Back to Journals » Journal of Pain Research » Volume 19
Cheek Acupuncture Reduces Postoperative Sore Throat After Double-Lumen Endobronchial Intubation: A Randomized Controlled Trial
Authors Zou X, Hu S, Li X, Zhu X, Wang L ![]() , Wu L
, Wu L ![]()
Received 21 February 2026
Accepted for publication 27 May 2026
Published 6 June 2026 Volume 2026:19 604498
DOI https://doi.org/10.2147/JPR.S604498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Xintong Zou,1 Suwen Hu,1 Xiaoyao Li,2 Xianfen Zhu,3 Liangrong Wang,1,* Linfeng Wu2,*
1Department of Anesthesiology, the First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang Province, 325000, People’s Republic of China; 2Department of Anesthesiology, Taizhou Central Hospital, Taizhou, Zhejiang Province, 318000, People’s Republic of China; 3Department of Rehabilitation, Taizhou Central Hospital, Taizhou, Zhejiang Province, 318000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Linfeng Wu, Department of Anesthesiology, Taizhou Central Hospital, No. 999, Donghai Avenue, Taizhou Economic Development Zone, Taizhou, Zhejiang Province, 318000, People’s Republic of China, Tel +8615168635333, Fax +86 57681899120, Email [email protected] Liangrong Wang, Department of Anesthesiology, the First Affiliated Hospital of Wenzhou Medical University, No. 2, Fuxue Road, Lucheng District, Wenzhou, Zhejiang Province, 325000, People’s Republic of China, Tel +8613587884540, Fax +86 86689476, Email [email protected]
Purpose: Postoperative sore throat (POST) is highly prevalent following double-lumen endobronchial tube (DLT) intubation and negatively impacts recovery. Cheek acupuncture, a micro-needle therapy, provides targeted analgesia through specific acupoint stimulation. This study aimed to evaluate the efficacy of cheek acupuncture in mitigating POST in patients undergoing thoracoscopic lung surgery with DLT intubation.
Patients and Methods: Eighty-eight patients were equally randomized to receive either cheek acupuncture (CA group) at bilateral cervical, upper energizer, and upper cervical points for 30 minutes before surgery completion, or sham acupuncture at identical acupoints (CT group). The primary outcome was overall POST incidence within postoperative 48 hours, and secondary outcomes included POST severity, wound pain, rescue analgesic consumption, postoperative nausea and vomiting (PONV) incidence, time to first flatus, postoperative pulmonary complications, adverse events, satisfaction scores, and hospitalization duration.
Results: The overall 48-hour postoperative POST incidence was 34.1% in the CA group versus 65.9% in the CT group (risk ratio: 0.517, 95% confidential interval: 0.326 to 0.821, P = 0.003), with the most pronounced reduction observed during the 0– 30 min interval (P < 0.05). Moreover, POST severity was significantly reduced in the CA group at 30 min postoperatively (P < 0.05). Cheek acupuncture was also associated with reduced early wound pain, rescue analgesic requirement, 48-hour PONV incidence, and improved overall anesthesia satisfaction (P < 0.05), and no significant intergroup difference in time to first flatus or hospitalization duration was found (P > 0.05).
Conclusion: A single intraoperative session of cheek acupuncture reduces the incidence of early POST after DLT intubation for thoracoscopic lung surgery, with a favorable safety profile.
Keywords: cheek acupuncture, microneedle therapy, postoperative sore throat, double-lumen endobronchial intubation, postoperative nausea and vomiting, pain
Introduction
One-lung ventilation is essential for optimal surgical exposure in video-assisted thoracic procedures, with the double-lumen endobronchial tube (DLT) remaining the preferred technique for achieving lung isolation. However, due to its larger external diameter compared to conventional single-lumen tube, which exceeds that of standard single-lumen endotracheal tube by approximately 30–40%, DLT intubation is associated with a significantly higher incidence and intensity of postoperative sore throat (POST), with a reported incidence of up to 66%.1 Although POST frequently occurs as a self-limiting complication, this prevalent complication can impair recovery and patient satisfaction.2 Various non-pharmacological interventions have been explored to reduce POST, but their efficacy remains inconsistent across studies, highlighting the need for alternative approaches.
Cheek acupuncture, a novel microneedle therapy developed by Wang Yongzhou et al, involves stimulating specific cheek acupoints among 16 standardized points on each cheek, with their precise orientation determined by the anatomic structure of the skull.3 Owing to its painless needling technique, ease of application, favorable safety profile, and immediate onset, it demonstrates certain advantages over conventional acupuncture and pharmacotherapy in pain management, with benefits including a lower incidence of adverse events. Thus, it may serve as an adjunctive therapy to conventional analgesic treatments in clinical practice.4–6 Cheek acupuncture theory is grounded in the concept of a holographic microsystem, wherein the cheek region is postulated to somatotopically represent the entire human body.3 According to this theory, the cervical point, upper cervical point, and upper energizer point correspond somatotopically to the neck and thoracic regions and are specifically indicated for sore throat and chest disorders, directly aligning with the pathogenesis of POST and the anatomical site of thoracic surgery. However, despite this theoretical rationale, no randomized controlled trial has specifically evaluated the efficacy of cheek acupuncture for POST following DLT intubation in thoracic surgery.
This study aimed to evaluate the efficacy of cheek acupuncture in reducing POST following thoracoscopic lung surgery with DLT intubation. The primary outcome was the overall incidence of POST within 48 hours postoperatively. Secondary outcomes included the incidence and severity of POST at specified time points, wound pain intensity, incidence of postoperative nausea and vomiting (PONV), time to first flatus, anesthesia satisfaction scores, local and systemic complications and hospitalization duration.
Methods
This single-center, randomized, controlled study was approved by the Ethics Committee of Taizhou Central Hospital (No. 2024L-06-19) on 1 July 2024. The study protocol was registered with the International Traditional Medicine Clinical Trial Registry (https://itmctr.ccebtcm.org.cn/mgt/project/view/-1544155896240888245, No. ITMCTR2025000052) on 10 January 2025 prior to the first participant recruitment. All participants provided written informed consent, and the trial was conducted at Taizhou Central Hospital in accordance with the Declaration of Helsinki. This study adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines for reporting. The detailed study protocol and statistical analysis plan are accessible within the methods section of the publication.
Patients scheduled for video-assisted thoracoscopic lung surgery with DLT intubation were screened for eligibility. Inclusion criteria were age 18–65 years, body mass index (BMI) 18–28 kg/m2, American Society of Anesthesiologists (ASA) physical status I or II, anticipated surgical duration of 1–3 hours, no significant organ dysfunction, no history of hypertension or diabetes (or well-controlled comorbidities if previously diagnosed), and no anticipated difficult airway. Exclusion criteria included requiring two or more intubation attempts, preoperative chronic pharyngeal pain, long-term analgesic use, coagulation disorders or anticoagulant therapy, facial pathologies (eg, trigeminal neuralgia or facial spasm) or localized infections at acupuncture sites, medical history of traumatic brain injury or epilepsy, psychiatric disorders or communication difficulties, unplanned postoperative ICU admission, intraoperative blood loss exceeding 500 mL, or allergy to trial medications.
The allocation sequence was generated with the PLAN procedure in SAS 9.4 (SAS Institute Inc.) by an independent research assistant, using a block size of 4. Eighty-eight eligible patients were randomly assigned to either the cheek acupuncture group (CA group) or the control group (CT group) with a 1:1 allocation ratio. To ensure allocation concealment and blinding, the randomization sequence was kept confidential by an independent investigator (Xintong Zou), who prepared sequentially numbered, opaque, sealed envelopes. Each envelope contained a card specifying the group assignment and was affixed inside an opaque folder to prevent accidental disclosure. The envelopes were opened 30 minutes before the end of the procedure by the investigator Xianfen Zhu, who administered the corresponding intervention and was not involved in follow-up. The outcome assessors remained blinded to group allocation throughout the study.
Patients in the CA group received bilateral needling at three predetermined acupoints (Figure 1): the cervical point (located at top edge of the root of the zygomatic arch), upper energizer point (located at the cross of the posterior coronoid of the mandible and the lower edge of the zygomatic arch), and upper cervical point (located at osseous transverse notch vertically above the cervical point). Following skin disinfection, sterile disposable thumbtack needles (0.20 mm × 1.3 mm) were inserted to the predetermined depth using a tapping technique, then secured with adhesive dressing and retained for 30 minutes. In the CT group, patients underwent identical preparation with a non-invasive technique. Sterile adhesive pads were applied to the same acupoint locations, and blunt needles were then inserted into gel pads without skin penetration to simulate tactile sensation without active stimulation, remaining in place for an equivalent 30-minute period.
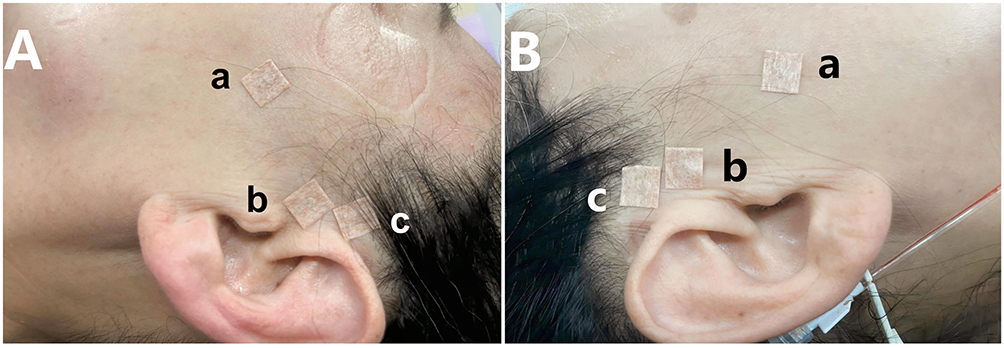 |
Figure 1 The selected acupoints for cheek acupuncture. (A) The left side; (B) The right side. (a) upper energizer point; (b) cervical point; (c) upper cervical point. |
All patients underwent preoperative fasting for 8 hours for solids and 2 hours for clear fluids. Upon arrival in the operating room, standard monitoring was established. After preoxygenation with 100% oxygen for 3 minutes, anesthesia was induced with intravenous propofol (2 mg/kg), sufentanil (0.5 μg/kg), and rocuronium (0.6mg/kg). DLT intubation was performed using a lubricated Mallinckrodt tracheal tube (Covidien, MA, USA) under video laryngoscopy by an experienced anesthesiologist who was not involved in follow-up. Tube size selection was based on preoperative computed tomography measurements of bronchial width, as previously described.7 Fiberoptic bronchoscopy confirmed and adjusted DLT position as needed before positioning the patient laterally. Anesthesia was maintained with continuous remifentanil, propofol and dexmedetomidine to keep bispectral index values between 40–60. Intermittent doses of rocuronium (0.15 mg/kg) were administered to maintain muscle relaxation. During the one-lung ventilation, tidal volume was set at 5–7 mL/kg ideal body weight, with ventilator parameters adjusted to maintain peak inspiratory pressure < 35 cmH2O and end tidal CO2 between 35–45 mmHg. Postoperative analgesia was initiated 10 minutes before surgery completion, consisting of sufentanil 2 μg/kg in 100 mL normal saline at 2 mL/h continuous infusion without bolus dosing. Prophylactic ondansetron (4 mg) was administered intravenously to prevent postoperative nausea and vomiting (PONV). Upon meeting extubation criteria, oropharyngeal suction was performed using a 12 F catheter with gentle aspiration, and the DLT was carefully removed by the same anesthesiologist. Patients were then transferred to the post-anesthesia care unit.
The primary outcome was the overall incidence of POST within postoperative 48 hours. POST has been defined as an unpleasant feeling of discomfort or irritation experienced either at rest or swallowing. Secondary outcomes included the following assessments: (1) Incidence of POST was assessed during five postoperative intervals (0–0.5, 0.5–6, 6–12, 12–24, and 24–48 hours). (2) POST severity was measured with throat pain scale (TPS) at 0.5, 6, 12, 24, and 48 hours postoperatively, based on an established scoring system,8 where 0 indicated no pain; 1, mild pain (less than a common cold); 2, moderate pain (similar to a common cold); and 3, severe pain (worse than a common cold). (3) Surgical wound pain was assessed using the Visual Analog Scale (VAS) at 6, 12, and 24 hours postoperatively, with 0 representing “no pain” and 10 indicating “the worst pain imaginable”. Patients with VAS scores ≥ 4 were administered intravenous flurbiprofen 100 mg as rescue analgesia. (4) PONV incidence was calculated as the proportion of patients who experienced at least one episode of nausea and / or vomiting during the observation period. (5) Time to first flatus was recorded as the time interval (hours) between the completion of surgical suturing and the patient’s first flatus. (6) Patient satisfaction with anesthesia was graded on a Likert scale (1–2: very dissatisfied, 3–4: dissatisfied, 5–6: neutral, 7–8: satisfied, 9–10: very satisfied). (7) Postoperative pulmonary complications (atelectasis, pulmonary edema, pulmonary effusion, pneumothorax, pneumonia, pulmonary thromboembolism, respiratory failure, or acute respiratory distress) occurring within postoperative 48 hours were recorded. (8) Local complications (cheek infection, subcutaneous hematoma, and nerve injury), systemic symptoms (dizziness and headache), and hospitalization duration were documented.
Sample size calculation was performed using PASS 2021 software (NCSS, LLC, Kaysville, UT, USA) with the incidence of POST within postoperative 48 hours as the primary outcome. Preliminary data from 20 cases per group showed POST incidences of 30% in the CA group versus 60% in the CT group. Based on a two-tailed α of 0.05 and 80% power for detecting this difference, 40 patients per group (1:1 allocation) were required. Accounting for 10% dropout rate, the final sample size was determined to be 88 participants.
Statistics followed the modified intention-to-treat principle, which included all participants who underwent laparoscopic surgery, received the intervention, and had no impairment in the assessment of the primary outcome in the analysis. Statistical analyses were conducted using SPSS 26.0 (IBM Corp). The Shapiro–Wilk test was used to assess the normality of continuous variables. Normally distributed continuous variables were expressed as mean ± standard deviation and compared using independent samples t-test, while non-normally distributed data were presented as median (Q1, Q3) and analyzed with the Mann–Whitney U-test. Categorical variables were reported as frequencies (percentages) and compared using the Chi-squared test or Fisher’s exact test, as appropriate. Longitudinal outcomes (POST incidence and TPS scores) were analyzed using generalized estimating equations (GEE) with an autoregressive (AR1) correlation structure, and both models included group, time, and their interaction as fixed effects. Repeated-measures ANOVA was used to analyze VAS scores across postoperative time points. The assumption of sphericity was assessed using Mauchly’s test, and the Greenhouse-Geisser correction was applied to adjust the degrees of freedom when sphericity was violated (P < 0.05). For the comparison of two proportions, confidence intervals (CIs) were calculated using the Newcombe-Wilson method. The Hodges-Lehmann method was used to estimate the median difference between groups along with its 95% CI. For the GEE model, model-based Wald-type CIs were derived from asymptotic standard errors. A P value < 0.05 was considered statistically significant.
Results
Of the 103 potentially eligible patients, 10 were excluded for not meeting the inclusion criteria, and 5 declined to participate. The remaining 88 patients were equally randomized into either the CA group or the CT group. All patients completed the study and were included in the final analysis, and no data imputation was performed. Figure 2 presented the CONSORT flowchart of the study. Demographic and clinical data were comparable between the two groups (P > 0.05, Table 1).
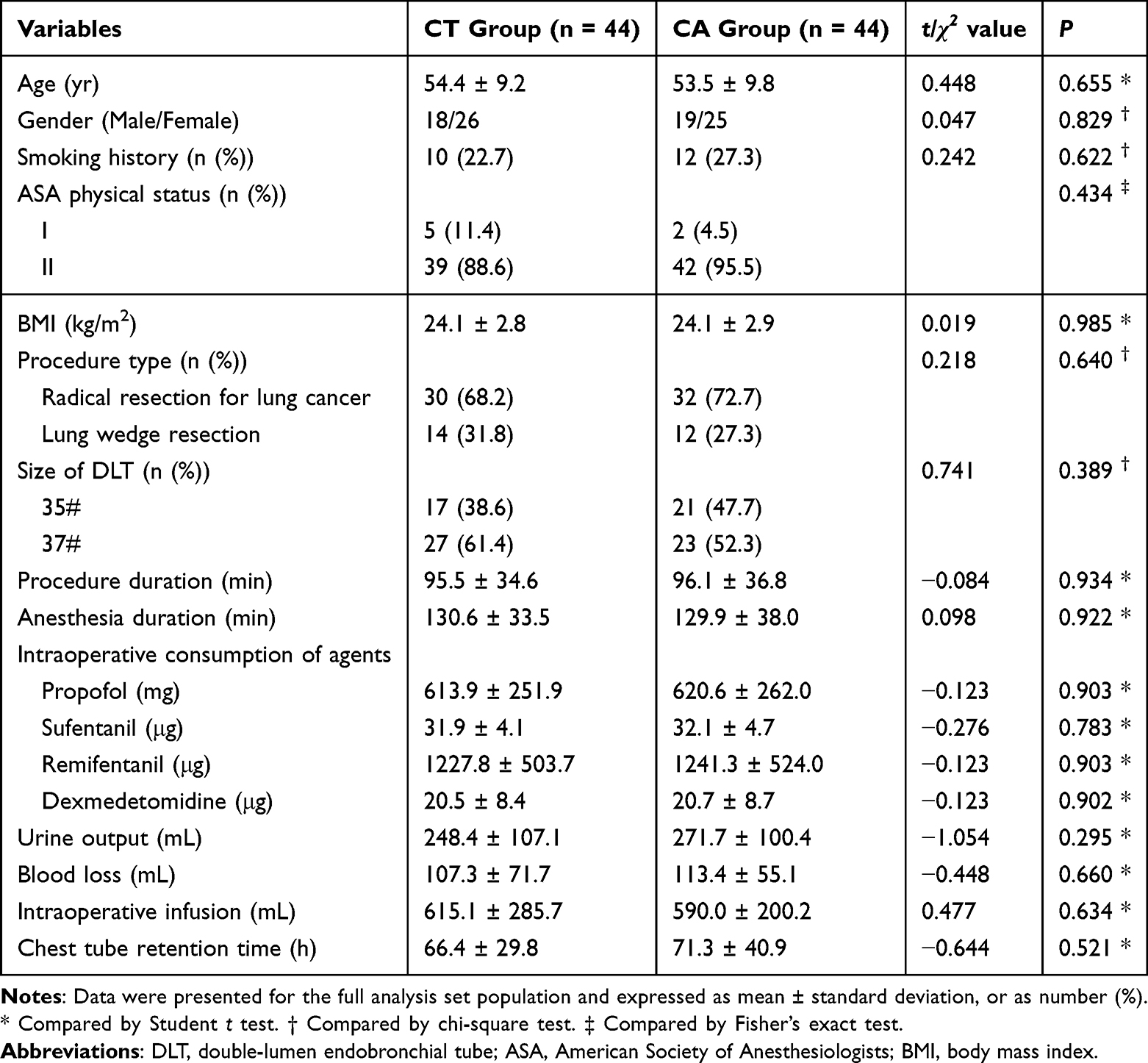 |
Table 1 Demographic and Clinical Data |
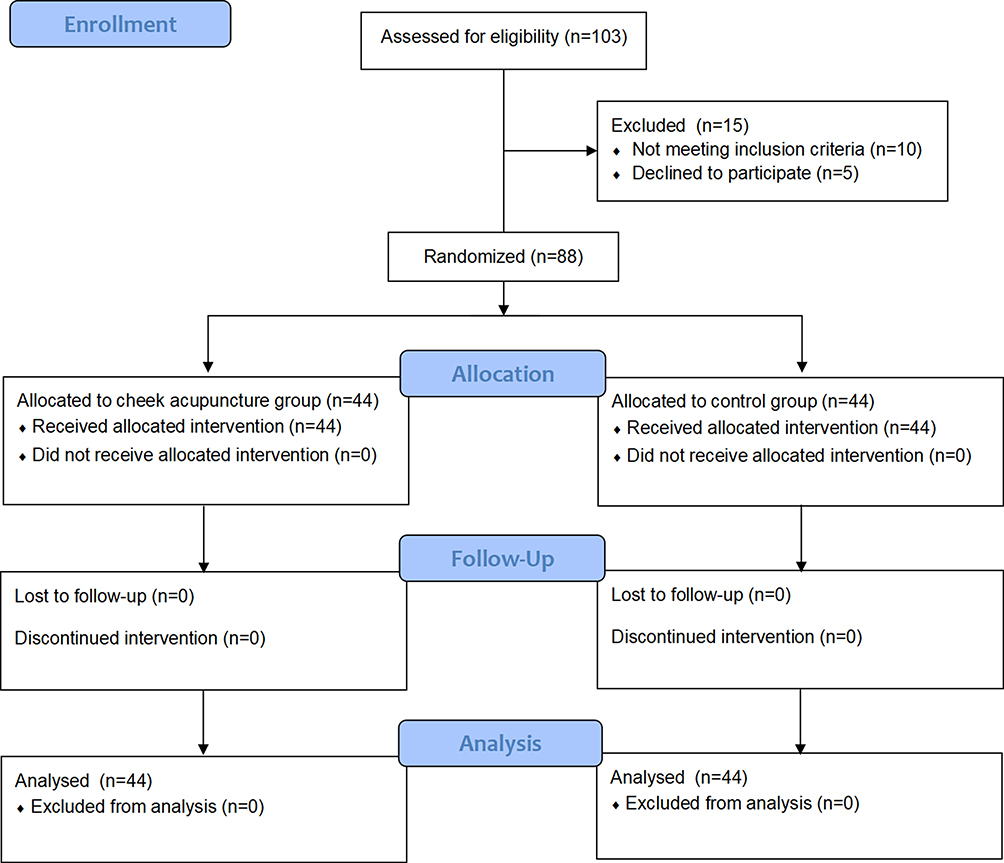 |
Figure 2 The CONSORT flowchart. Abbreviation: CONSORT, Consolidated Standards of Reporting Trials. |
The overall 48-hour postoperative POST incidence was 34.1% in the CA group versus 65.9% in the CT group, with a risk ratio (RR) of 0.517 (95% CI: 0.326 to 0.821, P = 0.003). GEE revealed significant main effects for group (Wald χ2: 143.916, P < 0.001) and time (Wald χ2: 258.147, P < 0.001). The group-by-time interaction effect was not statistically significant (Wald χ2: 0.53, P = 0.911), indicating similar trajectory of POST resolution between the groups. Subgroup analysis showed that after Bonferroni correction for multiple comparisons, the CA group had significantly lower POST incidence at the 0–30 min interval (P < 0.05, Table 2), and significantly lower TPS scores only at 30 min postoperatively (P < 0.05, Table 3). Nominal differences at other time points did not survive correction and should be considered exploratory. The distribution of TPS scores also differed significantly between groups (P < 0.05), with the CA group showing higher proportions of scores 0 and 1 (P < 0.05, Table 4).
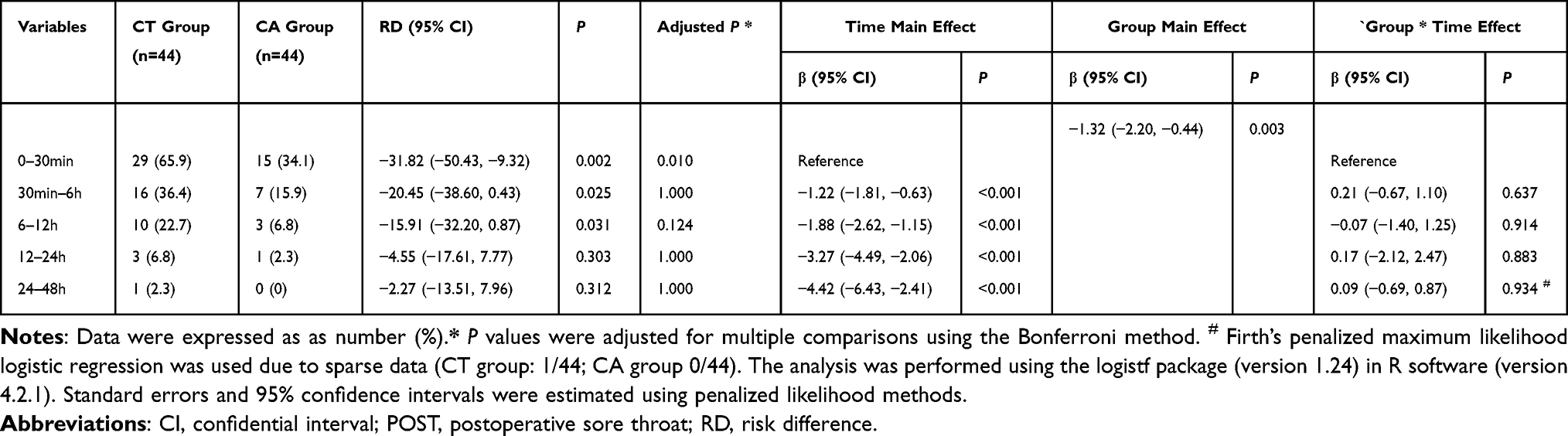 |
Table 2 Generalized Estimating Equation Analysis of the Incidence of POST |
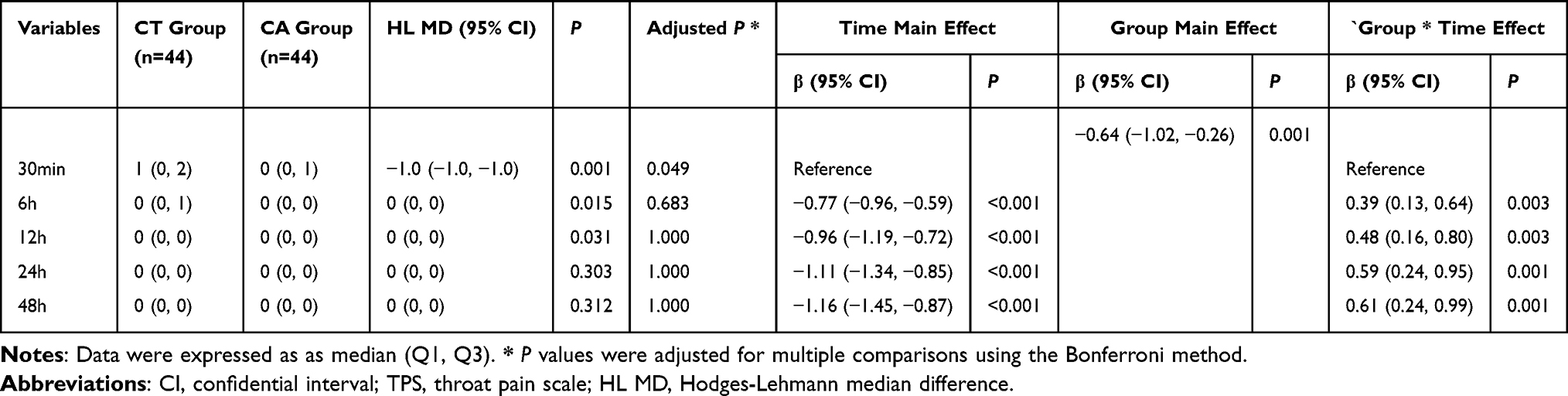 |
Table 3 Generalized Estimating Equation Analysis of TPS Scores |
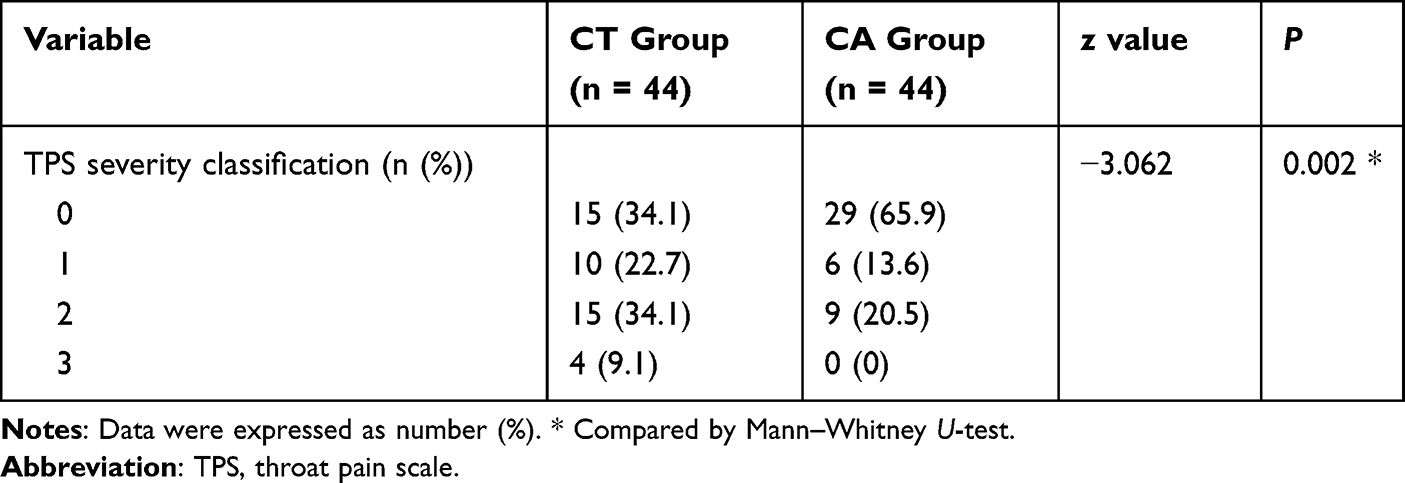 |
Table 4 TPS Severity Classification |
Mauchly’s test indicated violation of the sphericity assumption (W = 0.258, approx. χ2 = 114.467, P < 0.001), therefore, the Greenhouse-Geisser correction was applied (ε = 0.555). There was a significant main effect of time (F = 384.003, P < 0.001) and a significant time-by-group interaction (F = 4.944, P = 0.006), indicating that VAS trajectories differed between the two groups. Post-hoc comparisons showed that patients receiving cheek acupuncture demonstrated significantly lower wound VAS scores at 30 minutes postoperatively and reduced requirement for rescue analgesia within the 48-hour postoperative period compared to controls (P < 0.05, Table 5), despite comparable total sufentanil consumption between groups.
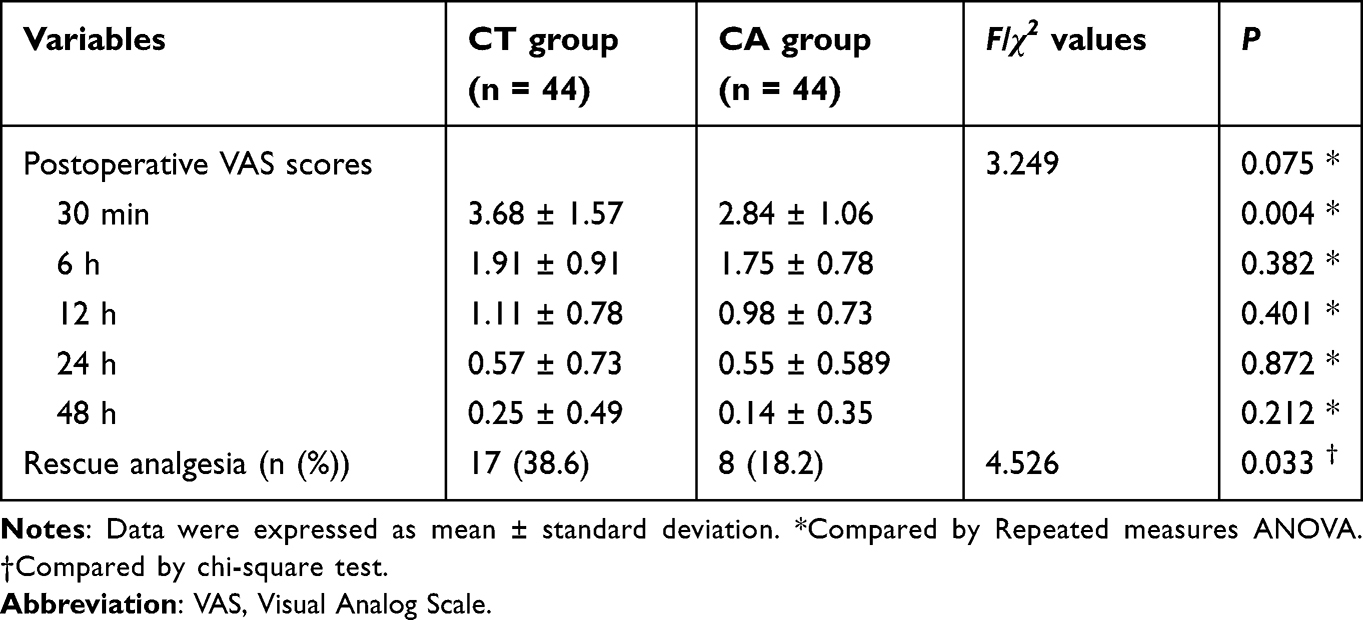 |
Table 5 Surgical Wound Pain |
Compared with the CT group, the CA group exhibited a significantly lower incidence of PONV within the first 48 hours (P < 0.05). In contrast, the time to first flatus did not differ between the two groups (P > 0.05, Table 6). Patients who underwent cheek acupuncture also reported higher anesthesia satisfaction scores (P < 0.05), whereas no statistically significant difference was found in the duration of hospital stay (P > 0.05, Table 6).
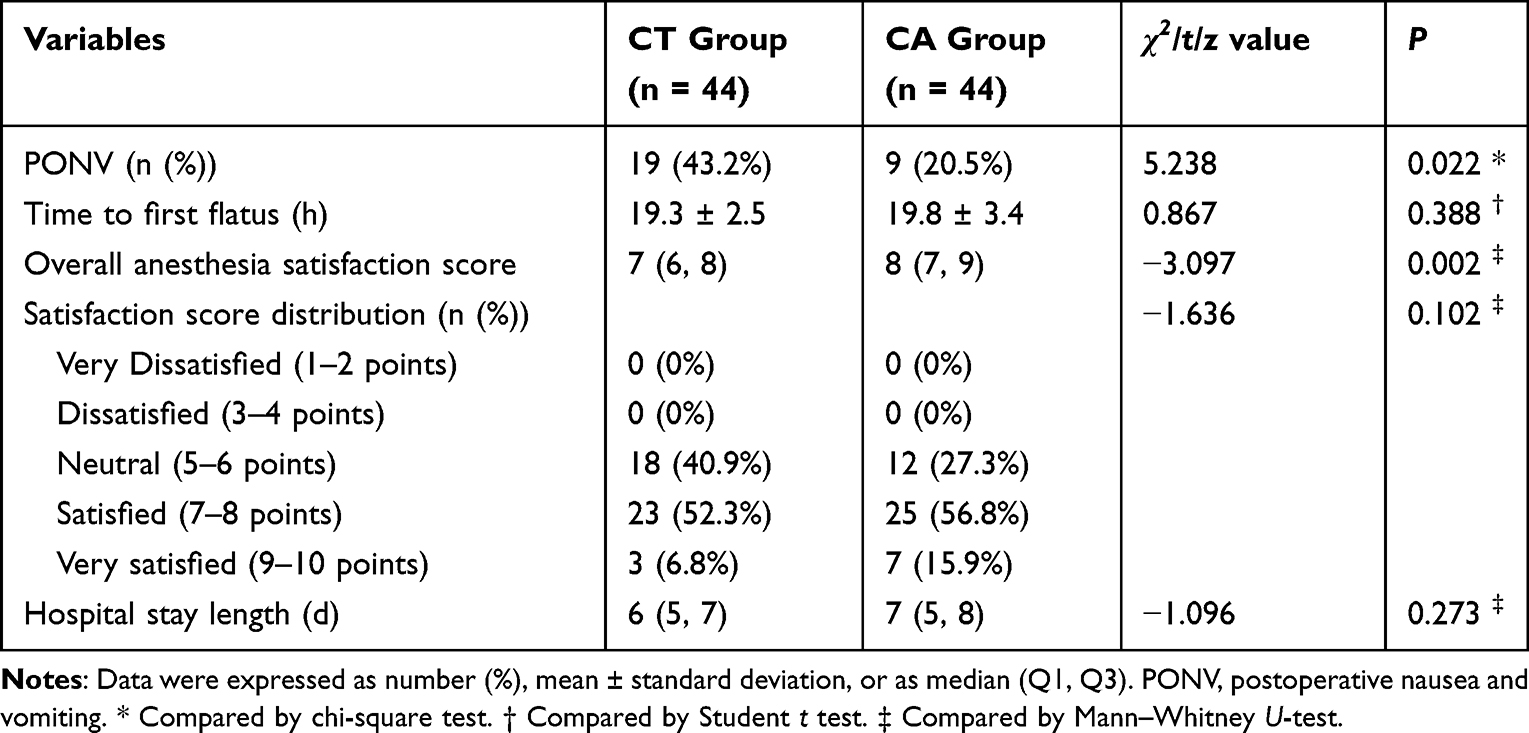 |
Table 6 Incidence of PONV, Time to First Flatus, Anesthesia Satisfaction Score and Length of Hospital Stay |
Safety analysis showed that in the CA group, two cases (4.5%) developed minor facial hemorrhage that resolved spontaneously within hours without intervention. Neither group exhibited severe headache, dizziness, cheek infection, nerve injury, or postoperative pulmonary complications.
Discussion
The primary findings of this study demonstrate that: (1) cheek acupuncture significantly reduced the overall incidence of POST within postoperative 48 hours in patients undergoing video-assisted thoracoscopic lung surgery with DLT intubation, with the most pronounced efficacy observed during the initial 30-minute postoperative period; (2) the intervention effectively alleviated surgical wound pain at 30 minutes postoperatively; and (3) cheek acupuncture decreased the incidence of PONV within postoperative 48 hours without significant local or systemic complications. These results suggest that cheek acupuncture may serve as a safe and effective adjunct for POST prevention in this surgical population.
POST represents a prevalent and clinically significant complication after general anesthesia that may be distressing for the patient. Endotracheal intubation remains a primary contributing factor due to mechanical trauma, sustained mucosal irritation, and cuff-induced ischemia. These pathogenic mechanisms are further exacerbated by several DLT-specific factors, including larger tube diameter, increased mucosal contact surface area, and frequent manipulation during lung isolation. Supporting this, comparative studies consistently show higher POST incidence and severity with DLTs compared to single-lumen tubes.9 POST associated with tracheal intubation can be influenced by multiple factors, such as patient characteristics (gender, smoking status), intubation conditions, tube size, and surgical variables (type and duration).10,11 In our cohort, these risk factors were well balanced between study groups, and control patients exhibited an overall POST incidence of 65.9% within the first 48 postoperative hours. Both this overall incidence and the immediate postoperative rate were comparable to published data,1,12 while later postoperative incidence appeared lower than previously reported values.13,14 This reduction may reflect our protocol of routine endotracheal tube lubrication, which likely reduces mucosal trauma during intubation and tube displacement. Although our inflation protocol (minimum volume to prevent air leakage) reflects routine clinical practice and avoids overinflation-related injury, the absence of cuff pressure monitoring may nevertheless confound POST risk. However, this limitation is partially mitigated by uniform application of the same protocol across both groups, which likely yields non-differential bias, as well as by the robust treatment effect observed despite this potential confounder. Future studies should incorporate routine cuff pressure monitoring to strengthen causal inference.
Numerous studies have primarily investigated pharmacological approaches for preventing POST. Common pharmacological strategies include dexamethasone, ketamine, lidocaine, and magnesium, which have demonstrated variable efficacy but may be associated with dose-dependent adverse effects such as delayed wound healing, sedation, or cardiovascular events.15 Various non-pharmacological interventions have also been explored, including endotracheal tube lubrication with water-soluble gel, thermal softening of DLTs before intubation,13 DLT material optimization,16 ultrasound-guided internal superior laryngeal nerve block,17 and refined intubation techniques.18,19 However, existing research has reported inconsistent outcomes regarding the efficacy of these methods. Compared with both pharmacological and non-pharmacological strategies, cheek acupuncture in our study achieved a significant reduction in POST incidence (from 65.9% to 34.1%) with a favorable safety profile-only two cases of self-limiting minor cheek hemorrhage were observed, and no systemic adverse events were reported. The observed effect size (an absolute risk reduction of 31.8%) is within the range of many existing interventions. Temporal analysis further revealed that this intervention effectively decreased both the incidence and severity of POST within the first 30 minutes postoperatively, a finding of particular clinical relevance given that the maximum incidence of POST (56.4%) has been reported to occur within the first postoperative hour.2 These findings collectively indicate that cheek acupuncture may serve as an effective approach for mitigating POST in this patient population, particularly when administered as repeated or scheduled sessions. Nevertheless, direct head-to-head comparisons are warranted to better define the role of cheek acupuncture in POST prevention.
Clinically, cheek acupuncture has demonstrated efficacy in pain management across diverse pathologies, particularly in reducing postoperative pain and improving recovery quality following radical resection of gastrointestinal cancers without significant adverse effects.20,21 However, the neurobiological mechanisms underlying its analgesic effects remain incompletely understood. From a traditional Chinese medicine perspective, cheek acupuncture’s therapeutic actions are interpreted through three theoretical frameworks: Da San Jiao, holography, and physical-mental integration. Modern physiological studies suggest that its analgesic effects are achieved through multi-level neuromodulatory mechanisms encompassing peripheral, spinal, and supraspinal pathways, principally involving the regulation of specific neurochemical mediators. Notably, endogenous opioid release concurrently induces nociceptor desensitization and suppresses proinflammatory cytokine production in both peripheral tissues and the spinal cord, whereas serotonin and norepinephrine modulate spinal nociceptive processing through phosphorylation of N-methyl-D-aspartate receptors.22 Furthermore, the downregulation of inflammatory cytokine signaling constitutes a complementary analgesic mechanism in acupuncture-mediated pain relief.23,24 In rheumatoid arthritis models, cheek acupuncture exhibited superior immediate analgesia compared to conventional body acupuncture, mechanistically linked to β-endorphin and cholecystokinin-8 modulation in cerebrospinal fluid,25 and also this technique displayed characteristic temporal effects due to elevated hypothalamic 5-hydroxytryptamine (5-HT) and reduced norepinephrine/5-HT ratio.26 Furthermore, animal studies indicated that adenosine, derived from adenosine triphosphate degradation following needle stimulation, may promote analgesia through adenosine receptor activation.27
Yi et al4 demonstrated that cheek acupuncture cheek acupuncture produces a temporally specific analgesic response, characterized by rapid onset (detectable within 5 minutes) and peak efficacy at 30 minutes post-stimulation. This distinct temporal profile demonstrates a physiologically determined pattern of progressively increasing pain thresholds, suggesting neurobiological mediation rather than cumulative therapeutic effects. Consistent with this profile, our study observed reduced wound VAS at 30 minutes but not at subsequent time points. This transient effect may be explained by two factors. First, the selected acupoints were primarily chosen to target POST, not surgical wound pain. Second, a single intraoperative session may be insufficient for extended wound analgesia, suggesting that repeated or postoperative acupuncture warrants further investigation. While traditional acupuncture, which contains more than 300 acupoints, may pose practical constraints in thoracic procedures requiring lateral positioning, our study’s thumbtack needle technique offers a potential solution. However, its comparative efficacy against standard cheek acupuncture (typically using 0.18 mm × 30 mm needles) for POST and surgical wound pain remains to be established. Notably, cheek acupuncture is well-tolerated, with minimal discomfort compared to traditional acupuncture, which frequently elicits needling sensations such as soreness, numbness, distension, or pain. Our study further confirmed its favorable safety profile, with only two instances of self-limiting minor cheek hemorrhage observed among all participants.
Our previous study demonstrated that cheek acupuncture targeting specific points (neck, dorsal, lumbar, middle energizer, and pelvic belt) significantly reduced early (6h) PONV in patients undergoing laparoscopic gynecological surgery, surpassing the efficacy of 5-HT receptor antagonist alone while accelerating gastrointestinal recovery.28 Current data further indicated that alternative point combinations (cervical, upper energizer, and upper cervical) effectively decreased postoperative 48-hour PONV incidence, though without affecting flatus time, suggesting distinct point-specific therapeutic profiles. The exact mechanisms underlying the antiemetic effect of cheek acupuncture remain unclear. Although neuropeptide modulation (eg, enkephalins, substance P, β-endorphin) has been implicated in acupuncture’s antiemetic action in general,29 direct evidence specifically linking cheek acupuncture to PONV reduction is lacking. Therefore, while our findings demonstrate a clinical benefit, the mechanistic explanation remains speculative and requires further investigation. Although the incidence of PONV was significantly reduced in the cheek acupuncture group, the time to first flatus did not differ between groups. This finding appears inconsistent with our prior gynecological study, where cheek acupuncture reduced both PONV and time to first flatus.27 Several factors may explain this discrepancy. First, bowel recovery is influenced by multiple factors, including surgical manipulation and opioid consumption. Second, the 48-hour observation period might have been insufficient to detect a significant difference in flatus time. Third, and most importantly, the acupoint selection in this study was primarily designed for postoperative analgesia rather than specifically targeting gastrointestinal motility. Further studies are needed to establish evidence-based protocols for acupoint selection that balance analgesia and gastrointestinal recovery.
The current study has several limitations. Firstly, as a single-center randomized controlled trial with a relatively small sample size, the generalizability of our findings requires validation through larger-scale multicenter studies. Additionally, the 48-hour follow-up period may be insufficient to fully capture wound pain and PONV, and employing more frequent (eg, hourly) assessments of POST within the first 6 postoperative hours may reveal additional time-specific effects not identified by our current intervals. Secondly, while the endobronchial tube cuff was inflated to the minimum volume necessary to prevent air leakage during ventilation, cuff pressure monitoring was not performed, which may represent a potential confounding factor. Thirdly, although all cheek acupoints were selected by a single experienced acupuncturist using fixed anatomical landmarks to ensure consistency, no objective method was available to independently verify acupoint accuracy, which represents a potential limitation of the study. Fourth, the potential biological mechanisms underlying the effectiveness of cheek acupuncture in preventing POST were not explored. Finally, the acupoint selection, needle retention duration, and optimal treatment frequency have not yet been standardized.
In conclusion, this single-center RCT suggests that cheek acupuncture is a promising adjunct for alleviating POST in patients undergoing thoracoscopic lung surgery with DLT intubation, while concurrently reducing wound pain and PONV with a favorable safe profile. However, cheek acupuncture did not significantly reduce time to first flatus or hospital stay, a finding that may be attributed to the complex, multifactorial determinants of these outcomes. Given the modest sample size and the absence of an active comparator, these findings should be considered preliminary. Larger, multicenter trials with standardized acupoint protocols are warranted, and implementation barriers (eg, acupuncturist training, workflow integration) require further attention.
Data Sharing Statement
The data that support the findings of this study are available on reasonable request from the corresponding author.
Acknowledgment
International Traditional Medicine Clinical Trial Registry (https://itmctr.ccebtcm.org.cn/mgt/project/view/-1544155896240888245, No. ITMCTR2025000052), registered on January 10, 2025, and the first participant was enrolled on January 12, 2025.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Park JJ, Huh H, Yoon SZ, et al. Two-handed jaw thrust decreases postoperative sore throat in patients undergoing double-lumen endobronchial intubation: a randomised study. Eur J Anaesthesiol. 2020;37:105–11. doi:10.1097/EJA.0000000000001149
2. Bihani P, Das D, Jaju R, Misra S. Postoperative sore throat following double-lumen tube insertion in adults undergoing surgery: a scoping review. J Cardiothorac Vasc Anesth. 2026;40:355–363. doi:10.1053/j.jvca.2025.08.031
3. Wang YZ. Buccal Acupuncture Therapy. Beijing People’s Health Publishing House Co. Ltd; 2017.
4. Yi Y, Huijun YE, Huiling Z, Lihua J. Clinical observation on 90 cases of primary dysmenorrhea treated by buccal acupuncture therapy: a randomized controlled study. J Tradit Chin Med. 2024;44:172–181. doi:10.19852/j.cnki.jtcm.20231110.001
5. Shan HH, Chen HF, Lu XH, et al. Buccal acupuncture combined with ultrasound-guided dry needle-evoked inactivation of trigger points to treat cervical and shoulder girdle myofascial pain syndrome. J Back Musculoskelet Rehabil. 2023;36:1139–1150. doi:10.3233/BMR-220321
6. Guo L, Jia T, Yang Y, Feng H, Jiang P. Efficacy and safety of buccal acupuncture for pain management: a systematic review and meta-analysis. Complement Ther Med. 2025;95:103297. doi:10.1016/j.ctim.2025.103297
7. Suvvari P, Kumar B, Singhal M, Singh H. Comparison between computerized tomography-guided bronchial width measurement versus conventional method for selection of adequate double lumen tube size. Ann Card Anaesth. 2019;22(4):358–364. doi:10.4103/aca.ACA_117_18
8. Tazeh-Kand NF, Eslami B, Mohammadian K. Inhaled fluticasone propionate reduces postoperative sore throat, cough, and hoarseness. Anesth Analg. 2010;111:895–898. doi:10.1213/ANE.0b013e3181c8a5a2
9. Zhong T, Wang W, Chen J, Ran L, Story DA. Sore throat or hoarse voice with bronchial blockers or double-lumen tubes for lung isolation: a randomised, prospective trial. Anaesth Intensive Care. 2009;37:441–446.
10. El-Boghdadly K, Bailey CR, Wiles MD. Postoperative sore throat: a systematic review. Anaesthesia. 2016;71:706–717. doi:10.1111/anae.13438
11. Bekele Z, Melese Z. Incidence and risk factors for postoperative sore throat after general anesthesia with endotracheal intubation: prospective cohort study. Ann Med Surg. 2023;85:2356–2361. doi:10.1097/MS9.0000000000000786
12. Park JW, Jo JH, Park JH, et al. Comparison of conventional and fibreoptic-guided advance of left-sided double-lumen tube during endobronchial intubation: a randomised controlled trial. Eur J Anaesthesiol. 2020;37:466–473. doi:10.1097/EJA.0000000000001216
13. Seo JH, Cho CW, Hong DM, Jeon Y, Bahk JH. The effects of thermal softening of double-lumen endobronchial tubes on postoperative sore throat, hoarseness and vocal cord injuries: a prospective double-blind randomized trial. Br J Anaesth. 2016;116:282–288. doi:10.1093/bja/aev414
14. Park SH, Han SH, Do SH, Kim JW, Rhee KY, Kim JH. Prophylactic dexamethasone decreases the incidence of sore throat and hoarseness after tracheal extubation with a double-lumen endobronchial tube. Anesth Analg. 2008;107:1814–1818. doi:10.1213/ane.0b013e318185d093
15. Mazzotta E, Soghomonyan S, Hu LQ. Postoperative sore throat: prophylaxis and treatment. Front Pharmacol. 2023;14:1284071. doi:10.3389/fphar.2023.1284071
16. Jeon J, Lee K, Ahn G, Lee J, Hwang W. Comparison of postoperative sore throat and hoarseness between two types of double-lumen endobronchial tubes: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2015;29:121–125. doi:10.1053/j.jvca.2014.05.028
17. Wang J, Chai B, Zhang Y, Zheng L, Geng P, Zhan L. Effect of postoperative ultrasound-guided internal superior laryngeal nerve block on sore throat after intubation of double-lumen bronchial tube: a randomized controlled double-blind trial. BMC Anesthesiol. 2022;22(1):276. doi:10.1186/s12871-022-01819-x
18. Seo JH, Kwon TK, Jeon Y, Hong DM, Kim HJ, Bahk JH. Comparison of techniques for double-lumen endobronchial intubation: 90 degrees or 180 degrees rotation during advancement through the glottis. Br J Anaesth. 2013;111:812–817. doi:10.1093/bja/aet203
19. Liu TT, Li L, Wan L, Zhang CH, Yao WL. Videolaryngoscopy vs Macintosh laryngoscopy for double-lumen tube intubation in thoracic surgery: a systematic review and meta-analysis. Anaesthesia. 2018;73:997–1007. doi:10.1111/anae.14226
20. Zhu ZX, Chen C, Zheng YF, et al. Buccal acupuncture alleviates postoperative pain in patients undergoing radical resection of gastrointestinal cancers: a randomized controlled pilot study. Chin J Integr Med. 2025;31:558–565. doi:10.1007/s11655-025-4128-y
21. Zhu DX, Yang YL, Yang L, et al. Effects of buccal acupuncture on postoperative analgesia in elderly patients undergoing laparoscopic radical gastrectomy: a randomized controlled trial. Front Neurol. 2024;15:1408360. doi:10.3389/fneur.2024.1408360
22. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120:482–503. doi:10.1097/ALN.0000000000000101
23. Ling F, Qi W, Li X, et al. Bibliometric analysis of acupuncture therapy for cancer pain over the past 10 years. J Pain Res. 2023;16:985–1003. doi:10.2147/JPR.S395421
24. Wang F, Peng P, Zheng Y, Cheng S, Chen Y. Effect of acupuncture on postoperative pain in patients after laparoscopic cholecystectomy: a randomized clinical trial. Evid Based Complement Alternat Med. 2023;2023:3697223. doi:10.1155/2023/3697223
25. Pu RS, Fang XL, Jie WJ, Liu DL, Su CH. Experimentally investigating the effect of buccal acupuncture on analgesic time-effect characteristics and monoamine neurotransmitters. J Acupunct Tuina Sci. 2018;16:229–235. doi:10.1007/s11726-018-1055-x
26. Jie W, Fang X, Pu R, et al. [Analgesic effect of buccal acupuncture on acute arthritis in rabbits and underlying mechanisms]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2017;42:517–521. Chinese. doi:10.11817/j.issn.1672-7347.2017.05.006
27. Tang Y, Yin HY, Liu J, Rubini P, Illes P. P2X receptors and acupuncture analgesia. Brain Res Bull. 2019;151:144–152. doi:10.1016/j.brainresbull.2018.10.015
28. Wang L, Zou X, Wu L, et al. Cheek acupuncture reduces postoperative nausea and vomiting in patients undergoing laparoscopic gynecological surgery: a randomized controlled trial. J Minim Invasive Gynecol. 2025;32:606–613. doi:10.1016/j.jmig.2025.01.011
29. Clement-Jones V, McLoughlin L, Tomlin S, Besser GM, Rees LH, Wen HL. Increased beta-endorphin but not met-enkephalin levels in human cerebrospinal fluid after acupuncture for recurrent pain. Lancet. 1980;2:946–949. doi:10.1016/S0140-6736(80)92106-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.