")
Back to Journals » Infection and Drug Resistance » Volume 17
Characteristics of Immunocytes and Cytokines in Patients with Bloodstream Infections Caused by Carbapenem-Resistant Klebsiella pneumoniae in China
Authors Guo W, Lian X, Li H, Jiang L, Chen Y, Shen P, Yu W
Received 24 August 2023
Accepted for publication 2 February 2024
Published 22 February 2024 Volume 2024:17 Pages 719—725
DOI https://doi.org/10.2147/IDR.S431207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Sandip Patil
Wenhui Guo,1,* Xiang Lian,2,* Hong Li,2 Lushun Jiang,1 Yingsha Chen,3 Ping Shen,1 Wei Yu1
1State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Department of Infectious Diseases, The Affiliated Xiangshan Hospital of Wenzhou Medical University; Xiangshan First People’s Hospital Medical and Health Group; Ningbo Fourth Hospital, Ningbo, People’s Republic of China; 3Department of Infectious Diseases, the Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ping Shen; Wei Yu, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Tel/Fax +86 571 87236421, Email [email protected]; [email protected]
Objective: To evaluate the characteristics of immunocytes and cytokines associated with bloodstream infections (BSIs) caused by carbapenem-resistant Klebsiella pneumoniae (CRKP).
Methods: Patients with BSIs K. pneumoniae (BSIs-Kpn) were enrolled in our hospital between 2015 and 2022. Whole blood and serum samples were collected on the first day after diagnosis. Immunocytes and cytokines profiles were assessed using multicolor flow cytometry and multiplex immunoassays, respectively. The test cytokines included interferon-gamma (IFN-γ), tumor necrosis factor-alpha (TNF-α), interleukin (IL)-2, IL-4, IL-6, IL-10, and IL-17A.
Results: A total of 313 patients had BSIs-Kpn, including 145 with CRKP, 43 with extended-spectrum β-lactamases (ESBL) producing Kpn (ESBL-Kpn) and 125 with non-CRKP or non-ESBL-Kpn (susceptible Kpn, S-Kpn). Absolute number of leukomonocyte (CD45+) in CRKP, ESBL-Kpn and S-Kpn were 280.0 (138.0– 523.0) cells/μL, 354.5 (150.3– 737.3) cells/μL, and 637.0 (245.0– 996.5) cells/μL, respectively. Compared with S-Kpn group, the absolute numbers of leukomonocyte (including T lymphocytes, B lymphocytes and natural killer cells) in patients with CRKP were significantly lower than that in patients with S-Kpn (P < 0.01). The levels of cytokines IL-2 and IL-17A were significantly higher in patients with S-Kpn than in those patients with CRKP (P< 0.05). The area under receiver operating curve (AUC) of IL-2, IL-4, and IL-17A for S-Kpn was 0.576, 0.513, and 0.561, respectively, whereas that for the combination of these three cytokines with immunocytes was 0.804.
Conclusion: Patients with BSIs-CRKP had lower leukomonocyte counts. High levels of IL-2 and IL-17A combined with immunocyte subpopulations showed relatively high diagnostic value for BSIs-S-Kpn from BSIs-CRKP.
Keywords: Klebsiella pneumoniae, immunocytes, IL-2, IL-4, IL-17A
Introduction
Bloodstream infections (BSIs) caused by Klebsiella pneumoniae (BSIs-Kpn), especially carbapenem-resistant Kpn (CRKP), are potentially life threatening to public health.1–3 BSIs-Kpn are responsible for 7.2% and 8.8% of community- and hospital-onset BSIs.2 Between 2014 and 2019, the number of BSIs-CRKP in China increased substantially from 7.0% to 19.6%.3 Previous studies have indicated that BSIs-CRKP are associated with increased morbidity and mortality.4–6 Recent data reported that the age-standardized mortality rate of BSIs-Kpn was 3.5% of all deaths caused by 33 bacterial pathogens in 2019.7 However, in China, the mortality rate of BSIs-CRKP has increased from 33.3% in 2012 to 42.8% in 2019.8
Owing to the lack of appropriate antibiotic options, BSIs-CRKP have become a great challenge for clinicians.4,5 Fortunately, the development of novel antibiotics has opened new prospects for combating BSI-CRKP. However, resistance to novel β-lactam/β-lactamase inhibitor combinations has been reported.9 Therefore, it is important to explore the interactions between the host and the CRKP proteins. Most evidence has shown that CRKP can hide its pathogen-associated molecular patterns and induce adaptive costs to regulate immune evasion, resulting in CRKP with long-term survival in the host.10–12 In addition, cytokines play a key role in the immune response to Kpn.13 Herein, we conducted integrated immunology and microbiology analyses to investigate the differences in the inflammatory response among CRKP, extended-spectrum β-lactamases (ESBL) producing Kpn (ESBL-Kpn), and non-CRKP or non-ESBL-Kpn (susceptible Kpn, S-Kpn).
Methods
Study Population
This study was an observational analysis. The clinical diagnosis of BSIs-Kpn among adult patients was screened by positive blood culture at The First Affiliated Hospital, Zhejiang University School of Medicine, from 2015 to 2022. The patients with fungal, viral or mixed bacterial co-infection were excluded. The medical records of patients included demographics, and laboratory examination.
Whole blood and serum samples were collected on the first day after diagnosis. Antibiotic susceptibility tests were performed using standard biochemical methods with VITEK® 2 Compact (bioMérieux, France). Carbapenem resistance was defined as resistance to imipenem, meropenem, or ertapenem according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.14
Analysis of Immunocytes Subpopulations with Flow Cytometry
Peripheral blood samples (7 mL) were drawn from the venous circulation of the BSIs-Kpn. Red blood cells were lysed in whole blood. The absolute counts or percentages of each immunocyte in whole blood were determined using multicolor flow cytometry (TBNK Kit - 6 Color Immunophenotyping Kit, Agilent Technology, United States) with a BD FACS Canto II flow cytometer (BD Biosciences, New Jersey, USA), and the results were analyzed using DIVA software and FlowJo 10.0. Immunocyte subpopulations included mature peripheral T lymphocytes (CD3+), helper T lymphocytes (CD3+CD4+), cytotoxic T lymphocytes (CD3+CD8+), B lymphocytes (CD3-CD19+), and natural killer cells (CD3-CD16+CD56+).
Cytokines Assay
Serum cytokines levels were measured using the Human Th1/Th2 Cytometric Bead Array (CBA) Kit II (Becton Dickinson, CA, USA). Levels of 7 cytokines were measured: interferon-gamma (IFN-γ), tumor necrosis factor alpha (TNF-α), interleukin (IL)-2, IL-4, IL-6, IL-10, and IL-17A. All samples were assayed according to the manufacturer’s instructions. The fluorescence intensity of the beads was measured using a BD FACSCanto II flow cytometer (BD Biosciences). Heat maps of cytokines profile were analyzed using TBtools.15
Statistical Analysis
The abnormal distribution of continuous variables was expressed as median (interquartile range). Cytokines were log10-transformed for statistical analysis. The chi-square test was used for comparisons between different groups. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic value of different cytokines alone or in combination with immunocyte subpopulations in terms of area under the ROC curve (AUC). Statistical significance was defined as a two-tailed P-value of < 0.05. SPSS 23.0, for Windows (SPSS Inc., Chicago, IL, USA) and GraphPad version 8 (San Diego, California, USA) were used to analyze the data.
Results
Study Population
In total, 313 patients with BSIs-Kpn were enrolled in this study. Among these patients, 145 had CRKP, 43 had ESBL-Kpn, and 125 had S-Kpn infections.
A comparison of the demographic characteristics is presented in Figure 1. The BSI-CRKP group consisted of 105 men and 40 women with a mean age of 54±15 years, ranging 18 from 91 years. There were no significant differences in gender, age, tumor incidence rate, white blood cell and hypersensitivity C reactive protein, among CRKP, ESBL-Kpn and S-Kpn groups (P>0.05) (Supplementary Table 1). The level of procalcitonin in patients with CRKP was lower than ESBL-Kpn and S-Kpn (P=0.041).
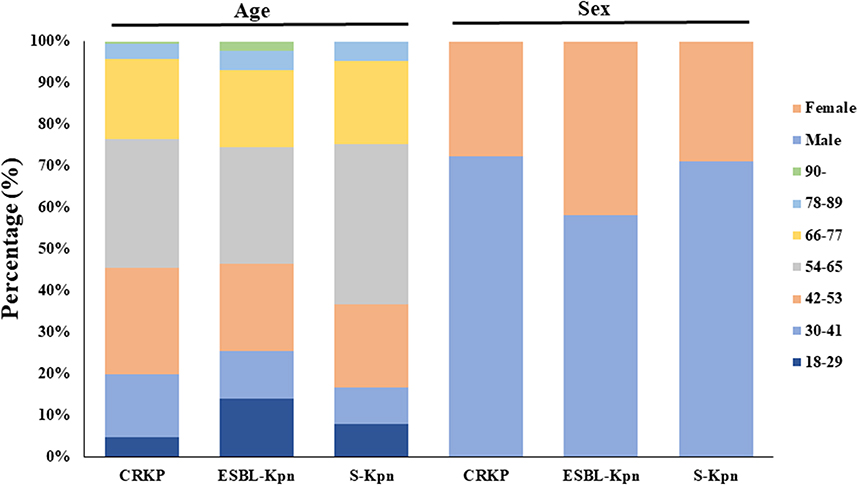 |
Figure 1 Demographic characteristics of included patients with BSIs-Kpn. CRKP, Carbapenem-resistant K. pneumoniae; ESBL-Kpn, extended-spectrum β-lactamases producing K. pneumoniae; S-Kpn, non-CRKP or non-ESBL-Kpn. |
The most common departments of the included BSIs patients with CRKP, ESBL-Kpn, and S-Kpn were hepatobiliary and pancreatic surgery, nephrology, and infectious disease, respectively (Supplementary Figure 1).
Subpopulations of Immunocyte
Immunocyte subpopulations were detected in 237 patients, including 111 with CRKP, 36 with ESBL-Kpn, and 90 with S-Kpn. Absolute number of leukomonocyte (CD45+) in CRKP, ESBL-Kpn and S-Kpn were 280.0 (138.0–523.0) cells/μL, 354.5 (150.3–737.3) cells/μL, and 637.0 (245.0–996.5) cells/μL, respectively (Table 1). Compared with S-Kpn group, the absolute numbers of mature peripheral T lymphocytes (CD3+), helper T lymphocytes (CD3+CD4+), cytotoxic T lymphocytes (CD3+CD8+), B lymphocytes (CD3-CD19+), natural killer cells (CD3-CD16+CD56+) in patients with CRKP were significantly lower (P < 0.01) (Figure 2).
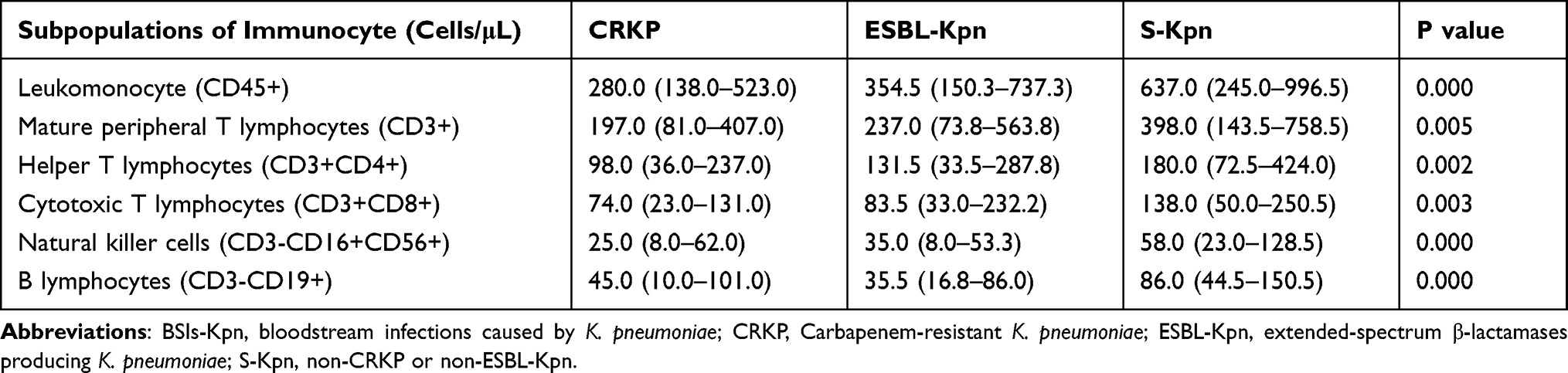 |
Table 1 Absolute Numbers of Immunocyte Subpopulations in Patients with BSIs-Kpn |
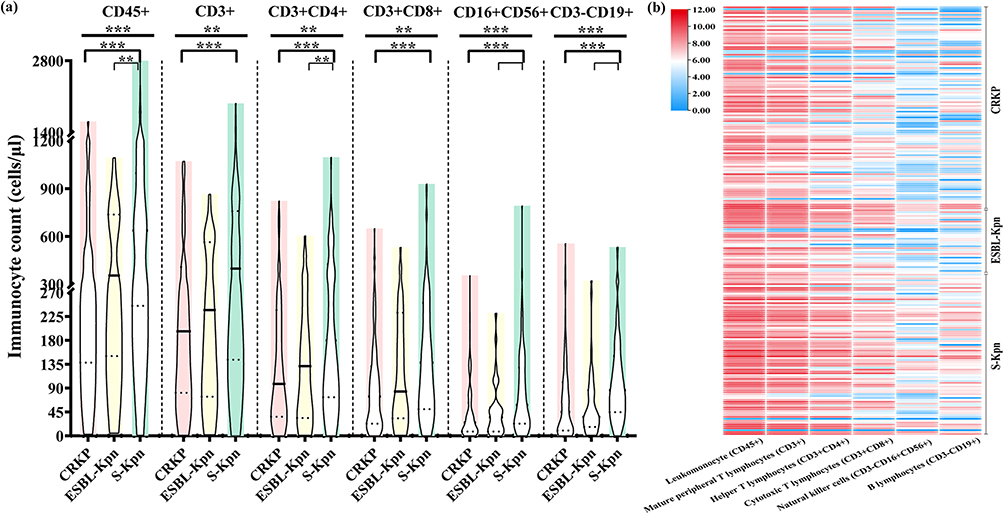 |
Figure 2 Immunocyte subpopulations in patients with BSIs-Kpn. (a) The absolute numbers of immunocyte subpopulations. (b) Heat map of immunocyte for each patient. Solid line represents median, dotted lines represent quartiles. P scales of<0.001 (***), <0.05 (**). |
Cytokines Profile Among the Patient Groups
The concentrations of IFN-γ, TNF-α, IL-2, IL-4, IL-6, IL-10, and IL-17A were assayed in the 145 patients (Figure 3). The levels of cytokines IL-2 and IL-17A were significantly higher in patients with S-Kpn than in those with CRKP (P<0.05) (Table 2). Although no significant difference was found among the three groups regarding the level of IL-6 (P=0.891), the IL-6 level of 113.25 (23.84–419.10) pg/mL in patients with CRKP was higher than that of 57.04 (31.40–297.09) pg/mL in patients with S-Kpn. There was no statistical difference in IL-4 among CRKP, ESBL-Kpn and S-Kpn groups (P=0.121), while the level of IL-4 in S-Kpn group was higher than that in CRKP group (P=0.048). The AUCs of IL-2, IL-4, and IL-17A for S-Kpn were 0.576 (95% CI:0.430–0.721), 0.513 (95% CI:0.368–0.658), and 0.561 (95% CI:0.416–0.705), whereas the AUC for the combination of these three cytokines with immunocytes was 0.804 (95% CI:0.686–0.921) (Supplementary Figure 2).
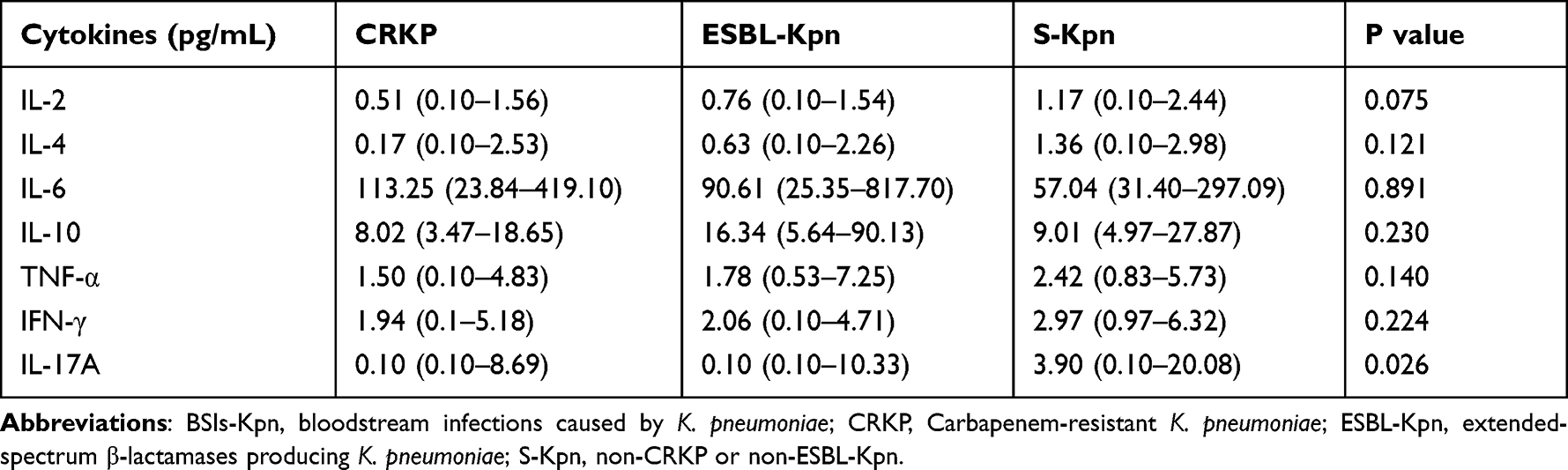 |
Table 2 Cytokines Profile of Patients with BSIs-Kpn |
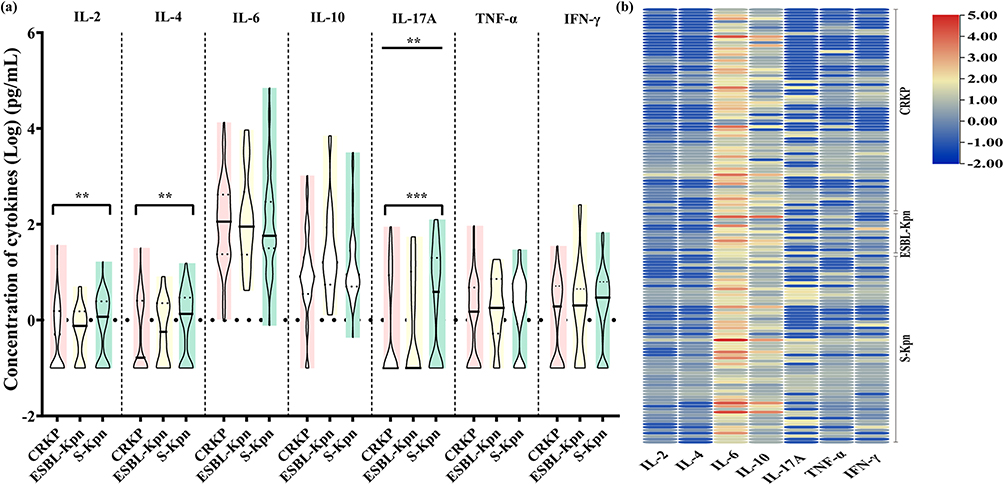 |
Figure 3 Cytokines concentrations in patients with BSIs-Kpn. (a) The concentration of IL-2, IL-4, IL-6, IL-10, IL-17A, IFN-γ, and TNF-α. (b) Heat map of cytokines concentrations for each patient. Solid line represents median, dotted lines represent quartiles. P scales of<0.01 (***), <0.05 (**). |
Discussion
The mortality rate of BSIs-CRKP is as high as 42.8%.8 In the past few decades, novel antibiotics have been used to treat CRKP.16 However, resistance to novel antibiotics has been reported in CRKP.9,17 Several studies have indicated that inflammation plays an important role in the clearance.10–12,18 To date, the correlation between immunocyte subpopulations, cytokines, and CRKP, especially for BSIs, remains unknown. In this study, we examined the levels of five immunocyte subpopulations and seven cytokines in patients with BSI-Kpn. The levels of IL-2 and IL-17A were higher in patients with S-Kpn than in those with CRKP. Additionally, levels of immunocyte subpopulations in patients with CRKP were lower than those in patients with CRKP.
Available research has demonstrated that Kpn can frustrate normal immune responses and capitalize on immunocompromised states, resulting in high mortality.19 Our data indicated that the absolute numbers of immunocyte subpopulations in patients with CRKP were significantly lower than those in patients with S-Kpn. There are two potential reasons for this observation. First, CRKP, isolated from BSIs, can establish protected reservoirs in the host to prevent eradication.19,20 A second possible reason is variations in host immunological defenses against BSIs-Kpn. A recent study showed that decreased complement pathway function is associated with lower survival, more BSIs, and impaired in vitro serum killing of CRKP during critical illness.21,22 Although Kpn possesses several adaptations to evade immunocytes killing, the degree of success of immune evasion differs among CRKP, ESBL-Kpn, and S-Kpn. However, the specific mechanisms involved in this remain unclear. Large-scale clinical studies are needed to explore common and unique strategies for immune evasion among diverse isolates of CRKP, ESBL-Kpn, and S-Kpn to develop novel therapeutic options against BSIs-Kpn.
Cytokines play key roles in both the innate and adaptive immune responses.23 In this study, BSIs-CRKP showed higher IL-6 levels than S-Kpn, although no statistical differences were found. Notably, IL-2, IL-17A and procalcitonin were significantly higher in BSIs patients with S-Kpn than in those with CRKP. Additionally, the AUC for the combination of these three cytokines with immunocytes increased. Consistent with our results, previous studies have shown that S-Kpn infection leads to increased IL-17 levels.24,25 In animal models with Kpn infections, Th17 or IL-17A deficiency could decrease in neutrophil recruitment and result in increased systemic disseminated infection and death.26–28 Therefore, Th17 and IL-17A may have a role in augmenting host defense against S-Kpn.24,28–30 However, research on the differences between CRKP- and S-Kpn-induced IL-17 production is limited. Therefore, dynamic studies of immunocytes and cytokines profiles would be valuable for understanding the interaction between BSIs-Kpn and immune responses.
This study had several limitations. First, the immunocytes and cytokines profiles of the inflammatory response induced by BSIs-CRKP are not dynamic. In addition, there are difficulties in recruiting patients due to bacterial identification and antimicrobial susceptibility testing with certain hysteresis. Therefore, the sample size of this study was limited. However, the results of the present study contribute to the understanding of inflammatory markers in BSIs-Kpn, particularly CRKP.
Conclusions
In conclusion, patients with BSIs-CRKP have low immunity. High expression levels of IL-2 and IL-17A, combined with immunocyte subpopulations, could be used as biomarkers for the diagnosis of BSIs-S-Kpn.
Ethical Approval
The work was in accordance with the Declaration of Helsinki. This study was approved by the recommendations of the Ethics Committee of The First Affiliated Hospital, Zhejiang University School of Medicine with written informed consent from all subjects (Reference Number: 2022337).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Department of Health of Zhejiang province (No. 2023KY713) and Independent Task of State Key Laboratory for Diagnosis and Treatment of Infectious Diseases (No. 2022zz01). The funder had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang M, Earley M, Chen L, et al. Multi-drug resistant organism network investigators. Clinical outcomes and bacterial characteristics of carbapenem-resistant Klebsiella pneumoniae complex among patients from different global regions (CRACKLE-2): a prospective, multicentre, cohort study. Lancet Infect Dis. 2022;22(3):401–412. doi:10.1016/S1473-3099(21)00399-6
2. Holmes CL, Anderson MT, Mobley HLT, Bachman MA. Pathogenesis of gram-negative bacteremia. Clin Microbiol Rev. 2021;34(2):e00234–20. doi:10.1128/CMR.00234-20
3. Chen Y, Ji J, Ying C, et al.; Blood Bacterial Resistant Investigation Collaborative System (BRICS) Study Group. Blood bacterial resistant investigation collaborative system (BRICS) report: a national surveillance in China from 2014 to 2019. Antimicrob Resist Infect Control. 2022;11(1):17. doi:10.1186/s13756-022-01055-5
4. Kern WV, Rieg S. Burden of bacterial bloodstream infection-a brief update on epidemiology and significance of multidrug-resistant pathogens. Clin Microbiol Infect. 2020;26(2):151–157. doi:10.1016/j.cmi.2019.10.031
5. Kohler PP, Volling C, Green K, Uleryk EM, Shah PS, McGeer A. Carbapenem resistance, initial antibiotic therapy, and mortality in Klebsiella pneumoniae bacteremia: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2017;38(11):1319–1328. doi:10.1017/ice.2017.197
6. Chen Y, Ying S, Jiang L, et al. A novel nomogram for predicting risk factors and outcomes in bloodstream infections caused by Klebsiella pneumoniae. Infect Drug Resist. 2022;15:1317–1328. doi:10.2147/IDR.S349236
7. GBD 2019 Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2022;400(10369):2221–2248. doi:10.1016/S0140-6736(22)02185-7
8. Chen J, Ma H, Huang X, et al. Risk factors and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary-care hospital in China: an eight-year retrospective study. Antimicrob Resist Infect Control. 2022;11(1):161. doi:10.1186/s13756-022-01204-w
9. Yu W, Luo Q, Shen P, et al. New options for bloodstream infections caused by colistin- or ceftazidime/avibactam-resistant Klebsiella pneumoniae. Int J Antimicrob Agents. 2021;58(6):106458. doi:10.1016/j.ijantimicag.2021.106458
10. Sá-Pessoa J, Przybyszewska K, Vasconcelos FN, et al. Klebsiella pneumoniae Reduces SUMOylation to limit host defense responses. mBio. 2020;11(5):e01733–20. doi:10.1128/mBio.01733-20
11. Wong Fok Lung T, Charytonowicz D, Beaumont KG, et al. Klebsiella pneumoniae induces host metabolic stress that promotes tolerance to pulmonary infection. Cell Metab. 2022;34(5):761–774.e9. doi:10.1016/j.cmet.2022.03.009
12. Castillo LA, Birnberg-Weiss F, Rodriguez-Rodrigues N, et al. Klebsiella pneumoniae ST258 negatively regulates the oxidative burst in human neutrophils. Front Immunol. 2019;10:929. doi:10.3389/fimmu.2019.00929
13. Feriotti C, Sá-Pessoa J, Calderón-González R, et al. Klebsiella pneumoniae hijacks the Toll-IL-1R protein SARM1 in a type I IFN-dependent manner to antagonize host immunity. Cell Rep. 2022;40(6):111167. doi:10.1016/j.celrep.2022.111167
14. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. 32th informational supplement; 2022. Available from: http://www.clsi.org/.
15. Chen C, Chen H, Zhang Y, et al. TBtools: an integrative toolkit developed for interactive analyses of big biological data. Mol Plant. 2020;13(8):1194–1202. doi:10.1016/j.molp.2020.06.009
16. Papp-Wallace KM. The latest advances in β-lactam/β-lactamase inhibitor combinations for the treatment of Gram-negative bacterial infections. Expert Opin Pharmacother. 2019;20(17):2169–2184. doi:10.1080/14656566.2019.1660772
17. Yu W, Shen P, Chen Y, Zhou K, Chi X, Xiao Y. Epidemiology and genomic characteristics of bloodstream infection caused by carbapenem-resistant Klebsiella pneumoniae with decreased susceptibility to Aztreonam/Avibactam in China. Front Cell Infect Microbiol. 2022;12:926209. doi:10.3389/fcimb.2022.926209
18. Cai S, Paudel S, Jin L, et al. NLRP6 modulates neutrophil homeostasis in bacterial pneumonia-derived sepsis. Mucosal Immunol. 2021;14(3):574–584. doi:10.1038/s41385-020-00357-4
19. Gonzalez-Ferrer S, Peñaloza HF, Budnick JA, et al. Finding order in the chaos: outstanding questions in Klebsiella pneumoniae pathogenesis. Infect Immun. 2021;89(4):e00693–20. doi:10.1128/IAI.00693-20
20. Ernst CM, Braxton JR, Rodriguez-Osorio CA, et al. Adaptive evolution of virulence and persistence in carbapenem-resistant Klebsiella pneumoniae. Nat Med. 2020;26(5):705–711. doi:10.1038/s41591-020-0825-4
21. Bain W, Li H, van der Geest R, et al. Increased alternative complement pathway function and improved survival during critical illness. Am J Respir Crit Care Med. 2020;202(2):230–240. doi:10.1164/rccm.201910-2083OC
22. Birnberg-Weiss F, Castillo LA, Pittaluga JR, et al. Modulation of neutrophil extracellular traps release by Klebsiella pneumoniae. J Leukoc Biol. 2021;109(1):245–256. doi:10.1002/JLB.4MA0620-099R
23. Martynova E, Rizvanov A, Urbanowicz RA, Khaiboullina S. Inflammasome contribution to the activation of Th1, Th2, and Th17 Immune responses. Front Microbiol. 2022;13:851835. doi:10.3389/fmicb.2022.851835
24. Wang F, Xu J, Liao Y, et al. Tim-3 ligand galectin-9 reduces IL-17 level and accelerates Klebsiella pneumoniae infection. Cell Immunol. 2011;269(1):22–28. doi:10.1016/j.cellimm.2011.03.005
25. Lei L, Zhang X, Yang R, et al. Host immune response to clinical hypervirulent Klebsiella pneumoniae pulmonary infections via transcriptome analysis. J Immunol Res. 2022;2022:5336931. doi:10.1155/2022/5336931
26. Ye P, Rodriguez FH, Kanaly S, et al. Requirement of interleukin 17 receptor signaling for lung CXC chemokine and granulocyte colony-stimulating factor expression, neutrophil recruitment, and host defense. J Exp Med. 2001;194(4):519–527. doi:10.1084/jem.194.4.519
27. Nicolò S, Mattiuz G, Antonelli A, et al. Hypervirulent Klebsiella pneumoniae strains modulate human dendritic cell functions and affect TH1/TH17 response. Microorganisms. 2022;10(2):384. doi:10.3390/microorganisms10020384
28. Liu JZ, Pezeshki M, Raffatellu M. Th17 cytokines and host-pathogen interactions at the mucosa: dichotomies of help and harm. Cytokine. 2009;48(1–2):156–160. doi:10.1016/j.cyto.2009.07.005
29. Ye P, Garvey PB, Zhang P, et al. Interleukin-17 and lung host defense against Klebsiella pneumoniae infection. Am J Respir Cell Mol Biol. 2001;25(3):335–340. doi:10.1165/ajrcmb.25.3.4424
30. Chuammitri P, Wongsawan K, Pringproa K, Thanawongnuwech R. Interleukin 17 (IL-17) manipulates mouse bone marrow- derived neutrophils in response to acute lung inflammation. Comp Immunol Microbiol Infect Dis. 2019;67:101356. doi:10.1016/j.cimid.2019.101356
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.