Back to Journals » Biologics: Targets and Therapy » Volume 19
Circulating PGC-1α and MOTS-c Peptide as Potential Mitochondrial Biomarkers in Patients Undergoing Aortic Valve Replacement
Authors Sánchez-Quintero MJ, Iboleón A, Martín Chaves L ![]() , Pozo Vilumbrales B, Carmona-Segovia ADM, Martínez López P, Romero-Cuevas M, Rodríguez-Capitán J
, Pozo Vilumbrales B, Carmona-Segovia ADM, Martínez López P, Romero-Cuevas M, Rodríguez-Capitán J ![]() , Becerra-Muñoz VM, Pavón-Morón FJ
, Becerra-Muñoz VM, Pavón-Morón FJ ![]() , Murri M
, Murri M
Received 2 November 2024
Accepted for publication 28 February 2025
Published 13 March 2025 Volume 2025:19 Pages 87—96
DOI https://doi.org/10.2147/BTT.S504289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Shein-Chung Chow
María J Sánchez-Quintero,1– 3,* Andrea Iboleón,4,* Laura Martín Chaves,1– 3 Bárbara Pozo Vilumbrales,1,5 Ada DM Carmona-Segovia,1– 3 Pilar Martínez López,1,6 Miguel Romero-Cuevas,1– 3 Jorge Rodríguez-Capitán,1– 3 Víctor M Becerra-Muñoz,1– 3 Francisco Javier Pavón-Morón,1– 3 Mora Murri1,2,7,8
1Instituto de Investigación Biomédica de Málaga y Plataforma en Nanomedicina (IBIMA Plataforma BIONAND), Málaga, Spain; 2Unidad de Gestión Clínica Cardiología y Cirugía Cardiovascular, Hospital Universitario Virgen de la Victoria, Málaga, Spain; 3Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Instituto de Salud Carlos III, Madrid, Spain; 4Unidad Docente Multiprofesional de Atención Familiar y Comunitaria. Distrito de Atención Primaria Málaga-Guadalhorce, Málaga, Spain; 5Department of Animal Biology, University of Málaga, Málaga, Spain; 6Unidad de Gestión Clínica de Cuidados Críticos y Urgencias, Medicina Intensiva. Hospital Universitario Virgen de la Victoria, Málaga, Spain; 7Unidad de Gestión Clínica de Endocrinología y Nutrición, Hospital Universitario Virgen de la Victoria, Málaga, Spain; 8Centro de Investigación Biomédica en Red de la Fisiopatología de la Obesidad y Nutrición (CIBEROBN), Instituto de Salud Carlos III, Madrid, Spain
*These authors contributed equally to this work
Correspondence: Francisco Javier Pavón-Morón, Instituto de Investigación Biomédica de Málaga y Plataforma en Nanomedicina (IBIMA Plataforma BIONAND), Málaga, 29590, Spain, Email [email protected] Mora Murri, Unidad de Gestión Clínica de Endocrinología y Nutrición, Hospital Universitario Virgen de la Victoria, Málaga, 29010, Spain, Email [email protected]
Purpose: Aortic valve disease (AVD) is a common condition that leads to pressure and/or volume overload in the left ventricle. Aortic valve replacement is the standard treatment, as no pharmacological therapies are currently available. The incidence of AVD is increasing in developed countries, making the discovery of new biomarkers for early detection crucial. The importance of mitochondria in heart function is well established, and various cardiovascular pathologies are associated with mitochondrial dysfunction. In this cross-sectional study, we evaluated for the first time the role of mitochondria in AVD, aiming to identify new pathways involved in the disease and discover potential biomarkers.
Patients and Methods: We recruited 17 patients diagnosed with AVD and scheduled for aortic valve replacement, and 22 healthy controls. Plasma levels of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC1α) and mitochondrial open reading frame of the 12S rRNA type-c peptide (MOTS-c) were measured by ELISA.
Results: We observed significantly reduced levels of both proteins in patients, suggesting that substantial mitochondrial dysfunction occurs in AVD patients, independent of sex or age, but directly related to the disease.
Conclusion: Mitochondria may represent a promising target for studying new pathways involved in AVD. We propose PGC1α and MOTS-c as potential plasma biomarkers for AVD detection. Further studies, including early-stage patients, are necessary to confirm the significance of our findings.
Keywords: aortic valve disease, biomarkers, mitochondria, PGC-1α, MOTS-c
Graphical Abstract:

Introduction
Aortic valve diseases (AVDs) are common valve lesions characterized by malfunction of the aortic valve, affecting more than 13% of the population over 75 years old.1 Currently, the incidence of AVD is increasing in developed countries due to the aging population.2,3 The pathophysiology of AVD includes angina, syncope, and dyspnea as late-stage symptoms, which occur after years of left ventricular overload. The lesions may be congenital, acquired, or a combination of both.4 AVD encompasses aortic valve stenosis and aortic valve regurgitation. Degenerative calcific AVD is the most common cause of aortic stenosis,5 leading to a narrowed aortic valve orifice. Due to mechanical stress, blood pressure increases, causing concomitant left ventricular pressure overload.6 Aortic regurgitation, however, can result from AVD and/or abnormalities of the aortic root,2 leading to both pressure and volume overload in the left ventricle. Currently, no pharmacological therapies are available for AVD, and transcatheter or surgical aortic valve implantation is the standard treatment, but only for appropriately selected patients.6,7
Various cardiac diseases are associated with mitochondrial dysfunction. For example, cardiac hypertrophy and heart failure are linked to uncontrolled production of reactive oxygen species (ROS).8 Patients with pulmonary arterial hypertension show decreased activity of complexes I and III in the oxidative phosphorylation system.9 Additionally, due to the high number of mitochondria in the heart, this organ is frequently affected by mitochondrial DNA (mtDNA) mutations, which can trigger the onset of several cardiovascular diseases such as cardiomyopathy, heart failure, arrhythmias, conduction defects, and vascular pathologies.10,11 A role for mitochondria in AVD has also been described in the literature.12 Studies have shown that various pathophysiological mechanisms involving mitochondria contribute to AVD, including oxidative stress and mitochondrial antioxidant capacity,13 hydrogen sulfide metabolism in mitochondria,14 mitochondrial calcium signaling,15 and hypoxia signaling leading to mitochondrial dysfunction.1 Impaired mitochondrial dynamics have also been implicated in AVD.16
Mitochondria possess their own genetic material, comprising 37 genes, including those involved in oxidative phosphorylation as well as genes encoding transfer RNA (tRNA) and ribosomal RNA (rRNA). A regulatory peptide named mitochondrial open reading frame of the 12S rRNA type-c (MOTS-c), encoded by mitochondrial 12S rRNA, was recently discovered.17 MOTS-c has been extensively studied as a mitokine, a signaling molecule that communicates mitochondrial stress in affected tissues to distant cells or tissues.18 Several studies have demonstrated the protective role of MOTS-c in cardiovascular diseases. MOTS-c prevents the development of heart failure, alleviates diabetic myocardial injury, and repairs myocardial damage in diabetic rats.19–21 Another crucial player in mitochondrial function is peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC1α), a protein encoded by the PPARGC1A gene in humans. PGC1α is a master regulator of mitochondrial biogenesis22–24 and is highly expressed in cardiac cells. PGC1α plays a protective role in certain cardiac diseases, such as myocardial ischemia/reperfusion (I/R) injury, by reducing mitochondrial membrane potential and, consequently, oxidative stress in mitochondria.25 PGC1α is also involved in the cardioprotective effects of tilianin and syringin in diabetic cardiomyopathy.26
There remain significant knowledge gaps in the diagnosis and treatment of AVD. For instance, these include the criteria for surgical intervention in asymptomatic patients, the assessment of severity in cases of aortic stenosis with low flow and low gradient, and the correlation between symptoms and valvular disease in patients with comorbidities that mimic valvular disease symptoms. In the present study, we focused on late-stage patients to expand our understanding on the involvement of mitochondria in AVD, a topic that is still poorly explored in the literature. Given their reported protective roles in other cardiovascular diseases, we measured plasma levels of PGC1α and MOTS-c as markers of mitochondrial function. To the best of our knowledge, this is the first study to assess these mitochondrial markers in the context of AVD. Additionally, we analyzed citrate synthase (CS) levels, an important mitochondrial enzyme commonly used as a quantitative marker for the presence of intact mitochondria. Considering the urgency of identifying early signs of the disease in asymptomatic patients, our ultimate goal is to discover or suggest new biomarkers for AVD diagnosis.
Materials and Methods
Ethics Statements
The present study was approved by the Regional Ethics Committee (Málaga Provincial Research Ethics Committee, Málaga, Spain) (code: 1981-N-21), in agreement with the World Medical Association Declaration of Helsinki. All participants were properly informed about the procedures, the aim of the study and privacy rights. Signing a written informed consent form was a requirement for all participants.
Participants and Patient Recruitment
This cross-sectional study comprised a total of 39 participants, categorized into two groups: a) Disease group or AVD group; and b) Healthy Control (HC) group. The AVD group consisted of 17 patients with AVD (9 men and 8 women), who were evaluated at Hospital Universitario Virgen de la Victoria (Málaga, Spain). All patients were indicated for aortic valve replacement. The clinical evaluation included blood test, electrocardiogram, echocardiogram and invasive coronarography. Clinical data of patients are summarized in Table 1. Patient eligibility criteria were defined as follows: 1) Patients with significant AVD, including stenosis and/or regurgitation, with at least one reaching a severe degree, who present with clinical indications for surgical intervention; 2) Age greater than 65 years; 3) Absence of mitochondrial pathology or comorbidities that could affect plasma levels of the mitochondrial proteins studied: PGC1α, MOTS-c, and CS. The control group consisted of 22 healthy individuals (12 men and 10 women) who attended for a routine blood test. Healthy controls were matched for sex and age, and were recruited at a primary care center (Centro de Salud Colonia Santa Inés, Málaga, Spain). The eligibility criteria included: 1) Age greater than 65 years; 2) Absence of cardiovascular or mitochondrial pathologies.
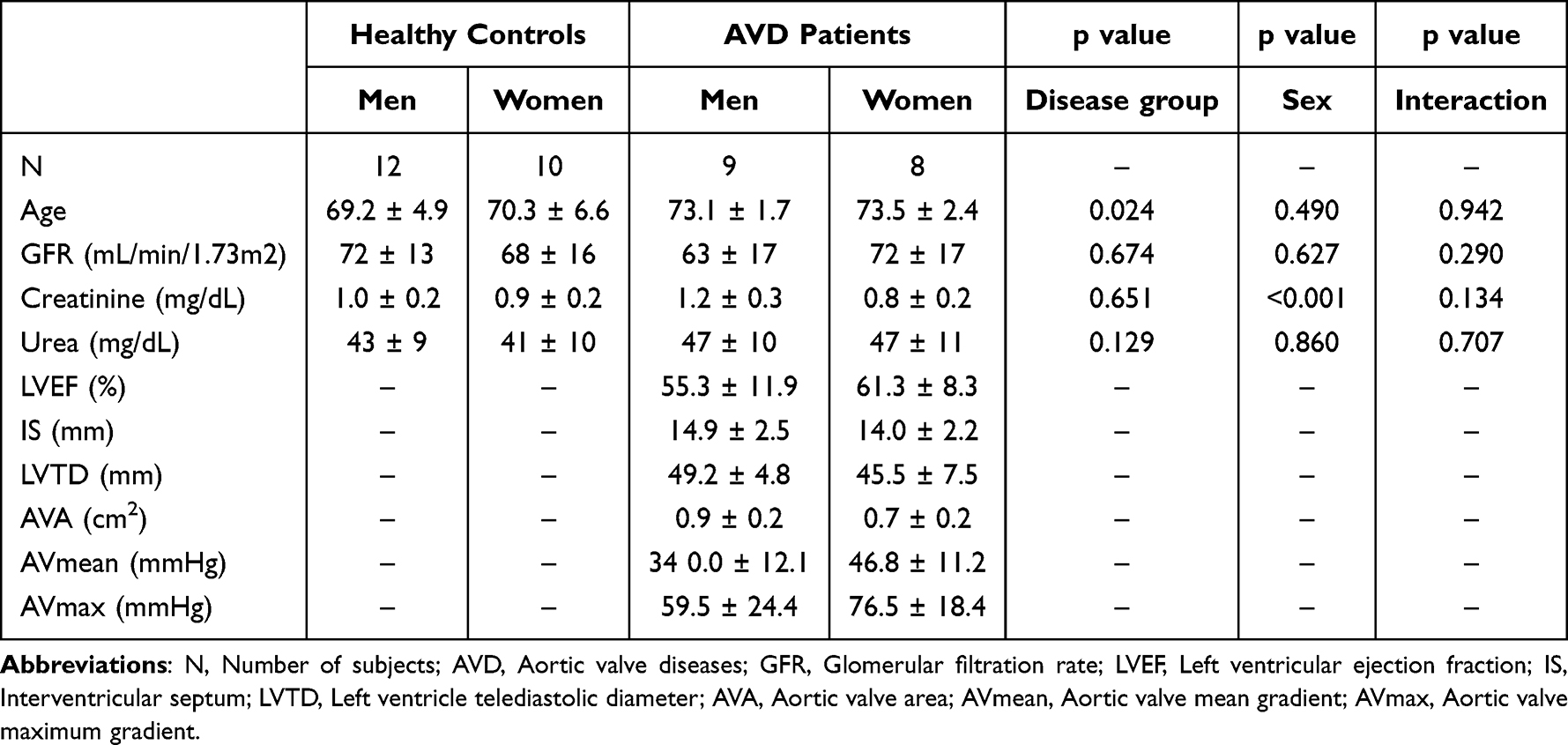 |
Table 1 Clinical Variables of Each Group |
Sample Collection and Biochemical Determinations
Samples were collected from patients at the time of surgery. A total of 3 mL of peripheral venous blood were collected from patients and controls after fasting 12-hour overnight. Samples were centrifugated at 2200 g during 15 minutes at 4 °C. Plasma was separated in aliquots and immediately frozen at −80 °C until their analysis. Plasma was collected from each participant and glomerular filtration rate (GFR), creatinine and urea were determined by standard enzymatic methods, using the hospital analyses service.
Determination of Circulating Mitochondrial Markers
To explore the role of mitochondria in AVD we selected three key proteins involved in mitochondrial activity, PGC1α, MOTS-c and CS, and we analyzed their plasma levels in patients. Quantitative measurement of PGC1α, MOTS-c and CS were performed in plasma from patients and controls using ELISA Kits from MyBioSource (San Diego, CA, USA), following manufacturer´s instructions. Absorbance at 450 nm was read in a microplate reader, and the concentrations of targets were calculated. The intra-assay coefficient of variation was less than 10%, while the inter-assay coefficient of variation was less than 12%. The selected ELISA kits have high sensitivity and excellent specificity for detection of PGC1α, MOTS-c and CS, respectively, and they are specific enzyme immunoassay techniques for the in vitro quantitative measurement of these markers in human serum or plasma.
Statistical Analysis
The results are expressed as either mean values ± standard deviation (SD), or median and interquartile range (IQR), unless otherwise stated. The normality of the datasets was assessed with the Kolmogorov–Smirnov test. Post-hoc power analysis for two-way Mann–Whitney tests assessing plasma levels of PGC1α, MOTS-c, and CS was conducted using G*Power (version 3.1.9.4). For each marker, the recruited sample size, observed mean values, SD, and α = 0.05 were considered.
Metabolic and mitochondrial markers were analyzed using non-parametric statistical procedures due to their non-normal distribution. Specifically, the Mann–Whitney U-test was used to assess differences between two groups, and the Kruskall-Wallis test was applied to assess differences among more than two groups.
Two-way analysis of covariance (ANCOVA) was performed to evaluate the main effects and interaction of independent factors [sample group (HC and AVD) and sex (men and women)] on PGC1α, MOTS-c and CS levels while controlling for age. Since PGC1α, MOTS-c, and CS concentrations exhibited a positively skewed distribution and did not pass the normality test, the raw data were log10-transformed to meet the parametric assumptions of ANCOVA. The estimated marginal means and 95% confidence interval (95% CI) of the log10-transformed PGC1α, MOTS-c and CS concentrations were back-transformed and displayed in the figures. Sidak’s test was used for post-hoc pairwise comparisons.
A logistic regression model was developed to differentiate between HC and AVD based on PGC1α, MOTS-c, and CS concentrations. Receiver operating characteristic (ROC) analysis was performed to evaluate the model’s accuracy using the area under the curve (AUC) along with estimates of sensitivity and specificity.
Spearman correlation (rho) tests were calculated to assess the association between age and the concentrations of these analytes.
All statistical analyses were conducted using the PSPP (GNU software) and GraphPad Prism (GraphPad Software, San Diego, CA, USA) programs. A p-value less than 0.05 was considered statistically significant.
Results
Characteristics of Subjects
We recruited 9 male and 8 female AVD patients, all of whom were indicated for surgical intervention. Additionally, we recruited 22 subjects as the control group. Demographic and clinical characteristic of subjects are detailed in Table 1. None of the controls presented cardiovascular issues or mitochondrial diseases. Age was slightly lower in controls respect to AVD patients. The observed difference is, however, clinically irrelevant, although is considered in further statistical analysis. Regarding the biochemical parameters, we measured GFR, creatinine and urea levels in blood. Results showed no significant differences between groups in GFR and urea levels. However, creatinine showed significant lower values in women. In the cardiac evaluation of the patients, we measured the left ventricular ejection fraction (LVEF), interventricular septum thickness (IS), left ventricular end-diastolic diameter (LVED), aortic valve area (AVA), aortic valve mean gradient (AVmean), and aortic valve maximum gradient (AVmax). The mean values of AVA, AVmean, and AVmax were calculated considering only patients with stenosis, that was observed in 5 men and 6 women. Additional data related to the clinical characteristics of the studied patients are presented in Table S1.
Decreased Levels of Circulating PGC1α, and MOTS-c in AVD Patients
When plasma levels of potential mitochondrial markers were analyzed, we found that AVD patients exhibited significantly lower levels of PGC1α and MOTS-c compared to healthy controls (Figure 1a and b). However, no statistical differences were observed in plasma levels of CS between AVD patients and the control group (Figure 1c). The achieved statistical power for PGC1α, MOTS-c and CS were 0.9999, 0.9997 and 0.0519, respectively. Since the reported decline in PGC1α with age could act as a confounding factor, particularly in our older patient population, we performed a correlation analysis between age and PGC1α levels. We observed that only the healthy control group showed a negative correlation between PGC1α levels and age (r = −0.4935, p = 0.0230), whereas no correlation was found in the patient group (r = −0.1366, p = 0.6120).
 |
Figure 1 Plasma levels of PGC1α, MOTS-c and CS in controls and AVD patients. Plasma levels of PGC1α (a), MOTS-c (b) and CS (c) in controls and AVD patients. Median and IQR are represented. Mann–Whitney U-test was used for analysis and asterisks denote significant differences compared with healthy controls (***, p<0.0001). |
Mitochondrial Proteins Concentration Based on Sample Group and Sex
To assess whether sex or age affect to the levels of the mitochondrial markers, values of plasma concentration of PGC1α, MOTS-c and CS were analyzed using a two-way ANCOVA, with sample group and sex as factors, while controlling for age. The statistical analysis found a main effect on the interaction between groups (HC and AVD patients) and mitochondrial proteins PGC1α and MOTS-c (Figure 2a and b, respectively), but not CS (Figure 2c). In contrast, no effect was found when the interaction between age and mitochondrial proteins were analyzed. Finally, no interaction was found between sex and mitochondrial proteins.
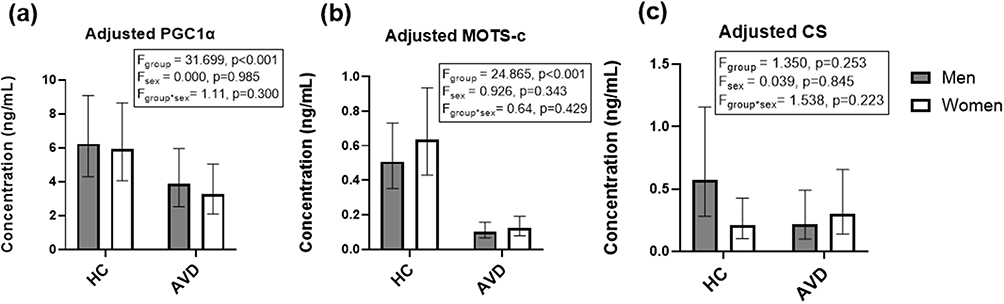 |
Figure 2 Plasma concentrations of PGC1α (a), MOTS-c (b) and CS (c) based on the sample group and sex factors. Plasma concentrations of PGC1α (a), MOTS (b) and CS (c) based on the sample group and sex factors. A two-way ANCOVA test was run with sample group (HC and AVD) and sex (men and women) as factors while controlling for age. The raw data were log10-transformed to meet the parametric assumptions of ANCOVA. The bars represent the estimated marginal means and 95% CI after back-transformation. F-statistics and p-values of ANCOVA are shown. N.s. denotes non-significant differences. |
Mitochondrial Protein Concentrations as Potential Biomarkers to Differentiate AVD Patients
Since PGC1α, MOTS-c and CS concentrations were examined in HC and AVD patients and significant differences were observed, we examined their potential as biomarkers using a logistic regression model (Table S2). As expected, these proteins were identified as predictive variables to distinguish AVD patients from healthy subjects. Furthermore, the ROC analysis showed a significant AUC of 0.989 (p < 0.001) (Figure 3a) and revealed a high discriminatory power of the model (Figure 3b).
 |
Figure 3 ROC analysis of the regression model. ROC curve analysis (a) and resulting probabilities (b) derived from a logistic regression model incorporating the concentrations of PGC1α, MOTS-c, and CS. The model demonstrated excellent predictive power, with an AUC of 0.989 (p < 0.001). |
Discussion
AVD is a type of heart valve disease in which normal blood flow is compromised due to a damaged or diseased aortic valve. The pathology can develop over several years, but symptoms are often detected only in the later stages, when the disease becomes severe. In this study, our aim was to identify new potential targets for the assessment of AVD. Mitochondrial dysfunction has been reported as relevant in various cardiovascular diseases.8,11,27,28 Given the importance of mitochondria in these conditions, we sought to investigate their role in AVD. We selected PGC1α, MOTS-c, and CS as mitochondrial markers due to their relevance in mitochondrial function and their involvement in cardiovascular diseases.
Our results revealed a significant decrease in plasma levels of PGC1α in AVD patients compared to the control group, indicating mitochondrial biogenesis dysfunction. The decrease in PGC1α expression in various tissues with aging is well documented.29–31 However, our patient and control groups were age-matched, and our statistical analyses showed that age only correlated with PGC1α levels in the HC group, not in the AVD group. Our findings suggest that the downregulation of PGC1α in AVD patients is independent of age, highlighting a dysregulation in mitochondrial biogenesis signaling as a potential disease mechanism in AVD.
Regarding the MOTS-c peptide, it has been previously reported as a mitokine, with a well-documented protective role in cardiovascular diseases, including the prevention of heart failure, alleviation of diabetic myocardial injury, and repair of myocardial damage.19–21 Consistent with these findings, we observed a marked decrease in plasma MOTS-c levels in AVD patients, all of whom were scheduled for aortic valve replacement.
In terms of CS, we found no significant differences in circulating levels between AVD patients and controls. CS is a mitochondrial enzyme encoded by the nuclear genome and localized within the mitochondrial matrix, responsible for the condensation of acetyl-CoA and oxaloacetate to form citrate. Its levels or activity are commonly used as a marker of mitochondrial mass.32–34 The similarity in CS plasma levels between AVD patients and controls suggests that the differences observed in PGC1α and MOTS-c are not due to alterations in mitochondrial mass, but rather to a failure to maintain normal levels of mitochondrial regulatory proteins in patients.
Although aortic stenosis tends to have a male predominance, men and women are equally represented among patients older than 75 years.4 In our study, we found no sex-related differences in plasma levels of PGC1α or MOTS-c. Therefore, our findings suggest that the mitochondrial dysfunction observed in AVD patients is primarily related to the disease itself, with neither sex nor age playing a significant role in the development of this dysfunction.
Several limitations of this study should be acknowledged. Although the sample number was small, according to the post-hoc power analysis, our sample size was large enough to detect the dramatic decreased of PGC1α and MOTS-c plasma levels observed in AVD patients. Furthermore, the logistic regression model used in this study supports the conclusion that these proteins are predictive variables capable of distinguishing AVD patients from healthy subjects. However, a proper validation in an independent cohort would be desirable to confirm our results. Second, this is a cross-sectional study, and longitudinal studies are needed to better understand how these markers evolve with disease progression. Notably, we studied late-stage patients, all of whom were scheduled for aortic valve replacement. It would be valuable to recruit early-stage or asymptomatic patients to assess the potential of these mitochondrial proteins as biomarkers for the early diagnosis of AVD.
Conclusions
In conclusion, we have demonstrated that the significant decreases in plasma levels of PGC1α and MOTS-c peptide observed in AVD patients are not associated with age—at least within the age range of the patients included in this study—or sex. This suggests that the observed mitochondrial dysfunction is most likely linked to the disease itself. Further studies involving patients at earlier stages of the disease are needed to validate the relevance of our findings and to explore the potential role of PGC1α and MOTS-c peptide as biomarkers for aortic valve disease.
Abbreviations
ANCOVA, Analysis of covariance; ANOVA, Two-way analysis of variance; AUC, Area under the curve; AVA, Aortic valve area; AVDs, Aortic valve diseases; AVmax, Aortic valve maximum gradient; AVmean, Aortic valve mean gradient; CI, Confidence interval; CS, Citrate synthase; GFR, Glomerular filtration rate; HC, Healthy Control; IS, Interventricular septum thickness; I/R, Ischemia/Reperfusion; LVED, Left ventricular end-diastolic diameter; LVEF, Left ventricular ejection fraction; MOTS-c, Mitochondrial open reading frame of the 12S rRNA type-c; mtDNA, Mitochondrial DNA; PGC1α, Peroxisome proliferator-activated receptor gamma coactivator 1-alpha; ROC, Receiver operating characteristic; ROS, Reactive oxygen species; rRNA, Ribosomal RNA; SD, Standard deviation; tRNA, Transfer RNA.
Data Sharing Statement
The data are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Informed consent was obtained from all subjects involved in the study. The present study was approved by the Regional Ethics Committee (Málaga Provincial Research Ethics Committee, Málaga, Spain) (code: 1981-N-21), in agreement with the World Medical Association Declaration of Helsinki. All participants were properly informed about the procedures, the aim of the study and privacy rights.
Acknowledgments
The authors would like to thank all patients and healthy volunteers for their participation in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by IBIMA Plataforma BIONAND (Ayuda Area 1 Plan Propio I+D+i IBIMA 2021); project funded by Consejería de Transformación Económica, Industria, Cono-cimiento y Universidades from Junta de Andalucía and ERDF/ESF (ProyExcel_01009); CIBERCV (CB16/11/00360) funded by Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación-from Gobierno de España and ERDF/ESF; Consejería de Salud y Consumo, Junta de Andalucía (PI-0245-2021). In addition, this study was supported by the following individual programs: M.J.S.Q. holds a Senior Postdoc Researcher contract funded by University of Málaga (Incorporación de Doctores del II Plan Propio de Investigación, Transferencia y Divulgación Científica de la Uni-versidad de Málaga en 2023); F.J.P.M. holds a Nicolas Monardes contract funded by Servicio Andaluz de Salud (C1-0049-2019); V.M.B.M. holds a Juan Rodés contract (AES 2022, N° Exp. JR22/00067); M.M. holds a Miguel Servet II contract (CPII22-00013) from ISCIII and co-funded by the European Union, and a Nicolas Monardes contract funded by Servicio Andaluz de Salud (C1-0002-2022). M.M. is supported by the projects “PI19/00507” and ‘PI23/00293’ from ISCIII and co-funded by the European Union. M.M. is also supported by UMA18-FEDERJA-285 co-funded by Malaga University, Junta de Andalucia and FEDER funds, CB06/03/0018 and PI-0297-2018 co-funded by FEDER funds and Consejeria de Salud y Consumo, Junta de Andalucia, Spain. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bouhamida E, Morciano G, Pedriali G, et al. The Complex Relationship between Hypoxia Signaling, Mitochondrial Dysfunction and Inflammation in Calcific Aortic Valve Disease: insights from the Molecular Mechanisms to Therapeutic Approaches. Int J mol Sci. 2023;24(13):11105. doi:10.3390/ijms241311105
2. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Rev Esp Cardiol. 2022;75(6):524. doi:10.1016/j.rec.2022.05.006
3. Yadgir S, Johnson CO, Aboyans V, et al. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990-2017. Circulation. 2020;141(21):1670–1680. doi:10.1161/CIRCULATIONAHA.119.043391
4. Bonow RO, Leon MB, Doshi D, Moat N. Management strategies and future challenges for aortic valve disease. Lancet. 2016;387(10025):1312–1323. doi:10.1016/S0140-6736(16)00586-9
5. Nick SRL, Zahid Khan GFW, Watts GF. Lipoprotein(a) and calcific aortic valve disease: current evidence and future directions. Curr Opin Clin Nutr Metab Care. 2024;27(1):77–86. doi:10.1097/MCO.0000000000000976
6. Joseph J, Naqvi SY, Giri J, Goldberg S. Aortic Stenosis: pathophysiology, Diagnosis, and Therapy. Am J Med. 2017;130(3):253–263. doi:10.1016/j.amjmed.2016.10.005
7. Fishbein GA, Fishbein MC. Pathology of the Aortic Valve: aortic Valve Stenosis/Aortic Regurgitation. Curr Cardiol Rep. 2019;21(8). doi:10.1007/s11886-019-1162-4
8. Siasos G, Tsigkou V, Kosmopoulos M, et al. Mitochondria and cardiovascular diseases—from pathophysiology to treatment. Ann Transl Med. 2018;6(12):256. doi:10.21037/atm.2018.06.21
9. Suliman HB, Nozik-Grayck E. Mitochondrial Dysfunction: metabolic Drivers of Pulmonary Hypertension. Antioxid Redox Signal. 2019;31(12):843–857. doi:10.1089/ars.2018.7705
10. Korepanov VA, Rebrova TY, Batalov RE, Afanasiev SA. Mitochondrial DNA Mutations in Cardiovascular Diseases. Russ J Genet. 2023;59(7):637–641. doi:10.1134/S1022795423070062
11. Dabravolski SA, Khotina VA, Sukhorukov VN, et al. The Role of Mitochondrial DNA Mutations in Cardiovascular Diseases. Int J mol Sci. 2022;23(2):952. doi:10.3390/ijms23020952
12. Phadwal K, Vrahnas C, Ganley IG, Macrae VE. Mitochondrial Dysfunction: cause or Consequence of Vascular Calcification. Front Cell Dev Biol. 2021;16(9):611922. doi:10.3389/fcell.2021.611922
13. Roos CM, Zhang B, Hagler MA, et al. Effects of Altering Mitochondrial Antioxidant Capacity on Molecular and Phenotypic Drivers of Fibrocalcific Aortic Valve Stenosis. Front Cardiovasc Med. 2021;8(June):1–11. doi:10.3389/fcvm.2021.694881
14. Eva K, Petra E, Whiteman M, et al. Redox Biology Hydrogen sulfide as an anti-calcification stratagem in human aortic valve: altered biogenesis and mitochondrial metabolism of H 2 S leads to H 2 S deficiency in calcific aortic valve disease. Redox Biol. 2023;60:102629. doi:10.1016/j.redox.2023.102629
15. Cherpaz M, Meugnier E, Seillier G, et al. Myocardial transcriptomic analysis of diabetic patients with aortic stenosis: key role for mitochondrial calcium signaling. Cardiovasc Diabetol. 2024;23(1):239. doi:10.1186/s12933-024-02329-5
16. Abudupataer M, Zhu S, Yan S, et al. Aorta smooth muscle-on-a-chip reveals impaired mitochondrial dynamics as a therapeutic target for aortic aneurysm in bicuspid aortic valve disease. Elife. 2021;1–26.
17. Mohtashami Z, Singh MK, Salimiaghdam N, et al. MOTS-c, the Most Recent Mitochondrial Derived Peptide in Human Aging and Age-Related Diseases. Int J mol Sci. 2022;23(19):11991. doi:10.3390/ijms231911991
18. Burtscher J, Soltany A, Visavadiya NP, et al. Mitochondrial stress and mitokines in aging. Aging Cell. 2023;22(2):1–18. doi:10.1111/acel.13770
19. Zhong P, Peng J, Hu Y, et al. Mitochondrial derived peptide MOTS -c prevents the development of heart failure under pressure overload conditions in mice. J Cell Mol Med. 2022;26(21):5369–5378. doi:10.1111/jcmm.17551
20. Tang M, Su Q, Duan Y, et al. The role of MOTS-c-mediated antioxidant defense in aerobic exercise alleviating diabetic myocardial injury. Sci Rep. 2023;13(1):1–12. doi:10.1038/s41598-023-47073-0
21. Wang M, Wang G, Pang X, et al. MOTS-c repairs myocardial damage by inhibiting the CCN1/ERK1/2/EGR1 pathway in diabetic rats. Front Nutr. 2023;9(January):1–12. doi:10.3389/fnut.2022.1060684
22. Abu Shelbayeh O, Arroum T, Morris S, Busch KB. PGC-1α Is a Master Regulator of Mitochondrial Lifecycle and ROS Stress Response. Antioxidants. 2023;12(5):1075. doi:10.3390/antiox12051075
23. Sano M, Wang SC, Shirai M, et al. Activation of cardiac Cdk9 represses PGC-1 and confers a predisposition to heart failure. EMBO J. 2004;23(17):3559–3569. doi:10.1038/sj.emboj.7600351
24. Whitehead N, Gill JF, Brink M, Handschin C. Moderate modulation of cardiac PGC-1α expression partially affects age-associated transcriptional remodeling of the heart. Front Physiol. 2018;9(MAR). doi:10.3389/fphys.2018.00242
25. Di W, Lv J, Jiang S, et al. PGC-1: the energetic regulator in cardiac metabolism. Curr Issues mol Biol. 2018;28:29–46. doi:10.21775/cimb.028.029
26. Yao J, Li Y, Jin Y, et al. Synergistic cardioprotection by tilianin and syringin in diabetic cardiomyopathy involves interaction of TLR4/NF-κB/NLRP3 and PGC1α/SIRT3 pathways. Int Immunopharmacol. 2021;96:107728. doi:10.1016/j.intimp.2021.107728
27. Tokuyama T, Yanagi S. Role of Mitochondrial Dynamics in Heart Diseases. Genes. 2023;14(10):1876. doi:10.3390/genes14101876
28. Culley MK, Chan SY. Mitochondrial metabolism in pulmonary hypertension: beyond mountains there are mountains. J Clin Invest. 2018;128(9):3704–3715. doi:10.1172/JCI120847
29. Sczelecki S, Besse-patin A, Abboud A, et al. Loss of Pgc-1α expression in aging mouse muscle potentiates glucose intolerance and systemic inflammation. Am J Physiol Endocrinol Metab. 2014;306(2):1–20. doi:10.1152/ajpendo.00578.2013
30. Ghosh S, Lertwattanarak R, Lefort N, et al. Reduction in Reactive Oxygen Species Production by Mitochondria From Elderly Subjects With Normal and Impaired Glucose Tolerance. Diabetes. 2011;60(August):2051–2060. doi:10.2337/db11-0121
31. Bo Y, Lihong H, Yunsong L, et al. PGC-1α Controls Skeletal Stem Cell Fate and Bone-Fat Balance in Osteoporosis and Skeletal Aging by Inducing TAZ. Cell Stem Cell. 2018;23(4):615–623. doi:10.1016/j.stem.2018.09.001
32. Wredenberg A, Wibom R, Wilhelmsson H, et al. Increased mitochondrial mass in mitochondrial myopathy mice. Proc Natl Acad Sci. 2002;99(23):15066–15071. doi:10.1073/pnas.232591499
33. Cormio A, Guerra F, Cormio G, et al. Mitochondrial DNA content and mass increase in progression from normal to hyperplastic to cancer endometrium. BMC Res Notes. 2012;5(1):1. doi:10.1186/1756-0500-5-279
34. Costanzini A, Sgarbi G, Maresca A, et al. Mitochondrial Mass Assessment in a Selected Cell Line under Different Metabolic Conditions. Cells. 2019;8(11):1454. doi:10.3390/cells8111454
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.