Back to Journals » Nature and Science of Sleep » Volume 17

Circadian Modulation of Sleep-Wake Behavior in Patients with Narcolepsy Type 1 and Idiopathic Hypersomnia
Authors Ryser F ![]() , Windirsch AS
, Windirsch AS ![]() , Baumann CR, Lambercy O
, Baumann CR, Lambercy O ![]() , Gassert R
, Gassert R ![]() , Werth E
, Werth E ![]()
Received 6 April 2025
Accepted for publication 10 June 2025
Published 1 November 2025 Volume 2025:17 Pages 2833—2851
DOI https://doi.org/10.2147/NSS.S520647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Franziska Ryser,1,* Ann-Sophie Windirsch,2,3,* Christian R Baumann,3,4 Olivier Lambercy,1 Roger Gassert,1 Esther Werth3,4
1Rehabilitation Engineering Laboratory, Department of Health Sciences and Technology, ETH Zurich, Zurich, Switzerland; 2Faculty of Medicine, University of Zurich, Zurich, Switzerland; 3Department of Neurology, University Hospital Zurich, Zurich, Switzerland; 4Sleep and Health Zurich (SHZ), University of Zurich, Zurich, Switzerland
*These authors contributed equally to this work
Correspondence: Franziska Ryser, Rehabilitation Engineering Laboratory, ETH Zurich, Gloriastrasse 37/ 39, Zürich, 8092, Switzerland, Email [email protected]
Study Objectives: Approximately 4.7 million subjects worldwide suffer from narcolepsy (type 1 and 2) and idiopathic hypersomnia and are impaired in their sleep and wakefulness behavior. However, the role of the circadian rhythm in their sleep-wake behavior remains largely unknown. With this study, we investigated the influence of the internal clock on vigilance and sleep in central disorders of hypersomnolence.
Methods: We implemented a nap protocol with 10 cycles of 80 minutes sleep and 160 minutes wake time and compared various sleep and wake parameters (vigilance, subjective sleepiness, sleep efficiency, stages of sleep, slow wave activity) of patients with idiopathic hypersomnia (N=12, ∅ 25.8 ± 4.1 years, 10 females) and narcolepsy type 1 (N=12, ∅ 25.0 ± 4.4 years, 8 females) with a healthy control group (N=12, ∅ 26.8 ± 4.7 years, 6 females) using a linear mixed-model analysis.
Results: Our protocol successfully disentangled the circadian rhythm from homeostatic sleep pressure and revealed an intact circadian melatonin pattern as assessed by dim light melatonin onset and offset in both patient groups. Patients with narcolepsy showed high sleep efficiencies of ∅ 94.3 ± 5.3% over all naps (group effect p < 0.001) and responded positively to the short sleep episodes with an increase in vigilance in the late afternoon (PVT speed @wake seven 2.5 ± 1.0 vs @wake ten 3.9 ± 0.6, p < 0.001). Patients with idiopathic hypersomnia showed an increased subjective sleepiness (group effect p < 0.001), yet practically no statistically significant differences in sleep parameters compared to healthy controls. Surprisingly, we observed a high number of SOREMPs in the healthy control group under low sleep pressure - a finding not previously reported in literature.
Conclusion: These findings argue against circadian disruption as a primary mechanism in idiopathic hypersomnia and point toward other underlying causes, such as altered sleep homeostasis or neurochemical dysregulation.
Plain Language Summary: This study is the first to test a nap schedule in people with narcolepsy type 1 and idiopathic hypersomnia that filters out the influence of the internal clock. Both conditions lack the brain’s ability to regulate sleep and wakefulness effectively. Surprisingly, we found that both groups had a normal daily rhythm, which contradicts some earlier studies. This suggests that idiopathic hypersomnia may not be caused by a problem with the internal clock. We examined various sleep-related measures and how they change over the day. Our findings help us better understand these conditions and show how well-timed naps can support treatment. For patients, the results offer practical advice on how to use their rhythm to stay more alert during the day.
Keywords: central disorders of hypersomnolence, circadian rhythm, narcolepsy, idiopathic hypersomnia, nap protocol
Graphical Abstract:

Introduction
Central disorders of hypersomnolence (CDH) denotes different neurological disorders (narcolepsy type 1, narcolepsy type 2, idiopathic hypersomnia, insufficient sleep syndrome and Kleine-Levin syndrome) and affect approximately 705 million people worldwide,1–6 whereas the majority of cases are accounted for by the insufficient sleep syndrome.4,5 In our study, we focused on the conditions of narcolepsy and idiopathic hypersomnia, which together affect approximately 4.7 million people worldwide.2,3 CDH are characterized by excessive daytime sleepiness (EDS), manifesting in episodes of falling asleep with or without prodromal symptoms, sleep attacks, the need of recurrent naps during the day, a prolonged yet unrefreshing main sleep episode, persistent difficulty and confusion after waking up, sleep inertia, or, in a more severe state, sleep drunkenness. EDS severely affect the quality of life of those affected, leading to a substantial medical and economic burden.7–15
From chronobiologic research with healthy subjects, we know that the propensity effect and sleep composition are affected by the circadian rhythm and thus depend on the time of day. The sleep regulation model explains this observation by two interlinked processes, sleep homeostasis (process S) and the circadian rhythm (process C).16–19 A non-linear interaction of the two processes was proven using the forced desynchrony paradigm.17,20,21 It has been shown that processes S and C contribute approximately equally to most sleep-wake variables, with the exception of slow wave activity (SWA). REM sleep has been shown to be regulated by the circadian system and a sleep-dependent disinhibition. By analyzing sleep, vigilance and circadian marker simultaneously, it was shown that in healthy individuals, the phase relation between the circadian pacemaker and the sleep-wake cycle is uniquely timed to maintain stable low sleepiness and high-performance levels during a typical 16-hour wake episode and to allow restorative sleep during the night. This results in a 2- to 3-hour phase before the onset of melatonin secretion in the evening, during which the circadian system maximizes wakefulness and performance. This period, in which napping is barely possible, is known as the “forbidden zone of sleep” (or wake maintenance zone).17,22–24 To disentangle the circadian rhythm from sleep homeostasis in an acceptable timeframe, Cajochen et al tested a nap protocol with a sleep-wake cycle of 75/150 minutes in elderly and subjects with depression.25–27 To date, no study has employed a nap protocol in patients with CDH, and the influence of the circadian system remains largely unknown.7,28
A deficiency or lack of the neurotransmitter orexin (= hypocretin) leads to narcolepsy type 1, which is characterized by excessive sleepiness, disrupted night sleep and a disordered regulation of rapid eye-movement (REM) sleep. REM sleep–like states in patients with narcolepsy type 1 can occur at any time of day, leading to a sudden loss of muscle tone and/or falling asleep, mostly triggered by strong emotions, known as cataplexy.7,29–33 In these patients, melatonin as a marker of process C was investigated, suggesting that the circadian drive remains intact.34–36 However, if, and to what extent, the disease-specific pathophysiology, such as a reduced level of orexin affecting the flip-flop-like stabilization of sleep and wake states,37,38 interact or override the circadian influence on the propensity and benefit of daytime naps, has not been investigated.
The pathophysiology of idiopathic hypersomnia, on the other hand, remains largely unknown.39 Although orexin levels have not been found to be altered,7 recent genetic data reported by Zou et al40 may offer novel insights into impaired orexin signaling as a contributing factor to the pathophysiology of idiopathic hypersomnia. The presence of endogenous gamma-aminobutyric acid (GABA)-like substances that modulates GABA-mediated inhibitory effects on arousal has been detected in the cerebral spinal fluid (CSF) of individuals with idiopathic hypersomnia.41,42 However, these findings could not be replicated by other groups.43 An altered circadian mechanism, such as a prolonged circadian period or a prolonged biological night, is under debate as a cause of the elongated night sleep and the perceived sleep inertia in the morning.44–48 If, and to what extent, the circadian rhythm influences the pronounced excessive daytime sleepiness in idiopathic hypersomnia, and if scheduled naps can provide temporal mitigation of the symptoms, has not yet been investigated.7,28
In this study, we designed and conducted a nap protocol to assess the circadian rhythm and its influence on sleep and wake parameters in patients with narcolepsy type 1 and idiopathic hypersomnia. Over a total of 40 h, multiple naps were carried out under a modified constant routine protocol, with sleep and wakefulness occurring at different circadian times. Sleep quality and the effect of naps were observed using sleep EEG, vigilance tests, continuous assessments of subjective sleepiness and measurements of melatonin secretion during wakefulness.
We hypothesize that a nap protocol would be able to decouple the circadian rhythm from the homeostatic sleep pressure in CDH patients. We expect that patients with narcolepsy type 1 have difficulties falling asleep during times of increased circadian wake drive. We further hypothesize an increased performance in vigilance tasks and a reduction in the perceived sleepiness due to the benefit of regular napping throughout the course of the protocol. We further expect patients with idiopathic hypersomnia to have an altered circadian rhythm, and therefore being less prone to the influence of the circadian wake drive in the late afternoon and early evening hours.
Insights into the circadian modulation in CDH patients and its impact on sleep characteristics and performance could not only contribute to a better understanding of the underlying mechanisms of these disorders but might also lead to well-founded therapy recommendations regarding daytime naps to counteract EDS and thus improve therapy approaches.
Methods
To unmask the influence of the circadian rhythm on sleep-wake behavior, we introduced and tested an adapted constant-routine protocol in CDH that disentangles the sleep-dependent homeostatic sleep pressure from the circadian drive. Therefore, an 80/160 minutes sleep/wake rhythm was applied, where ten regular sleep opportunities (“naps”) were provided throughout the protocol. The homeostatic sleep pressure built up in between two naps was then reduced instantaneously. Thereby, sleep pressure was kept at a constant level (for more explanations see Ryser F).49 Full ethics approval was received from the Swiss cantonal ethics committee (ClinicalTrials.gov Identifier: NCT03356938), and in compliance with the Declaration of Helsinki, all participants gave written informed consent to partake in the study.
Participants
Two different patient populations, narcolepsy type 1 (NT1) and idiopathic hypersomnia with long-sleep phenotype (IH), were compared to healthy control subjects (HC). Both patient groups were diagnosed at the University Hospital of Zurich or another, similarly qualified clinic according to the guidelines of the International Classification of Sleep Disorders, 3rd ed, text revision (ICSD-3-TR).
Clinically significant concomitant disease states or any other sleep disorders or disorders of the nervous system than IH or NT1 were excluded, as well as any medication intake affecting sleep or sleepiness, an excessive daily intake of caffeine or nicotine, regular shift work or a jetlag experienced within a month before the study intervention. Seven out of 12 in idiopathic hypersomnia and 10 out of 12 in narcolepsy patients have been medicated in everyday life prior to the study. During the protocol, their medication was withdrawn for at least five half-lives to minimize the effect on sleep parameters, as more than 95% of the drug is eliminated after this period, rendering any residual pharmacological effect negligible.
For optimal comparability, all subject groups contained individuals in the age range of 18–35 years without present concomitant (sleep/neurological) disorders. In order to compare circadian rhythms, only participants without extreme morning or evening chronotypes were included, as verified through patient documentation, telephone interviews, and questionnaires such as the Morningness-Eveningness Questionnaire (MEQ).50
After the initial recruiting process with a detailed phone interview and sleep questionnaires, all healthy control subjects underwent a screening night in the sleep laboratory, which included polysomnography, actigraphy and psychomotor vigilance task (PVT) to verify healthy sleep patterns and to rule out the first night effect. From a total of 52 subjects, 9 dropped out and 7 have been excluded: five healthy subjects due to extreme chronotype (1), elevated hypopnea score (1), low sleep efficiency (1), increased subjective sleepiness (2); one patient with narcolepsy due to an unclear diagnosis; one patient with idiopathic hypersomnia due to intake of antidepressant medication.
After the recruiting process, 36 subjects started the protocol (N=12 each for NT1, IH and HC), with one drop-out after nap seven in the NT1 group, whose data recorded up to that point were included in the analysis.
Nap Protocol
The nap protocol consisted of ten repetitive sleep-wake cycles (see Figure 1). In Phase I, participants maintained regular bedtimes at home for 7 consecutive days. Healthy controls were instructed to sleep 8 ± 1 hours without daytime naps to generate a sleep saturated state. In the patient groups, longer sleep episodes and daytime naps were allowed if also performed in regular life. Phase II–IV were conducted in the sleep laboratory facilities of the University Hospital of Zurich. The first night in the laboratory (phase II) served as a baseline night of 7 hours. Then, the nap protocol followed (phase III), including 10 cycles of 80 minutes sleep and 160 minutes wake. We defined naps one and five-seven as nighttime and naps two-four and eight-ten as daytime. The protocol ended with a recovery night of 7 hours (phase IV) (an example of a study protocol is attached to the supplemental material, see Figure S1).
 |
Figure 1 The nap protocol was structured into four phases: Phase I sets the subject into sleep saturated condition by following an eight-hour sleep protocol adjusted to their regular bedtimes, controlled via sleep diary and actigraphy. Phase II is a baseline night in the clinic, followed by the nap protocol with a short wake episode of 50 minutes and ten repetitive sleep/wake cycles of 80/160 minutes each. Phase IV is a recovery night lasting seven hours in the clinic. |
We designed a constant routine protocol to reduce the influence of exogenous factors. The room climate was controlled to 18°C according to the standards for clinical sleep laboratories. Ambient light was dimmed in all study areas to maximally 10 lux during wake episodes and turned off during naps. To reduce the influence of activity, the subjects stayed in sedentary position in the bed during all wake episodes. They only got up to visit the bathroom facility. The subjects were allowed to use electronic devices such as a smartphone, laptop, or television, if the brightness of the devices was reduced to one-third of the maximum brightness, and the subjects wore special glasses to filter out the blue light. Caloric requirements throughout the protocol (during phases II, III, and IV) were approximately adjusted to the subjects’ body weight. Food was served at room temperature, and no hot meals or cold beverages were served. For female participants, the protocol was tailored to the follicular phase of their menstrual cycle to reduce its effects. An overview of the measurements taken during each wake phase of the nap protocol is present in Figure 2.
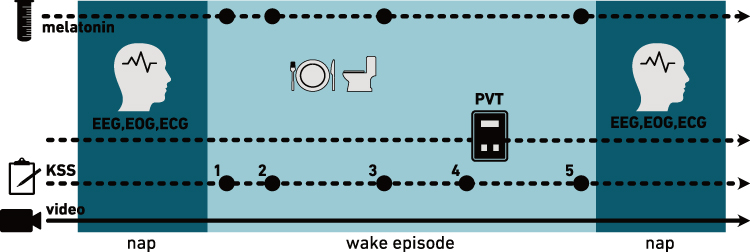 |
Figure 2 Overview of measurements taken during the nap protocol. Wake episodes are indicated in light blue, naps in dark blue. During each wake episode, we took four saliva samples to assess the melatonin level, performed a psychomotor vigilance task (PVT) and queried the Karolinska Sleepiness Scale (KSS) five times. Furthermore, we continuously recorded video and electrophysiological signals (EEG, EOG, ECG). |
Electrophysiology
In phases II–IV subjects underwent continuous electrophysiological measurements which included an electroencephalogram (EEG, 200 Hz) with 19 channels (Fp1, Fp2, F7, F3, Fz, F4, F8, T3, C3, Cz, C4, T4, T5, P3, Pz, P4, T6, O1, O2, M1, M2) according to the international 10–20 system, electrooculogram (EOG, 200 Hz) with two electrodes per eye, electromyogram (EMG, 200 Hz) on the chin and two electrocardiogram (ECG, 200 Hz) leads (Embla N7000, RemLogic v3.2). The EEG quality was checked multiple times during each wake phase by trained study personnel, especially directly before the beginning of a nap, and the EEG electrodes were adjusted as necessary. Sleep stages were analyzed by an experienced sleep scorer according to the standard criteria of the American Association of Sleep Medicine51 using the standard software of the recording system. EEG segments containing excessive artifacts were excluded from the scoring process. Further processing of the sleep architecture and the extraction of sleep parameters were performed with MATLAB2018b (MathWorks, Massachusetts, USA). Per baseline, recovery sleep and nap, we calculated various sleep parameters such as Total Sleep Time (TST) (the total sum of epochs scored as rapid eye movement sleep (REM) and non-rapid eye movement sleep (NREM)), Wake After Sleep Onset (WASO) (number of wake epochs after falling asleep the first time), Sleep Latency (SL) (the duration between lights off and the first epoch scored asleep) and Sleep Efficiency (SE) (percentage of time staying asleep).
Maintaining wakefulness between naps was of high priority. Therefore, we measured a maximum of two participants simultaneously, with at least one subject belonging to the group of healthy controls. Further, we employed continuous measurements of EEG/EOG/EMG combined with video documentation throughout the entire protocol (nap and wake phase). In average, (micro)sleep episodes during wake episodes were kept below 1.1% for HC and IH, except of wake six for IH (with 4.8%). NT stayed below 10% of the time and below 5% during daytime (wake one to wake five and wake eight to wake ten).
We conducted a spectral analysis of slow wave activity (SWA) to measure sleep pressure during the protocol based on exported raw EEG data (in EDF file format). To do this, preprocessing of the EEG signal included referencing the EEG to linked mastoid reference (for reducing electrocardiogram and other artifacts), filtering (0.5 Hz high-pass and 40 Hz low-pass filter), and artifact identification on the basis of a 5-s semiautomatic procedure based on power in the 0.75–4.5 Hz and 20–40 Hz bands and visual inspection. Artifact-free 5-s EEG spectra were collapsed and matched with the corresponding sleep stage scores when at least four of six 5-s epochs were artifact-free, otherwise, the whole 30-s epoch was rejected for further spectral analysis. The EEG power during NREM sleep from 0.5 to 4.5 Hz was defined as slow-wave activity (SWA). In a first step, absolute-all-night SWA power during baseline sleep was computed for NREM sleep (N1, N2, N3 for the three frontal derivations F3, Fz, F4) which was taken as reference to normalize SWA values per individual in further analysis. We calculated the relative SWA for the first 80 minutes of baseline and recovery sleep, as well as the relative SWA of the naps, each lasting 80 minutes, to ensure comparability of time points throughout the protocol. Additionally, Khatami et al demonstrate that sleep consolidation occurs during the first sleep cycle in narcolepsy type 1, facilitating further comparability between naps and baseline/recovery sleep.33
Melatonin
The hormone melatonin is used as a marker for the circadian drive, as it is modulated by the circadian rhythm, increasing in the evening hours and lowering during early morning.52–55 To assess the circadian rhythm over the protocol, four saliva samples were collected throughout each wake episode plus two samples in a short wake episode following baseline night (46 samples in total). Melatonin levels were extracted by means of a direct saliva melatonin ELISA kit (Bühlmann Laboratories, Schönenbuch, Switzerland, standard range 0.6–25pg/mL, LoQ 1.6pg/mL, LoD 0.5pg/mL). We applied a hockey-stick method, as described in Danilenko et al,56 to calculate the individual Dim-Light Melatonin onset (DLM on) and offset (DLM off) points, representing the beginning and ending of the biological night.
Subjective Sleepiness
Subjective sleepiness was determined using the Karolinska Sleepiness Scale (KSS), a questionnaire in which the test subjects rate their current, individually perceived sleepiness on a visual analogue scale from 1 (very alert) to 9 (very sleepy).57 The sleepiness was assessed regularly during scheduled wakefulness (after waking up, 30 minutes later to capture possible sleep inertia, halfway through the wake episode, right before and after the performance tasks). For the analysis, an overall sleepiness value was calculated per wake episode by averaging over the second, third and fifth KSS values per wake episode (excluding the effects of sleep inertia as measured with the first KSS), as well as with the workload of the vigilance test battery measured in the fourth KSS (see Figure 2). Besides the Karolinska Sleepiness Scale (KSS), we employed multiple objective measurement parameters, such as the addition tasks for sleep inertia assessments and the psychomotor vigilance tasks.18,58,59
Vigilance
To assess the subject’s vigilance at different times of day, a 10-minute Psychomotor Vigilance Task (10-min-PVT) was performed at the end of each wake episode. The PVT tests the subject’s reaction times to visual stimuli, by pressing a response pushbutton immediately after a counter on a small LED display has started. The PVT measures sustained attention.60 It has been validated as a sensitive method to assess sleepiness under different conditions, including CDH.12,61,62 During post-processing, the number of false starts (when the button was pressed too early) or lapses (when the buttons was not pressed for half a second after the stimulus was presented) were counted. Lapses lasting longer than 15 seconds were considered as sleep attacks and excluded from the analysis. Over the remaining responses, an average speed ( ) was calculated for each ten-minutes-trial and compared between groups and times of day.
) was calculated for each ten-minutes-trial and compared between groups and times of day.
Statistics
If not stated otherwise, statistical analysis was performed in R (RStudio, Inc.) using a linear mixed-model analysis of variance for repeated measures, with group (NT1, IH, HC) and naps as covariables. We called the resulting effects group effect and time of day effect. The model was adjusted for sex, the duration since the last time the subject effectively slept (to control for increased homeostatic sleep pressure) (napping), sleepiness with a dichotomous sleepiness value by thresholding the averaged KSS with 5 (KSS5_dich), the influence of the biological time (either “day” or “night”) (BiolTime) and within-subject variability (VP) (see Eq. 1). Analysis was conducted using the R-package “lme4”.

For all models, normal Q–Q plots were applied, demonstrating normality of the residuals. Moreover, the assumptions of homoscedasticity and linearity were verified using a Tukey-Anscombe plot and autocorrelation among residuals was excluded. P-values of post-hoc tests (R-package “emmeans”) were corrected for multiple comparisons using BenjaminiHochberg correction of false discovery rate.63 If not stated otherwise, data is written as mean ± standard deviation (SD). Statistical differences in sleep onset REM episodes (SOREMPs) were analyzed with a chi-square test and significance level of p < 0.05.
Results
Study Population
Clear characteristics of the individual disorders, namely narcolepsy and idiopathic hypersomnia, were observed. The three subject groups did not differ in terms of age and BMI; however, differences were noted in the distribution of gender. In the patient groups, a higher proportion of women were recruited.
Concomitant diseases were detected and excluded with a test battery of validated clinical questionnaires including a collection of sleep-wake questionnaires used as standard at the University Hospital of Zurich, the Pittsburgh sleep quality index64 (PSQI, threshold >5), Beck depression inventory65 (BDI, threshold >30), Beck anxiety inventory66 (BAI, threshold >25), and Morningness-eveningness questionnaire67 (MEQ, threshold <31 (evening type) and >79 (morning type)). We conducted the Epworth sleepiness scale (ESS, threshold >10) and the Fatigue severity scale (FSS, threshold >4) in a screening questionnaire.
The clinical assessments KSS, PSQI, BDI, BAI, MEQ, ESS, and FSS were used in this study on behalf of the University of Zurich and the University Hospital Zurich exclusively for scientific purposes. The study was conducted in 2018, and the assessments were provided by the University Hospital Zurich. A licence was obtained for ESS for this study. A detailed overview of the demographic data is found in Table 1.
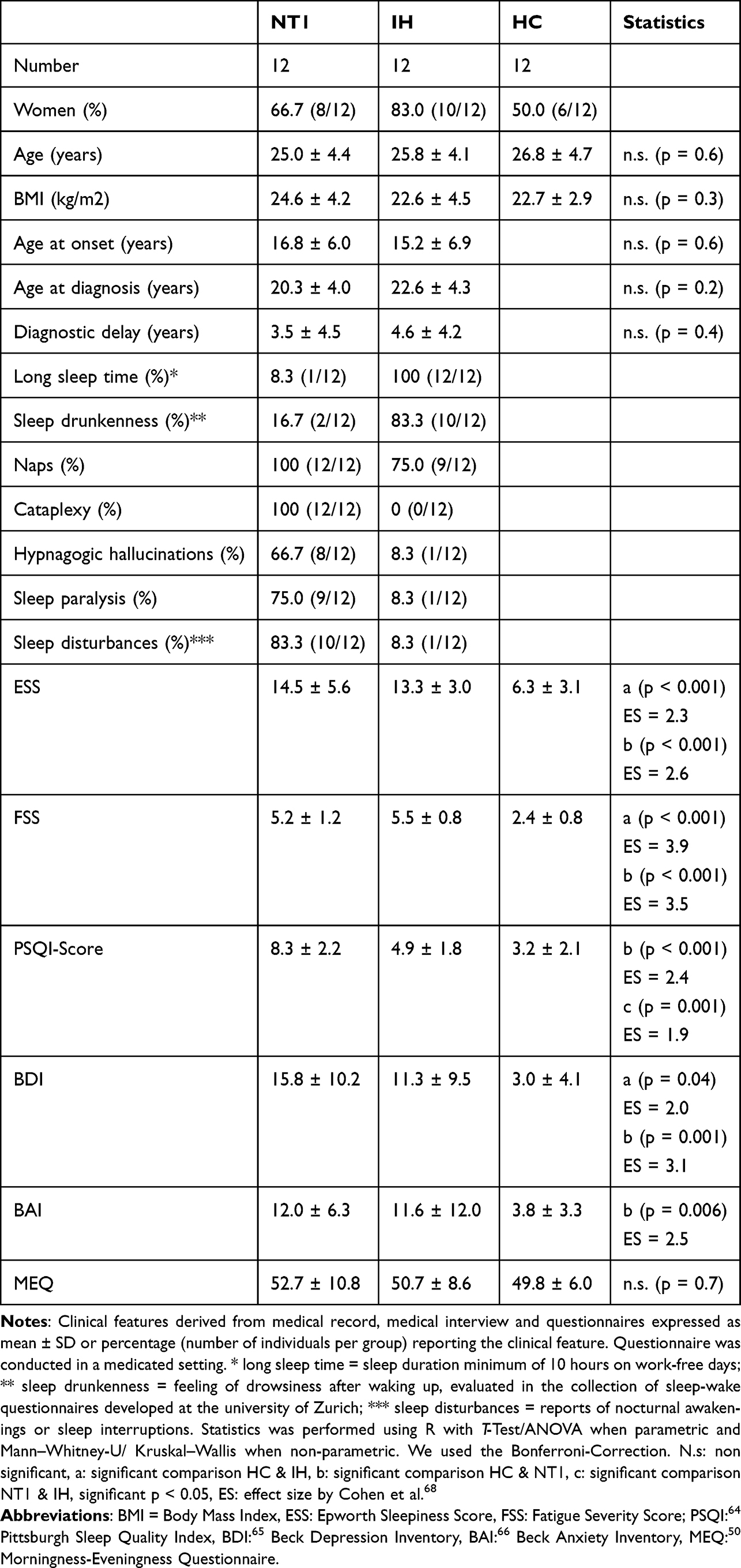 |
Table 1 Clinical Features of Patients with Narcolepsy (NT1), Idiopathic Hypersomnia (IH) and Healthy Controls (HC) |
Reduction of Homeostatic Sleep Pressure
Slow Wave Activity
To ensure that the protocol provided enough sleep to keep the homeostatic sleep pressure sufficiently low, we analyzed the slow wave activity for the first sleep cycles of the baseline and recovery nights and for all naps. Results are shown in Figure 3. A clear decrease in SWA was observed for all groups over the baseline night, from over 150% to 29.9% and 32% for IH and HC, respectively, and 64% for the NT1 group. Starting from this considerably lower level of SWA, an increase in SWA over the first three naps was observed. A saturation plateau converges in NT1 after three naps (limiting rate of 121.8% as modeled with a Michaelis–Menten regression). In HC and IH, a plateau is observed after four naps, on a level of 161.6% and 118.2%, respectively. Differences between the first day of the protocol (naps one-five) and the second day (naps six-ten) were statistically significant over all groups (frontal relative SWA in NT1 first day = 96%, second day = 114%, p = 0.03; frontal relative SWA in IH first day = 69%, second day = 86%, p < 0.001; frontal relative SWA in HC first day = 74%, second day = 119%, p < 0.001), yet stayed below the initial levels of the pre-baseline night.
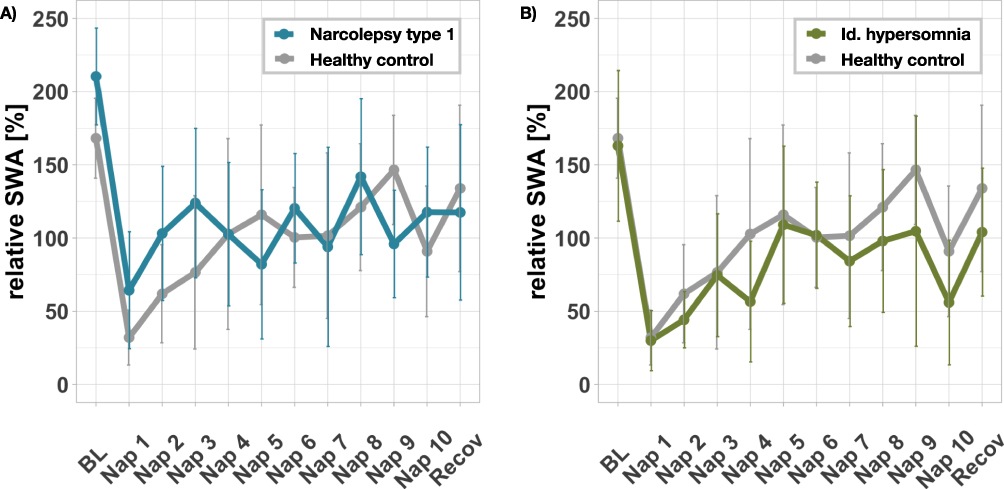 |
Figure 3 The figure shows the frontal relative slow wave activity (SWA) of NT1 compared to HC (A), and IH compared to HC (B), respectively, for the first sleep cycles of baseline and recovery nights and for all naps. The group average per time point is indicated together with its standard deviation. A decrease of SWA over the baseline night is visible, followed by a slight increase converging to a saturation plateau. This suggests that over the protocol, homeostatic sleep pressure can be kept low. |
Sleep Quality in the Recovery Night
We analyzed the sleep of all participants during baseline and recovery nights to notice protocol-induced differences of sleep quality and to exclude any sleep deficiencies (see Table S1 of the Supplemental Material for detailed data separated for each subject group). Compared to the baseline condition, we observed a reduced total sleep time in the recovery night over all groups (baseline TST = 390.0 ± 28.0min, recovery TST = 378.4 ± 23.2min, p < 0.001), less NREM sleep (baseline NREM-duration = 311.6 ± 25.4min, recovery NREM-duration = 291.4 ± 24.4min, p < 0.001), comparable levels of REM sleep (baseline REM-duration = 78.4 ± 27.3min, recovery REM-duration = 87.0 ± 24.7min, p = 0.06) and a decrease in sleep efficiency (baseline SE = 93.1 ± 6.2%, recovery SE = 90.0 ± 5.6%, p < 0.001), each without significant group effects (TST group effect p = 0.9, NREM duration group effect p = 0.8, REM duration group effect p = 0.7, SE group effect 0.8). All groups showed longer sleep latencies during recovery sleep compared to baseline (baseline SL = 6.2 ± 7.3min, recovery SL = 16.8 ± 15.8min, p < 0.001), including NT1. As expected from pathophysiology, a comparison between groups showed a significantly lower sleep latency in patients with narcolepsy compared to IH and HC in both baseline and recovery nights (group effect p < 0.001).
Circadian Modulation of Sleep Parameters
Circadian Rhythm
Our nap protocol allowed the collection of melatonin samples throughout day and night to reproduce its modulation as a marker for process C (see Figure 4). We compared the latest dim light melatonin onset (DLM On) and dim light melatonin offset (DLM Off) for each group (see Table 2). Compared to healthy controls (DLM On 21:55 o’clock ± 1:00 hours, DLM Off 7:54 o’clock ± 1:13 hours), no statistically significant delay of the circadian rhythm was observed in either patient group (NT1 DLM On 22:21 o’clock ± 1:35 hours, NT1 DLM Off 7:38 o’clock ± 1:35 hours; IH DLM On 21:54 o’clock ± 1:08 hours, IH DLM Off 7:15 o’clock ± 1:08 hours, p > 0.05). Further, none of the patient groups showed a significant increase in accumulated melatonin during the night nor an elongated phase of melatonin production. Thus, an unaltered circadian rhythm was found in all groups.
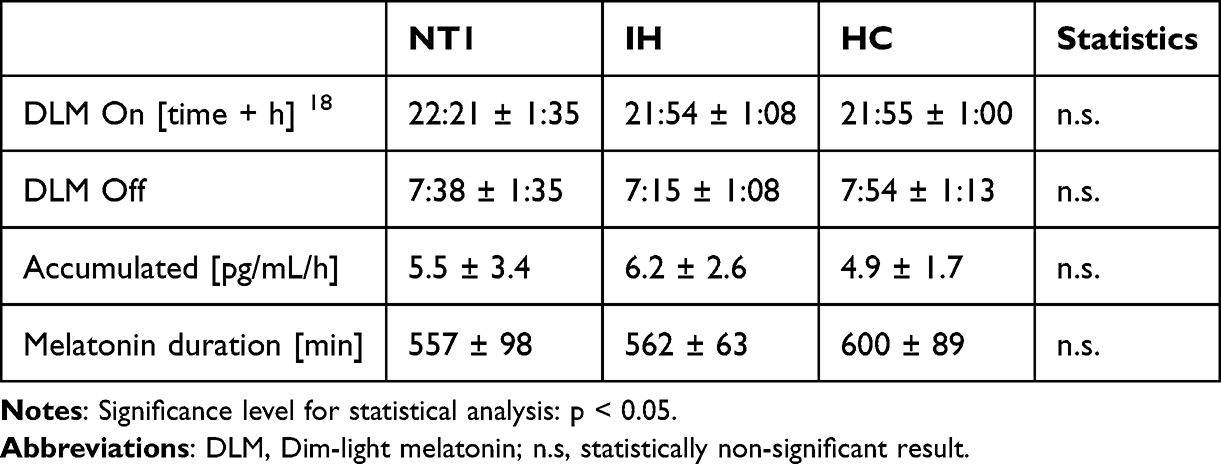 |
Table 2 Melatonin Measurements of Patients with Narcolepsy (NT1), Idiopathic Hypersomnia (IH) and Healthy Controls (HC) |
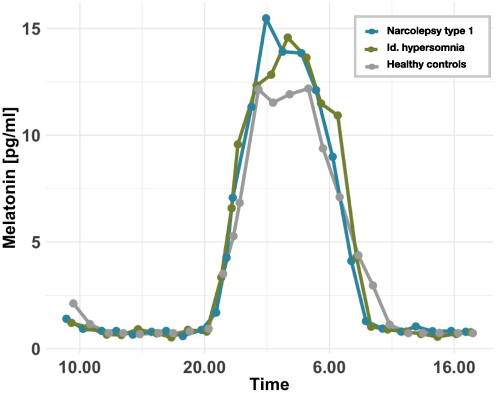 |
Figure 4 Melatonin values from saliva samples collected throughout the protocol and averaged per group. Results are shown for patients with narcolepsy (blue), idiopathic hypersomnia (green) and healthy controls (gray). In all groups, melatonin levels increase in the evening hours and decrease at Dawn, indicating an intact circadian rhythm in all groups. |
Objective Sleep Parameters
Sleep parameters, such as TST, SL and SE, varied throughout the protocol following a circadian modulation, especially in IH and HC. The effect of the time of day was statistically significant (p < 0.001) in all parameters (see Figure 5). In IH and HC, the TST was reduced during the day, from average 62.3 ± 18.9min to 39.4 ± 18.9min in IH and 56.4 ± 25.5min to 33.4 ± 30.4min in HC in the late afternoon (see nap four), indicating the presence of a typical sleep maintenance zone or “forbidden zone of sleep” in the late afternoon hours. Patients with NT1 overall showed a significantly higher TST (TST: NT1 = 761.1 ± 14.3min, IH = 622.9 ± 92.1min, HC = 558.9 ± 100.0min, group effect p < 0.001) without alteration during the “forbidden zone of sleep” (TST mean NT1 = 75.9 ± 4.5min, TST @nap four NT1 = 74.8 ± 5.2min, p = 0.9). The model showed significant interaction effects of group (mainly NT) and time of day (during naps three, four, five and ten). The NREM duration followed the same pattern from average 50.7 ± 16.4min in IH and 42.5 ± 20.2min in HC to 35.4 ± 20.4min in IH and 28.3 ± 25.8min in HC in the later afternoon (See Table S2 for further details on sleep stages). Compared to the other groups, patients with NT1 showed the highest SE (SE: NT1 = 94.3 ± 5.3%, IH = 70.1 ± 31.7%, HC = 77.5 ± 23.5%, group effect p < 0.001) and the least amount of WASO (WASO: NT1 = 2.7 ± 3.4%, IH = 7.7 ± 12.6%, HC = 4.9 ± 10.2%), yet without significant difference to healthy controls (except in nap seven during early morning hours).
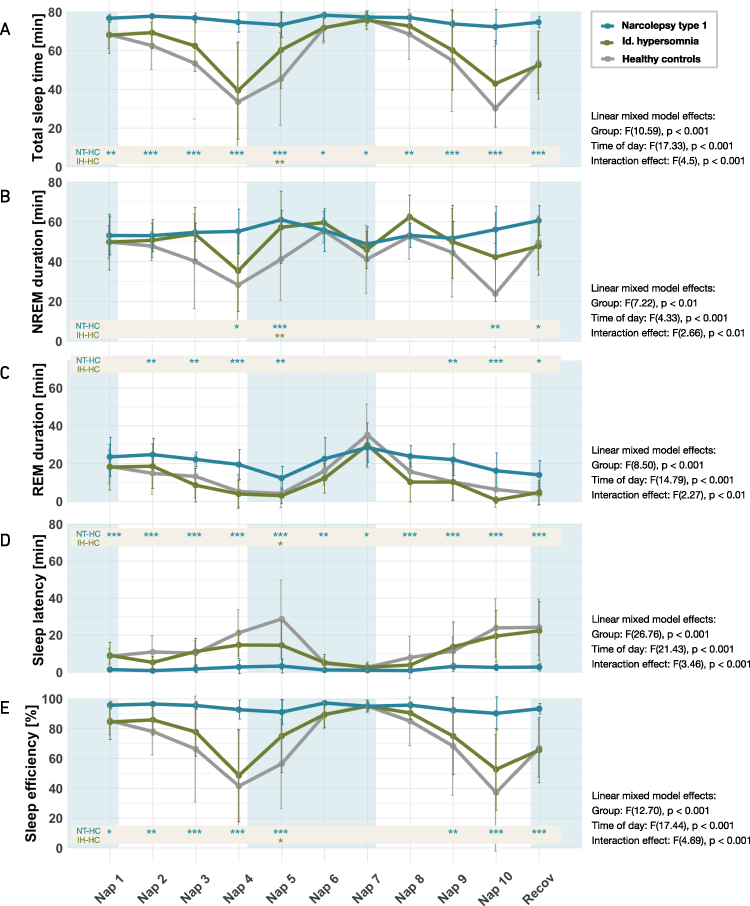 |
Figure 5 Sleep parameters during nap protocol for patients with narcolepsy (blue), idiopathic hypersomnia (green) and healthy controls (gray). Blue and white shaded areas indicate nighttime and daytime, respectively. The group means and standard deviations are indicated per time of day, revealing circadian modulations for Total Sleep Time (A), NREM duration (B), REM duration (C), Sleep latency (D), Sleep Efficiency (E). The linear mixed model effects with their significance levels are indicated per parameter on the right. A post-hoc comparison per time-point was performed to observe differences between patient groups and HC. The results are indicated at the bottom of each plot, with the following statistical significance levels applied: * p < 0.05; ** p < 0.01; *** p > 0.001. |
Patients with idiopathic hypersomnia showed no significant differences in TST (group effect p = 0.25), REM (group effect p = 0.82) and NREM duration (group effect p = 0.87), SE (group effect p = 0.96) and SL (group effect p = 0.43) compared to healthy controls.
Sleep Onset REM Episodes (SOREMPs)
SOREMP is known as a pathophysiological marker for NT1. Accordingly, patients with narcolepsy presented more SOREMPs than the other groups. During baseline and recovery sleep, in nine and ten out of twelve subjects, a SOREMP was observed, respectively. In IH, however, no SOREMP was observed at all, and in healthy controls only one SOREMP was measured during baseline and recovery sleep.
During the protocol, a total of 118 SOREMPs were observed in NT1, most during naps two to four and eight (see Figure 6). However, patients with idiopathic hypersomnia also showed a total of 17 SOREMPs and HC even 45 SOREMPs (group effect p < 0.001), distributed with a modulation over the time of day. Most SOREMPs were measured in the early morning hours (nap seven: NT1 vs HC p = 1.0, IH vs HC p = 0.2, NT1 vs IH p = 0.07), where an increased REM pressure is typically expected. In HC, the number of SOREMPs increased by more than 60% from the first to the second day at the same circadian time yet stayed under the level of SOREMPs in NT1.
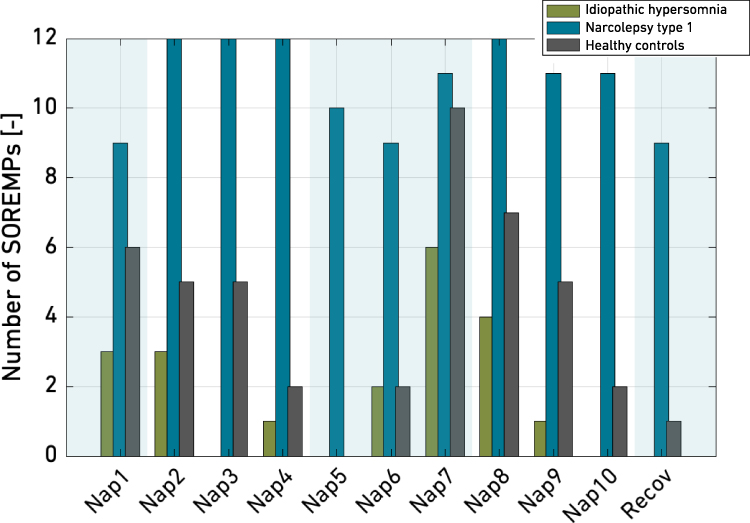 |
Figure 6 Distribution of SOREMPs (sleep onset REM episodes) over the nap protocol for NT1, IH and HC. In NT1, a minimum of nine SOREMPs were observed in each nap. The distribution follows a circadian modulation with ceiling effects in four naps, where the maximum of twelve subjects showed a SOREMP. Also in HC, a strong modulation was observed, peaking in nap seven with nearly as many SOREMPs than in NT1. Patients with IH showed only few SOREMPs, distributed with a slight modulation over all naps. |
Subjective Sleepiness
During the wake episodes, the subjects’ sleepiness levels were regularly queried with the Karolinska Sleepiness scale (see Figure 7). At the beginning of the protocol, high levels of pre-baseline sleepiness levels were only found in patients with IH and NT1 (KSS baseline: IH = 7.33 ± 1.0, NT1 = 8.08 ± 0.7). During the protocol, we observed a circadian modulation in all groups (nap-effect p = < 0.001), with highest subjective sleepiness levels during the night (KSS: NT1 = 5.5 ± 1.8, IH = 7.1 ± 0.9, HC = 5.1 ± 1.4) and lowest levels in the late afternoon (KSS @nap ten: NT1 = 3.7 ± 1.0, IH = 5.6 ± 0.9, HC = 3.8 ± 1.3).
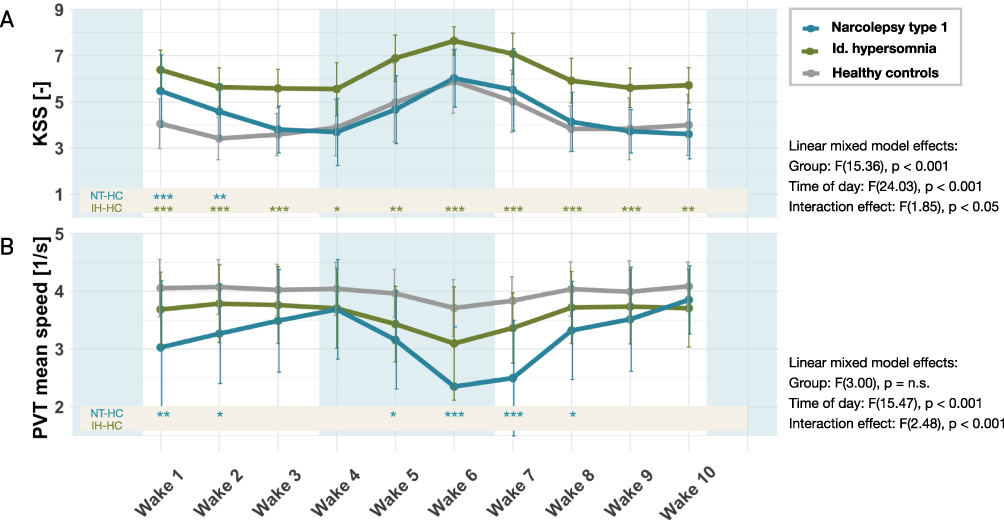 |
Figure 7 Subjective sleep and vigilance (PVT) during nap protocol for patients with narcolepsy (blue), idiopathic hypersomnia (green) and healthy controls (gray). Blue and white shaded areas indicate nighttime and daytime, respectively. The group means and standard deviations are indicated per time of day. A circadian modulation in the subjectively rated sleepiness can be observed (A) with IH showing highest values. All groups presented a smaller (IH, HC) or larger (NT) modulation in their vigilance (B). The linear mixed model effects with their significance levels are indicated per parameter on the right. A post-hoc comparison per time-point was performed to observe differences between patient groups and HC. The results are indicated at the bottom of each plot, with the following statistical significance levels applied: * p < 0.05; ** p < 0.01; *** p > 0.001. |
Patients with idiopathic hypersomnia showed the highest subjective sleepiness overall (KSS: NT1 = 4.5 ± 1.6, IH = 6.3 ± 1.1, HC = 4.3 ± 1.4, p < 0.001), while patients with NT1 indicated only slightly increased subjective sleepiness levels compared to HC during the first day and comparable levels to healthy controls during the second day (group effect NT1 and HC p = 0.4).
To evaluate the effect of the nap protocol on subjective sleepiness, we compared KSS levels before baseline sleep with KSS levels 24 hours later (“first day”), and 48 hours later (“second day”). We found a significant decrease in subjective sleepiness over the course of the protocol in patients with NT1 (KSS baseline NT1 = 8.1 ± 0.7, KSS first day NT1 = 5.2 ± 1.8, p < 0.001; KSS second day NT1 = 4.2 ± 1.8, p < 0.001). The same effect, although to a lesser extent, was observed in IH (KSS baseline IH = 7.33 ± 1.0, KSS first day IH = 6.1 ± 1.4, p = 0.01; KSS second day IH = 6.4 ± 1.2, p = 0.03).
Vigilance
An objective measure of the participant’s vigilance was assessed during each wake episode with a 10-min-PVT (see Figure 7). Healthy controls showed the highest and patients with NT1 the overall lowest performance (speed average: NT1 = 3.2 ± 1.0, IH = 3.6 ± 0.7, HC = 4.0 ± 0.5, p = 0.02). A modulation of vigilance was observed over time of day in all groups (time of day effect p < 0.001). Fastest reaction times with least number of lapses were assessed in the late afternoon and early morning hours, including the “forbidden zone of sleep”, before nap five (speed @wake four: NT1 = 3.7 ± 0.9, IH = 3.7 ± 0.7, HC = 4.0 ± 0.5) and nap eleven (speed @wake ten: NT1 = 3.9 ± 0.6, IH = 3.7 ± 0.7, HC = 4.1 ± 0.4). Slowest PVT results were measured during the night and the early morning hours before nap seven (speed @wake six: NT1 = 2.4 ± 1.0, IH = 3.1 ± 1.0, HC = 3.7 ± 0.5) and nap eight (speed @wake seven: NT1 = 2.5 ± 1.0, IH = 3.4 ± 0.6, HC = 3.8 ± 0.4). Patients with narcolepsy improved their performance significantly over daytime, with higher values on the second day and with highest PVT-speed in the evening hours (speed @wake seven 2.5 ± 1.0 vs speed @wake ten 3.9 ± 0.6, p < 0.001). Neither in IH nor in HC did we see a statistically significant difference between morning and evening hours.
Discussion
In this study, we investigated the circadian rhythm in patients with NT1 and IH in comparison to healthy controls and assessed its influence on sleep and vigilance. We therefore designed and implemented a nap protocol to unmask the circadian drive from homeostatic sleep pressure. We hypothesized that patients with NT1 have an intact circadian rhythm that modulates their sleep and vigilance performance during the day, whereas patients with IH have a circadian rhythm with a lengthened phase.
We devised and implemented a nap protocol for the first time in patients with CDH. The analysis of the sleep characteristics and the slow wave activity indicate that the protocol, indeed, was able to decouple the circadian rhythm from the homeostatic sleep pressure. Slow wave activity was decreased after the baseline night and, due to the regular sleeping opportunities, stayed low during the nap protocol. This is in line with the work of Cajochen et al, who implemented a comparable nap protocol with a sleep-wake cycle of 75/150 minutes in elderly and subjects with depression.25–27 Our analysis further suggests that the protocol did not impose any sleep restriction: the sleep architecture during the recovery night did not differ from the baseline night, the participants even presented lower sleep efficiencies and higher sleep latencies. While the original ultra-short sleep/wake protocols of only 90 minutes are suspected of restricting sleep, this does not appear to be the case with our longer naps.69,70 No signs of insufficient sleep, such as an increased NREM during recovery, was observed. A statement about the optimal length of a nap, however, is difficult to make. One may argue that longer naps would even more effectively reduce the homeostatic sleep pressure, especially as SWA increased from the first day to the second day. On the other hand, longer naps prolong the protocol and thus the subjects’ exposure and could also prevent vigilance measures from being carried out at certain times of the day. For further insights, a protocol comparing systematically different nap lengths would be needed. Concluding, this shows that this type of protocol, although complex in planning and execution, could be further used to better understand the circadian influence in neurological sleep disorders.
Based on saliva melatonin samples, we found an intact circadian rhythm in all three groups. This result matches previous observations in patients with narcolepsy.34–36 Surprisingly, we also observed a regular circadian rhythm in patients with idiopathic hypersomnia, in contrast to the hypothesis of a prolonged circadian rhythm discussed in some literature.44–48 The analysis of the various sleep parameters also shows a circadian modulation over 24 hours in all groups: be it sleep duration, sleep efficiency, modulation of sleep stages, especially REM, and a decrease in (subjective and objective) vigilance, which peaked in the early evening hours. It is noteworthy that IH did not differ significantly from the control group in any of the measured variables, except for nap five. At this time of the early night, a statistically significant deviation was recorded, with a slightly longer sleep duration, shorter latency, but increased efficiency and more NREM. Our results could be interpreted that the circadian wake drive is intact but slightly dampened in this circadian-sensitive time window (“forbidden zone of sleep”) compared to the healthy controls. It should be noted that we excluded extreme chronotypes according to the MEQ during the recruiting process. Nevertheless, an extended circadian period in IH would also have been observed with a phase shift. It could be argued that the measurement points (melatonin samples), which were taken every 70 to 90 minutes, were sampled at a very low frequency to capture changes in the amplitude. However, the sampling frequency was increased during time windows in which an increase or decrease in melatonin was expected. One reason could be that the subjects’ inner clocks were already entrained to a typical 24-hour day and thus did not show their unmasked circadian rhythms. Hence, it would be interesting to repeat the study with subjects being placed beforehand for several days in a time free environment.
For the IH group, the clearly increased subjective sleepiness is striking. This is significantly higher than the HC and NT1 groups – and effectively the only parameter in which the IH group differed from the healthy controls. The increased sleepiness corresponds to the picture of this disease. However, no fundamentally increased sleep pressure was measured. Although the IH showed a lower number of SOREMPs and less N3 sleep in the recovery night, there were no signs of altered sleep during the naps (SL, TST, SE) nor a significantly increased SWA throughout the protocol. A possible explanation would be that the typically increased sleep inertia persisted after the short naps and led to the consistently increased sleepiness. This hypothesis is contradicted by the fact that we measured sleepiness five times per waking phase and found no decrease after 30 or even 60 minutes – the typical length of sleep inertia.71
Our results suggest that the cause of daytime sleepiness in our sample of IH does not lie in the circadian system or in a physiologically increased sleep pressure – at least not one that would prevail over the circadian wake drive. However, further studies with a larger number of test subjects and DLMO measurements are needed to gain more insights and rule out any shifts in the circadian rhythm in IH.
Patients with NT1 showed higher TST and lower SL. What stands out is the high SE throughout the day. Only a minimal reduction in TST and SE in the late afternoon is evident. There was no NT1 patient who completely skipped a sleeping opportunity (which occurred one and twelve times in the IH and HC groups, respectively). The time window of the “forbidden zone of sleep” does not seem to exist in the NT1 group – even though they have a functioning circadian system. This is consistent with previous research, as described by Zeitzer in his review, according to which patients with NT1 showed a normal increase in sleep propensity during late biological night, but no decrease in sleep propensity during late biological day.22,23,69,72 One possible explanation therefore is that the instable state boundary control between sleep and wake is stronger than the influence of the circadian wake drive, so that patients with NT1 can fall asleep very quickly even at unfavorable sleep times. Surprising at the first glance, the consistently high sleep efficiency is also found in the first sleep cycle of the night sleep (eg, baseline and recovery night). In literature, patients with NT1 differ from healthy controls presenting longer total sleep times, lower sleep latencies and an increase in WASO due to sleep fragmentation.33,73 Only in the second and third cycles do the typical fragmentation and many waking phases become apparent. This effect was described as a possible explanation that NT1 patients reduce their NREM sleep pressure so rapidly within a cycle that it is subsequently no longer sufficient to ensure consolidated sleep. Our results would support this explanation: the short duration of the naps seem short enough to enable continuous sleep regardless of the time of day.
We observed an astonishing number of SOREMPs, especially in the REM-sensitive early morning hours between nap seven and nap nine – but not only in patients with narcolepsy. This is noticeable, as in narcolepsy, REM sleep at the beginning of a sleep episode is well described and even serves as a diagnostic marker (MSLT test).74 In our study setup, the NT1 group indeed showed the most SOREMPs, ranging from 8 – at times of circadian nadir – to a maximum of 12 out of 12 subjects. However, also in the HC group, SOREMPs were observed, with a peak of 10 out of 12 in the early morning (nap seven). It has been stated that 3.9% of a cohort of healthy subjects show more than two out of five SOREMPs during an MSLT, yet such a large number of SOREMPs has, to the authors’ knowledge, not previously been described in healthy individuals.75 Apparently, REM pressure is more pronounced in our subjects with very low N2 pressure and, thus, manifests itself more easily at the beginning of a sleep phase. This at the same time means that the time of day has an influence on the measurement, especially when used as a diagnostic marker. It may be argued that conducting diagnostic tests for narcolepsy type 1 during early morning hours – when REM pressure is highest in the overall population – could impair differential diagnosis due to increased SOREMP likelihood in healthy individuals.
The IH patients also showed up to 4 out of 12 SOREMPs, but less pronounced than the healthy subjects. This in itself is remarkable: it is the only parameter in which the NT1 and the IH group show a contrasting behavior compared to the healthy controls. However, when interpreting these results, it should be borne in mind that SOREMPs as a criterion in the MSLT for patients with IH and NT (but especially NT2, which we did not include) has already been criticized, as only insufficient test–retest reliabilities were achieved.76–78 A repetition of the study setup with IH would therefore be all the more valuable.
The subjective sleepiness and PVT results are of particular interest for the question of how the naps affected vigilance. To minimize the effect of sleep inertia directly after waking up as shown in recent literature of patients with central disorders of hypersomnia,61,79 we conducted the PVT before going back to sleep. In all groups, we saw that PVT speed follows a circadian modulation and improves throughout the day. The NT1 patients even performed at a speed in the late afternoon (wake episodes three, four, nine, and ten) that is comparable to that of healthy controls (no significant difference measurable). This is a new perspective, as previous research found the PVT to be sensitive to differences of CDH compared to control subjects yet did not find strong variations according to time of day the test was performed.12 Based on our results, a “zone of vigilance” seems to open up in the late afternoon – subjects with narcolepsy could benefit from the circadian wake drive around this time. Patients with NT1 could try to schedule concentration-intensive tasks such as an exam at school at this time (and take a nap beforehand to reduce homeostatic sleep pressure). This is further emphasized by individual feedback. Some participants felt markedly refreshed after the ten naps. The subjective sleepiness of the NT1 changed as expected: during the night, the subjects were very sleepy, which was also reflected in the PVT performance. It is interesting to note that the NT1 group, although they had the worst reaction time in the vigilance test, did not subjectively rate themselves as any sleepier than the healthy controls. One possible explanation is that they had become so accustomed to this state that they did not consider themselves to be unusually sleepy. However, this is contradicted by the fact that the IH group also suffers from chronic EDS and is well aware of this. Furthermore, the unstable state boundary control could ensure that they are not immune to sleep attacks, but, on the other hand, appear to have a high awareness for alertness. If subjective perception shows no sleepiness at all, is EDS still a problem for them? The answer is probably yes, as the effects on daily performance are still there, which in reality regularly leads to dropping out of school, occupational accidents, or job loss.
Based on our observations, a multi-phase sleep rhythm with several short naps instead of just one could be a promising approach for patients with narcolepsy to cope with everyday life. Especially since their nap sleep is of good quality at any time of the day, even during the forbidden zone of sleep, and they tend to benefit less from longer sleep durations over more than one cycle.
Conversely, for IH, we observed a slight improvement in subjective sleepiness from the first to the second day. This was in contrast to the oral feedback, which indicated a significant burden due to the protocol. The ability to sleep was dependent on the time of day, and they did not benefit from the circadian wake drive any more than healthy individuals do towards the end of the day. In this group, naps do not appear to be a suitable therapeutic approach to EDS.
There were several limitations to the study. Due to the complexity of the nap protocol, the sample size in our study was limited to 12 subjects in each group. Although we carefully selected participants to ensure homogeneity with respect to key demographic and clinical variables, future studies will be important to confirm our results and further explore their generalizability. Also, the influence of entrainment to a 24-h-rest-activity rhythm should be investigated more closely in this context.
As described in our demographic data, the IH group included more female participants. Given that lower skull thickness, which is more common in females, can affect EEG amplitude and thus absolute slow wave activity (SWA), we focused on relative SWA to reduce this anatomical bias. While this approach helps control for inter-individual variability, future studies with balanced sex distributions or direct measures of skull thickness would further improve comparability. The limitation of the naps to 80 minutes was a design choice that allowed us to compare the results of the SWA activity during baseline and recovery with the corresponding naps. However, no statements can be made about shorter or longer naps.
Conclusion
We conducted a nap protocol to investigate, for the first time, the circadian influence on sleep in patients with central disorders of hypersomnolence. We successfully reduced the homeostatic sleep pressure over 40 hours and compared sleep and vigilance parameters, and its exposure to the circadian system, at different times of day. We found an intact circadian rhythm in patients with NT1 and in IH. In both groups, REM and NREM sleep were modulated.
Sleep parameters of patients with narcolepsy varied significantly from those of healthy controls, eg with higher total sleep time, higher amount of SOREMPs and lower sleep latency as suspected by their pathophysiology. Surprisingly, patients with NT1 could profit from the nap protocol presenting with a low rate of sleep fragmentation, which was expressed in a low WASO and a lower subjective sleepiness. The forbidden zone of sleep was clearly visible in vigilance data using PVT with a higher alertness during evening hours, leading to a possible recommendation for therapeutic napping. To establish clear suggestions for nap timing and length in patients with narcolepsy, further studies are needed.
Patients with IH did not show any differences in objective sleep parameters except a lower amount of SOREMP compared to healthy controls. If this finding is also observed in a setting without low sleep pressure, it might be an interesting starting point to further investigate the number of SOREMPs as potential differentiating criterion between IH and other disorders of hypersomnolence. Subjective sleepiness varied in IH strongly compared to healthy controls, and it is not accompanied by objective circadian alteration under low sleep pressure. Moreover, we did not find a significant benefit in regular napping.
Abbreviations
CSF, Cerebral Spinal Fluid; ECG, Electrocardiogram; EDS, Excessive daytime sleepiness; EEG, Electroencephalogram; EMG, Electromyogram; EOG, Electrooculogram; HC, Healthy Control; IH, Idiopathic Hypersomnia; GABA, Gamma-aminobutyric acid; NREM, Non-rapid eye movement sleep; NT1, Narcolepsy type 1; PVT, Psychomotor Vigilance Task; REM, Rapid eye movement sleep; SL, Sleep Latency; SE, Sleep Efficiency; SOREMP, Sleep onset REM; SWA, Slow wave activity; TST, Total Sleep Time; WASO, Wake After Sleep Onset.
Data Sharing Statement
The data underlying this article will be shared on reasonable request (to achieve aims in the approved proposal) to the corresponding author. In particular, individual participant data that underlie the results reported in this article after deidentification will be shared (text, tables, figures, and supplemental material), beginning immediately and ending 2 years following article publication.
Acknowledgments
The authors thank E. Montvai, V. Boller, L. Makowski, G. Da Silva André, and A. Wachter for their support with subject recruitment and overnight data collection, and all participants for taking part in the study.
Author Contributions
Franziska Ryser: investigation, data curation, formal analysis, project administration, visualization, writing – original draft. Ann-Sophie Windirsch: investigation, data curation, formal analysis, writing – original draft. Christian Baumann: resources, methodology, Writing – Review & Editing. Olivier Lambercy: Conceptualization, supervision, writing – review and editing. Roger Gassert: Conceptualization, funding acquisition, writing – review and editing. Esther Werth: Conceptualization, funding acquisition, methodology, investigation, writing – review and editing.
All authors gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Funding
This work was supported in part by the Swiss National Science Foundation under Grant 320030_160075 and the ETH Zurich Foundation.
Disclosure
Aside from the grants indicated in the funding statement, the authors have no conflicts of interest to disclose. This paper is based on the thesis of Franziska Ryser. It has been published on the institutional website: https://www.research-collection.ethz.ch/handle/20.500.11850/588204.
References
1. Ohayon MM, Duhoux S, Grieco J, Côté M-L. Prevalence and incidence of narcolepsy symptoms in the US general population. Sleep Med. 2023;6:100095. doi:10.1016/j.sleepx.2023.100095
2. Abioye A, Dave S, Deyoung K, et al. Assessment of the diagnosed prevalence of Narcolepsy and Idiopathic Hypersomnia in the United States using real world data. Sleep Med X. 2022.
3. Sowa NA. Idiopathic hypersomnia and hypersomnolence disorder: a systematic review of the literature. Psychosomatics. 2016;57(2):152–164. doi:10.1016/j.psym.2015.12.006
4. Komada Y, Inoue Y, Hayashida K, Nakajima T, Honda M, Takahashi K. Clinical significance and correlates of behaviorally induced insufficient sleep syndrome. Sleep Med. 2008;9(8):851–856. doi:10.1016/j.sleep.2007.08.018
5. Pallesen S, Saxvig IW, Molde H, Sørensen E, Wilhelmsen-Langeland A, Bjorvatn B. Brief report: behaviorally induced insufficient sleep syndrome in older adolescents: prevalence and correlates. J Adolesc. 2011;34(2):391–395. doi:10.1016/j.adolescence.2010.02.005
6. Pérez-Carbonell L, Mignot E, Leschziner G, Dauvilliers Y. Understanding and approaching excessive daytime sleepiness. Lancet. 2022;400(10357):1033–1046. doi:10.1016/S0140-6736(22)01018-2
7. AASM, Medicine AAoS. International Classification of Sleep Disorders.
8. Trotti LM, Ong JC, Plante DT, Friederich murray C, King R, Bliwise DL. Disease symptomatology and response to treatment in people with idiopathic hypersomnia: initial data from the Hypersomnia Foundation registry. Sleep Med. 2020;75:343–349. doi:10.1016/j.sleep.2020.08.034
9. Pagel JF. Excessive daytime sleepiness. Am Fam Physician. 2009;79(5):391–396.
10. Slater G, Steier J. Excessive daytime sleepiness in sleep disorders. J Thorac Dis. 2012;4(6):608–616. doi:10.3978/j.issn.2072-1439.2012.10.07
11. Swanson LM, Arnedt JT, Rosekind MR, Belenky G, Balkin TJ, Drake C. Sleep disorders and work performance: findings from the 2008 National Sleep Foundation Sleep in America poll. J Sleep Res. 2011;20(3):487–494. doi:10.1111/j.1365-2869.2010.00890.x
12. Thomann J, Baumann CR, Landolt HP, Werth E. Psychomotor vigilance task demonstrates impaired vigilance in disorders with excessive daytime sleepiness. J Clin Sleep Med. 2014;10(9):1019–1024. doi:10.5664/jcsm.4042
13. Drake C, Roehrs T, Breslau N, et al. The 10-year risk of verified motor vehicle crashes in relation to physiologic sleepiness. Sleep. 2010;33(6):745–752.
14. Garbarino S, Nobili L, Beelke M, De Carli F, Ferrillo F. The contributing role of sleepiness in highway vehicle accidents. Sleep. 2001;24(2):203–206.
15. Gandhi KD, Mansukhani MP, Silber MH, Kolla BP. Excessive daytime sleepiness: a clinical review. Mayo Clin Proc. 2021;96(5):1288–1301. doi:10.1016/j.mayocp.2020.08.033
16. Borbély AA. A two process model of sleep regulation. Hum Neurobiol. 1982;1(3):195–204.
17. Dijk DJ, Czeisler CA. Contribution of the circadian pacemaker and the sleep homeostat to sleep propensity, sleep structure, electroencephalographic slow waves, and sleep spindle activity in humans. J Neurosci. 1995;15(5 Pt 1):3526–3538. doi:10.1523/JNEUROSCI.15-05-03526.1995
18. Burke TM, Scheer F, Ronda JM, Czeisler CA, Wright KP. Sleep inertia, sleep homeostatic and circadian influences on higher-order cognitive functions. J Sleep Res. 2015;24(4):364–371. doi:10.1111/jsr.12291
19. Borbely A. The two-process model of sleep regulation: beginnings and outlook. J Sleep Res. 2022;31(4):e13598. doi:10.1111/jsr.13598
20. Wyatt JK, Ritz-De Cecco A, Czeisler CA, Dijk DJ. Circadian temperature and melatonin rhythms, sleep, and neurobehavioral function in humans living on a 20-h day. Am J Physiol. 1999;277(4 Pt 2):R1152–63. doi:10.1152/ajpregu.1999.277.4.r1152
21. Borbély AA, Daan S, Wirz-Justice A, Deboer T. The two-process model of sleep regulation: a reappraisal. J Sleep Res. 2016;25(2):131–143. doi:10.1111/jsr.12371
22. Zeitzer JM. The neurobiological underpinning of the circadian wake signal. Biochem Pharmacol. 2021;191:114386. doi:10.1016/j.bcp.2020.114386
23. Strogatz SH, Kronauer RE, Czeisler CA. Circadian pacemaker interferes with sleep onset at specific times each day: role in insomnia. Am J Physiol. 1987;253(1 Pt 2):R172–8. doi:10.1152/ajpregu.1987.253.1.R172
24. Lavie P. Ultrashort sleep-waking schedule. III. ‘Gates’ and ‘forbidden zones’ for sleep. Electroencephalogr Clin Neurophysiol. 1986;63(5):414–425. doi:10.1016/0013-4694(86)90123-9
25. Cajochen C, Münch M, Knoblauch V, Blatter K, Wirz-Justice A. Age-related changes in the circadian and homeostatic regulation of human sleep. Chronobiol Int. 2006;23(1–2):461–474. doi:10.1080/07420520500545813
26. Frey S, Birchler-Pedross A, Hofstetter M, et al. Challenging the sleep homeostat: sleep in depression is not premature aging. Sleep Med. 2012;13(7):933–945. doi:10.1016/j.sleep.2012.03.008
27. Birchler-Pedross A, Frey S, Cajochen C, Chellappa SL. Circadian and sleep modulation of dreaming in women with major depression. Clocks Sleep. 2022;4(1):114–128. doi:10.3390/clockssleep4010012
28. Helmus T, Rosenthal L, Bishop C, Roehrs T, Syron ML, Roth T. The alerting effects of short and long naps in narcoleptic, sleep deprived, and alert individuals. Sleep. 1997;20(4):251–257. doi:10.1093/sleep/20.4.251
29. Scammell TE. Narcolepsy. N Engl J Med. 2015;373(27):2654–2662. doi:10.1056/NEJMra1500587
30. Baumann CR, Bassetti CL. Hypocretins (orexins) and sleep-wake disorders. Lancet Neurol. 2005;4(10):673–682. doi:10.1016/S1474-4422(05)70196-4
31. Roth T, Dauvilliers Y, Mignot E, et al. Disrupted nighttime sleep in narcolepsy. J Clin Sleep Med. 2013;9(9):955–965. doi:10.5664/jcsm.3004
32. Khatami R, Landolt HP, Achermann P, et al. Challenging sleep homeostasis in narcolepsy-cataplexy: implications for non-REM and REM sleep regulation. Sleep. 2008;31(6):859–867. doi:10.1093/sleep/31.6.859
33. Khatami R, Landolt HP, Achermann P, et al. Insufficient non-REM sleep intensity in narcolepsy-cataplexy. Sleep. 2007;30(8):980–989. doi:10.1093/sleep/30.8.980
34. Claustrat B, Besset BM. Circadian patterns of melatonin secretion in narcoleptic patients and in controls. Sleep. 1988.
35. Ahmed S, Sack RL. Twenty-four hour secretion of melatonin in normal narcoleptics. Sleep Res. 1991.
36. Blazejova K, Illnerova H, Hajek I, Nevsimalova S. Circadian rhythm in salivary melatonin in narcoleptic patients. Neurosci Lett. 2008;437(2):162–164. doi:10.1016/j.neulet.2008.03.076
37. Saper CB, Scammell TE, Lu J. Hypothalamic regulation of sleep and circadian rhythms. Nature. 2005;437(7063):1257–1263. doi:10.1038/nature04284
38. Saper CB, Chou TC, Scammell TE. The sleep switch: hypothalamic control of sleep and wakefulness. Trends Neurosci. 2001;24(12):726–731.
39. Evangelista E, Leu-Semenescu S, Pizza F, et al. Long sleep time and excessive need for sleep: state of the art and perspectives. Neurophysiol Clin. 2024;54(2):102949. doi:10.1016/j.neucli.2024.102949
40. Zou X, Ptacek LJ, Fu YH. The genetics of human sleep and sleep disorders. Annu Rev Genomics Hum Genet. 2024;25(1):259–285. doi:10.1146/annurev-genom-121222-120306
41. Rye DB, Bliwise DL, Parker K, et al. Modulation of vigilance in the primary hypersomnias by endogenous enhancement of GABAA receptors. Sci Transl Med. 2012;4(161):161ra151. doi:10.1126/scitranslmed.3004685
42. Trotti LM, Saini P, Koola C, LaBarbera V, Bliwise DL, Rye DB. Flumazenil for the treatment of refractory hypersomnolence: clinical experience with 153 patients. J Clin Sleep Med. 2016;12(10):1389–1394. doi:10.5664/jcsm.6196
43. Dauvilliers Y, Evangelista E, Lopez R, et al. Absence of γ-aminobutyric acid-a receptor potentiation in central hypersomnolence disorders. Ann Neurol. 2016;80(2):259–268. doi:10.1002/ana.24710
44. Vernet C, Arnulf I. Idiopathic hypersomnia with and without long sleep time: a controlled series of 75 patients. Sleep. 2009;32(6):753–759. doi:10.1093/sleep/32.6.753
45. Lippert J, Halfter H, Heidbreder A, et al. Altered dynamics in the circadian oscillation of clock genes in dermal fibroblasts of patients suffering from idiopathic hypersomnia. PLoS One. 2014;9(1):e85255. doi:10.1371/journal.pone.0085255
46. Materna L, Halfter H, Heidbreder A, et al. Idiopathic hypersomnia patients revealed longer circadian period length in peripheral skin fibroblasts. Front Neurol. 2018;9:424. doi:10.3389/fneur.2018.00424
47. Landzberg D, Trotti LM. Is idiopathic hypersomnia a circadian rhythm disorder? Curr Sleep Med Rep. 2019;5(4):201–206. doi:10.1007/s40675-019-00154-x
48. Thomas RJ, Bianchi MT. A circadian mechanism for idiopathic hypersomnia - a long biological night. Sleep Med. 2020;74:31–32. doi:10.1016/j.sleep.2020.07.023
49. Ryser F. Movement-Based Sleep Detection – A Wearable Sensor System to Assess Quantity and Quality of Sleep. ETH Zurich; 2022.
50. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97–110.
51. Berry RB, For the American Academy of Sleep Medicine, et al. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. American Academy of Sleep Medicine. 2023;3.
52. Shanahan TL, Czeisler CA. Light exposure induces equivalent phase shifts of the endogenous circadian rhythms of circulating plasma melatonin and core body temperature in men. J Clin Endocrinol Metab. 1991;73(2):227–235. doi:10.1210/jcem-73-2-227
53. Cajochen C, Khalsa SB, Wyatt JK, Czeisler CA, Dijk DJ. EEG and ocular correlates of circadian melatonin phase and human performance decrements during sleep loss. Am J Physiol. 1999;277(3 Pt 2):R640–9. doi:10.1152/ajpregu.1999.277.3.r640
54. Dijk DJ, Cajochen C. Melatonin and the circadian regulation of sleep initiation, consolidation, structure, and the sleep EEG. J Biol Rhythms. 1997;12(6):627–635. doi:10.1177/074873049701200618
55. Wehr TA, Aeschbach D, Duncan WC. Evidence for a biological Dawn and dusk in the human circadian timing system. J Physiol. 2001;535(Pt 3):937–951. doi:10.1111/j.1469-7793.2001.t01-1-00937.x
56. Danilenko KV, Verevkin EG, Antyufeev VS, Wirz-Justice A, Cajochen C. The hockey-stick method to estimate evening dim light melatonin onset (DLMO) in humans. Chronobiol Int. 2014;31(3):349–355. doi:10.3109/07420528.2013.855226
57. Gillberg M, Kecklund G, Akerstedt T. Relations between performance and subjective ratings of sleepiness during a night awake. Sleep. 1994;17(3):236–241. doi:10.1093/sleep/17.3.236
58. Trotti LM. Waking up is the hardest thing I do all day: sleep inertia and sleep drunkenness. Sleep Med Rev. 2017;35:76–84. doi:10.1016/j.smrv.2016.08.005
59. Hilditch CJ, Centofanti SA, Dorrian J, Banks S. A 30-minute, but not a 10-minute nighttime nap is associated with sleep inertia. Sleep. 2016;39(3):675–685. doi:10.5665/sleep.5550
60. Dinges DF, Powell JW. Microcomputer analyses of performance on a portable, simple visual RT task during sustained operations. Behavior Research Methods, Instruments, & Computers. 1985.
61. Trotti LM, Saini P, Bremer E, et al. The Psychomotor Vigilance Test as a measure of alertness and sleep inertia in people with central disorders of hypersomnolence. J Clin Sleep Med. 2022;18(5):1395–1403. doi:10.5664/jcsm.9884
62. Drummond SP, Bischoff-Grethe A, Dinges DF, Ayalon L, Mednick SC, Meloy MJ. The neural basis of the psychomotor vigilance task. Sleep. 2005;28(9):1059–1068.
63. Hochberg Y, Benjamini Y. More powerful procedures for multiple significance testing. Stat Med. 1990;9(7):811–818. doi:10.1002/sim.4780090710
64. Buysse DJ, Hall ML, Strollo PJ, et al. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med. 2008;4(6):563–571.
65. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
66. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi:10.1037//0022-006x.56.6.893
67. Urbán R, Magyaródi T, Rigó A. Morningness-eveningness, chronotypes and health-impairing behaviors in adolescents. Chronobiol Int. 2011;28(3):238–247. doi:10.3109/07420528.2010.549599
68. Cohen JNJLE. Statistical Power Analysis for the Behavioral Sciences.
69. Dantz B, Edgar DM, Dement WC. Circadian rhythms in narcolepsy: studies on a 90 minute day. Electroencephalogr Clin Neurophysiol. 1994;90(1):24–35. doi:10.1016/0013-4694(94)90110-4
70. Carskadon MA, Dement WC. Sleep studies on a 90-minute day. Electroencephalogr Clin Neurophysiol. 1975;39(2):145–155. doi:10.1016/0013-4694(75)90004-8
71. Tassi P, Muzet A. Sleep inertia. Sleep Med Rev. 2000;4(4):341–353. doi:10.1053/smrv.2000.0098
72. Broughton R, Dunham W, Newman J, Lutley K, Duschesne P, Rivers M. Ambulatory 24 hour sleep-wake monitoring in narcolepsy-cataplexy compared to matched controls. Electroencephalogr Clin Neurophysiol. 1988;70(6):473–481. doi:10.1016/0013-4694(88)90145-9
73. Hudson JI, Pope HG, Sullivan LE, Waternaux CM, Keck PE, Broughton RJ. Good sleep, bad sleep: a meta-analysis of polysomnographic measures in insomnia, depression, and narcolepsy. Biol Psychiatry. 1992;32(11):958–975. doi:10.1016/0006-3223(92)90058-8
74. Marti I, Valko PO, Khatami R, Bassetti CL, Baumann CR. Multiple sleep latency measures in narcolepsy and behaviourally induced insufficient sleep syndrome. Sleep Med. 2009;10(10):1146–1150. doi:10.1016/j.sleep.2009.03.008
75. Singh M, Drake CL, Roth T. The prevalence of multiple sleep-onset REM periods in a population-based sample. Sleep. 2006;29(7):890–895. doi:10.1093/sleep/29.7.890
76. Lopez R, Doukkali A, Barateau L, et al. Test-retest reliability of the multiple sleep latency test in central disorders of hypersomnolence. Sleep. 2017;40(12). doi:10.1093/sleep/zsx164
77. Trotti LM, Staab BA, Rye DB. Test-retest reliability of the multiple sleep latency test in narcolepsy without cataplexy and idiopathic hypersomnia. J Clin Sleep Med. 2013;9(8):789–795. doi:10.5664/jcsm.2922
78. Ruoff C, Pizza F, Trotti LM, et al. The MSLT is repeatable in narcolepsy type 1 but not narcolepsy type 2: a retrospective patient study. J Clin Sleep Med. 2018;14(1):65–74. doi:10.5664/jcsm.6882
79. Evangelista E, Rassu AL, Lopez R, et al. Sleep inertia measurement with the psychomotor vigilance task in idiopathic hypersomnia. Sleep. 2022;45(1). doi:10.1093/sleep/zsab220
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.