Back to Journals » Drug Design, Development and Therapy » Volume 20
Chinese Herbal Medicine in Ulcerative Colitis-Associated Carcinogenesis Treatment: Mechanisms, Progress, and Future Directions
Authors Gu F, Chen Z, Lim X ![]() , Zhang T
, Zhang T ![]() , Yuan J, Li L
, Yuan J, Li L ![]()
Received 14 October 2025
Accepted for publication 20 January 2026
Published 8 February 2026 Volume 2026:20 574142
DOI https://doi.org/10.2147/DDDT.S574142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Fanruo Gu,1,* Zexuan Chen,1,2,* Xueyee Lim,1,3 Tong Zhang,1,4 Jianlong Yuan,1,5 Ling Li1,4
1School of Pharmacy, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 2Shanghai Tufeng Pharmaceutical Technology Company Limited, Shanghai, 201203, People’s Republic of China; 3Shanghai University of Traditional Chinese Medicine International Education College, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 4State Key Laboratory of Integration and Innovation of Classic Formula and Modern Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, 201203, People’s Republic of China; 5Fujian Center for Drug Evaluation and Monitoring, Fuzhou, 350000, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Li, School of Pharmacy, Shanghai University of Traditional Chinese Medicine, Cailun Road No. 1200, Shanghai, 201203, People’s Republic of China, Email [email protected] Jianlong Yuan, Fujian Center for Drug Evaluation and Monitoring, Zhanqi Building Room 605, Dongpu Road No. 156, Fuzhou, Fujian, 350000, People’s Republic of China, Email [email protected]
Abstract: Colitis-associated colorectal cancer (CAC) is a highly prevalent malignancy of the digestive tract. The close association between ulcerative colitis (UC) and CAC makes inhibiting this carcinogenic transformation a critical preventive goal. Based on traditional Chinese medicine (TCM) theories of “dampness-heat stasis” and “latent pathogen-induced deficiency”, this review systematically explores the pathological process of ulcerative colitis associated carcinogenesis (UCAC) and its interpretation in TCM. We conducted a comprehensive literature search in CNKI and PubMed databases (2020– 2025), systematically analyzing about 79 relevant studies to summarize the clinical applications of TCM in preventing and treating UCAC progression, including oral and topical herbal therapies, as well as non-pharmacological interventions such as acupuncture. Furthermore, we elucidate the underlying mechanisms of TCM interventions in UCAC, with a focus on gut microbiota modulation and key inflammatory signaling pathways (eg, NF-κB, IL-6/JAK2/STAT3), offering new translational perspectives. The novelty of this review is twofold: firstly, it provides the first systematic synthesis of research progress on therapeutic methods, encompassing oral and topical herbal formulations as well as acupuncture, and molecular mechanisms of TCM for UCAC. Secondly, it advances the field by analyzing TCM theories through the lens of modern medicine, comparing TCM’s holistic approach with Western medicine’s targeted paradigm, and proposing an integrated “gut microbiota-metabolite-target” research framework. This framework aims to furnish a theoretical foundation for both the modernization of TCM and the development of combined therapeutic strategies that leverage the strengths of both medical systems.
Keywords: traditional Chinese medicine, ulcerative colitis associated carcinogenesis, inflammation, tumor prevention, review
Introduction
Colitis-associated colorectal cancer (CAC) is a malignant tumor originating in the colon and ranks third globally in cancer incidence, accounting for approximately 10% of all cancer case.1 CAC has more than 50% of its new cases occurring in Asia, followed by Europe (27.9%), with China accounting for 26.8% of global cases, ranking first worldwide.2,3 The etiology of CAC is attributed to multifactorial, involving genetic predisposition, environmental influences, and abnormal immune responses. Notably, dysregulation between the proinflammatory activity of Th17 cells and the immunosuppressive function of Treg cells (Treg) fosters chronic colitis. There is a well-established association between ulcerative colitis (UC) and CAC, with UC patients facing a 2–3 times higher incidence rate of CAC than the general population. The risk increases with disease duration, reaching an incidence of 16.9% in UC patients after 11 years.4 The progression of UC to CAC, also known as ulcerative colitis associated carcinogenesis (UCAC), is primarily driven by persistent local inflammatory response that disrupts the immune microenvironment and alters the composition of the intestinal microbiota. First, chronic inflammation leads to excessive production of reactive oxygen species (ROS), which hyperactivates the signal transducer and activator of transcription 3 (STAT3)/nuclear factor kappa-B (NF-κB) pathway, which significantly elevates the risk of DNA damage and mutations in proto-oncogenes.5,6 Second, the prolonged inflammation impairs the regulatory balance Th17 and Treg, weakening immune surveillance against tumor cells and facilitating cancer cell evasion.7 Third, chronic inflammation disrupts the balance of intestinal flora, characterized by an increase in pathogenic bacteria and a decrease in beneficial bacteria, altering metabolite profiles that compromise the integrity of the mucosal barrier. This shift alters metabolic profiles and damages the mucosal barrier, leading to sustained release of inflammatory mediators, exacerbating DNA damage, promoting cellular gene mutations, abnormal proliferation, and ultimately elevating the risk of cancer.8 In brief, the presence of inflammation increases the susceptibility of the intestine to dysplasia and malignant transformation. Hence, considerable attention is being directed toward the prevention and treatment of UCAC.
UCAC progresses through three stages: chronic enteritis, precancerous lesions, and malignant tumor formation. In the moderate or severe stage of UC, the treatment focuses on reducing excessive immune responses and blocking pro-inflammatory signaling pathways. Common medications for UC include anti-inflammatory drugs such as amino salicylic acid and glucocorticoids and immunomodulators like thalidomide. However, patients with moderate to severe UC often experience an inadequate response to treatment or drug intolerance.9 Thus, the immunosuppressants (eg, azathioprine, methotrexate) and biologic agents (eg, infliximab) are employed. Azathioprine is typically used for hormone-dependent UC patient, while methotrexate is prescribed for those who are ineffective or cannot tolerate azathioprine. Infliximab and JAK inhibitors are typically used when other drugs fail, but their effectiveness, potential side effects, risk of resistance, and high costs limit their broader use.10 Surgery is the main option for precancerous lesions and CAC. Nevertheless, clinical data show that around 50% of patients develop metastases, with a five-year survival rate of just 14%. Even with adjuvant chemotherapy, more than 25% of cases experience recurrence.11 This reveals significant shortcomings in current treatment methods for long-term management of UC and CAC prevention, especially regarding chronic progression such as UCAC. In such contexts, applying TCM for holistic regulation and long-term treatment demonstrates considerable advantages.
Traditional Chinese medicine (TCM) possesses a long history in prevention and treatment of tumors and inflammatory diseases. The Huangdi Neijing, one of the earliest TCM classics, not only records the earliest descriptions of tumor-related conditions, such as “abdominal masses”, but also systematically elaborates theories of inflammation, including “pathogenic fire” and “pathogenic heat”, particularly in the Suwen-Zhizhen Yao Da Lun, thereby laying an important foundation for modern research.12 Contemporary studies further confirm TCM’s significant value in treating tumors and inflammation, including the improvement of clinical symptoms, alleviation of treatment side effects, inhibition of postoperative tumor metastasis, and enhancement of patients’ quality of life.13 Specifically, TCM helps reduce inflammation and fight cancer by repairing intestinal mucosa, balancing gut microbiota, and regulating immune function. This makes TCM a promising approach for managing colorectal diseases and preventing UCAC.14 Consequently, TCM practice offers new strategies for addressing chronic inflammation and preventing its progression to malignancy.
This review systematically analyzed approximately 79 relevant studies retrieved from CNKI and PubMed (2020–2025), using core keywords such as “ulcerative colitis”, “colorectal cancer”, “colitis-associated carcinogenesis” and “signaling pathway”. It summarizes how TCM can be applied to prevent UCAC, highlighting TCM interventions including herbal compounds, prescriptions, and acupuncture, and exploring their mechanisms—particularly their effects on gut microbiota and molecular signaling pathways. Ultimately, the work seeks to provide new insights into using TCM to manage UCAC.
Basic Principles and Mechanism of TCM in UCAC
The clinical symptoms of UC, which include persistent or recurrent abdominal pain, diarrhea, and mucopurulent bloody stools, correspond to TCM symptoms of “intestinal obstruction (chang pi)” and “intestinal wind (chang feng)”.15 According to TCM theory, the pathogenesis of inflammation-induced carcinogenesis, as seen in UC, is primarily attributed to a combination of damp-heat stasis (a condition of chronic inflammation and metabolic imbalance, often resulting from overeating, which leads to impaired digestion and immune dysfunction) and qi deficiency caused by latent pathogenic factors (a state where a subclinical pathological factor persists within the body due to a weakened immune and homeostatic system).16 Figure 1 illustrates the relationship between UCAC and these underlying TCM pathological mechanisms.
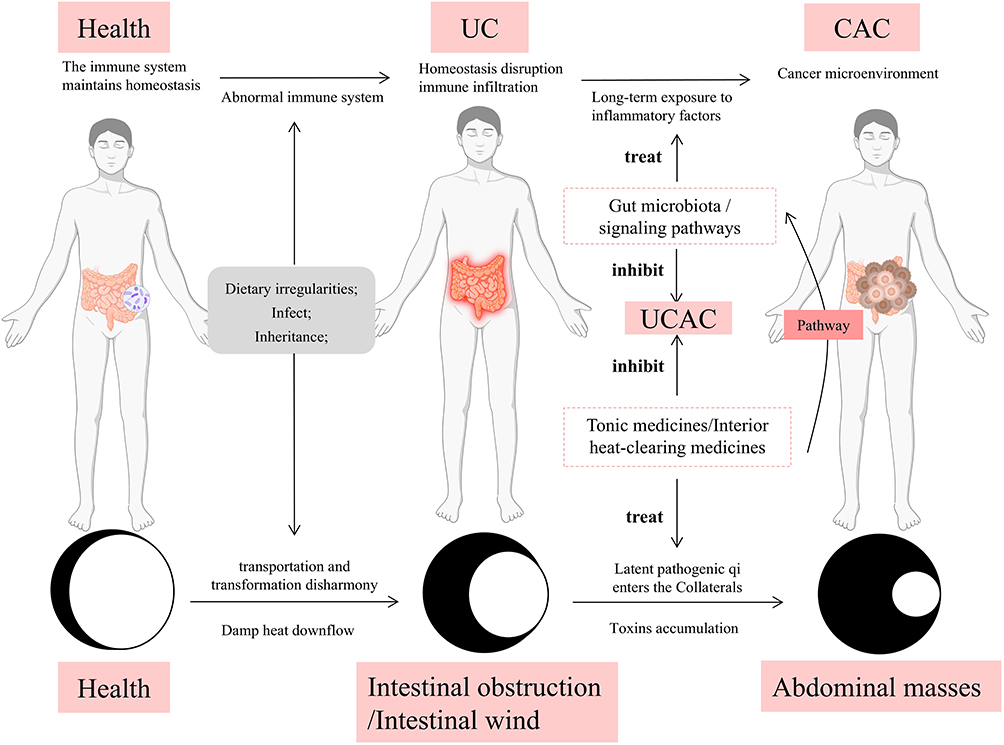 |
Figure 1 The correspondence between the transformation mechanism of UCAC in the theory of modern pathology. Notes: The black circle denotes latent pathogenic qi, and the white circle signifies healthy qi. Disease progression: Healthy qi → Qi deficiency → Latent pathogen qi dominance; Pathology: Spleen-stomach dysfunction → Dampness-heat → Intestinal obstruction/Intestinal wind → Latent pathogens → Qi / blood stasis → Abdominal masses; The human body diagram corresponds to the three stages of health, UC, and CAC. |
TCM management of UCAC follows a holistic principle targeting both symptoms and root causes. In managing UCAC, the core therapeutic strategy is to “reinforce healthy qi to eliminate pathogenic factors”, adopting the combined strategy of “strengthening the spleen and transforming dampness”, “circulating blood and transforming stasis”, as well as “clearing heat and detoxifying”. Together, these actions collectively inhibit abnormal cell proliferation and modulate systemic inflammation (symptom control), while restoring the intestinal microenvironment and immune regulation (root cause treatment). For example, Dampness-Resolving and Toxin-Removing Decoction (composed of Pulsatillae Radix, Citri Reticulatae Pericarpium, Phellodendri Chinensis Cortex, Scutellariae Radix, Coptidis Rhizoma, Taraxaci Herba, Bletillae Rhizoma, Aucklandiae Radix, Corydalis Rhizoma, Fraxini Cortex, Dioscoreae Rhizoma and Glycyrrhizae Radix et Rhizoma) may remove heat, detox, strengthen the spleen and eliminate dampness simultaneously, showing its effectiveness in clinical studies, such as restoring the balance of intestinal flora and improving inflammatory symptoms.17 Similarly, the Fufang Kushen Injection, composed of Sophora Flavescens Radix, Poria Cocos, etc., has significantly improved CD4+, CD8+, and CD4+/CD8+values, when it was combined with chemotherapy, while also reducing the side effects of chemotherapy.18
To specifically address the core pathogenesis of damp-heat, both Qingre Qushi Recipe and Xilei Powder show their anti-inflammation effects and like the first-line drugs mesalamine in TCM clinics, based on the combined strategy of “remove heat and dampness, as well as strengthening spleen and qi”.19 On the other hand, to deal with the deficiency of vital energy affected by latent pathogen, the Sijunzi decoction, is frequently used to strengthen the spleen and replenishing qi. It has been shown to promote intestinal mucosa repair in patients with UC.20 Finally, the Modified Gegen Qinlian Decoction (composed of Puerariae Lobatae Radix, Atractylodis Macrocephalae Rhizoma, Codonopsis Radix, Pulsatillae Radix, Coicis Semen, Poria, Angelicae Sinensis Radix, Dioscoreae Rhizoma, Coptidis Rhizoma, Phellodendri Chinensis Cort, Scutellariae Radix, Aucklandiae Radix, Notoginseng Radix et Rhizoma, Bletillae Rhizoma, Corydalis Rhizoma and Glycyrrhizae Radix et Rhizoma) is also used to dredge the meridians combined with acupuncture, and can significantly improve relief time for diarrhea, abdominal pain, mucous purulent stools of UC.21
Guided by the core pathogenesis of UCAC, characterized by “damp-heat stasis” and “latent pathogen-induced deficiency”, TCM clinical interventions focus on the principle of “reinforce healthy qi to eliminate pathogenic factors”. Integrated treatment modalities, including compound Chinese herbal formulations (oral/topical) and acupuncture, are employed to leverage multi-component, multi-target, and multi-effect mechanisms of herbal agents, as well as the neuro-immune regulatory effects of acupuncture. These strategies collectively exemplify the holistic approach and symptom–root dual-management principle of TCM.
TCM Application in Prevention and Treatment of UCAC
Oral Administration
The advantages of oral administration primarily lie in three forms: single herbal compounds with defined components and clear mechanisms, facilitating precise research and quality control, and targeting specific pathological processes; herbal formulas containing multiple components act synergistically at various targets, providing a holistic regulation of immune, inflammatory, and metabolic functions; while herbal extracts retain multiple active ingredients’ combined effects and, due to their simplified composition, are more amenable to mechanistic studies and quality control.
TCM Compound
TCM compounds are the primary form of clinical medicine and offer benefits in treating chronic diseases such as chronic inflammation and cancers. Among these, Shenbai Jiedu Formula is a notable TCM compound used in treating UCAC. Studies show this formula reverses G0/G1 cell cycle arrest in FHC cells, maintains cell cycle homeostasis and protects intestinal epithelial cells from UC.22 Animal studies show that high doses (42 g/kg) resulted in only a few low-grade tumors, suggesting protection against carcinogensis.23 Shaoyao Decoction, as a classic heat clearing prescription by Liu Wansu, restores the intestinal barrier, prevents mucosal injury due to inflammatory,24 and induces apoptosis in HT29 colon cancer cells.25 Research on representative TCM compounds such as Shenbai Jiedu Formula and Shaoyao Decoction primarily involves animal experiments (Table 1). Evidence suggests that Shaoyao Decoction, in particular, effectively repairs inflammation-induced mucosal injury and inhibits CAC development. In clinical practice, TCM compounds are often combined with chemotherapy to improve efficacy and reduce side effects. For example, a study conducted by Shanxi University of TCM compared outcomes in 40 CAC patients, receiving chemotherapy with or without a modified Mume Pill. Outcomes were assessed using TCM syndrome scores, clinical efficacy, activities of daily living scores, tumor markers (carcinoembryonic antigen, carbohydrate Antigen 19–9), inflammatory cytokines (tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6)), and adverse reaction rates (nausea/vomiting, myelosuppression, neurotoxicity, liver dysfunction). The combination therapy significantly improved clinical outcomes, reduced levels of tumor markers and inflammation, decreased adverse effects, and enhanced overall quality of life.26
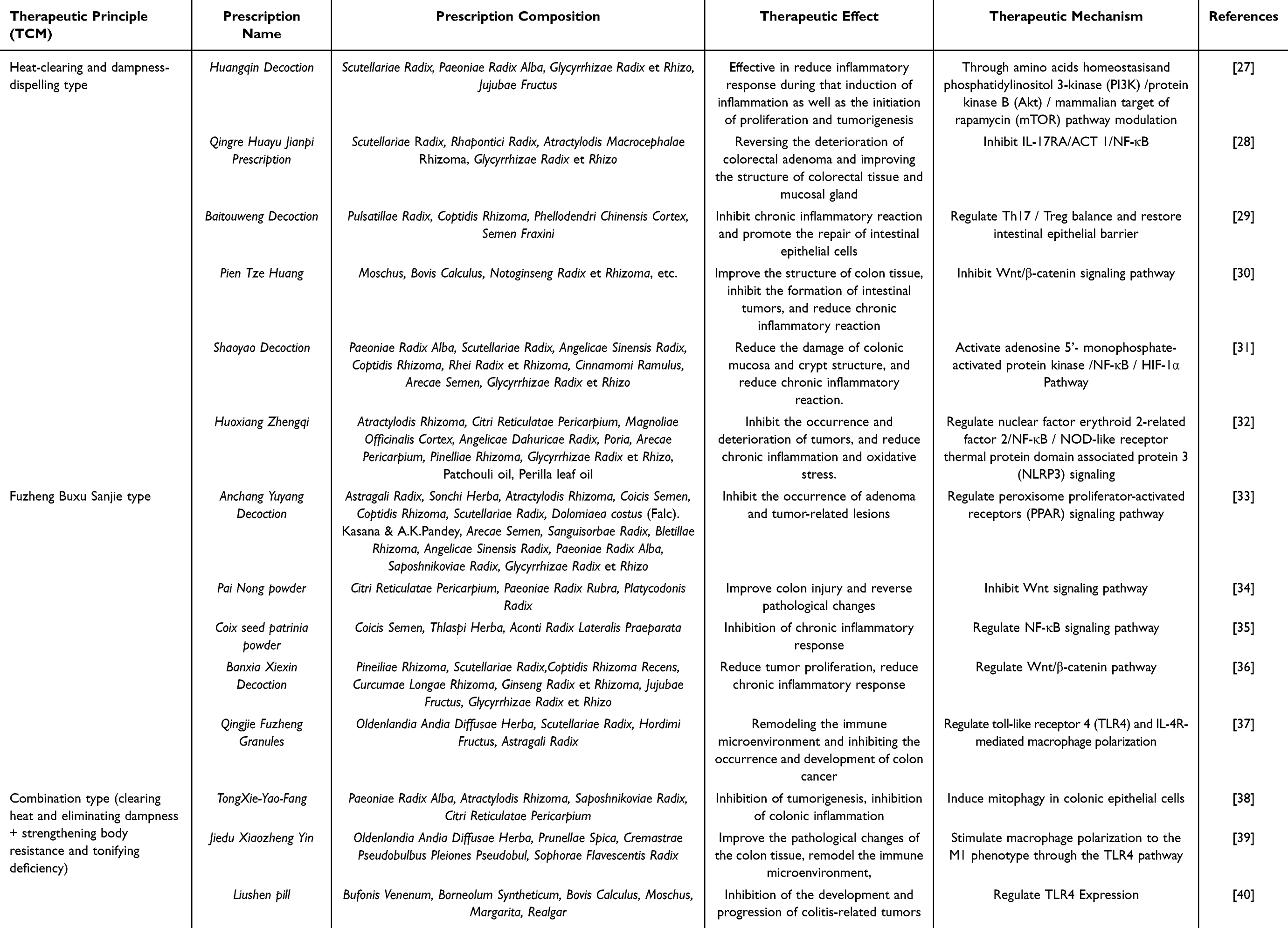 |
Table 1 Animal Experimental Study of TCM Compound in Treating UCAC |
TCM Extract
TCM extracts, obtained through modern extraction technologies, significantly enrich the active components of medicinal herbs, thereby enhancing both the efficacy and stability of pharmaceutical preparations. Compared to TCM compound, TCM extracts offer a clearer material basis and controllable quality standards. For example, the water extract of Phellinus Igniarius may improve the inflammatory cell infiltration of colinic mucosa and reduce the cytokine levels such as IL-6, IL-1β and TNF-α to relieve UCAC.41 Similarly, purple yam polyphenol extract, extracted from Dioscores species, exhibits comparable pharmacological effects to Phellinus Igniarius in reducing inflammation.42 TCM extracts offer several advantages in drug development, including higher concentration of therapeutic components and better-defined mechanisms of action. These features make TCM extracts a promising and flexible option for the prevention and treatment of UCAC.
Monomeric Compound
Monomeric compounds with defined chemical structures from herbal medicines are pivotal for elucidating structure–activity and dose–response relationships. They play a critical role in modulating inflammatory responses and improving the intestinal microenvironment during UCAC. Pharmacological effects and mechanisms of compounds from TCM against UCAC are detailed in Table 2. The structure–activity relationship analysis of representative compounds of each component type is shown in Figure 2.
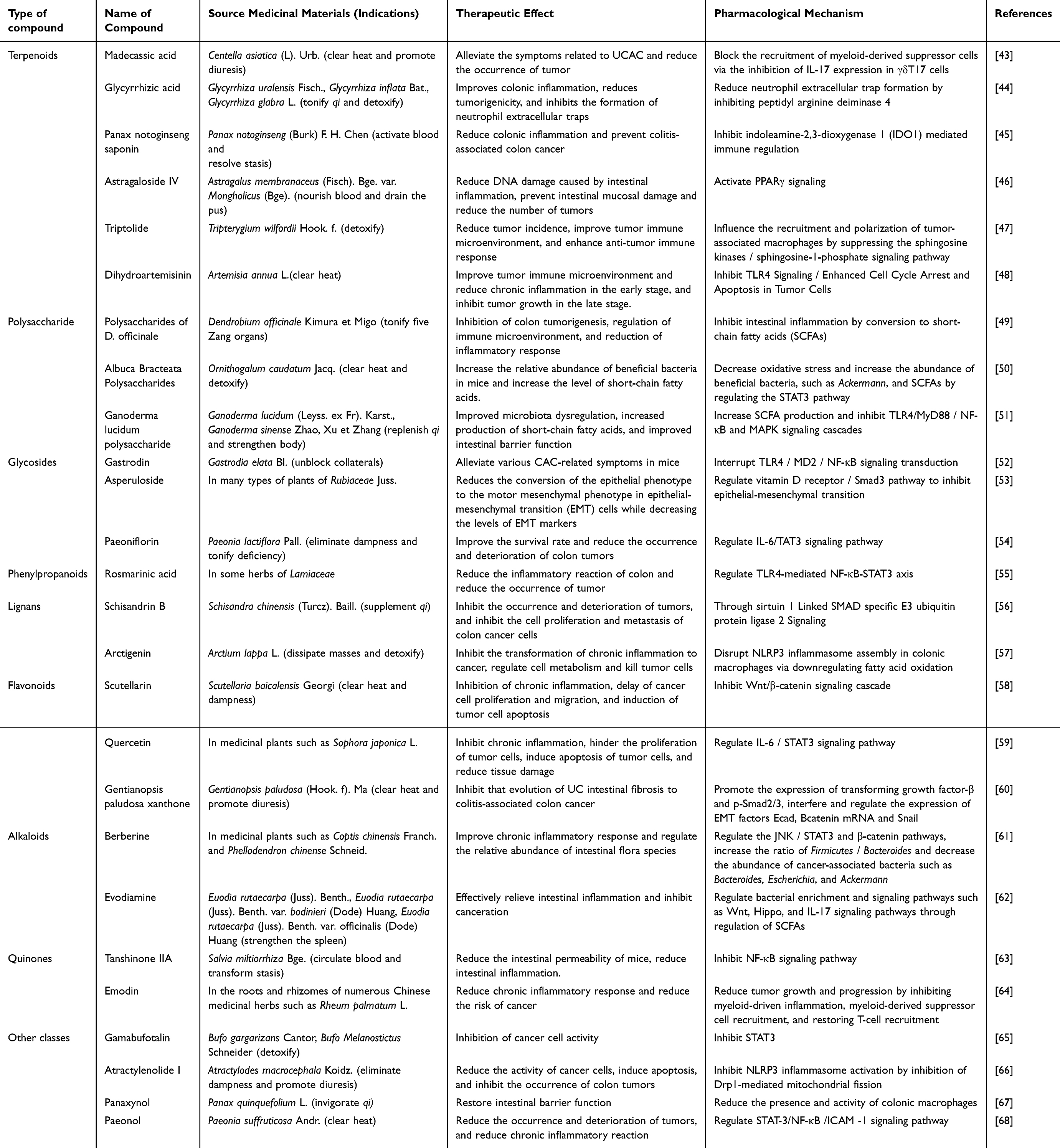 |
Table 2 Pharmacological Effects and Mechanisms of Compounds from TCM Against UCAC |
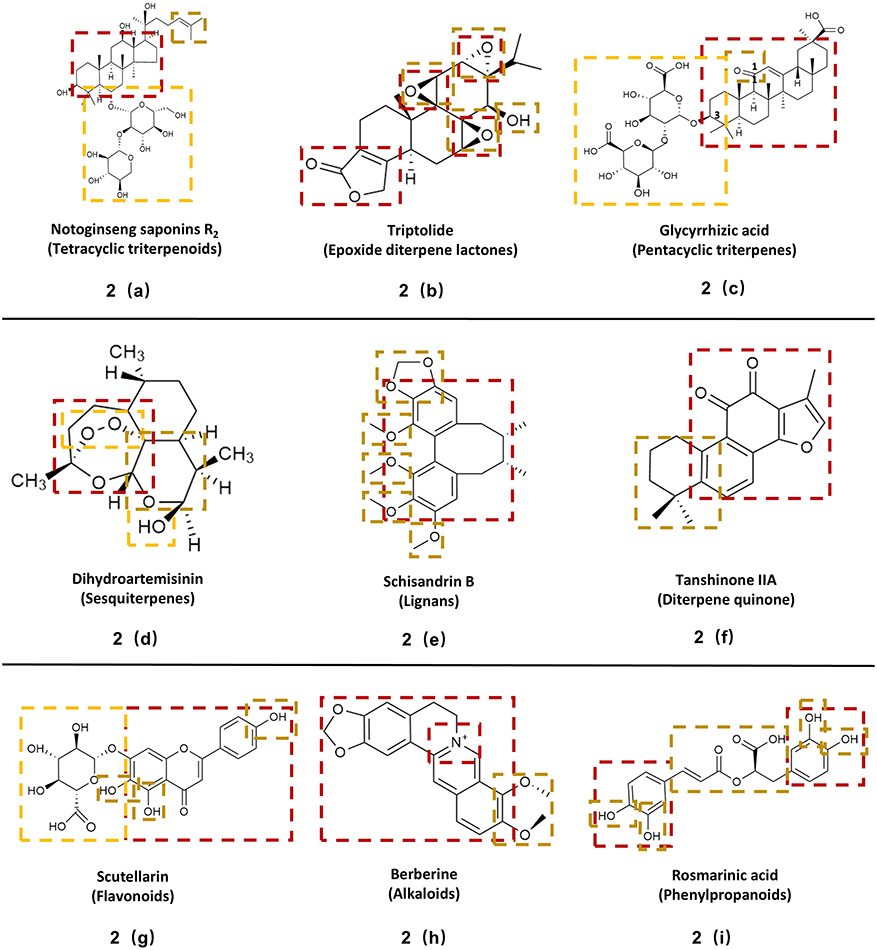 |
Figure 2 Structure–activity relationship diagram of representative compounds of each component type. Notes: The red frame region is the core basic pharmacodynamic structure, the brown frame region is the specific pharmacodynamic structure, and the yellow frame region is the structure affecting absorption and metabolism. 2(a): red frame region provides a rigid hydrophobic skeleton structure, which is conducive to the compound embedding in the hydrophobic site of the protein; brown frame region increases the hydrophobic volume of the molecular end, which is conducive to the stable binding of the compound to the protein; yellow frame affects the solubility and bioavailability of drugs; 2(b): red frame region engages the protein target through an electrophilic center created by its fused-ring system; brown frame contributes to binding by forming a specific hydrogen-bond network via its oxygen atoms acting as hydrogen-bond acceptors; 2(c) red frame region provides a hydrophobic plane structure, which is conducive to embedding the hydrophobic structure of the protein; brown frame region simulates the natural substrate of a specific enzyme to play a competitive inhibitory effect; yellow frame affects the solubility and bioavailability of drugs; 2(d) red frame region forms a hydrophobic contact surface, which provides hydrogen bond sites and triggers ROS generation; brown frame region fixes the conformation of the γ-lactone ring through covalent bonds to form a stable protein-binding region; yellow frame affect the solubility, stability and bioavailability of the compound; 2(e) red frame region forms a rigid planar structure, which is embedded in the hydrophobic structure of the protein target through hydrophobic interaction and π-π bond stacking; brown frame improves the key structures of binding stability and binding specificity to the target by affecting the steric hindrance and electron distribution of the stereostructure; 2(f) red frame region provides a rigid planar hydrophobic skeleton, which is embedded in the hydrophobic structure of the protein target through hydrophobic interaction and π-π bond stacking, while the conjugated system can enhance the antioxidant effect; brown frame affect the binding affinity of compounds to protein targets through hydrophobic effects and steric hindrance; 2(g) red frame region behalf that the planarity of the conjugated structure is conducive to the embedding of DNA double helix base pairs between tumor cells; brown frame region behalf that multiple phenolic hydroxyl groups provide hydrogen bond binding sites for protein binding, which is conducive to the stable combination of compounds and targets. The acidic properties of phenolic hydroxyl groups can chelate metal ions and reduce the generation of harmful free radicals; yellow frame affects solubility, targeting and bioavailability; 2(h) red frame region behalf that isoquinoline and dioxane of berberine form a positively charged planar structure, which can be inserted into the double helix structure of tumor cell DNA or competitively bind to specific gene fragments to inhibit the proliferation of cancer cells; brown frame enhances the hydrophobic interaction and van der Waals force between the compound and DNA and protein, and increases the stability of the compound binding to the target; 2(i) red frame region behalf that the active hydrogen atoms of the catechol structure can be combined with free radicals to play an antioxidant role; brown frame behalf that the connection structure formed by ester group and unsaturated double bond makes the molecular stereo structure relatively flexible and can be combined with different targets. |
Terpenoids, composed of isoprene units, include monoterpenes, sesquiterpenes, diterpenes, etc. Their planar polycyclic skeletons are crucial for binding to protein targets, while stereochemistry (cis/trans configuration), chiral center conformation, and hydrophobic group modifications significantly influence their anti-inflammatory and anti-tumor activities.69–71 The bioactivities of polysaccharides vary with monosaccharide composition, glycosidic linkage types, three-dimensional structure, and molecular weight. Polysaccharides featuring β-(1→3) and (1→6) glycosidic bonds, such as those from Ganoderma lucidum, are particularly important for anti-inflammatory and anti-tumor effects. Acetyl group modifications also significantly impact activity; for example, acetylation can enhance the activity of Dendrobium polysaccharides, whereas excessive acetylation may disrupt the triple-helix structure of Ganoderma lucidum polysaccharides and reduce their efficacy.70,72,73 The anti-inflammatory and anti-tumor activities of glycosides are determined by the aglycone type, sugar-chain structure, glycosidic bond type, and chemical modifications. Key factors include whether the aglycone possesses a planar structure facilitating intercalation into protein targets and its capacity to form hydrogen bonds.74,75 The bioactivity of phenylpropanoids and their derivatives (eg, phenolic acids) is determined by the combination of their phenylpropane (C6-C3) skeleton and functional groups such as phenolic hydroxyls. The electron-withdrawing capacity, number, and position of these functional groups are critical factors that influence the system’s electron distribution, leading to structural stability and antioxidant activity. Additionally, the conjugated double-bond system in the side chain (eg, the acrylic acid structure) serves as a key electron carrier and reactive site. Lignans, as dimeric phenylpropanoid derivatives, possess more complex structures. Their activity primarily depends on the overall three-dimensional shape and rigidity, dictated by the dimerization pattern and stereochemistry. This structural framework is crucial for their role as topoisomerase inhibitors or for high-affinity binding to specific protein pockets (eg, Keap1). The anti-inflammatory and anti-cancer activities of flavonoids primarily depend on the planar structure formed by their benzo-γ-pyrone/pyridone nucleus. Activity is further modulated by structural variations of the nucleus and the presence or absence of a C2-C3 double bond, among other factors.76 Alkaloids, as an important class of nitrogen-containing natural products, often combine a rigid planar structure with basic characteristics. Their anti-inflammatory and anti-tumor activities are affected by the skeletal structure, stereochemistry, functional groups, and variations in the heterocyclic system.77 Anthraquinones feature a coplanar tri-cyclic aromatic structure as their core pharmacophore. The hydrophobic interactions and receptor affinity generated by their side chains are key determinants of their potency.78
In summary, the core foundation for a pharmacologically active compound typically includes a rigid planar structure and the ability to form hydrogen bonds. The number, property, position, and linkage patterns of substituents are critical factors that modulate the potency and selectivity of its activity.
Topical Administration
In fact, the oral bioavailability of many active ingredients is limited, mainly due to the hepatic first-pass effect.79 Therefore, topical administration routes, including TCM enema, acupoint application, ear acupoint bean pressing and TCM atomization inhalation, have been clinically adopted to overcome this limitation and reduced systemic side effects. TCM enema allows for direct absorption through the intestinal mucosa, making it suitable for patients with lesions in the colon or rectum. Acupoint application involves applying medication to specific acupoints, combining the dual therapeutic effects of the drug and acupoint stimulation, and is suitable for patients requiring systemic regulation. Ear acupoint bean involves continuous gentle stimulation by pressing specific acupoints on the auricle, commonly used as an adjunctive therapy. TCM nebulization is administered via inhalation through the respiratory tract into circulation, suitable for drugs with low oral bioavailability or significant gastrointestinal irritation that require systemic efficacy.
TCM Enema
As a rectal dosage form, TCM enema allows direct drug absorption through intestinal mucosa, significantly reduces the first-pass effect and improves bioavailability. Clinical studies have shown that combining conventional Western medical injections with TCM retention enema therapy yields better outcomes than Western medicine alone.80 For instance, Yuxian Fang, composed of Sanguisorbae Radix, Portulacae Herba, Coicis Semen, Fraxini Cortex, Pulsatillae Radix, Phellodendri Chinensis Cortex, Agrimoniae Herba and Bletillae Rhizoma, a TCM formula with functions such as clearing heat, eliminating dampness, astringing and promoting tissue regeneration, has demonstrated efficacy in repairing intestinal mucosal damage when administered via enema.81 The TCM formulations selected for enema use typically focus on clearing heat and detoxifying, which can play a key role in relieving UC symptoms and preventing its progression to malignancy.
Acupoint Application
Acupoint application involves the application of TCM preparations or its pharmaceutical derivatives to one or more specific acupoints. The approach combines the therapeutic effects of both the medicinal substances and the targeted acupoints. Additionally, it can reduce hepatic first-pass effect and minimize gastrointestinal irritation. Commonly selected accupoints which include ST25 (Tianshu, invigorating spleen and regulating stomach)82 and RN08 (Shenque, regulating qi and blood)83 are often used as main acupoints, combined with individualized acupoints and drugs (such as Wumei Pill) to treat UC. Studies have shown that acupoint patching therapy can significantly alleviate ulcer formation, reduce inflammation, and enhance immune function. It is particularly effective for patients diagnosed with both cold and heat syndromes under TCM theory, showing notable advantages in reducing the risk of UCAC.84
Ear Acupoint Bean Pressing
Ear acupoint bean pressing involves attaching medicinal beans or magnetic beads to specific auricular acupoints using adhesive tape, followed by gentle stimulation of these points. This method is simple to perform, non-invasive and well accepted by patients. When combined with TCM enema therapy, it has been shown to significantly alleviate the clinical symptoms of UC such as bloody stool.85 Moreover, its combination with mesalamine enteric-coated tablets has demonstrated better therapeutic outcomes compared to treatment with Western medicine alone.86
TCM Atomization Inhalation
TCM atomization inhalation therapy involves converting liquid herbal medicine into fine aerosol particles through ultrasonic wave, allowing patients to inhale the medicine through the respiratory tract for therapeutic purposes.87 This method is characterized by a small required dose, rapid absorption and direct delivery to the target site of disease. Zanthoxylum bungeanum essential oil, extracted from the traditional pungent herb Zanthoxylum bungeanum, can overcome the limitations of traditional oral administration when delivered via aerosol inhalation.88 After being absorbed into bloodstream, it has been shown to inhibit the expression of IL-6 in colon tissue, thereby delaying the progression of UCAC.
Acupuncture and Moxibustion
Acupuncture and moxibustion exerts its therapeutic effects by stimulating specific acupoints to mobilize the body’s self-regulatory systems. This approach avoids the chemical residues and metabolic toxicity associated with pharmaceuticals, offering a high safety profile for long-term use. Compared to drug therapy, its advantages include fewer side effects and the promotion of visceral functional recovery. However, its effects manifest more slowly. Consequently, it is often used in combination with pharmacological treatment. Commonly used acupoints, locations, and indications are shown in Figure 3.
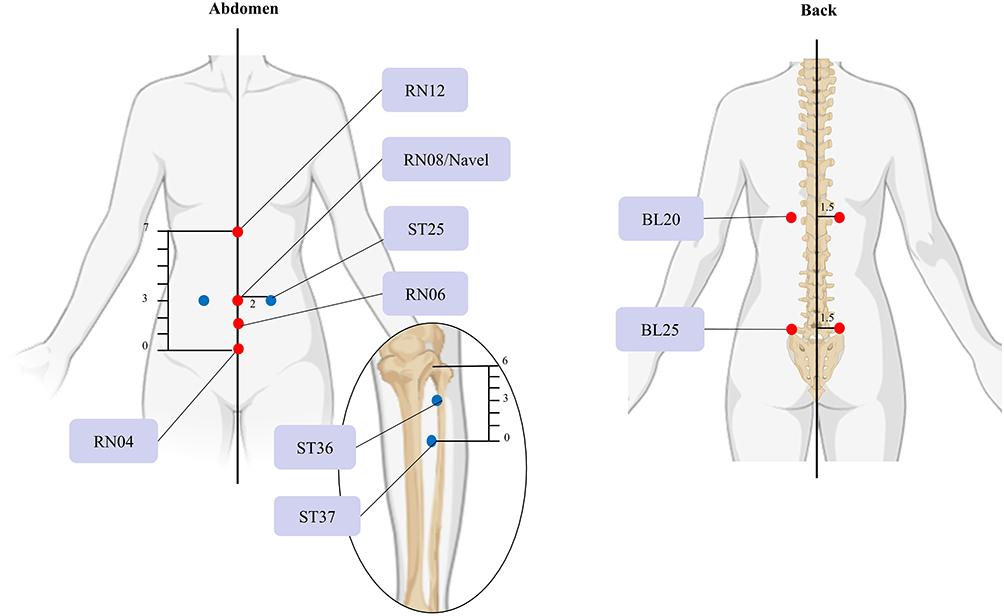 |
Figure 3 Common acupoints, locations and main treatments of acupuncture and moxibustion in UCAC therapy. Notes: The dimensions in the diagram are measured in cun, with 1 cun equalling 1 cm. Red dots indicate primary acupuncture points for moxibustion, while blue dots denote primary points for both acupuncture and moxibustion. RN12 (Zhongwan) is located on the anterior median line of the upper abdomen, 4 cun above the belly button; RN08 (Shenque) is located at the centre of the navel, with the small intestine lying deep beneath; ST25 (Tianshu) is located 2 cun lateral to the navel on either side; RN06 (Qihai) is located on the anterior midline of the lower abdomen, 1.5 cun below the navel; RN04 (Guanyuan) is located on the anterior midline of the lower abdomen, 3 cun below the navel; ST36 (Zusanli) is located on the lateral aspect of the lower leg, 3 cun below the depression beneath the knee; ST37 (Shangjuxu) is located on the lateral aspect of the lower leg, 6 cun below the depression beneath the knee; BL20 (Pishu) is located 1.5 cun lateral to the spinous process of the eleventh thoracic vertebra on the back; BL25 (Dachangshu) is located 1.5 cun lateral to the spinous process of the fourth lumbar vertebra. |
ST25 (Tianshu), as the Front-Mu point of the large intestine, has been demonstrated to modulate inflammatory cytokines such as IL-6, IL-10, and TNF-α, thereby suppressing UCAC.89 It acts synergistically with ST37 (Shangjuxu), the Lower He-Sea point of the large intestine, to regulate gastrointestinal function.90 Furthermore, the combination of ST25 and ST36 (Zusanli) is frequently used in clinical practice. Based on the TCM principle of fortifying the spleen and harmonizing stomach qi, electroacupuncture stimulation at these two points has been confirmed to alleviate intestinal inflammatory injury and promote mucosal repair.91
Moxibustion involves stimulating specific acupoints with heat generated by burning mugwort (Artemisia vulgaris). It exerts warming and tonifying effects, particularly on spleen Yang, making it especially suitable for UC patients with spleen deficiency during the remission phase. It can also inhibit inflammation-driven colonic tumor growth. Key acupoints for moxibustion include: ST25, RN12 (Zhongwan), RN08 (Shenque), RN04 (Guanyuan), ST36, RN06 (Qihai), ST37, BL20 (Pishu), and BL25 (Dachangshu).92 Studies show that bilateral moxibustion at ST25 significantly reduces ROS levels in colonic tissue, mitigating oxidative stress damage.93 Additionally, combined moxibustion at ST25 and RN06 effectively suppresses the β-catenin and GSK-3β signaling pathways, inhibiting the occurrence of colitis-associated carcinogenesis and reducing tumor incidence.94
Mechanisms of TCM in Treating Colitis-Associated Carcinogenesis
Regulation of Gut Microbiota
The human gut harbors diverse microbial communities that play crucial roles in modulating the immune system, synthesizing nutrients, and regulating various host physiological processes.95,96 During the fermentation and breakdown of intestinal contents, gut microbes produce a range of small-molecule metabolites, such as SCFAs. These metabolites act as key signaling molecules that interact with immune cells to exert immunomodulatory effects and stimulate neurotransmitter release from the central nervous system, thereby facilitating gut–brain axis communication. Thus, the balance or dysbiosis of the gut microbiota is a critical factor in both the development and treatment of UCAC.97,98
Modulating Microbial Abundance and Diversity
UCAC patients show marked dysbiosis, with reduced bacterial diversity and enriched pathogens (eg, Bacteroides fragilis, Candida).99 Harmful metabolites (eg, hydrogen sulfide, colibactin) promote DNA damage, immune evasion, and chemotherapy resistance.100,101 Thus, an effective strategy of TCM to suppress UCAC is modulating microbial abundance and diversity, thereby restoring a balanced microbiota. Firstly, macromolecular compounds from Chinese herbal medicine (eg, polysaccharides) serve as “food” for beneficial bacteria in the gut. Their fermentation produces SCFAs, which lower the intestinal pH, thereby inhibiting the growth of many harmful bacteria. For instance, Ganoderma lucidum polysaccharides, extracted from its spores or fruiting bodies, elevate Bifidobacterium and Lactobacillus abundance in CAC mouse models, mitigating inflammation and tumor susceptibility.51 Secondly, TCM compound extracts, through multi-component and multi-target synergistic actions, establish a beneficial host-microbe feedback loop to enhance barrier function and reduce inflammation. For example, the Man Kuining formula, designed to tonify qi, detoxify, and improving blood circulation, enriches the beneficial Akkermansia in UC mice, restoring microbial equilibrium and promoting mucosal repair.102
Regulation of Gut Microbiota Metabolites
The gut microbiota modulates intestinal immune responses by producing diverse metabolites, thereby establishing dynamic immune homeostasis. The analysis on how TCM treats ulcerative colitis (UCAC) by regulating the metabolic products of intestinal microorganisms is as follows (Figure 4 and Table 3).
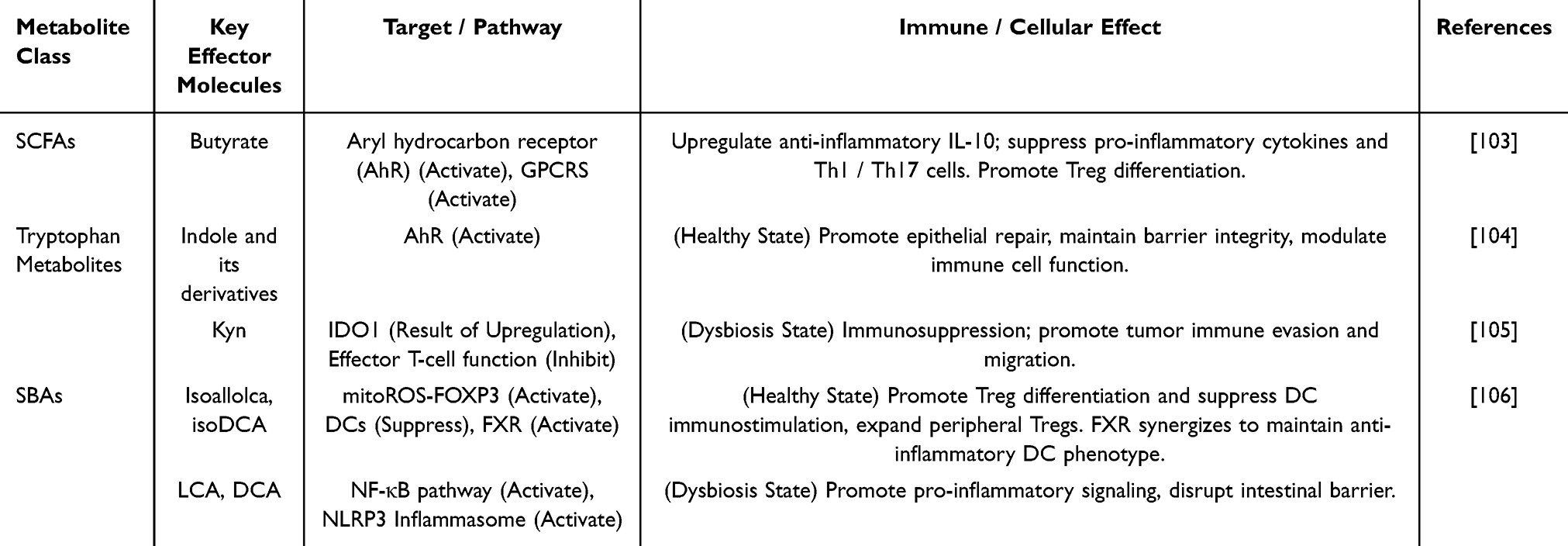 |
Table 3 Mechanisms of Gut Microbiota Metabolites in UCAC |
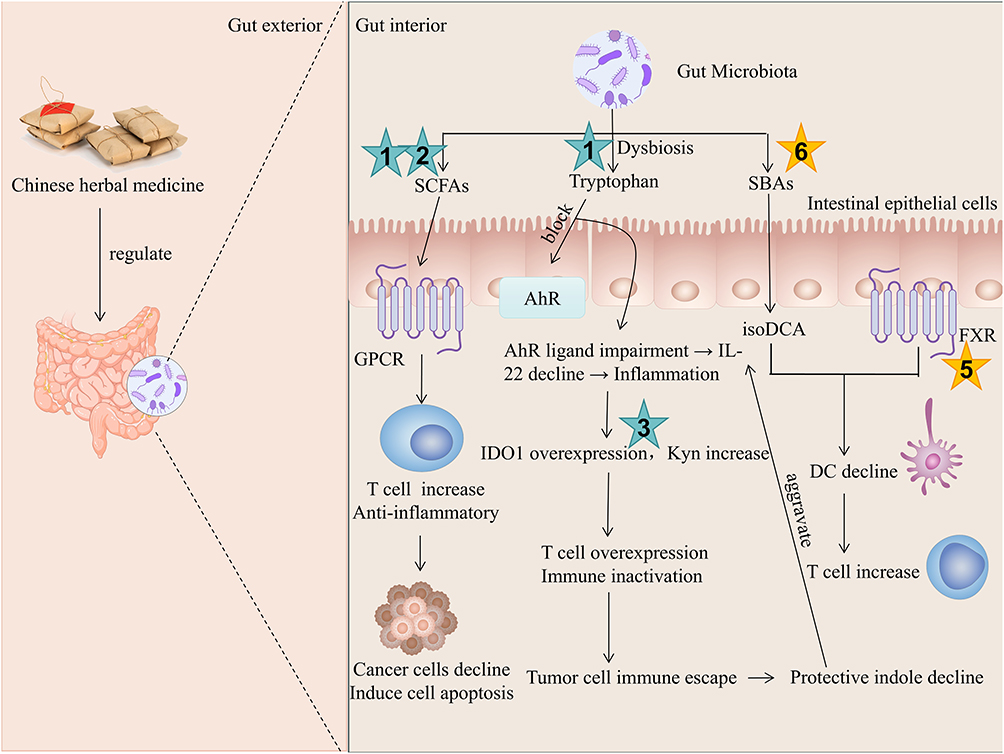 |
Figure 4 Schematic diagram of TCM regulating gut microbiota metabolites for the treatment of UCAC. Notes: Green Star 1: Ganoderma lucidum polysaccharide can increase short-chain fatty acid production and ameliorate AOM/DSS-induced microbiota dysbiosis;51 green Star 2: Astragalus polysaccharides can increase short-chain fatty acid production;107 green Star 3: Ginseng polysaccharides have the potential for reducing IDO activity and decreasing Kyn/Trp ratio;108 brown Star 5: Kuijiekang regulates intestinal FXR and affects bile acidmetabolism;109 brown Star 6: Huanglian Jiedu Decoction promotes the production of primary bile acids.110 |
SCFAs are primarily generated by gut microbiota through the fermentation of undigested fibers and resistant starch. Notably, butyrate, an SCFA produced by genera within the Firmicutes phylum (eg Faecalibacterium, Anaerostipes), plays a central role in maintaining intestinal homeostasis (Table 3).103 For instance, astragalus polysaccharides alleviate UC by increasing SCFA production and rebalancing Th17/Treg populations.107
Tryptophan is an essential amino acid. The gut microbiota can consume a portion of tryptophan and metabolize it primarily through kynurenine (Kyn), serotonin, and indole pathways, generating various catabolites influenced by microbial metabolism (Table 3).104,105,111 For example, ginseng polysaccharides can reduce IDO1 activity and Kyn production while modulating Treg levels, thereby slowing UCAC progression.108
Secondary bile acids (SBAs) (eg DCA and LCA) are microbial metabolites derived from the biotransformation of host-synthesized primary bile acids in the colon. SBAs exhibit dual roles, including anti-inflammatory effects via farnesoid X receptor (FXR)/Tregs and pro-inflammatory effects under dysbiosis (Table 3).106 For instance, Kuijiekang, composed of Poria, Atractylodis Macrocephalae Rhizoma, Citri Reticulatae Pericarpium, Paeoniae Radix Alba, Sanguisorbae Radix, Saposhnikoviae Radix and Notoginseng Radix et Rhizoma, has been shown to activate the intestinal FXR pathway to modulate bile acid metabolism and alleviate inflammation.109 Alternatively, Huanglian Jiedu Decoction, composed of Coptidis Rhizoma, Scutellariae Radix, Phellodendri Chinensis Cortex and Gardeniae Fructus, acts through multi-metabolic pathways, which modulates carbohydrate, amino acid, and fatty acid metabolism, promotes primary bile acid synthesis, and stimulates the proliferation of Clostridium species in the conversion of primary bile acids into SBAs. This process collectively establishes a positive feedback loop to restore overall metabolic balance.110
Molecular Mechanisms
The pharmacological mechanisms of TCM in treating UCAC mainly involve anti-inflammation, immune regulation, and inhibition of tumor cell activity and proliferation. Key pathways include NF-κB, IL-6/Janus kinase 2 (JAK2)/STAT3, Wnt/β-Catenin, and PI3K/Akt /mTOR signaling pathways.
NF-κB Signaling Pathway
TCM formulations and active constituents exert therapeutic effects by targeting critical nodes within the NF-κB pathway (Figure 5), such as the acetylation process of p65 and the phosphorylation of IκB kinase (IKK)-α/β.112,113 For instance, berberine—an alkaloid monomer—possesses a unique planar tetracyclic structure that allows it to intercalate into and bind specific functional domains of the p65 protein. This interaction inhibits p65 acetylation, ultimately suppressing the transcriptional activity of NF-κB and resulting in a targeted anti-inflammatory effect.114,115 Scutellaria barbata polysaccharide, a high-molecular-weight polysaccharide, contains specific carbohydrate chains that are likely recognized by pattern recognition receptors on immune cells. This recognition leads to upstream modulation of the IKK-IκB-NF-κB signaling cascade, markedly reversing the phosphorylation levels of key proteins and broadly suppressing the inflammatory response.116 Shenling Baizhu Powder, via the synergistic actions of its multiple bioactive components, inhibits the activation of IKK kinase. This inhibition blocks the phosphorylation and degradation of IκBα, effectively preventing NF-κB nuclear translocation and the transcription of inflammatory genes, thereby alleviating symptoms of IBD.117
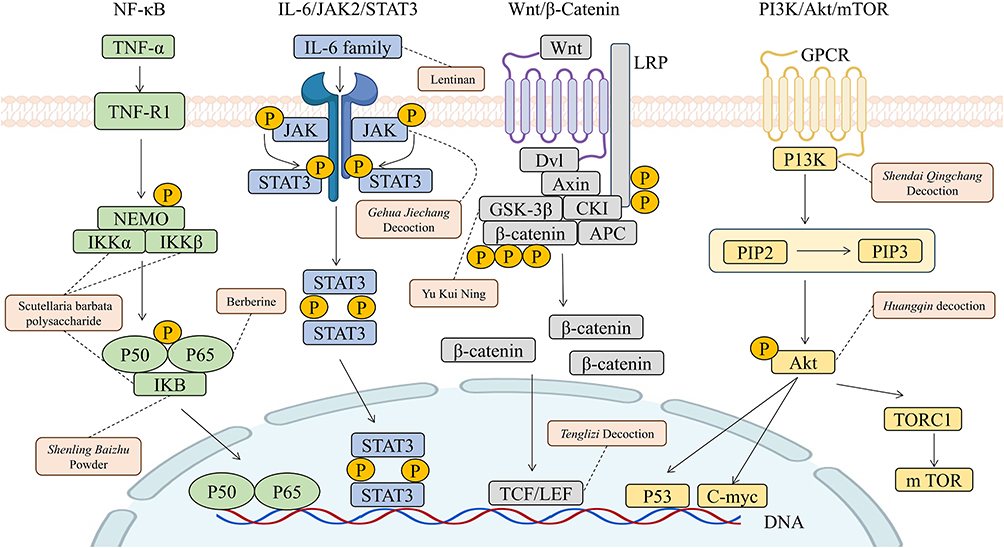 |
Figure 5 Schematic diagram of key targets in the four main signaling pathways of TCM treatment for UCAC. Notes: Green boxes indicate NF-κB pathway-related targets (Inflammation-related); blue boxes denote IL-6/JAK2/STAT3 pathway-related targets (Immune regulation related); gray boxes represent Wnt/β-catenin pathway-related targets (Proliferation-related); yellow boxes show PI3K/Akt/mTOR pathway-related targets (Survival and growth related); yellow circles indicate phosphorylation sites; Berberine reduces the acetylation of NF-κB subunit p65, leading to the inhibition of NF-κB translocation and transcriptional activity;114 Scutellaria barbata polysaccharide regulates the IKK-IκB-NF-κB signaling cascade;116 Shenling Baizhu Powder inhibits the degradation of IκBα;117 Lentinan reduces the level of IL-6;118 Gehua Jiechang Decoction inhibits JAK2 kinase phosphorylation to block STAT3 activation and nuclear translocation;119 Yu Kui Ning inhibits the level of GSK-3β to accelerate β-catenin phosphorylation and degradation;120 Compound Tenglizi Decoction disrupts the formation of a transcriptional complex with TCF/LEF;121 Shendai Qingchang Decoction reduces PI3K protein expression;122 Huangqin decoction inhibits Akt kinase activity.27 |
IL-6 / JAK2/STAT3 Signaling Pathway
Targeting the IL-6/STAT3 pathway (Figure 5) effectively inhibits UCAC progression by remodeling the immune microenvironment and blocking inflammation-driven carcinogenesis.123,124 For instance, lentinan, a β-glucan, is recognized by pattern recognition receptors (eg, Dectin-1) on immune cells due to its specific macromolecular polysaccharide structure. By modulating immune cell function, it significantly reduces serum levels of IL-6 and downstream pro-inflammatory cytokines IL-1β and IL-18 in CAC mouse models. This reduction diminishes the initial signal for STAT3 pathway activation, thereby remodeling the immune microenvironment and blocking the inflammation-driven carcinogenesis process.118 Similarly, active components in Gehua Jiechang Decoction—such as flavonoids (whose planar structures and phenolic hydroxyl groups enable competitive inhibition of ATP binding) and saponins (whose triterpenoid or steroidal structures may facilitate direct interaction with the JAK2 protein)—act synergistically. They directly or indirectly inhibit JAK2 kinase phosphorylation, block STAT3 activation and nuclear translocation, suppress the transcription of a suite of pro-oncogenic genes, and ultimately delay the progression from colitis to cancer.119 Notably, STAT3 synergizes with NF-κB via p65 acetylation to sustain pro-inflammatory signaling.125 This crosstalk exacerbates tumor-associated inflammation and cancer cell proliferation.
Wnt/β-Catenin Signaling Pathway
TCM formulations exert anti-UCAC effects by targeting key nodes of the Wnt/β-catenin pathway (Figure 5).126,127 For example, flavonoids and triterpenoid saponins in Compound Tenglizi Decoction utilize their phenolic hydroxyl and steroidal structures to directly or indirectly disrupt β-catenin stability or its formation of a transcriptional complex with TCF/LEF. This downregulates the expression of downstream pro-oncogenic proteins such as c-Myc and cyclin D1, ultimately inhibiting colorectal tumor growth.121 Alkaloids and glycosides in Yu Kui Ning Enema employ their specific chemical structures to inhibit the activity of upstream kinases like Akt or interfere with the stable interaction between Akt and GSK-3β. This relieves the inhibition on GSK-3β, restoring its kinase activity, accelerating β-catenin phosphorylation and degradation, suppressing aberrant Wnt/β-catenin signaling, and thereby ameliorating colitis.120
PI3K / Akt / mTOR Signaling Pathway
In the context of chronic inflammation, persistent activation of the maintains PI3K/Akt/mTOR (Figure 5) contributes to the uncontrolled survival and proliferation of tumor cells, accelerating the UCAC. Therefore, TCM formulations can intervene in the UCAC process by targeting multiple nodes of this pathway, such as suppressing PI3K transcription or inhibiting Akt phosphorylation.128–130 For example, flavonoids (eg, baicalin) in Huangqin decoction possess phenolic hydroxyl groups and planar structures that enable them to directly or indirectly inhibit Akt kinase activity, reducing its phosphorylation level. This relieves the suppression of apoptosis and promotes cancer cell death.27 Components such as saponins and alkaloids in Shendai Qingchang Decoction may regulate specific transcription factors (Saponins, with sugar chains and sapogenins, are amphiphilic and can bind to hydrophobic pockets of proteins, affecting cell and nuclear membrane permeability. Alkaloids, containing nitrogenous heterocyclic structures and often carrying a positive charge, readily interact with the phosphate backbone of DNA or negatively charged regions of proteins). This interaction interferes with the transcriptional process of the PI3K gene, reduces PI3K protein expression, and consequently attenuates the signaling intensity of the PI3K/Akt /mTOR pathway.122 Electroacupuncture stimulation at acupoints such as Zusanli (ST36) activates the body’s neuro-endocrine-immune regulatory network, eliciting broad biological effects. It downregulates multiple PI3K/AKT pathways-related genes, holistically suppressing the hyperactivation of this pathway at the transcriptional level, thereby alleviating intestinal inflammation. This provides a non-pharmacological physical intervention strategy for the prevention and treatment of UCAC, embodying the holistic theory of TCM.128
Other Relevant Pathways
The TLR4/MyD88/NF-κB, PPAR-γ, and NLRP3/Caspasee-1 pathways collectively constitute an inflammatory regulatory network in the intestine. When the intestinal barrier is compromised, pathogens or their components (eg, LPS) emerge as danger signals (PAMPs/DAMPs) and are first recognized by TLR4 on immune cell membranes. This immediately triggers the TLR4/MyD88 / NF-κB pathway, ultimately leading to the activation and nuclear translocation of the transcription factor NF-κB. The “priming signal” provided by NF-κB (eg, synthesis of NLRP3 components), combined with other stimuli (eg, ROS, K+ efflux, mitochondrial damage, often induced by TLR4 activation or tissue injury), co-stimulates the assembly of NLRP3, ASC, and pro-caspase-1 into a large protein complex—the NLRP3 inflammasome. Conversely, PPAR-γ antagonistically inhibits the progression of these pro-inflammatory pathways.131–133 TCM can intervene in UCAC by targeting key nodes across these different pathways. For instance, Curdlan polysaccharide, Sanhuang Xiexin Decoction, and oxymatrine (whose nitrogenous heterocyclic structure allows it to bind specific regions of the TLR4 receptor and interfere with MyD88 adaptor function) can modulate the expression of key proteins in the TLR4/MyD88/NF-κB pathway, such as TLR4, MyD88, and NF-κB.134–136 Ginsenoside Rg1 (whose steroidal sapogenin structure acts as a ligand to bind and activate the PPAR-γ receptor) and components of Huangqi Jianzhong Decoction can upregulate PPAR-γ expression, inhibit inflammatory stress and apoptosis, thereby protecting the colonic mucosa. In contrast, the activated NLRP3 inflammasome exacerbates inflammation and cell death by forming pores in the cellular and mitochondrial membranes, leading to swelling and cytokine release.137,138 Coptidis rhizoma and Scutellaria baicalensis in Banxia Xiexin Decoction are rich in flavonoids (eg, baicalin) and alkaloids (eg, berberine). The planar polycyclic structures and phenolic hydroxyl groups of these components enable them to inhibit the assembly of the NLRP3 inflammasome and the activation of Caspase-1.139 Furthermore, electroacupuncture combined with an intestinal-disease formula facilitates multi-dimensional “neuro-immune-epithelial” regulation. It initiates a systemic anti-inflammatory immune response through neural modulation, inhibits NLRP3 inflammasome proteins, reduces intestinal permeability in rats, and repairs the mucosal barrier.140
Conclusion and Perspectives
CAC remains a highly prevalent and lethal malignancy. Current standard therapies are often hampered by drug resistance, significant side effects, and high costs. In contrast, TCM guided by the principle of “disease prevention”, has the advantages like multi-target effects and low toxicity during the critical stage of colitis progressing to cancer. Based on TCM theory, this review systematically explains the pathogenesis and transformation process of UC turning into CAC and reviews therapies including oral administration (such as active ingredients like evodiamine and ginsenoside Rg1), external enemas, and acupuncture. It also summarizes related mechanistic studies, showing that TCM primarily inhibits inflammation-to-cancer transition by regulating gut microbiota and their metabolites, and by suppressing inflammation-related signaling pathways such as NF-κB and IL-6/JAK2/STAT3, demonstrating promising potential for prevention and treatment.
However, current research on UCAC still faces significant limitations. Most studies rely on a single animal model, lack in-depth mechanisms, and TCM research is largely at the stage of empirical medicine, with the active ingredients, structure–activity relationships, and mechanism of action still not clearly defined. To translate the empirical promise of TCM into rigorous, mechanistic science, we propose the following three interconnected research directions as critical pathways forward.
Future Direction 1: Establishing Standardized Research Models and Evaluation Systems for UCAC
A variety of animal and cellular models are currently employed to study UCAC, including chemically induced models (eg, AOM/DSS), genetically modified mice (eg, IL-10 KO), organoids, and humanized mouse models.141 Each model has distinct advantages and limitations in simulating different stages of UCAC pathogenesis. However, the lack of standardization across studies, in terms of model selection, induction protocols, endpoint assessments, and microbiota/immune reconstitution methods, has led to inconsistent results and hindered comparability between studies. For instance, variations in DSS concentration, administration cycles, and animal backgrounds can significantly influence disease phenotypes and therapeutic responses, complicating the translation of preclinical findings.
Therefore, future efforts should prioritize establishing standardized, reproducible, and clinically relevant model systems for UCAC research. Firstly, consensus protocols for widely used models need to be developed in order to harmonize induction regimens, monitoring parameters, and histopathological scoring criteria. Secondly, by using genetically stable and well-characterized animal strains, the effects of different species, strains, and ages of animals on the UCAC model need to be compared to obtain appropriate experimental subjects, thereby reducing the differences between laboratories. In addition, a reference dataset needs to be created to integrate multi-omics profiles (metagenomics, metabolomics, transcriptomics) from standardized models, enabling a systematic comparison of intervention effects across studies. The establishment of such standardized frameworks is a prerequisite for generating reliable and comparable preclinical data, which will form a solid foundation for the subsequent elucidation of mechanistic pathways.
Future Direction 2: Establishing a Holistic Mechanistic Research Framework Centered on “Microbiota-Metabolites-Target Pathways/Key Proteins”
Current research on the therapeutic mechanisms for UCAC primarily focuses on mitigating inflammation, restoring the mucosal barrier, and reestablishing gut microbiota homeostasis. However, existing studies on intestinal flora mainly examine the correlation between diseases and flora, with insufficient exploration of the relationships among intestinal flora, metabolites, and molecular signaling pathways. Emerging evidence suggests that active compounds from TCM, such as lentinan, can modulate the abundance of beneficial and pathogenic bacteria, thereby altering the production of key metabolites like SCFAs. These metabolites not only act locally on target cells to ameliorate the inflammatory milieu but also enter the systemic circulation, where they may directly or indirectly influence neurotransmitter release in the central nervous system. This hints at an integrated “microbiota-metabolite-immune/neuroregulation” mechanism. Nevertheless, this holistic pathway has not been experimentally validated in a connected manner, which limits the rigorous scientific interpretation and application of the systemic therapeutic advantages demonstrated by TCM formulations and extracts in clinical practice.
Importantly, the “microbiota-metabolite-target” research framework centered on TCM, as elucidated in this review, provides a systemic perspective complementary to mainstream Western medicine for the prevention and treatment of UCAC. While Western medical strategies often focus on intervening in highly specific molecular targets (eg, single cytokines or kinases), TCM aims to systemically reshape the host’s intestinal microenvironment and metabolic network through multi-component synergistic effects, thereby disrupting the “inflammation-cancer” transformation process.
Future research should strive to empirically construct and validate this integrated “microbiota-metabolite-target pathway/key protein” framework by employing systems biology technologies such as metagenomics and metabolomics. This will not only elucidate the multi-target, holistic regulatory mechanisms of TCM in modern scientific terms but also potentially offer a new paradigm to transcend the limitations of traditional “single-target” intervention thinking. Ultimately, it will lay a solid scientific foundation for establishing comprehensive prevention and treatment strategies based on the complementary strengths of Chinese and Western medicine.
Future Direction 3: Integrating Standardized Extraction and Quality Control with Structure-Activity Relationship (SAR) Research in TCM
This review synthesizes SAR and mechanisms of action of various TCM components, such as terpenoids and flavonoids, in the treatment of UCAC. It preliminarily reveals the intrinsic links between structural features (eg, rigid planar frameworks) and their anti-inflammatory and anti-tumor activities. However, current SAR research faces a fundamental bottleneck: the lack of standardized, chemically defined TCM extracts and purified compounds. Variability in extraction methods, raw material sources, and compositional profiles directly affects the consistency of bioactivity data, thereby obscuring true structure-activity correlations and hindering mechanistic validation. Without rigorous quality control and chemical standardization, SAR studies risk generating irreproducible or misleading results, which limits the reliability of subsequent drug design, structural modification, and clinical translation.
Therefore, future research must tightly couple standardized extraction and quality control systems with advanced SAR exploration. It is necessary to establish a chemical standardized library of TCM extracts. Through the design of quality-by-design methods, the chemical profile can be linked to biological activity, promoting the SAR research of standardized fractions and compounds, developing biomarkers for quality and efficacy assessment, in order to achieve the modernization and scientificization of TCM.
Beyond preclinical standardization and mechanistic elucidation, bridging the gap to clinical validation is paramount. However, a systematic search of major clinical trial registries (ClinicalTrials.gov, ChiCTR, WHO-ICTRP) confirms the absence of interventional clinical trials specifically evaluating TCM for UCAC. Current clinical research on UCAC remains predominantly observational, centered on elucidating its pathogenesis and diagnostic markers. Conversely, clinical investigations of TCM or integrative therapies are almost exclusively focused on managing mild-to-moderate or active UC (eg, trials involving Kuijie Fang). Therefore, future research must prioritize two sequential goals: first, achieving a consensus on the pathogenesis and diagnostic criteria for UCAC; second, initiating long-term cohort studies to track cancer risk in UC patients undergoing TCM therapy. Ultimately, prospectively designed, prevention-focused trials in high-risk populations are indispensable for generating robust clinical evidence on TCM’s potential to mitigate UCAC, laying the foundation for a scientific and systematic evaluation of its efficacy.
In summary, this review provides a systematic evaluation of TCM’s theoretical, applied, and mechanistic landscape in UCAC. By pursuing the integrated research avenues outlined above—ranging from “standardized models” and “holistic mechanistic frameworks” to “chemistry-led quality control and SAR”—we can better elucidate TCM’s mechanisms in contemporary biomedical terms. This concerted effort will derive actionable insights from natural products and accelerate the translation of basic research into clinically validated TCM strategies and TCM-inspired drug development.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We thank National Key R&D Program of China [Grant No. 2022YFC3501705], Shanghai Leading Talents Program [Grant No. SHLJ2019100] and Shanghai Rising-Star Program (Sailing Special Program) [Grant No. 24YF2741000] for financial support.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–23. doi:10.3322/caac.21834
2. Liu RF, Sun XZ, Mo Y, et al. Global estimates of incidence and mortality of colorectal cancer and its risk factors[J]. Chin. J. Cancer Prev. Treat. 2025;32(08):462–469. doi:10.16073/j.cnki.cjcpt.2025.08.02
3. Singh A. Global burden of five major types of gastrointestinal cancer. Prz Gastroenterol. 2024;19(3):236–254. doi:10.5114/pg.2024.141834
4. Schmitt M, Greten FR. The inflammatory pathogenesis of colorectal cancer. Nat Rev Immunol. 2021;21(10):653–667. doi:10.1038/s41577-021-00534-x
5. Neganova M, Liu J, Aleksandrova Y, et al. Therapeutic influence on important targets associated with chronic inflammation and oxidative stress in cancer treatment. Cancers. 2021;13(23):6062. doi:10.3390/cancers13236062
6. Hashimoto S, Hashimoto A, Muromoto R, et al. Central roles of STAT3-mediated signals in onset and development of cancers: tumorigenesis and immunosurveillance. Cells. 2022;11(16). doi:10.3390/cells11162618
7. Shan Y, Xie T, Sun Y, et al. Lipid metabolism in tumor-infiltrating regulatory T cells: perspective to precision immunotherapy. Biomark Res. 2024;12(1):41. doi:10.1186/s40364-024-00588-8
8. Hanahan D. Hallmarks of cancer: new dimensions. Cancer Discov. 2022;12(1):31–46. doi:10.1158/2159-8290.CD-21-1059
9. Inflammatory Bowel Disease Group. Chinese clinical practice guideline on the management of ulcerative colitis(2023,Xi’an). Chin. J. Inflamm. Bowel Dis. 2024;8(1):33–58. doi:10.3760/cma.j.cn101480-20240123-00017.
10. Zhu S, Yang Z, Liu Y, et al. Oral lipid nanoparticles for improving the efficiency of drug delivery systems in ulcerative colitis: recent advances and future prospects. Pharmaceutics. 2025;17(5):547. doi:10.3390/pharmaceutics17050547
11. Xue L, Williamson A, Gaines S, et al. An update on colorectal cancer. Curr Probl Surg. 2018;55(3):76–116. doi:10.1067/j.cpsurg.2018.02.003
12. Wang S, Wu W. Research progress and problems of chinese herbal compound for the treatment of cancer. J Oncol Chin Med. 2022;4(6):59–65. doi:10.19811/j.cnki.ISSN2096-6628.2022.11.010
13. Zuo Z, Jia J, Li H, et al. Adjuvant effects of Chinese medicinal tonics on gastric, liver, and colorectal cancers-OMICs-based contributions to understanding their mechanism of action. Front Pharmacol. 2022;13:986765. doi:10.3389/fphar.2022.986765
14. Yang Y, Zhao M, Kuang Q, et al. A comprehensive review of phytochemicals targeting macrophages for the regulation of colorectal cancer progression. Phytomedicine. 2024;128:155451. doi:10.1016/j.phymed.2024.155451
15. Cui Z, Yan J, Long S, et al. Study on the pathogenesis of ulcerative colitis associated colon cancer based on latent evil theory. J Basic Chin Med. 2021;27(11):1715–1716+1773. doi:10.19945/j.cnki.issn.1006-3250.2021.11.008
16. Xie J, Xu X, Ai F, et al. Pathogenesis and treatment of “inflammation cancer transformation” of ulcerative colitis based on “Kenang” theory. China J Chin Mater. 2025:1–8. doi:10.19540/j.cnki.cjcmm.20250206.501.
17. Zhang X, Liu S. Clinical study on the treatment of ulcerative colitis with syndrome of internal retention of dampness-heat with dampness-resolving and toxin-removing decoction. Henan Tradit. Chin. Med. 2024;44(02):249–253. doi:10.16367/j.issn.1003-5028.2024.02.0048
18. Song W. Clinical study of compound kushen injection combined with chemotherapy in treatment of advanced colon cancer. Liaoning J Tradit Chin Med. 2021;48(08):159–160. doi:10.16367/j.issn.1003-5028.2024.02.0048
19. Huang T, Tang W, Chen J, et al. Observation on the efficacy of enema with qingre qushi recipe combined with xilei powder in the treatment of mild to moderate damp-heat syndrome of ulcerative colitis. Clin Misdiagn Misther. 2025;38(09):92–96. doi:10.3969/j.issn.1002-3429.2025.09.016
20. Yang N, Wang Z, Yang B, et al. Clinical Efficacy of Modified Sijunzi Decoction in Treatment of Patients with Ulcerative Colitis and Its Regulatory Effect on Intestinal flora. World J. Tradit. Chin. Med. 2024;10(01):134–139. doi:10.13935/j.cnki.sjzx.240123
21. Chen T, Wang Z, Peng Y, et al. Clinical effects of supplemented gegen qinlian decoction combined with acupuncture on patients with ulcerative colitis of large intestinal dampness-heat pattern. Chin Tradit Pat Med. 2025;47(02):453–457. doi:10.3969/j.issn.1001-1528.2025.02.014
22. Jiang D, Xu C, Shen W, et al. Explore protective mechanism of Shenbai Jiedu decoction on colon epithelial cells of ulcerative colitis. Shaanxi J Tradit Chin Med. 2022. doi:10.3969/j.issn.1000-7369.2022.01.005
23. Liu J, Shen W, Cheng H, et al. Shenbai Jiedu Fang inhibits AOM/DSS-induced colorectal adenoma formation and carcinogenesis in mice via miRNA-22-mediated regulation of the PTEN/PI3K/AKT signaling pathway. J South Med Univ. 2022. doi:10.12122/j.issn.1673-4254.2022.10.03
24. Huang S, Lu A, Wang D, et al. Study on the repair mechanism of shaoyao decoction on mucosal barrier in ulcerative colitis based on MAPK/ERK pathway. J Zhejiang Chin Med Univ. 2022;46(12):1301–1309+1319. doi:10.16466/j.issn1005-5509.2022.12.001
25. Wang C, He S, Cheng X, et al. Effect of Shaoyao Decoction on apoptosis,cloning,migration and invasion of HT29 cells of colon cancer. Lishizhen Med. Mater. Med. Res. 2024;35(11):2545–2551.
26. Liu P, Zhang D, Zhou J, et al. Effect observation of mume pill combined with chemotherapy on patients with ulcerative colitis associated colorectal cancer with cold-heat complex syndrome. Acta Chin Med Pharmacol. 2024.
27. Wang D, Zhu L, Liu H, et al. Huangqin tang alleviates colitis-associated colorectal cancer via amino acids homeostasisand PI3K/AKT/mtor pathway modulation. J Ethnopharmacol. 2024;334:118597. doi:10.1016/j.jep.2024.118597
28. Duan Y, Lu Y, Liu Z, et al. Qingre Huayu Jianpi prescription alleviates the inflammatory transformation of colitis-associated colorectal cancer by inhibiting the IL-17RA/ACT1/NF-κB axis. J Ethnopharmacol. 2025;345:119554.
29. Miao Z, Chen L, Feng H, et al. Baitouweng decoction ameliorates ulcerative colitis in mice partially attributed to regulating th17/treg balance and restoring intestinal epithelial barrier. Front Pharmacol. 2020;11:531117. doi:10.3389/fphar.2020.531117
30. Liu L, Chen Y, Liu S, et al. Therapeutic potential of pien tze huang in colitis-associated colorectal cancer: mechanistic insights from a mouse model. Cancer Cell Int. 2024;24(1):250. doi:10.1186/s12935-024-03428-9
31. Chen X, Wang C, Yang B, et al. Mechanism of shaoyaotang in modulating MDSCs-related Immunosuppressive microenvironment in prevention and treatment of colitis-associated carcinogenesis. Chin J Exp Tradit Med Formulae. 31;01:10–19.
32. Dong M, Liu H, Cao T, et al. Huoxiang Zhengqi alleviates azoxymethane/dextran sulfate sodium-induced colitis-associated cancer by regulating Nrf2/NF-κB/NLRP3 signaling. Front Pharmacol. 2022;13:1002269. doi:10.3389/fphar.2022.1002269
33. Wei X, Liang J, Liu J, et al. Anchang Yuyang Decoction inhibits experimental colitis-related carcinogenesis by regulating PPAR signaling pathway and affecting metabolic homeostasis of host and microbiota. J Ethnopharmacol. 2024;326:117995. doi:10.1016/j.jep.2024.117995
34. Zhang MM, Yin DK, Rui XL, et al. Protective effect of Pai-Nong-San against AOM/DSS-induced CAC in mice through inhibiting the Wnt signaling pathway. Chin J Nat Med. 2021;19(12):912–920. doi:10.1016/S1875-5364(22)60143-2
35. Yang L, Zhan Y, Yu H, et al. Effects of Coix lacryma epiphyllum septicum on colon carcinogenesis in mice with colitis carcinoma transformation model through regulating NF-κB signaling pathway. Chin Tradit Pat Med. 2023;45(12):4131–4136.
36. Jiang YF, Huang YQ, Hu YE, et al. Banxia xiexin decoction inhibiting colitis-associated colorectal cancer infected with fusobacterium nucleatum by regulating Wnt/β-catenin pathway. Zhongguo Zhong Yao Za Zhi. 2024;49(5):1266–1274. doi:10.19540/j.cnki.cjcmm.20231114.701
37. Liu H, Yang R, Zhong H, et al. Mechanism of qingjie fuzheng granules in inhibiting colitis associated colorectal cancer by regulating TLR4 and IL-4R mediated macrophage polarization. J Ethnopharmacol. 2025;344:119511. doi:10.1016/j.jep.2025.119511
38. Xu Z, Zhao G, Zhang L, et al. Tong-Xie-Yao-Fang induces mitophagy in colonic epithelial cells to inhibit colitis-associated colorectal cancer. J Ethnopharmacol. 2024;334:118541. doi:10.1016/j.jep.2024.118541
39. Liu H, Yan S, Yang R, et al. Jiedu xiaozheng yin inhibits the progression of colitis associated colorectal cancer by stimulating macrophage polarization towards an m1 phenotype via the tlr4 pathway. Integr Cancer Ther. 2024;23:15347354241247061. doi:10.1177/15347354241247061
40. Zhang X, Chen Y, Li Z, et al. Analysis of therapeutic mechanism of Liushen Wan against colitis-associated colorectal cancer based on network pharmacology and validation in mice. J Southern Med Univ. 2023. doi:10.12122/j.issn.1673-4254.2023.07.01
41. Wu H, Zhong S, Huo J, et al. Prevention effect of sanghuang aqueous extract on acute ulce-rative colitis in mice and its underling mechanism. Acta Sericol Sin. 2021;47(03):247–254. doi:10.13441/j.cnki.cykx.2021.03.006
42. Yang X, Wang Q, Zhang X, et al. Purple yam polyphenol extracts exert anticolitis and anticolitis-associated colorectal cancer effects through inactivation of NF-κB/p65 and STAT3 Signaling Pathways. J Agric Food Chem. 2023;71(32):12177–12189. doi:10.1021/acs.jafc.3c00346
43. Yun X, Zhang Q, Fang Y, et al. Madecassic acid alleviates colitis-associated colorectal cancer by blocking the recruitment of myeloid-derived suppressor cells via the inhibition of IL-17 expression in γδT17 cells. Biochem Pharmacol. 2022;202:115138. doi:10.1016/j.bcp.2022.115138
44. Chen YL, Xu B, Pan ZF, et al. Glycyrrhizic acid reduces neutrophil extracellular trap formation to ameliorate colitis-associated colorectal cancer by inhibiting peptidylarginine deiminase 4. J Ethnopharmacol. 2025;341:119337. doi:10.1016/j.jep.2025.119337
45. Li XM, Yuan DY, Liu YH, et al. Panax notoginseng saponins prevent colitis-associated colorectal cancer via inhibition IDO1 mediated immune regulation. Chin J Nat Med. 2022;20(4):258–269. doi:10.1016/S1875-5364(22)60179-1
46. Liang J, Yang C, Li P, et al. Astragaloside IV inhibits AOM/DSS-induced colitis-associated tumorigenesis via activation of PPARγ signaling in mice. Phytomedicine. 2023;121:155116. doi:10.1016/j.phymed.2023.155116
47. Li H, Xing X, Zhang X, et al. Effects of triptolide on the sphingosine kinase - Sphingosine-1-phosphate signaling pathway in colitis-associated colon cancer. Int Immunopharmacol. 2020;88:106892. doi:10.1016/j.intimp.2020.106892
48. Bai B, Wu F, Ying K, et al. Therapeutic effects of dihydroartemisinin in multiple stages of colitis-associated colorectal cancer. Theranostics. 2021;11(13):6225–6239. doi:10.7150/thno.55939
49. Wan Z, Zheng G, Zhang Z, Ruan Q, Wu B, Wei G. Material basis and core chemical structure of Dendrobium officinale polysaccharides against colitis-associated cancer based on anti-inflammatory activity. Int J Biol Macromol. 2024;262(Pt 2):130056. doi:10.1016/j.ijbiomac.2024.130056
50. Qin Z, Yuan X, Liu J, et al. Albuca bracteata polysaccharides attenuate AOM/DSS induced colon tumorigenesis via regulating oxidative stress, inflammation and gut microbiota in mice. Front Pharmacol. 2022;13:833077. doi:10.3389/fphar.2022.833077
51. Guo C, Guo D, Fang L, et al. Ganoderma lucidum polysaccharide modulates gut microbiota and immune cell function to inhibit inflammation and tumorigenesis in colon. Carbohydr Polym. 2021;267:118231. doi:10.1016/j.carbpol.2021.118231
52. Yu Z, Yue B, Gao R, et al. Gastrodin attenuates colitis and prevents tumorigenesis in mice by interrupting TLR4/MD2/NF-κB signaling transduction. Anticancer Agents Med Chem. 2024;24(11):853–866. doi:10.2174/0118715206286233240328045215
53. Lu Y, Guan T, Xu S, et al. Asperuloside inhibited epithelial-mesenchymal transition in colitis associated cancer via activation of vitamin D receptor. Phytomedicine. 2022;101:154070. doi:10.1016/j.phymed.2022.154070
54. Si XL, Wang Y, Song BN, et al. Potential chemoprevention of paeoniflorin in colitis-associated colorectal cancer by network pharmacology, molecular docking, and in vivo experiment. Chem Biodivers. 2022;19(8):e202200295. doi:10.1002/cbdv.202200295
55. Jin BR, Chung KS, Hwang S, et al. Rosmarinic acid represses colitis-associated colon cancer: a pivotal involvement of the TLR4-mediated NF-κB-STAT3 axis. Neoplasia. 2021;23(6):561–573. doi:10.1016/j.neo.2021.05.002
56. Pu Z, Zhang W, Wang M, et al. Schisandrin B attenuates colitis-associated colorectal cancer through SIRT1 Linked SMURF2 signaling. Am J Chin Med. 2021;49:1773–1789. doi:10.1142/S0192415X21500841
57. Qiao S, Lv C, Tao Y, et al. Arctigenin disrupts NLRP3 inflammasome assembly in colonic macrophages via downregulating fatty acid oxidation to prevent colitis-associated cancer. Cancer Lett. 2020;491:162–179. doi:10.1016/j.canlet.2020.08.033
58. Zeng S, Chen L, Sun Q, et al. Scutellarin ameliorates colitis-associated colorectal cancer by suppressing Wnt/β-catenin signaling cascade. Eur J Pharmacol. 2021;906:174253. doi:10.1016/j.ejphar.2021.174253
59. Cai J, Ren Y, Li J, et al. Quercetin regulates IL-6/STAT3 signaling pathway in mouse models of inflammation-related colon cancer:a mechanistic study. Chin Rem Clin. 2020;20(06):896–899. doi:10.11655/zgywylc2020.06.006
60. Lu N, Jin Z, Zhang Y, et al. Effects of gentianopsis paludosa xanthone on the expression of TGF-β1/Smad Pathway and EMT factors during the evolution of ulcerative colitis-related intestinal fibrosis to CAC in rats. Pharmacol Clin Chin Mater Med. 2020;40(07):63–67. doi:10.11655/zgywylc2020.06.006
61. Deng J, Zhao L, Yuan X, et al. Pre-administration of berberine exerts chemopreventive effects in AOM/DSS-induced colitis-associated carcinogenesis mice via modulating inflammation and intestinal microbiota. Nutrients. 2022;14(4):726. doi:10.3390/nu14040726
62. Wang M, Zhou B, Cong W, et al. Amelioration of AOM/DSS-induced murine colitis-associated cancer by evodiamine intervention is primarily associated with gut microbiota-metabolism-inflammatory signaling axis. Front Pharmacol. 2021;12:797605. doi:10.3389/fphar.2021.797605
63. Liu L, Gao H, Wen T, et al. Tanshinone IIA attenuates AOM/DSS-induced colorectal tumorigenesis in mice via inhibition of intestinal inflammation. Pharm Biol. 2021;59(1):89–96. doi:10.1080/13880209.2020.1865412
64. Zhang Y, Pu W, Bousquenaud M, et al. Emodin inhibits inflammation, carcinogenesis, and cancer progression in the AOM/DSS model of colitis-associated intestinal tumorigenesis. Front Oncol. 2020;10:564674. doi:10.3389/fonc.2020.564674
65. Jiang N, Li S, Meng L, et al. Gamabufotalin inhibits colitis-associated colorectal cancer by suppressing transcription factor STAT3. Eur J Pharmacol. 2024;966:176372. doi:10.1016/j.ejphar.2024.176372
66. Qin Y, Yu Y, Yang C, et al. Atractylenolide I Inhibits NLRP3 inflammasome activation in colitis-associated colorectal cancer via suppressing drp1-mediated mitochondrial fission. Front Pharmacol. 2021;12:674340. doi:10.3389/fphar.2021.674340
67. McDonald SJ, Bullard BM, VanderVeen BN, et al. Panaxynol alleviates colorectal cancer in a murine model via suppressing macrophages and inflammation. Am J Physiol Gastrointest Liver Physiol. 2023;325(4):G318–G333. doi:10.1152/ajpgi.00119.2023
68. Liu B, Zhang C, Ma K, et al. Mechanism of action of paeonol in alleviating colitis-related colorectal cancer in mice: an analysis based on the STAT-3/NF-κB/ICAM-1 pathway. J Anhui Univ Chin Med. 2021. doi:10.3969/j.issn.2095-7246.2021.01.022
69. Yang Q, Wang Y, Zhang Z, et al. Terpenoids from Euphorbia wallichii and their anti-inflammatory therapeutic potential. Fitoterapia. 2025;185:106725. doi:10.1016/j.fitote.2025.106725
70. Liu C, Wu X, Liu J, et al. Research progress on anti-inflammatory activity mechanism and structure-activity relationship of plant polysaccharides. Sci Technol Food Ind. 2022;43(11):415–425.
71. Wang J, Wang F, Du P, et al. Research progress on synthesis and anti-tumor effects of panax notoginseng saponins and their derivatives. Chin Arch Tradit Chin Med. 2025;43:248–254. doi:10.13193/j.issn.1673-7717.2025.04.041
72. Li C, Xu G, Zhang H, et al. Progress on the structural characterization and antitumor activity of dendrobium polysaccharide. J. Hainan Norm. Univ. 2024;37:482–490. doi:10.12051/j.issn.1674-4942.2024.04.011
73. Yan X, Jiang S, Liu X, et al. Research progress on structure-activity relationship,extraction technology and pharmacological action of ganoderma lucidum polysaccharide. Acta Chin Med Pharmacol. 2024;52:117–122. doi:10.19664/j.cnki.1002-2392.240085
74. Wang X, Song L, Yang Z. Research progress in structural modification of Gastrodin. Chin J Ethnomedicine Ethnopharm. 2016;25:55–58. doi:10.3969/j.issn.1007-8517.2016.6.zgmzmjyyzz201606021
75. Li J, Qin CF, Chen ND. Evaluation of antioxidant, antidiabetic and antiobesity potential of phenylpropanoids (PPs): structure-activity relationship and insight into action mechanisms against dual digestive enzymes by comprehensive technologies. Bioorg Chem. 2024;146:107290. doi:10.1016/j.bioorg.2024.107290
76. Li Y, Cao R, Mao Y, et al. Research progress on structural modification and biological activity of quercetin. CHM. 2023;54:1636–1653. doi:10.7501/j.issn.0253-2670.2023.05.030
77. Liu X, Jia M, Liang J. Research progress on the synthesis of protoberberine skeleton and its anti-inflammatory activity. Chin J Org Chem. 2023;43:1325–1340. doi:10.6023/cjoc202209037
78. Hu Y. Study on the Molecular Mechanism and structure-activity Relationship of yellow anthraquinone Compounds in inhibiting LPS-induced Inflammatory response in macrophages. Chengdu Univ Tradit Chin Med. 2019. doi:10.26988/d.cnki.gcdzu.2019.000070
79. Li N, Shen L, Niu L, et al. Impact of hepatic-intestinal first-pass effect on the bioavailability of schizandrin in rats. Nanjing Univ Tradit Chin Med. 2022;38(03):228–235. doi:10.14148/j.issn.1672-0482.2022.0228
80. Zhuge W, Ding Y, Zheng L, et al. Therapeutic effect of xilei powder and berberine enema in treatment of ulcerative colitis. Liaoning J Tradit Chin Med. 2025. doi:10.13192/j.issn.1000-1719.2025.06.027
81. Yang Z, Wang Q, Yang C, et al. Study on the regulatory effect of Yuxian Formula on retention enema on PXR/NF-κB signaling pathway and inflammatory factors in rats with ulcerative colitis of damp-heat type in large intestine. Beijing J Tradit Chinese Med. 42(08):847–851. doi:10.16025/j.1674-1307.2023.08.008
82. Li G, Ma T, Zhang H, et al. Mechanism of action of acupuncture Tianshu point combined with medium frequency electrical stimulation to improve intestinal dysfunction after spinal cord injury. Liaoning J Tradit Chin Med. 1–19.
83. Yang Y, Rao X, Liu D, et al. Bibliometric analysis of clinical treatment scop and rules of shenque(RN8)in recent 5 years. J Traditional Chinese Med Pharm. 2023;29(05):194–203. doi:10.13862/j.cn43-1446/r.2023.05.044
84. Huang J, Diao L. Clinical effect of acupoint application combined with Wumei Pills concoction in the treatment of ulcerative colitis mixed with cold and heat type. China Modern Med. 2024. doi:10.3969/j.issn.1674-4721.2024.10.025
85. Wang H, Li Z. Clinical observation on the treatment of ulcerative colitis by auricular pressure bean combined with enema of Tongguang soup. Shanxi J. Tradit. Chin. Med. 2022;38(11):44–45. doi:10.20002/j.issn.1000-7156.2022.11.017
86. Dou L. Safety and efficacy of mesalazine enteric-coated tablets+auricular point pressing bean+Chinese medicine retention enema in the treatment of patients with ulcerative colitis. CHINA MED Pharm. 2023;(12). doi:10.3969/j.issn.2095-0616.2023.12.016
87. Qiu Q, Xu L, Sang F, et al. Clinical research progress and prospect of TCM herbal atomizing inhalation in treatment of respiratory diseases. Liaoning J Tradit Chin Med. 2024;51(11):213–216. doi:10.13192/j.issn.1000-1719.2024.11.053
88. Wen T, Wu H, Zhu J, et al. Effect of Atomization Inhalation of Huajiao (Zanthoxylum bungeanum) Essential Oil on Inflammatory and Cancer Transformation in CAC Mice and Its Mechanism. Chin Arch Tradit Chin Med. 2022;40(10):77–81+264–265. doi:10.13193/j.issn.1673-7717.2022.10.017
89. Han X, Wang Q. Analysis of the expression of inflammatory factors in rats with ulcerative colitis treated with acupuncture at tianshu(ST25). Information Tradit. Chin. Med. 2025;42(01):8–11+24. doi:10.19656/j.cnki.1002-2406.20250102
90. Xu A, Li Y, Yang J, et al. Tianshu(ST 25)and Shangjuxu(ST 37)as basic acupoints in the treatment of gastrointestinal diseases:a review. WJTCM. 2022;17(21):3096–3100. doi:10.3969/j.issn.1673-7202.2022.21.020
91. Wang X, Liu J, Qu Y, et al. Electroacupuncture improves colonic mucosal barrier damage by regulating NLRP3/Caspase-1/GSDMD signaling pathway and inhibiting pyroptosis in ulcerative colitis mice. Acupuncture Res. 2025;50(03):277–286. doi:10.13702/j.1000-0607.20240402
92. Zhang J, Zhu W, Wang X, et al. Current status of research and reflection on moxibustion in the treatment of ulcerative colitis. WJTCM. 2024;19(19):3039–3044. doi:10.3969/j.issn.1673-7202.2024.19.025
93. Liu L, Lu Y, Cao Y, et al. Effects of Moxibustion at “Tianshu” (ST25)on ferroptosis and oxidative damage in colon tissue of ulcerative colitis model rats. J Traditional Chin Med. 2023.
94. Lu Y, Gu M, Ding B, et al. Research on the effects of moxibustion on P2X7 receptor and wnt/β-catenin signaling pathway in colitis-associated cancer rats. Shanghai J Acupuncture Moxibustion. 2020;39(06):758–765. doi:10.13460/j.issn.1005-0957.2020.13.1042
95. Adak A, Khan MR. An insight into gut microbiota and its functionalities. Cell Mol Life Sci. 2019;76(3):473–493. doi:10.1007/s00018-018-2943-4
96. Ramsteijn AS, Louis P. Dietary fibre optimisation in support of global health. Microb Biotechnol. 2024;17(8):e14542. doi:10.1111/1751-7915.1454
97. Lloyd-Price J, Arze C, Ananthakrishnan AN, et al. Multi-omics of the gut microbial ecosystem in inflammatory bowel diseases. Nature. 2019;569(7758):655–662. doi:10.1038/s41586-019-1237-9
98. Tang X, Ren Y, He M, et al. Evaluation on the efficacy and advantages and mechanisms of tcm in preventing and treating “inflammation-cancer transformation” of colorectal adenoma-colorectal cancer. Chin J Inf Tradit Chin Med. 2025;32(02):20–24. doi:10.19879/j.cnki.1005-5304.202401278
99. Shen H, Zhu L, Xing J, et al. Strategies and methods of Traditional Chinese Medicine in the prevention and treatment of ulcerative colitis associated colorectal cancer. Chin J Integr Tradit West Med Dig. 2023;31(03):157–162.
100. De oliveira alves N, Dalmasso G, Nikitina D, et al. The colibactin-producing Escherichia coli alters the tumor microenvironment to immunosuppressive lipid overload facilitating colorectal cancer progression and chemoresistance. Gut Microbes. 2024;16(1):2320291. doi:10.1080/19490976.2024.2320291
101. Duizer C, De Zoete MR. The role of microbiota-derived metabolites in colorectal cancer. Int J Mol Sci. 2023;24(9):8024. doi:10.3322/caac.21834
102. Huang Y, Ji Y, Chen G, et al. Effect of mankuining decoction on expression of inflammatory factors and intestinal flora in mice with ulcerative colitis. Chin J Exp Tradit Med. 2022;28(12):86–95.
103. Singh V, Lee G, Son H, et al. Butyrate producers, “The Sentinel of Gut”: their intestinal significance with and beyond butyrate, and prospective use as microbial therapeutics. Front Microbiol. 2023;13:1103836. doi:10.3389/fmicb.2022.1103836
104. Agus A, Planchais J, Sokol H. Gut microbiota regulation of tryptophan metabolism in health and disease. Cell Host Microbe. 2018;23(6):716–724. doi:10.1016/j.chom.2018.05.003
105. Wyatt M, Greathouse KL. Targeting dietary and microbial tryptophan-indole metabolism as therapeutic approaches to colon cancer. Nutrients. 2021;13(4):1189. doi:10.3390/nu13041189
106. Cai J, Sun L, Gonzalez FJ. Gut microbiota-derived bile acids in intestinal immunity, inflammation, and tumorigenesis. Cell Host Microbe. 2022;30(3):289–300. doi:10.1016/j.chom.2022.02.004
107. Shin Y, Han S, Kwon J, et al. Roles of short-chain fatty acids in inflammatory bowel disease. Nutrients. 2023;15(20):4466. doi:10.3390/nu15204466
108. Huang J, Liu D, Wang Y, et al. Ginseng polysaccharides alter the gut microbiota and kynurenine/tryptophan ratio, potentiating the antitumour effect of antiprogrammed cell death 1/programmed cell death ligand 1 (anti-PD-1/PD-L1) immunotherapy. Gut. 2022;71(4):734–745. doi:10.1136/gutjnl-2020-321031
109. Xu R, Li X, Ma J, et al. Kui Jie Kang regulates intestinal FXR and affects bile acidmetabolism in treatment of ulcerative colitis in mice. Chin Pharmacol Bull. 2025. doi:10.12360/CPB202407041
110. Yang Y, Du H, Zhang G, et al. Exploring the changes in gut microbiota and metabolites of rats treated with huanglian jiedu decoction based on 16s sequencing and non targeted metabolomics. Modernization oTradit Chin Med Materia Medica-World Sci Technol. 2024. doi:10.11842/wst.20230606005
111. Gu J, Liu M, Liu X, et al. Study on mechanism of tryptophan metabolism regulating immune function and its application in pig production. Chin J Anim Nutr. 2024. doi:10.12418/CJAN2024.522
112. Guo Q, Jin Y, Chen X, et al. NF-κB in biology and targeted therapy: new insights and translational implications. Signal Transduct Target Ther. 2024;9(1):53. doi:10.1038/s41392-024-01757-9
113. Mussbacher M, Derler M, Basílio J, et al. NF-κB in monocytes and macrophages - an inflammatory master regulator in multitalented immune cells. Front Immunol. 2023;14:1134661. doi:10.3389/fimmu.2023.1134661
114. Zhang S, Xu P, Zhu Z, et al. Acetylation of p65Lys310 by p300 in macrophages mediates anti-inflammatory property of berberine. Redox Biol. 2023;62:102704. doi:10.1016/j.redox.2023.102704
115. Luo XF, Zhou H, Deng P, et al. Current development and structure-activity relationship study of berberine derivatives. Bioorg Med Chem. 2024;112:117880. doi:10.1016/j.bmc.2024.117880
116. Wu X, Xu N, Ye Z, et al. Polysaccharide from Scutellaria barbata D. Don attenuates inflammatory response and microbial dysbiosis in ulcerative colitis mice. Int J Biol Macromol. 2022;206:1–9. doi:10.1016/j.ijbiomac.2022.02.119
117. Chao L, Li Z, Zhou J, et al. Shen-ling-bai-zhu-san improves dextran sodium sulfate-induced colitis by inhibiting caspase-1/caspase-11-mediated pyroptosis. Front Pharmacol. 2020;11:814. doi:10.3389/fphar.2020.00814
118. Li X, Wu Y, Li H, et al. Inhibitory effect and mechanism of lentinan on colitis-associated colorectal cancer induced by AOM/DSS Through IL-6/STAT3 Pathway. Cancer Res Prev Treat. 2024. doi:10.3971/j.issn.1000-8578.2024.24.0340
119. Li X, Wu Y, Li H, et al. Preventive effect of Gehua Jiecheng Decoction in IL-6/JAK2/STAT3 pathway in”inflammation-cancer transformation”of ulcerative colitis with spleen deficiency and damp-heat. Chin J Immunol. 2024. doi:10.3969/j.issn.1000-484X.2024.07.018
120. Wang S, Xu Y, Yang R. Clinical observation of acupuncture combined with medicine inhibition of atypical dysplasia of ulcerative colitis based on Wnt/β-catenin pathway. China J Tradit Chin Med Pharm. 2019;34(10):4954–4956.
121. Liu Q, Lai X. Effects of compound Tenglizi Decoction on tumor growth and Wnt/β-catenin signaling pathway in nude mice with colon cancer cell transplantation tumor. Chin Tradit Pat Med. 2025. doi:10.3969/j.issn.1001-1528.2025.02.040
122. Du M, Lang X, Cui J, et al. Study on the effect of shendai qingchang decoction mediated pi3k/akt-mtor pathway on ulcerative colitis associated carcinogenesis. J Traditional Chinese Med Pharm. 2022;28(05):35–41. doi:10.13862/j.cn43-1446/r.2022.05.008
123. Huang B, Lang X, Li X. The role of IL-6/JAK2/STAT3 signaling pathway in cancers. Front Oncol. 2022;12:1023177. doi:10.3389/fonc.2022.1023177
124. Tsimberidou AM, Vining DJ, Arora SP, et al. Phase I Trial of TTI-101, a First-in-Class Oral Inhibitor of STAT3, in Patients with Advanced Solid Tumors. Clin Cancer Res. 2025;31(6):965–974. doi:10.1158/1078-0432.CCR-24-2920
125. Lee H, Herrmann A, Deng JH, et al. Persistently activated Stat3 maintains constitutive NF-kappaB activity in tumors. Cancer Cell. 2009;15(4):283–293. doi:10.1016/j.ccr.2009.02.015
126. Wang Z, Li Z, Ji H. Direct targeting of β-catenin in the Wnt signaling pathway: current progress and perspectives. Med Res Rev. 2021;41(4):2109–2129. doi:10.1002/med.21787
127. Yu F, Yu C, Li F, et al. Wnt/β-catenin signaling in cancers and targeted therapies. Signal Transduct Target Ther. 2021;6(1):307. doi:10.1038/s41392-021-00701-5
128. Fruman DA, Chiu H, Hopkins BD, Bagrodia S, Cantley LC, Abraham RT. The PI3K Pathway in Human Disease. Cell. 2017;170(4):605–635. doi:10.1016/j.cell.2017.07.029
129. Leiphrakpam PD, Are C. PI3K/Akt/mTOR Signaling Pathway as a Target for Colorectal Cancer Treatment. Int J Mol Sci. 2024;25(6):3178. doi:10.3390/ijms25063178
130. Nepstad I, Hatfield KJ, Grønningsæter IS, et al. The PI3K-Akt-mTOR Signaling Pathway in Human Acute Myeloid Leukemia (AML) Cells. Int J Mol Sci. 2020;21(8):2907. doi:10.3390/ijms21082907
131. Byndloss MX, Olsan EE, Rivera-Chávez F, et al. Microbiota-activated PPAR-γ signaling inhibits dysbiotic Enterobacteriaceae expansion. Science. 2017;357(6351):570–575. doi:10.1126/science.aam9949
132. Luo Q, Zhang Q, Kong Y, Wang S, Wei Q. Heart failure, inflammation and exercise. Int J Biol Sci. 2025;21(8):3324–3350. doi:10.7150/ijbs.109917
133. Sharma BR, Kanneganti TD. NLRP3 inflammasome in cancer and metabolic diseases. Nat Immunol. 2021;22(5):550–559. doi:10.1038/s41590-021-00886-5
134. Lin L, Zhu Z, Qing Y, et al. Extraction optimization, purification, characterization, and hepatoprotective effect of polysaccharides from Curcuma phaeocaulis Val. and its vinegar products. Int J Biol Macromol. 2025;320:145491. doi:10.1016/j.ijbiomac.2025.145491
135. Liu M, Liu F, Pan Y, et al. Oxymatrine ameliorated experimental colitis via mechanisms involving inflammatory DCs, gut microbiota and TLR/NF-κB pathway. Int Immunopharmacol. 2023;115:109612. doi:10.1016/j.intimp.2022.109612
136. Wu X, Fu S, Jiang M, et al. Sanhuang Xiexin decoction ameliorates DSS-induced colitis in mice by regulating intestinal inflammation, intestinal barrier, and intestinal flora. J Ethnopharmacol. 2022;297:115537. doi:10.1016/j.jep.2022.115537
137. Su F, Dong W, Su H, et al. Effects of ginsenoside rg1 on mice with inflammatory bowel disease via activating intestinal flora-short-chain fatty acid and PPARγ signaling pathway. Hebei Medicine. 2025. doi:10.3969/j.issn.1006-6233.2025.02.005
138. Wang M, Zhao W, Song P, et al. The effect and mechanism of Huangqi Jianzhong Tang on the colonic barrier of spleen stomach deficiency cold rats through PPAR-γ signaling. Chin J Gerontol. 2024;44(8):1911–1917.
139. Zhao Z, Liu L, Song N, et al. Effect of Banxia Xiexintang on NLRP3/caspase-1 pyroptosis pathway in rats with ulcerative colitis. Chin J Exp Tradit. 2022;28(16):29–34. doi:10.13422/j.cnki.syfjx.202201003
140. Jiang Z, Wu R, Xu H, et al. Effects of electroacupuncture with “intestinal disease prescription” on NLRP3 inflammasome and intestinal mucosal barrier in rats with acute ulcerative colitis. Chin Acupunct Moxibustion. 2024;44(4):441–448. doi:10.13703/j.0255-2930.20230716-k0001
141. Chen Q, Luo P, et al. The application and mechanism of organoid technology in ulcerative colitis. J Med Res. 2025;54:1–9.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Machine Learning Research Trends in Traditional Chinese Medicine: A Bibliometric Review
Lim J, Li J, Zhou M, Xiao X, Xu Z
International Journal of General Medicine 2024, 17:5397-5414
Published Date: 19 November 2024