Back to Journals » Advances in Medical Education and Practice » Volume 13
Characteristics of International Rotations for Undergraduate Medical Education at United States Medical Schools: A National Study
Received 2 July 2022
Accepted for publication 12 November 2022
Published 14 December 2022 Volume 2022:13 Pages 1475—1488
DOI https://doi.org/10.2147/AMEP.S380891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Video abstract presented by Elizabeth Sopdie
Views: 87
Elizabeth Sopdie,1 Shailendra Prasad2
1Rural and Metropolitan Physician Associate Programs, University of Minnesota, Minneapolis, MN, USA; 2Center for Global Health and Social Responsibility, University of Minnesota, Minneapolis, MN, USA
Correspondence: Elizabeth Sopdie, Rural and Metropolitan Physician Associate Programs, University of Minnesota, 420 Delaware St SE, MMC 293, Minneapolis, MN, 55455, USA, Tel +1 612-625-1582, Email [email protected]
Objective: Medical education is criticized that it does not prepare students to serve in an increasingly globalized society. Evidence that global educational experiences can alleviate these concerns have contributed to the rise in international medical education experiences. This study explores surrounding characteristics and institutional support for international rotations across medical schools in the US.
Methods: The authors conducted a sequential mixed methods exploratory national survey of international rotation coordinators at 185 US medical schools and 15 semi-structured interviews in fall 2018. Quantitative data were analyzed with descriptive statistics and qualitative data were coded and analyzed using interpretive description to identify themes across data.
Results: There were 57 responses to the survey for an overall response rate of 31%, with 77% percent of respondents (n = 44) indicating that their medical school offered international rotations. Fifteen individuals representing 13 medical schools were identified as interviewees for the second stage of the study. International rotation coordinators described components of international rotations, including partnerships with host communities, use of third-party organizations, and supporting administrative and academic structures.
Conclusion: Although international rotations are common in medical education, they are not positioned as core academic programming within medical schools. This leads to challenges in planning, implementation, and evaluation, and immense variation in rotation components across medical programs. Future research should explore best practices for pre-departure preparation, post-travel debriefing, and evaluation of student activity as well as impact on the host site. Additional research should include exploration of unique benefits of international versus domestic sites, and aspects of sustainable partnerships between medical schools and host communities.
Keywords: international rotation, global health education, medical education, US medical education, global rotation
Introduction
Undergraduate medical education in the United States is criticized that it does not prepare students to serve diverse patient populations, teach civic and advocacy roles of physicians, and raise awareness of social determinants of health.1–3 Forces of internationalization, globalization, and studies indicating that global experiences can address these deficiencies have contributed to the rise in international medical education experiences.4–8 Scholars have argued that international undergraduate medical education experiences can integrate professionalism, cultural competency, and an awareness of global health systems into training to serve a changing social landscape.9 In addition, international experiences have been found to expose students to a broader range of disease pathology and alternative health systems and are associated with heightening students’ awareness of cultural and socioeconomic factors of health as well as strengthening clinical and language skills.2,5,9
Due to rising student interest and the belief that international experiences can contribute to addressing many of the critiques of medical education, medical schools in the United States can experience pressure to provide and even expand international rotations without having a comprehensive understanding of how to create and support mutually beneficial relationships with partners in host communities and the sending institutions in the United States. Concerns of potential harm to students and host communities have been explored,2,9–12 however, there is little existing research surrounding characteristics, ethics, and institutional support for international rotations across medical schools in the United States. Studies that do exist often focus on single case studies within one medical school,13–15 and few studies explore the institutional perspectives within the sending institution in the United States, including organizational factors and the perspectives of stakeholders within medical schools. Scholars have called for studies of community-based and international experiences in medical education to include descriptions of program structures, faculty perspectives, and more specifics regarding course type, duration, service activity, funding, and characteristics of community partners.7,16,17
This study examines international rotations (IRs) across undergraduate medical education at medical schools in the United States and its territories by investigating characteristics of IRs, and structural and programmatic features necessary to support such rotations from the perspectives of international rotation coordinators (IRCs), the faculty and staff within medical schools who design and implement IRs. The research questions for this study were designed to address these calls and investigate questions such as: what do coordinators of international rotations identify as key characteristics of international rotations in US medical schools for undergraduate medical students? What are the foundational structural and programmatic components that are necessary for international rotations?
Method
Due to the exploratory nature of the research questions, we used a sequential mixed methods approach in a pragmatic framework with quantitative data collected in stage one through an online survey, and qualitative data collected in stage two through purposeful sampling and follow-up interviews with IRCs. A sequential mixed methods approach helped triangulate and explain relevant factors of international rotations in undergraduate medical education. In this study, “international rotation” (IR) referred to elective, non-elective, or required experiences in which U.S.-based medical students travel to different countries to meet medical education objectives. This study was deemed exempt by the University of Minnesota Institutional Review Board as it is not research involving human subjects as defined by DHHS and FDA regulations (STUDY00004201) because the questions focus on measuring program details from institutional stakeholders’ perspectives and not on the individuals themselves.
In stage one, we sent an online national survey to IRCs at all 185 medical schools in the US (MD- and DO-granting) that were fully accredited by the Liaison Committee on Medical Education (LCME) as of July 2018, representing the total population of IRCs at US medical schools. The survey contained 35 questions, both closed and open-ended, and took about 15 minutes to complete, and was designed to secure generalizable data from the total target population of institutional stakeholders within undergraduate medical education. Survey questions were designed after an extensive review of literature on IRs in US medical education. The questions were designed to investigate how IRs are designed and implemented, with non-identifying demographic information about the survey participant (eg, role of faculty or staff, length of time in position, ethnicity) and home institution (eg, size, public/private, faith-affiliated, etc.). The survey was reviewed for face and cognitive validity by three medical school stakeholders representing both faculty and staff with expertise in international community-based education, and then was pilot-tested for time requirements and usability by three additional medical school stakeholders. The survey is included in Appendix A.
IRCs were identified through publicly available information online using a systematic process identifying organizational roles responsible for IRs, and a school’s participation in IRs was cross-referenced with the AAMC’s Visiting Student Learning Opportunities database. The survey was distributed via email through the online platform Qualtrics©18 and remained open for one month, with two reminders sent to non-respondents after the initial survey email. Survey responses were assigned a code in a separate spreadsheet to link to subsequent interview responses without including identifying information. We analyzed survey data prior to conducting stage two and used the results to build on the qualitative approach and interview question design; codes were simply assigned to ensure that multiple interviews did not originate from one single institution. Cases that were outliers or stood apart from the rest of the data were contrasted with themes widely represented in the literature, and common themes were identified. The survey also asked participants to indicate if they were willing to be contacted for a follow-up interview. There was no incentive offered for completing the survey.
Stage two of the study involved one-hour, semi-structured interviews with 15 participants. These participants completed the survey in stage one and indicated their willingness and consented to be contacted for a follow-up interview. In total, 19 participants who expressed interest were invited to interview; of those, 15 participants followed up to schedule and completed phone interviews. The purposeful sampling allowed us to investigate quantitative results in greater depth through an explanatory process. Interview questions followed a semi-structured approach and focused on a series of themes that emerged from the initial analysis of survey responses, in addition to asking a series of foundational questions related to IR characteristics or steps taken to identify suitable rotation sites. Interviews were recorded with consent and were transcribed verbatim by the primary author, and all identifiers were removed. A list of interview questions is included in Appendix B. All data from surveys and interviews were stored securely in a password-protected online platform (Box Secure Storage) accessible only by the first author.
Analysis
We used SPSS (25)19 to calculate frequencies, percentages, means, and standard deviations for nominal data. The data set was not large enough to perform meaningful regression or predictive analyses of statistical significance. Qualitative data were uploaded to NVivo (11)20 and coded by the primary author using inductive methods, namely interpretive description, to determine cross-cutting themes, categories, and concepts.21,22 We chose interpretive description as the most appropriate method of analysis as it focuses on generating knowledge to inform practice and addresses complex experiential questions in health disciplines.23 Data were coded by congruence to themes widely represented in a literature review, outlier or extreme cases, and common emergent themes, using a constant comparison approach. The coding scheme was created by the primary author with review by the secondary author, and the second author reviewed the interviews to assess for data concordance and identify outlying themes. Coded sections of the data were compared against the original interview transcripts or survey data, allowing examination of coded sections against each other and across the institutional context identified in survey data. During this process, the authors wrote memos to make note of patterns and evaluative comments.
Results
There were 57 responses to the survey for an overall response rate of 31%. Seventy-seven percent of respondents (n = 44) indicated that their medical school offered IRs and 12% of respondents (n = 7) indicated that their medical school did not, while six participants did not answer this question. Interviewees for the second stage were identified, and 15 individuals representing 13 medical schools agreed to participate in an interview. Table 1 displays demographic information about respondents and medical schools. Although the demographic information about respondents (eg, staff or faculty role, ethnicity) was not found to be significant in any analysis, it is included to display the types of roles and individuals who fill IR coordinator positions.
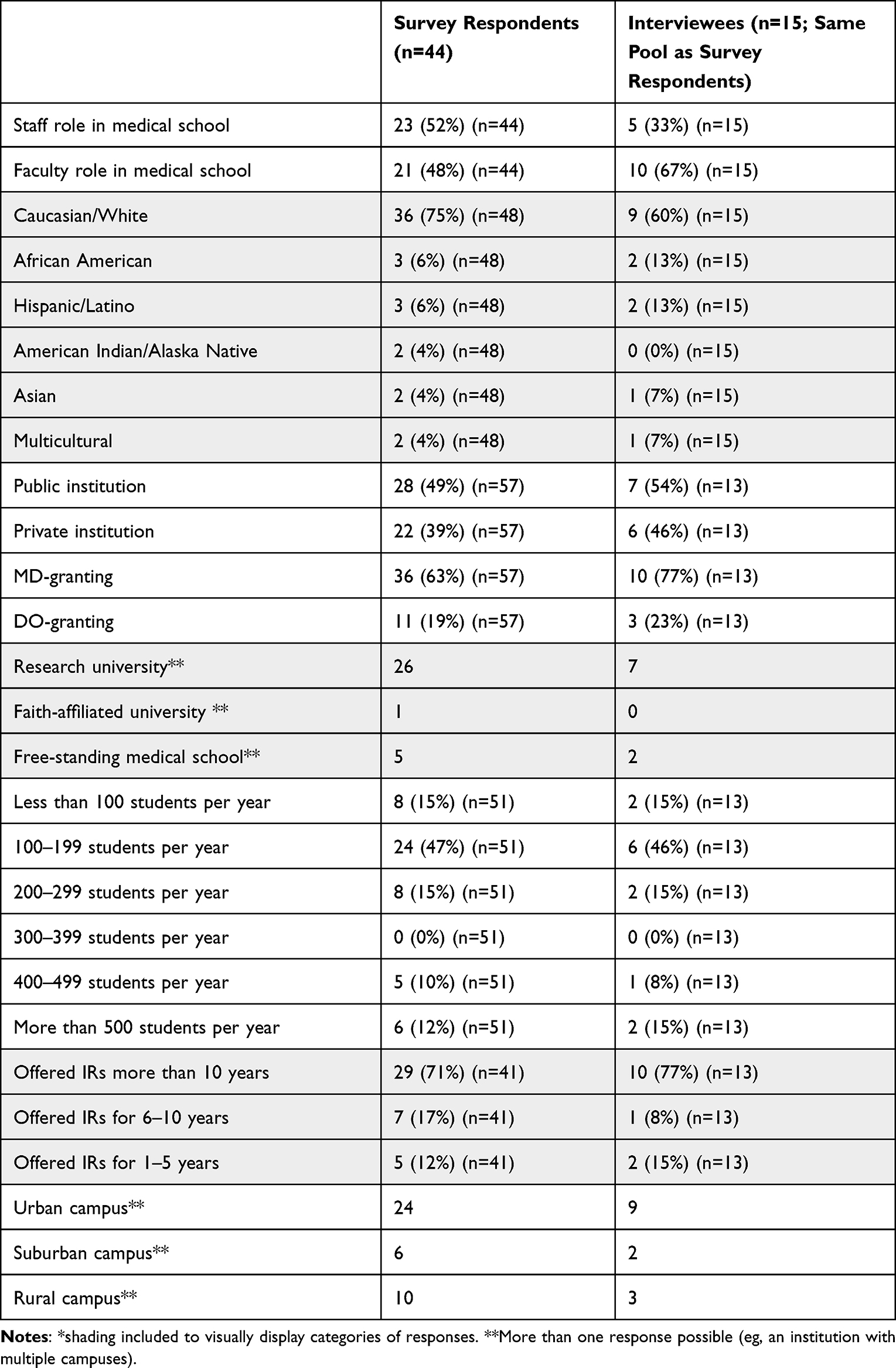 |
Table 1 Demographics of Study Participants and Institutions* |
Features of IRs
Most respondents (72%, n = 31) indicated that the duration of an IR at their medical school was one to three months. No respondents indicated rotations longer than three months; 23% (n = 12) indicated IRs of less than one-month duration. Three-quarters of respondents (n = 32) indicated IRs occurred mostly in low-income countries in their program; 16% of respondents (n = 7) in middle-income countries; and 2% of respondents (n = 1) in high-income countries, with 7% of respondents (n = 3) indicating they were unsure or did not know where most IRs occurred in their medical program. Most respondents (54%; n = 23) indicated that students tend to take one IR during medical school, while 40% (n = 17) indicated that students tend to take two IRs.
For an overwhelming majority of medical schools in this study, students take IRs as elective components of medical training rather than as a requirement (93%, n = 40); 7% of respondents (n = 3) indicated that they offered IRs as both required and elective rotations. No respondents indicated that they offered IRs as required rotations only. Electives tended to occur in the third and fourth year of medical training (70%, n = 28). The activities included in IRs are summarized in Table 2, and Table 3 displays the frequency at which certain program characteristics were represented in the curriculum.
 |
Table 2 Number of Medical Schools That Include Listed Activities in International Rotations |
 |
Table 3 Frequency at Which Program Characteristics Occur in International Rotations |
Interview data revealed greater variety in the ways IRs are designed and implemented. IRs differed from being completely student-designed, tailored to individual student needs, or standardized within the medical school. Relationships between medical institutions and host sites could be formal connections with memorandums of understanding (MOU), informal connections based on relationships with faculty members or students from the host country, or almost nonexistent except for connections to a third-party organization (TPO) which organizes and manages the logistics for students in place of the medical school.
Third- and fourth-year medical students were more likely to have longer IRs, such as four to six weeks, perform more clinical activities, and travel individually. First- or second-year medical students tended to have IRs for two to four weeks, sometimes without receiving academic credit, and performed more community service-based, observational, or research-related activities and traveled in groups. The timing of IRs during the four-year experience varied and often was constrained by testing or scheduling conflicts. Interviewees frequently expressed desire to match the capacity of the host site so students could reasonably and appropriately perform activities to match the host site’s needs. IRCs emphasized safety and supervision for all students. Table 4 contains information on each of the thematic components of IRs, along with illustrative quotations.
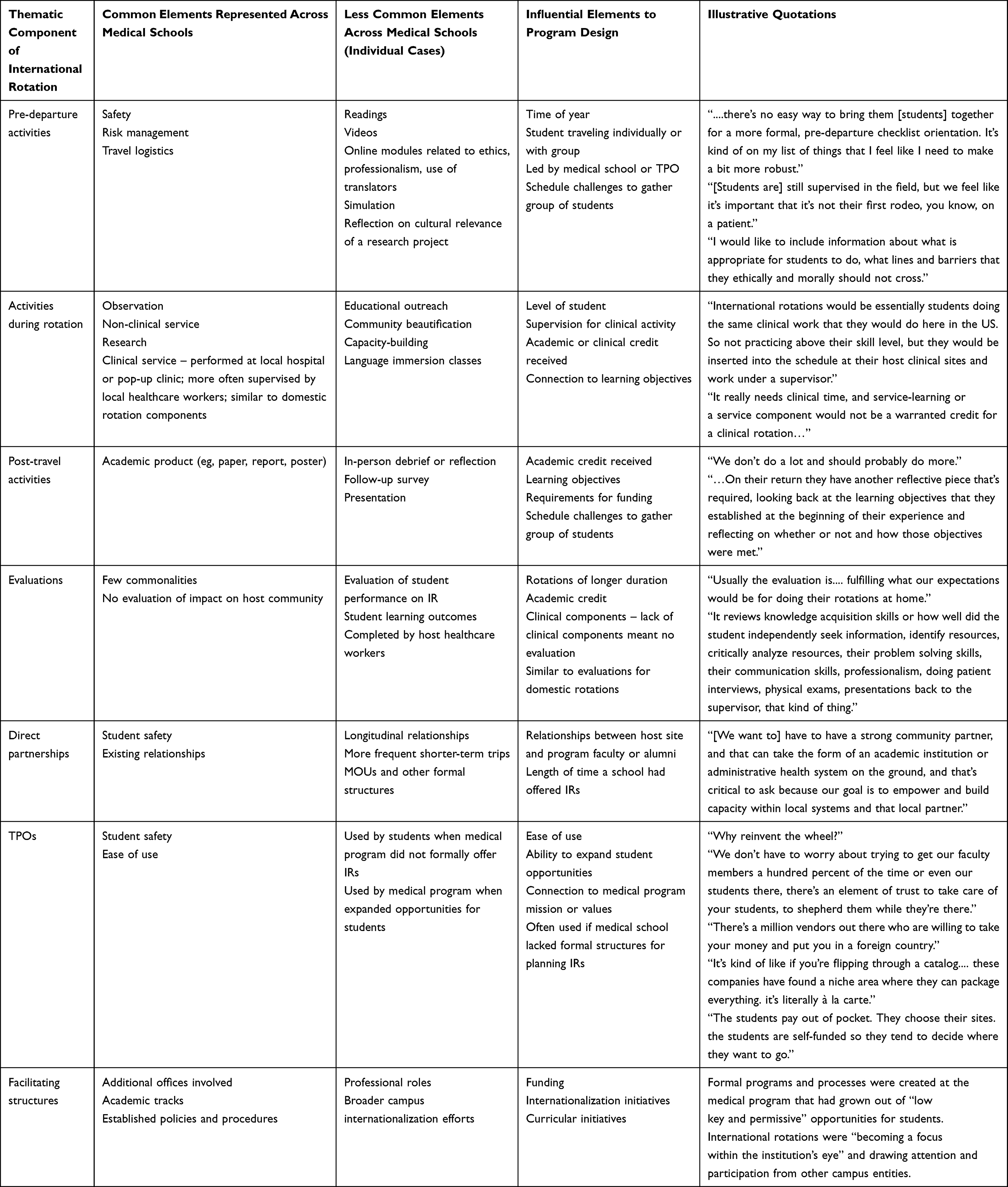 |
Table 4 Thematic Components of International Rotations |
Rotation Components
Rotation components across medical schools varied greatly and depended on motivation and capacity of IRCs to develop or include certain components. Activities were largely clinical and were almost always supervised by preceptors or mentors from the international site (95%, n = 41) or preceptors or mentors from the home program (72%, n = 31); in some cases, both. One interviewee stated, “International rotations would be essentially students doing the same clinical work that they would do here in the US.” Less than half of the medical schools included non-clinical service projects in IRs. Table 4 illustrates the variation in pre- and post-travel activities as well as clinical or non-clinical elements of the rotation.
Partnership with Host Site
There was significant variation in approaches to partnering with host sites, depending on intentions and design decisions made by IRCs. Programs varied from having reciprocal, one-to-one exchanges with medical schools in other countries to choosing sites based on community need; from having loose, informal relationships to having formal relationships with MOUs, or any combination referenced. The only element in common across medical schools was the prioritization of student safety when selecting host sites.
Participants described influential elements of a direct partnership, such as reciprocity, alignment of values, and ability to meet community needs, as well as formal, structured processes such as MOUs or financial stake in the site. Aspects that were described as informal or less structured with lower investment in the site from the medical school could jeopardize the sustainability of partnerships, as interviewees noted. One interviewee, represented in Table 4, noted that goals of creating a partnership included empowering and building capacity at IR sites.
Third-Party Organizations
Programs often used third-party organizations (TPOs), generally non-governmental organizations (NGOs), to send students on rotations where the medical school had no other relationship to the host site. In this study, TPOs tended to be used by smaller medical schools, though most programs in this study used TPOs in some capacity. Far fewer medical schools indicated working with faith-based organizations, private companies, or for-profit companies than NGOs.
IRCs described planning logistics of IRs as time consuming and difficult. Interviewees commented that TPOs can offer established programming and, in most cases, room and board, cultural activities, and insurance, although prices for TPOs can vary greatly. Some rotation experiences offered through TPOs, as described by interviewees, also included public health components or language immersion, which medical schools may not offer, or accommodate larger volumes of students.
Many interviewees commented on dangers of the transactional nature when students utilize TPOs, with one interviewee commenting, “There’s a million vendors out there who are willing to take your money and put you in a foreign country.” TPOs were described to be frequently more expensive for students to use and may not all operate within ethical norms of the profession. There may be no vetting process of the student to ensure the student’s preparation for the experience, or care taken to establish a mutual relationship with a host site. Interviewees also expressed varying opinions of TPOs that organize IRs, from the idea that certain organizations offer a “gold standard” for the field of global health to the opinion that organizations are only “in it for the money” (see Table 4).
Supporting Structures and Programmatic Components
Survey respondents were asked to name up to three offices engaged in planning or implementing IRs in collaboration with the medical school, and to leave blank if none. Twenty-two respondents (39%) indicated additional offices were engaged in planning or implementing IRs; the most common were university international offices such as study abroad, global health offices, and academic affairs in the medical school. In general, respondents also indicated that facilitating elements at their medical schools included factors related to leadership or student support (administrative or leadership support, high student interest), funding, and infrastructure (dedicated offices, academic tracks, school mission, established processes). Other supportive programmatic features were the creation of new curricula requiring or encouraging IRs, like medical language programs, global health certificates, or academic concentrations. One interviewee described the growth from “low key and permissive” opportunities for students into more formal programs, processes, and policies.
Additional Perspectives of IRs
IRCs interviewed for this study characterized IRs as avenues to introduce students to global health careers. The length of time of rotations, included activities, and academic credit requirements were factors that distinguished IRs from other international activities such as “mission trips” or “service trips.” Interviewees framed shorter-term IRs as opportunities for exposure to elements of global health careers and stated that short-term experiences may be more feasible in student schedules, more realistic for student comfort levels, and could occur in the context of longitudinal partnerships with host sites.
How a medical school defines and creates IRs might also differ from how students might engage as international activities. This was most evident at medical schools at which IRCs indicated had no formal IRs despite a high level of student interest in international activities. An IRC from a school that did not offer IRs indicated that students could pursue international activities on their own: they independently located host sites, determined the activities they would perform, and arranged their own travel and logistics.
Discussion
Our study aimed to characterize IRs in medical schools in the US. Since IRs are not required explicitly by medical licensure or accreditation standards,24 and have no standardized, national competencies, it is not surprising to find variety between medical schools in how IRs are designed, implemented, and supported, if included in the medical curriculum at all. There has also been no consensus formed to date in the literature around optimal length of time spent in a rotation, features of programs, impact on community and host partners, and impacts of long-term programs on participants and communities. These variations make it difficult to propose any broad generalizations about the key characteristics of IRs but demonstrate that there are many interconnected component parts that can influence how IRs are designed and implemented, particularly those referenced in Table 4. There is an urgent need to specify pedagogical models, curricular elements, and ethical frameworks of IRs lest these perpetuate concerns of colonialist and “savior” mentalities amongst learners and medical schools.
Although IRs are common in undergraduate medical education, our study showed that they have yet to be positioned as core academic programming within medical schools, leading to greater challenges in planning and implementation. Scheduling and financial concerns prevent IRs from being required at most medical schools. Our study shows that elective IRs are not standardized across medical schools with immense variations in rotation components. Additionally, when students self-fund IRs, medical schools often appeared to have less control over where, when, and how a student would implement the rotation.
The use of TPOs was notable in our study, something prior studies have not addressed. Currently, this is an unregulated industry. It will be important for medical schools that use TPOs to evaluate them carefully to ensure optimum and ethical conduct of IRs.
Medical schools should review tenets of experiential learning when designing and implementing IRs. Experiential learning theory states that preparation before an IR is a critical feature to include for student learning; specifically, preparatory activities that connect to the educational objectives for the experience, as well as post-experience reflection activities.25–29 Our study showed that such activities were few and were included by an IRC’s initiative rather than in a standardized curricular framework. Clinical components performed during IRs were often like clinical rotations a student would have otherwise experienced at their home institutions. Despite evidence that international experiential learning can produce outcomes not as effectively attained in domestic settings,4,5,7 including less reliance on diagnostic technology which promotes greater critical thinking,30 our study questions whether students receive greater learning benefit in international locations if the activities performed are the same as what students would do at home sites.
Scholars have cautioned practitioners against applying practices across settings without considering local context.31 Recent research has also reviewed global health activities through an ethical lens connecting IRs to the social contract, an implicit agreement between medical schools and society that grants physicians autonomy, self-regulation, and status in return for competent and responsive service to society.32,33 During IRs, the society that assumes the risk and inconvenience involved in training will not benefit from students’ future service as health professionals.34 Rather than including clinical components identical to those performed during a domestic rotation, medical schools can explore nonclinical and systems-based learning in international contexts,34 which teaches skills that students can apply in any setting and fulfills the social contract without creating undue burden on host communities to supervise clinical education.
Several interviewees referenced goals for engaging students in IRs as improving health equity, reducing disparities, and serving vulnerable populations in rural, low-income, or other underserved areas. This mission could drive medical schools to seek out opportunities in lower-income countries, although there are arguably many areas of need across the United States as well. Medical students are not considered members of the core health-care workforce while completing clinical rotations in the US and operate under a supervisory structure carefully vetted by medical schools. IRs in our study indicated that they considered host-country “needs” and students who could fit those capacities. This premise is concerning as medical students from the US, with varied levels of exposure to clinical sciences, should not be considered as fulfilling health worker functions of host communities. Doing so could contribute to concerns of neo-colonialism in global health, undermining of local health systems, and perpetuation of inequalities.35
Our study did not reveal formalized evaluation processes of IRs. Regular evaluation of partnerships and outcomes is a principle for institutionalizing relationships.36 Such evaluations should include an examination of structural features, like MOUs or a financial stake in the site, which are related to creating and maintaining partnerships.25,37–40 Evaluation of outcomes related to student learning and the impact on the community provides key information partnership maintenance. Evaluating these may also reveal potential power imbalances between medical schools and host sites or between personal relationships between learners and teachers and help guide medical schools from transactional relationships41 to reciprocal relationships of mutuality.42 Evaluation also provides insight into areas for change within medical schools and data regarding effectiveness of particular educational innovations;43,44 however, if evaluation components for IRs are the same as for domestic rotations, medical schools may lose the opportunity to evaluate the effectiveness of student learning in international settings.
Our study shows that many design elements of IRs depend on individual IRCs who plan and implement IRs, since participants indicated they were not aware of standardized options of IRs across medical schools. Although some resources exist for planning international experiences, they tend to be specialty-specific or aimed at residents45,46 rather than resources for undergraduate medical students. Given the influence of IRCs demonstrated in this study, medical schools could utilize IRCs as levers for change by providing training or encouraging the pursuit of professional development related to best practices and ethical guidelines for IRs.
IRs present a unique opportunity to evaluate student learning in international contexts, and medical schools can redesign evaluations to match this context rather than use existing evaluations generally used for domestic rotations. Evaluations should also explore the impact of IRs on host communities, which provides information to contribute to sustainability of partnerships.
The COVID-19 pandemic had a significant impact on medical schools and international medical education experiences, interrupting student exchange and training programs.47 Medical schools explored virtual rotation options, which disrupted the status quo of traditional didactic learning but still required real-world situations and learning.48 Despite the promises of virtual learning, community engagement strategies and skills remained critical for medical schools to respond to the novel public health crisis, counter disinformation, and expand health literacy.45,49 Community partnerships and the skills necessary for navigating a changing and diverse world remain as important as ever, and international rotations have been suggested as a way to expose medical students to these tenets.50
Future Research
Future research on IRs should explore best practices for pre-departure preparation, post-travel debriefing, and evaluation of student activity as well as impact on the host site. It should also investigate how particular components in IRs affect student outcomes or impacts on host sites. Our study also implied that in many cases, a student performs activities on the IR similar to the types of activities performed at the home institution on a similar rotation. Future studies should explore how learning opportunities at international sites differ from domestic settings and examine unique elements about the environment of low-income countries as opposed to middle- or high-income countries.
Aspects of partnerships between medical schools and host communities should also be a focus, to determine which factors contribute to effective and sustainable partnerships. Examinations of the institution’s stake in a partnership, financial or otherwise, also provides information regarding sustainability of partnerships even in the face of challenging circumstances, such as safety or funding concerns.
Limitations
With any survey research, frequencies may be overstated or not representative due to non-respondents, or discrepancies may be created by various interpretations of study terms. Additionally, the sampling method may exclude participants if IRs are not organized under academic or co-curricular units. Although there was an acceptable response rate to the survey, the data do not necessarily represent perspectives of all medical schools in the U.S, which may be influenced by contexts not represented in this data. Due to time and resource constraints, the focus on organizational and institutional perspectives, and the exploratory approach, the key perspective of community host populations could not be included in this study.
Conclusion
Although there is no scholarly consensus regarding the elements of IRs, such as length of time in the rotation or curricular features, medical schools are adopting IRs at a rapid pace in response to pressures that have led to the expansion of community-based learning opportunities. Our study revealed that there is no standardization of IRs across medical schools and immense variation in rotation components. Medical schools should create curricular frameworks that include preparatory activities connected to learning objects, post-experience reflection activities, and evaluations of the experience. Medical schools can also consider nonclinical and systems-based learning in international contexts to lessen the burden on host communities to supervise clinical education. Additionally, the use of TPOs was notable in our study, and is an area ripe for future study. Future research should also include exploration of best practices and aspects of sustainable partnerships between medical schools and host communities.
Similar pressures that affect medical education, such as globalization and a need to integrate international health perspectives into training, also affect other health professions.51,52 Given both the similar contexts affecting the fields and the growing inter-professionalization of health fields, our study offers lessons for additional health professions as IRs continue to across educational programs.
Previous Presentations
None. This manuscript has not been previously published and is not under consideration in the same or substantially similar form in any other journal.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon request. The survey and interview protocol for this study are attached as appendices and are available.
Ethical Approval
This study was deemed exempt by the University of Minnesota Institutional Review Board as it is not research involving human subjects as defined by DHHS and FDA regulations (STUDY00004201).
Consent to Participate
All study subjects were informed of the purpose of the study and consented to participate in the survey and/or follow-up interviews.
Consent for Publication
The authors grant consent to publish this manuscript as presented. Participant consent included publication of anonymized responses.
Acknowledgments
The authors would like to acknowledge Andrew Furco, Chris Johnstone, and Tania Mitchell for their support of this study. The authors would also like to thank all study participants for their invaluable participation, as well as those who provided early feedback on the design of this study: Judith Lasker, Mellissa Withers, Jess Evert, Shannon Benson, Cindy Howard, and Tricia Todd. This study stemmed from dissertation research carried out in 2018–2019.53
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
None. The authors report no conflicts of interest in this work.
References
1. Gregg J, Saha S. Losing culture on the way to competence: the use and misuse of culture in medical education. Acad Med. 2006;81(6):1. doi:10.1097/01.ACM.0000225218.15207.30
2. Hartman E. Community-engaged scholarship, knowledge, and dominant discourse: a cautionary tale from the global development sector. J Leadersh Stud. 2017;1(1):1.
3. Irby D, Cooke M, O’Brien B. Calls for reform of medical education by the Carnegie Foundation for the advancement of teaching: 1910 and 2010. Acad Med. 2010;85(2):220–227. doi:10.1097/ACM.0b013e3181c88449
4. Bringle R, Hatcher J. International service learning. In: Bringle R, Hatcher J, Jones S, editors. International Service Learning: Conceptual Frameworks and Research. Virginia: Stylus Publishing; 2011:3–28.
5. Jones S, Steinberg K. An analysis of international service learning programs. In: Bringle R, Hatcher J, Jones S, editors. International Service Learning: Conceptual Frameworks and Research. Virginia: Stylus Publishing; 2011:89–112.
6. Plater W. The context for international service learning: an invisible revolution is underway. In: Bringle R, Hatcher J, Jones S, editors. International Service Learning: Conceptual Frameworks and Research. Virginia: Stylus Publishing; 2011:29–56.
7. Tonkin H. A research agenda for international service learning. In: Bringle R, Hatcher J, Jones S, editors. International Service Learning: Conceptual Frameworks and Research. Virginia: Stylus Publishing; 2011:191–224.
8. Thompson MJ, Huntington MK, Hunt DD, Pinsky LE, Brodie JJ. Educational effects of international health electives on U.S. and Canadian medical students and residents: a literature review. Acad Med. 2003;78(3):342–347. doi:10.1097/00001888-200303000-00023
9. Lasker JN. Hoping to Help: The Promises and Pitfalls of Global Health Volunteering. Ithaca, New York: Cornell University Press; 2016.
10. DeCamp M. Scrutinizing global short-term medical outreach. Hastings Cent Rep. 2007;6:21–23. doi:10.1353/hcr.2007.0096
11. Sullivan N. Hosting gazes: clinical volunteer tourism and hospital hospitality in Tanzania. In: Prince R, Brown H, editors. Volunteer Economies: The Politics and Ethics of Voluntary Labour in Africa. Rochester. NY: James Currey; 2016:140–163.
12. Imperato PJ, Bruno DM, Sweeney M. Ensuring the health, safety and preparedness of U.S. medical students participating in global health electives overseas. J Community Health. 2016;41:442–450. doi:10.1007/s10900-016-0169-7
13. McKinley DW, Williams SR, Norcini JJ, Anderson MB. International exchange programs and U.S. medical schools. Acad Med. 2008;83(10 Suppl):S53–S57. doi:10.1097/ACM.0b013e318183e351
14. Heck JE, Wedemeyer D. International health education in US medical schools: trends in curriculum focus, student interest, and funding sources. J Fam Med. 1995;27(10):636–640.
15. Holmes D, Zayas L, Koyfman A. Student objectives and learning experiences in a global health elective. J Community Health. 2021;37:927–934. doi:10.1007/s10900-012-9547-y
16. Stewart T, Wubbena Z. An overview of infusing service-learning in medical education. Int J Med Educ. 2014;5:147–156. doi:10.5116/ijme.53ae.c907
17. Stewart T, Wubbena Z. A systematic review of service-learning in medical education: 1998–2012. Teach Learn Med. 2015;27(2):115–122. doi:10.1080/10401334.2015.1011647
18. Qualtrics, provo, UT, USA. Available from: https://www.qualtrics.com.
19. SPSS, IBM Corp. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp; 2017.
20. NVivo 11. QSR international. Available from: http://www.qsrinternational.com/products_nvivo.aspx.
21. Cooper S, Endacott R. Qualitative research: specific designs for qualitative research in emergency care? Emerg Med J. 2007;24:816–819. doi:10.1136/emj.2007.050641
22. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
23. Thorne S, Kirkham S, MacDonald-Emes J. Interpretive description: a noncategorical qualitative alternative for developing nursing knowledge. Res Nurs Health. 1997;20:169–177. doi:10.1002/(SICI)1098-240X(199704)20:2<169::AID-NUR9>3.0.CO;2-I
24. Liaison Committee on Medical Education. Functions and structure of medical school: standards for accreditation of medical education programs leading to the M.D. degree; 2018. Available from: http://www.lcme.org/functions2008jun.pdf.
25. Bringle R, Hatcher J. Institutionalization of service learning in higher education. J Higher Educ. 2000;71(3):273–290. doi:10.2307/2649291
26. Dewey J. Experience and Education. New York City, NY: Collier Books; 1938.
27. Giles D, Eyler J. The theoretical roots of service-learning in John Dewey: toward a theory of service-learning. Mich J Community Serv Learn. 1994;1(1):77–85.
28. Kolb DA. Experiential Learning: Experience as the Source of Learning and Development. Englewood Cliffs, NJ: Prentice-Hall; 1984.
29. Seifer S, Hermanns K, Lewis J. Introduction. In: Seifer S, Hermanns K, Lewis J, editors. Creating Community-Responsive Physicians: Concepts and Models for Service-Learning in Medical Education. Washington, DC: American Association for Higher Education; 2000:43–54.
30. Drain P, Primack A, Hunt D, Fawzi W, Holmes KK, Gardner P. Global health in medical education: a call for more training and opportunities. Acad Med. 2007;82(3):226–230. doi:10.1097/ACM.0b013e3180305cf9
31. Buck S. Service learning as local learning. In: Bringle R, Hatcher J, Jones S, editors. International Service Learning: Conceptual Frameworks and Research. Virginia: Stylus Publishing; 2011:125–144.
32. McCurdy L, Goode LD, Inui TS, et al. Fulfilling the social contract between medical schools and the public. Acad Med. 1997;72(12):1063–1070. doi:10.1097/00001888-199712000-00016
33. Wasylenki D, Byrne N, McRobb B. The social contract challenge in medical education. Med Educ. 1997;31(4):250–258. doi:10.1111/j.1365-2923.1997.tb02921.x
34. Prasad S, Sopdie E, Meya D, Kalbarczyk A, Garcia PJ. Conceptual framework of mentoring in low- and middle-income countries to advance global health. Am J Trop Med Hyg. 2019;100(1_Suppl):9–14. doi:10.4269/ajtmh.18-0557
35. Bleakley A, Brice J, Bligh J. Thinking the post-colonial in medical education. Med Educ. 2008;42(3):266–270. doi:10.1111/j.1365-2923.2007.02991.x
36. Torres J, Schaffer J. Benchmarks for Campus/Community Partnerships. Campus Compact; 2000.
37. Butin D. The limits of service-learning in higher education. Rev High Ed. 2006;29(4):473–498. doi:10.1353/rhe.2006.0025
38. Furco A. Institutionalising Service Learning in Higher Education. Higher Education and Civic Engagement: International Perspectives. Burlington, VT: Ashgate; 2007.
39. Holland B. Institutional impacts and organizational issues related to service-learning. Mich J Community Serv Learn. 2007;2007:52–60.
40. Holland B. Will it last? Evidence of institutionalization at Carnegie classified community engagement institutions. New Dir Higher Educ. 2009;2009(147):85–98. doi:10.1002/he.361
41. Clayton PH, Bringle RG, Morrison M. Differentiating and assessing relationships in service-learning and civic engagement: exploitative, transactional, or transformational. Mich J Community Serv Learn. 2010;2010:5–22.
42. Mwangi C. Partner positioning: examining international higher education partnerships through a mutuality lens. Rev High Ed. 2017;41(1):33–60. doi:10.1353/rhe.2017.0032
43. Driscoll A. Carnegie’s community engagement classification: intentions and insights. Change. 2008;40(1):38–41. doi:10.3200/CHNG.40.1.38-41
44. Ramaley JA. Embracing civic responsibility. AAHE Bull. 2000;52(7):9–13.
45. Galiatsatos P, Monson K, Oluyinka M, et al. Community calls: lessons and insights gained from a medical–religious community engagement during the COVID-19 pandemic. J Relig Health. 2020;59:2256–2262. doi:10.1007/s10943-020-01057-w
46. St Clair NE, Abdul-Mumin A, Banker SL, et al. Global guide: a comprehensive global health education resource for pediatric program directors. Pediatrics. 2020;145(2):1. doi:10.1542/peds.2019-2138
47. Bentata Y. The COVID-19 pandemic and international federation of medical students’ association exchanges: thousands of students deprived of their clinical and research exchanges. Med Educ Online. 2020;25(1):5. doi:10.1080/10872981.2020.1783784
48. Almarzooq Z, Lopes M, Kochar A. Virtual learning during the COVID-19 pandemic. J Am Coll Cardiol. 2020;75(20):2635–2638. doi:10.1016/j.jacc.2020.04.015
49. Ojikutu BO, Stephenson KE, Mayer KH, Emmons KM. Building trust in COVID-19 vaccines and beyond through authentic community investment. Am J Public Health. 2021;111(3):366–368. doi:10.2105/AJPH.2020.306087
50. Cherniak WA, Drain PK, Brewer TF. Educational objectives of international medical electives–a narrative literature review. Acad Med. 2013;88(11):1778. doi:10.1097/ACM.0b013e3182a6a7ce
51. Pechak C, Thompson M. A conceptual model of optimal international service-learning and its application to global health initiatives in rehabilitation. Phys Ther. 2009;89(11):1192–1204. doi:10.2522/ptj.20080378
52. Walsh LV. International service learning in midwifery and nursing education. J Midwifery Womens Health. 2003;48(6):449–454. doi:10.1016/S1526-9523(03)00310-6
53. Sopdie EAM Examining the role of international service-learning in American medical education: a national exploratory study [Order No. 13882256] [Doctoral dissertation], University of Minnesota, ProQuest Dissertations and Theses database; 2019.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.