")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Characteristics of Patients with Meningeal Carcinomatosis Combined with Myelopathy
Received 13 July 2021
Accepted for publication 22 October 2021
Published 19 May 2022 Volume 2022:18 Pages 1069—1075
DOI https://doi.org/10.2147/NDT.S329180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Lidong Jiao,1 Min Wei,1 Yongjuan Fu2
1Department of Neurology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 2Department of Pathology, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China
Correspondence: Lidong Jiao Department of Neurology, Xuanwu Hospital, Capital Medical University, No. 45 ChangChun Street, XiCheng District, Beijing, 100053, People’s Republic of China Tel +86-10-83198814 Email [email protected]
Objective: To explore the disease manifestations and radiological characteristics of patients with meningeal carcinomatosis (MC) combined with myelopathy.
Patients and Methods: The detailed medical information of patients who suffered from MC with myelopathy in record system were collected and reviewed.
Results: In these patients, five cases were male and two cases were female. The age was from fifteen to fifty-seven years. In the course of disease, tumor cells were discovered in cerebrospinal fluid of three patients and in biopsy samples of four patients. Cerebrospinal fluid (CSF) test results showed white blood cell counts increased in seven patients, protein increased in six patients and glucose reduced in five patients. In addition, MRI revealed that the white matter abnormalities showed in all cases and pia mater was enhanced in four patients, meningeal enhanced was observed in three patients. All patients were given appropriate therapy during hospitalization. Follow-up result showed that all patients passed away two to five months after diagnosis.
Conclusion: MC causes spinal membrane, spinal nerve root to be involved besides, also can produce the matter of myelopathy. Early detection of intramedullary lesion is conducive to strengthening the awareness of the diagnosis of MC.
Keywords: meningeal carcinomatosis, myelopathy, histopathological investigation, CSF cytology
Introduction
Meningeal carcinomatosis (MC), also known as carcinomatous meningitis, leptomeningeal carcinomatosis (LMC)1 or neoplastic meningitis (NM),2 is the diffusion of tumor cells within the leptomeninges and subarachnoid space.3 MC is mostly diagnosed in patients with leukemia and lymphoma (5–15%), followed by solid tumors (1–5%), and the least common in primary brain tumors (1–2%).4 MC is one of the most serious forms of brain metastasis which leads to critical morbidity and mortality with dismal prognosis.2 MC can lead to serious neurological complications involving cranial nerves, brain and spinal cord, which can reduce life expectancy to 4–6 weeks if leaving untreated or to the 2–6 month when aggressively treated.5 Early diagnosis and prompt treatment may have a significant impact on improving the prognosis. With the advances in clinical recognition and diagnostics, an increasing number of patients are diagnosed with MC. MC has been diagnosed in ten percent of the patients with metastatic cancer through the clinical process. Among those cases, it occurs in <10% at the time of diagnosis, and in 20% at first progress after initial treatment.3
MC is usually diagnosed by three methods: clinical symptoms, cytology in cerebrospinal fluid (CSF), and magnetic resonance imaging (MRI) of the brain and spinal cord.6 However, there are different limits to the sensitivity or specificity of each method. A recent study conducted by de Azevedo et al founded that fifty-five percent patients suffered from headache, fifty percent with cranial nerve paralysis, twenty-three percent with raised intracranial pressure, twenty percent with vertigo as well as twelve percent with seizure onset in a series case report of sixty patients with MC and breast cancer combined.7 The appearance of cancer cells in the CSF is an extremely helpful discovery to make a definite diagnosis and CSF cytology is still the gold diagnostic standard,2 however, sensitivity of CSF cytologic analysis are as low as forty-five percent in a single lumbar puncture (LP).5 It is difficult to make a diagnosis by clinical manifestations of acute, subacute or advanced stage neurological deficits during anticancer therapies; in a high number of cases the original examinations were confined to a CSF cytology, which had negative results frequently.8 In clinical practice, gadolinium magnetic resonance imaging (GdMRI) of the brain and spinal cord is still a preferable way for the diagnosis of MC.9 Although diffuse enhancement showed in the spinal meninges or nerve roots in MRI had been reported in many studies,10–12 but reports of meningeal carcinomatosis with myelopathy were still rare. Although we can show other metastatic diseases with whole-body 18F-FDG PET/CT (positron emission tomography (PET) with fluorine 18 (18F) fluorodeoxyglucose (FDG)),13 it has been reported that 18F-FDG PET/CT is insensitive to the discovery of brain metastases, especially small lesions might be ignored.14
The prognosis for MC is usually poor, so the early diagnosis and treatment are of great benefit to longer survival and prognosis improvement. In the previous studies, few articles concerning spinal cord parenchyma involvement caused by MC are reported. In order to enhance the early diagnosis of MC, we investigated clinical manifestations, imaging characteristics and CSF examination through a retrospective analysis of clinical characteristics of 7 patients by reviewing literatures. By greatly increasing imaging features recognition during diagnosis, it will provide effective help for the early diagnosis and treatment of MC.
Patients and Methods
Patients
A total of 7 patients diagnosed as MC with spinal cord lesions admitted to Department of Neurology, Xuanwu Hospital, Capital Medical University, from January 2013 to January 2017 were analyzed retrospectively.
Demographic Information and Clinical Characteristics
Demographic information on age and sex, as well as clinical characteristics, including chief complaint, disease duration and accompanying symptom were obtained from medical records and analyzed in detail.
Laboratory Tests
A standard cerebrospinal fluid (CSF) evaluation was performed. All 7 cases underwent lumbar puncture. CSF analyses include pressure, cell counts, protein, glucose and the IgG index.
Histopathological Assessment and Imaging Assessment
The collected samples are examined by histopathological investigation. Specimens were fixed in 10% neutral buffered formalin, and then paraffin-embedded, next routinely processed for light microscopy. Other then routine hematoxylin–eosin staining, immunohistochemical staining was performed on 4-μm sections using a BenchMark ULTRA autostainer, version 12.3 (Ventana Medical Systems, USA). Mouse monoclonal anti-human antibodies against CK, EMA, CK7 and CK5/6, as well as rabbit polyclonal anti-human antibodies against CK20 and P40 were purchased from ZS company. MRI enhanced scans of brain and spinal cord were performed in all patients.
Treatment and Prognosis
The patients were treated with radiotherapy and/or symptomatic treatment. All of patients were routinely followed up by telephone or outpatient visit for 2 months to 5 months.
Results
Demographic Information and Clinical Characteristics
In the present study, the clinical data of seven cases (five males and two females; age, 42.3±16.6 [15–57] years) confirmed patients have been analyzed retrospectively (Table 1).
 |
Table 1 Demographics and Clinical Characteristics of 7 MC Patients Accompanied by Spinal Cord Lesion |
Clinical characteristics and neurological examinations were summarized as follows: 3 cases with headache, 2 cases with dizziness, 2 cases with epilepsy, 3 cases with double vision, 2 cases with blurred vision, 5 cases with limb weakness, 4 cases with sensory dysfunction, 4 cases with micturition arduous, 6 cases with positive meningeal irritation sign, 5 cases with reduced tendon reflexes, 2 cases with hyperreflexia of upper limb combined with reduced ankle reflexes, 5 cases with reduction of body mass.
Laboratory Tests
All patients underwent lumbar puncture, CSF pressure increased in 3 cases, white blood cells increased in 7 cases, protein increased in 6 cases, glucose decreased in 5 cases, and IgG index increased in 7 cases. In cases 2, 6, 7, tumor cells were found in cerebrospinal fluid confirmed by immunohistochemical staining, and cases 1, 3, 4 and 5 were confirmed by biopsy of meninges and nerve root for diagnosis. In addition, all patients underwent blood and/or cerebrospinal fluid virus antibody, antibody against Lyme disease, Brucella agglutination test, tuberculosis antibody, serological test for syphilis, Cryptococcus capsular antigen and other related tests, and the results were negative.
Histopathological Assessment
The pathological findings are presented in Figure 1. Tumor cells were found in CSF of three patients, including case 2, case 6, case 7. Tumor cells in biopsy samples were found in four cases (case 1, case 3, case 4, case 5) (Figure 1).
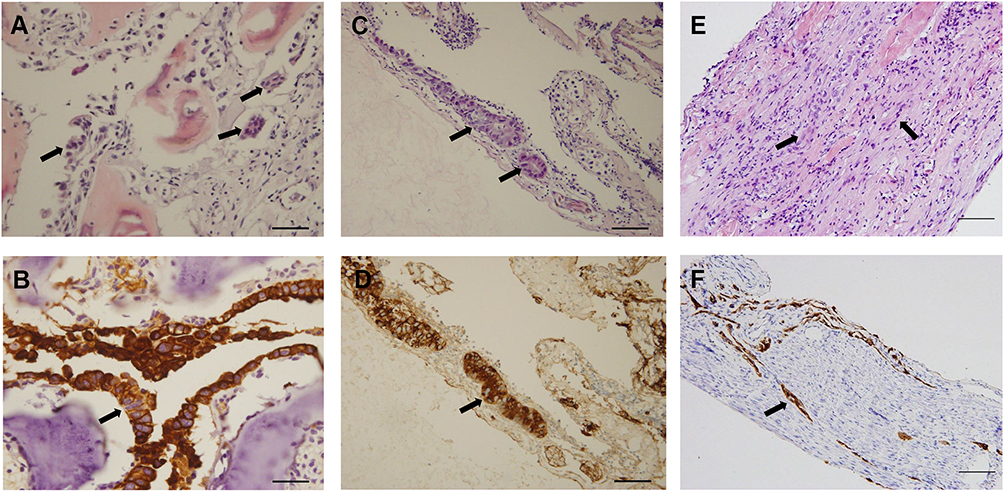 |
Figure 1 Histopathological and immunohistochemical findings of case 3 to 5. In case 4, adenocarcinoma was found metastasized to the vertebrae of L2 (A), with the tumor cells positive for CK7 (B). In case 5, adenocarcinoma had infiltrated the meningeal of L2 (C) and showed immunoreactivity for EMA (D). Nerve roots invasion of squamous cell carcinoma was observed in case 3 (E), with CK5/6 positive (F). (The arrows showed metastatic tumour cells. Bars =50 μm for (A, C, D and F). Bars=100 μm for (B and E). |
MRI Assessment
All seven patients underwent enhanced MRI scanning of brain and spinal cord. Findings showed white matter abnormalities in the spinal cord without reinforcement in all 7 patients (Figure 2). Pia mater enhancement was seen in four cases and meningeal enhancement was seen in three cases.
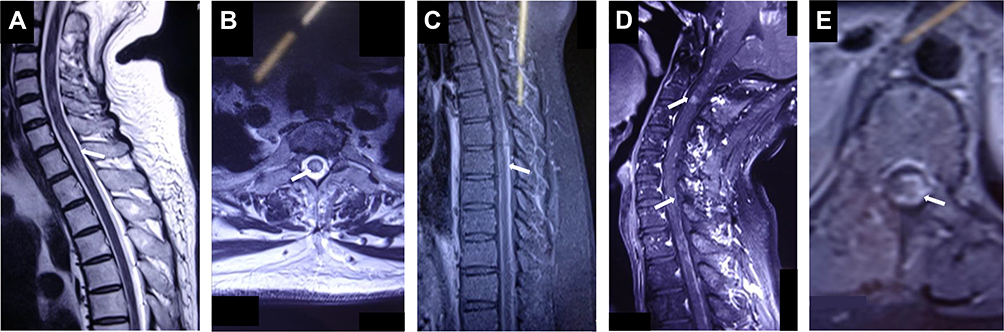 |
Figure 2 MR images. (A–E) MR images of the patients. (A) Sagittal T2-weighted MR images of the cervical spinal cord showed hyperintensity lesions (arrow showed). (B) Axial T2-weighted MR images of the cervical spinal cord showed hyperintensity lesions (arrow showed). (C) Contrast-enhanced MR scan showed sagittal enhancement of the spinal membrane (arrow showed). (D) MR contrast-enhanced sagittal scan showed disseminated implant metastases (arrows showed). (E) The enhancement of the spinal membrane in the axial view (arrow showed). |
Treatment and Prognosis
All patients were treated with radiotherapy and/or symptomatic therapy. Conventional treatments were composed of reducing intracranial pressure, preventing infection, relieving pain and other symptomatic treatment by using mannitol, neurotrophic drugs, and so on. After diagnosis, all patients were transferred to local hospitals or tumor hospitals for further treatment. All patients died within 2 to 5 months after diagnosis by telephone follow-up.
Discussion
In our study, we summarized the clinical characteristics, pathological features and imaging findings of 7 patients with MC, in order to increase the identification of suspected MC patients with spinal cord lesion for clinical workers. We reported 7 MC patients associated with myelopathy, whose initial symptoms were headache or cranial nerve involvement. After admission, all patients were confirmed as MC by histopathological assessment and they all received the radiotherapy and symptomatic treatment after diagnosis, but they all passed away within two to five months after discharge.
The clinical symptoms of MC are related to the involved sites of CNS. Meningeal involvement can be manifested as increased intracranial pressure; cerebral parenchyma involvement can be manifested as epilepsy or disturbance of consciousness; spinal nerve roots and cranial nerves involvement could be manifested as cranial nerve palsy and reduced tendon reflex. However, the early clinical manifestations of MC are often atypical, which can be manifested as 1 or 2 sets of symptoms and signs in cranial hypertension syndrome, cranial nerve palsy, and spinal nerve root damage. A study found that cranial nerve palsy, headache, and spinal nerve root injury were the most common clinical manifestations of MC.15 In our series, there were 4 (57.1%) cases with cranial nerve involvement and 3 (42.9%) cases with headache or epileptic seizure.
The diagnosis of MC relies on a combination of the clinical observation, neuroimaging studies, CSF cytopathology and histopathology.6 In MC, it is significant to examine meningeal irritation, nerve root symptoms, and myelopathy related to spinal parenchymal lesions based on the pathologic findings.16 The appearance of tumor cells in CSF is most helpful and simple pathway to confirm the diagnosis. Finding tumor cells in CSF is currently considered to be gold standard for diagnosis of MC, but there is a certain false-negative rate, which may require repeated CSF cytopathology.17 In case 3, 4 times of cerebrospinal fluid cytology were negative, and the diagnosis was finally confirmed by meningeal and nerve root biopsies, indicating that negative cytology could not rule out MC diagnosis.
For patients with clinical suspected MC, MRI manifestations will contribute to establishing the diagnosis. Suggestive MRI manifestation include the following four manifestations: 1.nerve thickening; 2. linear leptomeninges enhancement; 3. superficial multiple brain metastases; 4. intradural nodules. However, in patients not accompanied by previous tumor history, who appear a meningeal or sub-arachnoid space enhancement. Neurosarcoidosis, neuroschistosomiasis, chronic meningitis and Guillain–Barré syndrome are also able to produce gadolinium-enhanced in the above parts. In patients with LP, a linear enhancement could appear in the puncture site as well as along the neuroaxis, which may last from several weeks to a few months, followed with headache resulting from low intracranial pressure in many cases.18 Therefore, patients with suspicions of MC are supposed to have MRI examination before the LP. Kizawa et al16 found that not only meninges but also cauda equina showed enhanced after gadolinium administration in some patients, which suggested crucial prompts.
T.Kon et al19 found that carcinoma cells can spread to not only the subarachnoid space but also spinal cord. Tumor cells in subarachnoid can infiltrate the cranial nerves and the cells also can infiltrate the spinal nerves. In addition, cancer cells which was in nerve roots can extend to brain parenchyma and spinal cord beyond CNS and PNS connection. In MC, spinal nerve roots may be the pathway of parenchymal invasion as well as cranial nerve roots. The typical spinal cord involvement of MC mainly includes spinal cord compression by epidural metastases, meningeal carcinomas and intramedullary metastases, and few cases with MC associated with spinal white matter lesions have been reported in the previous literature.13,19–22 The meningeal involvement by neoplastic cells is considered to have some reasons, for example, the hematology invasion which include subarachnoid space/cerebral ventricles, and then the neoplastic cells spread to the CSF, such as in germinoma, ependymoma, primitive neuroectodermal tumors(PNETs) and so on. In addition, the neoplastic cells can direct spread to the endocranium, leptomenings, or ependyma, permitting local growth, as occurs in nasopharyngeal carcinoma, cortical-based brain metastase, epidural bone metastase.18 Autopsy of MC patients showed that no obvious spinal parenchymal damage was found in MC patients with mild subarachnoid space invasion, but pathological changes such as spinal white matter demyelination, axonal swelling, and small spongy changes caused by giant cell invasion were observed in patients with severe tumor cell invasion.16
In the present study, intramedullary neoplastic lesions were found in 2 patients and intraspinal white matter lesions were found in all. In some patients, MRI sagittal enhancement scan revealed obviously thickened linear enhancement of meninges and nodular enhancement. MC patients with myelopathy and meningeal enhancement need to be differentiated from infectious diseases, such as central nervous system tuberculosis, Lyme disease, neurobrucellosis and neurosarcoidosis. Some patients had already developed myelopathy prior to meningeal enhancement and suffered from spinal nerve root injury. For these patients, we cannot rule out MC and patients will be benefit from the CSF cytology and tumor screening.
Conclusion
The clinical manifestations of MC are various, involved with central and peripheral nervous systems, CSF cytology and enhanced MRI of brain and spinal cord are required for diagnosis. The spinal cord injury of MC mostly involves the spinal membrane and spinal nerve root as well as spinal cord lesions. It is of great significance to improve the prognosis and prolong the survival time of patients by improving the early diagnosis rate and early intervention. Thus, when suspected patients develop symptoms of spinal cord injury, it is necessary for clinical workers to be alert to the diagnosis of MC.
Ethics Statement
All enrolled patients provided written informed consent in accordance with the guideline of the Declaration of Helsinki of the World Medical Association Assembly. The investigation was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University. Informed consent was obtained from all patients or parents of the patient under 15 years old in our study.
Author Contributions
All authors made a substantial contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for the contents of the work.
Funding
There is no funding to report.
Disclosure
All authors state that there is no conflict of interest.
References
1. Chen G, Ma L, Xu M, et al. Meningeal carcinomatosis: three case-reports. World J Surg Oncol. 2018;16(1):78. doi:10.1186/s12957-018-1376-8
2. Zhao Y, He JY, Zou YL, et al. Evaluating the cerebrospinal fluid ctDNA detection by next-generation sequencing in the diagnosis of meningeal carcinomatosis. BMC Neurol. 2019;19(1):331. doi:10.1186/s12883-019-1554-5
3. Le Rhun E, Weller M, Brandsma D, et al. EANO-ESMO clinical practice guidelines for diagnosis, treatment and follow-up of patients with leptomeningeal metastasis from solid tumours. Ann Oncol. 2017;28(suppl_4):iv84–iv99. doi:10.1093/annonc/mdx221
4. Chamberlain MC. Leptomeningeal metastasis. Curr Opin Oncol. 2010;22(6):627–635. doi:10.1097/CCO.0b013e32833de986
5. Mammoser AG, Groves MD. Biology and therapy of neoplastic meningitis. Curr Oncol Rep. 2010;12(1):41–49. doi:10.1007/s11912-009-0079-2
6. Chamberlain MC, Glantz M, Groves MD, Wilson WH. Diagnostic tools for neoplastic meningitis: detecting disease, identifying patient risk, and determining benefit of treatment. Semin Oncol. 2009;36(4 Suppl 2):S35–S45. doi:10.1053/j.seminoncol.2009.05.005
7. de Azevedo CR, Cruz MR, Chinen LT, et al. Meningeal carcinomatosis in breast cancer: prognostic factors and outcome. J Neurooncol. 2011;104(2):565–572. doi:10.1007/s11060-010-0524-y
8. Glantz MJ, Chamberlin MC, Walters BC. Diagnosis and outcome measures in trials for neoplastic meningitis: a review of the literature and clinical experience. Neurosurg Focus. 1998;4(6):E6.
9. Passarin MG, Sava T, Furlanetto J, et al. Leptomeningeal metastasis from solid tumors: a diagnostic and therapeutic challenge. Neurol Sci. 2015;36(1):117–123. doi:10.1007/s10072-014-1881-7
10. Shirai H, Imai S, Kajihara Y, et al. MRI in carcinomatous encephalitis. Neuroradiology. 1997;39:437–440. doi:10.1007/s002340050441
11. Shen Y, Blumenthal DT, Digre K, Cessna MH, Gopez EV. Carcinomatous meningitis as the presenting manifestation of gallbladder carcinoma: case report and review of the literature. J Neurooncol. 2004;70:67–71. doi:10.1023/B:NEON.0000040822.12161.35
12. Rodesch G, Bogaert PV, Mavroudakis N, et al. Neuroradiologic findings in leptomeningeal carcinomatosis: the value interest of gadolinium-enhanced MRI. Neuroradiology. 1990;32:26–32. doi:10.1007/BF00593937
13. Carra BJ, Clemenshaw MN. Intracranial leptomeningeal carcinomatosis from breast cancer detected on 18F-FDG PET. J Nucl Med Technol. 2015;43(3):227–228. doi:10.2967/jnmt.114.148791
14. Rohren EM, Provenzale JM, Barboriak DP, Coleman RE. Screening for cerebral metastases with FDG PET in patients undergoing whole-body staging of non–central nervous system malignancy. Radiology. 2003;226(1):181–187. doi:10.1148/radiol.2261010920
15. Pavlidis N. The diagnostic and therapeutic management of leptomeningeal carcinomatosis. Ann Oncol. 2004;15(Suppl 4):iv285–iv291. doi:10.1093/annonc/mdh941
16. Kizawa M, Mori N, Hashizume Y, Yoshida M. Pathological examination of spinal lesions in meningeal carcinomatosis. Neuropathology. 2008;28(3):295–302. doi:10.1111/j.1440-1789.2007.00879.x
17. Kak M, Nanda R, Ramsdale EE, Lukas RV. Treatment of leptomeningeal carcinomatosis: current challenges and future opportunities. J Clin Neurosci. 2015;22(4):632–637. doi:10.1016/j.jocn.2014.10.022
18. Martins SJ, Azevedo CR, Chinen LT, Cruz MR, Peterlevitz MA, Gimenes DL. Meningeal carcinomatosis in solid tumors. Arq Neuropsiquiatr. 2011;69(6):973–980. doi:10.1590/S0004-282X2011000700024
19. Kon T, Funamizu Y, Miki Y, et al. An autopsy case of meningeal carcinomatosis with parenchymal invasion through the cranial and spinal nerve roots. Neuropathology. 2014;34(5):499–503. doi:10.1111/neup.12127
20. Ogul H, Ozel L, Polat G, Koltas O, Kantarci M. Massive leptomeningeal dissemination of a low-grade thalamic astrocytoma in an adult patient. Acta Neurol Belg. 2014;115(3):415–419. doi:10.1007/s13760-014-0379-7
21. Lipinski LJ, Fabiano AJ. En plaque spinal leptomeningeal carcinomatosis from metastatic melanoma. Spine J. 2014;14(8):1808–1809. doi:10.1016/j.spinee.2014.04.005
22. Sabou TC, Kamusella P, Andresen R. Leptomeningeal carcinomatosis with involvement of the cerebellar hemispheres and the spinal cord as first manifestation of a metastasizing breast carcinoma. Clin Neuroradiol. 2014;24(3):281–284. doi:10.1007/s00062-013-0239-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.