Back to Journals » Journal of Inflammation Research » Volume 16
Circulating Leukocyte as an Inflammatory Biomarker: Association with Fibrinogen and Neuronal Damage in Acute Ischemic Stroke
Authors Han L ![]() , Wang Z, Yuan J, He J, Deng Y, Zhu DS
, Wang Z, Yuan J, He J, Deng Y, Zhu DS ![]() , Guan YT
, Guan YT
Received 30 November 2022
Accepted for publication 14 March 2023
Published 21 March 2023 Volume 2023:16 Pages 1213—1226
DOI https://doi.org/10.2147/JIR.S399021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Lu Han,1 Ze Wang,1 Jian Yuan,2 Jun He,2 Yun Deng,2 De-Sheng Zhu,1,2 Yang-Tai Guan1
1Department of Neurology, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200127, People’s Republic of China; 2Department of Neurology, Baoshan Branch, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 200444, People’s Republic of China
Correspondence: Yang-Tai Guan, Department of Neurology, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, No. 160, Pujian Road, Shanghai, 200127, People’s Republic of China, Tel +86-13386271865, Fax +86-21-68383482, Email [email protected] De-Sheng Zhu, Department of Neurology, Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, No. 160, Pujian Road, Shanghai, 200127, People’s Republic of China, Tel +86-13564719779, Email [email protected]
Background and Purpose: Leukocytes and fibrinogen are inflammatory markers involved in circulating and central inflammatory response after ischemic stroke. However, the interaction between circulating leukocytes and serum fibrinogen and neuronal injury in acute ischemic stroke (AIS) patients is still unclear. The present study aimed to investigate the association between circulating leukocyte and serum fibrinogen and neuronal injury respectively in AIS.
Methods: A cross-section study with 431 hospitalized AIS patients from department of neurology was performed. Circulating leukocytes and fibrinogen were measured, and neuron-specific enolase (NSE) was detected to evaluate central neuronal damage. A propensity score matching method was used to minimize the effects of confounding factors. The relationship between leukocytes and NSE and fibrinogen was analyzed by linear curve fitting analysis and multiple logistic regression models respectively.
Results: The mean levels of NSE, leukocyte, and fibrinogen were significantly higher in the matched AIS group (n=89) than those of in the healthy control group (n=89) (all p< 0.05). Both serum NSE and fibrinogen were increased with the increasing of leukocyte in AIS patients (both p< 0.05). Smoothed plots suggested that there are linear relationships between leukocyte and NSE and fibrinogen respectively. Multiple logistic regression analysis showed the OR (95%) for the relationship between leukocyte and high NSE were 1.13 (1.01– 1.26, p=0.031) and 1.13 (1.00– 1.28, p=0.048), and between leukocyte and high fibrinogen were 1.40 (1.22– 1.61, p< 0.001) and 1.35 (1.15– 1.58, p< 0.001) in all AIS patients before and after adjusting for potential confounders.
Conclusion: Our study suggests that elevated circulating leukocyte was associated with high fibrinogen and neuronal injury in AIS. Therefore, there may be potential targets among circulating leukocyte, fibrinogen and NSE that should be intervened to reduce inflammatory reaction after ischemic stroke.
Keywords: acute ischemic stroke, fibrinogen, leukocyte, neuron-specific enolase, multivariate analysis
Introduction
Acute ischemic stroke (AIS) is a serious worldwide public health problem with high mortality and disability rates.1 The prevalence of stroke in China and most provinces has continued to increase during the period from 2013 to 2019.2 Post-ischemic inflammation may cause secondary brain injury and systemic immunosuppression. Increasing evidence demonstrates that inflammation is involved in the pathogenesis of brain injury after ischemic stroke.3 Multiple factors and immune cells are involved in the post-stroke immune response, which may lead to blood-brain barrier disruption, oxidative stress, microvascular injury, directing neuronal death.4,5 Early detection and intervention for inflammatory responses after stroke is beneficial for patients.
Fibrinogen, a major determinant of blood viscosity and platelet activation, is involved in the pathophysiological process of inflammation.6,7 Epidemiological studies have demonstrated that fibrinogen levels increase gradually over the first 24h,8 and elevated fibrinogen levels at admission are associated with poor outcomes in AIS patients.9,10 Peripheral circulating leukocytes, recruited by the proinflammatory signals such as immune mediators, are known to be potentially critical in the processes of neuronal damage after stroke.11,12 Additionally, neuron-specific enolase (NSE) has been considered as a reliable neurobiochemical protein marker, which is widely used in the evaluation of neuronal injury in cerebrovascular diseases.13,14
In clinical practice, we observed that both circulating leukocytes and fibrinogen increased in AIS patients. In the mouse model of middle cerebral artery occlusion, we also detected the fibrinogen deposition and neutrophil activation in the ischemic brain lesions. In 2021, Science magazine published an article which showed that fibrin is a critical regulator of neutrophil effector function, and fibrin-neutrophil engagement may be a pathogenic instigator for a prevalent mucosal disease.15 Therefore, clarifying the association between circulating leukocytes and fibrinogen and neuronal injury respectively may identify the potential intersection targets to reduce inflammatory reaction and neuronal damage after ischemic stroke.
Based on current evidence, both circulating leukocytes and fibrinogen infiltrates into ischemic lesion through the damaged blood-brain barrier (BBB) to aggravate the inflammatory reaction after stroke, while the NSE originated from the injured neurons in the lesion can flow into the peripheral circulation (Figure 1). Herein, we hypothesized that there is association between circulating leukocytes and NSE, and interaction between circulating leukocytes and fibrinogen after ischemic stroke. Thus, the present study aimed to assess the association between circulating leukocytes and fibrinogen and neuronal injury accessed by NSE in the AIS patients.
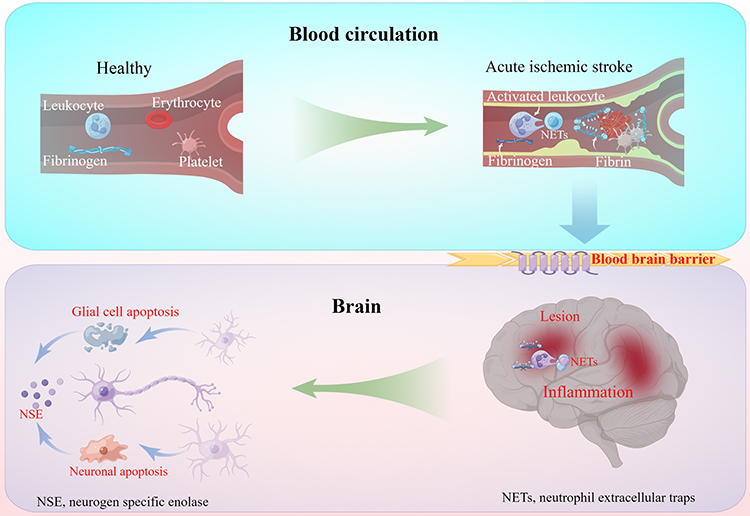 |
Figure 1 Inflammatory response in blood circulation and brain in acute ischemic stroke. Both circulating leukocytes and fibrinogen infiltrates into ischemic lesion through the damaged blood-brain barrier to aggravate the inflammatory reaction after stroke, while the NSE released by the injured neurons in the lesion flow into the peripheral circulation. |
Subjects and Methods
Ethics
In accordance with the Declaration of Helsinki, this study was approved by the ethics committee of Baoshan Branch, Shanghai Jiao Tong University School of Medicine Affiliated Renji Hospital, Shanghai, China (Ethics Approval Number 2022-KSSC-01). All study subjects or their immediate family members (Patients with consciousness disorder or dysarthria after AIS) provided informed consent prior to sample collection.
Design
The study was performed in a cross-sectional design aimed to explore the association between leukocyte and fibrinogen in the AIS patients. Consecutive AIS patients were enrolled in this study from Renji Hospital Baoshan Branch in China from January 1, 2018, and August 31, 2019. In the hospital’s Stroke Registry Database, patient data were recorded.
Study Subjects
AIS patients were diagnosed according to the World Health Organization criteria.16 The inclusion criteria were as follows: (1) AIS onset within 24 hours, (2) clinical symptoms and signs can be evaluated, (3) confirmed by brain imaging [computed tomography (CT) or magnetic resonance imaging (MRI)], and (4) aged 40 years or older.
The exclusion criteria were as follows: (1) transient ischemic attack, (2) intracerebral hemorrhage, (3) malignancies and post-splenectomy, (4) primary thrombocytopenia, megaloblastic anemia, post-splenectomy, leukemia, giant platelet syndrome, and aplastic anemia, (5) cardiac valvulopathy and acute myocardial infarction, and (6) clinical and laboratory data were not available for analysis, including unintegrated patient data.
Healthy control subjects were recruited and matched for age and sex via propensity score matching at the same time as the AIS patients included in our study. The exclusion criteria for the healthy control subjects who underwent health screening were as follows: (1) infection and inflammation within 4 weeks, (2) abnormalities in serum fat, serum sugar, hepatic function, and kidney function, (3) a history of hypertension, diabetes, CHD, and atrial fibrillation, and (4) a history of ischemic stroke, myocardial infarction, thrombophlebitis, and medical interview that might affect leukocytes and fibrinogen.
Clinical Characteristics and Laboratory Data
The baseline data for demographic characteristics, medical history [hypertension, coronary heart disease (CHD), diabetes, and atrial fibrillation], and drugs used before admission (antidiabetic drugs, antihypertensive drugs, lipid lowering drugs, anticoagulant drugs, and antiplatelet drugs) were collected in detail by interviewed with patients and their family members upon admission.
Fasting venous blood samples were obtained within one hour after admission and before administration of therapy, including intravenous recombinant tissue type plasminogen activator (rt-PA) and any angioplasty procedure in the emergency room. Blood sample was collected into an EDTA-containing vacuum tubes to assess levels of fibrinogen, which were measured with a commercially available fibrinogen kit (semi-automatic coagulation instrument) purchased from the Biotechnology Co., Ltd (Shanghai, China). The intra-assay and interassay coefficients of variation were 2.3% and 5.34%, respectively, while the detection limits ranged from 0.39 to 25.0 g/L for fibrinogen, and the normal reference range of fibrinogen ranged between 2 g/L and 4 g/L. Another 2 mL blood sample was collected into an EDTA-containing vacuum tube for leukocyte count, which was detected by XFA6100 automatic hematology analyzer. The intra-assay and interassay coefficients of variation were 4% and 10%, respectively. The normal reference range of leukocyte ranged between 4 and 10 ×1012/L. Levels of NSE were assessed using commercially available quantitative sandwich enzyme-linked immunosorbent assay (ELISA) kits purchased from R&D Systems (Shanghai, China). The intra-assay and interassay coefficients of variation were b=3% and b=7%, respectively. The minimum effective detection limit was 0.229 ng/mL, and the detection values ranged from 0.625 to 40 ng/mL for NSE, and the normal NSE value in our laboratory was < 16.3 mg/L as previously described in our study.17
Fasting blood samples were collected by venipunctures to measure routine blood examination [red blood cell (RBC) count, leukocyte count, lymphocyte count, neutrophil count, and platelet count], serum biochemical indexes [levels of alanine aminotransferase, total bilirubin, fasting blood sugar, creatine, uric acid, urea, homocysteine, glycosylated hemoglobin, and erythrocyte sedimentation rate], blood lipids [levels of triglyceride, low density lipoprotein cholesterol (LDL-C), and high density lipoprotein cholesterol (HDL-C)], clotting indexes (fibrinogen, D-Dimer, partial thromboplastin time, and prothrombin time). All determinations were performed by laboratory technicians blinded to all clinical data.
Groups
All include AIS patients were grouped by two criteria. 1), First, AIS patients were grouped by clinical normal reference values of NSE and fibrinogen in baseline characteristics analysis. High NSE was identified when its value was greater than or equal to 16.3 ng/mL. High fibrinogen was identified when its value was greater than 4 g/L. In additionally, AIS patients were categorized into the T1 (low), T2 (middle) and T3 (high) groups according to the leukocyte tertile levels in multivariate logistic regression for effects of leukocyte on high NSE and high fibrinogen. 2), Second, AIS patients were organized according to the normal reference values of laboratory indicators in the hierarchical analysis, including fasting glucose, LDL-C, and RBC. While dates of ALT, BUN, creatinine, lymphocyte count, and platelet were categorized into low and high groups by dichotomization according to statistical method.
Propensity Score Matching
Propensity score matching was performed to minimize the bias factors and control potential confounding factors between the AIS and healthy control groups based on baseline covariates. Thus, our study used a nearest-neighbor matching algorithm adjust for sex and age, and the tolerable caliper width was 0.01, with a 1:1 individual matching. We compared the levels of leukocyte and fibrinogen between the AIS group and healthy control group, and described the correlation between leukocyte and fibrinogen in the AIS and healthy control groups respectively after propensity score matching.
Statistical Analysis
The characteristics of study participants at baseline are presented by fibrinogen level. Categorical variables presented as frequency counts and percentages were analyzed using Chi-square and Fisher’s exact tests. Continuous variables were presented as means with standard deviations (SE) for normal distribution data, which were analyzed by t-tests, and they were expressed as medians with interquartile ranges (IQR) for abnormal distribution data, which were analyzed by Mann–Whitney U-tests. Differential expression of NSE, leukocyte, and fibrinogen were accessed between the AIS and healthy control groups, and receiver operating characteristic (ROC) analyses were also conducted to validate the difference. The 95% confidence interval (CI) and the area under the ROC curve (AUC) were calculated. An AUC of 1.0 represents perfect discrimination, whereas an AUC of 0.5 represents no discrimination.
The association between leukocyte and high fibrinogen (high NSE) were assessed by linear curve fitting analyses (generalize additive models) and multivariate logistic regression analysis. Baseline variables considered clinically relevant to leukocyte and fibrinogen (NSE) or that showed a univariate relationship with high fibrinogen (high NSE) were selected into multivariate logistic regression model. Both non-adjusted and adjusted models were used, and stratified analyses and interaction testing were performed. Figure 1 was drawn by Figdraw through online software (https://www.figdraw.com/static/index.html). Statistical analyses were performed using the Statistical Package for the Social Sciences Software (SPSS) (version 24.0, Chicago, IL, USA) and R (version 3.6.3). The statistical significance level was set at a two-tailed p-value of <0.05.
Results
Baseline Characteristics
At the time of the final survey in August 2019, a total of 595 consecutive AIS candidates were recruited for the study. Among these AIS candidates, patients who had met any exclusion criteria were excluded (n=37), patients who had missing data related to NSE, leukocyte, fibrinogen, sex and age were also excluded from the eligible candidates for the study (n=95). Those with unreliable values of fibrinogen (<0.5 g/L) (n=17) and those with implausible values of leukocyte (< 2×1012/L) (n=15) were also excluded from the eligible candidates. As a result, a total of 431 AIS subjects were included for the final analyses. According to the clinical normal range of fibrinogen, 431 AIS subjects were categorized into normal and high fibrinogen groups. Meanwhile, a total of 89 cases of healthy control were also included in this study to compare the levels of leukocyte and fibrinogen with 89 cases of AIS matched with age and sex via propensity score matching. A flowchart of the study is shown in Figure 2.
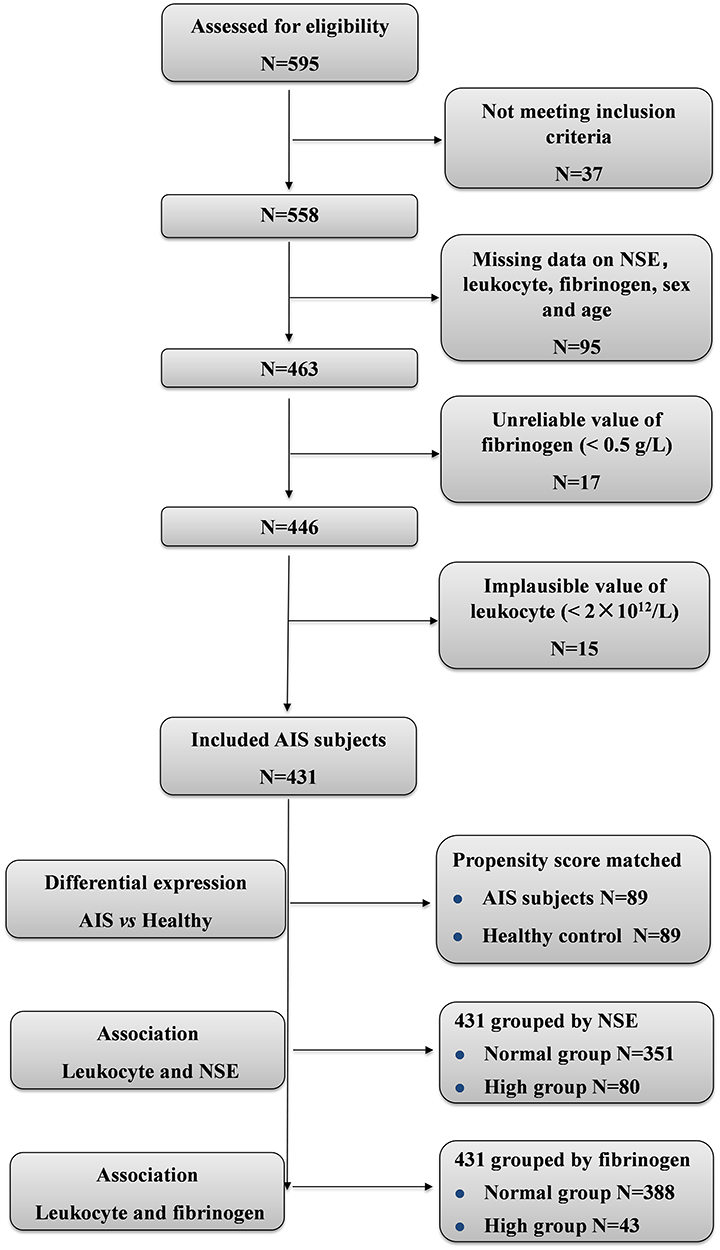 |
Figure 2 A flowchart of the study. |
Among 431 study AIS subjects, women accounted for 46.17% (n=199) and men for 53.83% (n=232). The age of the enrolled subjects ranged from 40 to 99 yr (women, 49–99 yr; men, 40–91 yr) with a mean age of 73.05±10.84 yr (women, 76.39±10.22 yr; men, 70.20±10.56 yr). The disease duration before admission ranged from 0.5 to 46 hours with a median and interquartile range of 7.0 (4.0–17.5) hours. The NSE ranged from 6.56 to 23.82 ng/mL, the leukocyte ranged from 2.26 to 14.15 ×1012/L, and the fibrinogen ranged from 1.23 to 6.23 g/L. The baseline characteristics of the included patients are shown in Tables 1, 2, Supplement Tables 1 and 2.
 |
Table 1 Baseline Characteristics of Participants by Leukocyte Level |
 |
Table 2 Clotting, tumor and medication use of Participants by Leukocyte Level |
Among 89 cases of healthy control, women accounted for 59.55% (n=53) and men for 40.45% (n=36). The age of the enrolled healthy control subjects ranged from 48 to 92 yr (women, 48–92 yr; men, 48–85 yr) with a mean age of 68.31±9.01 yr (women, 69.25±9.69 yr; men, 66.94±7.83 yr). The characteristics of AIS and healthy control groups after propensity score matching by sex and age are shown in Supplement Table 3. Which showed that the baseline characteristics of patients achieved balance between two groups after propensity score matching.
Differential Expression Levels of NSE, Leukocyte, and Fibrinogen in the Healthy Control and the Matched AIS Groups
Between the healthy control and matched AIS groups, there was no difference in sex and age after propensity score matching analysis. The mean level of NSE was higher in the matched AIS group than that of in the healthy control group (14.07 ± 3.13 ng/mL vs 12.79 ± 3.70 ng/mL, p=0.014) (Figure 3A), the mean level of leukocyte was higher in the matched AIS group than that of in the healthy control group (7.27±2.36*1012/L vs 6.11±1.81*1012/L, p<0.001) (Figure 3B), and the level of fibrinogen was also observed higher in the matched AIS group than that of in the healthy control group (2.94±0.81* g/L vs 2.66±0.65 g/L p=0.012) (Figure 3C). The AUC (95% CI) of the ROC curve for NSE, leukocyte, and fibrinogen between the healthy control and the matched AIS groups were 0.655 (0.573–0.736, p<0.001), 0.650 (0.568–0.730, p<0.001), and 0.626 (0.543–0.709, p=0.003), respectively (Figure 3D–F), which validated that the mean levels of NSE, leukocyte, and fibrinogen were higher in the matched AIS group than those of in the healthy control group. In addition, the Person’s correlation coefficient (95%) for the relationship between leukocytes and fibrinogen were 0.321 (0.121–0.496, p=0.002) in the matched AIS group, and 0.045 (−0.165–0.251, p=0.676) in the healthy control group. Which showed that the level of fibrinogen was observed increasing with the elevated level of leukocyte in the matched AIS group, but not in the healthy control group (Supplement Figure 1).
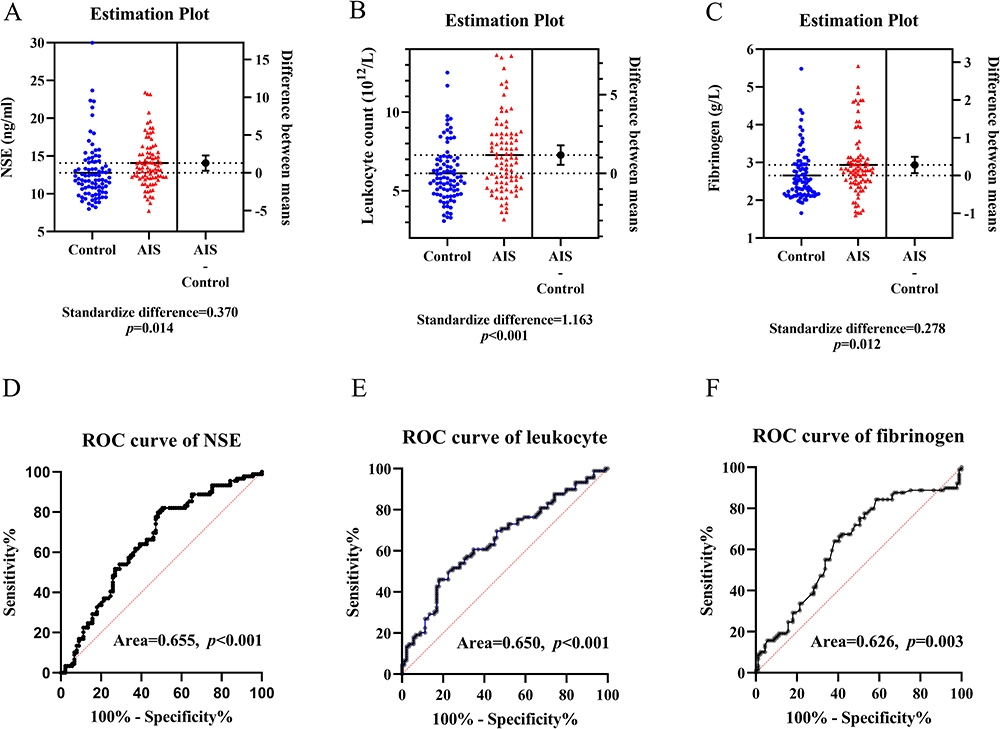 |
Figure 3 Differential expression of NSE, leukocyte and fibrinogen in healthy and AIS groups. (A–C) Between the matched healthy (n=89) and AIS (n=89) groups, mean levels of NSE, leukocyte, and fibrinogen were higher in the matched AIS group than those of in the healthy control group (all p<0.05). (D–F) ROC analysis validated the high expression of NSE, leukocyte, and fibrinogen in the matched AIS group (all p<0.05). |
Differential Expression Levels of NSE and Fibrinogen in AIS Patients Grouped by Leukocyte
In all included AIS patients, the mean serum NSE levels were 13.17±3.08 ng/mL, 13.44±3.30 ng/mL, and 14.11±3.34 ng/mL in the low (T1), middle (T2), and high (T3) leukocyte tertiles for all patients, respectively, and there was a significant difference among the three groups (p=0.002) (Figure 4A). Prevalence of high NSE were 14.69%, 16.08%, and 24.83% in the low (T1), middle (T2), and high (T3) leukocyte tertiles for all patients (p=0.056) (Figure 4B), respectively. Meanwhile, the mean serum fibrinogen levels were 2.67±0.68 g/L, 2.96±0.76 g/L, and 3.21±0.91 g/L in the low (T1), middle (T2), and high (T3) leukocyte tertiles for all patients (p<0.001) (Figure 4C), respectively. Prevalence of high fibrinogen were 4.20%, 9.09%, and 16.55% in the low (T1), middle (T2), and high (T3) leukocyte tertiles for all patients (p<0.001) (Figure 4D), respectively. Which showed that both serum fibrinogen levels and prevalence of high fibrinogen were increased with the increasing of leukocyte levels.
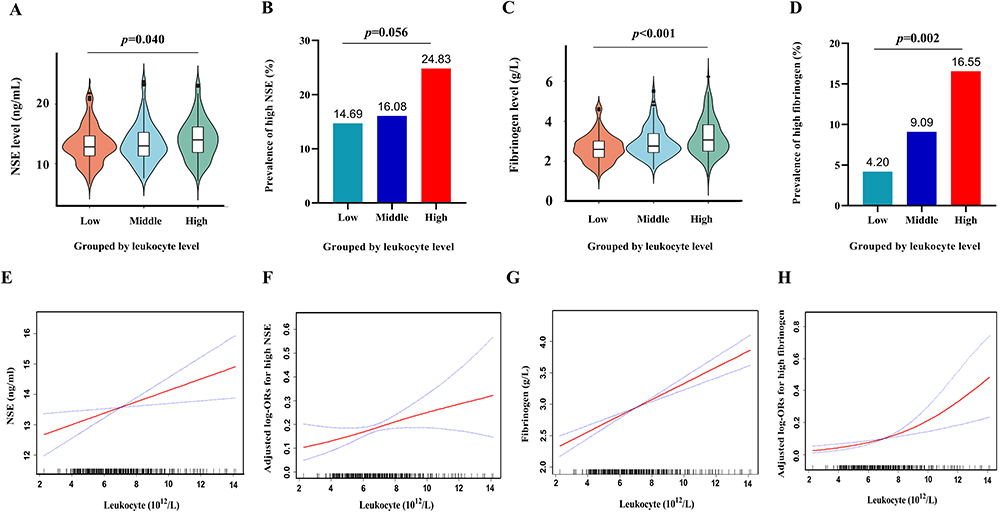 |
Figure 4 Differential expression of NSE and fibrinogen by fibrinogen and their linear curve fitting. (A–D) The mean levels of NSE and fibrinogen, and prevalence of high NSE and high fibrinogen were elevated with the increased leukocyte levels in AIS patients. (E–H) Smoothed plots suggested that there are linear relationships between leukocyte and NSE (high NSE) and fibrinogen (high fibrinogen) respectively after adjusting for confounding factors. Solid lines represent the fitting curve and dotted lines represent the corresponding 95% CI. |
Linear Curve Fitting of the Relationship Between Leukocyte and NSE and Fibrinogen, Respectively
Smoothed plots showed linear relationships between leukocyte and NSE (Figure 4E), and high NSE (Figure 4F) after adjusting for sex, age, CHD, RBC, creatinine, BUN, HCY, LDL-C, and fasting glucose, respectively. Additionally, smoothed plots also detected linear relationships between leukocyte and fibrinogen (Figure 4G), and high fibrinogen (Figure 4H) after adjusting for sex, age, diabetes, lymphocyte count, platelet, ALT, BUN, LDL-C, fasting glucose, lipid lowering drugs, and antiplatelet drugs, respectively. After hierarchical analysis by sex, it showed linear relationships between leukocyte and high fibrinogen in women (p=0.027) and men (p<0.001) (Supplement Figure 2).
Multiple Logistic Regression Analyses of the Relationship Between Leukocyte and High NSE and High Fibrinogen, Respectively
In multiple logistic regression analyses of the relationship between leukocyte and high NSE, baseline variables that were considered relevant to NSE and leukocyte by difference analysis or previous references or that showed a univariate relationship with high NSE were selected into multivariate logistic regression model. As a result, sex, age, CHD, RBC, creatinine, BUN, HCY, LDL-C, and fasting glucose were regarded as confounding factors related to high NSE. In multiple logistic regression analysis, the OR (95%) for the relationship between leukocyte and high NSE were 1.13 (1.01–1.26, p=0.031) and 1.13 (1.00–1.28, p=0.048) in all patients before and after adjusting for sex, age, CHD, RBC, creatinine, BUN, HCY, LDL-C, and fasting glucose. After adjusted confounding factors, the OR (95%) for the relationship between leukocyte and high NSE were 1.26 (1.05–1.51, p=0.011) and 1.09 (0.90–1.32, p=0.369) in men and women, respectively, and the OR (95%) showed a grade increase according to the leukocyte tertile’s by trend analysis (p=0.021) (Table 3), which showed a statistical significance. Hierarchical analysis, according to sex, age, CHD, RBC, creatinine, BUN, HCY, LDL-C, and fasting glucose, also showed that the association between leukocyte and high NSE was statistically significant (Figure 5A, Supplement Table 4).
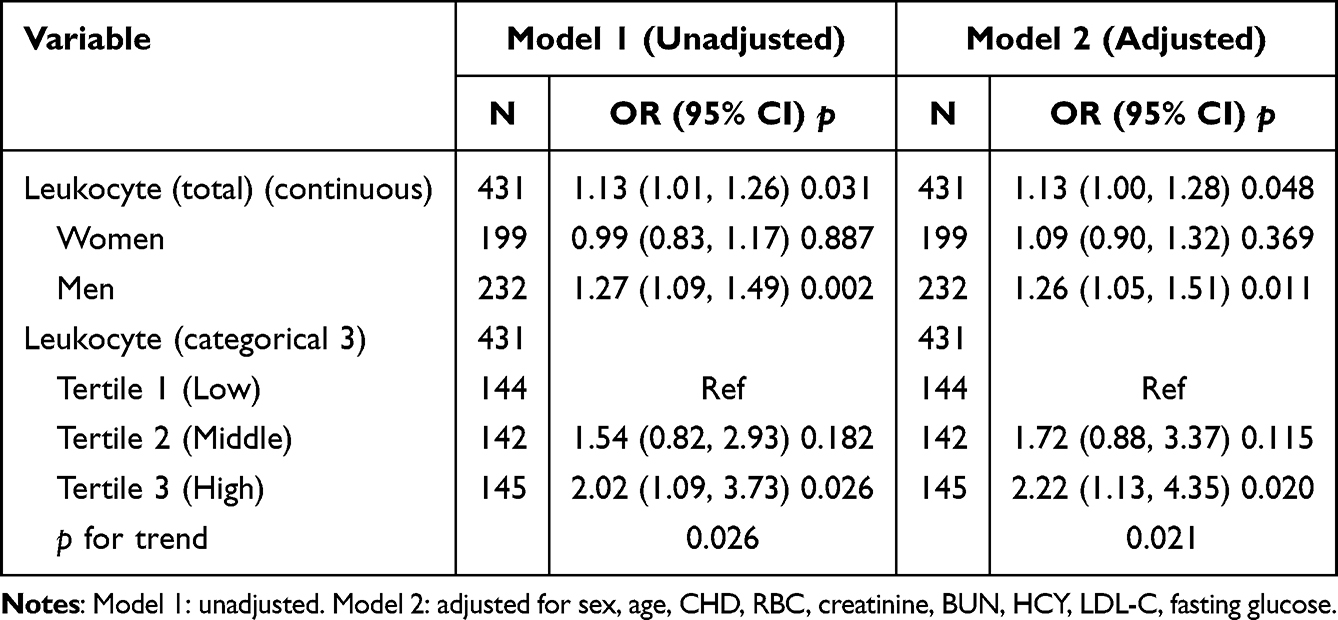 |
Table 3 Multivariate Logistic Regression for Effects of Leukocyte on High NSE |
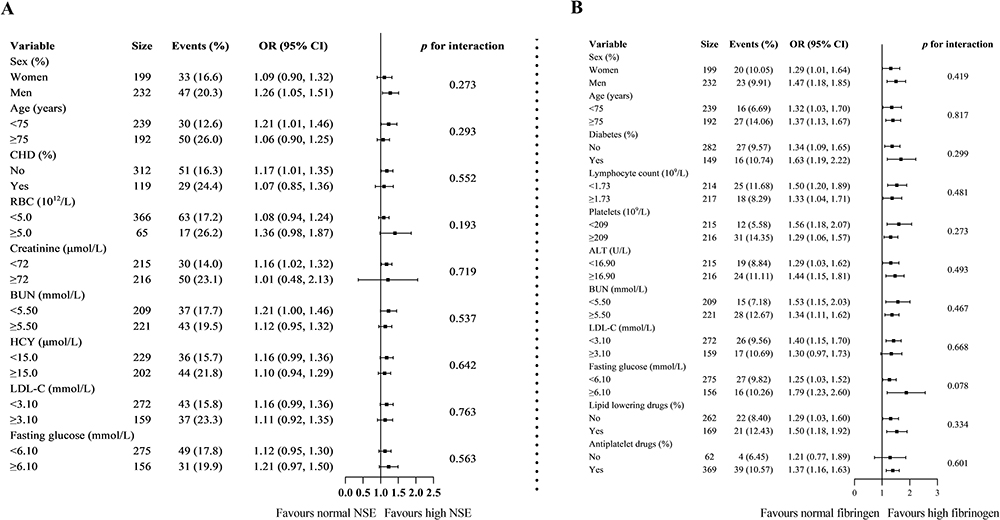 |
Figure 5 Forest plot of hierarchical analysis on relationship. (A) Hierarchical analysis on relationship of leukocyte and high NSE. Each stratification adjusted for all the factors (sex, age, CHD, RBC, creatinine, BUN, HCY, LDL-C, and fasting glucose) except the stratification factor itself. (B) Hierarchical analysis on relationship of leukocyte and high fibrinogen. Each stratification adjusted for all the factors (sex, age, diabetes, lymphocyte count, platelet, ALT, BUN, LDL-C, fasting glucose, lipid lowering drugs, and antiplatelet drugs) except the stratification factor itself. |
In multiple logistic regression analyses of the relationship between leukocyte and high fibrinogen, baseline variables that were considered relevant to leukocyte and fibrinogen by difference analysis or previous references or that showed a univariate relationship with high fibrinogen were entered into multivariate logistic regression model. As a result, sex, age, diabetes, lymphocyte count, platelet, ALT, BUN, LDL-C, fasting glucose, lipid lowering drugs, and antiplatelet drugs were regarded as confounding factors related to high fibrinogen. In multiple logistic regression analysis, the OR (95%) for the relationship between leukocyte and high fibrinogen was 1.40 (1.22–1.61, p<0.001) in all patients. When leukocytes were categorized into normal group and high group, the OR (95%) for the association between leukocyte and high fibrinogen was 8.60 (4.11–18.02, p<0.001) reference to normal leukocyte in all AIS patients. When the multivariate analysis was performed after adjusting for sex, age, diabetes, lymphocyte count, platelet, ALT, BUN, LDL-C, fasting glucose, lipid lowering drugs, and antiplatelet drugs, the OR (95%) for the relationship between leukocyte and high fibrinogen were 1.35 (1.15–1.58, p<0.001) in all patients and 7.79 (3.33–18.20, p=0.033) in high leukocyte group, respectively, and the OR (95%) showed a grade increase according to the leukocyte tertile’s by trend analysis (p<0.001) (Table 4), which showed a statistical significance. Hierarchical analysis, according to sex, age, diabetes, lymphocyte count, platelet, ALT, BUN, LDL-C, fasting glucose, lipid lowering drugs, and antiplatelet drugs, also showed that the association between leukocyte and high fibrinogen was statistically significant (Figure 5B, Supplement Table 5).
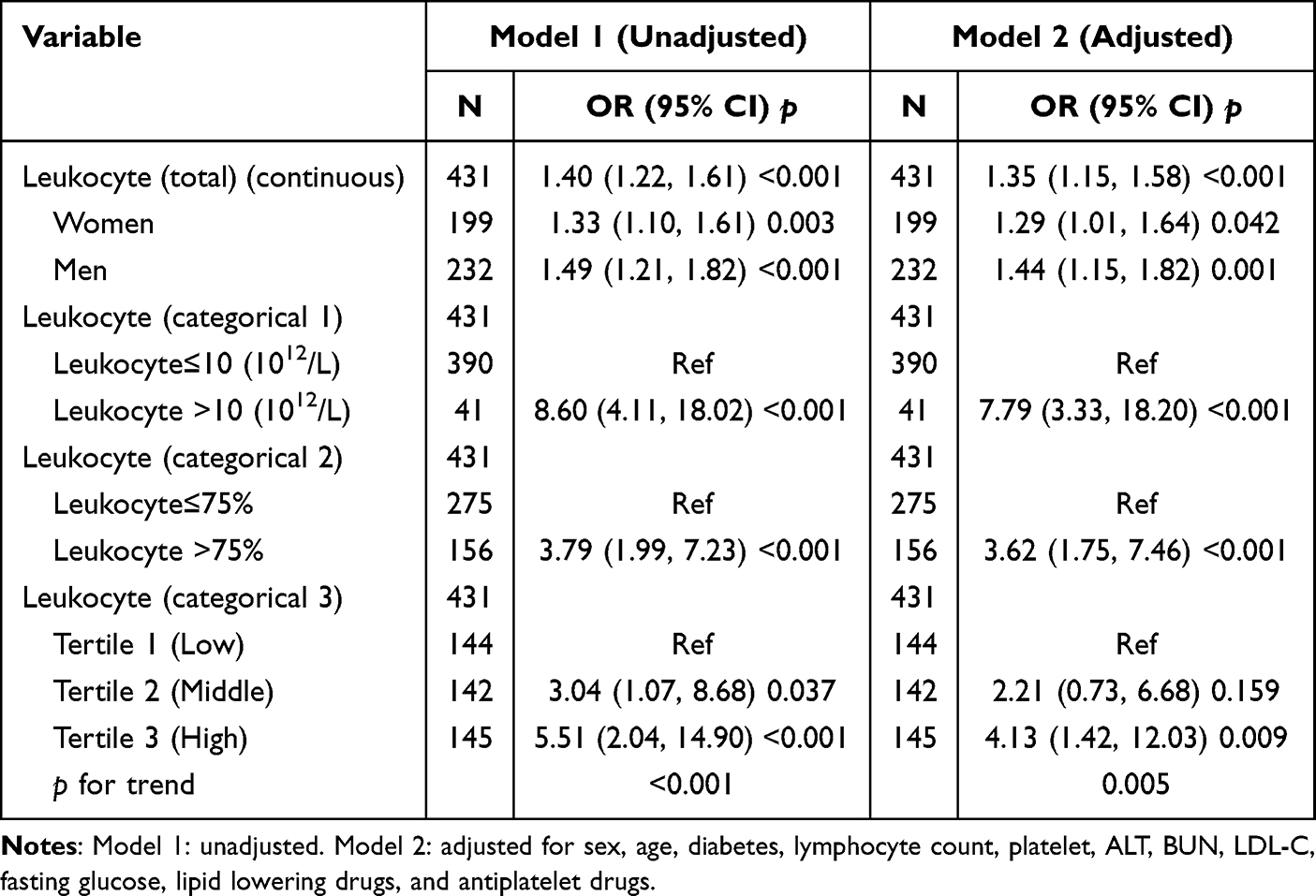 |
Table 4 Multivariate Logistic Regression for Effects of Leukocyte on High Fibrinogen |
Discussion
In the current study, clinical analysis found that elevated circulating leukocyte levels were independently associated with high NSE and high fibrinogen respectively in the AIS patients, and this positive effect was evident in all subgroups considered and after careful adjustments. Therefore, these results demonstrated that elevated circulating leukocyte was associated with high fibrinogen and neuronal damage in AIS patients.
Inflammation plays an important role in the pathophysiology of acute ischemic stroke, and inflammatory biomarkers have been demonstrated as reliable prognostic marker for outcomes events. In post-stroke inflammation, tumor necrosis factor alpha (TNF‑α), interleukin‑1 (IL-1), and interleukin‑6 (IL-6) are usually referred as primary pro-inflammatory cytokines, and are investigated as essential signaling proteins secreted by endothelial cells, immune cells, oligodendrocytes, and astrocytes in central nervous system.18–20 Clinical studies show that higher plasma levels of TNF‑α, IL-1β, and IL-6 are associated with serious inflammation and adverse outcome of ischemic stroke.21 Both circulating fibrinogen and C-reactive protein (CRP) are non-specific inflammatory mediators originated from liver. While circulating leukocytes were emerged from the bone marrow, and recruited into the brain lesions by inflammatory cytokines, including TNF‑α, IL-1, and IL-6.22 Furthermore, leukocytes subset (neutrophils, monocytes and lymphocytes) can also secrete various cytokines, such as interleukin, interferon, tumor necrosis factor, further to participate in the regulation of inflammation and immune response in ischemic stroke.
In recent years, NSE has been used as a stable and reliable biochemical indicator for neuronal damage in AIS patients.13 NSE is a kind of glycolytic enzyme, which participates in the anaerobic glycolysis process after ischemic stroke. It has been proved that the integrity of central neuron is destroyed in the hypoxic state, and NSE released into the intercellular space and cerebrospinal fluid.23 The energy metabolism disorder of glial cells after cerebral infarction will also lead to the increase of serum NSE expression.24 Because the blood brain barrier (BBB) in cerebral infarction is destroyed, thus the NSE will enter into circulating system, which will increase the expression level of NSE in the circulation in AIS patients.25 Inflammatory response in the ischemic lesion promotes neuronal apoptosis, which accelerates the release of NSE from central system to peripheral blood circulation.26,27 Inflammatory factors in the ischemic lesion originate from endogenous nerve tissues and exogenous blood circulation, the latter including circulating leukocyte and fibrinogen, and these two inflammatory factors have been observed in the ischemic lesion in previous studies.28 Infiltrating leukocytes can amplify ischemic inflammatory response by secreting a variety of proinflammatory mediators.29 In briefly, after the occurrence of ischemic stroke, peripheral leukocyte enters the ischemic focus through the damaged BBB and act as an inflammatory mediator to promote neuronal apoptosis, leading to an increased release of NSE. Our present clinical study showed that the circulating leukocyte was related to the expression of NSE. Furthermore, multiple logistic regression analysis showed that the peripheral circulating leukocyte may be an inflammatory risk factor that should be intervened for neuronal damage in AIS patients.
Previous studies focused on the role of leukocytes and fibrinogen in the thrombus formation in cardiovascular and peripheral vascular diseases.30,31 In cerebrovascular disease, some studies primary discovered the association between leukocyte and fibrinogen with clinical events respectively.32 Shi et al found that high fibrinogen levels on admission had a nearly 2-fold increased risk of thrombosis in AIS patients after intravenous thrombolysis.33 While Wijeratne et al showed an association of neutrophil-lymphocyte ratio and high fibrinogen in AIS patients undergoing mechanical thrombectomy.34 Skalny et al found that the combined effect of fibrinogen and leukocyte on worse outcome in AIS has not been well characterized.35 However, few literatures were found on the interaction between circulating leukocytes and fibrinogen in the inflammatory reaction after AIS. Our current study showed that patients with elevated leukocytes have a risk of high fibrinogen after the occurrence of AIS.
The mechanism of interaction between circulating leukocyte and high fibrinogen in AIS is still unclear, and inflammation and immunity-related response are two plausible mechanisms.36–38 The risk of thrombosis appears related to the level of neutrophilia, which are involved in the release of matrix metalloproteinase-9 as part of the breakdown of extracellular matrix in response to normal physiological processes.39,40 Recent studies have found that platelets, through interaction between P-selectin on the platelet surface and PSGL-1 on neutrophils, would trigger the formation of neutrophil extracellular traps (NETs), which will promote the occurrence of the coagulation cascade by activating the intrinsic pathway and degrading the inhibitor of the natural anticoagulant tissue factor (TF) pathway.36 Recently, elevated fibrinogen levels were reported involved in the process of stroke and other cardiovascular diseases.41,42 Luyendyk et al revealed that the fibrinogen played an important role in intensive and chronic low-grade inflammation.43 Another study showed that fibrinogen supports neutrophil activation by interacting with the human leukocyte adhesion glycoprotein αMβ2 integrin.44 An animal study also showed that fibrinogen could be synthesized and secreted during inflammatory stimulation.45 Therefore, it is important for AIS patients to identify the association between leukocyte and fibrinogen.
Despite its novelty, our study has several limitations that should to be considered. Firstly, this was a cross-sectional study, and establishing a causal link needs to be further verified in multicenter large sample prospective cohort studies. Secondly, there may be a bias in age toward AIS individuals, as the majority of included patients are over the age of 50 years (mean 73 years). Thirdly, the evidence of association between leukocyte and fibrinogen and NSE was originated from literatures and needs to be proved by related basic experiment. Despite these limitations, these data are impactful and reliability. We excluded subjects with underlying diseases that may affect the values of fibrinogen, such as malignancies and hematological system diseases. In this study, we did not use National Institute of Health stroke scale (NIHSS) score to assess the severity of central neuron injury. Because some cerebral infarction lesions could occur in non-functional areas without clinical symptoms, so there is a bias of low NIHSS score. On the contrary, NSE can directly reflect the damage of neurons in functional and non-functional regions. Therefore, NSE was used to assess the severity of central neuron injury, which ensures the scientific nature of the conclusion.
Conclusion
In summary, our results found that elevated circulating leukocytes were significantly related to the high levels of fibrinogen and NSE in AIS patients. Therefore, there may be potential intersection targets among leukocytes and fibrinogen and neuronal damage that could be intervened to reduce inflammatory reaction after ischemic stroke. Further studies are required a follow-up study and animal experimental research to define the therapeutic targets.
Human and Animal Rights Statement
This study was performed according to the principles of the Declaration of Helsinki and was approved by the ethics committee of Baoshan Branch, Shanghai Jiao Tong University School of Medicine Affiliated Renji Hospital, Shanghai, China (Ethics Approval Number 2022-KSSC-01). We obtained informed consent from all study subjects or their immediate family members (Patients with consciousness disorder or dysarthria after AIS) prior to sample collection.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author (De-Sheng Zhu) on reasonable request.
Funding
This work was supported by the Shanghai Cooperative Innovation Center for Translational Medicine (No. TM201706), the Shanghai Shenkang hospital development center clinical three-year action plan (No. SHDC2020CR2024B), and the Key projects of basic research of Shanghai Municipal Science and Technology Commission (No. 20JC1412000).
Disclosure
The authors declare that they have no competing interests.
References
1. Hollist M, Morgan L, Cabatbat R, Au K, Kirmani MF, Kirmani BF. Acute stroke management: overview and recent updates. Aging Dis. 2021;12(4):1000–1009. doi:10.14336/AD.2021.0311
2. Tu WJ, Hua Y, Yan F, et al. Prevalence of stroke in China, 2013–2019: a population-based study. Lancet Reg Health West Pac. 2022;28:100550. doi:10.1016/j.lanwpc.2022.100550
3. Baek BH, Kim HS, Yoon W, et al. Inflammatory mediator expression within retrieved clots in acute ischemic stroke. Ann Clin Transl Neurol. 2018;5(3):273–279. doi:10.1002/acn3.529
4. Shi K, Tian DC, Li ZG, Ducruet AF, Lawton MT, Shi FD. Global brain inflammation in stroke. Lancet Neurol. 2019;18(11):1058–1066. doi:10.1016/S1474-4422(19)30078-X
5. Chen J, Wang L, Xu H, Wang Y, Liang Q. The lymphatic drainage system of the CNS plays a role in lymphatic drainage, immunity, and neuroinflammation in stroke. J Leukoc Biol. 2021;110(2):283–291. doi:10.1002/JLB.5MR0321-632R
6. Huang J, Yin G, Duan L, et al. Prognostic value of blood-based inflammatory biomarkers in secondary hemophagocytic lymphohistiocytosis. J Clin Immunol. 2020;40(5):718–728. doi:10.1007/s10875-020-00801-x
7. Sun Y, Deng W, Yao G, et al. Citrullinated fibrinogen impairs immunomodulatory function of bone marrow mesenchymal stem cells by triggering toll-like receptor. Clin Immunol. 2018;193:38–45. doi:10.1016/j.clim.2018.01.008
8. Del Zoppo GJ, Levy DE, Wasiewski WW, et al. Hyperfibrinogenemia and functional outcome from acute ischemic stroke. Stroke. 2009;40(5):1687–1691. doi:10.1161/STROKEAHA.108.527804
9. Yang X, Lu T, Qu Z, Zhang Y, Liu P, Ma Y. Plasma D-dimer level is associated with clinical outcomes in patients with atrial fibrillation related acute ischemic stroke after pneumonia. BMC Neurol. 2021;21(1):137. doi:10.1186/s12883-021-02168-x
10. You S, Yin X, Liu H, et al. Hyperfibrinogenemia is significantly associated with an increased risk of in-hospital mortality in acute ischemic stroke patients. Curr Neurovasc Res. 2017;14(3):242–249. doi:10.2174/1567202614666170621103604
11. Kim JY, Park J, Chang JY, Kim SH, Lee JE. Inflammation after ischemic stroke: the role of leukocytes and glial cells. Exp Neurobiol. 2016;25(5):241–251. doi:10.5607/en.2016.25.5.241
12. Rayasam A, Hsu M, Kijak JA, et al. Immune responses in stroke: how the immune system contributes to damage and healing after stroke and how this knowledge could be translated to better cures? Immunology. 2018;154(3):363–376. doi:10.1111/imm.12918
13. Hu Y, Meng R, Zhang X, et al. Serum neuron specific enolase may be a marker to predict the severity and outcome of cerebral venous thrombosis. J Neurol. 2018;265(1):46–51. doi:10.1007/s00415-017-8659-9
14. Missler U, Wiesmann M, Friedrich C, Kaps M. S-100 protein and neuron-specific enolase concentrations in blood as indicators of infarction volume and prognosis in acute ischemic stroke. Stroke. 1997;28(10):1956–1960. doi:10.1161/01.STR.28.10.1956
15. Silva LM, Doyle AD, Greenwell-Wild T, et al. Fibrin is a critical regulator of neutrophil effector function at the oral mucosal barrier. Science. 2021;374(6575):eabl5450. doi:10.1126/science.abl5450
16. Pierot L, Jayaraman MV, Szikora I, et al. Standards of practice in acute ischemic stroke intervention: international recommendations. AJNR Am J Neuroradiol. 2018;39(11):E112–E117. doi:10.3174/ajnr.A5853
17. Hong RH, Zhu J, Li ZZ, et al. Red blood cell distribution width is associated with neuronal damage in acute ischemic stroke. Aging. 2020;12(10):9855–9867. doi:10.18632/aging.103250
18. Liberale L, Bonetti NR, Puspitasari YM, et al. TNF-alpha antagonism rescues the effect of ageing on stroke: perspectives for targeting inflamm-ageing. Eur J Clin Invest. 2021;51(11):e13600. doi:10.1111/eci.13600
19. Liberale L, Bonetti NR, Puspitasari YM, et al. Postischemic administration of IL-1alpha neutralizing antibody reduces brain damage and neurological deficit in experimental stroke. Circulation. 2020;142(2):187–189. doi:10.1161/CIRCULATIONAHA.120.046301
20. Liberale L, Ministrini S, Carbone F, Camici GG, Montecucco F. Cytokines as therapeutic targets for cardio- and cerebrovascular diseases. Basic Res Cardiol. 2021;116(1):23. doi:10.1007/s00395-021-00863-x
21. Tirandi A, Sgura C, Carbone F, Montecucco F, Liberale L. Inflammatory biomarkers of ischemic stroke. Intern Emerg Med. 2023. doi:10.1007/s11739-023-03201-2
22. Xiao Y, Jin J, Chang M, et al. Peli1 promotes microglia-mediated CNS inflammation by regulating Traf3 degradation. Nat Med. 2013;19(5):595–602. doi:10.1038/nm.3111
23. Wihersaari L, Tiainen M, Skrifvars MB, et al. Usefulness of neuron specific enolase in prognostication after cardiac arrest: impact of age and time to ROSC. Resuscitation. 2019;139:214–221. doi:10.1016/j.resuscitation.2019.04.021
24. Sawada Y, Konno A, Nagaoka J, Hirai H. Inflammation-induced reversible switch of the neuron-specific enolase promoter from Purkinje neurons to Bergmann glia. Sci Rep. 2016;6:27758. doi:10.1038/srep27758
25. Lissner Ostlund E, Levin H, Nielsen N, Frigyesi A, Lybeck A. Neuron-specific enolase and long-term neurological outcome after OHCA - A validation study. Resuscitation. 2021;168:206–213. doi:10.1016/j.resuscitation.2021.09.001
26. Rech TH, Vieira SR, Nagel F, Brauner JS, Scalco R. Serum neuron-specific enolase as early predictor of outcome after in-hospital cardiac arrest: a cohort study. Crit Care. 2006;10(5):R133. doi:10.1186/cc5046
27. Haque A, Polcyn R, Matzelle D, Banik NL. New insights into the role of neuron-specific enolase in neuro-inflammation, neurodegeneration, and neuroprotection. Brain Sci. 2018;8(2). doi:10.3390/brainsci8020033
28. Wang R, Zhu Y, Liu Z, et al. Neutrophil extracellular traps promote tPA-induced brain hemorrhage via cGAS in mice with stroke. Blood. 2021;138(1):91–103. doi:10.1182/blood.2020008913
29. Jin R, Liu L, Zhang S, Nanda A, Li G. Role of inflammation and its mediators in acute ischemic stroke. J Cardiovasc Transl Res. 2013;6(5):834–851. doi:10.1007/s12265-013-9508-6
30. Arnaoutoglou E, Kouvelos G, Papa N, et al. Prospective evaluation of postimplantation syndrome evolution on patient outcomes after endovascular aneurysm repair for abdominal aortic aneurysm. J Vasc Surg. 2016;63(5):1248–1255. doi:10.1016/j.jvs.2015.11.043
31. Whiteley W, Jackson C, Lewis S, et al. Association of circulating inflammatory markers with recurrent vascular events after stroke: a prospective cohort study. Stroke. 2011;42(1):10–16. doi:10.1161/STROKEAHA.110.588954
32. Derbisz J, Nowak K, Wnuk M, et al. Prognostic significance of stroke-associated infection and other readily available parameters in acute ischemic stroke treated by intravenous thrombolysis. J Stroke Cerebrovasc Dis. 2021;30(2):105525. doi:10.1016/j.jstrokecerebrovasdis.2020.105525
33. Shi J, Shi R, Qin W, et al. Dynamic changes in fibrinogen and prognosis of acute ischemic stroke patients treated with intravenous thrombolysis. Neurotox Res. 2020;38(3):775–784. doi:10.1007/s12640-020-00241-w
34. Wijeratne T, Sales C, Karimi L, Crewther SG. Acute ischemic stroke in COVID-19: a case-based systematic review. Front Neurol. 2020;11:1031. doi:10.3389/fneur.2020.01031
35. Skalny AV, Klimenko LL, Turna AA, et al. Serum trace elements are associated with hemostasis, lipid spectrum and inflammatory markers in men suffering from acute ischemic stroke. Metab Brain Dis. 2017;32(3):779–788. doi:10.1007/s11011-017-9967-6
36. Stark K, Massberg S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat Rev Cardiol. 2021;18(9):666–682. doi:10.1038/s41569-021-00552-1
37. Besteman SB, Callaghan A, Hennus MP, Westerlaken GHA, Meyaard L, Bont LL. Signal inhibitory receptor on leukocytes (SIRL)-1 and leukocyte- associated immunoglobulin-like receptor (LAIR)-1 regulate neutrophil function in infants. Clin Immunol. 2020;211:108324. doi:10.1016/j.clim.2019.108324
38. Jin R, Yang G, Li G. Inflammatory mechanisms in ischemic stroke: role of inflammatory cells. J Leukoc Biol. 2010;87(5):779–789. doi:10.1189/jlb.1109766
39. Mohammadhosayni M, Sadat Mohammadi F, Ezzatifar F, et al. Matrix metalloproteinases are involved in the development of neurological complications in patients with Coronavirus disease 2019. Int Immunopharmacol. 2021;100:108076. doi:10.1016/j.intimp.2021.108076
40. Serra R, Gallelli L, Grande R, et al. Hemorrhoids and matrix metalloproteinases: a multicenter study on the predictive role of biomarkers. Surgery. 2016;159(2):487–494. doi:10.1016/j.surg.2015.07.003
41. Ekblom-Bak E, Halldin M, Vikstrom M, et al. Physical activity attenuates cardiovascular risk and mortality in men and women with and without the metabolic syndrome - a 20-year follow-up of a population-based cohort of 60-year-olds. Eur J Prev Cardiol. 2021;28(12):1376–1385. doi:10.1177/2047487320916596
42. Yuan D, Jiang P, Zhu P, et al. Prognostic value of fibrinogen in patients with coronary artery disease and prediabetes or diabetes following percutaneous coronary intervention: 5-year findings from a large cohort study. Cardiovasc Diabetol. 2021;20(1):143. doi:10.1186/s12933-021-01335-1
43. Luyendyk JP, Schoenecker JG, Flick MJ. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood. 2019;133(6):511–520. doi:10.1182/blood-2018-07-818211
44. Kopec AK, Joshi N, Cline-Fedewa H, et al. Fibrin(ogen) drives repair after Acetaminophen-induced liver injury via leukocyte alphaMbeta2 integrin-dependent upregulation of Mmp12. J Hepatol. 2017;66(4):787–797. doi:10.1016/j.jhep.2016.12.004
45. Odrljin TM, Haidaris CG, Lerner NB, Simpson-Haidaris PJ. Integrin alphavbeta3-mediated endocytosis of immobilized fibrinogen by A549 lung alveolar epithelial cells. Am J Respir Cell Mol Biol. 2001;24(1):12–21. doi:10.1165/ajrcmb.24.1.3992
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.