Back to Journals » Patient Preference and Adherence » Volume 14
Characteristics, Preferences and Health Care Utilization in Patients Using a Dietary Supplement for Improving Sleeping Disturbances: Results from an Explorative Online Survey
Authors Di Gangi S ![]() , Markun S
, Markun S ![]() , Rosemann T
, Rosemann T ![]() , Plate A
, Plate A
Received 21 October 2020
Accepted for publication 1 December 2020
Published 30 December 2020 Volume 2020:14 Pages 2531—2539
DOI https://doi.org/10.2147/PPA.S287881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Stefania Di Gangi, Stefan Markun, Thomas Rosemann, Andreas Plate
Institute of Primary Care, University and University Hospital of Zürich, Zürich, Switzerland
Correspondence: Stefania Di Gangi
Institute of Primary Care, University of Zurich, Pestalozzistrasse 24, Zürich 8091, Switzerland
Tel +41 44 255 75 02
Fax +41 44 255 90 97
Email [email protected]
Purpose: Sleeping disturbances are highly prevalent in the general population, and pharmacological drug treatment harbours the risk of serious side effects. Many affected persons use dietary supplements for self-treating their symptoms, but little is known about the specific characteristics and preferences of these patients. Even less evidence exists about the consequences of a specific dietary supplement usage on health care utilization. The aim of this study was to explore characteristics, preferences and the impact on health care utilization in patients using a specific over-the-counter dietary supplement, which is promoted for improving sleeping disturbances.
Patients and Methods: We conducted a structured survey and invited a sample of 297 customers of a specific dietary supplement to participate. The survey was open between June and September 2020. Participants were invited by email. All participants accepted an informed consent.
Results: A total of 127 customers participated in the survey (participation rate: 42.8%). Of them, 87.7% were female and the mean age 50.5 years. Participants reported an overall good improvement of symptoms (7.66 on a ten-point Likert-scale) and showed a strong belief in the effectiveness of supplements in general; 67% of participants reported that the intake led to fever physician encounters, and 48.3% reported that they could stop the intake of other pharmaceutical sleeping drugs.
Conclusion: A significant proportion of participants reported a substantial reduction in pharmaceutical drug use and health care utilization. While these self-reports lack an adequate control, they are still real consumer experiences, and the large beneficial effects – whether placebo or not – explain the popularity of such supplements and their therapeutic potential in sleeping disorders.
Keywords: supplement use, sleeping disorders, usage patterns, drugs, health care utilization
Introduction
The use of dietary supplements is common, and it is estimated that up to three-quarters of adults use dietary supplements.1,2 In addition to being used to achieve a healthier lifestyle, dietary supplements are used as remedies for a variety of complaints and unspecific symptoms. Sleeping disorders are highly prevalent, and insufficient sleeping quality/quantity is associated with a wide range of negative health outcomes.3 Self-treatment with herbals, over-the-counter medication or prescribed medications is common.4 Classical pharmacological treatments of sleeping disorders (for example benzodiazepines or hypnotics) are associated with serious side effects and the risk for abuse or dependence.5 Consequently, a growing demand and offer of dietary supplements tackling sleeping disorders has been observed for many years. There is some evidence1 that dietary supplement users, aiming for a healthier lifestyle, are more frequently females with higher education and higher incomes compared to non-users. However, little is known about the characteristics, attitudes and beliefs of dietary supplements users who use the dietary supplements for sleeping disorders. In addition, there is no evidence on the impact of self-treatment on patients’ health care utilization, as sleeping disorders are a common reason for physician encounters.6–8 To gain a more detailed insight into this topic, we conducted an explorative survey among dietary supplement users using a specific over-the-counter dietary supplement, which is promoted for improving sleeping disturbances. The goal of the present explorative study was to determine characteristics, preferences and the impact of use on their health care utilization.
Patients and Methods
Methods
Data for this study were obtained by an anonymous online survey. The survey was conducted in Switzerland, and 297 customers of Sero-Night,9 a dietary supplement advertised for improving sleeping quality, were invited by email to participate in the survey. The dietary supplement’s main ingredients were L-tryptophan, ashwagandha extract, inositol, L-methionin as well as vitamins B 5/6/12. The survey was open for 11 weeks beginning from mid-June 2020, and customers received up to two reminders by email. We used a commercial survey software (Survey Monkey Inc., San Mateo, California, USA). For subgroup analysis, we used adaptive questioning depending on the previous answers of the customers. The survey had a total length of 13 screens, with a mean of 2.8 questions on each screen. All participants were able to review their answers. Software’s function was used to prevent multiple entries from the same device. The survey was fully anonymous, and no questions were mandatory. Questions were closed-ended (ie education, field of employment), open-ended (ie type of medication, further supplements), multiple choice (ie reasons for intake) and Likert-scale (ie overall satisfaction). A checklist for reporting results of internet e-surveys (CHERRIES)10 is provided in the supplemental material (Supplemental Table 1).
Statistics
Results are presented as means (standard deviations [SD]) for continuous variables and as number N (%), or only %, for categorical variables. The range (min–max) was reported for age and all variables defined in Likert-scale points. When necessary, we reported the missing values. In case of incomplete questionnaires, we analysed only the available data, without imputation. All statistical analyses were carried out using statistical package R, R Core Team (2016). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.
Ethics
Fully anonymous surveys do not fall under the scope of the Swiss national Human Research Act, and thus no ethics approval is necessary to perform health surveys. Participation to the survey was voluntary, and each participant signed an informed consent, which contained all information about the purpose of the study. All participants agreed to a scientific analysis and the publication of the data.
Results
A total of 127 customers participated in the survey, and the participation rate was 42.8% (127/297). Basic demographic and health data of the participants are reported in Table 1: 87.7% of participants were female, and the mean age was 50.5 (SD 10.3) years (range: 26−76 years). Furthermore, 33% of the participants had an education level equal to or higher than a Master degree, and 60% had an education level equal to or higher than a Bachelor degree. The most common fields of employment were economy, management (27%), education, social issues (23.5%) and health (17.4%). Mean self-reported wellbeing, on a ten-point Likert-scale, was 7.15 (SD 1.5). Active smoking was reported by 4.3% of participants, and one-fifth of participants reported no additional comorbidities. The most common reported comorbidities were sleeping disorders (31.5%) and postmenopausal complaints (24.4%). Participants reported a mean of 3.5 (SD 4.8) physician consultations within the previous twelve months.
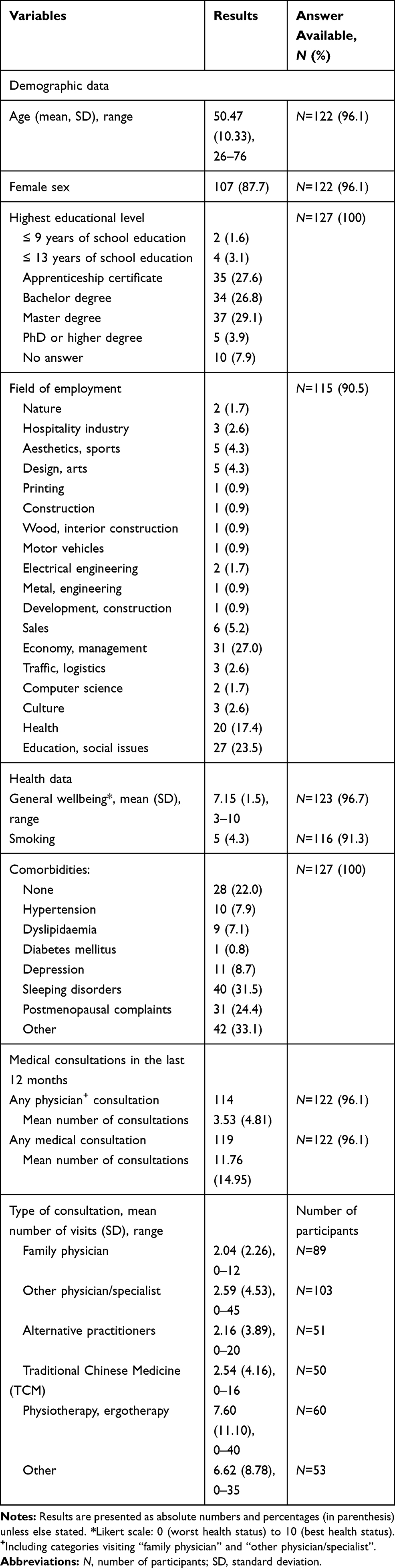 |
Table 1 Basic Demographic and Health Data of 127 Participants |
The specific user preferences of supplement use are reported in Table 2. The overall satisfaction of supplements, on a ten-point Likert-scale, was on average 7.59 (SD 2.9). Participants reported a mean duration of intake of 13.5 (SD 10.3) months with a mean of 5.9 (SD 1.8) intakes per week. Specialists or physicians different from family doctors generally recommended the supplements, in nearly 80% of the cases. More than 80% of the participants used the supplement in order to optimize their sleeping patterns. However, mood disorders (mood swings or depressive mood) were common additional reasons for the supplement use in up to one-third of patients. Regarding the improvement of symptoms, the mean satisfaction score, on a ten-point Likert-scale, was 7.66 (SD 2.1). Just over 70% of the participants who used the supplement to optimize their sleeping patterns reported improvement in staying asleep during the night. Generally, more than 81% of the participants did not experience side effects during the use of supplements. Almost 90% of all participants reported the use of a mean of 3.35 (SD 1.9) further supplements. Participants reported the intake of various combinations of vitamins, electrolytes, herbals and amino acids, with vitamin D the most commonly reported single supplement.
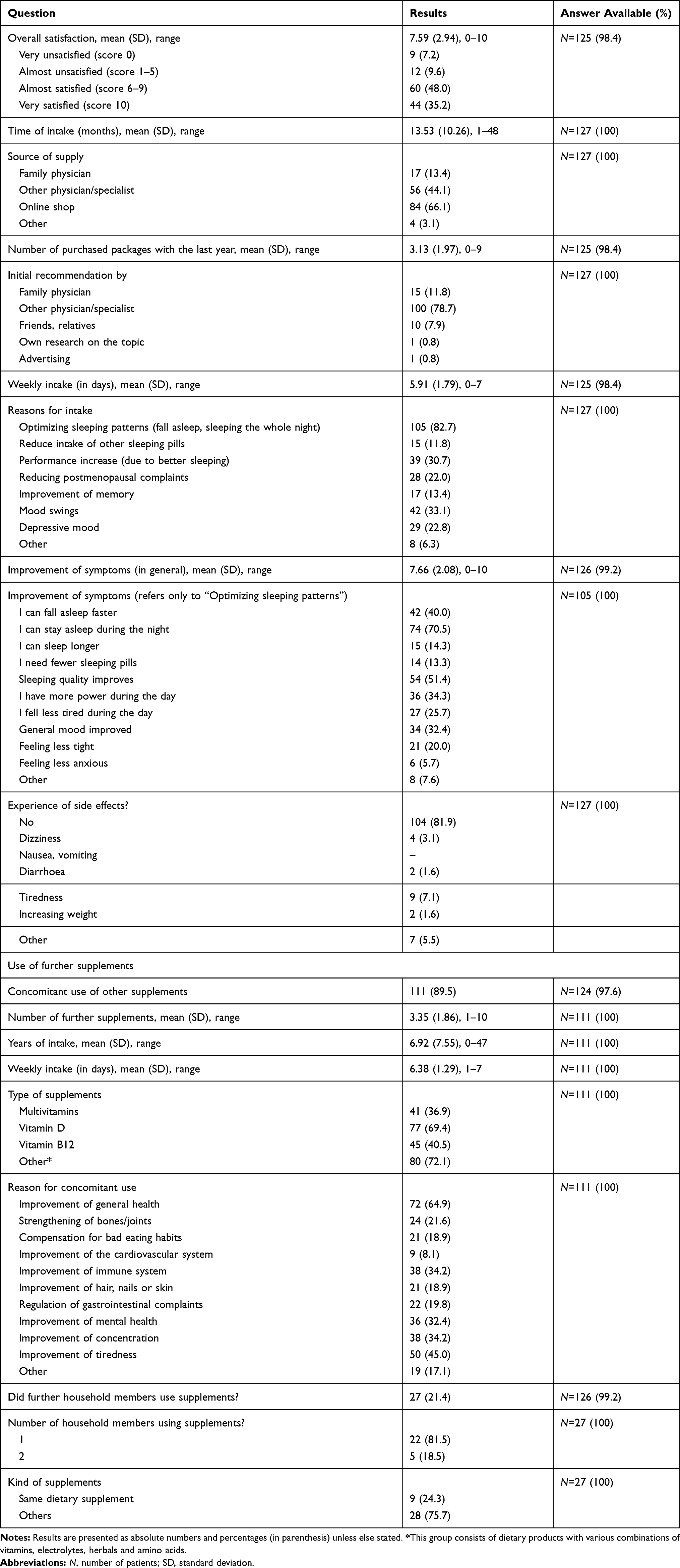 |
Table 2 Use of Supplements: Specific Characteristics and Preferences |
Results about the effects of supplements on co-medications and health care utilization are reported in Table 3. A total of 87.1% of participants reported a previous health care utilization because of index symptoms in the past, and more than two-third of them (67%) reported that the use of the supplement led to reduced physician consultations. Over one-half of participants reported the use of other medications (for example pharmaceutical drugs [56.4%] or herbals [49%]), with antidepressants, hypnotics and melatonin the most frequently used drugs and sleeping pills the most frequently used herbal medication (supplemental Table 2). In the subgroup of participants with other medications, 84.5% reported that the use of the supplement led to a stop or decrease in the uptake of additional medications (Table 3).
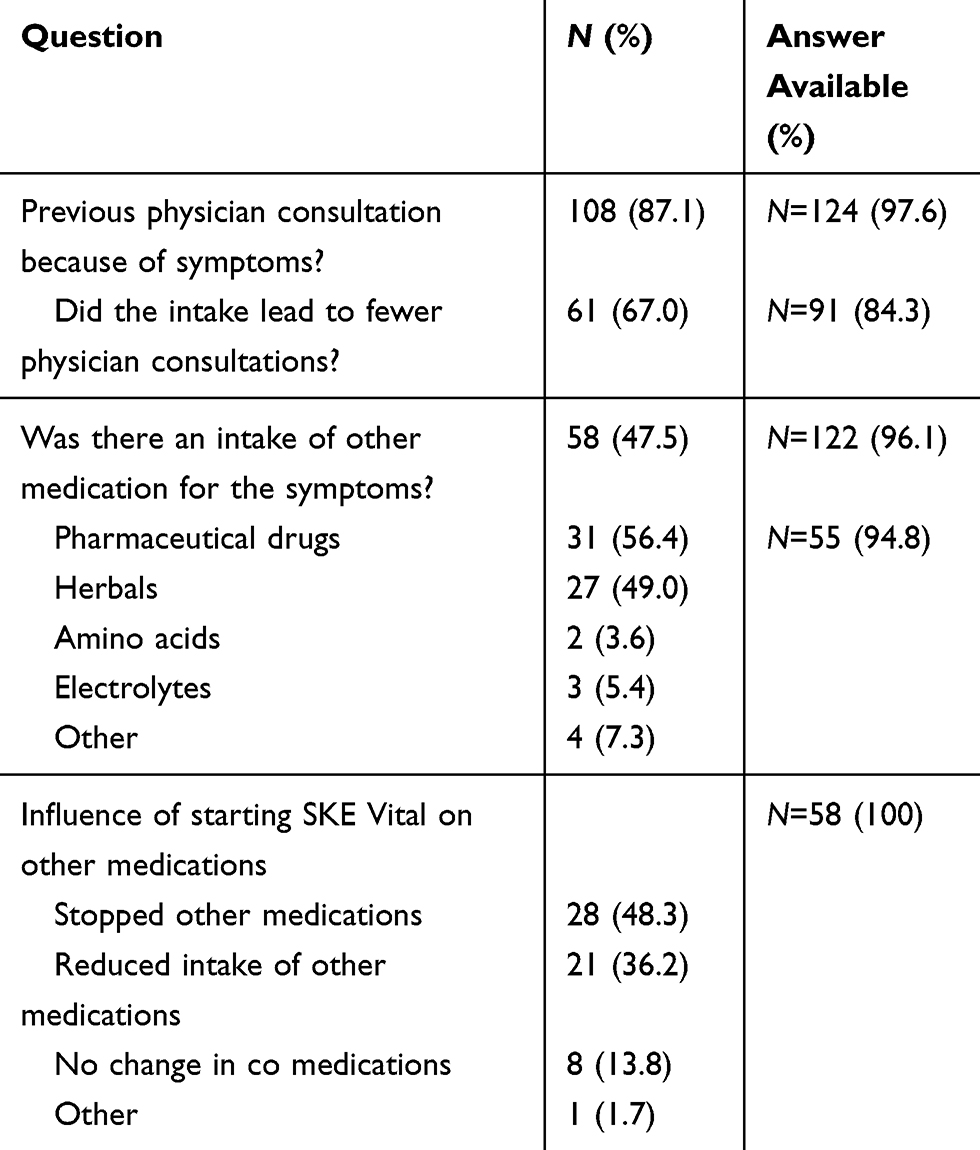 |
Table 3 Influence of Supplement Use on Co-Medications and Health Care Utilization |
Participants’ attitudes and beliefs regarding the effectiveness of dietary supplements for various health conditions are presented in Figure 1. Whereas nearly half of the participants (47.5%) disagreed with the statement that dietary supplements are a possibility to compensate for bad living habits in general (answer one [red] and two [yellow] on a five-point Likert-scale), most of the participants reported that they believed in the effectiveness of dietary supplements for various health complaints. An exception was cardiovascular health, where belief in the effectiveness of dietary supplements was considerably low.
 |
Figure 1 Attitudes and beliefs in effectiveness of dietary supplements. % of participants, for each point Likert-scale are shown. (A): Results from a five point Likert-scale (pink: totally agree to red: totally disagree). Bad habits: Dietary supplements as a compensation for bad life habits. (B): Results from a five point Likert-scale (pink: very effective to red: not effective). General: Improvement of general health; Bones/joints: Strengthening of bones/joints; Bad eating: compensation for bad eating habits; CVS: Improvement of the cardiovascular system; Immune system: improvement of the immune system; Hair/nails: improvement of hair, nails or skin; Gastrointestinal: regulation of gastrointestinal complaints; Mental: improvement of mental health; Concentration: improvement of concentration; Tiredness: improvement of tiredness. |
Discussion
In this study, we investigated characteristics, beliefs and preferences of supplement users taking a specific dietary supplement to improve sleeping quality. We found that users were predominantly highly educated females, experienced in supplement use and that the intake of the dietary supplement led to self-perceived reduced health care utilization and reduced consumption of pharmaceutical drugs.
Sleeping disorders are a common complaint in developed countries,3 and inadequate sleeping quality is associated with various adverse outcomes (ie depression,11 risk of falling,12 diabetes mellitus13). Several studies reported the association between sleeping disorders and health care utilization,14–16 but the impact of dietary supplements on improving sleeping disorders is unknown. For some ingredients of the studied dietary supplement, there is little/moderate evidence of a clinical effect in patients with sleeping disorders: the essential amino acid L-tryptophan, which is a precursor of the endogenous melatonin and serotonin synthesis, is often used to treat insomnia and depression,17,18 and sparse evidence suggests that ashwagandha extract can improve insomnia and anxiety.19,20 However, there are no comparative studies reported in the literature, and general transferability of study results is hardly feasible because ingredients and composition of the studied dietary supplements differ.
Basic Characteristics
Basic characteristics of our participants were similar to the characteristics reported in larger scale population-based surveys on supplement use.1,21 Most participants were highly educated females, and the overall wellbeing was high. With the exception of cardiovascular health, participants reported strong beliefs in the effectiveness of dietary supplements on various health conditions. Therefore, the majority of participants reported a long experience in supplement use, taking more than one supplement almost every day. Moreover, the low proportion of smokers in our patient group (4.3% vs 27.1% in the general population22) could reveal that the use of supplements is perceived as a way to help a healthier lifestyle.1
Health Care Utilization
Sleeping disorders are associated with health care utilization14–16 and are a common reason for physician encounters.6–8 Two large population-based surveys from Canada4 and Australia23 reported that between 11% and 13% of the population sought medical care because of sleeping disturbances. In patients diagnosed with an insomnia disorder, the proportion was up to 40%.4 The characteristics of our participants resembled the patterns described in the literature. Almost 90% of all participants reported a physician consultation because of symptoms, but the mean consultation numbers were close to the mean consultation numbers in the overall population (3.5 vs 4.3 per year24). However, two-thirds of participants in our study reported that the use of dietary supplement reduced the physician consultations. Available, sparse evidence showed no positive impact of supplement use in general and on health care costs,25 but its association in specific users is still unknown. Though we reported explorative data from a highly selected population of experienced supplement users, given the high prevalence of sleeping disorders, a relative reduction of consultations in two-third of patients, or in a subgroup of patients, could have an economic impact, in terms of health cost reduction, which should be confirmed in future studies.
Self-Medication of Sleeping Disorders
We found a self-perceived reduction in sleeping disorder-specific drug consumption. Sleeping disorders are a common indication for self-medication.26,27 Herbals and pharmaceutical drugs are the most commonly used medications, and their use differs internationally and depends on particular types of sleeping disorder.4,5 Accordingly, the participants of our survey reported the use of various herbals and pharmaceutical drugs. Major issues with pharmaceutical drugs are potential serious side effects, abuse or dependence.5 In addition, evidence on effectiveness of some commonly used drugs (for example antihistamines or melatonin) is limited.28,29 A reduction of these drugs would be beneficial as a kind of harm reduction. On the other hand, the consequences of excessive dietary supplement use is unknown,30 and still dietary supplements harbour a significant risk of serious side effects.31 Especially if multiple supplements are used, the recommended daily intake is often surpassed.32 In our patient group, half of the participants reported the use of other medication for improving symptoms before starting the supplement. In the subgroup of pharmaceutical drug users, the majority of participants reported to either have stopped or reduced the drug after starting the dietary supplement. We cannot know if a real effect based on the ingredients or a placebo effect of the supplement use led to a stop or reduction of the pharmaceutical drugs, or whether these patients would have stopped the drugs by themselves. However, taking into account that only 22% of this subgroup started the dietary supplement with the intention to reduce the intake of their other sleeping medications, there might be a beneficial effect, which should be confirmed and evaluated in further trials too.
Strengths and Limitations
Our study has some limitations. First, we reported results from a survey among a specific group of dietary supplement users, and second, our study lacked a control group. Therefore, it must be acknowledged that our results merely represent beliefs of this specific population, and our results must not be misunderstood for specific effects of the supplement. However, our findings highlight the beliefs of users and their perceptions of the supplement despite the paucity of supporting evidence available. Given the high prevalence of sleeping disorders in the general population there is a potential for relevant supplement use of unknown benefit, costs or even harm that needs to be better understood. In addition, given the fact that millions of people use supplements, it is of medical importance to understand patients’ attitudes, beliefs and expectations. Lastly, we are aware about a potential non-response bias: those with positive experiences associated with supplement intake may have been more likely to respond. However, available evidence suggested that the impact of the non-response bias in satisfaction surveys is limited.33,34
Conclusion
A significant proportion of participants reported a substantial reduction in pharmaceutical drug use and health care utilization. While these self-reports lack an adequate control, they are still real consumer experiences and beliefs. The large beneficial effects – whether placebo effect or not – explain the popularity of such supplements and their therapeutic potential in sleeping disorders.
Funding
The study was sponsored by SKE Vital. The sponsor had no influence on conceptualization of the study and analysing and interpreting of the obtained data.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dickinson A, MacKay D. Health habits and other characteristics of dietary supplement users: a review. Nutr J. 2014;13(1):14. doi:10.1186/1475-2891-13-14
2. Knudsen VK, Rasmussen LB, Haraldsdóttir J, et al. Use of dietary supplements in Denmark is associated with health and former smoking. Public Health Nutr. 2002;5(3):463–468. doi:10.1079/PHN2001276
3. Chattu VK, Manzar MD, Kumary S, Burman D, Spence DW, Pandi-Perumal SR. The Global Problem of Insufficient Sleep and Its Serious Public Health Implications. Healthcare. 2018;7:1.
4. Morin CM, LeBlanc M, Daley M, Gregoire JP, Mérette C. Epidemiology of insomnia: prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006;7(2):123–130. doi:10.1016/j.sleep.2005.08.008
5. Lie JD, Tu KN, Shen DD, Wong BM. Pharmacological Treatment of Insomnia. Peer Rev j Formulary Manage. 2015;40(11):759–771.
6. Fukushi M, Ishibashi Y, Nago N. Final diagnoses and probability of new reason-for-encounter at an urban clinic in Japan: A 4-year observational study. J Clin Med. 2017;96(22):e6999.
7. Liu Y, Chen C, Jin G, et al. Reasons for encounter and health problems managed by general practitioners in the rural areas of Beijing, China: A cross-sectional study. PLoS One. 2017;12(12):e0190036. doi:10.1371/journal.pone.0190036
8. Senthilvel E, Auckley D, Dasarathy J. Evaluation of sleep disorders in the primary care setting: history taking compared to questionnaires. J Clin Sleep Med. 2011;7(1):41–48.
9. Vital SKE. 2020; https://www.ske-vital.ch/produktseite/sero-night.
10. Eysenbach G. Improving the quality of Web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34. doi:10.2196/jmir.6.3.e34
11. Morphy H, Dunn KM, Lewis M, Boardman HF, Croft PR. Epidemiology of insomnia: a longitudinal study in a UK population. Sleep. 2007;30(3):274–280.
12. Stone KL, Ancoli-Israel S, Blackwell T, et al. Actigraphy-measured sleep characteristics and risk of falls in older women. Arch Intern Med. 2008;168(16):1768–1775. doi:10.1001/archinte.168.16.1768
13. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes mellitus and impaired glucose tolerance. Arch Intern Med. 2005;165(8):863–867. doi:10.1001/archinte.165.8.863
14. Kaufmann CN, Canham SL, Mojtabai R, et al. Insomnia and health services utilization in middle-aged and older adults: results from the Health and Retirement Study. J Gerontol a Biol Sci Med Sci. 2013;68(12):1512–1517. doi:10.1093/gerona/glt050
15. Kapur VK, Redline S, Nieto FJ, Young TB, Newman AB, Henderson JA. The relationship between chronically disrupted sleep and healthcare use. Sleep. 2002;25(3):289–296.
16. Novak M, Mucsi I, Shapiro CM, Rethelyi J, Kopp MS. Increased utilization of health services by insomniacs–an epidemiological perspective. J Psychosom Res. 2004;56(5):527–536. doi:10.1016/j.jpsychores.2004.02.007
17. Lieberman HR, Agarwal S, Fulgoni VL. Tryptophan Intake in the US Adult Population Is Not Related to Liver or Kidney Function but Is Associated with Depression and Sleep Outcomes. J Nutr. 2016;146(12):2609S–2615S. doi:10.3945/jn.115.226969
18. Simper T, Gilmartin M, Allwood D, Taylor L, Chappell A. The effects of a sleep/recovery supplement: ‘Night Time Recharge’ on sleep parameters in young adults. Nutr Health. 2019;25(4):265–274. doi:10.1177/0260106019875911
19. Langade D, Kanchi S, Salve J, Debnath K, Efficacy AD. Safety of Ashwagandha (Withania somnifera) Root Extract in Insomnia and Anxiety: A Double-blind, Randomized, Placebo-controlled Study. Cureus. 2019;11(9):e5797.
20. Lopresti AL, Smith SJ, Malvi H, Kodgule R. An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract: A randomized, double-blind, placebo-controlled study. Medicine. 2019;98(37):e17186. doi:10.1097/MD.0000000000017186
21. Satia-Abouta J, Kristal AR, Patterson RE, Littman AJ, Stratton KL, White E. Dietary supplement use and medical conditions: the VITAL study. Am J Prev Med. 2003;24(1):43–51. doi:10.1016/S0749-3797(02)00571-8
22. Zahlen BAG & Fakten: tabak. 2020; https://www.bag.admin.ch/bag/de/home/zahlen-und-statistiken/zahlen-fakten-zu-sucht/zahlen-fakten-zu-tabak.html.
23. Bartlett DJ, Marshall NS, Williams A, Grunstein RR. Predictors of primary medical care consultation for sleep disorders. Sleep Med. 2008;9(8):857–864. doi:10.1016/j.sleep.2007.09.002
24. Schweizerische Gesundheitsbefragung 2017. 2018; https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/erhebungen/sgb.assetdetail.6426300.html.
25. Kilonzo MM, Vale LD, Cook JA, Milne AC, Stephen AI, Avenell A. A cost-utility analysis of multivitamin and multimineral supplements in men and women aged 65 years and over. Clin nutrition. 2007;26(3):364–370. doi:10.1016/j.clnu.2006.11.002
26. Shehnaz SI, Agarwal AK, Khan N. A systematic review of self-medication practices among adolescents. J Adolescent Health. 2014;55(4):467–483. doi:10.1016/j.jadohealth.2014.07.001
27. Lund HG, Reider BD, Whiting AB, Prichard JR. Sleep patterns and predictors of disturbed sleep in a large population of college students. J Adolescent Health. 2010;46(2):124–132. doi:10.1016/j.jadohealth.2009.06.016
28. Ramar K, Olson EJ. Management of common sleep disorders. Am Fam Physician. 2013;88(4):231–238.
29. Brzezinski A, Vangel MG, Wurtman RJ, et al. Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Med Rev. 2005;9(1):41–50. doi:10.1016/j.smrv.2004.06.004
30. Chen F, Du M, Blumberg JB, et al. Association among dietary supplement use, nutrient intake, and mortality among u.s. adults: a cohort study. Ann Intern Med. 2019;170(9):604–613. doi:10.7326/M18-2478
31. Geller AI, Shehab N, Weidle NJ, et al. Emergency department visits for adverse events related to dietary supplements. N Engl J Med. 2015;373(16):1531–1540. doi:10.1056/NEJMsa1504267
32. Panel NS-o-tS. National institutes of health state-of-the-science conference statement: multivitamin/mineral supplements and chronic disease prevention. Am J Clin Nutr. 2007;85(1):257S–264S. doi:10.1093/ajcn/85.1.257S
33. Lasek RJ, Barkley W, Harper DL, Rosenthal GE. An evaluation of the impact of nonresponse bias on patient satisfaction surveys. J Int Med. 1997;35(6):646–652.
34. Perneger TV, Chamot E, Bovier PA. Nonresponse bias in a survey of patient perceptions of hospital care. Med Care. 2005;43(4):374–380. doi:10.1097/01.mlr.0000156856.36901.40
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.