Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
Chronic Microvascular Complication of Type 1 Diabetes Mellitus and Its Predictors Among Children with Type 1 Diabetes Mellitus in Ethiopia; A Single Center Experience: Ambi Directional Cohort Study
Authors Eshetu K ![]() , Regassa LD
, Regassa LD ![]() , Dehresa M
, Dehresa M ![]() , Genete D
, Genete D ![]()
Received 22 February 2024
Accepted for publication 9 May 2024
Published 23 May 2024 Volume 2024:15 Pages 201—212
DOI https://doi.org/10.2147/PHMT.S456541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Konjit Eshetu,1 Lemma Demissie Regassa,2 Merga Dehresa,3 Desta Genete4
1Department of Pediatrics and Child Health, School of Medicine, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 2Department of Epidemiology and Biostatistics, School of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 3Department of Maternal and Child Health, School of Public Health, College of Health and Medical Science, Haramaya University, Harar, Ethiopia; 4Department of Ophthalmology, School of Medicine, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
Correspondence: Konjit Eshetu, Department of pediatrics and child health, school of medicine, college of health and medical science, Haramaya University, Harar, Ethiopia, Tel +251936807604, Email [email protected]
Introduction: Type 1 diabetes mellitus is the most common pediatric endocrine disorder. Poor glycemic control in diabetes mellitus can result in microvascular complications (retinopathy, neuropathy, and nephropathy). There is no study done in our setting either about prevalence of pediatric type 1 diabetes mellitus or chronic microvascular complication among these patients, which gap this study is expected to fill.
Objective: This study aimed to assess the risk and predictors of chronic microvascular complication of type 1 diabetes mellitus among children with diabetes at Haramaya University Hiwot Fana Compressive Specialized Hospital from September 10, 2021 to January 30, 2023.
Methods: A hospital-based Ambi directional cohort study was conducted. Survival data are described by follow-up time and Kaplan–Meier graph. To determine predictors associated with chronic microvascular complication we used a Poisson regression optimal model selected using the information criterion. All associations are tested at the 95% confidence level and a reported IRR P-value less than 0.05 is declared as a significant association between variables.
Results: A total of 124 children with type 1 diabetes mellitus were followed with total 407.5 years risk time. The overall incidence rate of chronic microvascular complication was 83 per 1000 population per year (95% CI: 59− 116). The median time for detection of microvascular complication was 7 years after diagnosis. Being male with IRR 1.71 (95% CI: 0. 0.81– 3.56), being at pubertal age IRR 1.91 (95% CI: 1.05– 3.48), longer diabetes mellitus duration IRR 1.13 (95% CI: 1.07– 1.28), and poor glycemic control IRR 1.50 (95% CI: 0.46– 4.97) were found to be at higher risk for chronic microvascular complication.
Conclusion: There was high incidence of chronic microvascular complication of diabetes mellitus. Being pubertal age group and more than 3 years duration after diagnosis had statistically significant association with complication.
Keywords: pediatric diabetes mellitus, microvascular complication, Harar
Introduction
The global prevalence of chronic non-communicable diseases is on the rise, with the majority of affected populations in developing countries. Type 1 diabetes mellitus accounts for a large number of cases and is also the most common pediatric endocrine disorder, affecting 1 in 300–500 children younger than 18 years of age. Children with type 1 diabetes mellitus are dependent on exogenous administration of insulin as the major treatment modality. Monitoring and achieving optimal glycemic control is a critical therapeutic goal in the management. Individuals with T1 diabetes mellitus confront serious lifestyle alterations, including the need to monitor their own glucose level, daily injection of insulin, and the need to pay attention to dietary intake.1–4
Morbidity and mortality stem from a constant potential for acute metabolic derangements and from long-term complications. Potential acute complications include the development of hypoglycemia related to insulin excess or hyperglycemic ketoacidosis from insulin deficiency. Poor glycemic control can result in chronic microvascular complications (retinopathy, neuropathy, and nephropathy) in addition to macrovascular complications (cerebrovascular accident, coronary arterial disease, and peripheral vascular disease). However, strict glycemic control can prevent these complications although there may be a risk of hypoglycemia.4,5
Patients with type 1 diabetes diagnosed at less than 15 years of age had 3 times the mortality risk of the general population. Over half of the deaths were related to acute or chronic complications of diabetes. Despite recent improvements in therapy, diabetes-related mortality among children has not declined for 14 years. This finding may be partially attributable to socio-demographic factors influencing access to care, but the remaining mortality may defy available treatment methods. Reducing childhood diabetes mortality rates below the current apparent plateau may require new prevention and/or treatment strategies.5,6
The below-mentioned African published studies showed high prevalence rates of microvascular complication in patients with relatively short duration and at a young age. In these studies, a different degree of severity of retinopathy was observed from none in some studies to 33% of patients on other studies, macro albuminuria from 4% to 5%, hypertension from 8% to 11.7%, and peripheral neuropathy in 5.5% to 8% of patents.7,8
These chronic complications lower the quality of life and cause premature death in patients with diabetes. Clinically evident diabetes-related microvascular complications are rare in childhood and adolescence. However, early functional and structural abnormalities may be present a few years after the onset of the disease, and screening for these complications is important to identify their occurrence at an early stage even though the onset and type of screening for microvascular complications remain debatable.9–11
Long-term microvascular complication of diabetes mellitus has multi-systemic effects and significant impact on quality of life of the child and their caregiver despite being a complication that could be delayed or controlled with appropriate treatment and early screening practice. Sufficient data are lacking regarding pediatric type 1 diabetes mellitus and its long-term microvascular complication both at regional and national levels in Ethiopia.
This study demonstrates the magnitude and determinate factors of long-term microvascular complication of pediatric type 1 diabetes mellitus which is crucial for medical care improvement, development of screening practice, and disease control. In addition there is scarcity of literature and consciences when to initiate screening tests for detection of these complications among pediatric patients with DM. This study will address this gap by determining time to development of complication from diagnosis.
Methods and Materials
Study Design, Setting, and Period
An institutional-based Ambi directional cohort study was conducted at Haramaya University Hiwot Fana Compressive Specialized Hospital in Harari regional state. HUHFCSH was established in 1935 and is located in Harar city, Harari region, eastern Ethiopia. HFCSH is a teaching hospital serving as a referral hospital for the eastern part of the country.
The Pediatric and Child Health Department provide a weekly diabetic follow-up service. The clinic is attended by a pediatric nurse, year 1 resident, year 3 resident, and consulting pediatrician. Currently a total of 132 known diabetic patients are on monthly follow up at the clinic. The patients are provided with free insulin syringe, and regular and neutral protamine hagedorn insulin on each monthly follow up. Upon initial diagnosis they would be provided with a free glucometer for monitoring and come to the clinic with a monthly diary of random blood sugar record done at least 2 times per day. The study population were observed from the individual patient’s time of first diagnosis of diabetes mellitus to the end of the data collection period or diagnosis of one of the microvascular complication, whichever comes first, and the study was conducted from September 10, 2021 to January 30, 2023.
Study Participants and Eligibility Criteria
All pediatric patients aged less than 18 years diagnosed with type 1 diabetes mellitus and attending diabetic clinic, follow up for at least 1 year were included in the study after attaining informed and written consent. Diabetic patients with an incomplete medical record of follow up and newly diagnosed type 1 diabetes mellitus patients who are on follow up for less than 1 year were excluded from the study.
Sample Size Determination
Since the total number of pediatric patients attending the diabetic clinic is 132, all patients on follow up fulfilling inclusion and exclusion criteria will be included in the study.
Data Collection Methods
A structured data collection tool was be prepared which included socio-demographic characteristics of the patients, type of insulin used, method of insulin storage, injection and degree of primary caregiver involvement by interviewing the primary caregiver for children less than 12 years old and the children themselves who were above 12 years. In addition, secondary data collection from medical record review was done. Two BSC nurses attending the pediatric diabetic clinic and 2 pediatric residents were trained on the data collection tool and involved in data collection.
The assessment on predictors of chronic microvascular complication was performed during the clinic visit. On first arrival of the child to the diabetes mellitus clinic they were interviewed by validated structured questionnaire on socio-demographic characteristics.
Weight and height measurement was taken to calculate weight for height for children under 5 years and body mass index for children 5 years and above. Then standardized for age and gender using the WHO Z score curve to classify the child as severe acute malnourished, moderately malnourished, or well nourished. To assess blood pressure, the patient sat down for a few minutes (for rest) while being interviewed for any new compliant in the preceding month and then three measurements with a 5–10-minute interval, using an aneroid sphygmomanometer, were done and average of the 3 measurements was taken. Blood pressure was categorized according to BP tables from the fourth report of the National High Blood Pressure Education Program working group on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents, using age and height percentiles, with normotensive defined as blood pressure between 5th and 90th percentiles. Elevated hypertension defined systolic blood pressure and/or diastolic blood pressure between 90th to 95th percentiles, and stage 1 hypertension systolic blood pressure and/or diastolic blood pressure between 95th percentile and 95th percentile plus 12 mmHg. Stage 2 hypertension if systolic blood pressure and/or diastolic blood pressure greater than 95th percentile plus 12 mmHg. Hypotensive if systolic blood pressure and/or diastolic blood pressure was less than 5th percentile.
After compilation of the above evaluation a pupillary dilator was applied on both eyes (to facilitate well visualizing during fundoscopic examination) and rested for 30 minutes, Then they were taken to the ophthalmologic clinic accompanied by hospital runners where they were examined by ophthalmologist through dilated pupils using fundus photography once in the study period for assessment of diabetic retinopathy and its grade. The result were attached to the patient's medical record.
On second follow up during the observation period, after parents were advised how to take midstream urine, 5–10 mL of urine was collected in a sterile urine cup and sent to the pediatric laboratory where macro albuminuria was assessed by semi-quantitative urine dipstick testing (bright urine analysis reagent strip) and additionally on the next 2 follow-up visits too. The result was be taken as positive if trace and above on urine dipstick with urine specific gravity between 1.015 and 1.025. Screening was not performed if the child has urinary tract infection, hematuria, acute febrile illness, short-term pronounced hyperglycemia, uncontrolled hypertension, and heart failure. Positive dipstick has sensitivity of 100% and specificity of 82% in detection of proteinuria.12
On the subsequent visit the patients were sent to the center laboratory where a blood sample was taken by a laboratory professional and then chemistry tests of serum creatinine, BUN, and cholesterol level was done by chemistry machine DIRUI DR-7000D with regular calibration and Hemoglobin A1c was determined by hormone machine FINECARE with regular calibration.
On the third visit after routine follow-up evaluation the patients were taken to the neurologic clinic where they were evaluated by a pediatrician for features of peripheral neuropathy using the Douleur Neuropathique 4 questions (DN4)-questionnaire. The neurologic evaluation was done with thorough history and physical examination and the finding was scored out of 10 based on the DN4 checklist; if the score was 4 and above out of 10, it was taken as positive for peripheral neuropathy.
Operational Definitions
- Conventional insulin regimen: defined as the administration of 2 injections of insulin per day as a combination of regular short-acting and intermediate-acting insulin before breakfast and dinner.
- Pre pubertal age: child with chronological age less than 10 years.
- Pubertal age: child with chronological age greater than or equal to 10 and less than 14 years.
- Post pubertal age: child chronological age greater than or equal to 14 years.
- Follow-up time: all children diagnosed with diabetes mellitus and on follow up at the diabetic clinic and followed from September 1, 2021 to January 30, 2023.
- Event: having chronic microvascular complication will be defined by having one or more of the following events during the follow-up period.
- Diabetic nephropathy: macro albuminuria which is defined when urine protein dipstick +2 and above.
- Diabetic neuropathy: defined by history and clinical examination finding of tingling sensation, burning, numbness, stock and glove anesthesia, decreased pins or needles sensation, absent ankle reflex on extremities, dizziness or fainting, urinary retention, and excessive sweating.
- Hypertension: defined as having 3 elevated or above systolic or diastolic blood pressure for patients’ age, sex, and height.
- Diabetic retinopathy: defined as dilated eye examination finding of non-proliferative or proliferative retinal vascular change at any stage diagnosed by an ophthalmologist.
- Hyperlipidemia: defined as LDL cholesterol more than 190 mg/dL or more than 160 mg/dL with clinical symptoms.
- DKA: defined as the presence of ketones in the urine, a history of an altered level of consciousness of the patient or coma at the time of assessment, or an admission to hospital.
- Hypoglycemia: defined as the presence of three or more episodes of the following symptoms – sweating, hunger, tingling around the mouth, tremor, anxiety, weakness, headache, visual disturbances, slurred speech, vertigo and dizziness mental confusion, coma, and convulsion, with these symptoms being relieved by giving the child sugar-containing foods.
- Good glycemic control: mean HbA1c level ≤7.5%.
- Poor glycemic control: mean HbA1c level >7.5%.
- Pediatric age: according to AAP age <18 years.
Data Quality Control and Management
A standardized and properly designed data collection tool was utilized in the data collection process. The data collection tool was pretested before initiation of data collection, and the pretest results were not included in the study. Data collectors received training on the data collection tool. The principal and co-investigators supervised the data collection and each data point was checked for accuracy and completeness before data entry.
Data Processing and Analysis
The data were entered into Excel, cleaned there, and exported to STATA 14 software which was utilized for analysis. Further data cleaning was performed to check for outliers, missed values, and any inconsistencies before the data was analyzed using the software.
Descriptive statistics on socio-demographic data, insulin type, storage, and magnitude of chronic microvascular complication characteristics are described in proportion. Age at diagnosis, duration of disease, BMI, blood pressure, frequency of DKA, serum creatinine, serum cholesterol, HgA1c, and urine protein were described in terms of mean. Using survival analysis we calculated the incidence rate of chronic complications of type 1 diabetes mellitus, which is summarized in terms of nutritional status, primary caregiver educational status, availability of follow-up kit, duration of disease diagnosis, and glycemic control. Survival data are described by follow-up time and Kaplan–Meier graph. For determination predictors associated with chronic microvascular complication, fitness of model was done using Akaike’s information criterion and Bayesian information criterion and Poisson regression was done. All associations will be tested at 95% confidence level and p-value less than 0.05 will be declared as a significant association between variables.
Ethical Considerations
Ethical clearance was acquired from institutional health research ethics review committee (IHRERC) of Health and Medical Sciences, Haramaya University (Ref. No. IHRERC/160/2022) and the study complies with the Helsinki Declaration. Informed, voluntary, written, and signed consent was obtained from the parents or legal guardian of the child, and in addition assent was obtained from children above 12 years old for the face-to-face interview and laboratory sample submission. Data were treated with most confidentiality and used for study purposes only. Informed, voluntary, written, and signed consent was acquired from the hospital administration to acquire data from the patients and their medical record.
Results
Socio-Demographic Characteristics
During the follow-up period of 1 year and 6 months a total of 124 children with diagnosis of type 1 diabetes mellitus were observed. All of the patients were on mixed type of insulin with regular and neutral protamine hagedorn insulin. All of the patients were adherent to their monthly follow up and there were no drop outs during the study period. Among the patients 75 (60%) came from a rural area of catchment location. Regarding age distribution, the majority of the patients, 52 (41.9%), are at pubertal age group. The majority of the patients did not have family history of diabetes mellitus among first or second-degree relatives except 16 (12.9%) of the study population. The mean duration since the diagnosis of diabetes mellitus was 3 years and 2 months. Regarding educational status of the primary caregivers, 69 (55.6%) were unable to read and write and 27 (21.7%) were only able to read and write, and the remaining 28 (22%) had more than primary level education (Table 1).
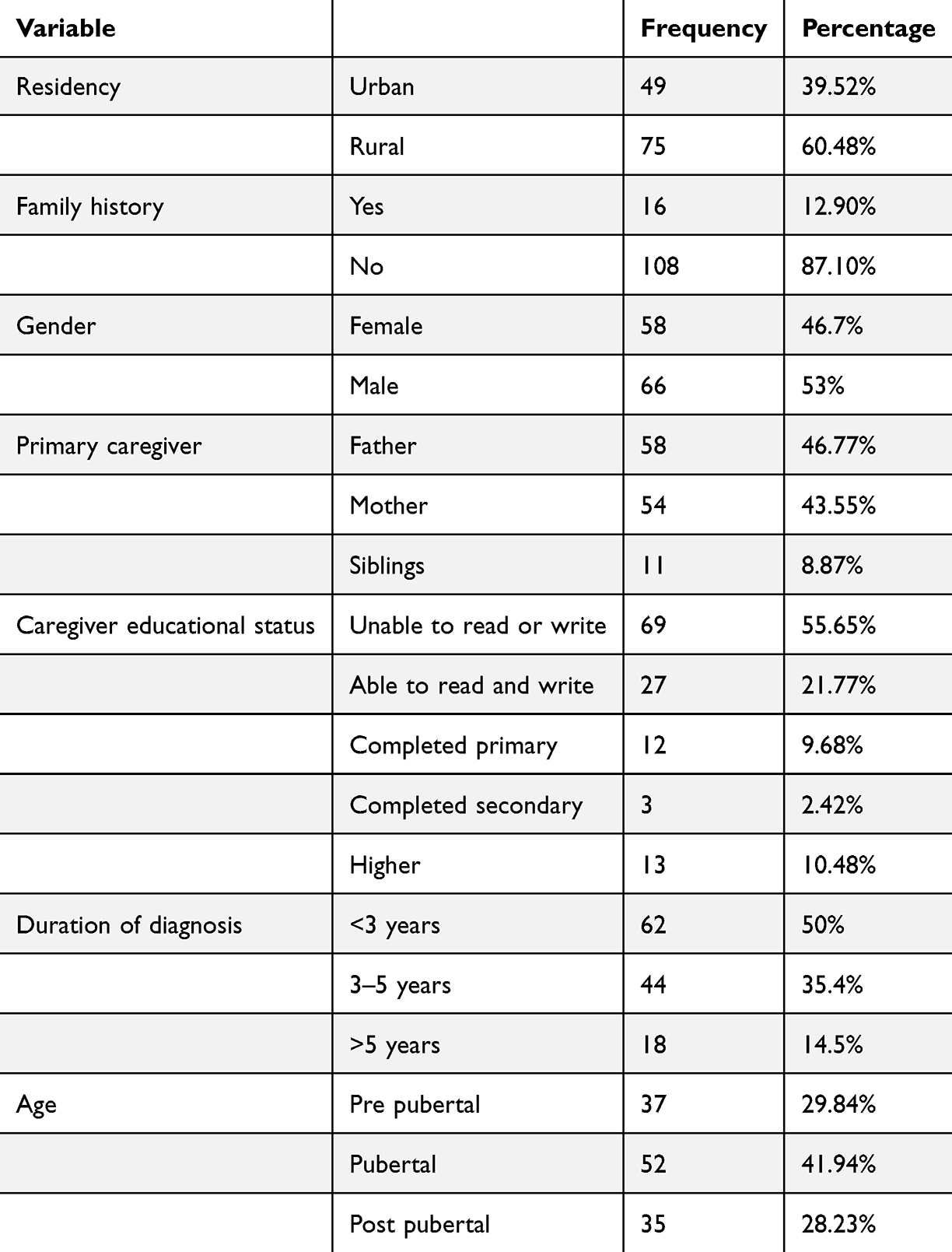 |
Table 1 Sociodemographic Characteristics of Patients with Chronic Microvascular Complication of Type 1 Diabetes Mellitus among Pediatric Patients Attending Diabetic Clinic at Haramaya University Hiwot Fana Compressive Specialized Hospital, Harar Town, Ethiopia, 2023 |
Clinical Characteristics
All of the patients use mixed type of insulin with NPH and regular insulin. The majority of the patients, 73 (58.8%), store the insulin in an underground digging hole under a shaded part of their living area, only 49 (39.5%) of the patients use a refrigerator as the storage mechanism. Insulin monitoring glucometer is provided by the hospital, and 114 (91%) of the patients have functional monitoring equipment during the study period. Of all observed patients, 34 (26%) of them were admitted to the hospital at least once for diagnosis and treatment of diabetic ketoacidosis in the last 6 months (Table 2).
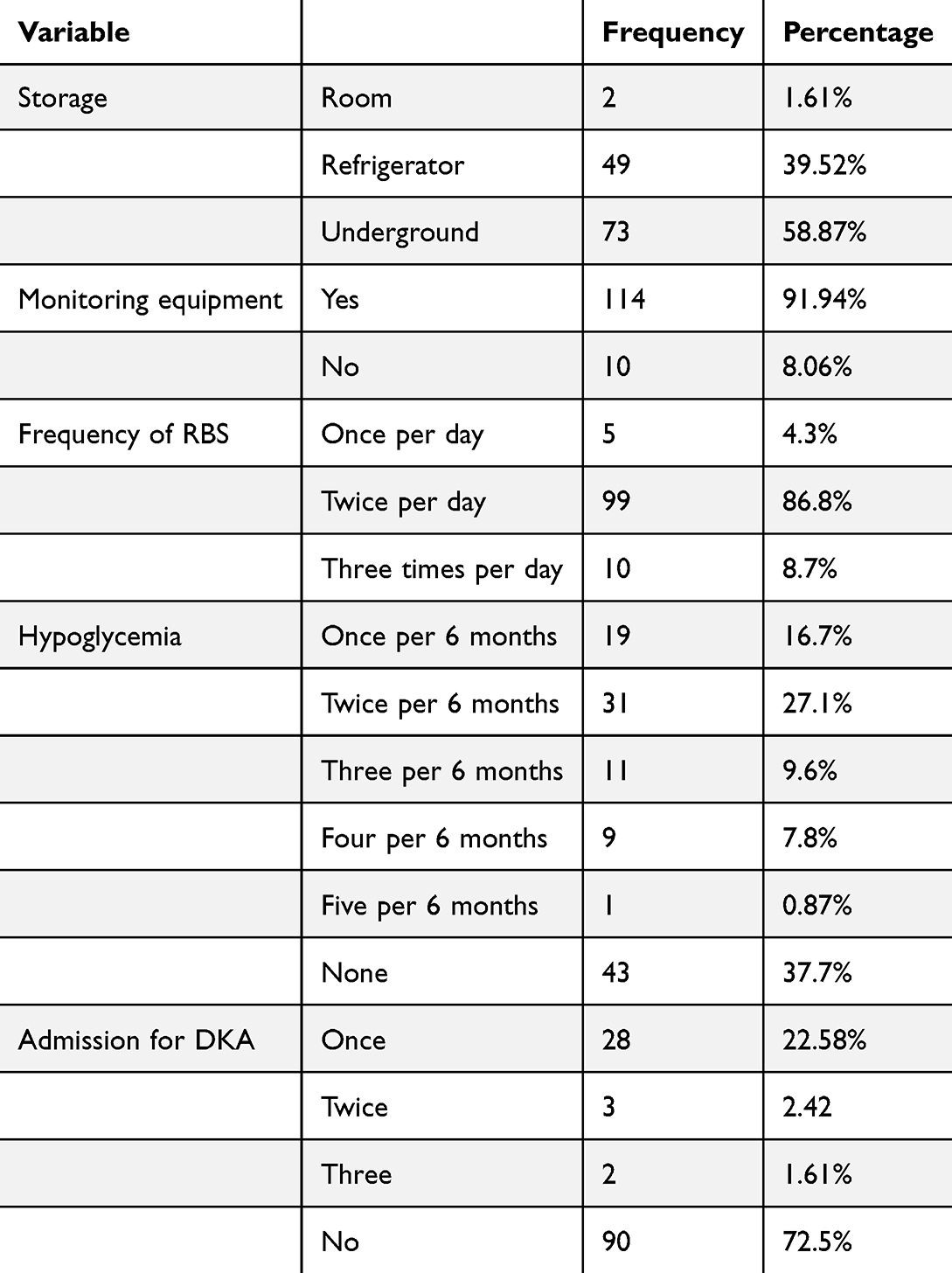 |
Table 2 Insulin Utilization and Monitoring of Patients with Chronic Microvascular Complication of Type 1 Diabetes Mellitus among Pediatric Patients Attending Diabetic Clinic at Haramaya University Hiwot Fana Compressive Specialized Hospital, Harar Town, Ethiopia, 2023 |
Incidence of Chronic Microvascular Complication of Type 1 Diabetes Mellitus
Long-term glycemic control was determined by the mean HgA1C during the observation period which was determined at least 3 times. Among the observed patients 103 (83%) had poor long-term glycemic control with mean HgA1C more than 7.5%. The mean HgA1C level was 10.8±2.5 mg/dL.
Among all of the study population, 34 (27.4%) of the patients had at least one of the major chronic microvascular complications of type diabetes mellitus. The overall incidence rate of chronic microvascular complication was 83 per 1000 population per year (95% CI: 59−116 per 1000 population per year). The incidence was highest in those with poor glycemic control with 87 per 1000 person years of observation. In addition microvascular complication was observed more in children with malnutrition with incidence of 130 per 1000 person years of observation in severe acute malnutrition and 74 per 1000 person years in moderate acute malnutrition (Table 3).
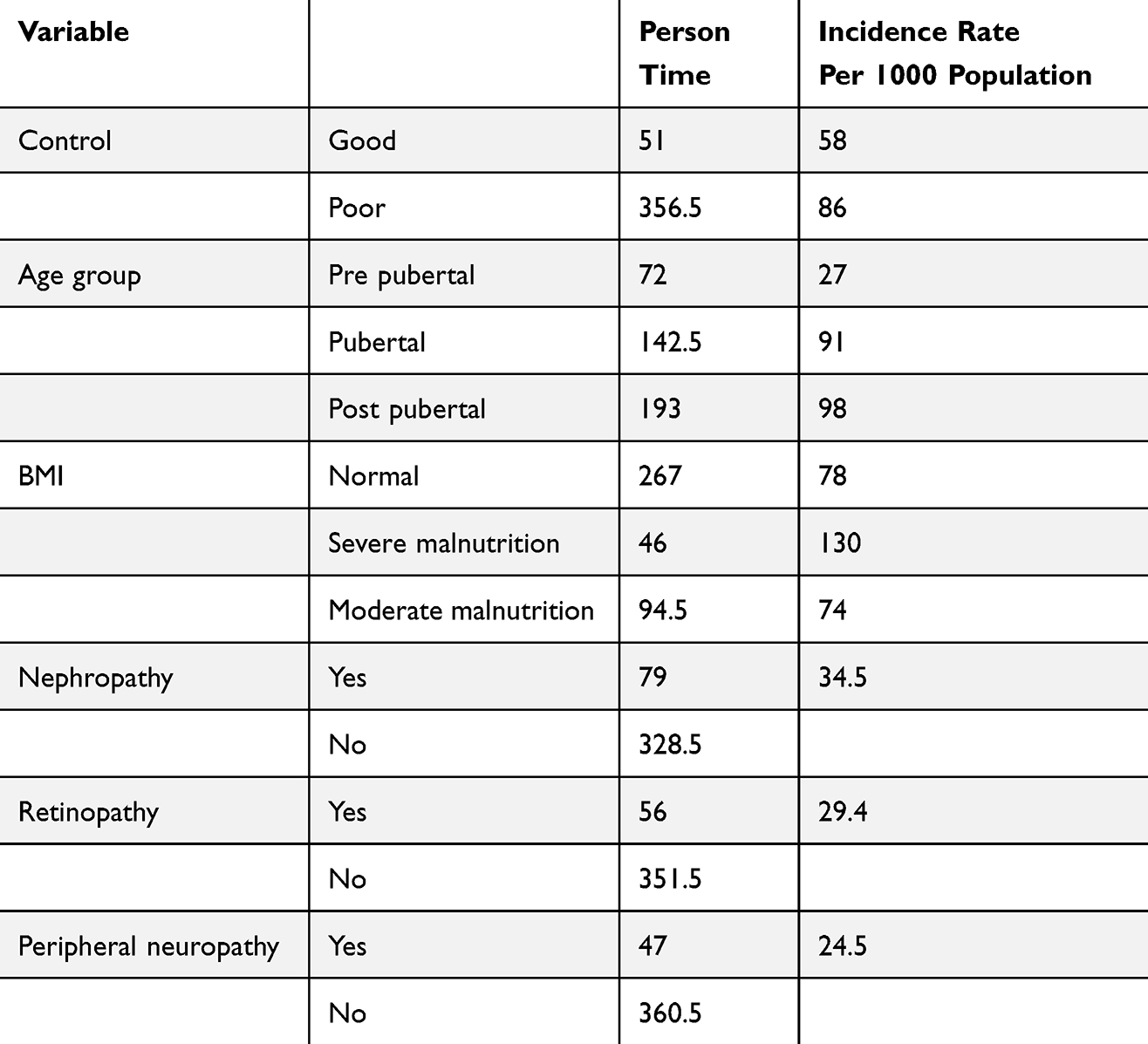 |
Table 3 Incidence of Microvascular Complication in Type 1 Diabetes Mellitus among Pediatric Patients Attending Diabetic Clinic at Haramaya University Hiwot Fana Compressive Specialized Hospital, Harar Town, Ethiopia, 2023 |
On urine dipstick examination for the presence of macro albuminuria, 10 (11.2%) of the patients had clinically significant proteinuria of +2 and above. Among the study population 7 (5%) had hyperlipidemia with cholesterol level more than 190 mg/dL and one child had stage 1 hypertension with concomitant hyperlipidemia. One child had stage 1 hypertension who also had significant albuminuria. Two other patients had both peripheral neuropathy and retinopathy (Table 3).
Time to Microvascular Complication
A total of 124 patients were observed for 1 year and 6 months with 407.5 total years at risk. Among these, 90 of the patients were censored at the end of the observation because they did not develop the event interest. None of the paints were lost to follow up during the study period. There was no incident of death during the observation period.
The incidence rate of chronic microvascular complication was 83 per 1000 population per year (95% CI: 59−116 per 1000 population per year). The median time for detection of complication was 7 years after diagnosis, but 25% of the patients were detected to have complication after 5 years of diagnosis and 75% of the population had event of interest after 8 years of diagnosis.
Among the microvascular complication, neuropathy was the earliest to develop with median time to complication of 5 years, while diabetic retinopathy was the last to develop with median time of 7 years.
Predictors of Chronic Microvascular Complication
For determination of covariates associated with chronic microvascular complication, fitness of model was done using Akaike’s information criterion and Bayesian information criterion. Fitted and empty model was compared for Poisson regression and zero inflated Poisson regression with AIC and BIC values of 142.8019/154.0831 and 148.1813/167.9233 for each model respectively. We took the mode with smallest value and good fit. In addition, the deviance was done using state software which was 131.3 divided by 118 (degrees of freedom) which was 1.1, since the deviance was close to 1, evidencing a better model.
When we see determining factors for chronic complication, the risk of having chronic microvascular complication was 1.6 (IRR 95% CI: 0.79–3.25) times at increased risk among male patients in comparison with female patients. The risk of detection of microvascular complication was 2.6 (IRR 95% CI: 1.59–4.47) times higher at pubertal age than patients in pre pubertal age group.
In relation to residential area, those patients residing in a rural area were 1.07 (IRR 95% CI: 0.54–2.12) times at increased risk for complication than those residing in an urban area. The majority of our patients had poor glycemic control, who were 2.10 (IRR95% CI: 0.64–6.89) times more at increased risk for complication than those patients with good glycemic control.
In another control related issue for those patients who had admission for diabetic ketoacidosis, their risk of complication was 1.38 (IRR 95% CI: 0.69–2.80) times higher than those patients without history of admission. Another crucial predictor factor was duration of diagnosis of type 1 diabetes mellitus. Those patients with more than or equal to 3 year duration of diagnosis had 2.39 (IRR 95% CI: 1.63−3.53) times increased risk of microvascular complication than patients with shorter duration of diagnosis.
In general, increased risk for microvascular complication was observed among patients who were male in gender, rural resident, poor glycemic control, and had history of admission for DKA. Among the predicting variables, statistically significant association with complication was observed among patients with pubertal age group as 1.91 (AIRR 95% CI: 1.05−3.48) and duration of diabetes mellitus more than or equal to 3 years as 1.13 (AIRR 95% CI: 1.07–1.28) (Table 4).
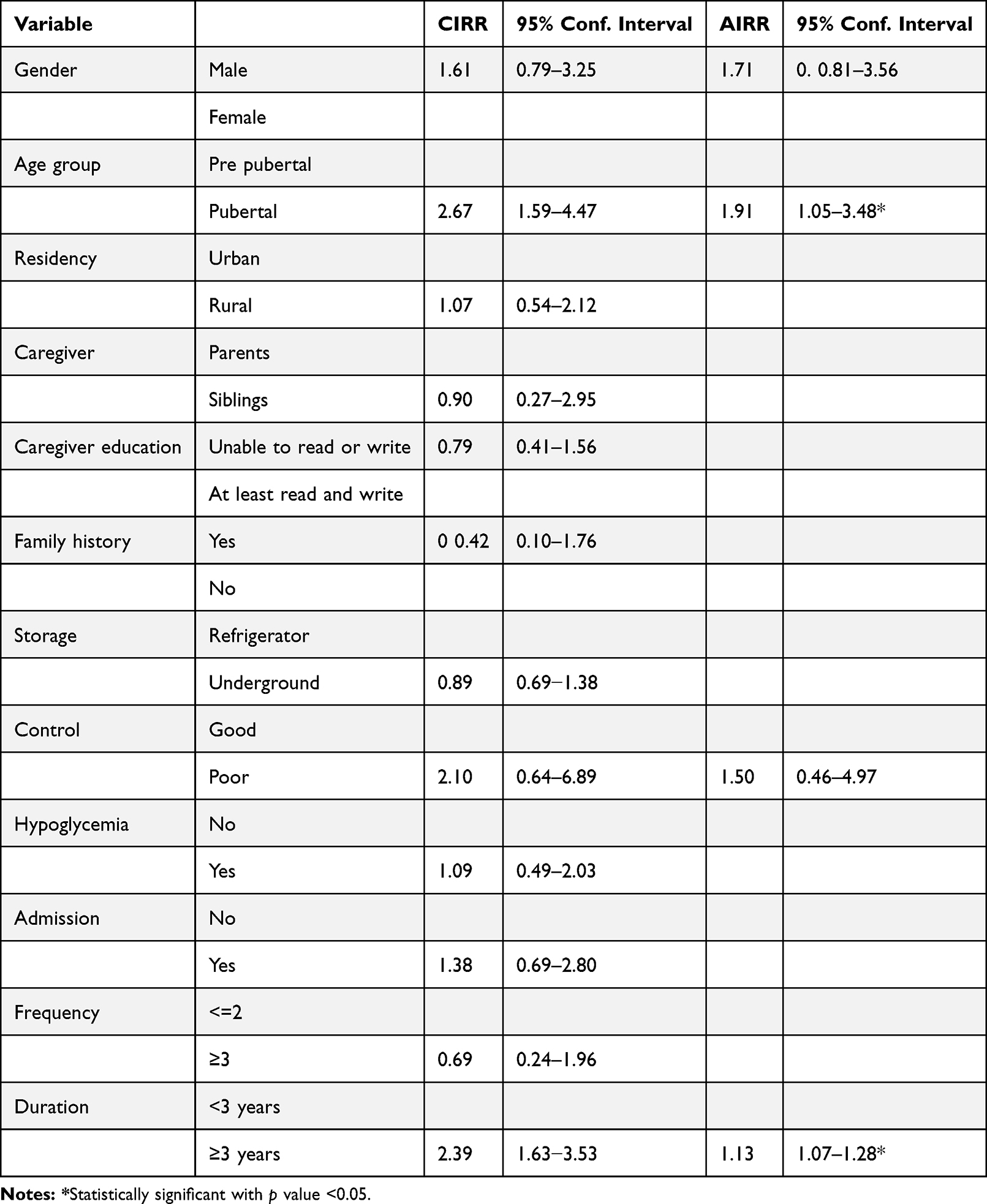 |
Table 4 Incidence Rate Ratio for Patients with Chronic Microvascular Complication of Type 1 Diabetes Mellitus among Pediatric Patients Attending Diabetic Clinic at Haramaya University Hiwot Fana Compressive Specialized Hospital, Harar Town, Ethiopia, 2023 |
Discussion
In our study the incidence of type 1 diabetes mellitus chronic microvascular complication among pediatrics was 83 per 1000 population per year (IRR 95% CI: 59−116). This may question adherence to treatment, or community awareness about self-care.
During our follow-up period 83% of the study population had poor glycemic control, which was comparable with Nigerian study by Chinwe et al 2021 in which 78.9% of the population had poor control, while better than Msekandiana et al 2020 in which 97.5% and Ahmed et al 2020 in which 90% had poor control. This is in contrast to the Indian study by Sudhanshu et al 2019 and the Turkey study by Simsek et al 2013 that had better control than our setting with 71% and 69.4% of study population having poor control respectively.5,13,14
When we see specific complication, 9.7% of the study population were detected to have mild nonproliferative type of retinopathy The incidence of retinopathy was significantly lower than Ahmed et al 2020 which is 33% and Msekandiana et al 2020 which was 22.2%. This difference is observed due to the higher number of patients with poor long-term glycemic control in the last studies. While it is higher than study according to Sudhanshu et al 2019 which was 6.2%, and Simsek et al 2018 which was 2.2%. This difference is due to better long-term glycemic control among patients in these two studies and population difference as the last 2 studies are from India and Turkey. This finding indicates the significant role of tight glycemic control in the prevention of complication.14,15
Diabetic kidney disease evidenced by macro albumin on urine dipstick test was detected in 11.2% of our patients, being the most commonly identified microvascular complication which was comparable with Simsek et al 2018 (8.3%). But it was higher than Kamaledeen et al 2018 and Msekandiana et al 2020 which was 1.1% and 4.8% respectively. These difference was observed due to longer duration of follow up and larger number of sample size in our study than the above study population. Also, our finding is significantly lower than Ahmed et al 2020 in which 33% had nephropathy. This difference is observed due to 90% of their study population had poor glycemic and 94% of their study population were pubertal age group which is different from our study population. According to David R. Weber and Nicholas Joseph, 2020 tight glycemic control will delay the progression of macro albuminuria and slow the progression of diabetic nephropathy.15–17
Being pubertal age group was significantly associated with microvascular complication in our study, which is probably due to behavioral factors affecting adherence, increased demand of insulin with age, and prolonged exposure to hyperglycemia. In line with this finding, children at pubertal age group had higher HgA1C level according to Simsek et al 2013, Ahmed et al 2020, and Msekandiana et al 2020.18,19
In the study by Sudhanshu et al 2018, during a 4-year period follow up period, 164 patients were eligible for microvascular complication screening. There was no significant difference in the frequency of any microvascular complication in urban vs rural and higher vs lower education-class patients, which aliens with our study finding in which residency did not have statistically significant impact on glycemic control.20
In addition, in our study statistically significant association was detected between microvascular complication and duration of diagnosis more than 3 years with incidence risk ratio of 1.13 (IRR 95% CI: 1.07–1.28). This was supported by Chinwe et al 2021 and Simsek et al 2013, in which duration diabetics was strong determinate of both glycemic control and development of complications special retinopathy and nephropathy.19,20
According to Sudhanshu et al 2019, patients with hypertension had significantly higher mean age 28.8 (6.6) vs 17.8 (7.3) years, P<0.001 and mean diabetes duration 16.1 (6.3) vs 8.5 (5.7) years, P<0.001 versus those who did not. In our study we had insignificant number of hypertension which is due to short duration since diagnosis of diabetes mellitus.
Conclusion
There was high magnitude of chronic microvascular complication of type 1 diabetes mellitus in our study, with a total of 34 (27.4%) patients detected to have at least one of the complications. The overall incidence rate of chronic microvascular complication was 83 per 1000 population per year. The specific complications were diabetic nephropathy, neuropathy, and retinopathy with incidence rate of 34.5, 24.5, and 29.4 per 1000 population. The median time for detection of microvascular complication was 7 years after first diagnosis of DM. The major identified determinate factor of microvascular complication were being male gender, pubertal age group, longer diabetes mellitus duration, poor glycemic control, and frequent admission for DKA, while being pubertal age group and more than 3 years duration of diagnosis had statistically significantly association with complication. In addition, the majority of the patients had poor glycemic control despite having comparable socio-demographic characteristics with other settings so we recommend further in-depth study to identify the root cause and possible population-based solution of poor glycemic control.
Acknowledgments
We would like to express our gratitude to all health care professional staff working at the pediatric diabetes mellitus follow-up clinic during the observation period and our coworkers who give us continuous support and constructive ideas from beginning to end of this thesis. We also forward our gratitude to Haramaya University for the opportunity, support, and availing the final thesis on the university website for accessibility. This paper is based on the epidemiology thesis of Konjit Eshetu, Lemma Demissie, and Merga Dehresa. It has been published on the institutional website: http://ir.haramaya.edu.et//hru/handle/123456789/7219
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Ahmed H, Elshaikh T, Abdullah M. Early diabetic nephropathy and retinopathy in patients with type 1 diabetes mellitus attending Sudan childhood diabetes centre. J Diab Res. 2020;2020:7181383. doi:10.1155/2020/7181383
2. Chinwe FO, Ugo NC, Chikosolu YO, Ugochi MI. Sociodemographic determinants of glycaemic control among children with type 1 diabetes in South Eastern Nigeria. PAMJ. 2021;38:1.
3. Majaliwa ES, Munubhi E, Ramaiya K, et al. Survey on acute and chronic complications in children and adolescents with type 1 diabetes at Muhimbili national hospital in Dar es Salaam, Tanzania. Diabetes Care. 2007;30:2187–2192. doi:10.2337/dc07-0594
4. Msekandian A, Chigayo G, Chiume S, et al. Complications and glycaemic control of type 1 diabetes mellitus amongst Children Aged 5 to 19 years attending diabetic clinic at Kamuzu central hospital in Malawi. Int J Diabetes Clin Res. 2020;7:117.
5. Ngwiri T, Were F, Predieri B, Ngugi P, Iughetti L. Glycemic control in Kenyan children and adolescents with type 1 diabetes mellitus. Int J Endocrinol. 2015;2015:761759. doi:10.1155/2015/761759
6. DiLiberti JH, Lorenz RA. Long-term trends in childhood diabetes mortality: 1968–1998. Diabetes Care. 2001;24(8):1348–1352. doi:10.2337/diacare.24.8.1348
7. Simsek DG, Aycan Z, Özen S, et al. Diabetes care, glycemic control, complications, and concomitant autoimmune diseases in children with type 1 diabetes in Turkey: a multicenter study. J Clin Res Pediatr Endocrinol. 2013;5:20–26. doi:10.4274/Jcrpe.893
8. Sudhanshu S, Nair VV, Godbole T, et al. Glycemic Control and long-term complications in pediatric onset type 1 diabetes mellitus: a single-center experience from Northern India. Indian Pediatr. 2019;56:191–195. doi:10.1007/s13312-019-1497-3
9. Shimelis D, Shimelis D, Abebe W. Prevalence of diabetes mellitus in 7-12 years old school children presenting to department of pediatrics and child health, tikur anbessa specialized Teaching Hospital, Addis Ababa, Ethiopia. Ethiopian Med J. 2017;55(3):43–47.
10. Cooke DW, Plotnick L. Type 1 diabetes mellitus in pediatrics. Pediatr Rev. 2008;29:374–384. doi:10.1542/pir.29.11.374
11. Daneman D. Early diabetes-related complications in adolescents. Hormone Res Paediatrics. 2005;63:75–85. doi:10.1159/000083692
12. Kamaleldeen EB, Mohammad HA, Mohamed EF, Askar AG. Microvascular complications in children and adolescents with type 1 diabetes mellitus in Assiut governorate Egypt. Egyptian Pediat Assoc Gazette. 2018;66:85–90. doi:10.1016/j.epag.2018.10.003
13. Mariye T, Bahretb D, Tasew H, et al. Determinants of Poor Glycemic Control among Diabetes mellitus in Public Hospitals of the Central Zone. In: Unmatched Case-Control Study. Tigray, North Ethiopia: Endocrinol Metab; 2020.
14. Noorani M, Ramaiya K, Manji K. Glycaemic control in type 1 diabetes mellitus among children and adolescents in a resource limited setting in Dar es Salaam - Tanzania. BMC Endocr Disord. 2016;16:29. doi:10.1186/s12902-016-0113-y
15. Svensson M, Eriksson JW, Dahlquist G. Early glycemic control, age at onset, and development of microvascular complications in childhood-onset type 1 diabetes: a population-based study in northern Sweden. Diabetes Care. 2004;27:955–962. doi:10.2337/diacare.27.4.955
16. Weber DR, Jospe N. Nelson Textbook of Pediatrics, Twenty-First Edition ISBN: 978-0-323-52950-1: Type 1 Diabetes Mellitus (Immune Mediated). Elsevier Inc; 2020.
17. Nathan DM; Nathan DIABETES MELLITUS; DCCT/EDIC Research Group. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. 17. Diabetes Care. 2014;37(1):9–16. PMID: 24356592; PMCID: PMC3867999. doi:10.2337/dc13-2112
18. Morgan E, Black CR, Abid N, Cardwell CR, McCance DR, Patterson CC. Mortality in type 1 diabetes diagnosed in childhood in Northern Ireland during 1989‐2012: a population‐based cohort study. Pediatric Diabetes. 2018;19(1):166–170. doi:10.1111/pedi.12539
19. Dayan CM, Besser REJ, Oram RA, et al. Preventing type 1 diabetes in childhood. Science. 2021;373(6554):506–510. PMID: 34326231. doi:10.1126/science.abi4742
20. Kanta A, Lyka E, Koufakis T, Zebekakis P, Kotsa K. Prevention strategies for type 1 diabetes: a story of promising efforts and unmet expectations. Hormones. 2020;19(4):453–465. doi:10.1007/s42000-020-00207-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.