Back to Journals » Nature and Science of Sleep » Volume 14
Circadian Type Determines Working Ability: Poorer Working Ability in Evening-Types is Mediated by Insufficient Sleep in a Large Population-Based Sample of Working-Age Adults
Authors Merikanto I ![]() , Pesonen AK, Paunio T, Partonen T
, Pesonen AK, Paunio T, Partonen T ![]()
Received 8 January 2022
Accepted for publication 23 March 2022
Published 26 April 2022 Volume 2022:14 Pages 829—841
DOI https://doi.org/10.2147/NSS.S356060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Ilona Merikanto,1– 3 Anu-Katriina Pesonen,4 Tiina Paunio,2,5 Timo Partonen2
1SleepWell Research Program, Faculty of Medicine, University of Helsinki, Helsinki, Finland; 2Department of Public Health and Welfare, Finnish Institute for Health and Welfare, Helsinki, Finland; 3Orton Orthopaedics Hospital, Helsinki, Finland; 4Department of Psychology and Logopedics and SleepWell Research Program, Faculty of Medicine, University of Helsinki, Helsinki, Finland; 5Department of Psychiatry and SleepWell Research Program, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
Correspondence: Ilona Merikanto, SleepWell Research Program, Faculty of Medicine, University of Helsinki, PL21, Helsinki, 00014, Finland, Email [email protected]
Background: Circadian phenotype has a crucial role in determining wellbeing and health prospective. Evening-types have higher risk for sleep and mental health problems, which is also reflected in work wellbeing. However, there are no population-based studies examining the association of working ability and circadian typology at different working-age-groups. Also, the role of predisposing factors, ie, sleep-related differences between circadian types, has not been studied in relation to working ability among circadian types in a population-based sample.
Methods: In this population-based sample of 13,114 working-age Finnish adults from 18 to 64 years of age, we examined the associations between circadian type, exhaustion and working ability and the roles of sleep-wake rhythm misalignment and insufficient sleep on these associations in 10-years-wide age-groups. Circadian type was assessed with the widely-used single item for self-assessed morningness/eveningness from the Horne-Östberg Morningness-Eveningness Questionnaire (MEQ).
Results: Evening-types, especially definite evening-types, were more exhausted and had poorer working ability than morning-types. Higher exhaustion among evening-types was apparent in all working ages with a peak at ages 45 to 54 years. Poorer working ability in definite evening-types as compared to definite morning-types was found only at ages 35 to 54 years. Evening-types, especially definite-evening-types, had also more social jet lag and they reported more insufficient sleep than definite morning-types. More frequent insufficient sleep associated with poorer working ability and partly mediated the association between circadian type and working ability.
Conclusion: Circadian phenotypes were found to differ in risk for exhaustion and in working ability, and this association was partly mediated by insufficient sleep. Our findings emphasize the importance to improve sleep especially among evening-types to ensure better work wellbeing.
Keywords: burnout, chronotype, circadian rhythms, epidemiology, sleep, work wellbeing
Introduction
In aging societies, lengthening work careers have become a global goal, but contradicting this effort are the high prevalence rates of burn out, work exhaustion, sickness leave and work disability in Western societies.1,2 Sufficient sleep and synchronized circadian rhythms have a key role in cognitive processing, mood regulation, and in maintaining physiological wellbeing.3–6 It is likely that higher risk for sleep, circadian rhythm and mental health problems are reflected in performance and work wellbeing and can be crucial driving causes to burn out and work exhaustion. It is well-established that evening-types suffer from more sleep problems and are more sleep-deprived on workdays than other circadian phenotypes.7–9 A recent population-based study demonstrated that insufficient sleep and misalignment of sleep-wake rhythm have increased across 10 years especially among working-age evening-type adults under 45 years of age.10
Circadian phenotype reflects the individual variation in the daily timing of physiological functions and behavior and determines the peak times for individual´s alertness state and performance.11,12 Genetic factors influence on the circadian phenotype from childhood to adulthood13–16 and although developmental changes during childhood/adolescence promote a shift towards later-timed circadian rhythms,8,15 the individual circadian phenotype is a rather stable feature during adulthood.17 Circadian rhythms react to environmental clues, such as light exposure,18,19 and can be misaligned if signals regarding environmental conditions, actualized behavior and the innate timing and period length of the circadian clock contradict with each other.20,21 This has been shown for later-timed evening-types, who suffer from sleep, circadian rhythm and mental health problems more often than other circadian types.4,7,10,22,23
Especially evening-types have a high risk for burnout already in young adulthood24 as well as for poorer working ability in a large regional sample of 46-year-old adults.25 However, there is a lack of knowledge on the specific age after which the difference in working ability can be detected between circadian types, and whether the previous findings can be generalized to the population level. It is also important to understand the underlying causes for poorer working ability in order to lengthen work careers and improve performance and wellbeing in work. Accordingly, this study aims to answer these open questions by examining, whether evening-types show an excess risk for exhaustion and poor working ability in a population-based sample of 13,114 working age adults of 18 to 64 years. We divided our sample into 10-years-wide age-groups in order to examine the age-effect on these associations and to study the potential role of circadian misalignment of sleep-wake rhythm and insufficient sleep on these associations.
Methods
Participants
The analytic sample in this study is from three nationwide population-based studies on Finnish adults, including the FINRISK 2007 Study, the FINRISK 2012 Study and the FinHealth 2017 Study. All these studies used random samples, stratified by gender and 10-year age-groups, of adults aged 25 to 74 years in 2007 and 2012 and from 18 years or older in 2017 from five large geographical areas in Finland. More details of the FINRISK 2007 and 2012 Studies are given in previous reports.10,23 A total of 13,114 participants of working age 18 to 64 years old with information on circadian type were included in this study.
Ethics Approval
The FINRISK 2007 and 2012 Studies and the FinHealth 2017 Study were approved by the Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa, Finland. They were conducted according to accepted international ethical standards in accordance with the Declaration of Helsinki and its amendments.
Consent to Participate
All the participants gave a written informed consent.
Circadian Type
Circadian type was assessed with the MEQ item 19 (MEQi19) derived from the original 19-item Horne-Östberg Morningness-Eveningness Questionnaire (MEQ).26 This item was available in all the three population-based studies. This question requests individuals to estimate their circadian type as either Definitely a “morning” person, More a “morning” than an “evening” person, More an “evening” than a “morning” person, or Definitely an “evening” person. The use of this single item from the MEQ is popular in circadian rhythm research as a feasible and reliable method.4,14
Sleep Indicators
The usual daily sleep duration was self-reported in all the datasets in hours. Insomnia symptoms were asked with a single item on whether the person had experienced insomnia during the past month. Assessment of social jet lag and midpoints of sleep were based on well-established surveys.27,28 Social jet lag was determined to indicate the average mismatch between social and biological rhythm as the difference between the average free day and weekday midpoints of sleep in hours and minutes.27 The average midpoint of sleep was calculated with the self-reported bedtimes and wake-up times, available in the FINRISK 2012 Study and the FinHealth 2017 Study, to indicate sleep schedule habits separately for weekdays and free days.29 Bedtime was asked separately for free days and working days as follows: “What time do you usually go to bed with the intention to falling asleep?”. Wake-up time was asked as follows: “What time do you usually arise without going back to bed?”. Insufficient sleep was assessed with the self-estimation of either getting enough sleep nearly always, often, or rarely/never as reported in all three datasets. We also had self-reported information on whether participants had obstructive sleep apnea diagnosed by a doctor.
Work and Well-Being
Work conditions were asked separately with the following two questions designed in the FINRISK and FinHealth Studies: 1) Physical work demand: “How demanding is your work physically?” (Mainly sitting, Walking but no lifting, Walking and lifting, Heavy manual labor); 2) Employment: “What is your present state of employment?” (Permanent full-time employment, Permanent part-time employment, Temporary employment, Independent contractor/entrepreneur, Full-time student, I am on maternity/paternity leave or on children’s home care leave, I am pensioned, On employment support: in training or employed, I am unemployed/laid off or out of work for other reasons).
Work well-being was asked separately regarding working ability and general exhaustion as follows designed in the FINRISK and FinHealth Studies: 1) Working ability: “Assume that your working ability at its best has achieved 10 points. How many points would you give to your current working ability? (0 = fully unable to work, 10 = working ability at its best); 2) General exhaustion: “Do you feel exhausted and overstressed?” (Never, Sometimes, Often).
Six questions derived from the Job Content Questionnaire (JCQ)30 assessing decision authority and psychological demand in current or previous work (if not working) were available only in the FINRISK 2007 and 2012 Studies. Questions on decision authority included: 1) I can make many independent decisions in my job; 2) I have a lot of say in how I can do my job; 3) I have very little freedom to decide how I do my job. Questions on Psychological work demand included: 1) My job requires working very hard; 2) I am expected to do an unreasonable amount of work; 3) I do not have enough time to get my work done. (Completely agree; Somewhat agree; Neither agree nor disagree; Somewhat disagree; Completely disagree).
Control Variables
Information on gender was received from the Population Information System of the national Population Register Centre. The age at participation was calculated based on the year of birth given from the Population Information System of the national Population Register Centre. The effect of gender and age were taken into account in the statistical analyses, as there are both age and gender related differences in sleep and circadian type in the Finnish adult population as reported previously in this sample.7,10
Season of Responding
Season of responding was assessed according to the photoperiods in Finland that are annually timed approximately as follows: Winter from 22nd of December until 20th of March, spring from 21st of March until 21st of June, summer from 22nd of June until 20th of September and autumn from 21st of September until 21st of December. As shown in Table 1, there were no significant differences in the season of responding between the circadian types. Most responses in the combined dataset were given during wintertime.
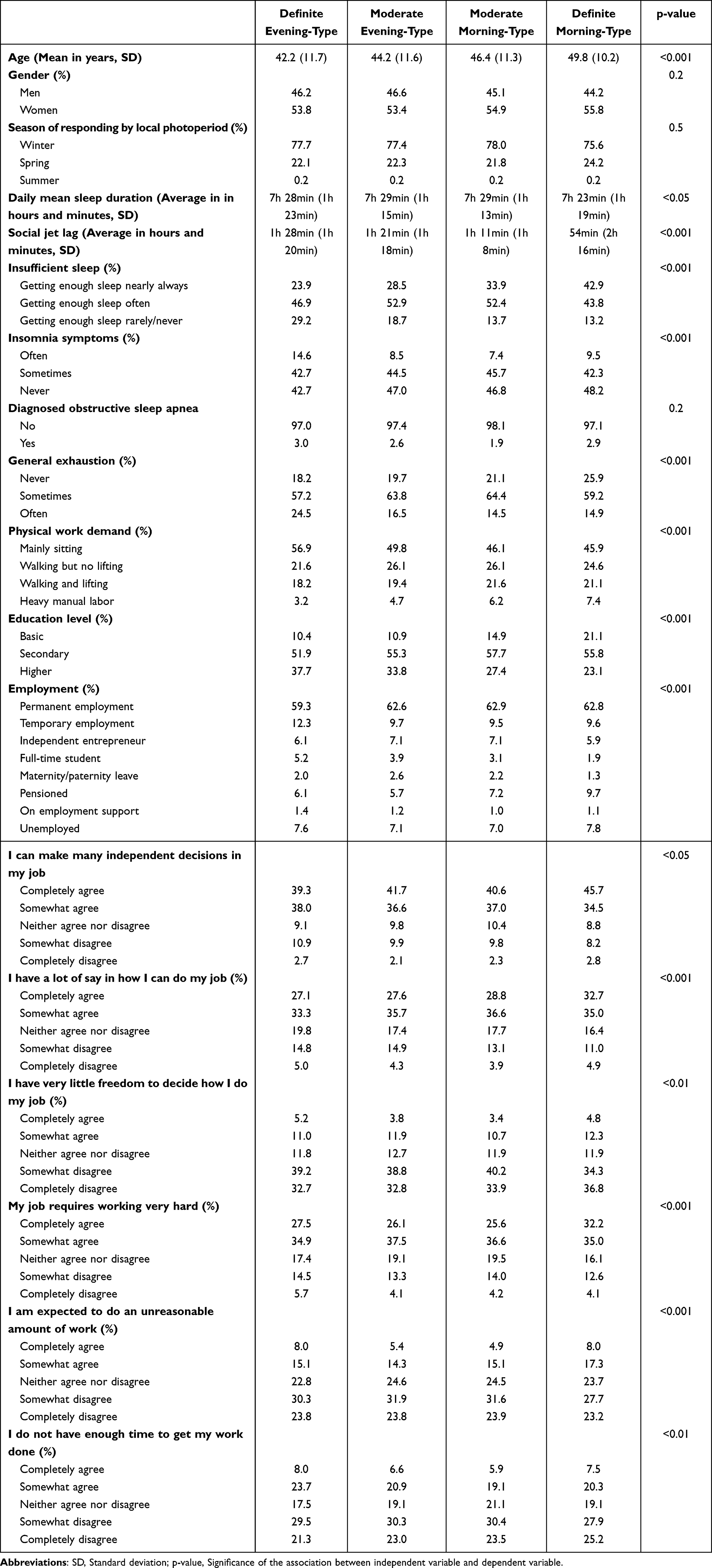 |
Table 1 Descriptive Information on Sleep and Work Situation by Circadian Type in the Population-Based Study Sample of Finnish Working Age Adults |
Statistical Analyses
For descriptive analyses of the sample, the differences between circadian types in the mean age, sleep and work situation and the distribution of gender were analyzed with one-way ANOVA (for continuous variables) and with chi-square test (for categorical variables).
Generalized linear models (GZM) and ordinal logistic GZM, respectively, were used to analyze; 1) the main question on how circadian type is associated with working ability or general exhaustion, 2) the association between circadian type and social jet lag or insufficient sleep and 3) how working ability is associated with social jet lag, insufficient sleep or work type by circadian type. All GZM were performed separately for each working-age group (18 to 34 years of age, 35 to 44 years of age, 45 to 54 years of age and 55 to 64 years of age) and adjusted with age and gender. Definite morning-types were set as the reference group, except when analyses were performed separately for each circadian type. In ordinal logistic regression models, either “Never exhausted/overstressed” or “getting enough sleep nearly always” were used as reference category along with definite morning-types when analyses were performed regarding general exhaustion or insufficient sleep, respectively. Bonferroni corrected p-values for significant results were calculated by multiplying the observed p-value by number of comparisons.
Finally, the possible influence of sleep on the association between circadian type and working ability was analyzed with mediation analysis employing the bootstrapping method with 5000 bootstrapping re-samples with the bias-corrected confidence intervals (CI). Mediation analysis, adjusted with age and gender, was performed with insufficient sleep as a mediator for the association between circadian type and working ability on those working-age groups showing a significant association between circadian type and working ability in GZM.
Results
Sociodemographic, Socioeconomic and Health Characteristics by Circadian Type
Of the analytic sample, 14.9% (N = 2119) of the participants were definite evening-types (Edef), 29.8% (N = 4312) moderate evening-types (Emod), 29.0% (N = 4201) moderate morning-types (Mmod) and 17.1% (N = 2482) definite morning-types (Mdef). As shown in Figure 1 presenting the distribution of circadian types within 10-years-wide age-groups, moderate evening-type was the most common (39.3% to 34.9%) and definite morning-type the least common circadian phenotype (8.8% to 14.9%) between ages 18 to 44 years, while moderate morning-type was most common (33.2% to 34.2%) and definite evening-type the least common circadian phenotype (13% to 11.5%) between ages 45 to 64 years.
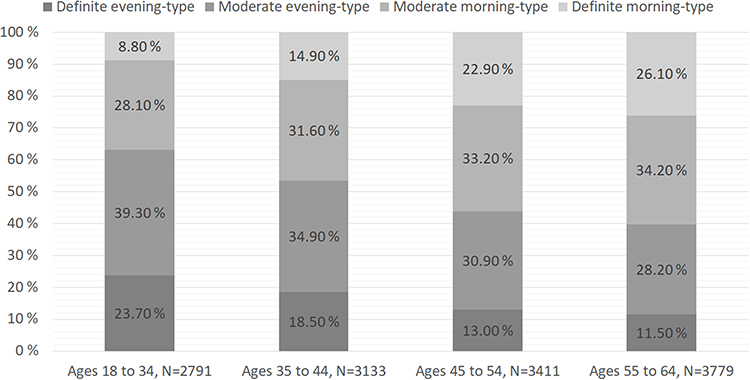 |
Figure 1 Distribution of circadian phenotypes by 10-years-wide age-groups among working-age adults. |
As shown in Table 1, no gender differences were observed in the circadian type distribution. The daily sleep duration was on average by 5 to 6 min longer in Edef and Emod as compared to Mdef. Edef were on average nearly 8 years younger, had about 34 minutes greater social jet lag, reported more often insufficient sleep (16%-units more), insomnia (about 5%-units more) and being more generally exhausted (about 10%-units more) than Mdef. Prevalence of obstructive sleep apnea diagnosed by a doctor did not differ significantly between circadian types. Physical work demand, on the other hand, was more common among Mdef than among Edef (about 4%-units more heavy manual labor), who mainly had sedentary work. Edef also had a higher education level than Mdef (about 15%-unit difference), but regarding employment they were less likely to have a permanent work contract. In terms of decision authority and psychological work demand, Mdef also felt they had more autonomy and time in organizing and completing their work although they assessed their work to be more consuming than Edef.
Working Ability and General Exhaustion by Circadian Type in Different Working-Age Groups
As shown in Table 2, Edef had significantly more general exhaustion than Mdef in each working-age group, but especially among those aged 45 to 54 years. Emod in the older age groups of 45 to 64 years were also more generally exhausted than Mdef, although to a lesser degree than Edef were. Mmod aged 55 to 64 years were somewhat more generally exhausted as compared to Mdef. Edef in the groups of 35 to 54 years reported lower working ability than Mdef, this being more emphasized in the 45-to-54-year group. No other significant differences between circadian types were found regarding working ability. As a supplementary analyses, we also analyzed the association between circadian phenotype and exhaustion as well as working ability with a model adjusted with age, gender, daily sleep duration, insomnia, education, work situation and physical work demand (Supplementary Table 1). Even after adjusting for these multiple variables, the associations between circadian phenotype, exhaustion and working ability remained and the results are essentially the same as shown in Table 2.
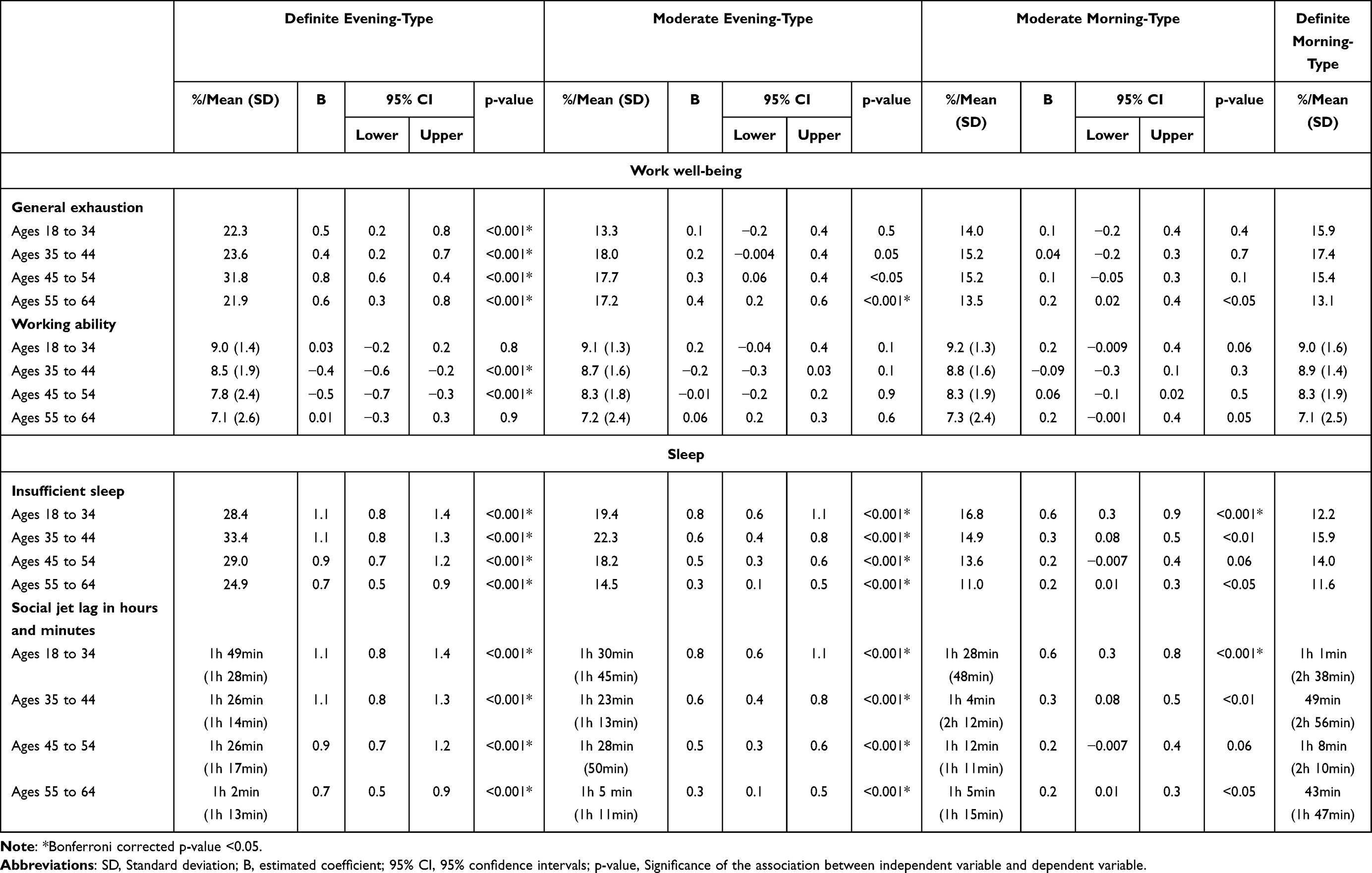 |
Table 2 Work Well-Being as General Exhaustion and Working Ability by Circadian Type and Sleep as Insufficient Sleep and Social Jet Lag by Circadian Type. Generalized Linear Models, Adjusted with Age and Gender, with Definite Morning-Types are as the Reference Group. Percentages in the Table are Given Regarding General Exhaustion on Those Reporting General Exhaustion Often and Regarding Insufficient Sleep on Those Reporting Getting Rarely or Never Enough Sleep |
Insufficient Sleep and Social Jet Lag by Circadian Type and Their Role in Working Ability in Different Working-Age Groups
As shown in Table 2, both Emod and Edef reported significantly more insufficient sleep as compared to Mdef in all working-age groups. Insufficient sleep was most common among Edef (25% to 33%), and the least common among Mdef (12% to 16%), the difference between the groups being most pronounced among those aged 35 to 44 years (17.5%-units). Similarly, both Emod and especially Edef had significantly more social jet lag than Mdef in all working-age groups, the difference varying from 18 to 48 minutes, being emphasized among those aged 18 to 34 years.
As shown in Table 3, working ability was significantly poorer for those reporting insufficient sleep as compared to those getting enough sleep among different circadian types depending on age. Insufficient sleep associated with lower working ability in Edef among the age-groups of 18 to 44 years and in Emod among the age-groups of 18 to 34 years and 45 to 54 years, while for Mdef and Mmod among all working-age groups of 35 years onwards. Poor working ability along with insufficient sleep was emphasized among older Mdef, aged 45 to 64 years. Social jet lag, on the other hand, was not as strongly associated with working ability as insufficient sleep. The most prominent association, although still weak, was on different circadian types among 55 to 64 years of age, with greater social jet lag associated with a higher working ability and especially among Edef.
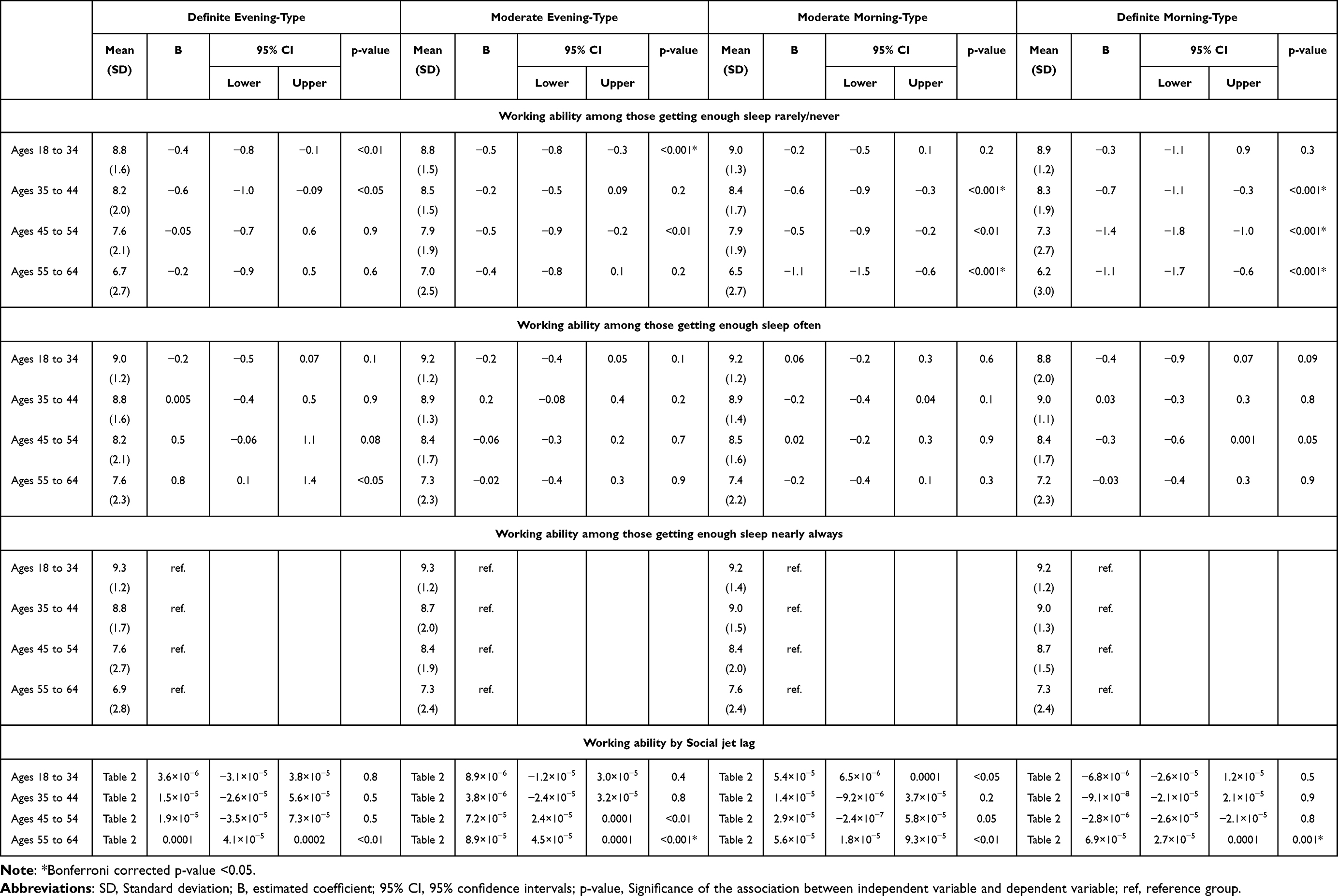 |
Table 3 Working Ability by Insufficient Sleep and Social Jet Lag for Each Circadian Type Separately. Generalized Linear Models, Adjusted with Age and Gender, with Those Getting Enough Sleep as the Reference Group |
As insufficient sleep was a stronger predictor than social jet lag for working ability based on these findings, we then used it as a mediator for the association between circadian type and working ability among age groups of 35 to 54 years. As shown in Figure 2, increased insufficient sleep partly mediated the association between eveningness and poor working ability among both these working-age groups.
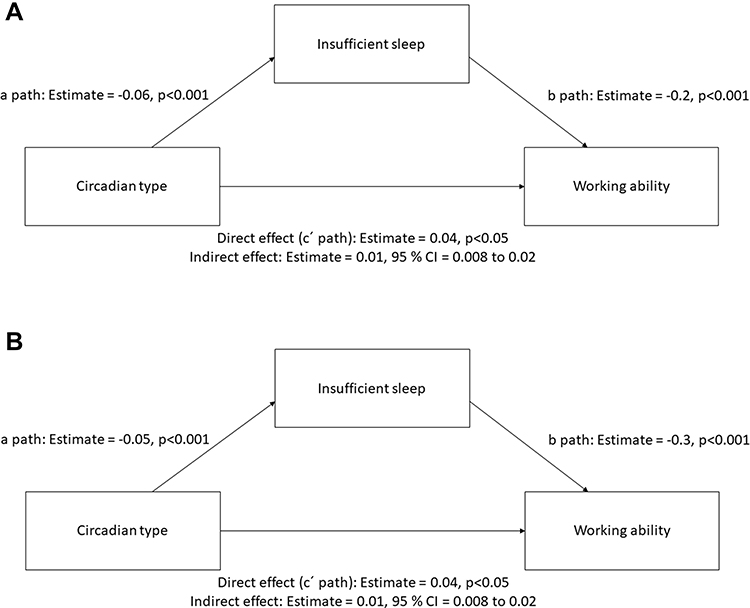 |
Figure 2 Mediation analysis with insufficient sleep as a mediator for the association between circadian type and working ability. Direct effect is the association between circadian type and working ability while controlling for insufficient sleep. Indirect effect is the measure of the mediation effect. (A) Mediation analyses for those aged 35 to 44 years, and (B) for those aged 45 to 55 years. |
Physical Work Demand by Circadian Type in Relation to Working Ability in Different Working-Age Groups
As a supplementary analyses, we also examined distribution of physical activity and whether working ability differed within the circadian type in relation to physical work demand at different ages (Supplementary Tables 2 and 3). In each age group, work consisting mainly sitting was more common among Edef as compared to other circadian types (Supplementary Table 2). As shown in Supplementary Table 3, working ability was significantly poorer for those with mainly sitting jobs as compared to those with more physical activity required at work, depending on age. Working ability was better for all circadian types with walking but no lifting required as compared to those with sitting jobs. For Edef this was apparent at ages 45 onwards, but for other circadian already since the age of 35 onwards. The difference in working ability among those with either sitting jobs or jobs requiring both walking and lifting was apparent among all circadian types only at the age of 55 to 64, but also at 35 to 44 years of age among Edef. Working ability was better among those with heavy manual labor than with sitting jobs only among Edef.
Discussion
This study examines the difference in working ability between circadian types among different working-age groups using a large population-based sample. Our findings in the Finnish working-age adult population indicated that working ability and the risk for exhaustion differ significantly between circadian types, and that they were partly mediated by the subjective experience of insufficient sleep duration. Although the focus of this study is on the effects of sleep and circadian problems on working ability, it is possible that there are also significant associations between work-related socioeconomic characters and exhaustion risk, as shown by a previous study on Swedish workers.31 They demonstrated that burnout is more common among those with higher demanding jobs or with less decision authority at the work place.31 However, the differences reported here between circadian types regarding work-related socioeconomic characters, such as morning-types having more often permanent employment, more autonomy in the workplace and higher demanding job description than evening-types, can be at least partly influenced by the difference in age between the circadian types, since evening-types were nearly 8 years younger than morning-types in this population-based sample. It was thus important that we performed our analyses on working ability and exhaustion between circadian types by 10-year-wide age-groups to minimize the age and potential socioeconomic effects on our results.
Our findings show that evening-types, especially definite evening-types, are significantly more exhausted than definite morning-types in all working ages, and the peak in exhaustion levels was seen among definite evening-types at the age range from 45 to 54 years. Higher levels of general exhaustion among evening-types as compared to morning-types was an expected finding, as eveningness associates with a higher level of sleep and mood problems and daytime tiredness than morningness,4,7,10,22,23,32 while morningness on the other hand has been associated with a lower level of burnout.24,33
Regarding differences in working ability between circadian types, our finding showed as a novel result a clear age-related effect. Definite evening-types had a significantly poorer working ability than definite morning-types at the age of 35 to 54 years, the difference between the circadian types being emphasized at the age group with the highest exhaustion levels among evening-types, ie, those aged 45 to 54 years. The significant differences in working ability were seen between the extreme circadian types. Our finding on poorer working ability among evening-types is in line with a regional sample study in Finland, where the participants were aged 46 years at the time of assessment.25 Besides this study, we are aware of only one other study examining the association between circadian typology and working ability.34 This study did not show any direct association between free day sleep-wake rhythm and working ability among a regional sample of chemical company workers in Germany, with a mean age of 42 years, but indicated that a higher social jet lag resulted in a poorer working ability among the shift workers.34 Although evening-types and especially definite evening-types had significantly more social jet lag than definite morning-types at all working ages in our sample, emphasized at the age of 18 to 34 years, social jet lag was only associated with working ability among the oldest working-age group of 55 to 64 years. However, this association was very weak, so no definite conclusions regarding social jet lag and working ability should be made based on these results. All in all, our results highlight the role of insufficient sleep on working ability.
Self-reported experience of insufficient sleep was more common among evening-types, especially among definite evening-types, than among definite morning-types at all working ages in our sample, but it was especially emphasized among the evening-types aged 35 to 44 years. A more frequent experience of insufficient sleep directly associated with poorer working ability in both evening- and morning-types. The association between insufficient sleep and poorer working ability was seen among evening-types in the age-groups younger than 55 years, and insufficient sleep partly mediated the association between working ability and circadian type at the ages when working ability significantly differed between circadian types. Previous studies have also shown a significant mediating role of insufficient sleep on the association between circadian type and health status, such as higher risks of depression and anxiety among evening-types as compared to morning-types.4 Mediating role of insufficient sleep on working ability among circadian types is not surprising, since sleep has a fundamental role in cognitive and physiological wellbeing.3,5,6 Poor sleep and impaired mental health have also a reciprocal association, meaning that poor sleep can lead to mental health issues and vice versa.35–37
Based on our findings, the daily sleep duration differed significantly between the circadian types, with evening-types having longer sleep only by few minutes. However, the difference between the amount of social jet lag and the reported insufficient sleep levels were far higher among circadian types, possibly suggesting that the sleep need is greater among evening-types than among morning-types. This could potentially be due to differences in circadian period lengths between the circadian types, as found earlier.12 Evening-types may report more insufficient sleep also due to a higher prevalence of insomnia or other sleep problems influencing sleep quality.7 A subjective experience of insufficient sleep can thus be a better indicator of whether circadian types sleep enough than the habitual sleep duration, as different circadian types might have different needs and perceptions regarding sufficient sleep duration. Higher levels of insufficient sleep and social jet lag among evening-types as compared to other circadian types indicate that misalignment of sleep-wake behavior and innate biological rhythms might be more common among evening-types than among morning-types. It is possible that poorer working ability among evening-types arise from work and leisure time schedules that are not optimal for evening-types in terms of biological peak times in wakefulness, alertness, and performance.
To summarize, although evening-types, and especially definite evening-types, were more exhausted than definite morning-types at all working-age-groups, poorer working ability among evening-types was apparent at the ages of 35 to 54 years. It is possible that evening-types with poor working-ability leave work life before reaching 55 years and therefore no significant differences in the working ability among different circadian types were seen in our study at the ages of 55 to 64 years. Insufficient sleep was most common among definite evening-types at the age of 18 to 44 years, and it only partly mediated the association between working ability and circadian type. Greater social jet lag did not explain poorer working ability among evening-types as compared to definite morning-types in this study. Therefore, it seems that additional factors influence the difference in working ability between circadian types beyond insufficient sleep, or that there is a higher resilience at younger age towards the negative impacts of insufficient sleep than there is after the age of 34 years among working-age adults. For instance, sedentary work consisting of mainly sitting was more common among definite evening-types and was also reflected negatively in their working ability at the age of 45 onwards. Further, it is to be noted, that the ages 35 to 44 are also peak child-caring years which can put pressure on working ability. Although whether there are any differences between circadian types in stress caused by child-caring that are reflected in working ability remains to be studied. To conclude, our study raises an important issue on differences between circadian types in age-related working ability to be considered regarding future improvement in work wellbeing and extension of work careers.
The strength of our study is the large random sample that is stratified by gender and age and recruited from different parts of Finland to represent the general adult population. As a limitation, we have information on the participant working ability status only in cross-section and therefore cannot estimate the development of work ability longitudinally. It would have been interesting to also examine the potential differences in the age of leaving work life between circadian types, but unfortunately, we did not have this information available. We also lack more specific information on the timing of work schedules that would have allowed us to estimate the potential misalignment of these schedules in relation to circadian type to examine its role in working ability. The questions assessing midpoint of sleep are not the most optimal in our dataset as they do not specify the actual habitual wake-up time from getting up from the bed or the wake-up time without the use of alarm clock for free days. Also to have a more accurate estimation of the sleep midpoint, a more detailed question on sleep latency would have been helpful to assess the falling asleep time rather than going to bed time. It could also be argued that using a single item to assess circadian type has limitations, but this single item is, on the other hand, highly used in epidemiological research targeting large samples. A single morningness/eveningness item also significantly correlates with both the timing of sleep-wake behavior4,14 and the polygenetic score for morningness/eveningness as expected.14 Furthermore, self-assessment of morningness/eveningness is not affected by age as much as behavioral midpoint of sleep on free days.14
Funding
This study was funded by The Academy of Finland (project 322312) and EVO/TYH2019315. Open access funded by Helsinki University Library. The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
Disclosure
Timo Partonen reports personal fees from Speakersforum Finland outside the submitted work; in addition, Timo Partonen has a patent, EPO Patent No. EP 3503794 pending to proprietor: Night Train Oy, Oulu, Finland. There are no competing financial interests. The authors report no conflicts of interest related to this work.
References
1. Van Rijn RM, Robroek SJ, Brouwer S, Burdorf A. Influence of poor health on exit from paid employment: a systematic review. Occup Environ Med. 2014;71(4):295–301. doi:10.1136/oemed-2013-101591
2. Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–1602.
3. Bishir M, Bhat A, Essa MM, et al. Sleep deprivation and neurological disorders. Bio Med Res Int. 2020;2020:1–19. doi:10.1155/2020/5764017
4. Merikanto I, Partonen T.Eveningness increases risks for depressive and anxiety symptoms and hospital treatments mediated by insufficient sleep in a population‐based study of 18,039 adults. Depress Anxiety.2021;38:1066–1077. doi:10.1002/da.23189
5. Watling J, Pawlik B, Scott K, Booth S, Short MA. Sleep loss and affective functioning: more than just mood. Behav Sleep Med. 2017;15(5):394–409. doi:10.1080/15402002.2016.1141770
6. Wright KP, Hull JT, Hughes RJ, Ronda JM, Czeisler CA. Sleep and wakefulness out of phase with internal biological time impairs learning in humans. J Cognit Neurosci. 2006;18(4):508–521. doi:10.1162/jocn.2006.18.4.508
7. Merikanto I, Kronholm E, Peltonen M, Laatikainen T, Lahti T, Partonen T. Relation of chronotype to sleep complaints in the general Finnish population. Chronobiol Int. 2012;29(3):311–317. doi:10.3109/07420528.2012.655870
8. Roenneberg T, Kuehnle T, Juda M, et al. Epidemiology of the human circadian clock. Sleep Med Rev. 2007;11(6):429–438. doi:10.1016/j.smrv.2007.07.005
9. Taillard J, Philip P, Bioulac B. Morningness/eveningness and the need for sleep. J Sleep Res. 1999;8(4):291–295. doi:10.1046/j.1365-2869.1999.00176.x
10. Merikanto I, Partonen T. Increase in eveningness and insufficient sleep among adults in population-based cross-sections from 2007 to 2017. Sleep Med. 2020;75:368–379. doi:10.1016/j.sleep.2020.07.046
11. Duffy J, Dijk D, Hall E, Czeisler C. Relationship of endogenous circadian melatonin and temperature rhythms to self-reported preference for morning or evening activity in young and older people. J investig med. 1999;47(3):141.
12. Duffy JF, Rimmer DW, Czeisler CA. Association of intrinsic circadian period with morningness–eveningness, usual wake time, and circadian phase. Behav Neurosci. 2001;115(4):895–899. doi:10.1037/0735-7044.115.4.895
13. Jones SE, Lane JM, Wood AR, et al. Genome-wide association analyses of chronotype in 697,828 individuals provides insights into circadian rhythms. Nat Commun. 2019;10(1):343. doi:10.1038/s41467-018-08259-7
14. Merikanto I, Kantojärvi K, Partonen T, Pesonen AK, Paunio T. Genetic variants for morningness in relation to habitual sleep-wake behavior and diurnal preference in a population-based sample of 17,243 adults. Sleep Med. 2021;80:322–332. doi:10.1016/j.sleep.2021.01.054
15. Merikanto I, Lahti J, Kuula L, et al. Circadian preference and sleep timing from childhood to adolescence in relation to genetic variants from a genome-wide association study. Sleep Med. 2018;50:36–41. doi:10.1016/j.sleep.2018.04.015
16. Morales-Muñoz I, Kantojärvi K, Uhre VM, et al. The effects of genetic background for diurnal preference on sleep development in early childhood. NSS. 2021;13:219–228. doi:10.2147/NSS.S287163
17. Broms U, Pitkäniemi J, Bäckmand H, et al. Long-term consistency of diurnal-type preferences among men. Chronobiol Int. 2014;31(2):182–188. doi:10.3109/07420528.2013.836534
18. Czeisler CA, Gooley JJ. Sleep and circadian rhythms in humans. Cold Spring Harb Symp Quant Biol. 2007;72(1):579–597. doi:10.1101/sqb.2007.72.064
19. Reppert SM, Weaver DR. Coordination of circadian timing in mammals. Nature. 2002;418(6901):935–941. doi:10.1038/nature00965
20. Baron KG, Reid KJ. Circadian misalignment and health. Int Rev Psychiatry. 2014;26(2):139–154. doi:10.3109/09540261.2014.911149
21. Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: misalignment of biological and social time. Chronobiol Int. 2006;23(1–2):497–509. doi:10.1080/07420520500545979
22. Malhi G, Kuiper S. Chronobiology of mood disorders. Acta Psychiatr Scand. 2013;128:2–15. doi:10.1111/acps.12173
23. Merikanto I, Kronholm E, Peltonen M, Laatikainen T, Vartiainen E, Partonen T. Circadian preference links to depression in general adult population. J Affective Disord. 2015;188:143–148. doi:10.1016/j.jad.2015.08.061
24. Merikanto I, Suvisaari J, Lahti T, Partonen T. Eveningness relates to burnout and seasonal sleep and mood problems among young adults. Nordic J Psychiatry. 2016;70(1):72–80. doi:10.3109/08039488.2015.1053519
25. Räihä T, Nerg I, Jurvelin H, Conlin A, Korhonen M, Ala-Mursula L. Evening chronotype is associated with poor work ability and disability pensions at midlife: a Northern Finland Birth Cohort 1966 Study. Occup Environ Med. 2021;78(8):567–575. doi:10.1136/oemed-2020-107193
26. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1975;4(2):97–110.
27. Roenneberg P, Zerbini W. Chronotype and social jetlag: a (self-) critical review. Biology. 2019;8(3):54. doi:10.3390/biology8030054
28. Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: daily temporal patterns of human chronotypes. J Biol Rhythms. 2003;18(1):80–90. doi:10.1177/0748730402239679
29. Ghotbi N, Pilz LK, Winnebeck EC, et al. The µMCTQ: an ultra-short version of the Munich ChronoType questionnaire. J Biol Rhythms. 2020;35(1):98–110. doi:10.1177/0748730419886986
30. Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322. doi:10.1037/1076-8998.3.4.322
31. Magnusson Hanson LL, Theorell T, Oxenstierna G, Hyde M, Westerlund H. Demand, control and social climate as predictors of emotional exhaustion symptoms in working Swedish men and women. Scand J Public Health. 2008;36(7):737–743. doi:10.1177/1403494808090164
32. Bakotic M, Radosevic-Vidacek B, Koscec Bjelajac A. Morningness-eveningness and daytime functioning in university students: the mediating role of sleep characteristics. J Sleep Res. 2017;26(2):210–218. doi:10.1111/jsr.12467
33. Randler C, Luffer M, Müller M. Morningness in teachers is related to a higher sense of coherence and lower burnout. Soc Indic Res. 2015;122(2):595–606. doi:10.1007/s11205-014-0699-2
34. Yong M, Fischer D, Germann C, Lang S, Vetter C, Oberlinner C. Are chronotype, social jetlag and sleep duration associated with health measured by Work Ability Index? Chronobiol Int. 2016;33(6):721–729. doi:10.3109/07420528.2016.1167728
35. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36(7):1059–1068. doi:10.5665/sleep.2810
36. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affective Disord. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
37. Tsuno N, Besset A, Ritchie K.Sleep and depression. J Clin Psychiatry.2005;66:1254–1269. doi:10.4088/JCP.v66n1008
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.