Back to Journals » Infection and Drug Resistance » Volume 19
Characterization of Clostridium perfringens Causing Liver Abscess Using Whole-Genome Sequencing: A Case Report and Literature Review
Authors Li M, Min Y, Ye K, Ye L, Guo L, Wang L
Received 26 October 2025
Accepted for publication 10 February 2026
Published 25 February 2026 Volume 2026:19 573692
DOI https://doi.org/10.2147/IDR.S573692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hemant Joshi
Muqi Li,1,* Yan Min,2,* Kun Ye,1 Liyan Ye,1 Ling Guo,1 Lifeng Wang1
1Department of Laboratory Medicine, the First Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Department of Laboratory Medicine, 960th Hospital of People’s Liberation Army, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lifeng Wang, Department of Laboratory Medicine, the First Medical Center of Chinese PLA General Hospital, Beijing, 100853, People’s Republic of China, Email [email protected]
Abstract: A patient who had previously undergone varicose vein surgery developed persistent postoperative fever. The results of ultrasonography and computed tomography (CT) indicated the possible presence of a liver abscess. Subsequent blood and drainage fluid cultures yielded Gram-positive bacilli exhibiting characteristic hemolytic rings. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) identified both isolates as Clostridium perfringens (C. perfringens), implicating this pathogen as the etiological agent of the liver abscess. The patient was treated empirically with cefuroxime, ornidazole, and cefoperazone–sulbactam, after which the fever gradually resolved and the patient was discharged in stable condition. To further characterize the microbiological features of the isolates, whole-genome sequencing (WGS) was performed. Comparative genomic analysis demonstrated that the similarity between the two strains was higher than 99.99%, indicating a clonal origin. Further genotypic characterization revealed the presence of the major toxin gene plc, along with several accessory toxin genes, including pfoA, colA, and cloSI. In addition, genes encoding neuraminidases and hyaluronidases were identified, suggesting enhanced tissue invasiveness. The strains also harbored multiple antimicrobial resistance–associated genes, including mprF, tetB(P), and cplR. To contextualize these findings, a literature review was conducted to summarize the clinical and etiological characteristics of liver abscesses caused by C. perfringens. Analysis of reported cases indicated that advanced age, male sex, underlying hepatobiliary disease, and diabetes mellitus were common predisposing factors. Among these cases, only six cases were tested for C. perfringens toxin genes: five cases were associated with the plc gene alone, while one case involved concurrent detection of both plc and pfoA. Overall, this study provided important molecular and clinical evidence to support improved diagnosis, risk assessment, and therapeutic management of liver abscesses caused by C. perfringens.
Keywords: Clostridium perfringens, liver abscess, whole-genome sequencing, virulence factors, case report
Introduction
C. perfringens is a Gram-positive obligate anaerobic bacterium that is pathogenic to both humans and animals.1 Based on the production of six major toxins, alpha toxin (CPA), beta toxin (CPB), epsilon toxin (ETX), iota toxin (ITX), NetB, and enterotoxin (CPE), C. perfringens is classified into seven toxinotypes (A–G).2 Each toxinotype is associated with distinct enterotoxin- and histotoxin-mediated disease profiles. In both humans and livestock, C. perfringens is responsible for a broad range of systemic and intestinal diseases, including gas gangrene, food poisoning, non-foodborne diarrhea, enterocolitis, and enterogenic toxemia. The clinical manifestations of these conditions largely depend on the specific toxin combinations produced by the infecting strain.3
Liver abscess is a common infectious disease of the liver encountered in clinical practice. In 2012, the reported incidence rate in China was 8.9 per 100,000 population.4,5 Notably, males exhibit a higher incidence than females, and a global upward trend in the annual incidence of liver abscesses has been observed. A variety of underlying conditions, including biliary tract disorders, liver diseases, and diabetes mellitus, have been identified as important predisposing factors.6 Liver abscesses typically arise when pathogens invade hepatic tissue through multiple routes, such as the biliary tract, hepatic artery, portal vein, or by direct spread, ultimately resulting in localized suppurative lesions.7 The causative pathogen spectrum is diverse and includes Gram-negative bacteria, Gram-positive bacteria, and anaerobes. However, C. perfringens is an infrequent cause of liver abscesses. According to PubMed search results up to June 30, 2025, only 71 cases of liver abscess caused by C. perfringens have been reported,8 which is substantially fewer than those attributed to common pathogens such as Klebsiella pneumoniae (K. pneumoniae) and Escherichia coli (E. coli). Host-related risk factors associated with C. perfringens liver abscess include advanced age, male sex, underlying liver and gallbladder diseases, and diabetes mellitus. On a global scale, the reported incidence of C. perfringens liver abscess varies geographically, with a higher number of cases documented in East Asia, possibly reflecting regional differences in dietary habits and the prevalence of hepatobiliary disorders. The pathogenesis of C. perfringens–associated liver abscess is predominantly mediated by toxin-induced tissue injury. For example, alpha toxin disrupts host cell membranes, while perfringolysin O facilitates tissue invasion. Liver abscess caused by C. perfringens may be complicated by intravascular hemolysis, with reported mortality rates reaching 25–50%.9 Therefore, timely etiological diagnosis and comprehensive treatment are critical for improving patient prognosis.
In the present study, we reported a case of liver abscess caused by C. perfringens following variceal surgery, which was complicated by bloodstream infection. Given the limited molecular characterization available in most previously reported C. perfringens–associated liver abscesses, this study aimed to investigate the genetic features of the causative pathogen using WGS and to summarize the associated clinical characteristics through a literature review, thereby providing a basis for diagnosis and treatment. Our findings demonstrated that the C. perfringens strain responsible for liver abscess harbored the toxin-typing gene plc, accessory toxin genes pfoA, colA, and cloSI, as well as neuraminidase genes (nanH, nanI, and nanJ) and hyaluronidase genes (nagH, nagI, nagJ, nagK, and nagL). In addition, the strain carried several antimicrobial resistance–associated genes, including mprF, tetB(P), and cplR. By reviewing previously reported cases of liver abscess caused by C. perfringens, we further summarized the molecular etiological characteristics of strains implicated in this condition. Collectively, this study provided a laboratory-based foundation for the diagnosis and treatment of liver abscesses caused by C. perfringens.
Case Report
A 55-year-old male patient had a more than 20-year history of varicose veins, characterized by persistent soreness, limb distension, weakness, and discomfort, which were aggravated by prolonged standing and walking. To seek definitive treatment, he underwent varicose vein surgery of the right lower extremity on March 27, 2024. Following the procedure, the patient developed postoperative fever accompanied by markedly elevated inflammatory markers. Although the surgical incision healed well, the fever persisted and recurred. Laboratory examinations performed on March 28, 2024, revealed a white blood cell (WBC) count of 22.77 × 109/L, a neutrophil proportion of 90.3%, alanine aminotransferase (ALT) of 44.2 U/L, γ-glutamyl transpeptidase (γ-GT) of 241.2 U/L, and a total bilirubin level of 60.6 mg/dL (Table 1).
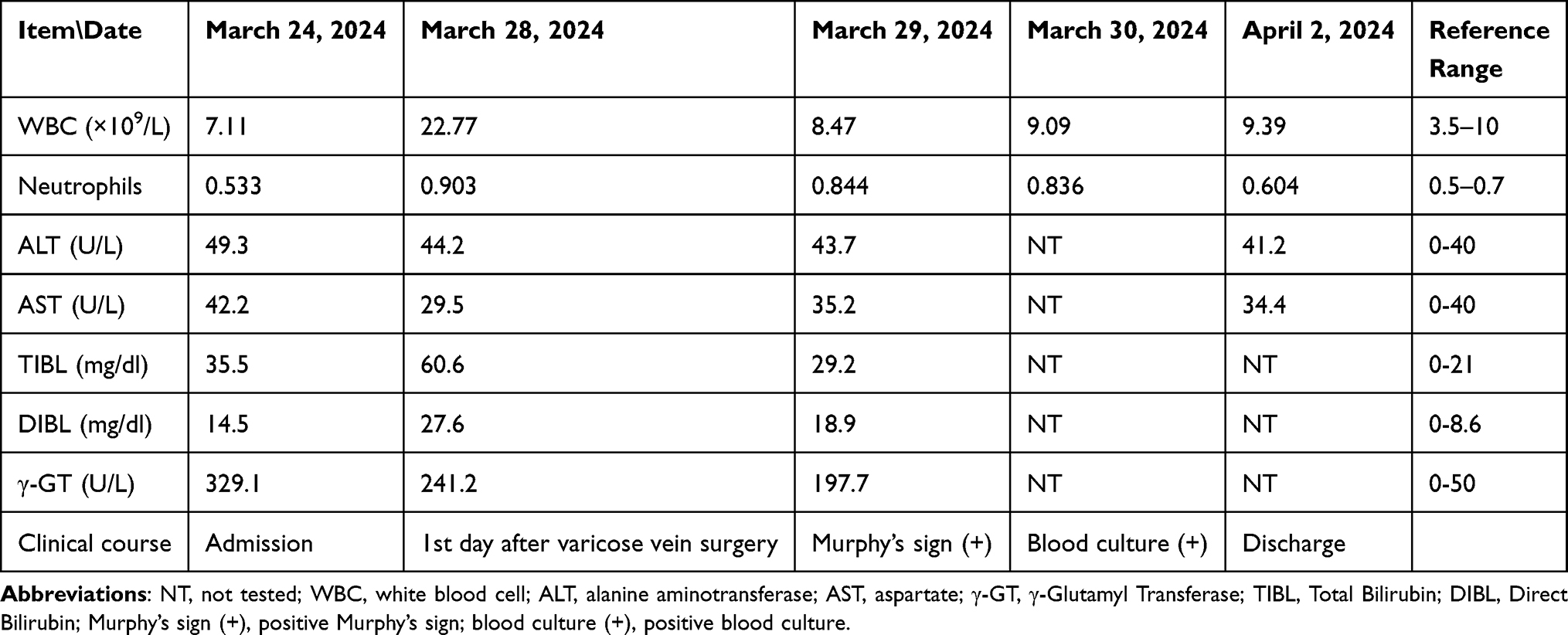 |
Table 1 Changes in the Patient’s Laboratory Tests After Admission |
On March 29, 2024, repeat laboratory testing showed a WBC count of 8.47 × 109/L, neutrophils accounting for 84.4%, ALT of 43.7 U/L, γ-GT of 197.7 U/L, and total bilirubin of 29.2 mg/dL (Table 1). Physical examination demonstrated a positive Murphy’s sign. Subsequently, abdominal ultrasonography and CT were performed. Based on the combined findings of B-mode ultrasonography and CT imaging, a liver abscess was strongly suspected (Figure 1A and B). On the same day, peripheral blood samples were collected for both aerobic and anaerobic cultures. Approximately 18 hours later, the anaerobic blood culture yielded positive growth, whereas the aerobic culture remained negative. The positive blood culture underwent overnight subculture on an anaerobic blood agar plate. This subculture revealed gram-positive bacteria and colonies encircled by distinct hemolytic rings (Figure 1C and D). The causative pathogen of the bloodstream infection was identified as C. perfringens using MALDI-TOF-MS.
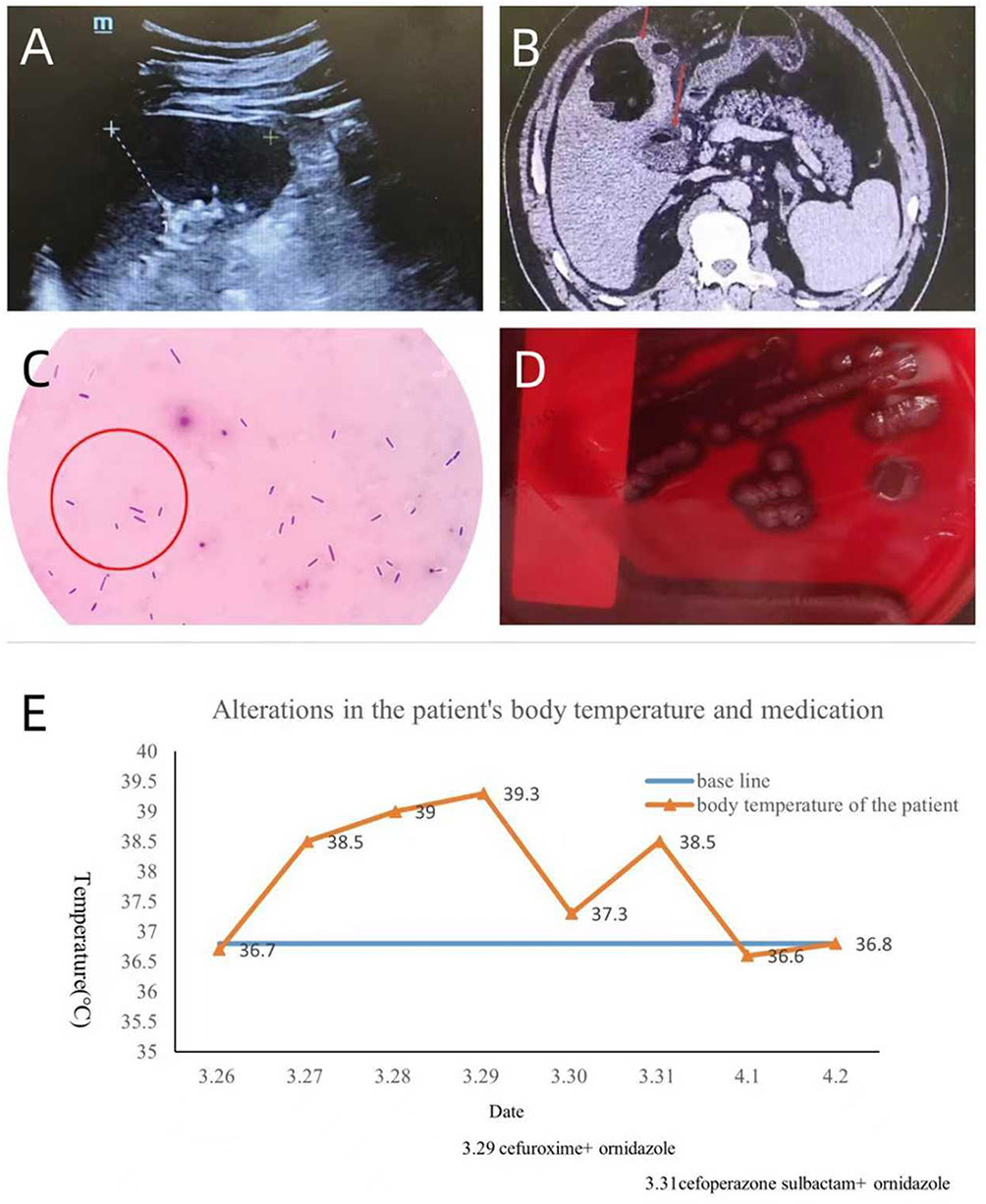 |
Figure 1 (A and B) Abdominal B-ultrasound and CT imaging examination: (A) shows a space-occupying lesion, consistent with liver abscess, “+” and dashed line: measurement scale; (B) indicates the presence of gas within the cavity, red arrows: gas accumulation in the cavity. (C and D) Smear and culture of positive bottles for the patient’s blood culture: (C) shows gram-positive bacilli, red circle: bacilli that are Gram-positive and have capsules; (D) shows colonies with hemolytic rings on blood plates. (E) The change in body temperature: The patient’s body temperature peaked at 39.3°C on March 29th, normalized on March 30th after initial antimicrobial therapy, increased again on March 31st, and normalized on April 1st after antibiotic adjustment, “+”: the combined use of two antibiotics. |
On March 31, 2024, ultrasound-guided percutaneous drainage of the liver abscess was performed, and the drainage fluid was submitted for microbiological analysis. The culture of the drainage fluid demonstrated hemolytic activity and Gram-positive bacilli. Both the microscopic appearance and colony morphology were consistent with those observed in the blood culture isolates. Further identification confirmed C. perfringens in the drainage fluid, with no other aerobic bacteria detected. Taken together, these findings indicated that the patient most likely developed a C. perfringens–induced liver abscess, which subsequently progressed to secondary bloodstream infection.
The patient developed a fever on March 28, with a peak body temperature of 39.3 °C recorded on March 29. Following imaging-based confirmation of a liver abscess, antimicrobial therapy with cefuroxime and ornidazole was initiated on March 29, resulting in normalization of body temperature by March 30. However, on March 31, the patient experienced a recurrence of fever, which was considered likely attributable to incomplete eradication of C. perfringens. To achieve more effective infection control, the antimicrobial regimen was escalated to cefoperazone–sulbactam combined with ornidazole. Given its broader antibacterial spectrum against anaerobic organisms,10 cefoperazone–sulbactam is more appropriate for the management of severe anaerobic infections. After adjustment of the treatment strategy and supportive care, the patient’s fever subsided, and inflammatory marker levels gradually decreased. On postoperative day 6, the patient was discharged in stable condition with a liver drainage tube in situ and scheduled for outpatient follow-up.
The C. perfringens isolates obtained from blood cultures and liver abscess drainage fluid were subjected to WGS to assess their genetic relatedness. The sequencing data were deposited in the NCBI database under accession number PRJNA1346668. The assembled genome of C. perfringens was 3,292,478 bp in length, with a GC content of 28.06%. Comparative genomic analysis demonstrated that the two isolates shared >99.99% sequence identity, indicating a clonal origin. The number of single-nucleotide polymorphisms (SNPs) between the two genomes was 32. These results suggested that the two isolates were clonally related and derived from the same source. Further molecular characterization revealed that both strains harbored the toxin-typing gene plc, accessory toxin genes pfoA, colA, and cloSI, as well as neuraminidase genes (nanH, nanI, and nanJ) and hyaluronidase genes (nagH, nagI, nagJ, nagK, and nagL). In addition, this C. perfringens strain carried multiple antimicrobial resistance–associated genes, including mprF, tetB(P), and cplR (Supplementary Table 1A and B).
A retrospective analysis of 71 reported cases of C. perfringens–associated liver abscess was conducted to elucidate their clinical and etiological characteristics. The patient cohort comprised 81.7% males and 13.3% females, with a mean age of 68.8 years. The most common underlying conditions were diabetes mellitus (35.2%), liver cancer (15.3%), and a history of hepatobiliary surgery (22.5%). The overall mortality rate among these cases was 68.6%. Among the 71 cases, only six cases were tested for C. perfringens toxin genes: five cases were associated with plc alone, while one case involved both plc and pfoA. Serotyping information was available for a limited number of cases, with four isolates identified as serotype A and the remainder lacking detailed serotype data (Table 2). In addition, we reviewed reported cases of C. perfringens liver abscess in China and identified 10 case reports involving 11 patients. Most patients were male, seven had diabetes mellitus, and three had liver cancer. Notably, none of these reports provided molecular-level characterization of the causative strains (Table 2).
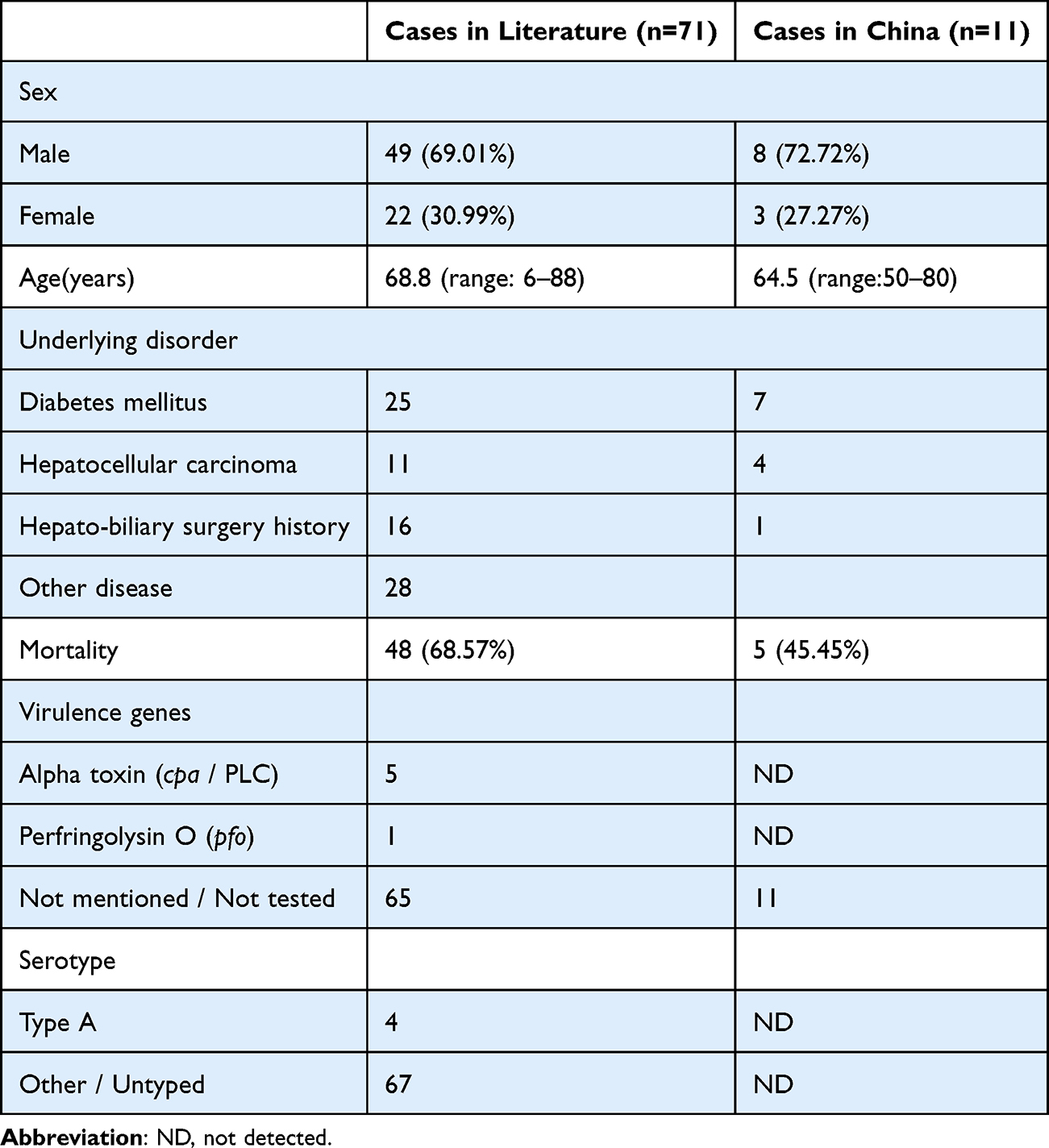 |
Table 2 Summary of the Clinical and Microbiological Characteristics of C. Perfringens Liver Abscesses in the World and China |
Discussion
Liver abscess is a common hepatobiliary disease encountered in clinical practice, for which timely etiological diagnosis and comprehensive treatment are essential to achieving a favorable prognosis.11K. pneumoniae, E. coli, and anaerobic bacteria are the most frequently implicated pathogens, while C. perfringens remains a rare etiological agent of liver abscess.12 In this study, we reported a case of C. perfringens–associated liver abscess occurring in an immunocompetent patient following varicose vein surgery and complicated by bloodstream infection. After precise pathogen identification and appropriate antimicrobial management, the patient recovered and was successfully discharged. To further elucidate the etiological characteristics of C. perfringens, WGS was performed on two isolates obtained from blood and liver abscess drainage fluid to characterize their genetic features. In parallel, we reviewed 71 previously reported cases of C. perfringens–related liver abscesses to enhance the understanding of their clinical and etiological profiles.
Accurate pathogen identification is pivotal in the diagnosis of suppurative liver abscess, as it directly informs the selection of targeted antimicrobial therapy, particularly in cases complicated by bacteremia.13 As an obligate anaerobe, C. perfringens poses technical challenges for routine clinical cultivation and may therefore be underrecognized as a causative pathogen in liver abscesses.14 In the present case, C. perfringens was rapidly detected in both blood and abscess drainage fluid, enabling the timely initiation of effective antibiotic therapy and contributing to a favorable clinical outcome. This case highlighted the importance of considering C. perfringens in the differential diagnosis of liver abscesses and underscored the necessity of incorporating its detection into routine microbiological diagnostic workflows.
The patient, who was immunocompetent and had undergone varicose vein surgery, subsequently developed a postoperative liver abscess. The consistent isolation of C. perfringens from both blood and liver abscess drainage prompted further consideration of the infection source and dissemination route. Laboratory findings obtained on admission on March 24 demonstrated abnormal liver function indices and elevated bilirubin levels, and the postoperative leg wound healed well. These observations suggested that C. perfringens might have initially caused a liver abscess, followed by hematogenous dissemination into the bloodstream, resulting in secondary bacteremia.
WGS demonstrated that the C. perfringens isolates obtained from blood and liver abscess drainage fluid were genetically homologous. The detection of the toxin-typing gene plc classified the strain as toxin type A. In addition, the isolates harbored the pfoA toxin gene, as well as multiple neuraminidase- and hyaluronidase-associated genes. Strains positive for pfoA are known to exhibit potent cytotoxicity and are commonly associated with severe infections such as neonatal necrotizing enterocolitis and gas gangrene. Neuraminidases constitute a group of enzymes that cleave sialic acid residues from the terminal positions of glycoproteins, glycolipids, and oligosaccharides.15 Multiple neuraminidase-related genes, including nanH, nanI, and nanJ, have been identified in C. perfringens.16 Among these, nanI plays a critical role in promoting intestinal colonization, enhancing cytotoxicity, and facilitating the interaction between major C. perfringens toxins and host cells.17
Hyaluronidases are key enzymes involved in the regulation of physiological and pathological processes through the degradation of hyaluronic acid within the extracellular matrix.18–20The presence of five hyaluronidase genes (nagH, nagI, nagJ, nagK, and nagL) in the present C. perfringens strain suggested a broad tissue-invasive capacity and a high pathogenic potential.21 Through synergistic degradation of host tissue matrices and amplification of major toxin activities, these virulence determinants might facilitate the development of severe infections. Accordingly, identification of such genetic features indicated that clinicians should consider intensified anti-infective strategies in combination with appropriate symptomatic and supportive care.
Despite the high virulence potential suggested by its genetic profile, the patient in this case presented only with fever and a positive Murphy’s sign, without progression to intravascular hemolysis, rapidly enlarging hepatic abscess, or systemic sepsis. The patient was successfully discharged with a drainage tube in place on postoperative day 6. This favorable outcome was likely attributable to timely empirical antibiotic therapy, rapid etiological identification, rational escalation of antimicrobial treatment, effective percutaneous drainage of the liver abscess, and the patient’s preserved immune function. Although the strain carried antimicrobial resistance–associated genes, including mprF, tetB(P), and cplR, phenotypic resistance was supposed mainly to be against agents such as defensin, tetracycline, and lincomycin.22,23 In contrast, the isolate remained susceptible to commonly used clinical agents, including ornidazole, cefazolin, and cefoperazone–sulbactam.
We further reviewed 71 previously reported cases of liver abscesses attributed to C. perfringens and systematically analyzed their clinical and pathogenic characteristics. The results indicated that C. perfringens–associated liver abscesses predominantly occurred in elderly male patients and were frequently accompanied by underlying conditions such as diabetes mellitus and hepatobiliary diseases, findings that were consistent with earlier case-based reviews. Nevertheless, only a small number of studies have investigated the molecular features of C. perfringens strains responsible for liver abscess formation. Among the 71 cases reviewed, virulence gene profiling was performed in only six cases: five isolates carried the plc gene, while one harbored both plc and pfoA, which appeared to be associated with disease severity and prognosis. Notably, the majority of the reviewed cases were complicated by intravascular hemolysis and were associated with a high mortality rate, underscoring the aggressive clinical course typically associated with C. perfringens liver abscess.
This study represented a documented application of WGS to a clinical C. perfringens isolate obtained from a liver abscess. Genomic analysis demonstrated that the isolate belonged to toxin type A and harbored multiple accessory toxin genes, neuraminidases, and hyaluronidases, in addition to several antimicrobial resistance–associated genes. Despite its genetic classification as a highly virulent strain, the patient achieved a favorable clinical outcome. This apparent discrepancy between the predicted pathogenic potential of the strain and the benign clinical course observed in the patient warrants further investigation. The successful therapeutic approach applied in this case, characterized by early empirical therapy, rapid etiological identification, rational antibiotic escalation, and effective abscess drainage, might provide valuable insights for the management of similar infections and merits broader consideration and dissemination. A limitation of the present study is the absence of functional assays to directly validate the biological activity of the identified virulence and resistance genes. Future investigations incorporating in vitro functional experiments are needed.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of The First Medical Center of Chinese People’s Liberation Army General Hospital (Approval No. S2024-777-01 and S2026-092-01). The approval explicitly covers the publication of the case details, including clinical data, imaging results, and microbiological findings. Informed consent was obtained from the patient for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This case report was not supported by any research project.
Disclosure
The authors report no potential conflicts of interest in this work.
References
1. Ba X, Jin Y, Ning X, et al. Clostridium perfringens in the intestine: innocent bystander or serious threat? Microorganisms. 2024;12(8):1610. doi:10.3390/microorganisms12081610
2. Camargo A, Ramírez JD, Kiu R, Hall LJ, Muñoz M. Unveiling the pathogenic mechanisms of Clostridium perfringens toxins and virulence factors. Emerg Microbes Infect. 2024;13(1):2341968. doi:10.1080/22221751.2024.2341968
3. Talukdar PK, Banawas S, Sarker MR. Clostridium perfringens. Trends Microbiol. 2025;33(1):130–8. doi:10.1016/j.tim.2024.09.009
4. Tian L-T, Yao K, Zhang X-Y, et al. Liver abscesses in adult patients with and without diabetes mellitus: an analysis of the clinical characteristics, features of the causative pathogens, outcomes and predictors of fatality: a report based on a large population, retrospective study in China. Clin Microbiol Infect. 2012;18(9):E314–30. doi:10.1111/j.1469-0691.2012.03912.x
5. Long Q, Zhao X, Chen C, Hao M, Qin X. Clinical features and risk factors for pyogenic liver abscess caused by multidrug-resistant organisms: a retrospective study. Virulence. 2024;15(1):2356680. doi:10.1080/21505594.2024.2356680
6. Wang J-L, Hsu C-R, Wu C-Y, Lin -H-H. Diabetes and obesity and risk of pyogenic liver abscess. Sci Rep. 2023;13(1):7922. doi:10.1038/s41598-023-34889-z
7. Suzuki H, Kidder I, Tanaka T, Goto M. Incidence of colorectal cancer in patients diagnosed with pyogenic liver abscess. JAMA Network Open. 2023;6(12):e2348218. doi:10.1001/jamanetworkopen.2023.48218
8. Peng J, Zhai Q, Li J, et al. Clostridium perfringens liver abscess disguised as biliary disease: a report of two cases and a review of the literature. Infect Drug Resist. 2023;16:5209–5222. doi:10.2147/idr.S415347
9. Yu F, Guo Y, Li Y, et al. Liver abscess and septic shock due to Clostridium perfringens infection: a case report and literature review. Front Med Lausanne. 2025;12:1575454. doi:10.3389/fmed.2025.1575454
10. Li C-H, Hsu C-K, Lai -C-C, et al. Effectiveness and safety of high-dose versus standard-dose cefoperazone-sulbactam in severe infections: a multicenter retrospective study. Infect Drug Resist. 2025;18:6269–6278. doi:10.2147/idr.S551491
11. Gu L, Wang Y, Wang H, Xu D. Analysis of clinical and microbiological characteristics of invasive Klebsiella pneumoniae liver abscess syndrome. BMC Infect Dis. 2025;25(1):626. doi:10.1186/s12879-025-10981-9
12. Angeles-Solano M, Tabashsum Z, Chen L, Rowe SE. Klebsiella pneumoniae liver abscesses: pathogenesis, treatment, and ongoing challenges. Infect Immun. 2025;93(8):e0050824. doi:10.1128/iai.00508-24
13. Hullahalli K, Dailey KG, Hasegawa Y, et al. Genetic and immune determinants of E. coli liver abscess formation. Proc Natl Acad Sci U S A. 2023;120(51):e2310053120. doi:10.1073/pnas.2310053120
14. Geremia N, Sanson G, Principe L, et al. A subanalysis of Clostridium perfringens bloodstream infections from a 5-year retrospective nationwide survey (ITANAEROBY). Anaerobe. 2024;90:102901. doi:10.1016/j.anaerobe.2024.102901
15. Bourguet E, Figurska S, Frączek MM. Human neuraminidases: structures and stereoselective inhibitors. J Med Chem. 2022;65(4):3002–3025. doi:10.1021/acs.jmedchem.1c01612
16. Mehdizadeh Gohari I, AN M, Li J, Shrestha A, Uzal F, AM B. Pathogenicity and virulence of Clostridium perfringens. Virulence. 2021;12(1):723–753. doi:10.1080/21505594.2021.1886777
17. Wang Y-H. Sialidases from Clostridium perfringens and their inhibitors. Front Cell Infect Microbiol. 2020;9:462. doi:10.3389/fcimb.2019.00462
18. Geier RR, Rehberger TG, Smith AH. Comparative genomics of Clostridium perfringens reveals patterns of host-associated phylogenetic clades and virulence factors. Front Microbiol. 2021;12:649953. doi:10.3389/fmicb.2021.649953
19. Kumon T, Oiki S, Hashimoto W. Molecular identification of hyaluronate lyase, not hyaluronidase, as an intrinsic hyaluronan-degrading enzyme in Clostridium perfringens strain ATCC 13124. Sci Rep. 2024;14(1):24266. doi:10.1038/s41598-024-73955-y
20. Lu J, Zhao Z, Pan L, et al. Hyaluronidase: structure, mechanism of action, diseases and therapeutic targets. Mol Biomed. 2025;6(1):50. doi:10.1186/s43556-025-00299-y
21. Yanxia S, Xuewei W, Gang L, Wei J. Analysis on characteristics and multilocus sequence typing of Clostridium perfringens in western China. J Antimicrob Chemother. 2025;80(1):216–226. doi:10.1093/jac/dkae399
22. Kiu R, Caim S, Alexander S, Pachori P, Hall LJ. Probing genomic aspects of the multi-host pathogen Clostridium perfringens reveals significant pangenome diversity, and a diverse array of virulence factors. Front Microbiol. 2017;8:2485. doi:10.3389/fmicb.2017.02485
23. Obana N, Takada H, Crowe-McAuliffe C, et al. Genome-encoded ABCF factors implicated in intrinsic antibiotic resistance in Gram-positive bacteria: vmlR2, Ard1 and CplR. Nucleic Acids Res. 2023;51(9):4536–4554. doi:10.1093/nar/gkad193
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.