Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Chronic Obstructive Pulmonary Disease in Hemodialysis Patients: Prevalence, Morbidity and Mortality Risks
Authors Wand O ![]() , Abu Husseine AF Sr, Nacasch N, Benchetrit S, Grupper A, Shashar M
, Abu Husseine AF Sr, Nacasch N, Benchetrit S, Grupper A, Shashar M ![]() , Hod T, Cohen-Hagai K
, Hod T, Cohen-Hagai K
Received 29 May 2025
Accepted for publication 30 September 2025
Published 30 October 2025 Volume 2025:20 Pages 3495—3500
DOI https://doi.org/10.2147/COPD.S543586
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Ori Wand,1,2 Amer Fares Abu Husseine Sr,3,4 Naomi Nacasch,4,5 Sydney Benchetrit,4,5 Ayelet Grupper,4,6 Moshe Shashar,7 Tammy Hod,4,8 Keren Cohen-Hagai4,5
1Division of Pulmonary Medicine, Barzilai University Medical Center, Ashkelon, Israel; 2Faculty of Health Sciences, Ben-Gurion University of the Negev, Beer-Sheva, Israel; 3Department of Internal Medicine A, Meir Medical Center, Kfar Saba, Israel; 4Faculty of Medical and Health Science, Tel Aviv University, Tel Aviv, Israel; 5Department of Nephrology and Hypertension, Meir Medical Center, Kfar Saba, Israel; 6Department of Nephrology and Hypertension, Tel Aviv Sourasky Medical Center, Tel Aviv, Israel; 7Department of Nephrology and Hypertension, Laniado Hospital, Netanya, Israel; 8Renal Transplant Center and Nephrology Department, Sheba Medical Center, Ramat Gan, Israel
Correspondence: Ori Wand, Division of Pulmonary Medicine, Barzilai University Medical Center, Hahistadrut 2 St, Ashkelon, Israel, Email [email protected]
Introduction
The prevalence of subjects who develop end-stage kidney disease (ESKD), requiring renal replacement therapy, most commonly by hemodialysis (HD), is increasing worldwide. ESKD patients have a significantly increased mortality, especially from cardiovascular causes. This risk is associated with comorbidities such as diabetes, hypertension, and atherosclerosis, which are common among HD patients.
Chronic obstructive pulmonary disease, COPD, leads to significant morbidity and mortality by itself, is also frequently associated with comorbidities, some of which are explained by shared risk factors such as smoking and increased age.
Chronic kidney disease (CKD) is common among subjects with COPD and is associated with cardiovascular events and mortality, as well as with reduced quality of life and worse breathlessness.1 Possible pathophysiological mechanisms for the association between COPD and CKD, include systemic inflammation, impaired phosphate metabolism, hormonal and acid-base imbalance, oxidative stress, and chronic hypoxemia.2 Those interactions may contribute to worse outcomes among individuals who suffer from both conditions.
A few studies assessed the impact of COPD among HD patients. In one prospective study, 46% of maintenance HD patients who underwent spirometry had an obstructive pattern. However, respiratory symptoms, exacerbations and clinically meaningful outcomes were not assessed.3
Outcomes of HD patients with or without COPD were compared in just one study from the USA during 1995–2004. The prevalence of COPD increased during this time-period, as were age and other comorbidities.4 HD patients with COPD experienced higher mortality and significantly lower rates of kidney transplantation (KT).4 Being the only study on this subject, those results are difficult to generalize. Indications for HD and KT, patients’ characteristics and treatment modalities differ between countries. Pharmacological treatment for COPD has evolved during the last decade with a positive effect on outcomes but was not previously assessed.
We aimed to measure the prevalence of COPD among HD patients and study how it relates to significant outcomes of mortality and morbidity.
Methods
This comparative, retrospective cohort study was performed in Meir Medical Center, Israel, which provides in-hospital chronic dialysis treatment to 150 HD patients.
Participants were adults (≥18 years-old) who initiated maintenance HD for ESKD during 2015–2018. Subjects who required HD for acute kidney injury or without available clinical data were excluded.
Participants were categorized into one of the two study groups, with or without COPD. Medical records and lung function tests were reviewed by a specialist in pulmonary medicine to ascertain the diagnosis of COPD, which required the presence of a fixed obstructive abnormality on spirometry (post-bronchodilator FEV1/FVC<0.7).
Data were extracted from medical records, including: sociodemographic and anthropometric data; comorbidities; dialysis vintage and adequacy parameters, and baseline laboratory test results collected at the beginning of the first HD session. For the COPD group, we also collected results of pulmonary function tests and regular therapies provided for COPD. Data were collected until December 31st, 2021, or until death. In addition to HD session visits, all subjects undergo a routine monthly visit during which they are assessed by a dedicated nephrologist.
We compared outcomes between study groups from the day of HD initiation for each participant. The primary outcomes were overall mortality rates and mortality over time. Secondary outcomes were the rates of acute coronary syndrome (ACS), registration as KT candidacy, and successful KT.
For the COPD group, we also measured the incidence and number of severe COPD exacerbations, defined as those requiring hospitalization or emergency department visit, treated with systemic corticosteroids and/or antibiotics, in addition to bronchodilators and supportive care. Medical records of severe exacerbations were reviewed by an experienced pulmonologist to increase diagnostic certainty.
Sample Size Calculation
We assumed a 3-year mortality rate of 30% for HD patients without COPD and 60% for HD patients with COPD. We also assumed that a sixth of HD would suffer from COPD. To detect this mortality difference with a power of 80% and an alpha error of 5% required a sample size of 150 subjects.
Statistical Analysis
Descriptive statistics are presented as means with standard deviations or absolute numbers with percentages. Comparison between groups was performed using Mann–Whitney, chi-square or t-test, according to the measured variables. Pearson and Spearman correlations were applied as appropriate. Predictors of ACS and mortality were analyzed using univariate and multivariate models (logistic regression analysis). A multivariable Cox proportional hazards model was constructed to obtain covariate-adjusted measures of mortality rates among COPD and non-COPD patients. The multivariate models included age and other relevant variables according to univariate analysis (p<0.1). A p-value <0.05 was considered statistically significant.
Data were analyzed with SPSS Version 27 (IBM, Armonk, USA).
Ethical Considerations
The study was approved by the Ethics Committee of Meir Medical Center (application MMC-360-20). The committee waived the requirement for participants’ informed consent due to the retrospective nature of the study. The study was performed in accordance with the Declaration of Helsinki and GCP guidelines. Study data were anonymized to maintain confidentiality.
Results
The final study population includes 234 subjects out of a total of 303 who initiated HD between January 1st, 2015, and December 31st, 2018 (Supplementary Figure S1).
Forty-three of 234 were also diagnosed with COPD (18.4%). Compared to subjects without COPD, they were more often males (90.7% vs 64.9%, p=0.001), with a higher prevalence of active smoking (34.9% vs 11%, p<0.001), and had higher incidences of ischemic heart disease and heart failure. Previous KT was less common among subjects with COPD (Table 1).
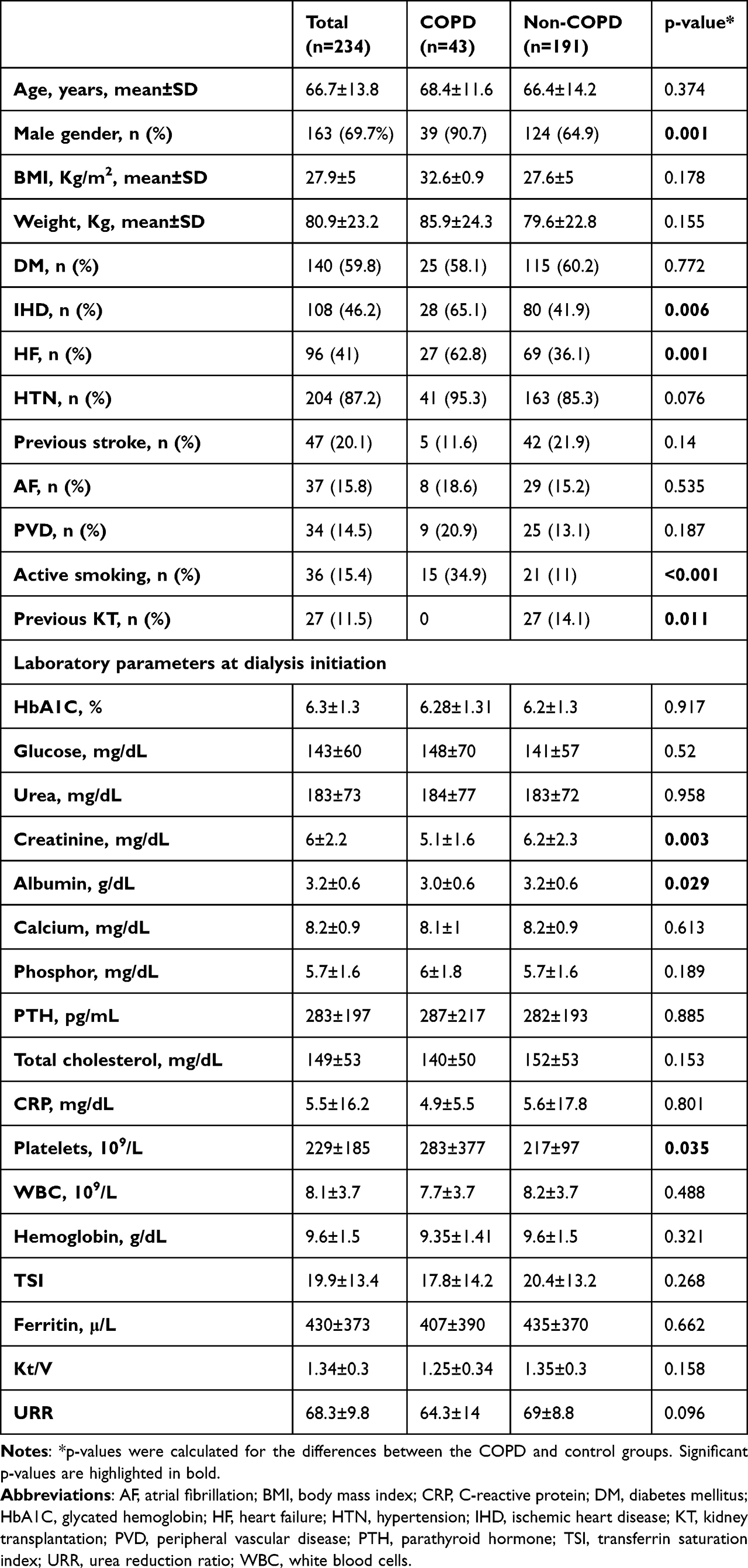 |
Table 1 Baseline Characteristics of Participants |
Average follow-up was longer among the non-COPD group (47.5±23.1 months vs 36.1±23.7 months, p=0.004).
Most baseline laboratory parameters were comparable between groups, except for serum albumin and serum creatinine which were lower for COPD patients, and platelets count which was higher (Table 1).
Subjects with COPD
For the subjects with COPD, the average FEV1%pred and FVC%pred were 60% and 71%, respectively. Eighteen subjects (41.8%) had an FEV1%pred<50% (Supplementary Table S1).
Regular inhaled therapy included long-acting beta-agonists (LABA) in 62% inhaled corticosteroids (ICS) in 63% of COPD patients, short-acting muscarinic antagonists (SAMA) and beta-agonists (SABA) were utilized in 26% and 15%, respectively. Long-acting muscarinic antagonists (LAMA) were regularly used by 28% of HD patients with COPD. Chronic use of prophylactic antibiotics (azithromycin) or roflumilast was uncommon, 4% and 2% of patients, respectively.
Over half of the COPD patients received home oxygen therapy, 24/43, 55.8%, and 10/43 (23.3%) were treated with domiciliary non-invasive ventilation.
Thirty-eight of 43 subjects in the COPD group (88.4%) were hospitalized for COPD exacerbations during follow-up, averaging 3.6±3.2 severe exacerbations per patient during a mean follow-up period of 36.1 months. Of all severe exacerbations, 22.8% (31/136) led to intensive care unit admission, and 26.5% (36/136) required mechanical ventilation. There were no associations between comorbidities or treatment for COPD and severe exacerbations.
Outcomes Comparison Between Groups
During the study period, 39.5% of the COPD group (17 patients) had an ACS vs 23.6% from the control group (45 patients), p=0.026; odds ratio (OR) for ACS for the COPD group was 2.2 (95% CI=1.1–4.4). In a multivariate regression analysis, this association was of similar magnitude, yet with a larger confidence interval (OR=2.19, 95% CI 0.98–4.93, p=0.056) (Supplementary Table S2). The most important predictor of ACS was preexisting coronary heart disease.
Kidney transplantations were numerically less common among HD patients with COPD: 1/43, 2.3% vs 21/191, 11%, p=0.078, as were the rates of registrations as KT candidates: 13/43, 30.2% vs 81/191, 42.4%, p=0.14 (19 patients were still undergoing evaluation for KT candidacy during the study period).
During follow-up, 121 subjects died (51.7% of the cohort). Mortality rates were significantly higher for subjects who suffered from COPD (72.1% vs 47.1%, p=0.003). Odds-ratio for all-cause mortality among COPD patients was 2.87 (95% CI=1.39–5.92).
COPD remained a significant predictor for a fatal outcome after adjusting for age, gender, heart failure, diabetes mellitus and ischemic heart disease, with an adjusted HR for all-cause mortality of 1.7 (95% CI=1.1–2.6, p=0.02). Adjusted mortality rates over time were also higher among HD patients with COPD (Figure 1).
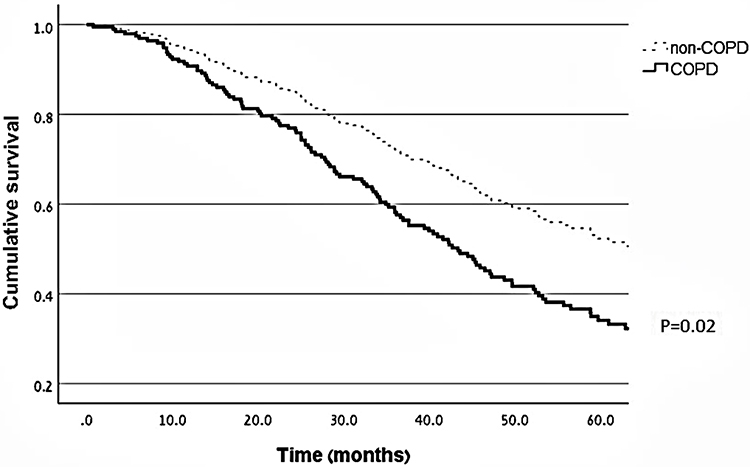 |
Figure 1 Adjusted survival curves of subjects with and without COPD. A multivariable Cox proportional hazards model was constructed to compare covariate-adjusted measures of mortality rates over time between study groups. The model was adjusted for age, gender, presence of heart failure, diabetes mellitus and ischemic heart disease. |
Discussion
A significant proportion of subjects who initiated HD for ESKD suffered from COPD. HD patients with COPD had worse outcomes, including increased mortality and higher rates of ACS.
Some of our results are in-line with the previous report on the subject. In this study by Kent et al, subjects with COPD at dialysis onset were more often males, with higher incidences of comorbidities such as coronary disease and heart failure, and higher rates of active smoking.4 However, the proportion of dialysis patients with COPD between 1995 and 2004 was 7.5%, lower than in our study. This may reflect different lifestyle factors in the studied populations, different indications for HD, and changing temporal trends, as the rate of COPD increased over the years in the study by Kent et al, which reported on subjects 10–20 years prior to our current study. Both studies report on the increased mortality and lower rates of KT among subjects on dialysis with COPD.4 Other studies which reported increased mortality among subjects with CKD and COPD, compared to those without COPD, did not include patients who required HD.5
Several large-scale studies reported higher mortality of HD patients who smoked, irrespective of COPD diagnosis, and an increased risk for cardiovascular-related hospital admissions among HD patients with COPD.6 Overall, our findings are supported by those previous reports associating COPD with increased morbidity and mortality among subjects on HD.
COPD patients in our study had significant disease burden and high-risk features, including recurrent severe exacerbations, need for oxygen and home-ventilatory support, and low pulmonary function tests. Despite this high-risk profile, maintenance inhaler appears to be underutilized. Inhaled medications are the cornerstone of drug therapy for COPD, and they are effective in preventing exacerbations, and improving symptoms and quality of life. It should be acknowledged that we could not assess treatment adherence and prescription rates, or the reasons for underuse of COPD therapies in out cohort.
COPD itself is associated with an increased cardiovascular risk, and a significantly increased risk for cardiovascular events shortly following exacerbations, and up to a year afterward. Thus, preventing exacerbations may be especially crucial in COPD patients with concomitant cardiovascular diseases.7 Despite some concern regarding an association of combination inhaled therapies and risk for adverse cardiovascular events, there is no guidance to avoid inhaled medications based on cardiovascular comorbidities among COPD patients, especially when acknowledging their benefits.8 It is worth noting that safety and cost-benefit of inhaled therapies have not been performed in HD patients since they are generally excluded from studies of medications for other diseases, limiting our understanding of disease behavior and treatment effects in this population. Possible reasons for the underuse of COPD therapy in our cohort may include low adherence rates, less attention to COPD as a comorbidity, or fear of deleterious effects. However, those plausible causes cannot be ascertained in our study.
Limitations of our study include its retrospective, single-center design. The study groups were not balanced at baseline. We tried to compensate for possible confounding by performing multivariate regression analyses of outcomes. While we found no association between COPD therapy and severe exacerbation rates, this may result from the relatively small group of COPD patients. The control group may have included subjects with undiagnosed, pauci-symptomatic COPD, since spirometry was not universally performed, which could also bias the results. The diagnosis of severe COPD exacerbations was based on hospitalizations notes and current definition of exacerbations, which is not specific, and difficult to ascertain retrospectively. Other acute illnesses which are common in HD patients (respiratory infections, pulmonary congestion) might have been misclassified as exacerbations. Significant variables which impact COPD patients were not available for assessment, including symptoms burden, functional capacity, physical activity and frailty. Considering the relatively small group of COPD patients, and since the vast majority (88%) suffered severe COPD exacerbations, it was not possible to assess associations between severe exacerbations and other significant outcomes such as ACS and mortality.
In conclusion, COPD is common among subjects who initiate HD for ESKD. Subjects requiring chronic HD are negatively affected by COPD, which is associated with severe exacerbations, acute coronary syndrome and increased mortality.
Data Sharing Statement
All data analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
We thank Faye Schreiber, MS, for editing the manuscript. She is an employee of Meir Medical Center. Abstract of this paper was presented at the 2004 CHEST Annual Meeting name as a poster presentation and was published in ‘Poster Abstracts’ in CHEST, 2024; 166:4, Supplement A, 4890-A4891. https://journal.chestnet.org/article/S0012-3692(24)03700-0/fulltext.
An abstract of this paper was also presented at the 2024 61st ERA Congress as a poster presentation and was published in ‘Poster Abstracts’ in Nephrology Dialysis Transplantation, 2024; 39:1 supplement, gfae069-1613-2075. https://doi.org/10.1093/ndt/gfae069.1613.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
OW reports a relationship with AstraZeneca, GlaxoSmithKline and Sanofi that includes consulting or advisory and lecture fees, and with Boehringer Ingelheim and Kamada Ltd that includes lecture fees. KCH reports a relationship with GlaxoSmithKline, AstraZeneca, CTSpharma and Boehringer Ingelheim that includes consulting or advisory and lecture fees, and with Fresenius Medical Care that includes consulting or advisory. None of these relationships have impacted this work. The authors report no other conflicts of interest in this work.
References
1. Trudzinski FC, Alqudrah M, Omlor A, et al. Consequences of chronic kidney disease in chronic obstructive pulmonary disease. Respir Res. 2019;20(1):151. PMID: 31299972; PMCID: PMC6626422. doi:10.1186/s12931-019-1107-x
2. Bollenbecker S, Czaya B, Gutiérrez OM, Krick S. Lung-kidney interactions and their role in chronic kidney disease-associated pulmonary diseases. Am J Physiol Lung Cell Mol Physiol. 2022;322(5):L625–L640. PMID: 35272496. doi:10.1152/ajplung.00152.2021
3. Plesner LL, Warming PE, Nielsen TL, et al. Chronic obstructive pulmonary disease in patients with end-stage kidney disease on hemodialysis. Hemodial Int. 2016;20(1):68–77. PMID: 26245152. doi:10.1111/hdi.12342
4. Kent BD, Eltayeb EE, Woodman A, Mutwali A, Nguyen HT, Stack AG. The impact of chronic obstructive pulmonary disease and smoking on mortality and kidney transplantation in end-stage kidney disease. Am J Nephrol. 2012;36(3):287–295. PMID: 22965176. doi:10.1159/000342207
5. Lai CC, Wu CH, Wang YH, et al. The association between COPD and outcomes of patients with advanced chronic kidney disease. Int J Chron Obstruct Pulmon Dis. 2018;13:2899–2905. PMID: 30271136; PMCID: PMC6147210. doi:10.2147/COPD.S174215
6. Li NC, Thadhani RI, Reviriego-Mendoza M, Larkin JW, Maddux FW, Ofsthun NJ. Association of smoking status with mortality and hospitalization in hemodialysis patients. Am J Kidney Dis. 2018;72(5):673–681. PMID: 29909936. doi:10.1053/j.ajkd.2018.04.004
7. Løkke A, Hilberg O, Lange P, et al. Exacerbations predict severe cardiovascular events in patients with COPD and stable cardiovascular disease–a nationwide, population-based cohort study. Int J Chron Obstruct Pulmon Dis. 2023;18:419–429. PMID: 37034899; PMCID: PMC10075268. doi:10.2147/COPD.S396790
8. Regard L, Burgel PR, Roche N. Inhaled therapy, cardiovascular risk and benefit-risk considerations in COPD: innocent until proven guilty, or vice versa? Eur Respir J. 2023;61(2):2202135. PMID: 36758999. doi:10.1183/13993003.02135-2022
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.