Back to Journals » Infection and Drug Resistance » Volume 19
Chronic Mycobacterium kansasii Pleural Infection Mimicking Metastatic Breast Cancer: A Seven-Year Diagnostic Odyssey and the Critical Role of Metagenomic Sequencing
Authors Fang T ![]() , Hu P, Zhang Y, Hu B
, Hu P, Zhang Y, Hu B ![]() , Miao Q
, Miao Q
Received 8 November 2025
Accepted for publication 3 February 2026
Published 26 February 2026 Volume 2026:19 580064
DOI https://doi.org/10.2147/IDR.S580064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Tingting Fang,1,* Pengcheng Hu,2,* Yao Zhang,1,* Bijie Hu,1 Qing Miao1
1Department of Infectious Diseases, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China; 2Department of Nuclear Medicine, Zhongshan Hospital, Fudan University, Shanghai, 200032, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bijie Hu, Department of Infectious Diseases, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, People’s Republic of China, Email [email protected] Qing Miao, Department of Infectious Diseases, Zhongshan Hospital, Fudan University, 180 Fenglin Road, Shanghai, 200032, People’s Republic of China, Email [email protected]
Introduction: Nontuberculous mycobacteria such as Mycobacterium kansasii can mimic malignancy on imaging and pathology, leading to prolonged diagnostic uncertainty and inappropriate anticancer therapy.
Case Report: A 76-year-old woman with remote right breast carcinoma (mastectomy and adjuvant therapy in 1996) had a persistent right chest-wall lesion with rib changes and encapsulated pleural effusion repeatedly interpreted as metastatic disease from 2017 to 2023, despite multiple biopsies showing only fibrous hyperplasia. In August 2024, fever and cough prompted re-evaluation. PET-CT demonstrated a hypermetabolic pleura-adjacent lesion (SUVmax 10.8) without distant metastases. Plasma metagenomic next-generation sequencing (mNGS) yielded a low-level M. kansasii signal; pleural fluid mNGS identified 146 reads (94% relative abundance), later confirmed by culture. Targeted anti-NTM therapy stabilized the infection; however, the patient developed severe varicella-zoster virus infection and cardiac complications and subsequently died. The death was attributed to these complications rather than the progression of the M. kansasii infection.
Conclusion: Chronic M. kansasii pleural infection can masquerade as metastatic breast cancer for years. PET-CT alone is insufficient to distinguish infection from malignancy; careful imaging review combined with unbiased mNGS can establish the diagnosis and avert unnecessary anticancer therapy. Multidisciplinary collaboration is essential for timely recognition and management.
Keywords: Mycobacterium kansasii, pleural infection, metastatic breast cancer mimicry, metagenomic sequencing, chronic infection diagnosis, PET-CT
Introduction
Mycobacterium kansasii is a slow-growing, photochromogenic nontuberculous mycobacterium (NTM) that is typically acquired via inhalation of aerosolized water (often treated municipal water).1 It is one of the more common NTM pathogens worldwide, but its incidence varies regionally.1,2 M. kansasii infections classically cause chronic pulmonary disease in patients with underlying lung conditions (such as chronic obstructive pulmonary disease or prior tuberculosis).1,2 Because M. kansasii shares antigens (ESAT-6, CFP-10) with M. tuberculosis, clinical syndromes and imaging features are usually indistinguishable from tuberculosis.1 Extrapulmonary involvement is uncommon (<10%), but when present may involve pleura, lymph nodes, skin, bone, or genitourinary sites.3,4 In practice, diagnosis is challenging: conventional culture methods are slow (often requiring weeks), and histopathology or imaging can be nonspecific.
Because granulomatous infections can form mass-like lesions, M. kansasii disease can mimic malignancy on imaging. For example, 18F-FDG PET/CT often shows intense uptake in infectious foci. In one series of NTM patients, lesions demonstrated a median SUV of ~8;5 high glucose metabolism in infected tissue may therefore be misinterpreted as cancer. Indeed, cases of M. kansasii pulmonary infection have been mistaken for tumors on PET imaging.6 In a reported case, an apical lung mass due to M. kansasii exhibited an SUV of 12.5 on PET/CT and was initially diagnosed as a Pancoast tumor.6 Thus, routine imaging modalities cannot reliably distinguish NTM lesions from malignancies.
Given these diagnostic pitfalls, new microbiological tools are increasingly important. Metagenomic next-generation sequencing (mNGS) can detect and sequence all microbial DNA in a clinical specimen without requiring specific culture conditions.7–10 This unbiased approach has been shown to identify NTM species (including M. kansasii) directly from patient samples.11,12 In complex or indeterminate cases, mNGS can therefore complement traditional methods by rapidly revealing unexpected pathogens. In summary, the background of M. kansasii – a waterborne NTM causing TB-like lung disease – and the nonspecific imaging findings (often PET-avid) set the stage for potential misdiagnosis of infection as malignancy. The advent of PET/CT and mNGS is thus highly relevant to obtaining an accurate diagnosis in such scenarios.
Detailed Case Description
The subject of this case is a 76-year-old female with a protracted history of right-sided breast carcinoma. In July 1996, she underwent a mastectomy accompanied by an axillary lymph node dissection. Pathological analysis revealed a tumor measuring 3×4 cm, with 4 out of 8 axillary lymph nodes testing positive for malignancy, while the subclavian lymph nodes exhibited no signs of involvement (0/2). Following the surgical intervention, the patient received six cycles of CAF (cyclophosphamide, doxorubicin, and fluorouracil) chemotherapy, succeeded by localized radiotherapy. Notably, endocrine therapy was not included in her adjuvant treatment protocol.
From 2017 to 2023, the patient experienced recurrent metastatic disease affecting the lungs, bones, and lymph nodes. Specifically, since 2018, imaging studies consistently revealed a solid mass in the right chest wall, accompanied by adjacent rib destruction and encapsulated right pleural effusion. Multiple biopsy attempts during this period (including a chest-wall biopsy in 2019 and a pulmonary biopsy in 2022) yielded fibrous tissue hyperplasia without definitive malignant evidence, yet the lesions were persistently interpreted and treated as metastatic disease. Despite the lack of malignant cells in biopsies, the clinical team proceeded with empirical chemotherapy. This decision was driven by the high index of suspicion for metastasis given the patient’s history, the “tumor-like” hypermetabolic features on imaging, and the concern for false-negative biopsy results due to sampling error. In 2019, the patient commenced treatment with carboplatin and etoposide (transitioning to a VP-16 chemotherapy regimen in 2022), transitioning in 2022 exclusively to VP-16 (etoposide), which was ultimately discontinued in June 2024 due to a significant decrease in white blood cell count severe leukopenia.
In August 2024, the patient was admitted to the Infectious Diseases Department presenting with fever (38.6°C), a productive cough, and exacerbated fatigue. A positron emission tomography-computed tomography (PET-CT) scan revealed a metabolically active lesion (SUVmax 10.8) adjacent to the right lung’s chest wall, characterized by a soft tissue mass accompanied by rib destruction and an encapsulated pleural effusion (Figure 1A). These imaging findings were initially interpreted as indicative of metastatic disease, accompanied by tumor-related fever.
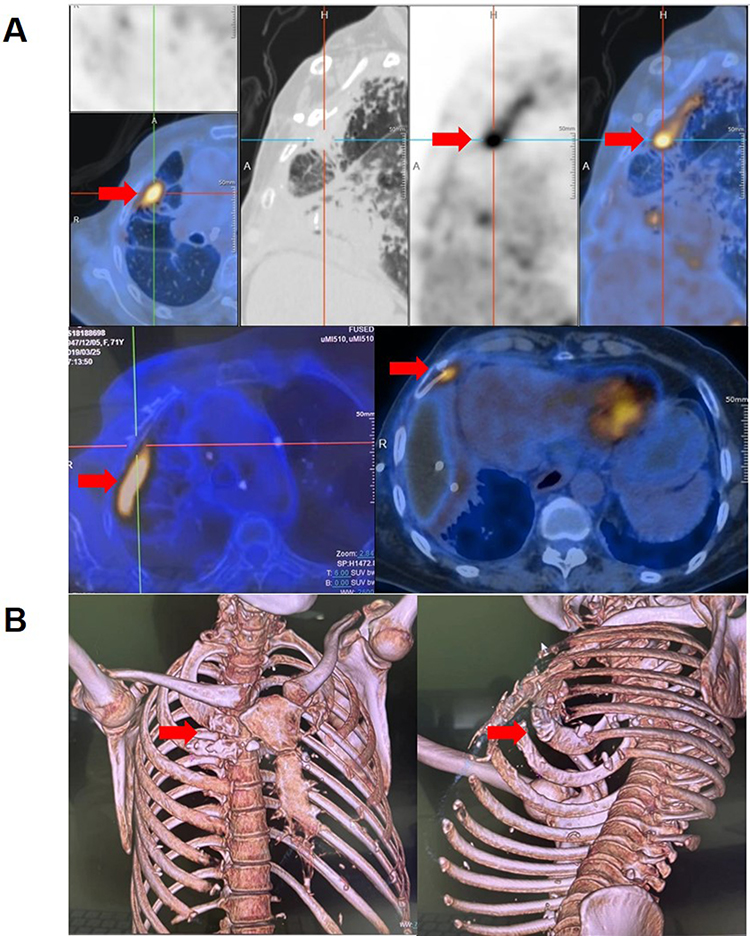 |
Figure 1 Imaging Characteristics. (A) Axial PET-CT scan reveals a hypermetabolic lesion located on the right chest wall (SUVmax 10.8; indicated by arrow) accompanied by rib destruction. (B) Three-dimensional volume rendering illustrates rib cortical hyperplasia (indicated by arrowhead) and pleural fibrosis, which are not indicative of metastatic disease. |
Given the patient’s prolonged anticoagulant therapy for pulmonary embolism, the risks associated with pulmonary puncture were deemed significant. Consequently, plasma metagenomic next-generation sequencing (mNGS) was employed to explore potential infectious causes. The plasma mNGS identified a single read of Mycobacterium kansasii, suggesting a possible nontuberculous mycobacterial (NTM) infection (Figure 2A). Following a thorough risk assessment and family consent, thoracentesis was performed. Approximately 200 mL of bloody pleural effusion was aspirated, with cytological analysis yielding negative results. Additionally, mNGS of the pleural fluid detected 146 reads of Mycobacterium kansasii, with a 94% abundance rate (Figure 2B). Fifteen days later, culture results confirmed the presence of pleural M. kansasii infection. The patient initially received treatment with azithromycin, rifabutin, and ethambutol. However, due to a prolonged QT interval detected by ECG monitoring after one month of therapy, azithromycin and ethambutol were discontinued. Subsequently, she was prescribed linezolid and clofazimine in combination with rifabutin. During this adjusted regimen, she developed a severe varicella-zoster virus (VZV) infection, further complicating her condition, and ultimately succumbed to cardiac arrhythmias likely related to treatment-induced cardiotoxicity.
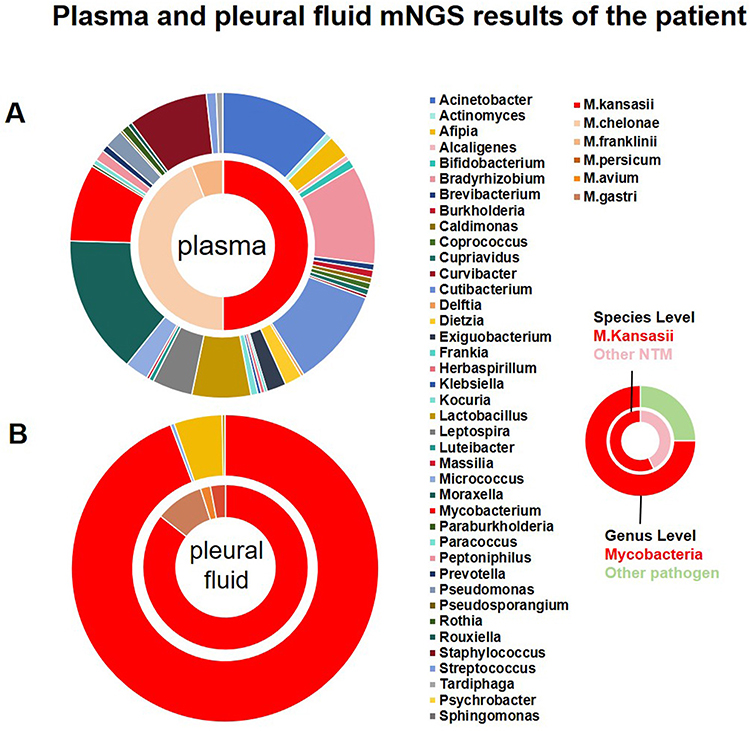 |
Figure 2 Results of mNGS Analysis from Plasma and Pleural Fluid of the Patient. (A) Plasma analysis yielded one read of M. kansasii (with a detection threshold of ≥5 reads). (B) Analysis of pleural fluid revealed 146 reads (94% abundance), thereby confirming the presence of infection. |
Discussion
Through our comprehensive literature review, we identified several pertinent case reports (Table 1)13–19 that elucidate the diagnostic complexities associated with NTM infections, which can often mimic malignancies. The duration from the onset of symptoms to a definitive diagnosis exhibited considerable variability, frequently spanning several months to years, with initial misdiagnoses commonly attributing symptoms to metastatic cancer, lymphoma, or primary tumors. Approximately half of the cases involved PET-CT, which typically revealed hypermetabolic lesions, thereby heightening the suspicion of malignancy. A significant number of patients underwent multiple biopsies prior to achieving a conclusive diagnosis. While histopathological examination and culture were employed in the majority of instances, molecular diagnostic techniques, including polymerase chain reaction (PCR) and mNGS, played a crucial role in confirming the diagnosis in approximately six out of nine cases. These observations underscore the limitations of PET-CT in differentiating malignancies from NTM infections and highlight the critical role of molecular diagnostics in this differentiation.
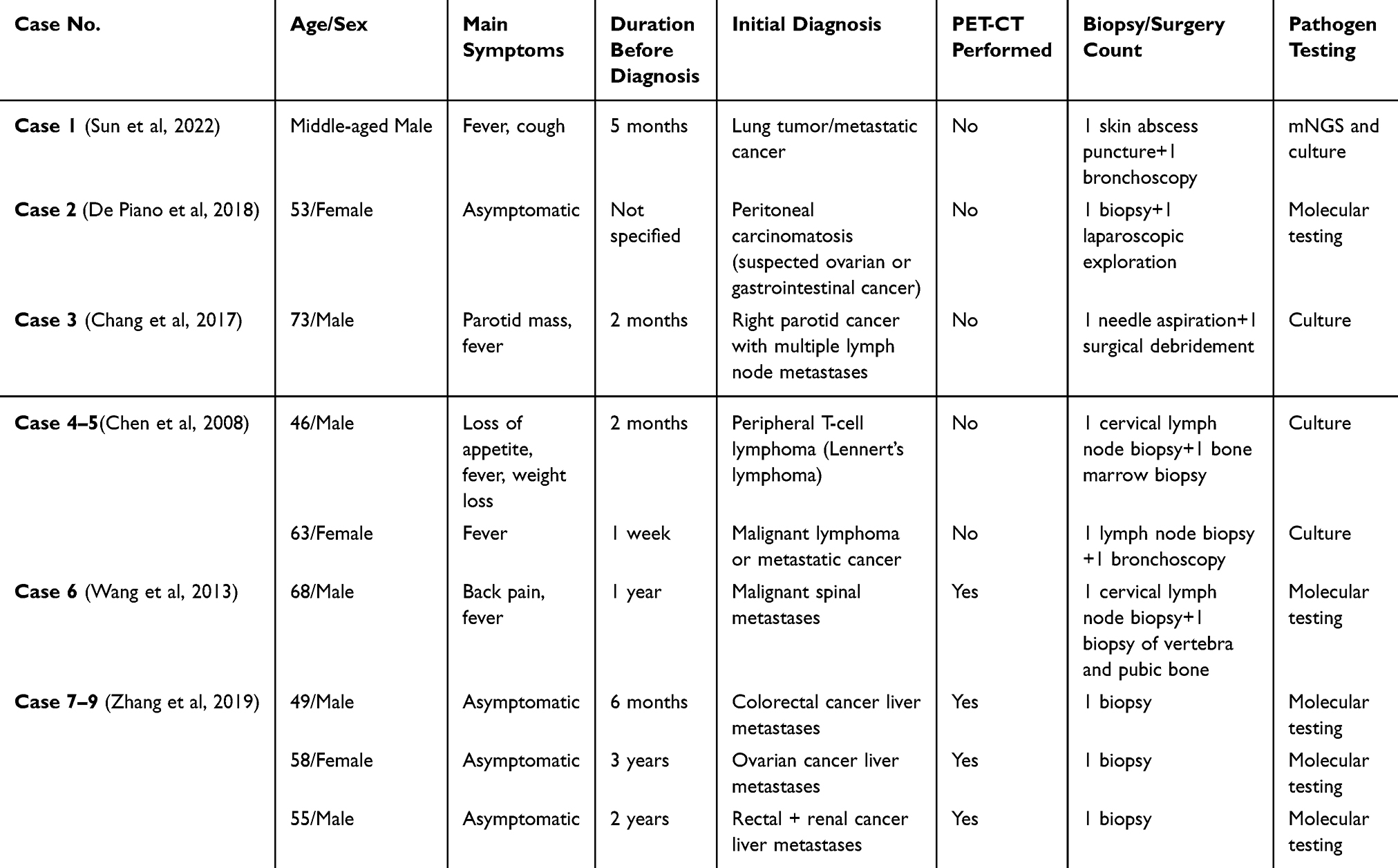 |
Table 1 Reported Cases of Nontuberculous Mycobacteria (NTM) Infections Misdiagnosed as Malignancies: Clinical Characteristics, Imaging Findings, and Diagnostic Methods |
This case notably exemplifies diagnostic pitfalls: oncologists administered chemotherapy for over three years, guided primarily by tumor-like imaging characteristics, despite multiple biopsies consistently showing only fibrous tissue hyperplasia. Retrospectively, the absence of typical granulomas or acid-fast bacilli in previous biopsies was likely due to the dominance of fibrous hyperplasia and the paucibacillary nature of the chronic pleural infection. This non-specific fibrotic reaction masked the underlying pathogen, leading to repeated false-negative pathological assessments. Upon review, our nuclear medicine specialists conducted a thorough analysis of all imaging studies and identified several previously overlooked signs that pointed to an infectious process rather than metastatic disease. Firstly, the significant contraction and deformation of the right thorax suggested chronic lesions leading to fibrosis, rather than malignancy. Secondly, cortical hyperplasia of the ribs, located far from the pleural lesion, indicated chronic infectious stimulation rather than metastatic bone destruction. Thirdly, from a three-dimensional perspective, the flat pleural lesion, which showed no involvement of the bone, was inconsistent with metastatic disease (Figure 1B). Lastly, PET-CT imaging revealed no evidence of lymph node, liver, lung, or bone metastases, making it highly unlikely that the right pleura represented an isolated metastatic site.
This case exemplifies the necessity of a comprehensive imaging assessment in differentiating malignancies from chronic infections, thereby preventing prolonged and misdirected treatments. Our prior research has indicated that the diagnostic efficacy of mNGS for NTM infections is inferior to that for other pathogens and does not provide a significant advantage over traditional diagnostic methods. Specifically, the sensitivity of mNGS for suspected NTM cases was marginally lower than that of culture (29.8% versus 35.1%).9 Moreover, even when integrating multiple molecular diagnostic approaches, including targeted next-generation sequencing (tNGS), mNGS, and PCR, the maximum detection rate for NTM was only 54.8%, representing the optimal performance of molecular techniques in clinical specimens.20 This highlights the ongoing challenges in molecular diagnostics, such as mycobacterial cell wall disruption, low nucleic acid yield, and the necessity for refined interpretation standards.10 In this instance, an extremely low number of Mycobacterium kansasii reads in plasma provided the initial critical clue, prompting further testing, while abundant reads in pleural fluid ultimately confirmed the diagnosis. Thus, despite these limitations, mNGS proved invaluable in guiding the diagnostic pathway and achieving a timely definitive diagnosis in this complex clinical scenario.
This case, in conjunction with relevant literature, underscores the difficulties in distinguishing NTM infections, particularly chronic low-virulence forms, from malignancies, which can lead to unnecessary anti-tumor treatments that compromise immune function and potentially shorten cancer survival. It emphasizes the limitations of conventional imaging and pathology in differentiating infections from metastasis, highlighting the need for further research into the roles of mNGS and PET-CT in enhancing diagnostic accuracy. Additionally, it reinforces the importance of incorporating infectious disease specialists into multidisciplinary tumor boards to mitigate misdiagnosis and optimize patient management.
Conclusion
This case illustrates several important lessons for clinical practice. First, non-tuberculous mycobacterial infections (including M. kansasii) can masquerade as metastatic cancer. Disseminated NTM may involve multiple organs and present like malignancy on imaging,4 leading to prolonged diagnostic delays if not considered. Clinicians should maintain a high index of suspicion for NTM in patients with indolent mass lesions or effusions, especially when standard cancer workup is negative.
Second, molecular diagnostics are pivotal in preventing misdiagnosis. In our patient, metagenomic NGS ultimately identified M. kansasii and enabled appropriate therapy. As demonstrated in prior studies, culture-independent methods like mNGS—by sequencing all microbial DNA in a sample—can rapidly detect rare pathogens that conventional testing may miss.7,21 Incorporating mNGS into infectious workups for atypical cases can shorten “diagnostic odysseys” and guide targeted treatment.
Finally, this case underscores the importance of a multidisciplinary approach. Coordination among oncology, pulmonology, infectious disease, radiology, pathology, and microbiology specialists was critical to re-evaluating the diagnosis. Multidisciplinary collaboration and advanced diagnostics are shown to improve outcomes in rare infections.20,22 Early consultation between clinical teams and the use of novel technologies can therefore avoid unnecessary invasive procedures, reduce delays, and ensure that mimickers of cancer – such as chronic M. kansasii infection – are recognized and treated promptly.
Reporting Guideline Compliance
This case report adheres to the CARE reporting guideline; the completed CARE checklist is provided as Supplementary File S1.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Zhongshan Hospital, Fudan University (B2024-021). Institutional approval to publish was not required. All procedures involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments, most recently updated by the WMA General Assembly in October 2024 (https://www.wma.net/policies-post/wma-declaration-of-helsinki/).
Consent for Publication
Written informed consent for publication of this anonymized case was obtained from the patient’s next of kin (daughter).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Fujian Province Youth Innovation Project (2024J08352, Q. Miao) and Zhongshan Hospital, Fudan University (2023ZSLC24, B. Hu).
Disclosure
The authors declare no competing interests in this work.
References
1. Johnston JC, Chiang L, Elwood K. Mycobacterium kansasii. Microbiol Spectr. 2017;5(1):TNMI7–0011–2016. doi:10.1128/microbiolspec.TNMI7-0011-2016
2. Narimisa N, Bostanghadiri N, Goodarzi F, Razavi S, Jazi FM. Prevalence of Mycobacterium kansasii in clinical and environmental isolates: a systematic review and meta-analysis. Front Microbiol. 2024;15:1321273. doi:10.3389/fmicb.2024.1321273
3. Pan C, Dong Z, Zhang W, Wang F, Wang H. Severe disseminated Mycobacterium kansasii infection due to autoantibodies against IFN-γ. J Clin Immunol. 2023;43:76–7. doi:10.1007/s10875-022-01350-9
4. Zhang M, Feng M, He JQ. Disseminated Mycobacterium kansasii infection with cutaneous lesions in an immunocompetent patient. Int J Infect Dis. 2017;62:59–63. doi:10.1016/j.ijid.2017.07.029
5. Chen D, Chen Y, Yang S, et al. The additional value of 18F-FDG PET/CT imaging in guiding the treatment strategy of nontuberculous mycobacterial patients. Respir Res. 2024;25:132. doi:10.1186/s12931-024-02873-1
6. Min Z, Amlani M. Pulmonary Mycobacterium kansasii infection mimicking malignancy on the 18F-FDG PET scan in a patient receiving etanercept: a case report and literature review. Case Rep Pulmonol. 2014;2014:973573. doi:10.1155/2014/973573
7. Duan H, Li X, Mei A, et al. The diagnostic value of metagenomic next-generation sequencing in infectious diseases. BMC Infect Dis. 2021;21:62. doi:10.1186/s12879-020-05746-5
8. Li N, Cai Q, Miao Q, Song Z, Fang Y, Hu B. High-throughput metagenomics for identification of pathogens in the clinical settings. Small Methods. 2021;5:2000792. doi:10.1002/smtd.202000792
9. Miao Q, Liang T, Pei N, et al. Evaluation of respiratory samples in etiology diagnosis and microbiome characterization by metagenomic sequencing. Respir Res. 2022;23:345. doi:10.1186/s12931-022-02210-5
10. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(Suppl 2):S231–S240. doi:10.1093/cid/ciy693
11. Xie D, Xian Y, You J, et al. Co-infection pneumonia with Mycobacterium abscessus and Pneumocystis jiroveci in a patient without HIV infection diagnosed by metagenomic next-generation sequencing. Infect Drug Resist. 2021;14:879–888. doi:10.2147/IDR.S292768
12. Shen Y, Li Y, Li H, et al. Diagnosing MonoMAC syndrome in GATA2 germline mutated myelodysplastic syndrome via next-generation sequencing in a patient with refractory and complex infection: case report and literature review. Infect Drug Resist. 2021;14:1311–1317. doi:10.2147/IDR.S305825
13. Chen YP, Yen YS, Chen TY, et al. Systemic Mycobacterium kansasii infection mimicking peripheral T-cell lymphoma. APMIS. 2008;116(9):850–858. doi:10.1111/j.1600-0463.2008.00935.x
14. Yu XJ, Lin YD, Hu P, et al. Imaging findings of vertebral osteomyelitis caused by nontuberculous mycobacterial organisms: three case reports and literature review. Medicine. 2022;101(24):e29395. doi:10.1097/MD.0000000000029395
15. Zhang L, Lin WM, Li H, et al. Hepatic nontuberculous mycobacterial granulomas in patients with cancer mimicking metastases: an analysis of three cases. Quant Imaging Med Surg. 2019;9(6):1126–1131. doi:10.21037/qims.2019.04.10
16. Sun X, Zhang T, Sun H, et al. Disseminated nontuberculous mycobacterial infection with cryptic immunodeficiency mimicking malignancy: a case report. BMC Pulm Med. 2022;22(1):452. doi:10.1186/s12890-022-02227-0
17. Wang CS, Feng SW, Huang LJ, et al. Atypical mycobacterial spondylitis as a challenging differential diagnosis to metastatic disease of the spine: a case report. Eur J Orthop Surg Traumatol. 2013;23(Suppl 2):S135–S139. doi:10.1007/s00590-012-1068-y
18. Chang PH, Chuang YC. Anti-interferon-gamma autoantibody-associated disseminated Mycobacterium abscessus infection mimicking parotid cancer with multiple metastases: a case report. Medicine. 2017;96(39):e8118. doi:10.1097/MD.0000000000008118
19. De Piano F, Savoldi F, Ruju F, et al. A cancer-mimicking diagnosis of peritoneal carcinosis: report of a case of abdominal non-tuberculous mycobacterial infection. ecancermedicalscience. 2018;12:860. doi:10.3332/ecancer.2018.860
20. Batarda SP, Ferro M, Alves CJ, et al. Multidisciplinary approaches and molecular diagnostics in new-onset refractory status epilepticus and nontuberculous mycobacterial CNS infections in the ICU: a case report. Cureus. 2024;16:e76449. doi:10.7759/cureus.76449
21. Li Y, Jiao M, Liu Y, Ren Z, Li A. Application of metagenomic next-generation sequencing in Mycobacterium tuberculosis infection. Front Med Lausanne. 2022;9:802719. doi:10.3389/fmed.2022.802719
22. Wang L, Chen Y, Wang Q, et al. Comparison of molecular testing methods for diagnosing non-tuberculous mycobacterial infections. Eur J Clin Microbiol Infect Dis. 2025;44(1):109–116. doi:10.1007/s10096-024-04981-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.