Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Characterizing Different Multidisciplinary Team Models Implemented Within One Comprehensive Cancer Center
Authors Alfieri S ![]() , Brunelli C
, Brunelli C ![]() , Borreani C, Capri G, Angi M, Bianchi GV, Lo Dico S, Spada P, Fusetti V, Zecca E, Caraceni A
, Borreani C, Capri G, Angi M, Bianchi GV, Lo Dico S, Spada P, Fusetti V, Zecca E, Caraceni A
Received 16 January 2023
Accepted for publication 15 May 2023
Published 29 June 2023 Volume 2023:16 Pages 1845—1855
DOI https://doi.org/10.2147/JMDH.S402348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sara Alfieri,1,* Cinzia Brunelli,2,* Claudia Borreani,1 Giuseppe Capri,3 Martina Angi,4 Giulia V Bianchi,3 Silvia Lo Dico,2 Pierangelo Spada,5 Viviana Fusetti,2,6 Ernesto Zecca,2 Augusto Caraceni2,7
1Clinical Psychology Unit, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 2Palliative Care, Pain Therapy and Rehabilitation Unit, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 3Medical Oncology 1, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 4General Oncology Surgery 4, Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 5Nursing, Technicians and Rehabilitation Management Service (SITRA), Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy; 6Biomedicine and Prevention Department, University of Rome “Tor Vergata”, Rome, Italy; 7Department of Clinical and Community Sciences, Università degli Studi, Milan, Italy
*These authors contributed equally to this work
Correspondence: Cinzia Brunelli, Palliative Care, Pain Therapy and Rehabilitation Unit, Fondazione IRCCS Istituto Nazionale dei Tumori, Via Venezian 1, Milan, 20133, Italy, Tel +39 0223903179, Email [email protected]
Background: The multidisciplinary approach is considered “best practice” in oncology. Multidisciplinary Teamwork (MDTW) can be broadly classified into Multidisciplinary Team Meetings (MDTM) and Multidisciplinary Cancer Clinics (MDCC; involving also patients), yet both models are heterogeneously implemented.
Purpose: This study aims at describing the different MDTW implemented models in a Comprehensive Cancer Center.
Methods: All clinical unit directors of the hospital were contacted to identify any MDTW activities the personnel of the unit were involved in. Structured interviews were carried out to collect MDTWs information, ie, type (MDTM vs MDCC), team composition, aims, disease phase, use of Patient Reported Outcome Measures (PROMs). Descriptive analyses and Social Network Analysis (SNA) were performed.
Results: Among 38 structured interviews, 25 concerned MDTMs and 13 in MDCCs. Responders were mainly surgeons (35%) and oncologists (29%), 35% of them were team leaders. Teams were mostly composed of physicians only (64% in MDTMs, 69% in MDCCs). Case managers (8% and 31%), palliative care specialists (12% and 23%) and psychologists (20% and 31%) were involved to a lesser extent, mainly when dealing with advanced disease. MDTWs were mainly aimed at integrating the skills of the different specialists (respectively 72% for MDTMs and 64% for MDCCs) and offering the best overall patient care pathway (64%, 61.5%). MDTWs were directed at patients in both diagnostic (72%, 61.5%) and locally advanced/metastatic (32%, 38.4%) disease. PROMs were seldom used (24%, 23%). SNA shows a similar density in the two MDTWs, but in the MDCCs two nodes remain isolated (pathologists and radiologists).
Conclusion: Despite a high number of MDTWs for advanced/metastatic disease, there is limited involvement of palliative care specialists, psychologists, and nurses.
Keywords: case conferences, multidisciplinary cancer conferences, multidisciplinary visits, oncology, tumor board, tumor conferences
Introduction
The term “multidisciplinary” is used in medicine to describe a treatment planning approach or team that integrates relevant healthcare disciplines that have a direct or indirect impact on patient management.1 In oncology, this concept was introduced by Henry Kaplan and Saul Rosenberg at the Stanford University in the 1960s to point out
A need-based approach adopted by the oncologic community to facilitate interdisciplinary interaction, foster patient and care-giver confidence, optimize patient care, and help improve outcomes. (p. 72)2
Starting from the intuition of Kaplan and Rosenberg, “Multidisciplinary” Teamwork (MDTW) has entered common clinical practice in the management of cancer patients.3,4 The Organization of European Cancer Institute (OECI) issues the accreditation only if cancer-centers can provide evidence of multidisciplinary clinical meetings.5 Despite an ever-increasing diffusion of MDTWs, the evidence showing their impact on clinical outcomes is limited and sometimes contradictory.6–9
Heterogeneous types of MDTWs emerge in the literature,10 with respect, at least, to objectives, team composition, referral criteria. Most often, MDTWs focus on one type of cancer (ie, lung) or group of cancers (ie, genitourinary). Therefore, the team composition will vary depending on cancer type and is often left to local discretion, the only common aspect being the co-presence (physical or virtual) of several specialists at the same time. The primary specialists are generally oncologists, surgeons and radiation oncologists.1 Together with these professionals, Taberna et al also suggested the presence of oncological radiology: they call them “the four pillars” of Optimal multidisciplinary care.11
Some studies question the feasibility of MDTWs due to limited resources of time, staff, and spaces. Authors suggest the importance of having access to clinical case management and administrative support to speed up and optimize processes.9,12
Depending on whether the patient is present or not, two main MDTW models may be identified (13): Multidisciplinary Team Meetings (MDTM; also known as “Multidisciplinary cancer conferences”, “Case conferences”, “Tumor Conferences”, “Tumor Boards”) and Multidisciplinary Cancer Clinics (MDCC; also known as “Multidisciplinary Visits”). However, there are some exceptions: literature has documented experiences in Germany and Australia where patients were also invited to participate in MDTMs.13,14
MDTMs are meetings held on a regular basis, in which different specialists discuss clinical cases to propose joint and guideline treatment plans, in the absence of the patient.15 The objectives of the MDTMs can vary. Wright et al16 pointed out that MDTMs aim to ensure all appropriate tests, options, and treatments for individual case discussion. Gatcliffe et al17 highlights that MDTMs are mechanisms aimed at reaching a consensus on the treatment of the patient through an interdisciplinary consultation based on dialogue. Hammer and Prime,18 instead, defined an MDTM as a “meeting, where a team of expert clinicians discuss complex cases to determine the best possible treatment plan for a patient” (p.2214). However, there are common views on two aspects: 1. the importance for the professional growth of healthcare professionals participating; 2. the identification of potentially eligible patients to clinical trial.16–20 In the systematic review by Wright et al,16 differences also emerged with respect to referral criteria (eg, all patients vs new cancer cases vs patients selected by the coordinator), meeting format (frequency and time length), team members (group composition), roles and responsibilities (chair and coordinator).
While MDTMs are well established in oncology practice, there is also growing support for the implementation of MDCCs. In MDCCs, the patient is present and the clinicians directly interact with him or her. (13) The patient receives input about his clinical condition and treatment plan proposal from a multidisciplinary team; a shared decision is then reached jointly taking into account the patient preferences and perspective.
Page et al19 highlight some differences between MDTMs and MDCCs. The first and most important is that, while MDTMs are primarily aimed at reaching professional consensus on treatment recommendations based on disease characteristics, in MDCCs the treatment decision process is based on the consensus between the physicians and the patient; for this reason, the consensus reached is not only “disease centered”, but “patient-centered”. A second difference is that MDTMs are open to more practitioners, while MDCCs usually include only professionals involved in patient care. Although the composition of the teams is similar as regards clinical representation, in MDCCs it can be necessary to increase its clinical representation to other support staff, such as social workers, primary care physicians, psychologists, clergy and others. Given the wide variability in MDTW models, the aim of the present study is to provide a real-world description of different multidisciplinary approaches implemented in a Comprehensive Cancer Center.
Methods
Study Design
A survey was carried out in Milan at the Fondazione IRCCS Istituto Nazionale dei Tumori (INT) from January to May 2021. All clinical unit directors of INT were contacted by email by the principal investigator [AC]. They were asked to indicate: 1. which MDTMs and/or MDCCs their department organized and/or participated in; 2. the names of professionals in their unit participating in any MDTMs and/or MDCCs; 3. the authorization to contact the above professionals for a short and structured interview (by telephone, online, or face to face). All the professionals listed were contacted.
Assessment
An ad hoc and structured questionnaire (please see Appendix 1) was developed to investigate characteristics of MDTWs on the basis of the existing literature and in accordance with the interests of the research group: type (MDTM and/or MDCC), name of MDTW, disease phase (diagnostics, pre-surgical, post-surgical, locally advanced/metastatic and others), years since establishment, description of aims of the MDTW, composition of the team (profession coordinator and permanent professionals), frequency of the meetings, referral criteria, recommended documentation for the MDTW, reporting documentation, use of Patient Reported Outcomes Measures (PROMs), and inclusion in a formalized/institutional care pathway. Two further items investigated responders’ opinions with respect to a possible need for training: “Do you deem it useful for professional involved in MDTW to undergo a specific training on multidisciplinary working?” and “What aspects, in your opinion, should the training deal with?”.
Most of the questions required “closed answers” with the possibility of multiple choices. However, three open questions were chosen for the description of aims, the referral criteria, and the topics to be treated in the training. No closed alternative answers were proposed to leave free expression and argument to respondents. The answers to these questions were categorized based on meaning by authors [SA and CB] and analyzed quantitatively as “closed answer”.
Statistical Analyses
Descriptive Statistics
Percentages (%), medians, means (M) and Standard Deviations (SD) were calculated for descriptive purposes.
Social Network Analysis (SNA)
SNA was applied with the aim of obtaining information about the structure of the two different MDTWs. SNA is a set of structural analyses techniques based on the assumption that the explanation of social phenomena should be based on the analysis of the relationships that bind the elements rather than from the characteristics of such elements. A network is composed of “nodes” which can be actors (in our case permanent professionals variable) or events (in our case different MDTWs variable), and of “ties”, indicating the “connections”/result of interactions between nodes.21,22 Although SNA has been widely used to analyze workgroups,23–25 to date there are no applications to MDTWs. In order to reflect the level of connectedness in the MDTWs, we calculated density, which represents one of the main descriptive statistics and is often used as an indicator of the degree of network cohesion. Density is the ratio between the number of effective connections between nodes and the highest number of connections theoretically possible in the network. Thus, it is an indicator that provides information about the entire network, and not only on a specific MDTW. The density varies from 0 (when the network is empty and no node is connected to another) to 1 (when the network is complete and all nodes are connected to each other). Density was calculated separately for MDCCs and MDTMs using the same set of theoretically potential actors. The graphic configuration of the network is also presented, as it provides immediate information about the nodes and their ties.
We used IBM Statistical Package for Social Science (SPSS) Version 26.0® for descriptive analyses and UCINET® (demo version) for SNA.
Context
INT is a public foundation and government-designated clinical and research hospital; it is a leading cancer center in Italy pursuing mainly clinical and translational research, aimed at providing prevention, early diagnosis, and treatment of cancer, as well as at improving patients’ quality of life. INT has been designated as Comprehensive Cancer Centre by OECI and is a member of the Cancer Core Europe Consortium.26
Ethical Issues
The project was approved by INT’s institutional review board (INT 269/20) and all responders provided oral informed consent to survey participation. The study is part of a broader project that aims to explore the feasibility and the effect on patient experience of care of an MDCC model for patients with advanced cancer.
Results
Participants
Clinical unit directors reported 38 MDTWs and provided the names of 31 professionals to be contacted for the interview; all of them agreed to participate. Six participants responded for two or three MDTWs. Of the 38 interviews analyzed, 65.8% (n = 25) referred to MDTMs and 34.2% (n = 13) to MDCCs. The full list of the 38 MDTWs is reported in Appendix 2.
Responders were surgeons (35.5%; n = 11), medical oncologists (29.0%; n = 9), nurses (9.7%; n = 3), psychologists (6.5%; n = 2), radiotherapist (3.2%; n = 1), 9.7% and other professionals (16.1%; n = 5). 54.8% (n = 17) of the participants were women; 35.5% (n = 11) were the team leaders.
MDTMs Characteristics
Table 1 shows detailed information for both MDCCs and MDTMs. As far as MDTMs are concerned, the most frequent disease phases are the diagnostic and locally advanced/metastatic ones (in both cases 72.0%). Meetings are most frequently coordinated by physicians, mainly surgeons (24.0%); in around one-third of the cases (36.0%), the meeting is not formally led by anyone. Core team components include medical oncologists (68.0%), surgeons (64.0%), radiotherapists (52.0%), radiologists (52.0%); other, yet heterogeneous, professionals are also common (80%). About 28.0% of responders reported the participation of a case manager in MDTMs. However, upon a request for further information on the role of the case manager, respondents reported that they could be either nurses or administrative professionals. In most cases (64.0%), the MDTMs include only physicians; the average number of permanent components is 3.9 (Range: 2–6; SD = 1.1; median = 4.00), and the average time since MDTMs establishment is 11.39 years (Range: 1–23; SD = 7.2; median = 10.0). The first two MDTMs, which started in 1998, were those related to breast cancer and pediatrics (no tumor-specific). In the last 5 years, 6 MDTMs have begun: pathological anatomy, molecular tumor board, colon rectal tumors, terminal management of the pediatric patient, hereditary tumors of the digestive system and genitourinary tumors. Most MDTMs take place once a week (68%). The documentation requested for the visit is mainly related to imaging (60%). Thirty-six percent of clinical reports are not included in an institutional database. Less than one-third (32%) of MDTMs are known to be included in a formalized/institutional care pathway, and 28% of responders declare not to be aware of it. The use of PROMS was reported by 24% of responders.
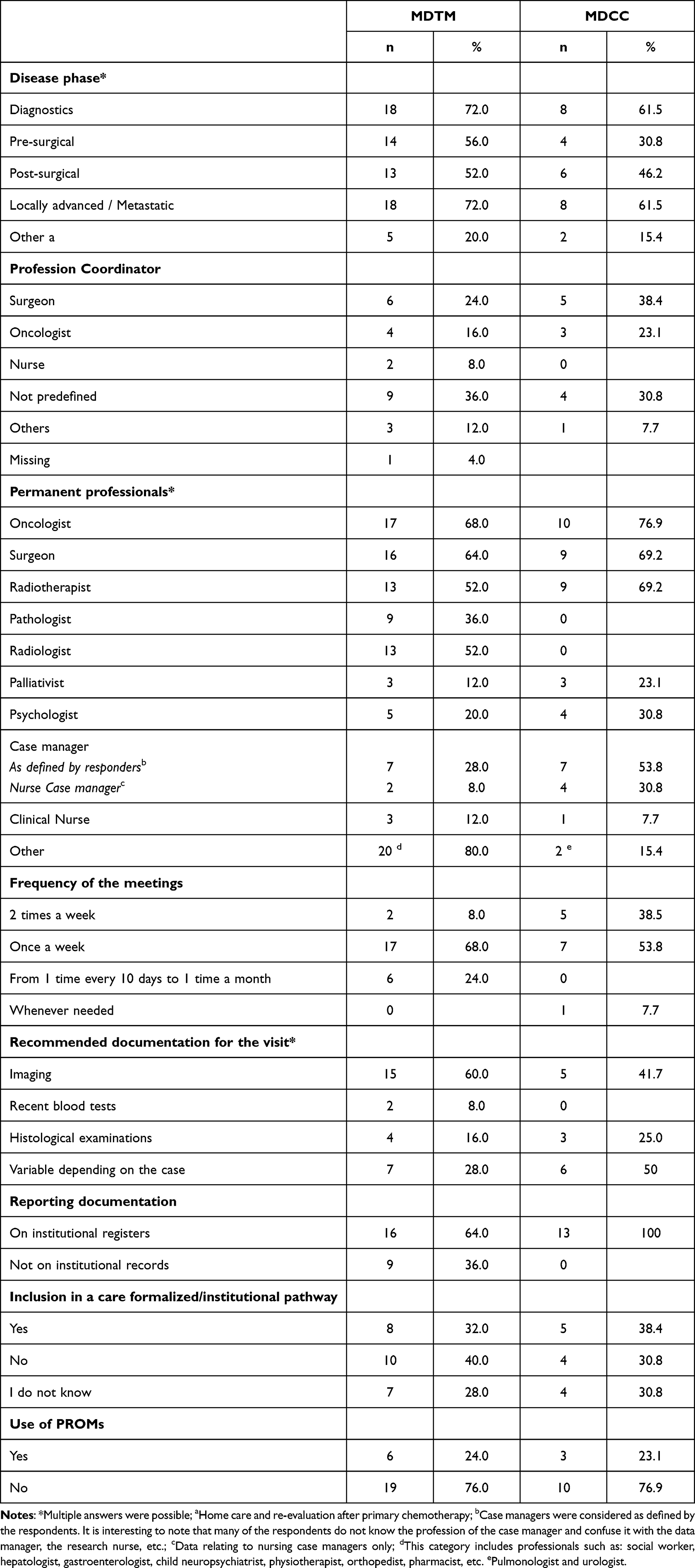 |
Table 1 Characteristics of MDTM and MDCC |
Table 2 shows MDTWs objectives as reported by responders (open-answers): MDTMs are reported to be mainly aimed at integrating the skills of the different specialists (72.0%) and at planning a more personalized diagnostic-therapeutic pathway (64.0%); the most frequently applied referral criteria for the MDTMs are specific diagnostic-clinical criteria (56.0%) and problematic or complex cases (52.0%).
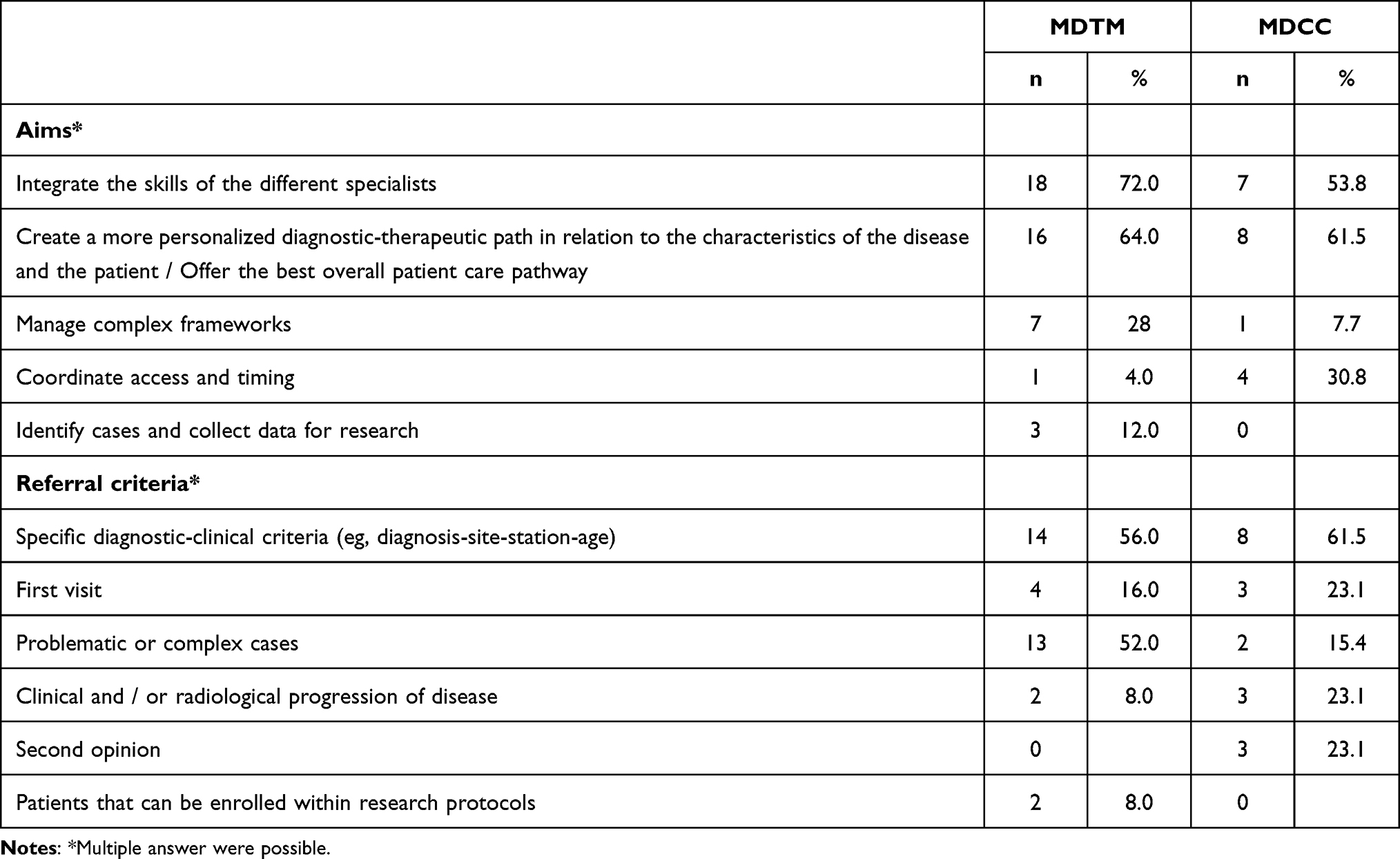 |
Table 2 Aims and Referral Criteria of MDTM and MDCC |
Half of respondents (n = 15, 50.0%, 1 missing) reported that training needs are related to MDTWs participation; in particular, they deem relevant to improve both communication and leadership skills.
MDTMs Network
Figure 1a describes the structure of the MDTMs network. SNA shows a network of 35 nodes and 99 ties, with a density of 0.39 (SD = 0.48), which indicates a low level of network cohesion, as only 39% of all possible links are present. Although all nodes have at least one tie (and, therefore, no node is excluded from the network), some professionals have few ties, in particular palliative care specialists, psychologists, and nurses (case managers and clinical nurses).
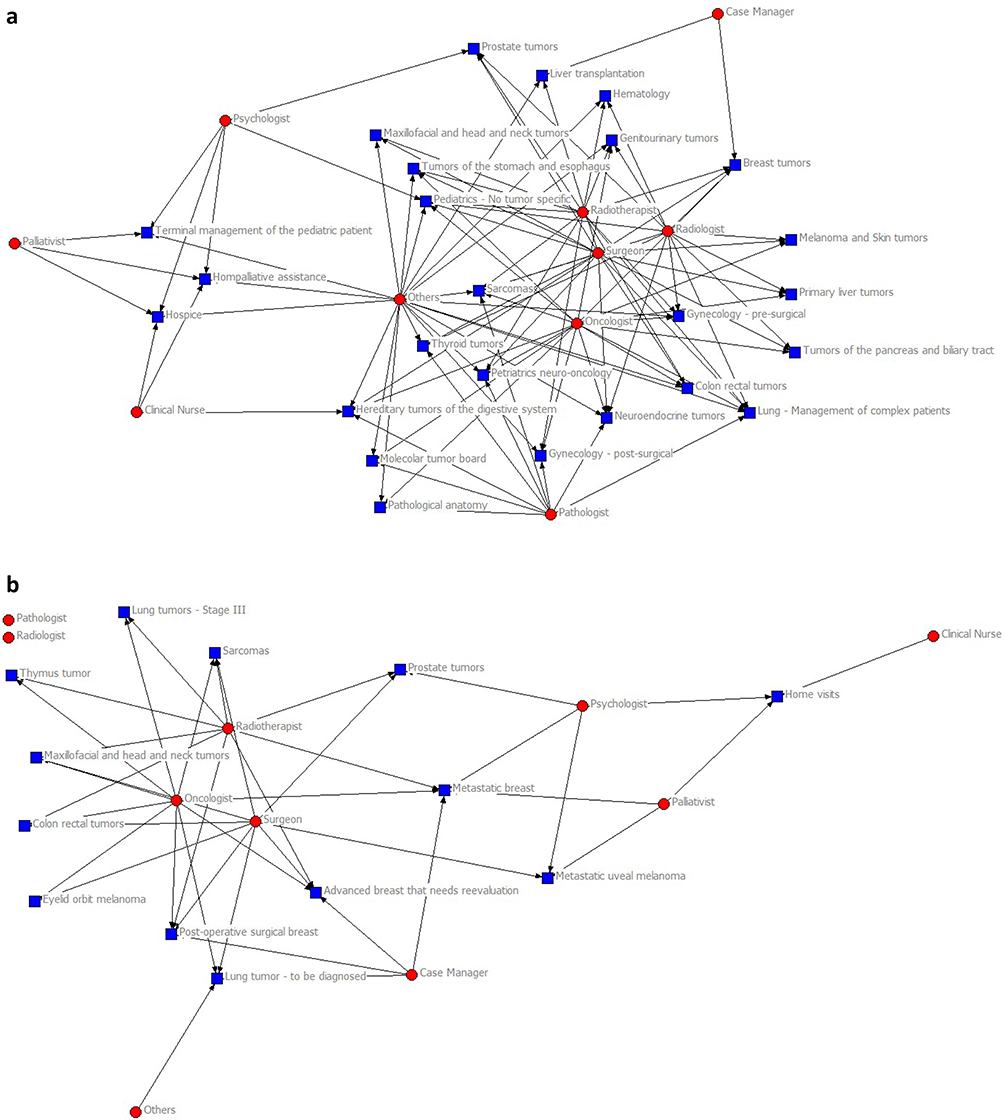 |
Figure 1 (a) MDTM Network. (b) MDCC Network. |
MDCCs Characteristics
Also, MDCCs show a fairly balanced distribution between the diagnostic and locally advanced/metastatic disease phases involved (in both cases 61.5%). In 38.5% of the cases, the coordinator is a surgeon; it is not defined in 31% of them and it is represented by a medical oncologist in 23%.
Surgeons are among the professionals most often included in the core team (69%), together with oncologists and radiotherapists (both 69%). In most cases (69%), the MDCCs include only physicians; the average number of permanent members is 2.9 (Range: 2–5; SD = 0.75; median = 3.00) and these MDCCs were established for an average of 8.4 years (Range: 1–34; SD = 10.0; median = 3.0). The first MDCC dates back to 1987 and was related to home palliative care activation. In the last 5 years, 8 MDCCs have been launched: post-operative surgical breast, advanced breast that needs re-evaluation, metastatic breast, lung (to be diagnosed), thymus tumors, colon rectal tumors, eyelid orbit melanoma, metastatic uveal melanoma. Most MDCCs take place once a week (53.8%). Also in this case, the documentation required for the visit is mainly related to imaging (42%). Clinical reports from all MDCCs are entered in the electronic medical record. 38.4% of the MDCCs are included in a formalized/institutional care pathway and PROMS are not regularly used (only 23.1%).
Respondents report that MDCCs are aimed at planning a more personalized diagnostic-therapeutic pathway (61.5%) and to integrate the skills of the different specialists (53.8%); also, coordinate access and timing is reported (30.8%). The MDCCs referral criteria are mainly specific diagnostic clinical criteria.
MDCCs Network
Figure 1b shows the graphic structure of the MDCCs network. SNA shows a network with 23 nodes and 41 ties, with a density of 0.31 (SD = 0.46), which indicates a low level of network cohesion, as only 31% of all possible links are present. Pathologists and the radiologists are excluded from the network, not being connected to any node. Moreover, in MDCCs, psychologists, palliative care specialists and nurses (case managers and clinical nurses) have few ties.
Discussion
The present study confirms the variability of MDTW models applied in clinical practice in a Comprehensive Cancer Center. In agreement with the findings of Wright et al,16 differences emerged with respect to: objectives, disease phase, referral criteria, group composition, meeting format, documentation suggested for the visit, reporting documentation, etc. This variability seems to be functional to two aspects: the kind of pathology and the resources available for that pathology.
Most frequently, coordinators and core team members were medical oncologists and surgeons; this agrees with the structure of a Comprehensive Cancer Center organized in departments, the main ones being surgical and medical oncology ones.11 Accordingly radiotherapists were also very commonly included as core members while only rarely radiologists could attend although considered important. Unlike what suggested by Page et al,19 in our survey, the number of team members is greater for MDTMs than for MDCCs.
SNA highlighted similar density values for the two MDTWs. This means that in both cases the professionals who participated in MDTWs were less than a third of those who could participate. However, it should be emphasized that these analyses do not determine whether it makes sense for a specific professional to participate or not in a MDTW. Pathologists and radiologists were completely isolated nodes in the MDCCs network, in fact they did not participate in any MDTWs. The number of radiologists in our Comprehensive Cancer Center is not sufficient to cope with all the requests that come in. This causes radiologists to perform services only when strictly necessary and MDCCs are probably not considered as so. Yet, oncological radiology is one of the “four pillars” of the Optimal multidisciplinary care along with radiation oncology, medical oncology and surgical oncology.11 On the other hand, we do not have certain information regarding the figure of the anatomic-pathologist; however, we can suppose that, in some MDCCs, his or her figure is either not considered fundamental or, again, his or her absence is due to scarcity of resources.
Both MDCC and MDTM teams were predominantly made up of physicians as the number of non-medical professionals was very low. In this sense, it is correct to speak of “multidisciplinarity”, but not of “multi-professionalism”. In particular, clinical, researchers, and case managers nurses were missing, while oncology nurses should have a leading role in the patient’s care process.27 Nurse-led interventions improve specific cancer-related symptoms, service coordination and patient satisfaction,28,29 therefore, its presence can be especially important within the MDCCs. Nurse case managers are considered particularly important in the literature both for the optimization of existing resources and for improving patient satisfaction.30,31 Furthermore, it should be emphasized that in our Comprehensive Cancer Center there is no involvement of an ‘expert’ patient in MDTWs. ‘Expert’ patients should be present as members of MDTWs. Patient involvement may increase the quality of clinical practice as their experiential knowledge can complement scientific evidence. Patient involvement is also a characteristic of a system that pays attention to patient-centeredness.32
Furthermore, despite the high number of MDCCs and MDTMs for advanced/metastatic cancer phases, the involvement of palliative care specialists and psychologists was limited. There is evidence that transition to the advanced phases is smoother and the perception of being “abandoned” prevented when palliative care specialists are met early in the disease trajectory.33 As already emerged in the literature, “needs for supportive care must be managed through multidisciplinary engagement outside the meeting arena” (p. 205).34
In agreement with previous literature,13,15 the identification of the optimal care pathway, tailored to the specific patient and disease characteristics, was the most frequently reported goal for both MDTMs and MDCCs, followed by the aim of integrating the skills of the different specialists. However, MDCCs were often answering to practical issues (ie, to coordinate patient access and visit scheduling), while MDTMs were more often required to manage patients complex clinical conditions. The possibility of discussing complex cases with colleagues is an important aspect also emerged in the literature (ie,)14; in fact, MDCCs and MDTMs represent collaborative working methods that can reassure team members when facing difficult treatment choices, allowing to share responsibilities with colleagues.
In agreement with other experiences reported in the literature,6 MDCCs and MDTMs are well established practices in our cancer center, as they have been present for an average of 8 and 10 years, respectively. The number of MDTWs is increasing: in the last 5 years, 6 MDTMs and 8 MDCCs have been developed. One one hand, this could testify both the usefulness of these devices and the feasibility of implementation; however, it should be underlined that the presence of MDTWs is a requisite for quality certifications (eg, OECI).5
According to Atwal and Caldwall,35 the inclusion of MDCCs and MDTMs in care pathways is a valuable tool for enhancing interprofessional and interorganizational relationships. Our results show that MDTMs were rarely included in formalized/institutional care pathways and the reporting was not fully recorded on institutional platforms, while, on the other hand, MDCCs inclusion in formalized/institutional care pathways and reporting on institutional platforms was more common. It would therefore seem that the MDTMs have a more “informal” character than the MDCCs. Prades and Borras9 also found a lack of formalization of MDTMs in Spanish cancer hospitals; half of the interviewees in their study declared that they did not record their decisions on electronic clinical records. However, the authors stress the importance of a formal process, as formality enables more transparent and accessible decision process which is valuable for the institution. Furthermore, they specify the importance of recording the outcomes of the MDTWs especially when there is no consensus about the decisions taken as this can play an important role from a legal perspective too.
Although, use of PROMs in the clinic can improve symptom control, patient well-being and the performance of healthcare systems.34,36 They are rarely applied in MDTWs reflecting what happens in routine clinical oncology practice.37,38 This could represent another indicator of low patient-centeredness.32,34
Finally, a high percentage of professionals supported the importance of training in MDTWs and they stressed the importance of improving communication skills and leadership. The existing literature focuses on the importance of addressing research and treatment coordination in MDTWs trainings for specialists. However, communication and leadership abilities are essential elements of any work team. Team leadership is important as it influences the group spirit and the ability for participants to feel free to express their opinions. This could prevent the floor from being taken exclusively by clinicians involved in tumour staging decisions and treatments,11 diminishing then the effectiveness of MDTWs.34,39
The study presents some limitations. The first is that the data presented are not “objective” but reported by the participants. This may have affected the accuracy of some information. However, this survey is one of the few studies that systematically describes all the MDTW models present in one institution. Second limitation is constituted by the way in which the MDCCs and MDTMs are identified: despite all the clinical unit directors were asked to indicate all the MDTMs and MDCCs their unit personnel were involved in, it is possible that some were missed.
Future studies could compare MDTMs and MDCCs in terms of feasibility and efficacy (taking into account both patients’ and the professionals’ points of view). In particular, it would be interesting to compare the efficacy of MDTWs for advanced/metastatic phases of the disease, with and without the presence of different professionals such as palliative care specialists, psychologists and nurses in order to study the impact of different MDTW models.
Conclusion
The widespread adoption of MDTWs in cancer care has occurred despite a lack of homogeneity of existing models. Results of this research confirm a great variability of the existing models. However, common elements are represented by the lack of some key professions (palliative care specialists, psychologists and nurses) and an organizational culture that is not yet patient-centered as well as often not specifically trained in multidisciplinary teamwork.
Data Sharing Statement
Results data are available upon request to the corresponding author.
Ethical Approval
This observational study was approved by the institutional Ethics Committee of Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy (registration number: INT 269-20). All followed procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975.
Acknowledgments
We thank Michela Monfredini for the English revision.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analyses and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by “5 per 1000” Funds 2017 - Financial support for healthcare research and “Ricerca Corrente” funds (Italian Ministry of Health).
Disclosure
Dr Cinzia Brunelli reports grants from Italian Ministry of Health, during the conduct of the study; Dr Giulia V Bianchi reports personal fees from Roche, personal fees from Daichi/astraZeneza, personal fees from Seagen, personal fees from Novartis, personal fees from Lilly, outside the submitted work; Professor Augusto Caraceni reports grants from Italian Ministry of Health, during the conduct of the study; personal fees from Mundipharma, personal fees from Molteni, personal fees from Eli Lilly, personal fees from Kiowa Kirin, outside the submitted work. The authors report no other conflicts of interest.
References
1. Dictionary of Cancer Terms. Definition: multidisciplinary. US: National Cancer Institute. Available from: https://www.cancer.gov/search/results?swKeyword=multidisciplinary.
2. Gupta T. Multidisciplinary clinics in oncology: the hidden pitfalls. J Oncol Pract. 2007;3(2):72–73. doi:10.1200/JOP.0722505
3. Borras JM, Albreht T, Audisio R, et al. Policy statement on multidisciplinary cancer care. Eur J Cancer. 2014;50(3):475–480. doi:10.1016/j.ejca.2013.11.012
4. Department of Health. Multidisciplinary cancer care. Literature review. Melbourne: State of Victoria; 2012. Available from: www.health.vic.gov.au/cancer.
5. Boomsma F, van Harten W, Oberst S, et al. Accreditation and designation user manual version 2.0. Brussels-Genoa: Eurocan Platform. Available from: https://www.oeci.eu/Attachments/OECI_ACC_Manual_2_0.pdf.
6. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: a systematic review of the literature. Cancer Treat Rev. 2016;42:56–72. doi:10.1016/j.ctrv.2015.11.007
7. Brar SS, Hong NL, Wright FC. Multidisciplinary cancer care: does it improve outcomes? J Surg Oncol. 2014;110(5):494–499. doi:10.1002/jso.23700
8. Croke J, El-Sayed S. Multidisciplinary management of cancer patients: chasing a shadow or real value? An overview of the literature. Curr Oncol. 2012;19(4):232–238. doi:10.3747/co.19.944
9. Prades J, Borràs JM. Multidisciplinary cancer care in Spain, or when the function creates the organ: qualitative interview study. BMC Public Health. 2011;11(1):1–10. doi:10.1186/1471-2458-11-141
10. Bunnell CA, Weingart SN, Swanson S, Mamon HJ, Shulman LN. Models of multidisciplinary cancer care: physician and patient perceptions in a comprehensive cancer center. J Oncol Pract. 2010;6(6):283–288. doi:10.1200/JOP.2010.000138
11. Taberna M, Gil Moncayo F, Jané-Salas E, et al. The multidisciplinary team (MDT) approach and quality of care. Front Oncol. 2020;10:85. doi:10.3389/fonc.2020.00085
12. Wulff CN, Thygesen M, Søndergaard J, Vedsted P. Case management used to optimize cancer care pathways: a systematic review. BMC Health Serv Res. 2008;8(1):1–7. doi:10.1186/1472-6963-8-227
13. Ansmann L, Kowalski C, Pfaff H, Wuerstlein R, Wirtz MA, Ernstmann N. Patient participation in multidisciplinary tumor conferences. Breast. 2014;23(6):865–869. doi:10.1016/j.breast.2014.09.004
14. Butow P, Harrison JD, Choy ET, Young JM, Spillane A, Evans A. Health professional and consumer views on involving breast cancer patients in the multidisciplinary discussion of their disease and treatment plan. Cancer. 2007;110(9):1937–1944. doi:10.1002/cncr.23007
15. Jazieh AR. Tumor boards: beyond the patient care conference. J Cancer Educ. 2011;26(3):405–408. doi:10.1007/s13187-011-0209-z
16. Wright F, De Vito C, Langer B, Hunter A. Multidisciplinary cancer conferences: a systematic review and development of practice standards. Eur J Cancer. 2007;43(6):1002–1010. doi:10.1016/j.ejca.2007.01.025
17. Gatcliffe TA, Coleman RL. Tumor board: more than treatment planning—a 1-year prospective survey. J Cancer Educ. 2008;23(4):235–237. doi:10.1080/08858190802189014
18. Hammer RD, Prime MS. A clinician’s perspective on co-developing and co-implementing a digital tumor board solution. Health Informatics J. 2020;26(3):2213–2221. doi:10.1177/1460458219899841
19. Page AJ, Cosgrove D, Elnahal SM, Herman JM, Pawlik TM. Organizing a multidisciplinary clinic. Chin Clin Oncol. 2014;3(4):3865.
20. Fleissig A, Jenkins V, Catt S, Fallowfield L. Multidisciplinary teams in cancer care: are they effective in the UK? Lancet Oncol. 2006;7(11):935–943. doi:10.1016/S1470-2045(06)70940-8
21. Baumeister RF, Leary MR. The need to belong: desire for interpersonal attachments as a fundamental human motivation. Interpe Develop. 2017;2017:57–89.
22. Wasserman S, Faust K. Social Network Analysis: Methods and Applications. Cambridge Cambridge University Press; 1994.
23. Herrera RF, Mourgues C, Alarcón LF, Pellicer E. Understanding interactions between design team members of construction projects using social network analysis. J Constr Eng Manage. 2020;146(6):04020053. doi:10.1061/(ASCE)CO.1943-7862.0001841
24. Lockhart NC. Social network analysis as an analytic tool for task group research: a case study of an interdisciplinary community of practice. J Special Group Work. 2017;42(2):152–175. doi:10.1080/01933922.2017.1301610
25. Marqués-Sánchez P, Muñoz-Doyague MF, Martínez YV, et al. The importance of external contacts in job performance: a study in healthcare organizations using social network analysis. Int J Environ Res Public Health. 2018;15(7):1345. doi:10.3390/ijerph15071345
26. Cancer for Europe. Seven leading cancer centers improve cancer health in Europe. Available from: https://cancercoreeurope.eu/.
27. Associazione Italiana per la Ricerca sul Cancro (AIRC). Non più solo assistenza ma anche comunicazione e ricerca [Not only assistance but also communication and research]. Milan: Fondazione AIRC per la Ricerca sul Cancro; 2018. Italian. Available from: https://www.airc.it/news/non-piu-solo-assistenza-ma-anche-comunicazione-e-ricerca.
28. Kelly D, Campbell P, Torrens C, et al. The effectiveness of nurse-led interventions for cancer symptom management 2000–2018: a systematic review and meta-analysis. Health Sci Rev. 2022;2022:100052.
29. Kerr H, Donovan M, McSorley O. Evaluation of the role of the clinical nurse specialist in cancer care: an integrative literature review. Eur J Cancer Care. 2021;30(3):e13415. doi:10.1111/ecc.13415
30. Johansson P, Oleni M, Fridlund B. Patient satisfaction with nursing care in the context of health care: a literature study. Scand J Caring Sci. 2002;16(4):337–344. doi:10.1046/j.1471-6712.2002.00094.x
31. Koç Z, Saglam Z, Senol M. Patient satisfaction with the nursing care in hospital/hastanede hemsirelik bakimi ile ilgili hasta memnuniyeti. Türkiye Klinikleri Tip Bilimleri Dergisi. 2011;31(3):629.
32. Mihaljevic AL, Doerr-Harim C, Kalkum E, Strunk G. Measuring patient centeredness with German language PATIENT-REPORTED EXPERIENCE MEasures (PREM) - A systematic review and qualitative analysis according to COSMIN. PLoS One. 2022;17(11):e0264045. doi:10.1371/journal.pone.0264045
33. Greer JA, Jackson VA, Meier DE, Temel JS. Early integration of palliative care services with standard oncology care for patients with advanced cancer. CA Cancer J Clin. 2013;63(5):349–363. doi:10.3322/caac.21192
34. Lamprell K, Arnolda G, Delaney GP, Liauw W, Braithwaite J. The challenge of putting principles into practice: resource tensions and real‐world constraints in multidisciplinary oncology team meetings. Asia Pac J Clin Oncol. 2019;15(4):199–207. doi:10.1111/ajco.13166
35. Atwal A, Caldwell K. Do multidisciplinary integrated care pathways improve interprofessional collaboration? Scand J Caring Sci. 2002;16(4):360–367. doi:10.1046/j.1471-6712.2002.00101.x
36. Kotronoulas G, Kearney N, Maguire R, et al. What is the value of the routine use of patient-reported outcome measures toward improvement of patient outcomes, processes of care, and health service outcomes in cancer care? A systematic review of controlled trials. J Clin Oncol. 2014;32(14):1480–1510. doi:10.1200/JCO.2013.53.5948
37. Brunelli C, Zito E, Alfieri S, et al. Knowledge, use and attitudes of healthcare professionals towards patient-reported outcome measures (PROMs) at a comprehensive cancer center. BMC Cancer. 2022;22(1):1–10. doi:10.1186/s12885-022-09269-x
38. Giolla Easpaig B N, Tran Y, Bierbaum M, et al. What are the attitudes of health professionals regarding patient reported outcome measures (PROMs) in oncology practice? A mixed-method synthesis of the qualitative evidence. BMC Health Serv Res. 2020;20(1):1–24.
39. Lamb BW, Brown KF, Nagpal K, Vincent C, Green JS, Sevdalis N. Quality of care management decisions by multidisciplinary cancer teams: a systematic review. Ann Surg Oncol. 2011;18:2116–2125. doi:10.1245/s10434-011-1675-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.