C-type lectin receptor CLECSF8 (CLEC4D) is expressed by myeloid cells and triggers cellular activation through Syk kinase. J Biol Chem. 2012;287(31):25964–25974. doi:10.1074/jbc.M112.384164
6. Zhao XQ, Zhu LL, Chang Q, et al. C-type lectin receptor dectin-3 mediates trehalose 6,6’-dimycolate (TDM)-induced Mincle expression through CARD9/Bcl10/MALT1-dependent nuclear factor (NF)-kappaB activation. J Biol Chem. 2014;289(43):30052–30062. doi:10.1074/jbc.M114.588574
7. Drewry AM, Samra N, Skrupky LP, Fuller BM, Compton SM, Hotchkiss RS. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock. 2014;42(5):383–391. doi:10.1097/SHK.0000000000000234
8. Wilson GJ, Marakalala MJ, Hoving JC, et al. The C-type lectin receptor CLECSF8/CLEC4D is a key component of anti-mycobacterial immunity. Cell Host Microbe. 2015;17(2):252–259. doi:10.1016/j.chom.2015.01.004
9. Wang T, Pan D, Zhou Z, et al. Dectin-3 deficiency promotes colitis development due to impaired antifungal innate immune responses in the gut. PLoS Pathog. 2016;12(6):e1005662. doi:10.1371/journal.ppat.1005662
10. Kerscher B, Wilson GJ, Reid DM, et al. Mycobacterial receptor, Clec4d (CLECSF8, MCL), is coregulated with Mincle and upregulated on mouse myeloid cells following microbial challenge. Eur J Immunol. 2016;46(2):381–389. doi:10.1002/eji.201545858
11. Hamade B, Huang DT. Procalcitonin: where Are We Now? Crit Care Clin. 2020;36(1):23–40. doi:10.1016/j.ccc.2019.08.003
12. Steichen AL, Binstock BJ, Mishra BB, Sharma J. C-type lectin receptor Clec4d plays a protective role in resolution of Gram-negative pneumonia. J Leukoc Biol. 2013;94(3):393–398. doi:10.1189/jlb.1212622
13. Ip WKE, Hoshi N, Shouval DS, Snapper S, Medzhitov R. Anti-inflammatory effect of IL-10 mediated by metabolic reprogramming of macrophages. Science. 2017;356(6337):513–519. doi:10.1126/science.aal3535
14. Vincent JL, Opal SM, Marshall JC, Tracey KJ. Sepsis definitions: time for change. Lancet. 2013;381(9868):774–775. doi:10.1016/S0140-6736(12)61815-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.