")
Back to Journals » Infection and Drug Resistance » Volume 16
Characteristics of TB/HIV Co-Infection and Patterns of Multidrug-Resistance Tuberculosis in the Northwest Amhara, Ethiopia
Authors Seid A , Girma Y, Abebe A, Dereb E, Kassa M, Berhane N
Received 31 March 2023
Accepted for publication 12 June 2023
Published 16 June 2023 Volume 2023:16 Pages 3829—3845
DOI https://doi.org/10.2147/IDR.S412951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Aynias Seid,1,2 Yilak Girma,3 Ayenesh Abebe,3 Eseye Dereb,3 Meseret Kassa,3 Nega Berhane2
1Department of Biology, College of Natural and Computational Science, Debre-Tabor University, Debre-Tabor, Ethiopia; 2Department of Medical Biotechnology, Institute of Biotechnology, University of Gondar, Gondar, Ethiopia; 3TB Culture Laboratory, University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia
Correspondence: Aynias Seid, Email [email protected]
Background: Multidrug-resistant tuberculosis (MDR-TB) has continued to be a serious public health threat and significantly challenges global TB control and prevention efforts, where the TB/HIV co-infection epidemic makes the situation much worse. The aim of the study was to determine the determinant factors associated with patterns of MDR-TB among pulmonary TB patients in the Northwest Amhara, Ethiopia.
Methods: A hospital-based cross-sectional study was conducted from May 2022 to February 2023 in the Northwest Amhara, Ethiopia. Data on the participants’ socio-demographics and clinical characteristics were obtained using a pre-tested checklist. Phenotypic susceptibility testing to first-line anti-TB drugs was performed on 180 isolates by automated BD BACTEC MGIT 960 system. Logistic regression analysis was performed to determine the association of risk factors with patterns of MDR-TB. A p-value ≤ 0.05 was considered statistically significant.
Results: The overall proportion of TB with HIV co-infected cases was 19.8% (50/252). Culture positivity was confirmed in 203/252 (80.6%) of sputum samples. Among 168 isolates, the DST showed that 119 (70.8%) isolates were pan-susceptible to all first-line drugs and prevalence of any resistance to first-line drugs was 49,168 (29.2%). Among the resistant isolates, 28 (16.7%) were any mono-resistance and 12 (7.1%) were determined to be resistant to MDR-TB. TB with a previous TB treatment (aOR = 6.73, 95% CI: 1.78– 25.47, p = 0.005) and HIV co-infected (aOR = 0.252, 95% CI: 0.73– 0.875, p = 0.03) were significantly associated with MDR-TB.
Conclusion: Higher prevalence of TB and MDR-TB was examined among TB patients in the study area. In the study, history of previous TB treatment was the strongest risk factor MDR-TB infection followed by TB with HIV co-infected cases. Therefore, there is a need of strengthening TB control and prevention programs to reduce the increase of TB incidence, further emergence and transmission of a public health threat of MDR-TB cases.
Keywords: drug resistance, MDR-TB, prevalence, risk factors, TB/HIV co-infection
Introduction
Tuberculosis (TB) is a communicable contagious disease caused by a single infectious agent, the Mycobacterium tuberculosis (M. tuberculosis) complex strain. It is the most prevalent opportunistic bacterial infection. According to the World Health Organization (WHO) Global TB Report 2022, there were an estimated 10.6 million (9.9–11 million) cases of TB worldwide in 2021, of which 6.7% were TB/HIV co-infected cases, an increase of 4.5% from the estimates of 10.1 million (9.5–10.7 million) in 2020; 1.6 million deaths (1.4 million among HIV-negative individuals and 187, 000 among HIV-positive individuals); and close to 141, 953 multidrug-resistant (MDR-TB) cases (defined as TB resistant to the two most effective first-line anti-TB drugs called isoniazid (INH) and rifampicin (RIF)) in 2021,1 an increase by 6.4% in 2020.2 The highest incidence of TB cases in 2021 was among South-East Asia (45%) WHO area followed by Africa (23%). Ethiopia is one of the 30 global lists of high-burden countries for TB and HIV-associated TB, but transitioned out of MDR-TB list.1 The current effective global TB control approach is based on an early diagnosis and sufficient treatment regimens using anti-TB medications globally.1 Nonetheless, the emergency and spread of drug resistance such as MDR-TB remains one of the ongoing problems in the global TB control campaign.3 The extent of occurrence of drug-resistant TB including MDR-TB and its burden varies significantly from country to country and from region to region but is high in resource-poor countries.4 The emergency of MDR-TB arises from spontaneous chromosomal resistance-conferring mutations at a low frequency, and they can be transmitted directly from one person to another by resistant bacteria that possess these variants.5 Besides, the majority of drug-resistant strains are also acquired by environmental exposure due to physician error including selection pressure brought on by inappropriate anti-TB drug prescriptions, poor diagnostic capabilities or insufficient infrastructure in healthcare facilities, inadequate treatment follow-up, improper management of TB control programs, and poor patient compliance.6–8
TB/HIV co-infection is also the main significant risk factor for developing MDR-TB infection. The co-infection of TB with HIV is considered to be the human deadliest “syndemic” disease, that act upon one another synergistically to magnify the burden of the disease.9,10 This co-infection may impair the host’s immune responses to both diseases and the pharmacokinetics of TB medications,11 make clinical diagnosis more difficult, lengthen the time it takes for TB treatments to be effective by increasing the bacilli load, and lead to MDR-TB in those who have it.12 The TB burden is highly concentrated in resource-limited settings mainly in Asia and African countries including Ethiopia, where the prevalence of TB/HIV twin epidemic was highest.1,13 The risk of TB is now elevated 15–22 times more likely in HIV co-infected cases than HIV-negative,9 when the immunological effect of HIV on CD4 cell count remains high. Thus, it is recommended that all patients with active or latent TB undergo HIV testing and begin antiretroviral therapy (ART) to increase absolute CD4 cell counts in to stop the spread of any other opportunistic infections.11
In Ethiopia, the rise of drug resistant TB including MDR-TB continuing to pose a serious threat to public health14,15 and is interfering with the country’s overall TB control and prevention strategy.16 Despite newer modalities for diagnosis and treatment, people are still suffering from this disease. However, there was limited information on the evolutionary patterns of MDR-TB in the TB/HIV twin epidemic condition in the study area. Investigating the patterns and proportion of MDR-TB in the context of HIV co-infection has contributed a significance role for reducing the emergency and transmission of TB infection. Moreover, the well-known drug-resistance profile is kept to aid with the challenges of co-treating TB with HIV and to offer an epidemiological indicator to measure the dissemination of resistant bacteria in the community. This study aimed to characterize the epidemiological situation and patterns of drug resistance of M. tuberculosis strains isolated from newly diagnosed pulmonary TB patients in the high-TB-burden area of the Northwest Amhara, Ethiopia.
Methods and Materials
Study Area, Period and Design
A hospital-based cross-sectional study was conducted in the Northwest Amhara, Ethiopia, from May 2022 to February 2023. This study was carried out at six selected governmental hospitals in the region (Figure 1), which include the University of Gondar Comprehensive Specialized Hospital (UoGCSH) in the Central-Gondar Zone of Gondar town; the Felege-Hiwot Specialized Hospital (FHSH) and Tibebe-Giwon Specialized Hospital (TGSH) in the West-Gojam Zone of Bahir-Dar town; the Debre-Tabor Comprehensive Specialized Hospital (DTCSH) in the South-Gondar Zone of Debre-Tabor town; the Metema General Hospital (MGH) in the West-Gondar Zone of Metema town; and the Debark General Hospital (DGH) in the North-Gondar Zone of Debark town, which are located 727, 566, 667, 924 and 847 km far away from Addis Ababa, the capital city of Ethiopia, respectively.
 |
Figure 1 Map of the study area. |
Presently, all the study site hospitals were selected based on the availability of baseline GeneXpert® MTB/RIF diagnostic tools during the study period. Moreover, these hospitals provided drug-resistant TB treatment follow-up care services and TB diagnostic services for other nearby primary health centers that do not have a GeneXpert® MTB/RIF test. Until the start of the study, UoGCSH was the only hospital to provide TB culture, phenotypic, and molecular-based susceptibility testing. The Amhara area, one of Ethiopia’s 13 regions, is situated in Northwestern Ethiopia between 36°20′ and 40°20′ E longitude and 9°20′ and 14°20′ N latitude. According to the central statistics agency (CSA) of Ethiopia’s 2015 census, the region has an estimated area of 154,708.96 km2 and a total population of 20,018,988 of which the study area has a total area of 146,705.14 km2 and a population of 7,086,962 people.17
Source of Population and Study Participants
All newly registered pulmonary TB suspected cases (new or re-treated cases) with suggestive signs and symptoms who visited the study site hospitals in the Amhara region during the study period were the source of population. GeneXpert-positive pulmonary TB patients with HIV-positive and/or HIV-negative who were volunteered to participate in the study were enrolled as study participants. A “new case” of TB was defined as a newly registered TB patient with signs and symptoms, and who has never had a treatment regime for TB or who has received it for less than one month, while a “re-treated case” of TB was defined as a newly registered TB patient with a history of more than 30 days of an anti-TB treatment regime.
Sample Size Determination and Sampling Technique
The study participant sample size was determined using a single population proportion formula, n = z2p (1-p)/d2.18 The minimum required number of GeneXpert-positive pulmonary TB patients living with HIV co-infection and/or HIV-negative (n), the standard normal distribution value at 95% confidence interval (95% CI), which is 1.96 (z), and the previous pooled prevalence of TB/HIV co-infection in the Amhara region of Ethiopia (20%) at 95% CI (p), as defined by Teweldemedhin et al,19 5% margin error (d), and 5% non-response rate were all taken into consideration. A total of 259 GeneXpert-positive cases of pulmonary TB with HIV-positive and HIV-negative were included in the study. During the designated study period, a convenient sampling technique was used to enroll eligible study participants until the necessary sample size was achieved at the study site hospitals. A unique personal identification was given to each patient who agreed to participate in the study. They were also informed that they had the opportunity to withdraw from the study at any point while the data was being collected.
Inclusion and Exclusion Criteria
The newly recorded GeneXpert-positive hospitalized pulmonary TB patients’ who were 18 years of age, who were not received TB treatment follow-up services at the time of sample collection, who were willing to provide a face-to-face interview and signed written informed consent were included in study. Suspected TB patients with a negative Xpert MTB/RIF, poor quality sputum samples from pulmonary TB patients, critically ill pulmonary TB patients who may have impacted on the socio-demographic data and sputum quality and extra-pulmonary (EPTB) cases were excluded from the study.
Study Variables
The exhaustive study of patient’s information on the socio-demographic (ie, sex, age, religion, place of residence, marital status, and history of contact with active-TB cases), clinical (ie, TB/HIV co-infection status, previous TB treatment history), and behavioral (ie, window opening, alcohol intake, cigarette smoking, and status of Khat chewing) characteristics were considered as independent variables as well as the distribution patterns of drug-resistance in M. tuberculosis clinical isolates was a dependent variable.
GeneXpert® MTB/RIF Assay
All the suspected TB patients attending hospitals in the study sites during the study period were provided a primary 4 mL “on-The-spot” sputum sample for clinical pulmonary TB diagnosis using GeneXpert® MTB/RIF assay according to the WHO implementation manual and the manufacturer’s instructions.20 Briefly, a 1:2 ratio was used to mix the collected 2 mL of sputum with 4 mL of commercially prepared sample reagent (SR). The homogenized, diluted sample was incubated for 15 minutes at room temperature. A pre-labeled test cartridge was then filled with 2–3 mL of each treated sputum mixture, scanned with a barcode reader, and fed into the GeneXpert® MTB/RIF equipment for testing. The GeneXpert® MTB/RIF assay then identified isolates of the M. tuberculosis complex and RIF-resistance. Following the national MoH and GLI standard guidelines, sputum samples were then stained using Ziehl-Neelsen’s (ZN) method for the isolation of acid-fast bacilli (AFB) mycobacterium colonies.21,22
HIV Testing
HIV counseling and testing were performed for TB patients at the study hospitals during the study period. On the sputum examination request document, the study’s TB patients who also had HIV co-infection status were noted. Participants were given an HIV/AIDS diagnosis after giving their consent if they had never been tested for the condition. The HIV testing was carried out using SD BIO LINE® HIV 1/2 3.0 rapid test (Standard Diagnostics, INC).23,24 A 50 µL of freshly collected blood was placed on the HIV test strip’s sample pad, allowed to freely diffuse into the strip, and then left at room temperature for 15 minutes. The control and patient portions of the strip’s corresponding color changes were used to read the test findings.
Sputum Sample Collection and Pre-Processing
Following the use of GeneXpert® MTB/RIF to confirm pulmonary TB cases, single 5–10 mL new “morning” sputum samples were collected by trained laboratory technologists at each hospital using properly labeled 50 mL screw cap disposable falcon tubes by following Ethiopian MoH and GLI guidelines.21,22 To prevent the mycobacteria from losing viability, all of the collected sputum samples were temporarily refrigerated at −20 °C, carefully packed, and kept in a cool box while being transferred to the UoGCSH TB culture laboratory, Gondar, within 4–5 days after collection. Upon arrival, sputum samples were pre-treated immediately using an equal volume of N-Acetyl-L-Cysteine/sodium-hydroxide (NALC/NaOH) technique with a final 2% NaOH concentration according to the manufacturer’s instructions as described by Kubica et al.25 Notably, the quality of the sputum samples was determined by direct Gram-staining smear microscopy as described previously,26,27 based on the minimum number of squamous epithelial cells (SCE) per a low power field (LPF) of view (10x). Sputum smear having an average number of <10 SCE per LFP was considered good quality, while ≥10 SCE per LFP was poor quality and were rejected, which indicates that the sputum was contaminated with saliva. A good-quality sputum sample was cleaned, digested with an equal volume of NALC and NaOH, and then transferred into a 50 mL centrifuge sample tube. The suspension tubes were vortexed every 5 minutes until they became liquefied, and then the sample was centrifuged at 3000 rpm for 15 minutes, with the supernatant being discarded. The pellet was centrifuged at 3000 rpm for 15 minutes after being neutralized in 50 mL of phosphate-buffered saline (PBS, pH 6.8).
Mycobacterium Culturing and Identification of Isolates
A processed sputum was then inoculated into Lowenstein-Jensen (LJ) egg media containing 0.6% glycerol at 37 °C for up to 8 weeks.22 Briefly, a 200 μL of processed suspension was inoculated on two sterile LJ mediums by distributing over the entire surface or into MGIT 960 vials. Primary identification of mycobacteria was carried out based on the culture’s growth, characteristic of colony morphology and color, which are slow-growing (not earlier than 3–4 weeks of incubation), waxy, non-pigmented (buff in color), rough, crumbly, or resembling breadcrumbs on LJ solid culture. Mycobacterial cultures were considered “positive” when the growth of colonies was seen after the second week of incubation, while “negative” when no colonies were seen after a maximum week of incubation. The primary identification of strains included microscopic confirmation of the acid-fast bacilli (AFB) mycobacterium colonies were determined using Ziehl-Neelsen’s (ZN)-staining by following the national MoH and GLI standard guidelines.21,22 According to the manufacturer’s instructions, immunochromatographic SD BIOLINE TB Ag MPT64 Rapid® test (Standard Diagnostics, Inc. South Korea)28 was used for the identification of M. tuberculosis complex clinical isolates from non-tuberculosis mycobacteria (NTM) species. The test was applied to samples cultured on LJ solid media. A sample of 2 to 3 loopful colonies was scraped and suspended in 200 μL of extraction buffer. A sample of 100 μL of this suspension was then applied to the test device and incubated at room temperature for 30 minutes. The presence of two colored bands “T” and “C” in the result strip indicated a positive result.
Antimicrobial Agents Solution Preparation
All of the first-line anti-TB drugs, including streptomycin (STR), isoniazid (INH), rifampicin (RIF), and ethambutol (EMB), were purchased from Sigma-Aldrich in chemically pure powder form. The powders were kept at −20 °C. The lyophilized stock solutions (µg/mL) of STR, INH, RIF, and EMB anti-TB drugs were prepared in 4 mL of sterile deionized water. All stock solutions were sterilized by 0.2 μm membrane filter units. Small aliquots of each stock solution were kept at −20 °C until use. To obtain the appropriate critical concentrations (CCs) of drugs in the BBL Mycobacteria Growth Indicator Tube (MGIT) tube, the working solution was freshly made from the stock solutions. After thawing, the solutions were immediately used, and the leftovers were thrown away.
MGIT Sub-Culturing
Before being assessed for susceptibility testing, among all LJ-grown mycobacteria, MGIT sub-cultures were performed in liquid medium using BACTEC MGIT 960 tubes (BD Diagnostics, Sparks, MD, USA) at 37 °C for a maximum of 42 days by monitoring once weekly for mycobacterial colony growth29,30 for better yield. A sterile loop was used to scrape up 1–2 loopful colonies from the active stage of positive LJ growth (1–2 weeks) to prepare the bacterial culture suspensions. The colonies were suspended in a sterile tube measuring 16.5×128 mm and covered with a saline-filled cap. The bigger clumps in the bacterial suspensions were broken up by vigorous vortexing for 2–3 minutes, and the mixture was then allowed undisturbed for 20–30 minutes to allow the sediment to settle to the tube’s bottom. The suspensions were then allowed to stand for a further 15 minutes after the supernatant fluids were transferred to another sterile tube without transferring any sediment. A 1.0 McFarland standard was applied to the bacterial suspensions. After that, 0.5 mL adjusted inoculums were transferred into a 7 mL BBL MGIT tube with 4 mL of MGIT growth supplement and MGIT PANTA (an antibiotic mixture of Polymyxin B, Amphotericin B, Nalidixic Acid, Trimethoprim, and Azlocillin) following the manufacturer’s instructions. To obtain the positive MGIT seed, the suspension tubes were cultured for a week. The MIGT seed tube was vortexed for one minute and then let to settle for 15 to 20 minutes. The inoculums were simply used for the MGIT 960 testing tubes for the MGIT-positive seeds that were between one and two days old as well as the growth control (GC) serial dilutions of 1:100 (1% GC) was made by mixing 0.1 mL of the MGIT seed with 9.9 mL of sterile saline. Nevertheless, 1:5 dilution of suspensions were created for MGIT seeds that were 3–5 days old by mixing 1 mL of positive MGIT seeds with 4 mL of sterile saline, whereas the GC serial 1:100 dilution culture suspensions were made by mixing 0.1 mL of the 1:5 dilution with 9.9 mL of sterile saline. By gently flipping the mixtures 4–5 times, the GC suspensions were well blended.31,32
Phenotypic Drug Susceptibility Testing (DST)
An automated BACTEC MGIT 960 growth detection method (BD, Sparks, MD, USA) was used to perform culture-based phenotypic drug susceptibility testing (DST) on four first-line anti-TB drugs (STR, INH, RIF, and EMB). The critical concentrations (CCs) of drugs for STR 1.0 µg/mL, INH 0.1 µg/mL, RIF 1.0 µg/mL, and EMB 5.0 µg/mL were utilized as recommended by GLI and WHO22,33 by following to manufacturer’s instruction. An antibiotic susceptibility testing (AST) set and TB exit, which includes one GC MGIT tube and one MGIT tube for each tested anti-TB drug along with the specimens, were used to conduct the susceptibility test. Briefly, the four first-line drugs (using SIRE kit) were labeled on four 7 mL MGIT 960 tubes, and a GC tube was on one of the tubes. For each test M. tuberculosis clinical isolate, all MGIT tubes were inserted in the five-tube AST set carrier, going from left to right (GC, S, I, R, E). The MGIT 960 SIRE supplements were then aseptically added to each of the MGIT 960 DST tubes at a volume of 0.8 mL. Thereafter, using different micropipette tips for each drug under test, 0.1 mL appropriately reconstituted drug working solutions were added into each of the marked MGIT 960 tubes. Then, using a different pipette, 0.5 mL of the thoroughly blended culture suspensions were inoculated into MGIT 960 DST tubes containing each anti-TB drug. To compare growth, 0.5 mL of the 1:100 GC suspensions was concurrently added to the identical specimen’s MGIT 960 drug-free control tube. After securing the tube caps, the inoculated broth was thoroughly mixed by gently inverting the tube a few times. Finally, the automated BACTEC MGIT 960 system (Becton Dickinson, Franklin Lakes, NJ, and USA) was loaded with the AST carriers containing the inoculated MGIT 960 DST tubes using the susceptibility test set entry feature and incubated at 37 °C as directed by the manufacturer until the MGIT 960 instrument flagged positively.22,33
Based on the relative growth ratio of the tested M. tuberculosis clinical isolates between the drug-containing tube and drug-free GC tube when the GC tube reached a 400-growth unit (GU) within 4–13 days, the software algorithm of the BACTEC MGIT 960 system keeps track of growth (or susceptibility) patterns. The outcomes were categorized automatically as sensitive or resistant. A strain was considered “susceptible” when the GU of the drug-containing tubes of isolates was less than 100, while “resistant” if more than 1% (more than 100) of the test population grew in the presence of the drug’s CCs.22,33
Data Collection Procedure
Using a face-to-face interview and semi-structured questionnaires, trained health workers at each hospital collected the socio-demographic, clinical, and behavioral data from the study participants with their consent. The questionnaires used to gather data were written in English and then translated into Amharic, the native language in the study area. Also, all laboratory data, including the phenotypic first-line drug-resistance patterns, were accurately gathered by the laboratory technicians and/or principal investigator.
Quality Control
The study patients’ personnel data were collected correctly. The data collectors were trained and strictly adhered to the data collection procedures. Standard operating procedures (SOPs) were followed for culture, identification, and susceptibility testing. The standard susceptible M. tuberculosis H37Rv reference strain (ATTCC 27294) was used as a positive quality control strain and molecular water was utilized as the negative control in each batch for all procedures. Before entering data, the investigators carefully verified each day that the data-collecting procedures were accurate and consistent. To reconcile all the available data entered, two individuals performed double data entry.
Data Entry and Statistical Analysis
The data were entered using EpiData version 3.1 and analyzed using SPSS version 23.0. (Statistical Package for the Social Sciences, IBM, Chicago, IL, United States). The study participants were categorized into two groups: pulmonary TB with HIV co-infection as well as those with TB but not HIV co-infection. Descriptive analysis was carried out to measure frequencies and proportions for categorical variables and presented in tables. The mean and interquartile range (IQR of the study participants’ age were assessed. The profiles of drug-resistance TB were determined. A logistic regression analysis was utilized to assess the potential impact of each associated independent variable on the drug-resistance patterns (such as the association of HIV-co-infection with patterns of MDR-TB) while controlling the confounding effects of other parameters. Predictor variables that are significant in bivariate analysis at a cut point of P-value 0.25 were included in the multivariate analysis. Odds ratios (OR) and 95% confidence intervals (CI) were also estimated. A p-value ≤0.05 was considered statistically significant for all variable analysis.
Ethical Considerations
The study was ethically approved by the Institutional Review Board (IRB) of the University of Gondar (UoG) (Ref: VP/RTT/05/829) after reviewing the study proposal. A written letter of support was obtained from the Amhara Public Health Institute (APHI), Bahir Dar branch (Ref: APHI/W/D/03/146). Besides, written and signed informed consent was obtained from each study subject to participate gladly in the study. The privacy rights of study subjects were protected. The authors confirmed that the ethical principle was followed by the Declaration of Helsinki.
Results
Socio-Demographic and Clinical Characteristics of Study Patients
A total of 259 primarily GeneXpert-positive of the 2316 pulmonary TB cases were provided further fresh sputum samples and enrolled in the study based on the inclusion criteria stated. Of which, 252/259 (97.3%) were provided good-quality sputum samples and complete personnel data record entries, while 7/259 (2.7%) were saliva-contaminated samples, mislabeled sample tubes, and incomplete data and were excluded from further laboratory analysis. Of the 252 study participants, 50/252 (19.8%) were known cases of pulmonary TB with HIV-positivity and referred to as the TB/HIV co-infected group, whereas 202/252 (80.2%) had pulmonary TB with HIV-negativity and/or unknown HIV status also known as the TB with HIV uninfected group (Figure 2). TB can affect anyone, regardless of age, sex or ethnicity. The mean age of the study participants was 36 years old (range was 27 to 54), 134/252 (53.2%) were young adults (18–34 years old), and 13/252 (5.2%) were over the age of 65. The TB incidence in males was higher (156/252, 61.9%) than that in females (96/ 252, 38.1%). Of which, the TB/HIV co-infection among male vs female was 33 (66%) vs 17 (34%), respectively. The majority of participants (216/252, 85.7%) had developed new TB cases, whereas 36/252 (14.3%) had a history of previously treated TB cases. There was a highest percentage of new TB cases among HIV-positive (38/50, 76%) vs HIV-negative (178/202, 88%) compared to retreatment TB cases among TB with HIV-positive (12/50, 24%) vs HIV-negative (24/202, 12%) (Table 1).
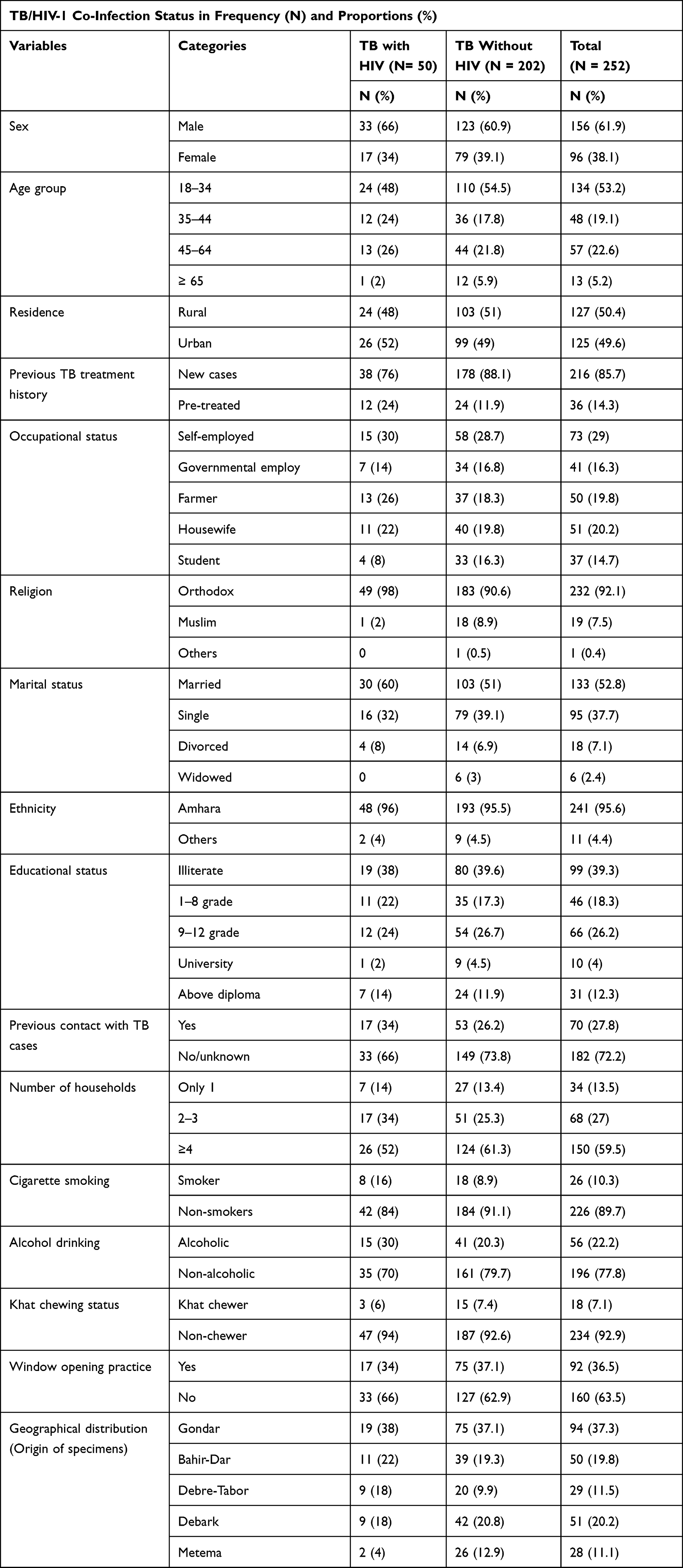 |
Table 1 Characteristics of Study TB Patients by TB/HIV Co-Infection Status (N = 252) |
 |
Figure 2 Flow chart of the laboratory procedure and data collection. Abbreviations: LJ, Lowenstein-Jensen; NTM, non-tuberculosis mycobacteria; MIGT, mycobacteria growth indicator tube; DST, drug susceptibility testing; MDR-TB, multidrug resistant tuberculosis. |
Seventy-three of the study patients (73/252, 29%) were in the self-employed socio-economic category and the most affected followed by housewives (51/252, 20%), farmers (50/252, 19.8%), and government workers (41/252, 16.3%), while 37/252 individuals (14.7%) were still in school. The TB incidence in the urban population (127/252, 50.4%) was slightly similar with the rural areas (125/252, 49.6%), of which (24/50, 48%) and (26/50, 52%) were TB patients with HIV co-infection, respectively. The majority of participants (232/252, 92.1%) were Orthodox followers, 241/252 (95.6%) were from Amhara ethnic group and 99/252 (39.3%) were not educated at all, of which the highest prevalence of TB/HIV co-infected cases 49/50 (98%), 48/50 (96%) and 19/50 (38%) were found, respectively. Of the most affected participants (182/252, 72.2%) had not prior contact with active TB cases, 160/252 (63.5%) had not had a window opening practice, and 150/252 (59.5%) lived together with four or more families (Table 1).
Married individuals accounted for the majority of 133 (52.8%) of the cases followed by 95 (37.7%) single patients, while the least cases, 6 (2.4%) were occupied by widowed participants. The highest rate of respondents 234 (92.9%), 226 (89.7%), and 196 (77.8%) were non-chewers, nonsmokers, and nondrinkers. Of these, it was revealed that there were 47, 42, and 35 incidences of TB patients who were also HIV-positive, respectively. The majority of the samples (94/252, 37.3%) were originated from Gondar town (UoGCSH), followed by Debark (DGH) 51 (20.2%), Bahir-Dar (FHSH & TGSH) 50 (19.8%), Debre-Tabor (DTSH) 29 (11.5%), and Metema (MDH) 28 (11.1%). Of these, 19 (38%), 9 (18%), 11 (22%), 9 (18%), and 2 (4%) patients were found in respective origin order among the 50 TB/HIV co-infected cases (Table 1).
Patterns of Multidrug-Resistance in M. tuberculosis Isolates
As shown in Figure 2, a total of 203 (80.6%) specimens from the 252 samples were culture-positive on LJ media, while 43 (17.1%) samples were produced no growth or negative culture results and 6 (2.4%) were contaminated. Of the 203 culture positive isolates, 196 (96.6%) were identified as M. tuberculosis complex isolates, while 7 (3.4%) were identified as non-tuberculosis mycobacteria (NTM) and were excluded from further laboratory analysis. The phenotypic DST for the first-line drugs was performed on the 180 (91.8%) of the 196 culture-positive M. tuberculosis complex isolates using the BACTEC MIGT SIRE 960 DST system, while 16 (8.2%) were lost their viability after MIGT sub-cultured. One hundred sixty-eight (93.3%) of the 180 M. tuberculosis complex isolates were had successful DST results for the tested first-line drugs, but 12 (6.7%) of them were failed because 5 of them developed before 4 incubated days (overgrowth of x400 error) and 7 did not grow within 13 incubation days (undergrowth) (X200 error). Among the 168 isolates that underwent phenotypic DST evaluation, 101 (60.1%) and 67 (39.9%) isolates were taken from male and female participants’, 144 (85.7%) and 24 (14.3%) were found in new and previously treated TB cases, and 36 (21.3%) and 132 (78.7%) were taken from pulmonary TB patients with HIV co-infected and HIV-negative cases, respectively.
In the study, of the 168 DST performed isolates among TB patients, the highest isolates (119/168, 70.8%) were pan-susceptible to all studied anti-TB drugs and 49/168 (29.2%) were any resistance to at least one or more drugs. Of the overall resistant isolates, the prevalence of MDR-TB isolates was found to be 12/49 (24.5%). The most frequent MDR-TB isolates were resistance to four combined drug STR+INH+RIF+EMB pattern (5/12, 41.7%), followed by isolates with two combined drug RIF+INH (4/12, 33.3%), three combined drug STR+INH+RIF (2/12, 16.7%), and single isolate (8.3%) with three combined drug INH+RIF+EMB resistance pattern. Twenty-eight isolates (28/49, 57.1%) were any mono-resistant to either of drugs. Of them, the highest mono-resistant to drug was observed against STR-mono (15/28, 53.6%), followed by INH-mono (10/28, 35.7%), EMB-mono (3/28, 10.7%), and none of them were RIF-mono-resistant isolates. Nine M. tuberculosis isolates (9/49, 18.4%) were any poly-resistant other than MDR-TB, with a proportion of resistance to drug combination of INH + STR (66.7%), followed by STR+EMB (22.2%) and INH + STR + EMB (11.1%) (Table 2).
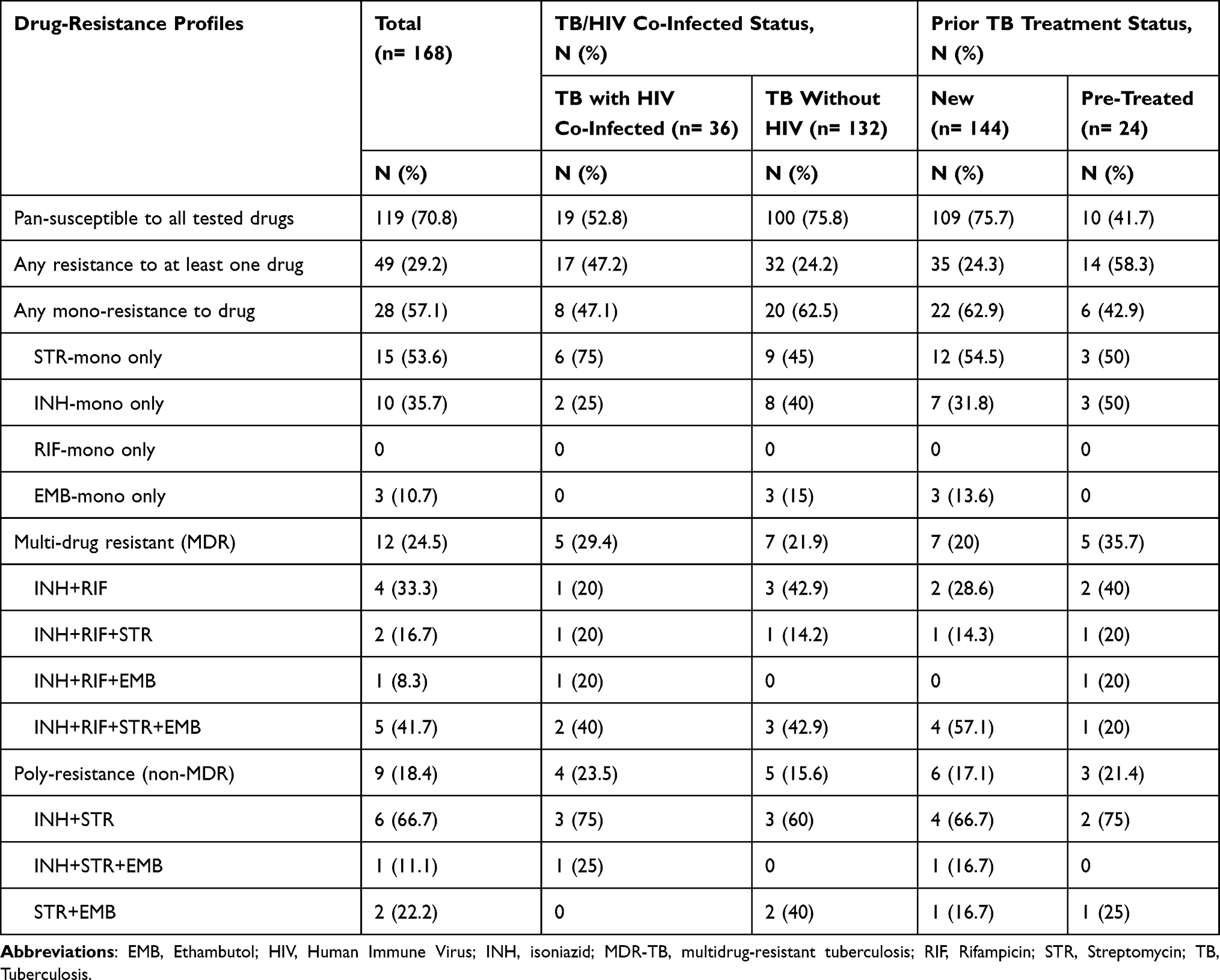 |
Table 2 Patterns of Drug-Resistance in M. tuberculosis Isolates by TB/HIV Co-Infection and Previous TB Treatment Status (N = 168) |
Moreover, the proportion of any-susceptible to all studied drugs, any resistant to at least one or more drugs, any mono-resistant, and MDR-TB among all TB patients with HIV-positive vs HIV-negative was 19/36 (52.8%) vs 100/132 (75.8%), 17/36 (47.2%) vs 32/132 (24.2%), 8/36 (22.2%) vs 20/132 (15.2%), and 5/36 (13.9%) vs 7/132 (5.3%), respectively. Of which, except the four combined drug INH+RIF+STR+EMB resistance pattern (2/36, 5.6%), only a single MDR-TB isolate (2.8%) of each with two or three combined drug resistance pattern was obtained from TB with HIV-positive cases. The proportion of any mono-resistant isolates and MDR-TB among all TB patients with new vs previously treated cases was 22/144 (15.3%) and 6/24 (25%) vs 7/144 (4.9%) and 5/24 (20.8%), respectively (Table 2).
Geographical Distribution Patterns of Drug-Resistance Isolates
The study found that most of the geographic background of the drug-resistance profiles in M. tuberculosis complex isolates from the Gondar district were 49 (29.2%) pan-susceptible to all drugs, 13 (7.7%) any-resistant to at least one drug excluding MDR-TB isolates, and 4 (2.4%) MDR-TB followed by Debark 24 (14.3%), 7 (4.2%), and 1 (0.6%); and Bahir-Dar 24 (14.3%), 5 (3%), and 3 (1.8%), in respective order.
Determinant Predictors Associated with Multidrug-Resistance
In the study, bivariate and multivariate regression models were used to investigate the relationship between drug-resistance patterns and TB/HIV co-infection status after controlling the effects of other variables including previous TB treatment status, age, and sex. The TB/HIV co-infection was significantly associated with MDR-TB (aOR = 0.252, 95% CI: 0.73–0.875, p = 0.03) and STR-related resistance (aOR = 0.298, 95% CI: 0.113–0.787, p = 0.015), but not associated with INH-related resistance (aOR = 0.57, 95% CI: 0.178–1.82, p = 0.342) when compared to patients with susceptible TB strains (Table 3).
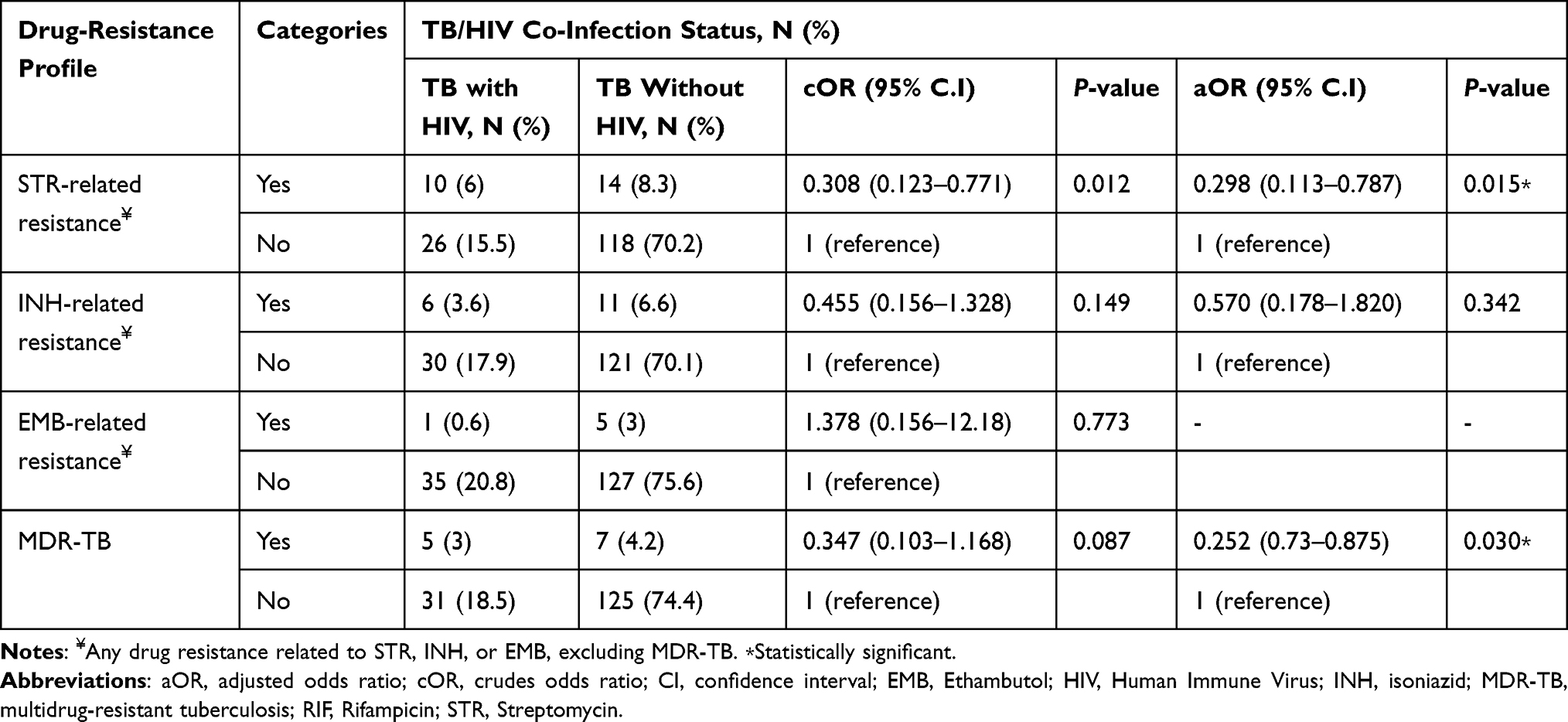 |
Table 3 Bivariate and Multivariate Analysis of Drug-Resistance Profiles by TB-HIV Co-Infection Status (N = 168) |
The association of different socio-demographic, clinical, and behavioral determinant factors other than TB/HIV co-infection status with any resistance to drugs and MDR-TB was also performed. After adjusting for any confounding variable effects, three studied variables were determined to be independent determining factors for the emergency of any drug-resistant TB strains. In a univariate analysis, the pulmonary TB patients who had previously undergone TB treatment (aOR = 2.92, 95% CI: 1.10–7.75, p = 0.03), previous contact with active TB patients (aOR = 2.95, 95% CI: 1.38–6.32, p = 0.005), and drinking alcohol (aOR = 2.66, 95% CI: 1.16–6.11, p = 0.02) were significantly associated with any drug-resistant TB. Nevertheless, both sex (aOR = 1.11, 95% CI: 0.49–2.48, p = 0.798) and smoking cigarettes (aOR = 1.38, 95% CI: 0.43–4.41, p = 0.58) were not significantly associated with any drug-resistant TB strains. Moreover, a multivariate analysis revealed that pulmonary TB with previous TB treatment was significantly linked with a high rate of MDR-TB (aOR = 6.73, 95% CI: 1.78–25.47, p = 0.005) as compared to new TB cases (Table 4).
 |
Table 4 Multivariate Analysis of Patients’ Socio-Demographic and Clinical Factors with Any Resistance to Drugs and MDR-TB (N = 168) |
Discussion
TB was a significant cause of co-morbidity, co-mortality and negative socioeconomic impact in people with HIV/AIDS (PLHIV) around the world due to the capability of disarming the host’s immune responses through mechanisms that are not fully understood.1 TB patient co-infected with HIV has diagnostic and therapeutic challenges, which exert extreme pressure on healthcare systems predominantly in resource-constrained developing nations like Ethiopia.10,13 Early detection of drug-resistance patterns has a key importance for clinicians to select appropriate anti-TB treatment regimen, optimize treatment regimen composition via DST at baseline, and to direct infection control measures to block transmission of MDR-TB. In this study, the prevalence, distribution patterns of drug resistance and their association with TB/HIV co-infection and other risk factors were evaluated. The study was found a higher prevalence of TB/HIV co-infection (50/252, 19.8%), which is slightly in consistent with the other findings from the Amhara region (20% and 25.6%)19,34 and North India (20%).35 Higher rate of TB/HIV co-infection cases were reported from Addis Ababa, Ethiopia (57%),8 Western Kenya (48%),36 and Zambia (44%);37 while a lower rate from Northwest Ethiopia (12%)38 and Saudi Arabia (0.7%).39 The higher rate of TB with HIV co-infected cases might be explained by impairing the host’s immune responses to both diseases, lengthening the time it takes for TB treatments to be effective by increasing the bacilli load, which could make the bacteria resistant to anti-TB drugs, and lead to MDR-TB. Also, due to immunosuppression, drug-resistant TB strains like MDR-TB pose a severe threat to public health and cause high rates of morbidity and mortality in communities of people who are HIV-positive.5,9
As far as we are aware, this study provides important information on the patterns of MDR-TB and associated determinant predictors among pulmonary TB co-infected with HIV-positive vs HIV-negative cases in the study area. In the study, the overall prevalence of resistance to one or more first-line anti-TB drugs among all TB patients was 49/168 (29.2%) as well as among HIV-positive vs HIV-negative patients was 17/36 (47.2%) vs 32/132 (24.2%). This is slightly similar to earlier studies conducted in Zambia (23.5%)37 and China.40 These similarities in prevalence with our study could be attributed to the high TB burdens and HIV/TB co-infections across all countries.1
The overall prevalence of MDR-TB among all studied TB patients was 12/168 (7.1%), which is in agreement with the studies conducted from Saudi Arabia (5%),39 Zambia (9.8%),37 and Tanzania (5.7%)41 among TB patients. While, the higher rate of MDR-TB was reported from Russia (67.9%),42 North India (17.4%),35 and Amhara region (87%)34 among the RIF-resistant patients. Our study also revealed that the MDR-TB isolates among HIV-positive vs HIV-negative patients was found to be 5/36 (13.9%) vs 7/132 (5.3%), respectively. The proportion of MDR-TB among HIV-positive patients (22.2%) in our finding is higher than the previous finding from Western Kenya (12%),36 and slightly lower than from North India (27.3%)35 among HIV-positive patients.
Moreover, the overall prevalence of any first-line mono-resistant isolates among all TB patients was 28/168 (16.7%), as well as among HIV-positive vs HIV-negative patients was 8/36 (22.2%) vs 20/132 (15.2%), respectively. Of which, the present study showed that STR-mono-resistant isolates was accounted a high rate of 15/28 (53.6%), followed by INH-mono-resistant isolates (10/28, 35.7%). This high rate of isolates resistance to STR-mono could be due to the common use of the drug for treatment of respiratory and any bacterial infections, poor prescription and treatment practice, and early introduction for TB treatment. However, in the study, there was no RIF-mono resistant isolate found, and all RIF-related resistant cases were also resistant to INH-related which are known as MDR-TB cases, which has significant implications since practicing TB programs to use RIF-resistance as a surrogate marker for MDR-TB diagnosis and is an essential drug during the course of TB treatment. Compared to our findings, previous studies were reported higher rate of INH-mono resistant from Western Kenya (28.5%)36 and RIF-mono resistant from Amhara region (6%),34 Western Kenya (14.6%),36 Tanzania (2.5%),41 and Zambia (3%);37 as well as lower rate of any mono-resistant to tested drugs from Russia (13.9%),42 INH mono-resistant from Amhara region (2%)34 and Zambia (9.8%),37 and STR-mono resistant from Zambia (0.8%)37 among TB patients.
The possible reasons for the proportion difference in drug-resistance patterns of isolates among different studies of several countries could be due to variations on the study settings, source population and study participants, study designs, sample size, study period, diagnostic methodological techniques (culture vs susceptibility techniques), geographical location and time of sputum samples collection, laboratory setup and resources for the isolation of drug-resistant strains, TB control and prevention practice, and mutational heterogeneity in the target genes associated with anti-TB drug-resistance. Our assumption was supported by previous investigations.8,34,39
Besides, the patterns of drug-resistance were disproportionately distributed in districts of the Northwest Amhara region. Sixty-two (37%) of cases were reported from central Gondar zone, Gondar. The possible explanation for this could be that there was frequent population migration from the neighboring zones and woredas at the time of local armed conflict, which makes the city more crowded, unstable, and favors the transmission of infections in the area.
Another finding of the current study revealed that the prevalence of overall drug resistance to at least one or more drugs and MDR-TB among new vs previously treated cases was 35/144 (24.3%) vs 14/24 (58.3%) and 7/144 (4.9%) vs 5/24 (20.8%), respectively. The prevalence of MDR-TB among previous TB treatment cases in our study was higher compared to previous reports from Northwest Ethiopia,16 Eastern Ethiopia,43 and Thailand;44 but lower than from Addis Ababa Ethiopia,8 North India,35 and Zambia.37 This higher rate reported in our study could be due to the fact that the study was conducted during the time of local armed conflict, where individuals were migrated and supply of TB medications were interrupted. Moreover, this enhanced frequency of MDR-TB in participants who had a history of previous treatment can be influenced by the acquisition of resistance in the intensive and continuation phases of treatment and that indicates high transmission of TB infection and MDR-TB in the community. So, serious emphasis should be given for the control and prevention to limit its transmission. Furthermore, the explanation for enhanced rate of MDR-TB among patients with the age range of 18–34 years (6/12, 50%) could be probably due to high mobility, mainly involved in outdoor activities, have more frequent contact with TB patients and high-risk behavior, as well as their propensity to stop receiving TB treatment.
Although, drug-resistant TB is primarily resulted from chromosomal alterations due to mutations or deletions, there are several associated factors that have a significant impact on the increasing emergency and transmission of drug-resistant TB strains. Our study showed that the TB with HIV-co-infection was significantly associated with a lower rate of MDR-TB (aOR = 0.252, 95% CI 0.73–0.875, p = 0.03). This finding is in consistent with earlier findings that showed MDR-TB was substantially correlated to TB/HIV co-infection (aOR = 5.59, p = 0.00) in central Ethiopia8 (aOR = 2.3, 95% CI, 1.000–5.350; p = 0.05) in North India,35 and (OR = 3.83; 95% CI: 1.02–14.38; p = 0.047) in Thailand.45 It is, therefore, mostly the TB patients with HIV-positive cases are could be true that increase the risk of developing MDR-TB by dropping the immune response due to their immunocompromised state. However, other investigators did not find any significant association of HIV co-infection with MDR-TB from central Ethiopia,46 Korea,47 and Mali.48 Significantly, TB patients who had previously treated cases were six times more likely to develop MDR-TB (aOR = 6.73, 95% CI: 1.78–25.47, p = 0.005). This result is in line with that MDR-TB infection was associated with a history of previous TB treatment case (χ² = 6.9, p = 0.055) in Eastern Ethiopia,43 (OR = 51.86; 95% CI: 12.35–217.79; p < 0.001) in Thailand,45 and (OR 7.6; 95% CI: 1.60–36.0) in Saudi Arabia.39 It is well documented that previous TB treatment cases could be true that increase the risk of developing MDR-TB infection than new TB cases.
Conclusion
The frequency of TB patients with HIV-positive and a history of previous TB treatment were high compared to HIV-negative and new cases, and also significantly associated with MDR-TB in the Northwest Amhara, Ethiopia. Hence, it is likely that the current control strategies are insufficient to reduce the emergency of drug-resistant TB strains. Therefore, the findings in our study could be an important indicator for the health care system and clinicians to design and implement more effective and appropriate TB treatment regimens to TB patients and improve their clinical outcomes in the area. As a result, an appropriate control and prevention methods should be applied to reduce the emergence and transmission of drug-resistant TB strains such as MDR-TB in the community. Thus, health care workers, physicians, health programmers and other implementers should give special attention on enhancing patient adherence to anti-TB medications and appropriate prescriptions, uninterrupted supply of anti-TB drugs and support of TB patients for treatment compliance, further counseling of TB/HIV co-infection, and design a package in TB control program that addresses such areas where thousands of people are living in overcrowded environments.
Strength and Limitation of the Study
In contrast to earlier studies in the area, this study provides new insights into the impact of HIV co-infection on the MDR-TB profile of TB patients. However, the study has its own limitations. Due to resource constraints, only sputum samples from individuals with pulmonary TB cases were used and the extra-pulmonary TB cases were excluded. The sample size may not be adequately powered for the risk factors assessed in this study. The MDR-TB clinical isolates were not tested for phenotypic drug susceptibility pattern of second-line anti-TB drugs. Characterization of mutations conferring resistance to first-line and second-line anti-TB drugs was not determined. A rapid and economical genotypic test requires detailed knowledge of the prevalent patterns of MDR-TB and extensively drug resistant (XDR-TB) and resistant conferring gene mutations.
Abbreviations
DST, drug susceptibility testing; EMB, ethambutol; HIV, Human Immunodeficiency Virus; INH, isoniazid; LJ, Lowenstein-Jensen; MDR-TB, Multidrug-resistant tuberculosis; MIGT, mycobacteria growth indicator tube; NTM, non-tuberculosis mycobacteria; RIF, Rifampicin; STR, Streptomycin; WHO, World Health Organization.
Data Sharing Statement
Datasets used in the study are available from the corresponding author upon reasonable request.
Acknowledgments
Foremost, the authors would like to acknowledge all the study participants for their willingness to participate in this study and for providing the necessary information. The University of Gondar, Institute of Biotechnology, Department of Medical Biotechnology; UoGCSH TB Culture laboratory staff; and the corresponding hospitals of data collectors are also acknowledged for their remarkable support during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the University of Gondar (UoG) and the Minister of Higher Education (MoE), Ethiopia. The funders had no role in study design, data collection and analysis, preparation of the manuscript, and/or decision to publish.
Disclosure
The authors have declared that no competing interests exist.
References
1. World Health Organization. Global TB report 2022. Geneva: World Health Organization; 2022. Available from: https://www.who.int/publications/i/item/9789240061729.
2. World Health Organization. Global tuberculosis report 2021. Geneva: World Health Organization; 2021. Available from: https://www.who.int/publications/i/item/9789240037021.
3. Seung KJ, Keshavjee S, Rich ML. Multidrug-resistant tuberculosis and extensively drug-resistant tuberculosis. Cold Spring Harb Perspect Med. 2015;5(9):a017863. doi:10.1101/cshperspect.a017863
4. Workicho A, Kassahun W, Alemseged F. Risk factors for multidrug-resistant tuberculosis among tuberculosis patients: a case-control study. Infect Drug Resist. 2017;10:91–96. doi:10.2147/IDR.S126274
5. Khan PY, Yates TA, Osman M, et al. Transmission of drug-resistant tuberculosis in HIV-endemic settings. Lancet Infect Dis. 2019;19(3):1–25. doi:10.1016/S1473-3099(18)30537-1
6. Mgogwe J, Semvua H, Massay O, Nyombi B, Chilongola J. Demographic and clinical determinants of multi drug resistant tuberculosis among HIV infected patients in Tanzania. Int J Med Med Sci. 2020;12(2):23–32. doi:10.5897/IJMMS2020.1415
7. Sharma SK, Mohan A. Multidrug-resistant tuberculosis: a menace that threatens to destabilize tuberculosis control. Chest. 2006;130(1):261–272. doi:10.1378/chest.130.1.261
8. Mesfin EA, Beyene D, Tesfaye A, et al. Drug-resistance patterns of Mycobacterium tuberculosis strains and associated risk factors among multi drug-resistant tuberculosis suspected patients from Ethiopia. PLoS One. 2018;3(16):1–16. doi:10.1371/journal.pone.0197737
9. Wong K, Nguyen J, Blair L, et al. Pathogenesis of human immunodeficiency virus-Mycobacterium tuberculosis co-infection. J Clin Med. 2020;9(11):3575. doi:10.3390/jcm9113575
10. Waters R, Ndengane M, Abrahams MR, Diedrich CR, Wilkinson RJ, Coussens AK. The Mtb-HIV syndemic interaction: why treating M. tuberculosis infection may be crucial for HIV-1 eradication. Future Virol. 2020;15(2):101–126. doi:10.2217/fvl-2019-0069
11. Walker NF, Meintjes G, Wilkinson RJ. HIV-1 and the immune response to TB. Future Virol. 2013;8(1):57–80. doi:10.2217/fvl.12.123
12. French CE, Glynn JR, Kruijshaar ME, Ditah IC, Delpech V, Abubakar I. The association between HIV and antituberculosis drug resistance. Eur Respir J. 2008;32(3):718–725. doi:10.1183/09031936.00022308
13. Ismail N, Ismail F, Omar SV, et al. Drug resistant tuberculosis in Africa: current status, gaps and opportunities. Afr J Lab Med. 2018;7(2):1–11. doi:10.4102/ajlm.v7i2.781
14. Temesgen B, Kibret GD, Alamirew NM, Melkamu MW, Hibstie YT, Petrucka P. Incidence and predictors of tuberculosis among HIV-positive adults on antiretroviral therapy at Debre Markos referral hospital, Northwest Ethiopia: a retrospective record review. BMC Public Heal. 2019;19(1). doi:10.1186/s12889-019-7912-9
15. Singh A, Prasad R, Balasubramanian V, Gupta N. Drug-resistant tuberculosis and HIV infection: current perspectives. HIV/AIDS - Res Palliat Care. 2020;12:9–31. doi:10.2147/HIV.S193059
16. Yigzaw WB, Torrelles JB, Wang SH, Tessma B. Magnitude of phenotypic and MTBDRplus line probe assay first-line anti-tuberculosis drug resistance among tuberculosis patients; Northwest Ethiopia. Infect Drug Resist. 2021;14:497–505. doi:10.2147/IDR.S292058
17. CSA. The Central Statistical Agency of the Government of Ethiopia. CSA; 2015.
18. Lwanga SK, Lemeshow S Sample size determination in health studies: a practical manual. World Health Organization; 1991. Available from: https://apps.who.int/iris/handle/10665/40062.
19. Teweldemedhin M, Asres N, Gebreyesus H, Asgedom SW. Tuberculosis-Human Immunodeficiency Virus (HIV) co-infection in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2018;18(1):1–9. doi:10.1186/s12879-018-3604-9
20. Cepheid. GeneXpert® operator’s manual and the Xpert® MTB/RIF protocols (CD-ROM) for compre_hensive operating instructions, including important warnings relating to operator safety. Anim Genet. 2013;39:542.
21. Ethiopia Ministry of Health. National Comprehensive Tuberculosis, Leprosy and TB/HIV Training Manual for Health Care Workers. Addis Ababa: Ethiopia Ministry of Health; 2016.
22. GLI. Mycobacteriology Laboratory Manual. Global Laboratory Initiative; Advancing TB Diagnosis. GLI; 2014:47–51.
23. Kone B, Sarro YS, Baya B, et al. Diagnostic performances of three rapid diagnostic tests for detecting HIV infections in Mali. Infect Dis Diagnosis Treat. 2019;3(1):1–17.
24. Chaillet P, Tayler-Smith K, Zachariah R, et al. Evaluation of four rapid tests for diagnosis and differentiation of HIV-1 and HIV-2 infections in Guinea-Conakry, West Africa. Trans R Soc Trop Med Hyg. 2010;104(9):571–576. doi:10.1016/j.trstmh.2010.05.007
25. Kubica GP, Dye WE, Cohn MG, Middlebrook G. Sputum digestion and decontamination with N-acetyl-L-cysteine-sodium hydroxide for culture of mycobacteria. Am Rev Respir Dis. 1963;87:775–779. doi:10.1164/arrd.1963.87.5.775
26. Khan MS, Dar O, Tahseen S, Godfrey-Faussett P. Judging respiratory specimen acceptability for AFB microscopy: visual vs. microscopic screening. Trop Med Int Heal. 2009;14(5):571–575. doi:10.1111/j.1365-3156.2009.02260.x
27. Budayanti NS, Suryawan K, Iswari IS, Sukrama DM. The quality of sputum specimens as a predictor of isolated bacteria from patients with lower respiratory tract infections at a Tertiary Referral Hospital, Denpasar, Bali-Indonesia. Front Med. 2019;6:1–6. doi:10.3389/fmed.2019.00064
28. Pinhata JMW, Lemes RA, Simeão FC, De Souza AR, Chimara E, Ferrazoli L. Use of an immunochromatographic assay for rapid identification of Mycobacterium tuberculosis complex clinical isolates in routine diagnosis. J Med Microbiol. 2018;67(5):683–686. doi:10.1099/jmm.0.000726
29. Siddiqi SH, Rusch-Gerdes S. MGIT procedure manual. Foundation for Innovative New Diagnostics (FIND), Geneva, Switzerland. 2006.
30. World Health Organization. The Use of Liquid Medium for Culture and Drug Susceptibility Testing (DST) in Low and Medium Income Settings. Geneva: World Health Organization; 2007.
31. Agarwal A, Kumar N, Kishore K. Evaluation of manual Mycobacterium growth indicator tube for isolation and susceptibility testing of Mycobacterium tuberculosis for implementation in low and medium volume laboratories. Med J Armed Forces India. 2018;74(3):220–226. doi:10.1016/j.mjafi.2017.02.012
32. Genestet C, Hodille E, Westeel E, et al. Subcultured Mycobacterium tuberculosis isolates on different growth media are fully representative of bacteria within clinical samples. Tuberculosis. 2019;116:61–66. doi:10.1016/j.tube.2019.05.001
33. World Health Organization. Technical Manual for Drug Susceptibility Testing of Medicines Used in the Treatment of Tuberculosis. Geneva, Switzerland: World Health Organization; 2018.
34. Shibabaw A, Gelaw B, Gebreyes W, Robinson R, Wang S-H. The burden of pre-extensively and extensively drug-resistant tuberculosis among MDR-TB patients in the Amhara region, Ethiopia. PLoS One. 2020;15(2):1–13. doi:10.1371/journal.pone.0229040
35. Sunil S, Abhishek M, Dhatwalia SK, et al. Prevalence of multidrug resistance in Mycobacterium tuberculosis isolates from HIV seropositive and seronegative patients with pulmonary tuberculosis in north India. BMC Infect Dis. 2013;13(137). doi:10.1186/1471-2334-13-137
36. Ogwang MO, Imbuga M, Ngugi C, Mutharia L, Magoma G, Diero L. Distribution patterns of drug resistance Mycobacterium tuberculosis among HIV negative and positive tuberculosis patients in Western Kenya. BMC Infect Dis. 2021;21(1):1–15. doi:10.1186/s12879-021-06887-x
37. Monde N, Munyeme M, Chongwe G, et al. First and second-line anti-tuberculosis drug-resistance patterns in pulmonary tuberculosis patients in Zambia. Antibiotics. 2023;12(1):166. doi:10.3390/antibiotics12010166
38. Toru M, Baye A, Gebeyehu Z, Abebaw A, Reta A. Prevalence, associated factors and rifampicin resistance pattern of pulmonary tuberculosis among HIV-positive patients attending antiretroviral treatment clinic at East Gojjam Zone, Ethiopia: an institution-based cross-sectional study. J Clin Tuberc Other Mycobact Dis. 2022;29. doi:10.1016/j.jctube.2022.100336
39. Sambas MF, Rabbani U, Al-Gethamy MMM, et al. Prevalence and determinants of multidrug-resistant tuberculosis in Makkah, Saudi Arabia. Infect Drug Resist. 2020;13:4031–4038. doi:10.2147/IDR.S277477
40. Lv XT, Lu XW, Shi XY, Zhou L. Prevalence and risk factors of multi-drug resistant tuberculosis in Dalian, China. J Int Med Res. 2017;45(6):1779–1786. doi:10.1177/0300060516687429
41. Mchaki BR, Mgaya FX, Kunambi PP, Matee MI. Can resistance to either isoniazid or rifampicin predict multidrug resistance tuberculosis (MDR-TB). Bull Natl Res Cent. 2023;47(23). doi:10.1186/s42269-023-01001-4
42. Kostyukova I, Pasechnik O, Mokrousov I. Epidemiology and drug resistance patterns of Mycobacterium tuberculosis in high-burden area in Western Siberia, Russia. Microorganisms. 2023;11(2):425. doi:10.3390/microorganisms11020425
43. Worku G, Gumi B, Girma M, et al. Drug sensitivity of clinical isolates of Mycobacterium tuberculosis and its association with bacterial genotype in the Somali region, Eastern Ethiopia. Front Public Heal. 2022;10. doi:10.3389/fpubh.2022.942618
44. Kamolwat P, Nateniyom S, Chaiprasert A, et al. Prevalence and associated risk factors of drug-resistant tuberculosis in Thailand: results from the fifth national anti-tuberculosis drug resistance survey. Trop Med Int Heal. 2021;26(1):45–53. doi:10.1111/tmi.13502
45. Jitmuang A, Munjit P, Foongladda S. Prevalence and factors associated with multidrug-resistant tuberculosis at Siriraj Hospital, Bangkok, Thailand. Southeast Asian J Trop Med Public Health. 2015;46(4):697–706.
46. Hirpa S, Medhin G, Girma B, et al. Determinants of multidrug-resistant tuberculosis in patients who underwent first-line treatment in Addis Ababa: a case control study. BMC Public Health. 2013;13(1). doi:10.1186/1471-2458-13-782
47. Lee S, Lee SH, Mok JH, et al. Is multi-drug resistant tuberculosis more prevalent in HIV-infected patients in Korea? Yonsei Med J. 2016;57(6):1508–1510. doi:10.3349/ymj.2016.57.6.1508
48. Baya B, Achenbach CJ, Kone B, et al. Clinical risk factors associated with multidrug-resistant tuberculosis (MDR-TB) in Mali. Int J Infect Dis. 2019;81:149–155. doi:10.1016/j.ijid.2019.02.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.