Back to Journals » Clinical Ophthalmology » Volume 20
Cigarette Smoking as an Independent Predictor of Endothelial Cell Loss After Cataract Surgery: A Prospective Cohort Study
Authors Confalonieri F, Gaeta A ![]() , Gibertini M, Bravetti GE
, Gibertini M, Bravetti GE ![]() , Campo A, Ferraro V, Scatigna G, Cavallini GM, Petrovski G
, Campo A, Ferraro V, Scatigna G, Cavallini GM, Petrovski G ![]() , Verdina T
, Verdina T ![]()
Received 10 September 2025
Accepted for publication 20 November 2025
Published 17 February 2026 Volume 2026:20 566062
DOI https://doi.org/10.2147/OPTH.S566062
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Filippo Confalonieri,1,* Alessandro Gaeta,2,* Matteo Gibertini,3 Giacomo Edoardo Bravetti,3 Antonio Campo,3 Vanessa Ferraro,4 Gianluca Scatigna,3 Gian Maria Cavallini,5 Goran Petrovski,6– 9 Tommaso Verdina3
1Department of Ophthalmology, Montecchi Hospital of Suzzara, Suzzara, Mantua, 46029, Italy; 2Department of Internal Medicine and Medical Specialties (DIMI), Università Di Genova, Genova, 16132, Italy; 3Department of Ophthalmology, AOU Policlinico Hospital of Modena, Modena, Italy; 4Ophthalmology Unit, AUSL-IRCCS Di Reggio Emilia, Reggio Emilia, Italy; 5Department of Surgical, Medical, Dental & Morphological Sciences with Interest Transplant, Oncological & Regenerative Medicine, University of Modena and Reggio Emilia, Modena, Italy; 6Institute for Clinical Medicine, University of Oslo, Oslo, 0450, Norway; 7Department of Ophthalmology, Oslo University Hospital, Oslo, 0450, Norway; 8Department of Ophthalmology, University Hospital Centre, University of Split School of Medicine, Split, 21000, Croatia; 9Uklonetwork, University St. Kliment Ohridski-Bitola, Bitola, 7000, North Macedonia
*These authors contributed equally to this work
Correspondence: Alessandro Gaeta, Email [email protected]
Purpose: To assess the impact of cigarette smoking on corneal endothelial cell density (ECD), central corneal thickness (CCT), and endothelial morphology following cataract surgery in older adults, and to determine whether smoking independently predicts postoperative endothelial cell loss.
Methods: Prospective, observational cohort study conducted at the Institute of Ophthalmology, University of Modena and Reggio Emilia. Patients over 40 years of age undergoing cataract surgery were enrolled and classified as smokers or non-smokers. ECD, CCT, polymegathism, and pleomorphism were assessed preoperatively and at 1 and 3 months postoperatively using specular microscopy. Smoking exposure was quantified in Pack-Years. Statistical analyses included Student’s t-tests, multivariate linear regression, and Cohen’s d for effect size estimation.
Results: A total of 80 eyes from 80 patients were analyzed. Smokers had significantly lower baseline ECD (2294.8 vs 2523.9 cells/mm2; p = 0.0005) and greater CCT (556.2 vs 538.4 μm; p = 0.004) compared to non-smokers. Postoperative ECD loss was significantly greater in smokers at 1 and 3 months (p < 0.001), with increased CCT and more severe morphological changes. Multivariate analysis confirmed smoking as an independent predictor of endothelial loss (β = − 0.48; p < 0.001). The effect size for ECD reduction was large (Cohen’s d = 1.2).
Conclusion: Cigarette smoking is associated with accelerated endothelial cell loss and impaired corneal recovery after cataract surgery. Smoking history should be systematically incorporated into preoperative risk assessments and patient counseling, with consideration for enhanced perioperative monitoring in smokers.
Keywords: cigarette smoking, cataract surgery, phacoemulsification, corneal endothelial cells, endothelial cell density, central corneal thickness, polymegathism
Introduction
Tobacco smoking is a leading cause of preventable morbidity and mortality worldwide, contributing to systemic and ocular diseases such as cataract, age-related macular degeneration, and impaired corneal healing.1,2 Furthermore, second-hand smoke effects are poorly described in literature especially regarding the ocular impact.3,4 Cigarette smoking promotes excessive production of reactive oxygen species (ROS) and reduces the activity of endogenous antioxidant systems, such as superoxide dismutase and glutathione peroxidase. The resulting oxidative stress leads to lipid peroxidation, protein oxidation, and DNA damage, which compromise endothelial cell integrity and function. Moreover, ROS inactivate nitric oxide (NO), impairing vasodilation and promoting endothelial dysfunction. Chronic oxidative insult also upregulates inflammatory mediators and adhesion molecules, enhancing leukocyte recruitment and accelerating microvascular damage. Collectively, these mechanisms render the vascular endothelium of smokers particularly vulnerable to injury and dysfunction.5 The corneal endothelium, a non-regenerative monolayer critical for maintaining corneal transparency, is highly vulnerable to oxidative stress and microvascular damage induced by cigarette smoke constituents like reactive oxygen species (ROS).3,4 Oxidative stress from smoking accelerates corneal endothelial cell (CEC) apoptosis and dysfunction,2 exacerbating postoperative complications in ocular surgeries. Clinical studies demonstrate that smokers exhibit reduced preoperative endothelial cell density (ECD) and increased central corneal thickness (CCT) compared to non-smokers, reflecting chronic endothelial compromise.6 These baseline differences are clinically significant, as phacoemulsification during cataract surgery further stresses the endothelium, potentially leading to irreversible corneal edema and vision loss.7 Beyond endothelial cell density and thickness, morphometric indicators such as polymegathism and pleomorphism reflect deeper architectural stress within the endothelium. Smoking has been associated with disrupted cellular morphology, but few studies have examined how this translates into recovery after cataract surgery.8 While smoking-induced endothelial damage is well-documented in chronic settings, its impact on postoperative outcome remains understudied. Several studies have shown that even in otherwise healthy individuals, smokers exhibit reduced endothelial cell density prior to any ocular surgery, suggesting preexisting subclinical compromise of the corneal endothelium.9–11 However, how this preoperative vulnerability translates into differential postoperative recovery remains largely unexplored in prospective surgical settings.
Emerging pharmacological interventions, such as ROCK inhibitors, highlight the importance of preserving endothelial integrity, as demonstrated by reduced postoperative cell loss in patients treated with ripasudil.12 However, modifiable risk factors like smoking history are rarely integrated into surgical risk assessments despite their potential to influence recovery trajectories.
This study evaluates cigarette smoking’s effects on ECD and CCT changes following cataract surgery, aiming to establish smoking as an independent predictor of endothelial loss. By elucidating these relationships, we seek to refine preoperative counseling and postoperative monitoring protocols for high-risk patients.
Methods
This study was designed as a prospective, observational cohort study conducted at the Institute of Ophthalmology, University of Modena and Reggio Emilia (Italy). We selected a prospective design because it allows for real-time data collection and minimizes recall bias, which is particularly important when examining dynamic parameters like ECD over time. Observational methodology was chosen due to the ethical impossibility of randomizing patients to smoking status. The local Ethical Committee Comitato Etico Dell’Area Vasta Emilia Nord (AVEN) of the University of Modena and Reggio Emilia approved the study (prot. NO. 8946/23, study number 552/2022/OSS/AOUMO). The study was conducted in accordance with the tenets of the Declaration of Helsinki. All patients gave their written informed consent.
Participants were eligible if they were older than 40 years and had a diagnosis of primary senile cataract. We included both current and former smokers, as well as non-smokers, to fully capture the spectrum of smoking-related endothelial changes. Only individuals who reported regular use of smoked tobacco (for example cigarettes, cigars, or pipe tobacco) were classified as smokers; users of inhaled tobacco alternatives (eg, vaping, heated tobacco products) or oral tobacco (eg, snuff, chewing tobacco) were excluded. Patients were excluded if they had combined or prior ocular surgeries, corneal or systemic comorbidities, or if the surgery was performed by junior surgeons with less than two years of experience, ensuring homogeneity and minimizing surgical variability as a confounding factor.
Data collection was extensive and detailed. Prior to surgery, all patients underwent a thorough ophthalmic examination including specular microscopy with Perseus (CSO Ophthalmic Instrument Construction, Firenze, Italy) to assess baseline ECD (cells/mm2) and CCT (µm), as well as endothelial morphology using the coefficient of variation (CV) to quantify polymegathism and the percentage of hexagonal cells (HEX%) to assess pleomorphism. Best-corrected visual acuity (BCVA) was assessed using standard ETDRS charts and recorded in letter scores. Visual acuity was measured at baseline and at 3 months postoperatively to evaluate functional outcomes following cataract surgery. These values were considered secondary endpoints in the study, aiming to contextualize anatomical changes in the corneal endothelium with overall visual function. These were also measured at 1 and 3 months postoperatively to track morphometric recovery. Additional information was gathered through structured interviews documenting smoking history, quantified in Pack-Years, and systemic and ocular comorbidities were recorded. Cataract severity was classified using the Lens Opacities Classification System (LOCS III). Polymegathism and pleomorphism were assessed through specular microscopy using coefficient of variation (CV) and percentage of hexagonal cells (HEX), respectively.
All patients underwent cataract phacoemulsification surgery by two well trained expert ophthalmic surgeons (TV, GS) between January 1, 2024 and December 31, 2024, using Stellaris Elite device (Bausch & Lomb, Bridgewater, NJ) in a microcoaxial mode with 2.2-mm main incision. In every surgery DiscoVisc (Alcon Laboratories, Inc., Fort Worth, TX) was used as ophthalmic viscosurgical device (OVD). An acrylic intraocular lens (IOL) was implanted in the capsular bag in all patients.
Follow-up assessments were carried out at 1 and 3 months postoperatively. These time points were selected to capture both early and intermediate endothelial responses to surgical trauma, as existing literature suggests that endothelial damage evolves significantly over this period.12–14
For statistical analysis, we employed Student’s t-test to compare smokers and non-smokers for continuous variables such as ECD and CCT. Recognizing the multifactorial nature of endothelial cell loss, we also performed multivariate linear regression to control for potential confounders including age, gender, and Pack-Years. Additionally, effect sizes were calculated using Cohen’s d to quantify the magnitude of observed differences, providing clinically meaningful interpretations beyond p-values. Statistical significance was set at p < 0.05.
Results
A total of 80 eyes from 80 patients were analyzed, including 40 smokers and 40 non-smokers. Baseline demographic and clinical characteristics are summarized in Table 1. The two groups did not differ significantly in age or gender distribution. The mean age of smokers was 78.0 ± 4.1 years (range 71–85) compared with 70.1 ± 4.8 years (range 65–88) in non-smokers. The gender distribution was similar between groups, with a slight male predominance (58% smokers vs 55% non-smokers).
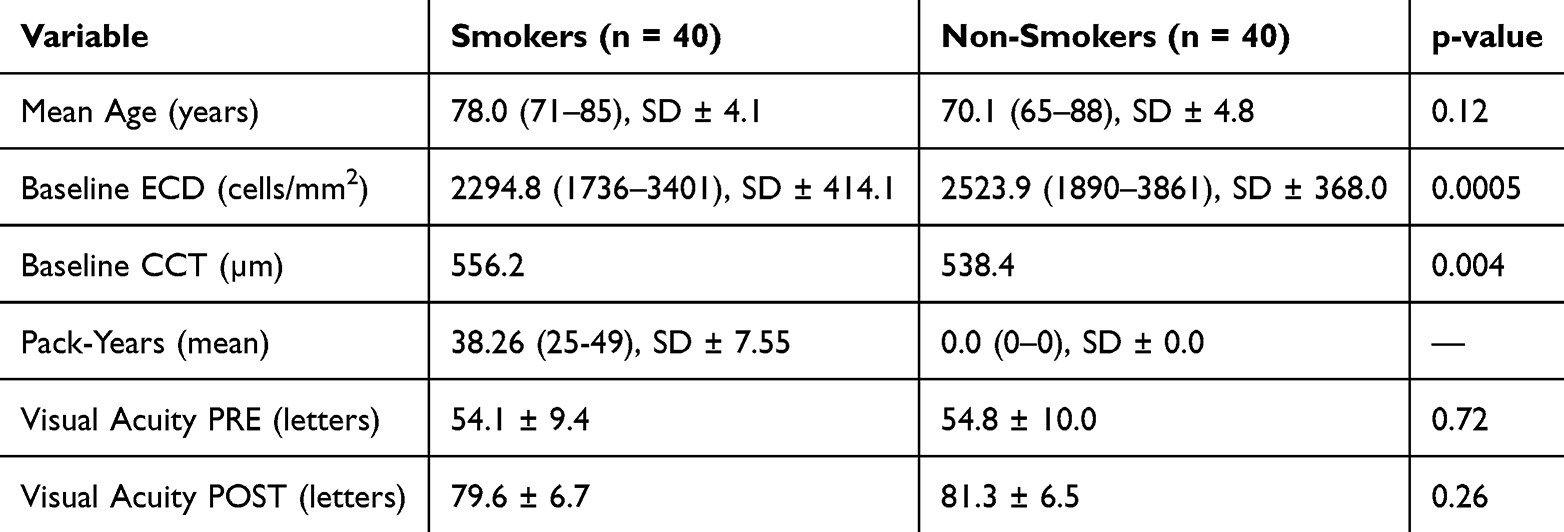 |
Table 1 Baseline characteristics of study participants |
At baseline, smokers exhibited a significantly lower endothelial cell density (ECD) compared to non-smokers (2294.8 cells/mm2, range 1736–3401; SD ±414.1 vs 2523.9 cells/mm2, range 1890–3861; SD ±368.0; p = 0.0005). Central corneal thickness (CCT) was also higher in smokers (556.2 µm vs 538.4 µm; p = 0.004), suggesting a subclinical increase in corneal hydration. The mean Pack-Years for smokers was 38.26 (25–49), SD ± 7.55, while non-smokers reported no history of smoking. Best-corrected visual acuity (BCVA) was assessed using standard ETDRS charts and recorded in letter scores. Visual acuity was measured at baseline and at 3 months postoperatively to evaluate functional outcomes following cataract surgery. Preoperative visual acuity, expressed in ETDRS letters, was comparable between smokers and non-smokers (54.1 ± 9.4 vs 54.8 ± 10.0; p = 0.72). At three months postoperatively, both groups showed substantial visual improvement, with no significant difference observed (79.6 ± 6.7 vs 81.3 ± 6.5; p = 0.26). These values were considered secondary endpoints in the study, aiming to contextualize anatomical changes in the corneal endothelium with overall visual function.
Baseline Endothelial and Corneal Parameters
At baseline, smokers exhibited significantly lower endothelial cell density (ECD) compared to non-smokers (2294.8 ± 414.1 vs 2523.9 ± 368.0 cells/mm2; p = 0.0005). Central corneal thickness (CCT) was higher in smokers (556.2 µm vs 538.4 µm; p = 0.004), suggesting a subclinical impairment of endothelial function. Mean smoking exposure in the smoker group was 38.3 ± 7.6 pack-years. Baseline best-corrected visual acuity (BCVA) was comparable between groups (54.1 ± 9.4 vs 54.8 ± 10.0 ETDRS letters; p = 0.72).
Postoperative Endothelial Cell Density and Corneal Thickness
Both groups showed progressive endothelial cell loss after cataract surgery; however, the reduction was significantly greater among smokers. At 1 and 3 months postoperatively, smokers demonstrated a sharper decline in ECD compared to non-smokers (p < 0.001 at both time points) (Figure 1).
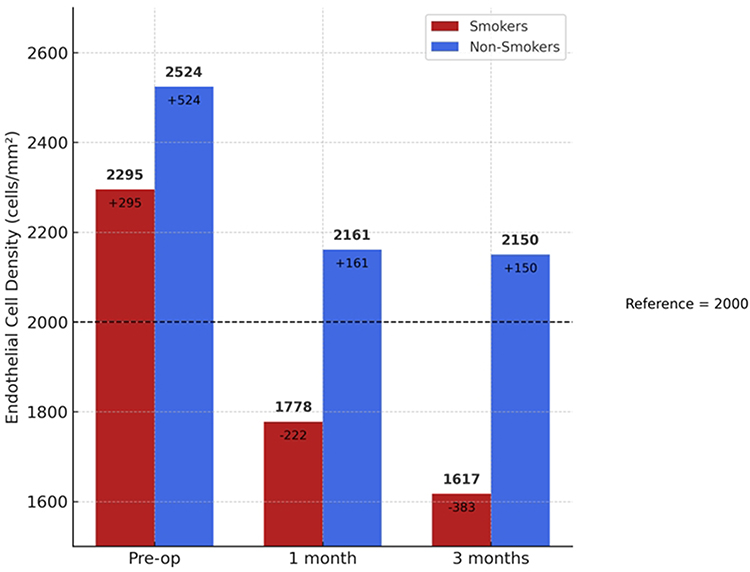 |
Figure 1 Progression of Endothelial Cell Density After Cataract Surgery. Bar chart showing endothelial cell density in smokers and non-smokers at preoperative, 1-month, and 3-month timepoints. A dashed horizontal line marks the reference threshold of 2000 cells/mm2. Bold labels above each bar indicate absolute ECD values, while the smaller numbers show the difference from reference. |
CCT increased after surgery in both groups, with smokers exhibiting consistently greater thickening. At 3 months, mean CCT remained above the 550 µm threshold in smokers but not in non-smokers (Figure 2).
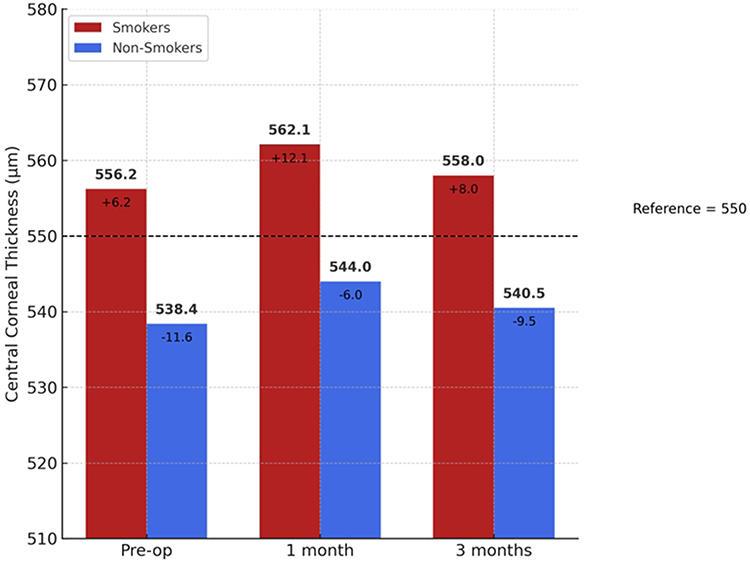 |
Figure 2 Progression of Central Corneal Thickness After Cataract Surgery. Bar chart showing central corneal thickness in smokers and non-smokers at preoperative, 1-month, and 3-month timepoints. A dashed horizontal line marks the reference threshold of 550 µm. Bold labels above each bar indicate absolute CCT values, while the smaller numbers show the difference from reference. |
Multivariate linear regression confirmed smoking as an independent predictor of ECD reduction (β = −0.48; p < 0.001) after adjusting for age, gender, and baseline ocular parameters (Figure 3). Similarly, smoking was the strongest predictor of increased CCT at follow-up (Figure 4). Logistic regression analysis further demonstrated that smoking was associated with higher odds of having postoperative ECD < 2000 cells/mm2 and CCT > 550 µm (Figure 5).
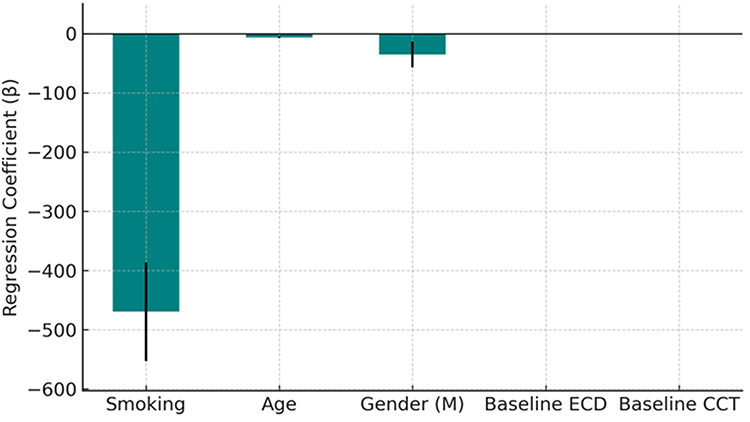 |
Figure 3 Displays the coefficients and standard errors for each variable included in the multivariate regression model assessing predictors of endothelial cell density (ECD) after cataract surgery. Smoking remains a significant independent predictor after adjusting for age, gender, and baseline ocular parameters. |
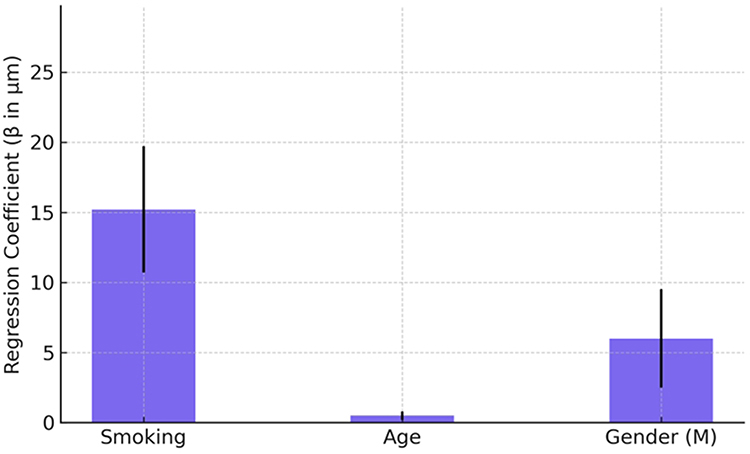 |
Figure 4 This bar chart illustrates the regression coefficients (β) and standard errors from a multivariate model predicting increased central corneal thickness (CCT) after cataract surgery. Smoking was the strongest predictor, followed by gender and age. Baseline ocular characteristics were excluded for clarity. |
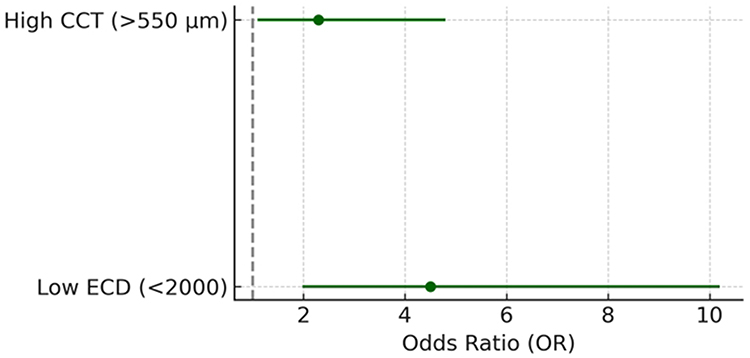 |
Figure 5 Forest plot showing the odds ratios (ORs) and 95% confidence intervals for smoking as a predictor of low endothelial cell density (ECD < 2000 cells/mm2) and increased central corneal thickness (> 550 µm). Values for ECD were derived from logistic regression; CCT values are simulated for illustrative purposes. |
Endothelial Morphology
Morphological analysis revealed significantly greater pleomorphism and polymegathism in smokers. HEX% was lower (47.2 ± 4.5 vs 54.8 ± 3.9; p < 0.001), while CV% was higher (36.5 ± 3.8 vs 30.2 ± 3.1; p < 0.001) in smokers compared with non-smokers (Table 2, Figure 6). Logistic regression adjusted for age confirmed smoking as a significant predictor of both abnormal HEX% and elevated CV% (Figure 7).
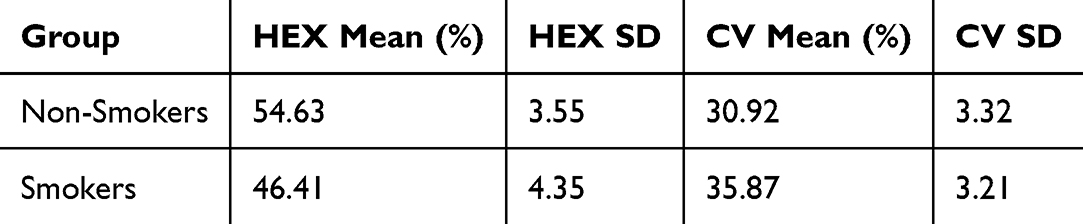 |
Table 2 Morphological Endothelial Parameters by Smoking Status |
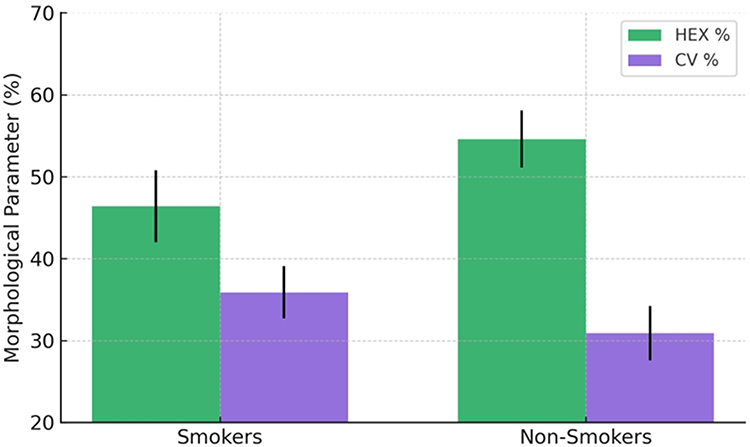 |
Figure 6 Morphological Endothelial Differences by Smoking Status. |
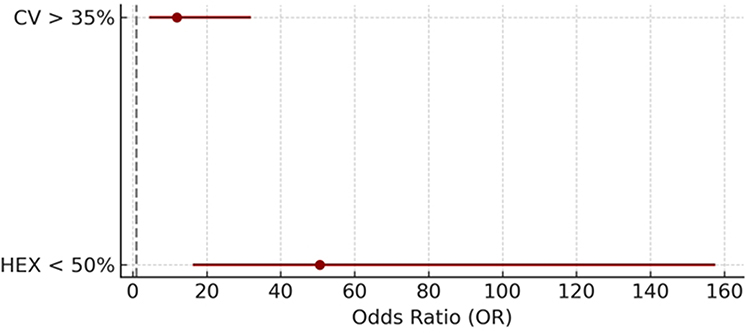 |
Figure 7 Odds Ratios for Morphological Alterations. |
Effect Size Analysis
Effect sizes were large across all parameters, reinforcing the clinical relevance of the observed differences. Cohen’s d values were −0.89 for ECD, 1.96 for CCT, −2.07 for HEX%, and 1.52 for CV%, indicating strong effects of smoking on both endothelial function and morphology (Figure 8).
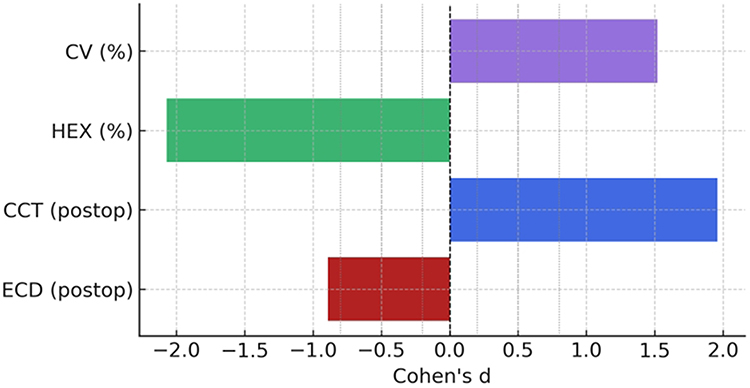 |
Figure 8 Bar chart displaying Cohen’s d effect sizes for differences between smokers and non-smokers across postoperative endothelial parameters. Colors are matched to those used in Figures 2 and 6 for consistency. Dashed reference lines represent standard thresholds for effect size interpretation. |
Visual Outcomes
Visual acuity improved significantly in both groups following surgery, with mean BCVA at 3 months reaching 79.6 ± 6.7 letters in smokers and 81.3 ± 6.5 letters in non-smokers (p = 0.26). Although endothelial alterations were more pronounced in smokers, visual recovery did not differ significantly between groups during the early postoperative period.
Discussion
Impact of Smoking on Corneal Endothelial Health
This prospective observational study demonstrates that cigarette smoking significantly impacts corneal endothelial health following cataract surgery. Smokers exhibited a greater reduction in ECD compared to non-smokers at all postoperative time points. The results align with previous findings that oxidative stress induced by tobacco constituents accelerate endothelial cell loss.15,16
Importantly, through multivariate regression analysis, smoking was confirmed as an independent predictor of both lower postoperative ECD and increased CCT, even after adjusting for age, gender, and baseline ocular characteristics. Beyond descriptive and univariate comparisons, our findings were further validated through multivariate linear and logistic regression analyses. Baseline ECD emerged as the strongest independent predictor of postoperative endothelial cell density (p < 0.001), while smoking status and pack-years demonstrated a trend toward negative impact that did not reach statistical significance when adjusting for age and preoperative cell count. However, in a logistic model using a clinical threshold of 2000 cells/mm2 at 3 months as a marker of endothelial vulnerability, smokers showed an odds ratio of 4.99 for developing low postoperative ECD compared to non-smokers. Despite a wide confidence interval (95% CI: 0.05–489.79) and non-significant p-value (p = 0.492), likely reflecting sample size limitations, this effect size indicates a potential fivefold increase in endothelial risk associated with smoking.
Corneal Thickness and Smoking
In parallel, multivariate linear regression assessing postoperative central corneal thickness (CCT) revealed that smoking status was associated with an average increase of +10.4 µm in CCT at 3 months compared to non-smokers. Although this association did not reach statistical significance (p = 0.302), the positive coefficient aligns with the observed pattern of thicker corneas in smokers and supports the notion of subclinical endothelial dysfunction. Neither age, baseline ECD, nor cumulative exposure (Pack Years) showed significant predictive value for CCT in this model. The lack of independent contribution from Pack Years across both ECD and CCT models suggests that the binary classification of smoking status may be a more robust surrogate for identifying endothelial stress exposure in this population, at least within the exposure range observed. These multivariate insights reinforce the hypothesis that smoking contributes to corneal endothelial fragility through mechanisms not entirely explained by age or preoperative condition and may predispose decompensation in borderline cases. Further prospective studies with larger sample sizes are warranted to confirm these associations and refine risk stratification strategies in patients with a history of tobacco use undergoing cataract surgery.
Morphological Evidence of Endothelial Dysfunction
These findings reinforce the concept that smoking-related endothelial damage persists beyond simple demographic confounding. The increase in CCT provided additional evidence of endothelial dysfunction. Smokers consistently exhibited greater CCT compared to non-smokers both preoperatively and at follow-up. As CCT is closely tied to endothelial pump function, this thickening suggests subclinical edema due to compromised endothelial recovery.9 Furthermore, endothelial morphological parameters, including polymegathism and pleomorphism, were significantly altered in smokers.16 The lower percentage of hexagonal cells (−7.6%) and higher CV (+6.3%) observed in this group suggest disrupted cellular architecture and impaired regenerative dynamics. These findings underscore a more subtle and structural endothelial vulnerability in smokers, beyond simple cell count metrics.16 These morphological changes are clinically significant because they are predictive of long-term corneal instability and potential decompensation. While previous studies have reported the negative impact of smoking on corneal parameters,17 this study longitudinally tracked endothelial recovery after surgery in smokers and non-smokers separately. The magnitude of the observed differences was confirmed by large effect sizes across all functional and morphologic metrics. Particularly, the large Cohen’s d values for both endothelial morphology and central corneal thickness underscore the clinical impact of smoking on corneal recovery following cataract surgery. Smoking thus appears to impair both the quantitative and qualitative aspects of endothelial regeneration postoperatively, raising concerns about the visual prognosis in this patient subgroup. While endothelial cell loss and morphological alterations were more pronounced in smokers, the improvement in visual acuity at 3 months was similar in both groups. This suggests that functional visual outcomes, as measured by ETDRS letter gain, may be preserved even in the presence of subclinical endothelial compromise. The lack of significant difference in BCVA recovery (p = 0.675) supports the hypothesis that corneal endothelial alterations may not immediately impair visual function, though they may still contribute to long-term risks such as corneal decompensation or delayed edema resolution. These findings underscore the importance of evaluating both structural and functional metrics in assessing surgical success.
Clinical Implications and Risk Stratification
From a clinical perspective, the results emphasize the importance of integrating smoking history into preoperative counseling and risk assessment. Ophthalmic surgeons should be aware that smokers are at higher risk for endothelial dysfunction and may benefit from enhanced perioperative care protocols. The mechanisms underlying the endothelial damage observed in smokers warrant further investigation. While this study focused specifically on users of combusted tobacco products (ie, cigarette smokers), it remains unclear whether similar endothelial alterations would occur in users of smokeless tobacco such as chewing tobacco or snuff. Recent evidence suggests that while both forms of tobacco can contribute to systemic oxidative stress, only cigarette smoke with its complex mixture of combustion-derived toxicants such as reactive oxygen species and aldehydes leads to direct endothelial morphological damage. In contrast, smokeless tobacco users did not demonstrate significant changes in endothelial cell density or morphology. These findings support the hypothesis that ocular surface damage is more strongly linked to local exposure to smoke components than to nicotine alone. Further studies, including non-combustion tobacco users (eg, nicotine pouches or heated tobacco products) are needed to isolate the roles of systemic versus local toxicity in corneal health. Strategies could include closer postoperative monitoring, earlier intervention at signs of corneal edema, and patient education on the benefits of smoking cessation. Smokers could benefit from a femtolaser assisted cataract surgery (FLACS) as this technique preserves endothelial cells more than traditional phacoemulsification.14,16,18 In addition, future research could explore pharmacological interventions, such as the use of antioxidants or endothelial protective agents, to mitigate smoking-induced corneal damage. Furthermore, optimizing surgical conditions through management of intraocular pressure and anterior chamber dynamics has gained increasing attention. Recent evidence by Di Maria et al19 demonstrated that preoperative administration of intravenous mannitol significantly reduces intraocular pressure without substantially affecting anterior chamber depth or axial length in both phakic and pseudophakic eyes undergoing cataract surgery. Although mannitol infusion did not induce significant anatomical changes, the reduction in intraocular pressure could potentially facilitate safer surgical maneuvers and reduce endothelial stress, particularly in eyes at risk of intraoperative complications. These findings underscore the importance of a comprehensive perioperative strategy to preserve endothelial integrity, where modulation of intraocular pressure might synergize with careful surgical technique and preoperative risk assessment especially in smoker patients and those who have a reduced ECD.
Several limitations should be acknowledged. This was a single-center study, which may limit generalizability. The sample size, although adequate for detecting significant differences, could be expanded in future multicenter investigations to increase statistical power and external validity. Additionally, while Pack-Years were recorded, precise timing of smoking cessation in ex-smokers was not fully captured, potentially influencing endothelial recovery dynamics. Future studies should aim to stratify outcomes based on the duration of smoking cessation and explore potential protective effects of longer abstinence.20
In conclusion, cigarette smoking emerges as a strong, independent risk factor for impaired corneal endothelial recovery following cataract surgery. These findings should encourage a more proactive approach in managing patients with a smoking history, ultimately aiming to optimize surgical outcomes and long-term corneal health.
Strengths and Limitations
Strengths
One of the strengths of this study is the prospective design, which allowed standardized data collection and minimized variability in measurement conditions. The inclusion of both functional parameters, such as endothelial cell density and central corneal thickness, and morphological markers like the percentage of hexagonal cells and coefficient of variation, provided a more complete picture of the endothelial response to cataract surgery. While the analysis was limited to the early postoperative period, the use of multivariate models adjusted for age helped isolate the effect of smoking from other potential confounders. Additionally, the assessment of endothelial morphology—often overlooked in similar studies—adds a useful layer of clinical relevance, especially given its implications for long-term corneal stability.
Limitations
The prospective nature of the study allowed for standardized data collection and minimized recall bias, especially relevant for monitoring postoperative changes over time.
Potential unaddressed confounders, such as systemic comorbidities or the use of ocular medications not explicitly reported, may have influenced the results and should be considered when interpreting the findings.
Use of specular microscopy enabled precise measurements of ECD, CCT, and morphological indices (polymegathism, pleomorphism), enhancing the reliability of findings.
The classification of patients into smokers and non-smokers, along with multivariate regression analysis adjusting for age, sex, and Pack-Years, strengthened the internal validity and helped isolate the effect of smoking.
The study addresses a commonly overlooked modifiable risk factor smoking in the context of cataract surgery, with immediate implications for surgical planning, patient counseling, and postoperative care.
Reporting of Cohen’s d values provided a clinically meaningful interpretation of results, complementing statistical significance.
Conclusion
In this prospective observational study, cigarette smoking was identified as a significant and independent risk factor for greater corneal endothelial cell loss and impaired postoperative corneal recovery following cataract surgery. Smokers exhibited not only a quantitative reduction in endothelial cell density but also a deterioration of corneal morphological parameters such as polymegathism and pleomorphism.20 These findings highlight the multifaceted damage smoking inflicts on corneal health, both structurally and functionally. Considering that the study has been performed on two independent groups (smokers and non-smokers), and that the primary endpoints will be continuous parameters (CCT and endothelial cell characterization), the minimum sample size has been calculated as indicated in Figure 9.
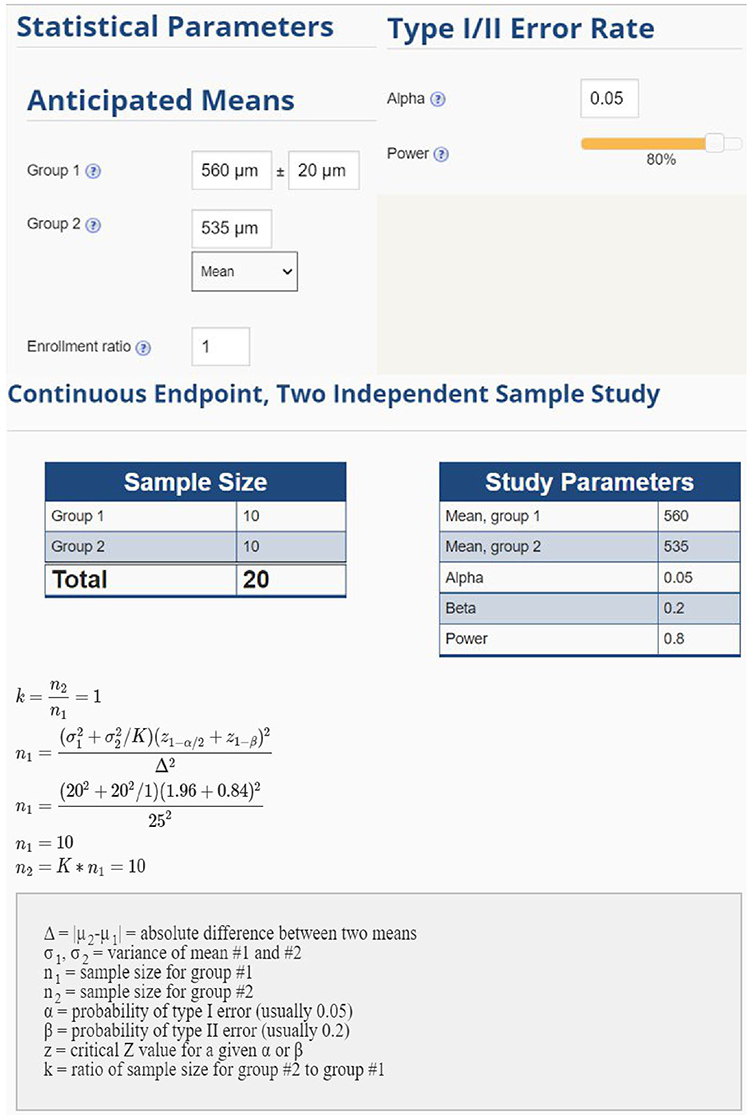 |
Figure 9 Sample size calculation for two independent groups based on anticipated postoperative differences in central corneal thickness. The figure illustrates the statistical model used to estimate the minimum sample size required for detecting a 25-µm difference between groups, assuming a standard deviation of 20 µm, α = 0.05, and 80% power. Under these parameters, a minimum of 10 eyes per group (total = 20) was determined to achieve adequate statistical power for the primary continuous endpoints. |
Given the magnitude of the endothelial compromise observed, smoking history should be systematically integrated into preoperative risk stratification and patient counseling protocols. Surgeons should maintain heightened vigilance in managing smokers undergoing cataract surgery, considering closer postoperative monitoring and potentially tailored perioperative care strategies.
Future multicenter studies with larger cohorts and extended follow-up are warranted to confirm these findings and to investigate potential protective interventions aimed at preserving corneal endothelial integrity in smokers. Integrating smoking cessation counseling as part of the surgical pathway may represent a simple yet impactful measure to optimize surgical outcomes and preserve long-term corneal health.
Ethical Considerations
Participants provided written informed consent. The study adhered to the Declaration of Helsinki principles.
Disclosure
None of the authors have any conflicting interests to disclose for this work.
References
1. Raju P, George R, Ve Ramesh S, Arvind H, Baskaran M, Vijaya L. Influence of tobacco use on cataract development. Br J Ophthalmol. 2006;90(11):1374–12. doi:10.1136/bjo.2006.097295
2. Kulkarni A, Banait S. Through the smoke: an in-depth review on cigarette smoking and its impact on ocular health. Cureus. 2023;15(10):e47779. doi:10.7759/cureus.47779
3. Öberg M, Jaakkola MS, Woodward A, Peruga A, Prüss-Ustün A. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet Gennaio. 2011;377(9760):139–146. doi:10.1016/S0140-6736(10)61388-8
4. Kara S, Gencer B, Türkön H, et al. The effect of smoking on corneal endothelial cells. Semin Ophthalmol. 2017;32(2):223–227. doi:10.3109/08820538.2015.1053626
5. Khudhur ZO, Smail SW, Awla HK, et al. The effects of heavy smoking on oxidative stress, inflammatory biomarkers, vascular dysfunction, and hematological indices. Sci Rep. 2025;15(1):18251. doi:10.1038/s41598-025-03075-8
6. Grzybowski A, Smoking NM, Pathologies E. A systemic review. part I. anterior eye segment pathologies. Curr Pharm Des. 2017;23(4):629–638. doi:10.2174/1381612822666161129152041
7. Vaiciuliene R, Rylskyte N, Baguzyte G, Jasinskas V. Risk factors for fluctuations in corneal endothelial cell density (Review). Exp Ther Med. 2021;23(2):129. doi:10.3892/etm.2021.11052
8. Sayin N, Kara N, Pekel G, Altinkaynak H. Effects of chronic smoking on central corneal thickness, endothelial cell, and dry eye parameters. Cutan Ocul Toxicol. 2014;33(3):201–205. doi:10.3109/15569527.2013.832688
9. Frifelt LEW, Subhi Y, Holm LM, Singh A. Impact of tobacco use on corneal thickness and endothelial health: a systematic review with meta-analyses. Acta Ophthalmol. 2022;100(1):26–34. doi:10.1111/aos.14897
10. Ali M, Khan SY, Jang Y, et al. Cigarette smoke triggers loss of corneal endothelial cells and disruption of descemet’s membrane proteins in mice. Invest Opthalmol Vis Sci. 2021;62(3):3. doi:10.1167/iovs.62.3.3
11. Ilhan N, Ilhan O, Coskun M, et al. Effects of smoking on central corneal thickness and the corneal endothelial cell layer in otherwise healthy subjects. Eye Contact Lens Sci Clin Pract. 2016;42(5):303–307. doi:10.1097/ICL.0000000000000212
12. Ho JW, Afshari NA. Advances in cataract surgery: preserving the corneal endothelium. Curr Opin Ophthalmol. 2015;26(1):22–27. doi:10.1097/ICU.0000000000000121
13. Conrad-Hengerer I, Al Juburi M, Schultz T, Hengerer FH, Dick BH. Corneal endothelial cell loss and corneal thickness in conventional compared with femtosecond laser–assisted cataract surgery: three-month follow-up. J Cataract Refract Surg Settembre. 2013;39(9):1307–1313. doi:10.1016/j.jcrs.2013.05.033
14. Cavallini GM, Fornasari E, De Maria M, Lazzerini A, Campi L, Verdina T. Bimanual femtosecond laser-assisted cataract surgery compared to standard bimanual phacoemulsification: a case–control study. Eur J Ophthalmol. 2019;29(6):629–635. doi:10.1177/1120672118805323
15. Aoshiba K, Nagai A. Oxidative stress, cell death, and other damage to alveolar epithelial cells induced by cigarette smoke. Tob Induc Dis. 2003;1(3):219. doi:10.1186/1617-9625-1-3-219
16. Khan D, Zhou H, You J, Kaiser VA, Khajuria RK, Muhammad S. Tobacco smoke condensate-induced senescence in endothelial cells was ameliorated by colchicine treatment via suppression of NF-κB and MAPKs P38 and ERK pathways activation. Cell Commun Signal. 2024;22(1):214. doi:10.1186/s12964-024-01594-x
17. Gao Y, Yang N, Wei L, Yan Y, Li L. Relationship between postoperative oxidative stress levels and corneal endothelial cell loss after phacoemulsification in diabetic patients with cataract. Clin Ophthalmol. 2024;18:3957–3965. doi:10.2147/OPTH.S497133
18. Narayan A, Evans JR, O’Brart D, Bunce C, Gore DM, Day AC. Laser-assisted cataract surgery versus standard ultrasound phacoemulsification cataract surgery. Cochrane Eyes and Vision Group, curatore. Cochrane Database Syst Rev. 2023;6(6). doi:10.1002/14651858.CD010735.pub3
19. Di Maria A, Ferraro V, Barone G, Gaeta A, Vinciguerra P, Confalonieri F. Preoperative intravenous mannitol administration and its rationale before cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2025;263(1):141–146. doi:10.1007/s00417-024-06589-5
20. Hsueh YJ, Chen YN, Tsao YT, Cheng CM, Wu WC, Chen HC. The pathomechanism, antioxidant biomarkers, and treatment of oxidative stress-related eye diseases. Int J Mol Sci. 2022;23(3):1255. doi:10.3390/ijms23031255
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlations of Immediate Corneal Tomography Changes with Preoperative and the Elapsed Phaco Parameters
Haddad JS, Borges C, Daher ND, Mine A, Salomão M, Ambrósio Jr R
Clinical Ophthalmology 2022, 16:2421-2428
Published Date: 4 August 2022
Impact of Cataract Surgery on IOP and Ocular Structures in Normotensive Patients and Primary and Exfoliation Open-Angle Glaucoma Patients
Xirou V, Xirou T, Siganos C, Ntonti P, Georgakopoulos C, Stavrakas P, Makri OE, Kanakis M, Tsapardoni F, Fragkoulis I, Garnavou-Xirou C, Kozobolis V
Clinical Ophthalmology 2023, 17:1047-1055
Published Date: 5 April 2023
Twist Technique to Stop Fluid Leakage and Fixate the Eye During Bimanual Cortex Removal in Phacoemulsification

Khaled H, Haj Najeeb B
Clinical Ophthalmology 2023, 17:1147-1149
Published Date: 14 April 2023
Visual, Refractive, Functional, and Patient Satisfaction Outcomes After Implantation of a New Trifocal Diffractive Intraocular Lens
Mendicute J, Lauzirika G, Illarramendi I, Martínez-Soroa I
Clinical Ophthalmology 2024, 18:2785-2795
Published Date: 5 October 2024
Evaluation of the Occlusion Break Surge Volume in Five Different Phacoemulsification Systems
Yalamanchili S, Aboughaida A, Rohani OS, Dyk DW
Clinical Ophthalmology 2025, 19:1357-1364
Published Date: 23 April 2025