Back to Journals » Infection and Drug Resistance » Volume 16
Chlamydia psittaci Pneumonia-Induced Pulmonary Thrombosis: A Case Report
Received 8 September 2023
Accepted for publication 26 October 2023
Published 6 November 2023 Volume 2023:16 Pages 7063—7069
DOI https://doi.org/10.2147/IDR.S435246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Changquan Fang,1 Limin Xu2
1Department of Pulmonary and Critical Care Medicine, Huizhou Central People’s Hospital, Huizhou, Guangdong Province, Peoples’ Republic of China; 2Department of Geriatrics, Huizhou First People’s Hospital, Huizhou, Guangdong Province, People’s Republic of China
Correspondence: Limin Xu, Department of Geriatrics, Huizhou First People’s Hospital, No. 20 Sanxin South Road, Huicheng District, Huizhou City, Guangdong Province, 516000, People’s Republic of China, Tel +86 136-3199-9563, Email [email protected]
Abstract: Chlamydia psittaci pneumonia frequently leads to various extrapulmonary complications; however, reports of C. psittaci-pneumonia complicated by pulmonary thrombosis are uncommon. We report a case of severe C. psittaci pneumonia in a patient with a history of poultry contact and clinical manifestations including hyperpyrexia, dyspnea, and respiratory failure, which necessitated tracheal intubation for assisted ventilation. C. psittaci in bronchoalveolar lavage fluid was detected with metagenomic next-generation sequencing. Following targeted antibiotic therapy, the fever subsided, although dyspnea persisted without significant improvement, and chest pain developed. Compared to previous measurements, the D-dimer level increased, and CT pulmonary angiography revealed thromboses in the pulmonary artery trunk and left pulmonary artery. The symptoms improved after anticoagulant treatment, and the patient was discharged subsequently. This study suggests that C. psittaci infection may be associated with the formation of pulmonary thrombosis. Additional clinical data are required to support this inference. Following targeted antibiotic therapy, if persistent dyspnea, chest pain, and increased D-dimer level are present, pulmonary thrombosis should be considered, and pulmonary artery angiography can confirm the diagnosis.
Keywords: Chlamydia psittaci, pneumonia, pulmonary thrombosis, metagenomic next-generation sequencing
Introduction
Chlamydia psittaci infection induces a systemic disease that can affect multiple organ systems.1 Characterized by strong pathogenicity, C. psittaci infection can lead to lung involvement and injuries to other extrapulmonary organs. The frequently reported extrapulmonary complications include hepatitis, endocarditis, and meningitis, among others,2,3 whereas concurrent pulmonary thrombosis is a rare complication. Pulmonary thrombosis constitutes a group of diseases caused by various emboli that obstruct the pulmonary arterial system, with pulmonary thrombosis being the most prevalent. Factors that are often related to the occurrence of pulmonary thrombosis include trauma, surgery, and malignant tumors, among others, whereas infection-induced cases are less common.4 The non-specific clinical symptoms of C. psittaci pneumonia, the complexity of routine diagnostic methods, and a low incidence rate5 have contributed to the rarity of reports of C. psittaci pneumonia with pulmonary thrombosis. Herein, we report for the first time a case of C. psittaci pneumonia with acute pulmonary thrombosis diagnosed by metagenomic next-generation sequencing (mNGS), with the aim to enhance clinicians’ understanding of this disease.
Case Presentation
The patient was a 47-year-old woman who was hospitalized on May 16, 2023, due to fever and cough with breathing difficulty. A week prior to admission, she developed a fever of unknown origin (maximum temperature 41.0°C) which was associated with headaches, chills, poor appetite, fatigue, and paroxysmal minimally productive cough with white sputum. Initial treatment at a local hospital included intravenous antibiotic therapy with ceftriaxone (2.0 g q.d.) for 3 days. However, the high fever persisted, and breathing difficulty worsened. Upon arrival at our emergency department, a chest CT revealed multiple patchy exudations in both lungs, along with large consolidated shadows in the right lower lung (Figure 1A–C). Arterial blood gas analysis (FiO2 of 50%) showed a pH of 7.513, PO2 67.0 mmHg, PCO2 32.1 mmHg, HCO3 25.8 mmol/L. Therefore, the patient was hospitalized with a diagnosis of severe community-acquired pneumonia. The patient had no history of underlying diseases, atrial fibrillation, thrombosis, long-term bed rest, surgery, tumors, and smoking or drinking.
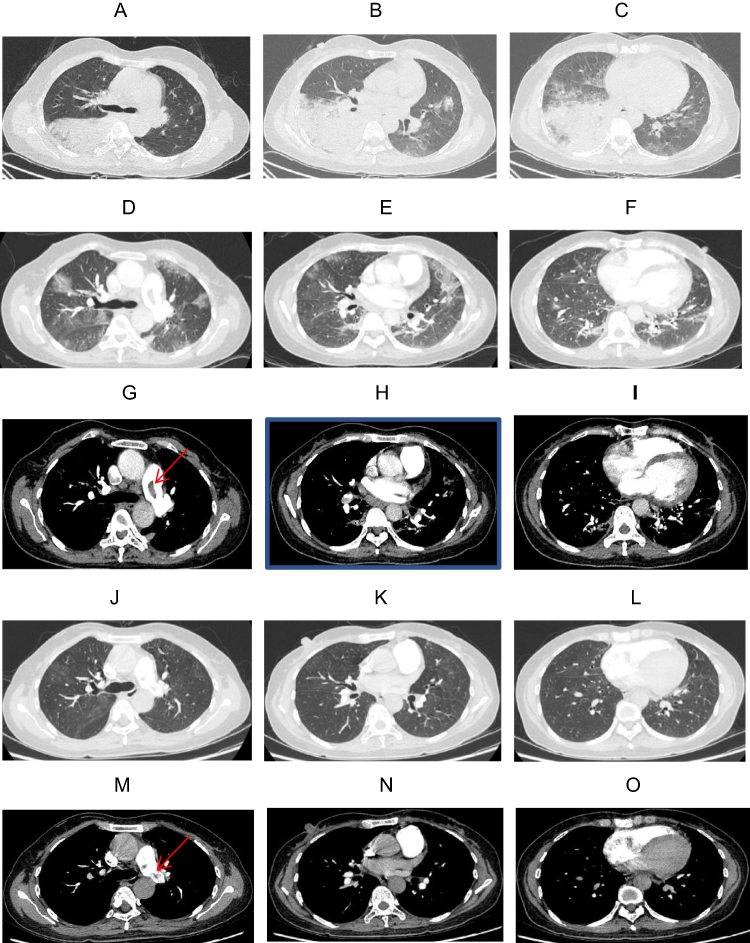 |
Figure 1 Chest computed tomography at different time points after treatment. (A–C) The day of admission. Multiple patchy exudations in both lungs, along with large consolidated shadows in the right lower lung. (D–I) Ten days after admission. CT pulmonary angiography indicated pulmonary artery trunk and left pulmonary artery thrombosis, with significant absorption of right lower lung consolidation and a slight increase in left lung exudation. (J–O) 2 weeks after discharge. CT pulmonary angiography showed shrinkage of pulmonary thrombosis in the pulmonary artery trunk and left pulmonary artery as well as significant absorption of exudations in both lungs. (red arrow indicates thrombus). |
Physical examination upon admission revealed temperature 39.8°C, pulse 104 beats/min, respiratory rate 30 breaths/min, blood pressure 142/90 mmHg, pulse oximetry-based oxygen saturation 91% (FiO2 50%), weight 60 kg, and height 163 cm. The patient was conscious, mentally weary, without jaundice, urticaria, or superficial lymphadenopathy. Systemic examination revealed tachypnea, bilateral coarse sounds in the lungs, moist rales in the right lower lung, heart rate of 104 beats/min, and regular rhythm, without murmurs over the valve auscultation areas; on palpation, the abdomen was soft, without tenderness or rebound tenderness, and there was no edema in both lower limbs.
Laboratory examination revealed negative results for nucleic acids of COVID-19 in nasopharyngeal swab and dengue virus in peripheral venous blood; Influenza A and B virus antigens; the Weil-Felix test, Widal test, 1,3-β-D-glucan assay, galactomannan test, and respiratory pathogens (ie, parainfluenza virus, Pneumocystis, Mycoplasma pneumoniae, respiratory syncytial virus, “Q fever” rickettsia, adenovirus, Legionella); IgM antibodies; and blood and sputum culture, along with sputum smear for acid-fast bacillus. Additional laboratory test results are summarized in Table 1.
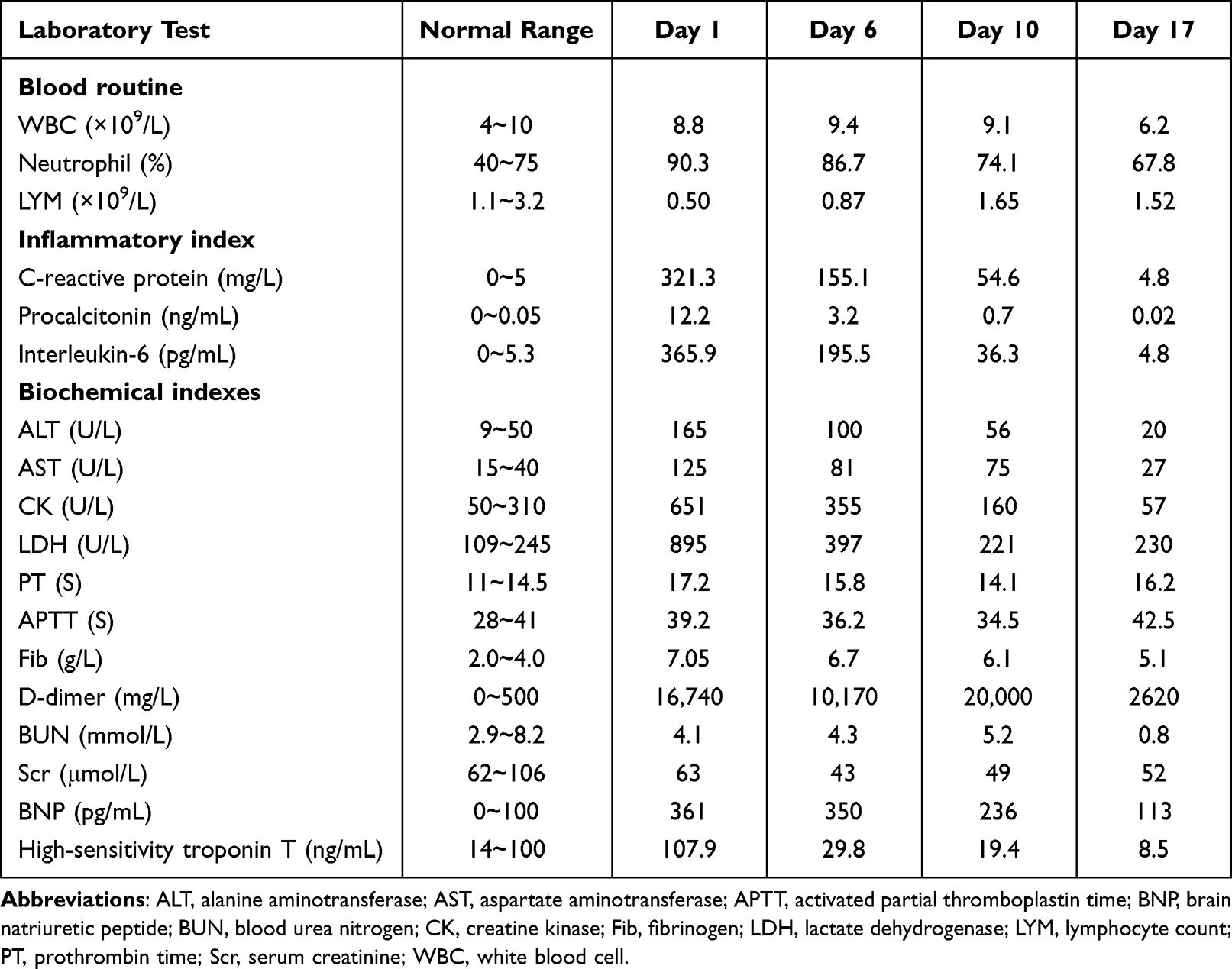 |
Table 1 Patient’s Laboratory Test Results |
Following admission, empirical antibiotic therapy with intravenous infusion of imipenem–cilastatin (1.0 g q. 8h) and levofloxacin (0.5 g q.d.) was initiated, in addition to symptomatic support measures, such as hepatoprotective agents (polyene phosphatidylcholine), antipyretics, and noninvasive assisted ventilation. On the second day, the patient’s respiratory dysfunction worsened, Acute Respiratory Distress Syndrome (ARDS) was considered, leading to tracheal intubation and assisted ventilation. A bedside bronchoscope was used to obtain secretions from the right lower-lobe bronchus for bacterial and fungal smears and cultures, and the alveolar lavage fluid was sent for mNGS examination. The next day, mNGS results revealed C. psittaci (read count 839, coverage 95%). Further inquiry into the patient’s history revealed that she had reared chickens and ducks at home for many years. The history of poultry farming, chest imaging findings, and results of etiological detection collectively led to a diagnosis of severe C. psittaci pneumonia. The antibiotic treatment was modified to an intravenous infusion of levofloxacin (0.5 g q.d.) and oral administration of doxycycline (100 mg q. 12h). Within 24 hours of treatment initiation, the patient achieved normothermia, the dyspnea was gradually alleviated, and inflammatory markers and organ-function indicators on laboratory tests improved (Table 1). The respiratory support pressure was gradually reduced, with successful removal of the tracheal tube on Day 7 of admission, followed by sequential therapy with nasal high-flow oxygen therapy. On Day 10 of admission, the patient experienced dyspnea and chest pain, with a significant elevation in the D-dimer level (Table 1). Accordingly, acute pulmonary thrombosis could not be excluded. Further examinations and imaging studies were undertaken, and CT pulmonary angiography indicated pulmonary artery trunk and left pulmonary artery thrombosis, with significant absorption of right lower lung consolidation and a slight increase in left lung exudation (Figure 1D–I); echocardiography revealed a 2.7 cm*1.7 cm echoic lesion in the pulmonary artery trunk, suggestive of thrombosis (Figure 2); and color Doppler ultrasound of veins in the bilateral upper and lower limbs showed no thrombosis. Laboratory tests, including serum immunoglobulins, anti-nuclear antibody spectrum, anti-neutrophil cytoplasmic antibody, tumor markers, antithrombin III, Protein C, Protein S, lupus anticoagulant, and anti-cardiolipin antibody levels, were all within the normal range. Based on the patient’s clinical manifestations and examination results, the patient was diagnosed with C. psittaci pneumonia with acute pulmonary thrombosis. Subcutaneous injection of enoxaparin sodium (6000 U q. 12h) was administered, which was later switched to oral warfarin (3.0 mg q.d.) for anticoagulation to ensure that the International Normalized Ratio (INR) was maintained at 2.0–3.0. The patient’s symptoms of dyspnea and chest pain gradually improved. By Day 17 of admission, the inflammatory indicators were overall normal, and organ function had significantly improved (Table 1). The patient was discharged the following day and continued oral doxycycline (100 mg q. 12h) treatment for a week. Two weeks after discharge, a follow-up CT pulmonary angiography showed shrinkage of pulmonary thrombosis in the pulmonary artery trunk and left pulmonary artery as well as significant absorption of exudations in both lungs (Figure 1J–O), and the D-dimer was reverting to normal.
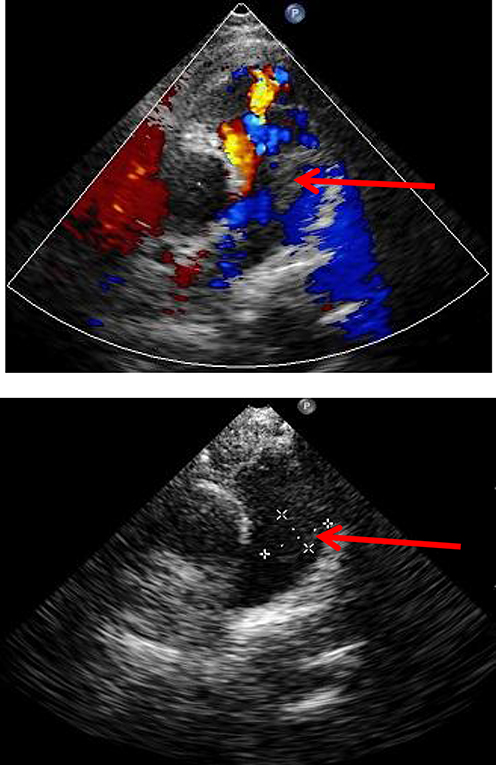 |
Figure 2 Cardiac ultrasound imaging. Echocardiography revealed a 2.7 cm*1.7 cm echoic lesion in the pulmonary artery trunk, suggestive of thrombosis. (red arrow indicates thrombus). |
Discussion
C. psittaci pneumonia, or parrot fever, is a zoonotic infectious disease caused by C. psittaci that is mainly characterized by lung infection and may be accompanied by multiorgan damage. Although rarely detected in clinical practice, C. psittaci pneumonia constitutes 1.03% of community-acquired pneumonia cases and predominantly occurs in middle-aged individuals. Direct contact with infected birds, poultry, and their excrements serves as an independent risk factor for human infection.3,6,7 Therefore, in cases of community-acquired pneumonia with a history of contact with birds or poultry, clinicians must exclude a C. psittaci infection.
C. psittaci pneumonia is classified as atypical pneumonia and suspected patients should first undergo a pulmonary examination. Radiological characteristics manifest with varying degrees of exudation and consolidation, mainly in the lower lobes of the lungs, and severe cases often present large consolidated shadows.8 Compared to other bacterial pneumonias, the lack of specific clinical manifestations of C. psittaci pneumonia makes the possibility of misdiagnosis and missed diagnosis fairly common. As seen in this case and literature reports, patients often exhibit hyperpyrexia, dyspnea, relatively slow pulse, and, often, normal white blood cell counts, along with liver function abnormalities, elevated muscle enzyme levels, and neurological symptoms.8–10 Clinicians should remain vigilant for C. psittaci pneumonia when treating pneumonia with the abovementioned clinical presentations and undertake specific laboratory examinations as early as possible. Traditional microbial culture, serological tests, and PCR have significant limitations in detecting C. psittaci, and this leads to low detection rates.11,12 Recently, with its ability to rapidly detect various pathogenic microorganisms without specific amplification, mNGS has been widely used for diagnosing infectious diseases and is the fastest and most accurate detection method for unknown pathogens.13 C. psittaci is not a regular flora of the respiratory tract; therefore, if C. psittaci DNA sequence is detected, it should be considered a possible pathogen.14 In this case, the patient had a history of poultry contact, and mNGS detected the sequence of C. psittaci. Both clinical and radiological manifestations aligned with C. psittaci pneumonia; therefore, targeted antimicrobial therapy proved effective and, thereby, supported the diagnosis of C. psittaci pneumonia.
During the patient’s antibiotic treatment, the dyspnea intensified, and chest pain was reported. Upon rechecking the D-dimer level, an increase was observed, and CT pulmonary angiography confirmed a concurrent pulmonary thrombosis. The clinical diagnosis was C. psittaci pneumonia complicated by acute pulmonary thrombosis. Risk factors for pulmonary thrombosis include genetic and acquired categories, with the latter primarily including trauma, surgery, and malignant tumors, among other factors. Infection-induced cases are relatively rare.4 Atypical pneumonia, caused by M. pneumoniae, legionella, and other organisms, can cause pulmonary thrombosis.15,16 However, reports of pulmonary thrombosis coinciding with C. psittaci pneumonia are rare, and its pathogenesis may be attributed to the release of inflammatory mediators that are stimulated by C. psittaci infection, which indirectly or directly injure endothelial cells, activate inflammatory responses and the coagulation system, and promote thrombosis.17–19 Clinical manifestations of pulmonary thrombosis lack specificity, and they range from asymptomatic to typical symptoms, such as hemoptysis, chest pain, and dyspnea. When co-occurring with pneumonia, these symptoms are often misinterpreted as a worsening of the original pneumonia or pleurisy, leading to misdiagnosis or undiagnosed conditions.19,20 D-dimer is an essential screening test for pulmonary thrombosis: a negative result can exclude pulmonary thrombosis whereas, a positive result indicates the potential presence of various diseases, including pulmonary thrombosis.21,22 Therefore, if patients with C. psittaci pneumonia exhibit poor improvement in dyspnea, experience chest pain, or even hemoptysis after targeted anti-infection treatment, particularly if the D-dimer level is elevated. Therefore, increased vigilance for the possibility of pulmonary thrombosis should be exercised.
Tetracyclines are the first-choice drugs for treating human C. psittaci infection; moreover, macrolides and fluoroquinolones exhibit satisfactory antibacterial activity against C. psittaci.3 In treating C. psittaci pneumonia combined with acute pulmonary thrombosis, conventional anticoagulant therapy is typically administered on the basis of targeted antibiotic treatment. In case of hemodynamic instability, a thrombolytic treatment is required.23,24 In the present case, the causative pathogen was identified soon after the patient’s hospitalization, and pulmonary thrombosis was recognized at an early stage. Targeted antibiotic and anticoagulant treatments were administered, leading to a smooth recovery and discharge of the patient.
In general, once the presence of Chlamydia psittaci infection is considered, serological tests and PCR should be conducted. Unfortunately, the hospital where the patient was located did not have the necessary equipment and resources to conduct serological tests or PCR.
Conclusion
In summary, although C. psittaci pneumonia accompanying acute pulmonary thrombosis might not be a frequent occurrence, it constitutes a serious extrapulmonary complication. During targeted antibiotic treatment, careful observation of symptoms, such as chest pain and hemoptysis, and assessment of the degree of improvement in dyspnea are imperative. Vigilance toward the potential onset of pulmonary thrombosis, monitoring of D-dimer, and integration of imaging examinations for timely detection of thrombosis can preclude both misdiagnosis and delay in treatment.
Ethics Approval and Informed Consent
The Ethics Committees of Huizhou Central People’s Hospital (LLBA201946A) approved this study. A signed consent statement was obtained from the patient for the publication of their case details.
Consent for Publication
Signed consent was obtained for the publication of the case details from the participant.
Author Contributions
All authors made a substantial contribution to the work reported, including study conception, design, and execution; data acquisition, analysis, and interpretation. All authors were involved in drafting, revising, or critically reviewing the article. All authors provided the final approval of the version to be published in the journal and agree to be accountable for all aspects of the work. All authors have read and approved the manuscript.
Funding
This study was supported by the Science and Technology Special Project of Huizhou (Grant no. 2020Y105).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fang C, Xu L, Tan J, et al. Case Report: Chlamydia psittaci pneumonia complicated by Guillain-Barré syndrome detected using metagenomic next-generation sequencing. Front Cell Infect Microbiol. 2023;12:1070760. doi:10.3389/fcimb.2022.1070760
2. Knittler MR, Sachse K. Chlamydia psittaci: update on an underestimated zoonotic agent. Pathog Dis. 2015;73(1):1–15. doi:10.1093/femspd/ftu007
3. Balsamo G, Maxted AM, Midla JW, et al. Compendium of measures to control Chlamydia psittaci infection among Humans (Psittacosis) and Pet Birds (Avian Chlamydiosis), 2017. J Avian Med Surg. 2017;31(3):262–282. doi:10.1647/217-265
4. Lutsey PL, Zakai NA. Epidemiology and prevention of venous thromboembolism. Nat Rev Cardiol. 2023;20(4):248–262. doi:10.1038/s41569-022-00787-6
5. Zhang Z, Zhou H, Cao H, et al. Human-to-human transmission of Chlamydia psittaci in China, 2020: an epidemiological and aetiological investigation. Lancet Microbe. 2022;3(7):e512–e520. doi:10.1016/S2666-5247(22)00064-7
6. Hogerwerf L, Gier DE, Baan B, et al. Chlamydia psittaci (psittacosis) as a cause of community-acquired pneumonia: a systematic review and meta-analysis. Epidemiol Infect. 2017;145(15):3096–3105. doi:10.1017/S0950268817002060
7. He Y, Wang S, Deng J, et al. Chlamydia psittaci pneumonia complicated with lower extremity atherosclerotic occlusive disease. Infect Drug Resist. 2023;16:2141–2145. doi:10.2147/IDR.S393256
8. Li H, Hao B, Wang Y, et al. Metagenomic next-generation sequencing for the diagnosis of Chlamydia psittaci pneumonia. Clin Respir J. 2022;16(7):513–521. doi:10.1111/crj.13519
9. Yang M, Yang DH, Yang H, et al. Clinical characteristics of Chlamydia psittaci pneumonia infection in Central South China. Infect Dis Ther. 2022;11(4):1631–1647. doi:10.1007/s40121-022-00662-4
10. Yang F, Li J, Qi B, et al. Clinical symptoms and outcomes of severe pneumonia caused by Chlamydia psittaci in Southwest China. Front Cell Infect Microbiol. 2022;11:727594. doi:10.3389/fcimb.2021.727594
11. Liu S, Cui Z, Carr MJ, et al. Chlamydia psittaci should be a notifiable infectious disease everywhere. Lancet Microbe. 2023;4(2):e62–e63. doi:10.1016/S2666-5247(22)00306-8
12. Chen X, Cao K, Wei Y, et al. Metagenomic next-generation sequencing in the diagnosis of severe pneumonias caused by Chlamydia psittaci. Infection. 2020;48(4):535–542. doi:10.1007/s15010-020-01429-0
13. Cui Z, Meng L. Psittacosis pneumonia: diagnosis, treatment and interhuman transmission. Int J Gen Med. 2023;16:1–6. doi:10.2147/IJGM.S396074
14. Li N, Cai Q, Miao Q, et al. High-throughput metagenomics for identification of pathogens in the clinical settings. Small Methods. 2021;5(1):2000792. doi:10.1002/smtd.202000792
15. Song S, Xu Y. A retrospective study of the clinical characteristics of 9 children with pulmonary embolism associated with Mycoplasma pneumoniae pneumonia. BMC Pediatr. 2023;23(1):370. doi:10.1186/s12887-023-04188-7
16. Rókusz L. Case of Legionella pneumonia complicated with pulmonary thromboembolism. Acta Microbiol Immunol Hung. 2010;57(4):401–406. doi:10.1556/AMicr.57.2010.4.6
17. Zhang Z, Wang P, Ma C, et al. Host inflammatory response is the major factor in the progression of Chlamydia psittaci pneumonia. Front Immunol. 2022;13:929213. doi:10.3389/fimmu.2022.929213
18. Poor HD. Pulmonary thrombosis and thromboembolism in COVID-19. Chest. 2021;160(4):1471–1480. doi:10.1016/j.chest.2021.06.016
19. Zhang Y, Zhou Q, Zou Y, et al. Risk factors for pulmonary embolism in patients preliminarily diagnosed with community-acquired pneumonia: a prospective cohort study. J Thromb Thrombolysis. 2016;41(4):619–627. doi:10.1007/s11239-015-1275-6
20. Jolobe OMP. Similarities between community-acquired pneumonia and pulmonary embolism. Am J Med. 2019;132:e863. doi:10.1016/j.amjmed.2019.03.002
21. Kearon C, de Wit K, Parpia S, et al. Diagnosis of pulmonary embolism with d-Dimer adjusted to clinical probability. N Engl J Med. 2019;381(22):2125–2134. doi:10.1056/NEJMoa1909159
22. Crawford F, Andras A, Welch K, et al. D-dimer test for excluding the diagnosis of pulmonary embolism. Cochrane Database Syst Rev. 2016;2016(8):CD010864. doi:10.1002/14651858.CD010864.pub2
23. Freund Y, Cohen-Aubart F, Bloom B. Acute pulmonary embolism: a review. JAMA. 2022;328(13):1336–1345. doi:10.1001/jama.2022.16815
24. Tritschler T, Kraaijpoel N, Le Gal G, et al. Venous thromboembolism: advances in diagnosis and treatment. JAMA. 2018;320(15):1583–1594. doi:10.1001/jama.2018.14346
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.