Back to Journals » Advances in Medical Education and Practice » Volume 14
Characteristics of University Hospitals Implementing the Postgraduate Clinical Training “Tasukigake Method” and Their Correlation with Program Popularity: A Cross-Sectional Study
Authors Watanabe S, Kataoka K ![]() , Sekine M
, Sekine M ![]() , Aune D, Shikino K
, Aune D, Shikino K ![]() , Nishizaki Y
, Nishizaki Y
Received 21 December 2022
Accepted for publication 13 March 2023
Published 31 March 2023 Volume 2023:14 Pages 323—332
DOI https://doi.org/10.2147/AMEP.S402259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sadatoshi Watanabe,1 Koshi Kataoka,2 Miwa Sekine,2 David Aune,2 Kiyoshi Shikino,3 Yuji Nishizaki1,2
1Clinical Translational Science, Juntendo University Graduate School of Medicine, Tokyo, Japan; 2Division of Medical Education, Juntendo University Faculty of Medicine, Tokyo, Japan; 3Department of Medical Education, Chiba University School of Medicine, Chiba, Japan
Correspondence: Yuji Nishizaki, Clinical Translational Science, Juntendo University Graduate School of Medicine, 2-1-1 Hongo, Bunkyo-Ku, Tokyo, 113-8421, Japan, Tel +81-3-3813-3111, Fax +81-3-5689-0627, Email [email protected]
Purpose: In 2004, the postgraduate clinical training system in Japan was radically revised by introducing a super-rotation matching system. Although postgraduate clinical training became a mandatory 2 years of training, the program and operation were left to each facility’s discretion, leading to training-program popularity differences. The Japanese Tasukigake method provides clinical training in which “hospitals where junior residents work” and “external hospitals/clinics that provide clinical training” conduct clinical training alternately on a 1-year basis. The study aimed to identify the characteristics of university hospitals that implement the Tasukigake method to help educators and medical institutions create more attractive and effective programs.
Methods: All 81 university main hospitals were included in this cross-sectional study. The information regarding Tasukigake method implementation was collected from the facilities’ websites. The training program’s matching rate (popularity) was calculated from the Japan Residency Matching Program’s interim report data (academic 2020). We used multiple linear regression analysis to evaluate the association between Tasukigake method implementation, program popularity, and university hospital characteristics.
Results: The Tasukigake method was implemented by 55 (67.9%) university hospitals, significantly more by public university hospitals (44/55, 80%) than by private (11/55, 20%) (P < 0.01) and by hospitals without branches (38/55, 69.1%) than with branches (17/55, 30.9%) (P < 0.001). The maximum hiring capacity of junior residents (P = 0.015) and number of branches (P < 0.001) were negatively correlated, and the population of the hospital’s city (P = 0.003) and salary/month (P = 0.011) were positively correlated with the Tasukigake method implementation. Multiple linear regression analysis results showed no significant association between the matching rate (popularity) and Tasukigake method implementation.
Conclusion: The results show no association between Tasukigake method and program popularity; also, highly specialized university hospitals in cities with fewer branch hospitals were more likely to implement the Tasukigake method.
Keywords: clinical training, Japanese residency matching program, junior residents, residency rotations, super-rotation, Tasukigake method
Plain Language Summary
Why was the Study Done?
- Numerous university hospitals in Japan have implemented the so-called “Tasukigake method” in postgraduate clinical training.
- However, we do not know what kind of university hospitals would use the Tasukigake method as a training program or the relationship between this method and the program’s popularity.
What did the Researchers Do and Find?
- We conducted an analysis to identify the characteristics of all 81 university hospitals that use the Tasukigake method in postgraduate medical training.
- We collected publicly available data from various websites and analyzed the characteristics of university hospitals implementing the Tasukigake method.
- We found that the Tasukigake method is implemented more by public medical school hospitals and university hospitals without branch hospitals.
- We also found that hospitals that implemented the Tasukigake method had a smaller capacity for resident recruitment, lower popularity, and fewer ambulance cases but also a higher city population and offered higher monthly salaries.
What Do these Results Mean?
- To attract medical students, the Tasukigake method has been shown to supplement and reinforce postgraduate clinical training by providing experience in the treatment of various common illnesses or conditions.
Introduction
Currently, clinical rotation training is implemented in many countries to provide newly qualified medical residents with additional practical experience in clinical skills through engagement with various clinical cases under the supervision of attending physicians.1 In the United States or Australia, postgraduate medical students are required to undertake clinical rotations in various medical specialties, such as internal medicine, surgery, and emergency medicine, because early exposure to these disciplines and clinical settings provides important clinical experience when training residents.
In 2004, the Japanese Ministry of Health, Labor, and Welfare (MHLW) implemented a 2-year-long structured set of residency rotations as compulsory postgraduate clinical training2 to establish a national matching system administered by the new Japanese Residency Matching Program (JRMP).3–5 The JRMP provides the match-making system to medical students expecting to graduate or graduates and training hospitals that are looking for newly graduated physicians. In this system, residency applicants and training hospitals are optimally matched by a specific computed algorithm.
After graduating from a 6-year medical school and passing the National Examination for Medical Practitioners, medical students then participate in postgraduate clinical training called “super-rotation residencies”, a 2-year-long structured set of rotations among seven specialties (internal medicine, surgery, emergency medicine, pediatrics, obstetrics/gynecology, psychiatry, and community-based medicine), as well as experience general outpatient management in Japan (Figure 1). Physicians in these postgraduate clinical training years are called junior residents in Japan. The MHLW formulates the guidelines for each facility to create training programs, which are revised every 5 years, including setting the objectives for basic clinical skills, communication skills, professionalism, and ethics.6 Medical students apply to postgraduate clinical training programs provided by 1021 hospitals in their senior year through the computerized matching system noted above,4,7 and the popularity of each hospital among medical students is published by JRMP yearly and draws considerable media attention.8,9 Attaining excellent prospects is not the only interest of hospitals in Japan because it is also a fundamental need of many hospitals worldwide; indeed, many hospitals even utilize social media to attract medical students.10,11
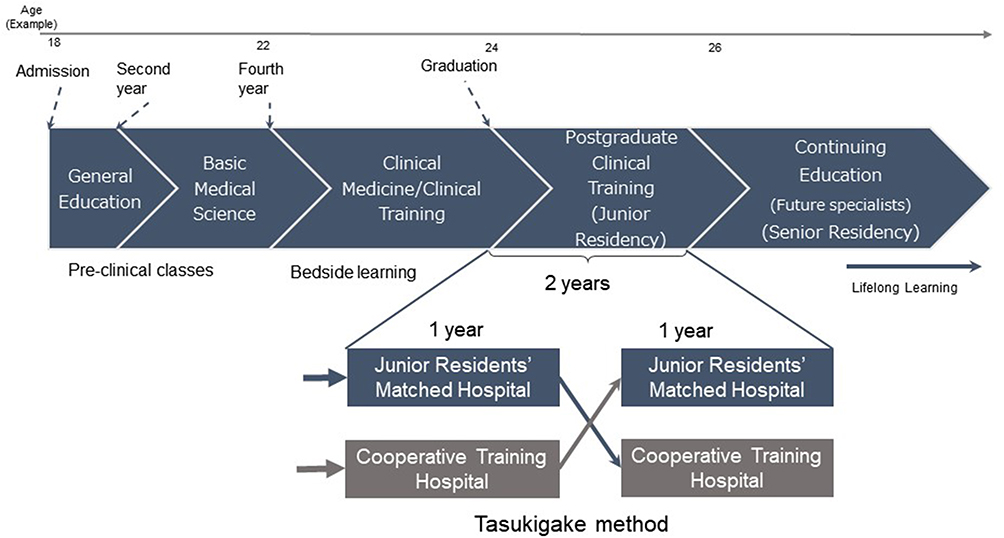 |
Figure 1 Medical education in Japan. |
The three main roles of university hospitals in Japan are (1) education, (2) research, and (3) providing advanced medical care.12 In addition to the list above, university hospitals in rural areas have important roles of providing physicians and health care to the neighboring remote areas. Conversely, community hospitals in Japan are accessible to the general public and provide medical care as well as disease preventive care and health education and promotion. In short, community hospitals are broadly clinically oriented regional hospitals. The MHLW reported that the ratio of the number of job offers at university hospitals fell below 40% for the first time (university hospital junior-resident prospects: 3513, other clinical training hospital junior-resident prospects: 5529).9 Given the increasing popularity of community hospitals and declining popularity of university hospitals in addition to the need of providing more physicians to rural areas,13–15 developing attractive training programs has become a pressing issue16 among university hospitals. However, there have been few studies regarding popular training programs at university hospitals in Japan.
The Tasukigake method is a clinical training method in Japan in which “hospitals where junior residents work” and “external hospitals/clinics that provide clinical training (so-called cooperative clinical training hospitals)” conduct clinical training alternately on a 1-year basis (Figure 1). In this study, we investigated the number of university hospitals that implemented the Tasukigake method as a postgraduate clinical training program and the characteristics of those universities, as well as whether the implementation of Tasukigake method is associated with the programs’ matching rate (popularity), using 2020 data from the JRMP,9 Residency Electronic Information System (REIS),17 and Foundation for Promotion of Medical Training.18
Materials and Methods
Study Design
This was a cross-sectional study using nationwide matching data open to the public and the information from the websites of each hospital. This study did not include human participants, so informed consent was not needed according to the Ethical Guidelines for Medical and Biological Research Involving Human Subjects.
Data Source
Basic Information
We collected the following data from the websites of the Ministry of Education, Culture, Sports, Science, and Technology (MEXT), the MHLW, the Physician Clinical Training Matching Council, the Clinical Training Program Search Site, the Medical Training Promotion Foundation, and of each university hospital: (i) postgraduate clinical training matching system interim report data (academic year 2020);19 (ii) details of postgraduate clinical training programs, Tasukigake method implementation, salary/month (10,000 yen); (iii) university type (public, private), salary/month, number of beds, number of accepted ambulance cases/year, and certification as a tertiary emergency center for each hospital compiled from the REIS;17 and (iv) populations of the cities where the hospitals were located and the presence of stations for shinkansen (bullet trains).20
Hospital Selection
There are 82 medical schools in Japan (42 national schools, 8 public schools, 31 private schools, and the National Defense Medical College) (Supplementary Table 1). We excluded the National Defense Medical College because of jurisdictional differences and the restriction on postgraduate clinical training choices. Based on the information from the postgraduate clinical training matching system interim report data (academic year 2020), we selected 81 university main hospitals (42 national hospitals, 8 public hospitals, and 31 private hospitals) from the MEXT’s university hospital webpage.19,21 The number of branch hospitals was compiled according to each main hospital’s webpages.
Matching Rate (Popularity) of the Postgraduate Clinical Training Program
We calculated the matching rate (popularity) of postgraduate clinical training programs using postgraduate clinical training matching system interim report data (the academic year 2020).19 First, we set the training program with the highest hiring capacity of each university’s main hospital as a flagship program. Next, the number of students who registered in the program as the first choice was considered a numerator, and the matching rate of each training program was evaluated using the number of capacities for the flagship program as the denominator (matching rate [popularity] = number of students enrolled in the program as the first choice/hiring capacities). We adopted the interim match result rather than the final match result because the latter seems to reflect the pure preference of medical students.
Determination of Tasukigake Method Implementation
We defined the Tasukigake method as a method in which the university main hospital and external clinical training hospitals (cooperative clinical training hospitals) provide training alternately on a 1-year basis (Figure 1).
Statistical Analysis
The data are presented as frequencies and percentages for categorical variables, median (25%, 75%) for nonparametric variables, and means ± standard deviations for parametric variables. Sample size was not calculated because we used a complete list of all medical universities in Japan. To assess the normality, the Shapiro–Wilk test and box plots were used. The significance of differences was determined using the Mann–Whitney test for nonparametric variables and Pearson chi-square test for categorical variables. To assess the association between programs for junior residency using the Tasukigake method in university hospitals and its popularity, first, multiple linear regression analysis was performed using the Tasukigake method with or without a dependent variable, and characteristics, such as the maximum hiring capacity of the program, number of accepted ambulance cases/year, number of branch hospitals, population/city (1000), and salary/month (10,000 yen), were used as explanatory variables; then, multiple linear regression analysis was performed using popularity as a dependent variable and the number of branch hospitals, population/city, salary/month, ambulance cases/year, number of beds, and certification as an emergency center as explanatory variables. Of note, we excluded the university category as an explanatory variable owing to a high correlation with the number of branch hospitals (ρ = 0.819, P < 0.001). All statistical analyses were performed using IBM SPSS Statistics for Windows, Ver. 28.0. (IBM Corp., Armonk, NY). In this study, P < 0.05 was considered to be indicative of a statistically significant result.
Results
Basic Characteristics
Of 81 university hospitals, 55 (67.9%) implemented the Tasukigake method for their clinical training program. Significantly more public university hospitals than private university hospitals (44/55, 80% vs 11/55, 20%, P < 0.001) and significantly more university hospitals without branch hospitals than with branch hospitals (38/55, 69.1% vs 17/55, 30.9%, P < 0.001) implemented the Tasukigake method. No significant difference was observed in the Tasukigake method implementation between hospitals certified as secondary emergency medical facilities or tertiary emergency medical facilities nor if the bullet train station was within the city where the hospitals were located. Additionally, hospitals implementing the Tasukigake method had a significantly lower maximum hiring capacity for the program (P = 0.014), popularity (P = 0.046), and number of ambulance cases/year (P < 0.001). On the other hand, hospitals implementing the Tasukigake method had a significantly higher city population (P = 0.014) and salary/month (P = 0.005). Furthermore, no significant difference was observed between hospitals that implemented the Tasukigake method and the number of beds (Table 1 and Table 2).
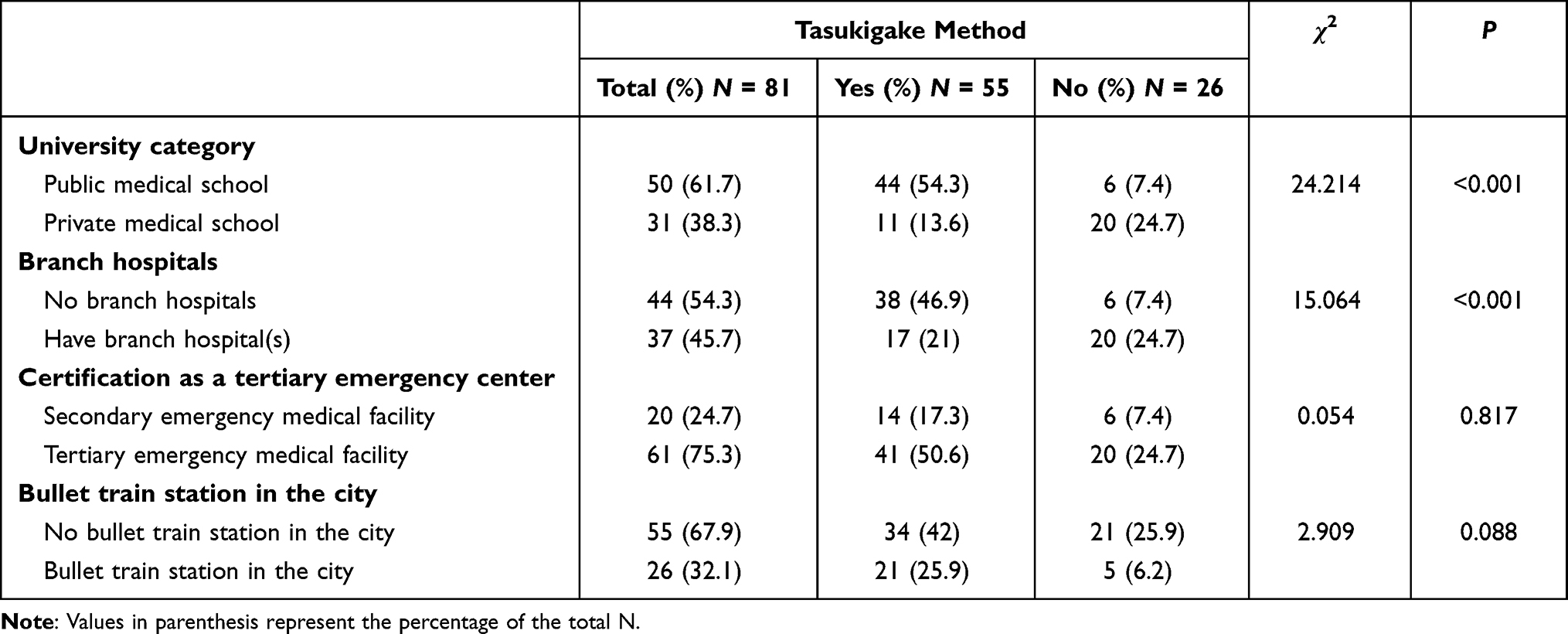 |
Table 1 Comparison of Clinical Training Programs That Did or Did Not Use the Tasukigake Method |
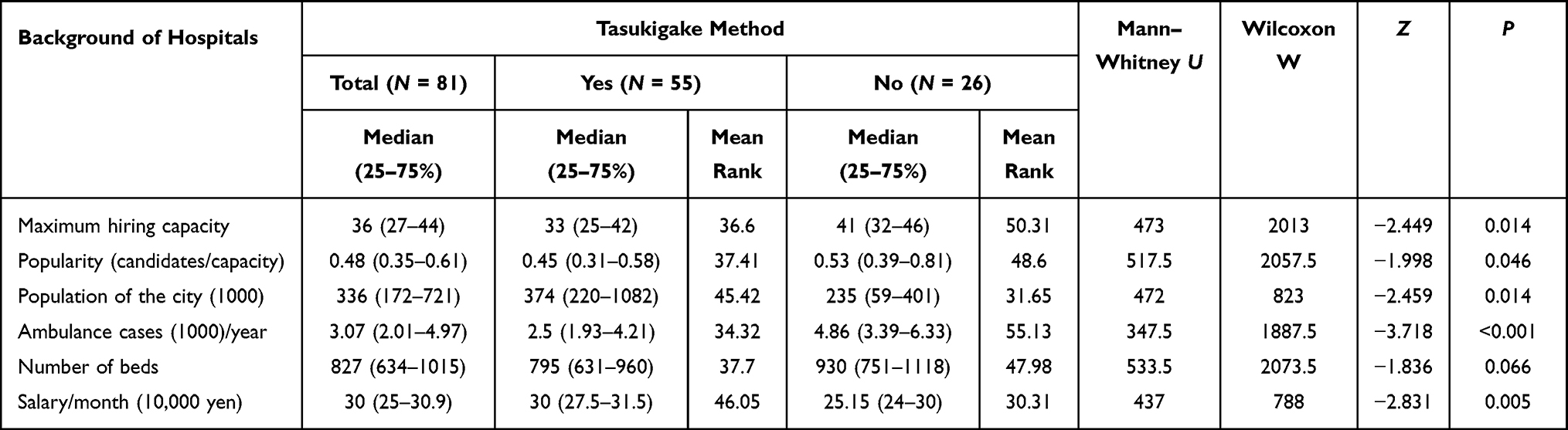 |
Table 2 Comparison Between Clinical Training Programs That Did or Did Not Use the Tasukigake Method |
Multiple Linear Regression Analysis
The multiple linear regression analysis for the Tasukigake method revealed no significant association between ambulance cases/year and the number of beds. On the other hand, other factors, such as the capacity of hiring junior residents (P = 0.015), number of branch hospitals through which junior residents could potentially rotate (P < 0.001), city population (P = 0.003), and salary/month (P = 0.011), significantly associated with the Tasukigake method implementation (Table 3). Moreover, although there was no significant association between the matching rate (popularity) and Tasukigake method implementation, the matching rate (popularity) tended to correlate with the number of branch hospitals (P = 0.053; Table 4; Figure 2).
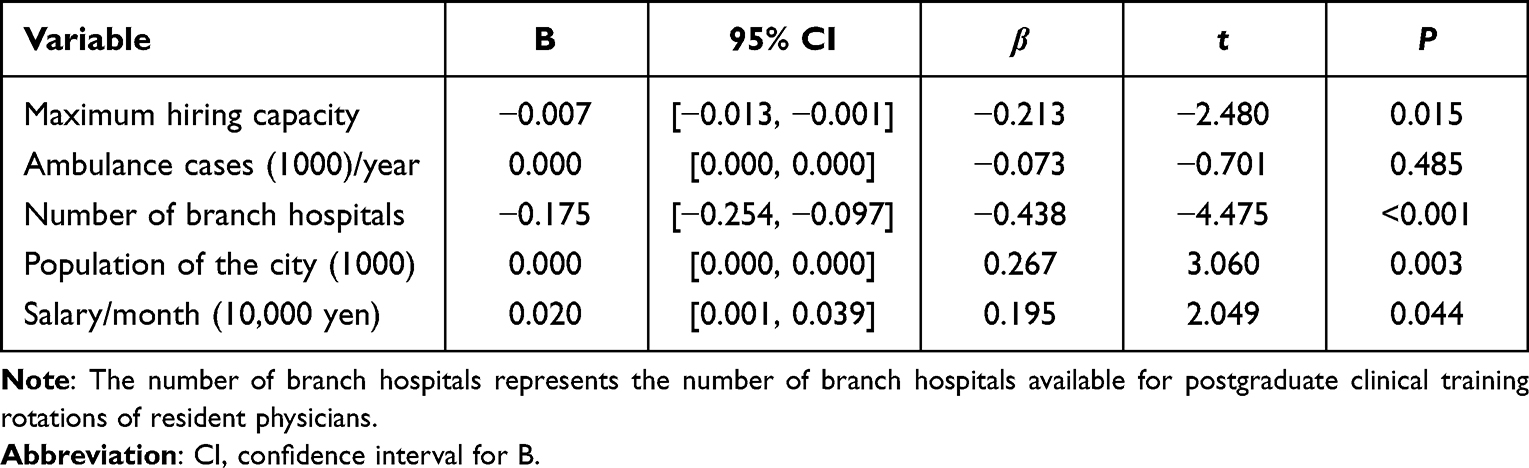 |
Table 3 Regression Coefficients for the Residency Programs That Used the Tasukigake Method |
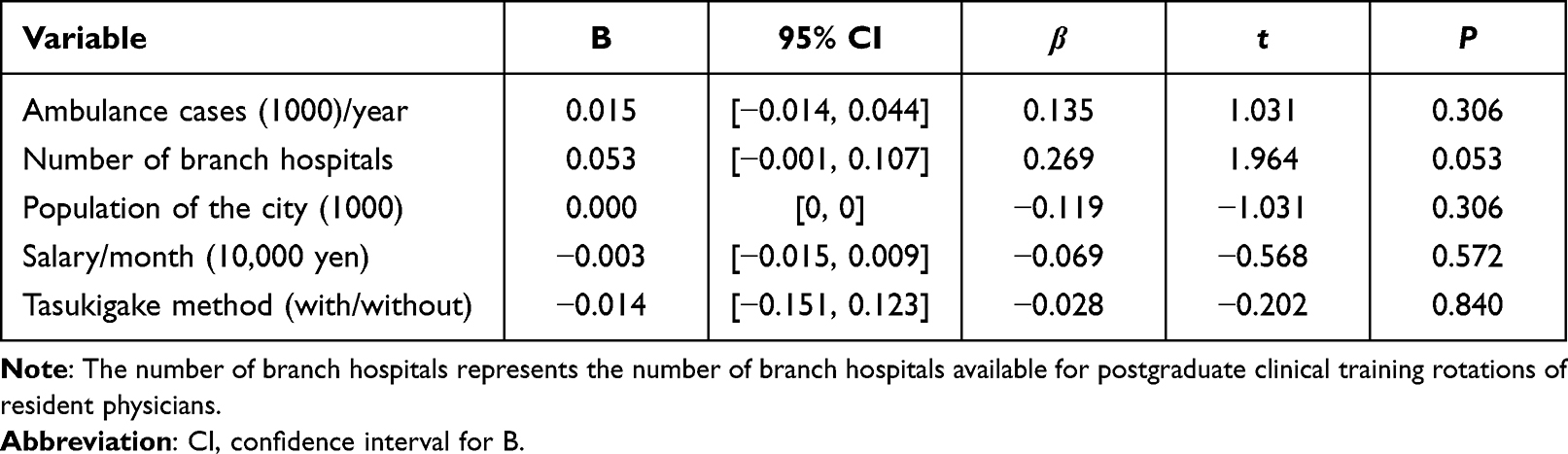 |
Table 4 Regression Coefficients for the Matching Rate (Popularity) for the Residency Program |
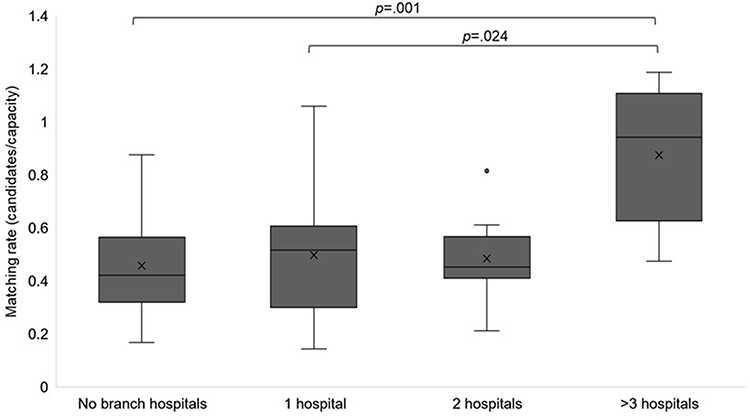 |
Figure 2 Matching rate (popularity) based on the hospital branch number. |
Discussion
This study examined the implementation of the Tasukigake method as a postgraduate clinical training program and the characteristics of hospitals in which the programs were implemented, as well as their associations with the popularity of the clinical training program in Japan. To the best of our knowledge, studies regarding clinical training programs using the Tasukigake method have not been investigated previously in Japan. The results showed that the majority of university hospitals implemented the Tasukigake method, but more public than private university hospitals and hospitals without branch hospitals implemented the Tasukigake method. Moreover, the hospitals that implemented the Tasukigake method had certain characteristics, such as lower hiring capacity, lower popularity, fewer ambulance cases per year, higher city populations, and higher monthly salaries.
These results suggest that public university hospitals with less activity in education for postgraduate physicians in the emergency department in highly populated areas, possibly smaller-scale hospitals, are more likely to implement the Tasukigake method for postgraduate clinical training programs. Despite the slightly debatable roles of university hospitals in recent years due to the patient concentration in university hospitals,22,23 the missions are as follows: (i) to act as educational institutions for the training of physicians; (ii) to be research institutions that conduct research and development of novel medical technologies; and (iii) to be regional core medical institutions that provide advanced medical care.24 Moreover, most of these university main hospitals are certified as special functioning hospitals,25 which provide advanced medical care, develop/assess advanced medical technologies, and conduct advanced medical care training.26
In contrast, the MHLW defines the goal of postgraduate clinical training in the guidelines, including fundamental values as physicians (professionalism), competencies and capabilities, symptomatology, clinical reasoning, and knowledge of diseases that junior residents should experience treating during the 2-year clinical training from the perspective of a generalist.6 These diseases listed in the guidelines are rather common diseases, such as hypertension, dyslipidemia, heart failure, renal failure, lung cancer, asthma, dementia, and depression, as well as emergency medical care rather than advanced medicine. For junior residents to have experience with all of those common diseases, training hospitals must have a high ambulance acceptance rate as well as treat patients with common diseases listed in the guidelines.6 In our opinion, the disparity between the hospital roles listed above and goals for junior residents, especially for highly advanced and specialized hospitals in metropolitan areas, lead to Tasukigake method implementation to supplement common disease cases along with emergency medical care, thereby explaining why university hospitals with fewer ambulance cases implement the Tasukigake method. Internationally, postgraduate medical education programs have a tendency to integrate multidisciplinary clinical training. A number of studies have shown that early practical training in clinical rotation programs for postgraduate trainees may be associated with improved medical knowledge, improved attitudes toward patients, confidence in delivering medical care, and improved clinical performance.27–31
Reportedly, junior residents working for community hospitals score higher than those working for university hospitals on the General Medicine In-Training Examination (GM-ITE),32 which assesses junior residents’ medical knowledge,33 indicating that junior residents can learn more from clinical cases in early phases32 because community hospitals primarily provide care to as many local residents as possible. In addition, factors related to the GM-ITE high score were rotation in the general medicine department,34 more admitted patients to care for,35 and receiving clinical training in rural areas.33 Although certain factors, such as ambulance cases/year, population of the city, the prefecture,36 and the monthly salary,37 correlated with the junior-resident prospects preferences, university hospitals might not be able to change some of those conditions. Remarkably, a questionnaire survey conducted by the MHLW for physicians who completed clinical training in 2019 revealed that highly specialized medicine, an advanced facility, and the equipment or a future diploma were not the main reasons to choose training hospitals by most physicians; instead, substantial programs, quality of supervisors, and the number of clinical cases they could experience were the top reasons for selecting hospitals.38 Furthermore, the number of branch hospitals significantly associated with Tasukigake method implementation, suggesting that university hospitals with branch hospitals have their own network with community hospitals that functions in a manner similar to the Tasukigake method to supplement common clinical cases and emergency medical cases.
Generally, highly populated areas have numerous clinics and hospitals,39 enabling university main hospitals in such areas to be highly specialized and research oriented. Conversely, university hospitals in low-population areas have various roles40 because of the lack of clinics and hospitals or even physicians, resulting in the university hospitals treating many more clinical cases, including common and emergency cases. In addition, the multiple linear regression analysis for popularity in this study revealed that the number of branch hospitals was almost significantly associated with program popularity (P = 0.053), suggesting that medical students seek uniform education with diverse clinical cases. In Japan, the education system in many medical schools and training hospitals follows the “Yanegawara (tiled roof) education” approach, wherein supervisors teach senior residents, senior residents teach junior residents, junior residents teach clinical clerkship students, and clinical clerkship students teach students in early-exposure training classes, making it easier to cultivate teacher- and apprentice-like mentorships. This approach could also lead medical students to seek training within network hospitals, which are university hospitals with branch hospitals rather than university hospitals without branch hospitals.
Overall, these findings suggest that highly specialized university hospitals in metropolitan areas with fewer branch hospitals implemented the Tasukigake method to supplement the fewer case numbers, such as for common cases or emergency cases, to attract excellent resident prospects, whereas private university hospitals or university hospitals in rural areas can fulfill the requirements within their network as well as offer uniform education. Training medical students to become competent physicians and the adequacy of physician supply are vital to maintain a healthy society,41 especially for a country like Japan with a rapidly aging population. Thus, our study indicates two necessary components for training of residents: (i) university hospitals that serve as educational institutions, research institutions, and that practice highly advanced medicine and (ii) community hospitals providing health care to as many local residents as possible and training of those who treat those residents. Both of these components supplement each other. Differences regarding time, location, community and other demographic factors all produce diverse needs for healthcare and medical personnel. This matching system could help facilitate the matching of both hospitals’ needs and future physicians’ needs, rather than relying on a simple calculus of points and scores. To keep up with the ever-changing needs of society, educators and educational institutions should prepare better suited cooperative training hospitals based on researching medical students’ needs, eg, using questionnaires, and offer more choices that meet the area’s needs as well as medical students’ needs. We believe that researching future physicians’ needs and offering more choices can be beneficial to both local residents as well as resident physicians, and attract more suitable students to the area’s needs, resulting in more effective training programs.
To the best of our knowledge, this is the first study to focus on Tasukigake method implementation of postgraduate clinical training using a complete list of medical universities in Japan. However, this study also had several limitations. First, although the study used a complete list of all Japanese medical universities, there are only 82 medical schools in Japan; thus, the total sample size was relatively small. We did not calculate a sample size because the data from all medical schools in Japan, except from defense medical colleges, were used in this study. Second, there might be other factors that could have an effect on reputation or popularity of the programs. We used publicly available data as variables in this study; hence, we could not include variables, such as the advertisement costs of each hospital. Third, restrictions on hospital tours for resident prospects owing to the COVID-19 pandemic, cancellation of training hospital briefing sessions, and restrictions on movement across prefectures might have affected factors to evaluate popularity. Thus, a prospective study and further analysis of more detailed information on the training programs of each university hospital are needed in the future.
Conclusion
The study results suggest that although Tasukigake method implementation is not associated with the program’s popularity, highly specialized university hospitals in metropolitan areas with fewer branch hospitals are more likely to implement the Tasukigake method to supplement common clinical cases to attract resident prospects. More diverse choices for junior-resident prospects will allow junior residents to encounter various common diseases and a variety of situations while learning the role of medicine and health care in society. To meet diverse educational needs as well as personnel needs, educators and educational institutions should prepare better suited cooperative training hospitals based on researching medical students’ needs, eg, using questionnaires, and offer more choices that meet the area’s needs as well as medical students’ needs. This could lead to more attractive and more effective training programs.
If utilized effectively, the Tasukigake method could supplement and reinforce the postgraduate clinical training system to better meet the needs of a healthy society.
Data Sharing Statement
The corresponding author will respond to inquiries on data analyses.
Ethics Approval and Informed Consent
This study did not include research on human participants, so it was exempted from approval and informed consent by the Ethics Review Board.
Acknowledgments
The authors thank Enago for the English language review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors acknowledge that all those entitled to authorship are listed as authors.
Funding
This study has not received any funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Muroya S, Ohde S, Takahashi O, Jacobs J, Fukui T. Differences in clinical knowledge levels between residents in two post-graduate rotation programmes in Japan. BMC Med Educ. 2021;21(1):226. doi:10.1186/s12909-021-02651-6
2. Ministry of Health LaW. History of clinical resident training system. Available from: https://www.mhlw.go.jp/english/wp/wp-hw3/dl/2-055.pdf.
3. Japan residency matching program. Available from: https://www.jrmp.jp/.
4. Teo A. The current state of medical education in Japan: a system under reform. Med Educ. 2007;41(3):302–308. doi:10.1111/j.1365-2929.2007.02691.x
5. Ministry of Health Law. History of post graduate clinical training system (in Japanese). Available from: https://www.mhlw.go.jp/topics/bukyoku/isei/rinsyo/hensen/.
6. Ministry of Health Law. Objectives, strategies, and evaluation in residency training. Available from: https://www.mhlw.go.jp/content/10800000/000719078.pdf.
7. Kozu T. Medical education in Japan. Acad Med. 2006;81(12):1069–1075. doi:10.1097/01.ACM.0000246682.45610.dd
8. Agency HI. Hospitals popularity ranking (in Japanese); 2020. Available from: https://hospia.jp/wp/archives/287.
9. The result of Japanese residency matching programme (in Japanese); 2021. Available from: https://www.mhlw.go.jp/content/10803000/000559449.pdf.
10. St Claire KM, Rietcheck HR, Patel RR, Dellavalle RP. An assessment of social media usage by dermatology residency programs. Dermatol Online J. 2019;25:1.
11. McHugh SM, Shaffer EG, Cormican DS, Beaman ST, Forte PJ, Metro DG. Use of social media resources by applicants during the residency selection process. J Educ Perioper Med. 2014;16(5):E071.
12. Role of university hospitals (in Japanese). Available from: https://www.mext.go.jp/b_menu/shingi/chousa/koutou/009/toushin/970701.htm#02.
13. Nomura K, Inoue S, Yano E. The shortage of pediatrician workforce in rural areas of Japan. Tohoku J Exp Med. 2009;217(4):299–305. doi:10.1620/tjem.217.299
14. Sakai R, Wang W, Yamaguchi N, Tamura H, Goto R, Kawachi I. The impact of Japan’s 2004 postgraduate training program on intra-prefectural distribution of pediatricians in Japan. PLoS One. 2013;8(10):e77045. doi:10.1371/journal.pone.0077045
15. Ono K, Hiratsuka Y, Murakami A. Geographical distribution of ophthalmologists before and after the New Postgraduate Training Program in Japan. Ophthalmic Epidemiol. 2010;17(2):125–130. doi:10.3109/09286581003624988
16. Koike S, Ide H, Yasunaga H, Kodama T, Matsumoto S, Imamura T. Postgraduate training and career choices: an analysis of the National Physicians Survey in Japan. Med Educ. 2010;44(3):289–297. doi:10.1111/j.1365-2923.2009.03582.x
17. Ministry of Health. LaW. Residency electronic information system (in Japanese). Rights Transferred to Local Government. Available from: https://www.iradis.mhlw.go.jp/.
18. PMET. Foundation for promotion of medical training (in Japanese). Available from: https://www.pmet.or.jp/.
19. Postgraduate clinical training matching system interim report data (academic year) (in Japanese); 2020. Available from: https://jrmp2.s3.ap-northeast-1.amazonaws.com/chukan/2020chukan.pdf.
20. Communications MoIAa. View data municipality data. System of Social and Demographic Statistics (SSDS). search by areas portal site of official statistics of Japan. Available from: https://www.e-stat.go.jp/en/regional-statistics/ssdsview/municipality.
21. Ministry of Education. C, sports, science and technology. University hospitals web pages (in Japanese). Available from: https://www.mext.go.jp/a_menu/koutou/iryou/1337441.htm.
22. Ministry of Health LaW. Prevention of the concentration of patients in large hospitals. Available from: https://www.mhlw.go.jp/content/12401000/000607031.pdf.
23. Hong du P, Song J. The effective distribution system for the concentration of patients to extra-large hospitals. J Korean Surg Soc. 2011;80(6):373–383. doi:10.4174/jkss.2011.80.6.373
24. Ministry of Education. Culture, Sports, Science and Technology (MEXT) (in Japanese). Available from: https://www.mext.go.jp/b_menu/shingi/chukyo/chukyo4/gijiroku/attach/1415436.htm.
25. Ministry of Health. LaW. List of special functioning hospitals (in Japanese). Available from: https://www.mhlw.go.jp/content/10800000/000930284.pdf.
26. Ministry of Health LaW. Special functioning hospitals regional medical care support hospitals (since 1997). Available from: https://www.mhlw.go.jp/english/wp/wp-hw4/dl/health_and_medical_services/P40.pdf.
27. De Witt C, Smit I, Jordaan E, Koen L, Niehaus DJH, Botha U. The impact of a psychiatry clinical rotation on the attitude of South African final year medical students towards mental illness. BMC Med Educ. 2019;19:114. doi:10.1186/s12909-019-1543-9
28. Mohan S, Follansbee C, Nwankwo U, Hofkosh D, Sherman FS, Hamilton MF. Embedding patient simulation in a pediatric cardiology rotation: a unique opportunity for improving resident education. Congenit Heart Dis. 2015;10:88–94. doi:10.1111/chd.12239
29. Zaorsky NG, Malatesta TM, Den RB, et al. Assessing the value of an optional radiation oncology clinical rotation during the core clerkships in medical school. Int J Radiat Oncol Biol Phys. 2012;83:e465. doi:10.1016/j.ijrobp.2012.01.058
30. Ahmed NN, Farnie M, Dyer CB. The effect of geriatric and palliative medicine education on the knowledge and attitudes of internal medicine residents. J Am Geriatr Soc. 2011;59:143–147. doi:10.1111/j.1532-5415.2010.03235.x
31. Johnson GA, Pipas L, Newman-Palmer NB, Brown LH. The emergency medicine rotation: a unique experience for medical students. J Emerg Med. 2002;22:307–311. doi:10.1016/S0736-4679(01)00497-8
32. Nishizaki Y, Nozawa K, Shinozaki T, et al. Difference in the general medicine in-training examination score between community-based hospitals and university hospitals: a cross-sectional study based on 15,188 Japanese resident physicians. BMC Med Educ. 2021;21(1):214. doi:10.1186/s12909-021-02649-0
33. Shimizu T, Tsugawa Y, Tanoue Y, et al. The hospital educational environment and performance of residents in the general medicine In-training examination: a multicenter study in Japan. Int J Gen Med. 2013;6:637–640. doi:10.2147/IJGM.S45336
34. Nishizaki Y, Shimizu T, Shinozaki T, et al. Impact of general medicine rotation training on the in-training examination scores of 11, 244 Japanese resident physicians: a Nationwide multi-center cross-sectional study. BMC Med Educ. 2020;20(1):426. doi:10.1186/s12909-020-02334-8
35. Mizuno A, Tsugawa Y, Shimizu T, et al. The impact of the hospital volume on the performance of residents on the general medicine in-training examination: a multicenter study in Japan. Intern Med. 2016;55(12):1553–1558. doi:10.2169/internalmedicine.55.6293
36. Nishizaki Y, Ueda R, Shinozaki T, Tokuda Y. Hospital characteristics preferred by medical students for their residency programs: a nationwide matching data analysis. J Gen Fam Med. 2020;21(6):242–247. doi:10.1002/jgf2.370
37. Enari T, Hashimoto H. Does salary affect the choice of residency in non-university teaching hospitals? A panel analysis of Japan Residency Matching Programme data. Hum Resour Health. 2013;11:12. doi:10.1186/1478-4491-11-12
38. Summary of questionnaire survey results for those who completed clinical training in 2019 (in Japanese). Available from: https://www.mhlw.go.jp/content/000744938.pdf.
39. Ministry of Health LaW. Portal site of official statistics of Japan, e-stat. Available from: https://www.e-stat.go.jp/stat-search/files.
40. Ogawa A. The role of the university hospital in the community medicine (in Japanese). Clin Exp Med. 2009;228(3):254–258.
41. Macinko J, Starfield B, Shi L. Quantifying the health benefits of primary care physician supply in the United States. Int J Health Serv. 2007;37(1):111–126. doi:10.2190/3431-G6T7-37M8-P224
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.