Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Chatbot-Mediated Learning For Caregiving Relatives of People With Dementia: Empirical Findings and Didactical Implications For Mulitprofessional Health Care
Received 6 September 2023
Accepted for publication 20 November 2023
Published 16 January 2024 Volume 2024:17 Pages 219—228
DOI https://doi.org/10.2147/JMDH.S424790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Daniela Schmitz,* Britta Becker*
Department for Human Medicine, Junior Professorship for Innovative and Digital Methods of Teaching and Learning in Multiprofessional Health Care, Witten/Herdecke University, Witten, NRW, Germany
*These authors contributed equally to this work
Correspondence: Daniela Schmitz, Witten/Herdecke University, Department for Human Medicine, Junior Professorship for Innovative and Digital Methods of Teaching and Learning in Multiprofessional Health Care, Stockumer Straße 12, Witten, North-Rhine Westphalia, 58453, Germany, Tel +49 2302 926 216, Email [email protected]
Purpose: Supporting family caregivers is a major challenge for the healthcare system. The first points of contact are physicians, nurses and social services, which are not easily accessible. For this reason, an information platform has been developed to provide information for family caregivers caring for people with dementia at home. The aim of this article is to provide an insight into the didactic design of this platform.
Sample and Methods: A didactic concept was developed based on didactic target group analysis and interviews with caring relatives (n=6).
Results: The didactic concept of the digital platform takes into account the characteristics of family caregivers as learners, such as time constraints and reciprocity. Therefore two different learning paths, a long and a short version, are offered. Reciprocity is supported by information which are related to individual characteristics of the caring relation. This is made possible by an adaptation of the didactic method “anchored instructions”: Family caregivers experience a problematic caring situation. They use the platform and central concepts related to this situation are offered as anchors. In chatbot mediated learning, these concepts are identified and, ideally, relevant information is provided in a short version. These concepts are displayed as a learning map and must be proactively selected. Chatbot mediated learning has the advantage that matching concepts are offered as a pre-selection. Especially for inexperienced carers who are not familiar with the concepts, this learning path seems to be suitable.
Conclusion: The combination of learning through the “Information for Relatives” website and CML seems to meet all needs. In order to promote learner motivation, the chatbot should not only offer the identified concept, but also those related to this concept, in order to link new knowledge in one’s own knowledge network.
Keywords: informal care, dementia, didactic concept, didactic target group analysis, concept learning, anchored instructions
Introduction
In this paper, we present findings from a multidisciplinary healthcare project in Germany involving researchers from different disciplines: nursing science, higher education didactics, dementia researchers, service and user experience designers, computer scientists and ethicists. The eDem CONNECT project (2020–2023) was funded by the Federal Ministry of Education and Research. The aim of the project was to develop a chatbot-based communication and service platform for family caregivers to deal with agitation in people with dementia and to promote aspects of stability of care in the domesticity.
Dementia is one of the most popular chronic diseases in Germany. At the end of 2021, there were almost 1.8 million people with dementia living in Germany, 1.18 million of them women. The estimated number of people with dementia per square kilometre in Germany is 4.75.1 Detailed figures are published by the German society for Alzheimer’s disease.2 People with dementia suffer from the loss of cognitive abilities. Possible affected abilities are divided into executive functions (such as memory, judgement) and social cognition (such as language and motor skills). Essential for the disease is the progression of impairment. Agitation is the third most common neuropsychiatric symptom associated with dementia, the most are apathy and depression.3 Agitation is characterized by restlessness, aggressiveness, increased motor activity and emotional distress.3 About one in three people is affected with a prevalence of approximately 30% for agitation.3 Because of this changes, the distress and unmet needs of the person with dementia, resistance to care can arise, that upset the caregiving relatives.4
Digital approach to patients’ care have become in particular popular during and after the COVID.19 pandemic. To support caregiving relatives new technologies and non-pharmacological interventions can be helpful.5 A chatbot can be used as a low-threshold option for caregivers to support care activities, although we know that younger caregivers are more likely to be able to support the use of digital technologies in care processes.6
Our work package in the project, from which we present findings, focused on the didactic conditions of chatbot development and use. To support family caregivers of people with dementia, domain-specific knowledge is a prerequisite for chatbot development. Therefore a chatbot was generated in levels of development stages from a minimal viable product to different prototypes. The chatbot is integrated into an information website, where family caregivers, such as children, spouses or neighbors, can interact with it. They are able to give user-feedback on information and can save individual pieces of information, and use the ability to share diary entries with multiple users.
A chatbot is defined as
A computer program that has the ability to hold a conversation with human using Natural Language Speech7
The eDem connect is a text-based chatbot which asks questions and gives answers by responding to specific keywords. In complex care situations, a chatbot could be a hindrance. Chatbots - apart from ChatGPT, which is primarily a large language model and not a didactic tool - are still in their infancy in the education sector.8 According to Sonderegger and Seufert (2022),8 there are three maturity levels of chatbots in education: chatbots for individual chatbot learning based on domain knowledge, chatbots for social or collaborative chatbot learning based on social and contextual knowledge, and chatbots for metacognition and analytics acting as omniscient generative AI with a focus on learning progress and assessment.There are only few chatbots that address topics related to neurological disorder.9 In their mapping study of chatbots designed to change health behaviour, the authors found only three chatbots. Cho et al10 consider in their pilot study of a chatbot for physician training in cardiac auscultation, suggest that there are several advantages to chatbot-mediated learning. When a chatbot provides prompts to learners, this can be motivating for learning. There can also be environmental cues to support learning. Feedback plays an important role in the learning process. A chatbot is able to give immediate feedback and therefore supports learning.
To facilitate a successful learning scenario in an informal care setting, the environment needs to be taken into account. This environment includes the learning situation and the care situation. The carer’s learning situation is congruent with the caring situation and both influence each other. Mobile and microlearning are used as didactic approaches to address the burden of care and time resources. They allow time and local flexibility.11 To date, there are no didactic approaches that focus on carers of people with dementia as learners, nor assistive technologies that support the management of agitated behaviour.
Managing agitation is one of the most stressful factors for both caregivers and people with dementia.12 Daily family caregiving takes place between personal needs and the needs of the person with dementia. The family caregiver has to balance stability. That means stability is a trajectory as a cyclical process of changes in care and balancing of needs between the carer role, the dyadic relationship between caregiver and person with dementia, and the context of care.13 The social context also plays a central role. Relationships with other people and being integrated into social networks are important for family caregivers.14 Seidel and Thyrian15 furthermore emphasize the importance of knowledge about caregiver burden. Based on this knowledge, appropriate interventions can be developed to reduce burden. Tretteteig et al16 point out that family caregivers have to find a balance between their own needs and with those of the person with dementia.
But what are the specific needs and requirements of family caregivers of people with dementia who are experiencing agitation to engage with a chatbot? How can they benefit from a chatbot? How can family caregivers learn with a chatbot when they are experiencing a caregiving situation or in the aftermath of a caregiving situation? To answer these questions we conducted a literature-based target group analysis and qualitative interviews with the target group. Our research is based on the assumption that chatbot-mediated learning can support carers and that it can be designed didactically.
Materials and Methods
This study has a qualitative-exploratory research design. Based on a literature review on learning needs problem-based guided interviews were conducted. Our guiding research question was.
How can the didactic approach of mobile and micro learning for knowledge transfer via an information platform with integrated Chabot be transferred to caring relatives of people with dementia?
How must the content of the Chabot be didactically prepared so that the required information is formulated in a meaningful and understandable way for the target group? And What kind of learning strategies and learning styles are used by family carers of people with dementia? How can these strategies and styles be enabled by platform and chatbot? The German Society for Nursing Science (DGP e.V.) reviewed the research design and provided an ethical clearance. Family Caregivers received relevant information about the research and gave their informed consent.Didactic Target Group Analysis
By analyzing German and English literature published up to the beginning of the year 2020 using the terms dementia and family caregivers in various combinations with learning, teaching, eLearning, mobile learning, micro-learning, smartphone, digital media, Chabot, didactics, we found some indications of the target group. We searched in the following databases: CINAHL, Google Scholar and the comprehensive library catalogue of the TU Dortmund University Library. Inclusion criteria were: focus on caregivers and described learning behaviour or learning needs or formulated learning goals or motivation to learn. Exclusion criteria were not the right target group and no reference to the subject of learning. From 205 hits we removed duplicates and screened titles and abstracts. Twenty-five articles were analyzed for evidence of didactic and family caregivers. Six articles remained left with relevant evidence for the didactic target group analysis. Categories to describe the target group of family caregivers as learners are: heterogeneity and diversity, prior knowledge, motivation to learn, duration of learning, attitudes and experiences, place and time of learning.
Guided Interviews with Family Care Givers
The problem-based-interview-guide included questions about the target group’s handling of information, knowledge and experiences with chatbots. Six interviews were conducted via video chat between April 2021 and June 2022. On average, the interviews lasted 55 minutes with a range from 42 to 72 minutes. Six women and 2 men were interviewed (see Table 1).
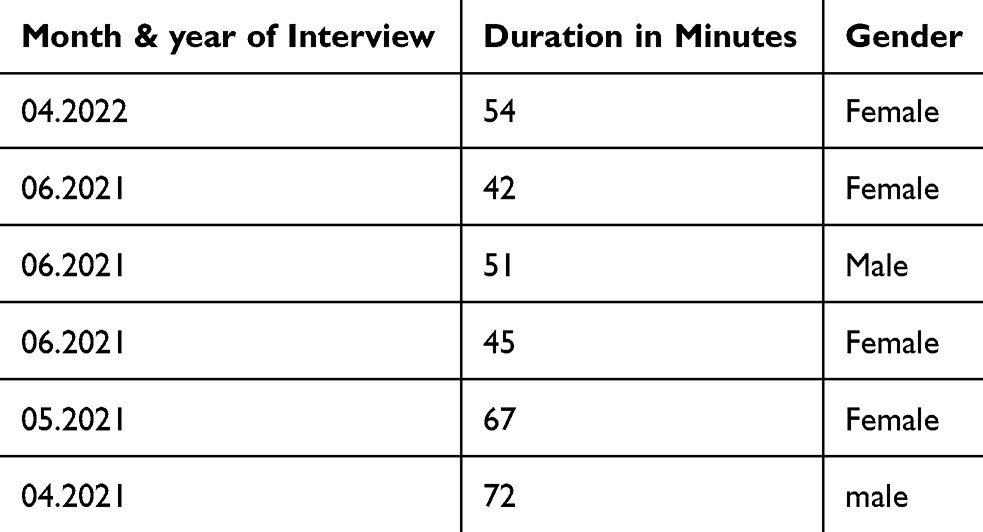 |
Table 1 Summary of Findings from the Didactic Target Group Analysis |
The interviews were recorded, anonymised and the audio was transcribed. Informed consent included publication of anonymised responses, and participants were informed of this. The interviews were analysed using Kolb and Kolb’s (2013) deductive experiential learning category system. According to this, learning occurs through the resolution of creative tensions between four learning modes. These learning modes can be understood as a double dialectic of action/reflection and experience/abstraction.17
Results
Results of the Didactic Analysis of the Target Group
Heterogeneity and Diversity
Carers of people with dementia are more likely to be women.18 While men tend to care exclusively for their partners, women are responsible for caring for their partners, (in-)parents and siblings.19 Hudson et al18 report the average age of family caregivers to be 59 years, with a range of 20 to 84 years. The age distribution of family caregivers in Paulicke et al20 ranges from 20 to over 60, with most falling into the 50–59 age range. However, in many care arrangements, several relatives provide care together. Carers experience high levels of stress, which can manifest in symptoms such as eating disorders, anxiety and depression.
Studies of spouses of cancer patients, many in the terminal stage of care, have reported eating disturbances, anxiety and depression due to the stress of caregiving21
Both the type of dementia and the severity of the illness influence the extent of the carer’s responsibility.The family caregiver role is strongly influenced by the type and severity of the illness and the responsibilities21
Although caring is experienced as a burden, carers feel the need to cope with the caring situation and to face the burden.Prior Knowledge
Prior knowledge refers to the cognitive schemas of caring relatives into which new knowledge can be integrated. It includes domain-specific prior knowledge, such as caring for people with dementia, and procedural prior knowledge, such as controlling learning, managing with media learning and media literacy. Hudson et al18 describe family caregivers as being experienced with caring. Similarly, they urge that these experiences must be examined more closely. They point out that experience can refer to simple support or to complex needs. And that it does not allow general conclusions to be drawn about caregiving competencies.18 Family caregivers have knowledge about different types of technical aids and how to use them.20 However, they should be addressed as medical laypersons so that information can be understood and used.21 In addition to a positive, confident attitude, communicative skills are to be conducive to a successful care situation.
Motivation to Learn
Motivation to learn can be used to identify what motivates caregivers to engage with digital media, technology, caring for people with dementia and learning. Similar to prior knowledge, this can be used to find points of contact for the learning opportunities that can be used to support motivation. Learners can be intrinsically motivated if they engage with a topic because they are interested or enjoy it. Alternatively, learners may be extrinsically motivated if they are pursuing goals such as a degree, higher status or increased income. Stoltz et al22 identify both duty and affection as motivations:
Some turned caring into labor, while others cared from a sense of duty or a sense of love
Motivation can also be understood as part of a cycle from success (in the care situation) to validation (doing the right thing) to motivation (through validation) to cooperation (in the care situation).21 The relationship between family caregivers and people with dementia is mutually beneficial. Stoltz et al22 confirm this assumption and identify feelings of reciprocity as a prerequisite for satisfaction. Houts et al21 therefore recommend assessing the motivation of carers so that they can be involved in a problem-solving process.There is evidence that family caregivers of people with dementia are not motivated to participate in external support programmes:
The fact that some caregivers do not feel comfortable in leaving their house to attend these programs (even with the option of having volunteers or others to stay with the patient) reinforces the need for the option of one-on-one interventions delivered at home to be available18
Duration of Learning
The duration of learning must be flexible, depending on external factors given by the care situation. The duration of learning is likely to be based on criteria related to the current care situation (tense versus relaxed) and the occasion of use (urgent problem or future scenario). The choice of learning forms is based on different temporal aspects. These are transferred to the learning content in a learning offer that is characterized by a range from micro-learning to enabling deep drilling. The enabling didactics23 is appropriate here, in which the needs of the learners are placed at the centre of all didactic activities. As access to the information platform is unrestricted 24/7, so that in addition to the main carer, other relatives or professional carers can also use the information, synergies are possible in this way.
Attitudes and Experiences
With regard to technical equipment, an experienced target group can be assumed, as technical care aids and technical equipment such as tablets and GPS watches are known.20 These are used when human assistance is unavailable or insufficient. However, women over the age of 65 are inexperienced in using Chabot. Therefore, they should receive instruction before using the information platform. This could take the form of a demonstration of how to use the Chabot, followed by an opportunity to test it under supervision.
Place and Time of Learning
The time and place of learning is determined by family caregiver and needs to be flexible. Mobile learning can make this possible. In combination with micro-learning, information units are tailored to the target group, limited in time and reduced to the essentials.11 These two elements are complemented by aspects of enabling didactics.23 Enabling didactics facilitates different ways of learning and supports learning with individual learning strategies. This means, for example, that individual learning content can be deepened at a later time, if the care situation is stable. The most important findings are summarized in Table 2.
 |
Table 2 Summary of Findings from the Didactic Target Group Analysis |
Results: Learning Strategies
Learning strategies are unique ways of individuals dealing with information and knowledge. Analysis of the interviews provides insights into how family carers deal with information and knowledge. Information is assessed in terms of its scope, its relevance to one’s own caring situation and its adaptability to the situation. Information becomes knowledge when strategies can be developed to deal with it or when it proves itself in practice. Information is relevant to the extent that it corresponds to the care situation or can be adapted to it. In addition to searching for information in analogue or digital media, carers prefer to consult experts or other carers. Consulting experts refers to social aspects of learning.
Learning is a process17 that can be ideally described as follows: it begins with a concrete experience. The learner reflects this experience, compares it to his or her previous knowledge and analyses the experience to construct abstract concepts. Active experimentation with new concepts and conclusion of reflections can lead to new experiences.
The interviewed person G describes a complete learning process:
The information in the seminar that that people with dementia are often no longer able to can no longer follow the words, but very precisely - whether you are facing the person and treat them nicely and kindly and affectionate, is much more important than what you actually say. (Interview G)
Describes the concrete experience. On the basis of this experience G reflects:This insight, I found very groundbreaking and has helped me very well, for example with my father-in-law’s girlfriend
G conceptualizes this reflection:And I actually think the words were completely unimportant, but just the looking and the smiling and talking to one
G concludes by experimenting with the concepts of looking and smiling:And that was, that wasn’t demanding, you didn’t have to think about it, you just said any words and smiled and always, you emphasize differently and yes and hm, somehow like that, no, like you do in normal conversation.
Nine different learning strategies can be used by learners in the learning processes of the four modes of concrete experience, reflective observation, abstract conceptualisation and active experimentation.
In the analysis of the interviews, the participants could be assigned to different learning styles, but the narrative sequences often contain strategies that are combined in one statement. The learning style initiating initiates action in order to create new experiences and situations.17 For example G states the importance of being prepared:
But then I always like to have a bit of a, like a, like a contingency plan in the back of my mind. What happens if, if tomorrow is this or that (G: 99–99)
Interview D points out getting initiated byI would like to have several delivered so that I can try - - one after the other. Because it does not mean that the first hit is necessarily the most suitable for me (D: 116–116)
The experiencing styles involves deep involvement in experiences. For example C, explains this about gathering information:
I have to be able to read it. Again and again. So not just once, ne, but again and again, gosh, how was that and then again (C: 114–114)
The Imagining style is the ability to imagine possibilities for observation or experience.17 An example for this style is described by G:
It’s always much easier when the person - so with a lot of imagination, I think you, you need a relatively lot of imagination to implement some things like that, in order to, because that might not fit on the one, but if you then with, with an idea, you don’t do it in red, but in green. (G: 118 - 118)
A strong motivation for goal directed action is describes by the acting style. K gives an example how to save and act with information:
Take photos with your mobile phone, label these photos and you can also use a great drawing program to make a circle or an arrow and, no, important or important part or there, there’s the reset point or something. (K: 170 −170)
In the balancing style, the learner weighs up the pros and cons of doing, reflecting on or experiencing something. We found an example of H:
When someone tells me that I need to know this, I always ask first: Do I really need to know this? Is that important for me? (H: 94–94).
In the reflecting style, experiences and ideas are linked with reflection. G reflects on information that fits to the individual caregiving situation.
Yes, of course they have to fit the respective life situation. Everyone is different (G: 101–101).
D points out that learning activities must take into account other tasks and the workplace.
In the deciding style theories and models are used as a basis for decision-making.17 The caregivers we interviewed did not mention theories, but they did point out that they prefer to consult experts or other knowledgeable people:
What I need at the moment, of course I always try to ask for and get immediately from the people I know (G: 85–85).
The thinking style concerns abstract and logical reasoning. A emphasizes the need to visualize information for better understanding and to make connections between the information presented:
than if, then I already need a precise answer. So a) it is possible and b) now, if we stay with the example - so it was not possible now, but that it is nevertheless, when I ask where one could get such a (laughs) a - product, which I just asked for, in my neighbourhood, who offers it, […] the more I could then already get information in advance. (A: 48 - 49)
In the ninth style analyzing involves abilities to integrate and systematize ideas through reflective activities. G describes this style as follows:
But these are more general things that don’t affect me yet, but I always like to have a bit of background knowledge. When things get worse, what I have at hand and what alternatives there are. (G: 85 - 85)
Discussion
Key findings from the results are, that the learning situation is simultaneously the caring situation in which learning can potentially take place around the clock. The boundaries between caring and learning are fluid. Adult learning should build on previous knowledge up and integrate the learners’ previous experiences.24 Adult Learning should be self-determined and problem-oriented. Learning content must also be relevant and practicable, according to the respondents. Modular sentence structure restricts the ability to get a detailed overview of the entire learning content.
Otherwise, Raunig25 points to a serendipity effect, which describes how learners can learn something that was not intended. Based on this finding, we developed a didactic concept for the target group of family caregivers and compared informal chatbot-mediated learning habits with technical requirements and environmental factors. The aim is to provide information on how to deal with agitation in people with dementia via a digital information platform. The focus is on the concepts of pain in people with dementia and communication with people with dementia. Both are potential causes of agitated behavior. There are no teachers in this informal teaching/learning setting, the chatbot cannot and should not take the role of a teacher. When learning with a chatbot (chatbot-mediated learning) or digital learning, the reflection of the learning path and the initiation of social exchange play an essential role. In addition to the chatbot with micro-content, there is an information area with the complete learning content. Learners can choose whether they want to learn with the chatbot or browse the content to get an overview.
One principle to support learners is concept learning. Learners have a cognitive conceptual network that has more or fewer links (ie relationships) between concepts depending on their state of knowledge. Learners have individual knowledge maps in their heads. The chatbot can build bridges between previous and new knowledge in this map. The aim of concept learning is to enable learners to find individual points of contact in their own knowledge network in order to be able to connect new knowledge. The didactic method Anchored Instruction is used to provide individual information while taking into account time constraints. The chatbot offers different media as narrative anchors, such as text, image, video. This avoids “inert knowledge” and instead supports the acquisition of knowledge that can be flexibly applied to different situations. This should take place in real, authentic and complex situations in which solutions to problems are open.26 Learning outcomes are the analysis of problems in daily care and their constituent factors, and the application of new knowledge to care. With regard to the care situation, each learning content is offered in a short version with the most important information and in a long version with detailed information on the phenomena of agitation in people with dementia, according to didactic reduction and possible deepening. For example, a learning objective for pain is:
The learner will recognize when their relative with dementia is in pain and how they express pain, and take appropriate measures to prevent or treat pain
Deep drillings in this case are decision making for problem solving and reflection on problem solving activities.In addition to its answer to a question, the chatbot suggests as micro-content possible deep dives into the topic. At the end of the chatbot dialogue, the chatbot encourages reflection on the new knowledge gained. Learners acquire this knowledge on their own responsibility and check the individual fit to their care situation.
As stated by Pereira and Daiz,9 the enabling factors for the use of chatbots depend on anonymity, asynchrony, consumability, authentication, personalisation and scalability. These aspects are also relevant for didactical design, as our findings show. Asynchrony from a didactic perspective means that the chatbot is used after problematic situations, so that the application scenario does not have to be identical to the care situation. Anonymity is also relevant for caregivers, who have the possibility to interact anonymously. In particular, caregivers point to the ability of chatbots to be customized to their needs and personal situation. Personalization from a didactic perspective refers to enabling didactics and the two learning paths, the short one and the longer one.
In contrast to Cho et al10 the learning situation and the caring situation must be decoupled, so that given prompts from the chatbot will not be helpful or motivating for learning because the caring situation does not allow that. Creating individual feedback will be a task for future didactical chatbot concepts.
Limitations
Due to the qualitative methodological approach, only a small, regional sample from an urban area was involved in the project and the development of the chatbot. In particular, the pandemic had a strong influence, as the pandemic restrictions started immediately after the start of our project. As a result, the participation of family caregivers was less intensive and took place via videoconferencing rather than face-to-face in workshops. The development of generative AI at the same time as the pandemic is a limitation. The specialized chatbot developed for a specialized target group works with an expert ontology for this topic and can therefore be extended to link to related topics. Future work has to address questions of generative AI and specialized products in research and education. We also use our findings in our teaching of health students.
Conclusion
Answering the guiding research questions mobile and micro-learning are didactical approaches that can be used for chatbot-mediated learning for family caregivers. Information should be offered in different ways, eg a long and a short version, depending on the individual circumstances of the caring situation. Caregivers, like the rest of us, use different learning styles. Their learning is characterized by the caring situation. Facilitating factors mentioned by the respondents for chatbot-mediated learning are: information in different forms like text, video or pictures, the possibility to save or print the information offered by the chatbot, lists of information as overviews, short and precise information, information adapted to individual needs, understandable information, social context or possibility to talk with others about the information as well as facts instead of long stories.
Barriers to chatbot mediated learning from caregivers’ perspective are: lack of context, no direct reference to individual needs, too much information, information not relevant to the question. Mobile learning, ie location-independent learning with a mobile phone or tablet, and micro-content, ie didactically reduced, short information, are used to counteract the high stress levels and time constraints. Chatbot mediated learning offers the advantage of situatedness. Learners are given the opportunity to gain conceptual clarity about concepts. Thus, domain-specific chatbots can be a supportive moment for caregivers.
On the one hand, they are compatible with both behaviourist and more progressive settings; on the other hand, a priori and general assessments of the effectiveness of learning with chatbots seem difficult - these depend on the concrete (successful) implementation, so that a judgement is reserved for subsequent empirical studies.27
Acknowledgments
We would like to thank the family caregivers for their support of the project and their views on learning with chatbots.
Disclosure
The study was funded by the German Federal Ministry of Education and Research. The authors report no conflicts of interest in this work.
References
1. Thyrian JR, Boekholt M, Hoffmann W, et al. Die Prävalenz an Demenz erkrankter Menschen in Deutschland – eine bundesweite Analyse auf Kreisebene. Nervenarzt. 2020;91(11):1058–1061. doi:10.1007/s00115-020-00923-y
2. Deutsche Alzheimer Gesellschaft e. V. Informationsblatt 1: die Häufigkeit von Demenzerkrankungen. Available from: https://www.deutsche-alzheimer.de/fileadmin/Alz/pdf/factsheets/infoblatt1_haeufigkeit_demenzerkrankungen_dalzg.pdf.
3. Carrarini C, Russo M, Dono F, et al. Agitation and Dementia: prevention and Treatment Strategies in Acute and Chronic Conditions. Front Neurol. 2021;12:644317. doi:10.3389/fneur.2021.644317
4. Mast BT, Ertle EM, Kolanowski A, Mountain G, Moniz-Cook E, Halek M. Person-centered assessment of apathy and resistance to care in people living with dementia: review of existing measures. Alzheimers Dement. 2022;8(1):e12316. doi:10.1002/trc2.12316
5. Toniolo S, Scarioni M, Di Lorenzo F, et al. Dementia and COVID-19, a Bidirectional Liaison: risk Factors, Biomarkers, and Optimal Health Care. J Alzheimers Dis. 2021;82(3):883–898. doi:10.3233/JAD-210335
6. Arighi A, Fumagalli GG, Carandini T, et al. Facing the digital divide into a dementia clinic during COVID-19 pandemic: caregiver age matters. Neurol Sci. 2021;42(4):1247–1251. doi:10.1007/s10072-020-05009-w
7. Abdul-Kader S, Woods J. Survey on Chatbot Design Techniques in Speech Conversation Systems. ijacsa. 2015;6(7). doi:10.14569/IJACSA.2015.060712
8. Sonderegger S, Seufert S. Chatbot-mediated Learning: conceptual Framework for the Design of Chatbot Use Cases in Education. In:
9. Pereira J, Díaz Ó. Using Health Chatbots for Behavior Change: a Mapping Study. J Med Syst. 2019;43(5):135. doi:10.1007/s10916-019-1237-1
10. Cho K, Foo YM, Dalziel B, Hu W. Chatbot-mediated learning of cardiac auscultation. Intern Med J. 2022;52(12):2176–2180. doi:10.1111/imj.15971
11. Sirwan Mohammed G, Wakil K, Sirwan Nawroly S. The Effectiveness of Microlearning to Improve Students’ Learning Ability. Int J Educ Res Rev. 2018;3(3):32–38. doi:10.24331/ijere.415824
12. Maust DT, Kales HC, McCammon RJ, Blow FC, Leggett A, Langa KM. Distress Associated with Dementia-Related Psychosis and Agitation in Relation to Healthcare Utilization and Costs. Am J Geriatr Psychiatry. 2017;25(10):1074–1082. doi:10.1016/j.jagp.2017.02.025
13. Köhler K, Dreyer J, Hochgraeber I, et al. Towards a middle-range theory of ‘Stability of home-based care arrangements for people living with dementia’ (SoCA-Dem): findings from a meta-study on mixed research. BMJ Open. 2021;11(4):e042515. doi:10.1136/bmjopen-2020-042515
14. Pinkert C, Köhler K, von KM, et al. Social inclusion of people with dementia – an integrative review of theoretical frameworks, methods and findings in empirical studies. Ageing Society. 2021;41(4):773–793. doi:10.1017/S0144686X19001338
15. Seidel D, Thyrian JR. Burden of caring for people with dementia - comparing family caregivers and professional caregivers. A descriptive study. J Multidiscip Healthc. 2019;12:655–663. doi:10.2147/JMDH.S209106
16. Tretteteig S, Vatne S, Rokstad AMM. Meaning in family caregiving for people with dementia: a narrative study about relationships, values, and motivation, and how day care influences these factors. J Multidiscip Healthc. 2017;10:445–455. doi:10.2147/JMDH.S151507
17. Kolb A, Kolb D The Kolb Learning Style Inventory 4.0: a Comprehensive Guide to the Theory, Psychometrics, Research on Validity and Education Applications; 2013. Available from: https://learningfromexperience.com/research-library/the-kolb-learning-style-inventory-4-0/.
18. Hudson P, Thomas T, Quinn K, Cockayne M, Braithwaite M. Teaching family carers about home-based palliative care: final results from a group education program. J Pain Symptom Manage. 2009;38(2):299–308. doi:10.1016/j.jpainsymman.2008.08.010
19. Brügger S, Jaquier A, Sottas B. Belastungserleben und Coping-Strategien pflegender Angehöriger. Perspektive der Angehörigen. Z Gerontol Geriatr. 2016;49(2):138–142. doi:10.1007/s00391-015-0940-x
20. Paulicke D, Buhtz C, Meyer G, Jahn P. Beratungsansätze zu assistiven Technologien in der Pflege von Menschen mit Demenz. Pflege. 2019;32(6):315–323. doi:10.1024/1012-5302/a000701
21. Houts PS, Nezu AM, Nezu CM, Bucher JA. The prepared family caregiver: a problem-solving approach to family caregiver education. Patient Educ Couns. 1996;27(1):63–73. doi:10.1016/0738-3991(95)00790-3
22. Stoltz P, Udén G, Willman A. Support for family carers who care for an elderly person at home - a systematic literature review. Scand J Caring Sci. 2004;18(2):111–119. doi:10.1111/j.1471-6712.2004.00269.x
23. Arnold R. Learning and Teaching in adult education. In: Sava S, Novotny P, editors. Researches in Adult Learning and Education. The European Dimension. firenze university press; 2016:43–54.
24. Knowles MS, Holton EF III, Swanson RA, Robinson PA. The Adult Learner. Routledge; 2020.
25. Raunig M. Lernmedium Chatbot. Medien in der Wissenschaft; Band 78. In: Wollersheim H-W, Karapanos M, Pengel N, editors. Bildung in der Digitalen Transformation. Münster, New York: Waxmann Verlag; 2021:101–110.
26. Gerstenmaier J, Mandl H. Wissenserwerb unter konstruktivistischer Perspektive. Zeitschrift für Pädagogik. 1995;41. doi:10.25656/01:10534
27. Rauner F. Gestaltungskompetenz: Die Leitidee der modernen Berufsbildung. Wiesbaden, Heidelberg: Springer VS; 2021.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.