")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Characteristics, Burden of Care and Quality of Life of Next of Kin of People with Dementia Attending Farm-Based Day Care in Norway: A Descriptive Cross-Sectional Study
Authors Taranrød LB , Eriksen S , Pedersen I , Kirkevold Ø
Received 24 June 2020
Accepted for publication 11 September 2020
Published 2 November 2020 Volume 2020:13 Pages 1363—1373
DOI https://doi.org/10.2147/JMDH.S268818
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Liv Bjerknes Taranrød,1,2 Siren Eriksen,1,3 Ingeborg Pedersen,4 Øyvind Kirkevold1,5,6
1Norwegian National Advisory Unit on Ageing and Health, Vestfold Hospital Trust, Tønsberg, Norway; 2University of Oslo, Faculty of Medicine, Oslo, Norway; 3Department of Bachelor Education, Lovisenberg Diaconal University College, Oslo, Norway; 4Department of Public Health Science, Norwegian University of Life Sciences, Ås, Norway; 5Centre of Old Age Psychiatry Research, Innlandet Hospital Trust, Brumunddal, Norway; 6Norwegian University of Science and Technology (NTNU), Department of Health Sciences in Gjøvik, Trondheim, Norway
Correspondence: Liv Bjerknes Taranrød
Norwegian National Advisory Unit on Ageing and Health, Vestfold Hospital Trust, Tønsberg N-3103, Norway
Tel +47 913 70 028
Email [email protected]
Purpose: Caring for people with dementia is often associated with burden of care and may influence the quality of life of the next of kin. The aim of this study was to describe the characteristics of the next of kin to people with dementia attending farm-based day care service (FDC) and identify characteristics associated with burden of care and quality of life (QoL) of next of kin.
Participants and Methods: Ninety-four dyads of people with dementia and their next of kin were included from 25 FDCs in Norway in this descriptive cross-sectional study. The Relative Stress Scale (RSS) and the QoL–Alzheimer’s Disease Scale (QoL-AD) were used as outcomes measures.
Results: The participants consisted of those who lived with a person with dementia (spouse/partner, 62%) and those who did not (children), with significant differences in age, education level, work employment, perceived social support, depression symptoms, burden of care, and QoL. In multiple regression models, RSS and QoL were associated with living with the person with dementia, anxiety symptoms and perceived social support. In addition, RSS was associated with neuropsychiatric symptoms (NPS) in the people with dementia.
Conclusion: Our findings underline the importance of obtaining knowledge about the next of kin’s burden of care and QoL, of people with dementia attending an FDC. This knowledge is essential for those responsible for providing the best possible services for the next of kin and for developing targeted interventions to support the next of kin.
Keywords: dementia, family caregiver, adult day care service, green care
Introduction
Caring for a person with dementia is often associated with negative consequences. The term burden of care, defined as a multidimensional construct that includes mental, physical, social and financial elements, is frequently used to describe the situation of the next of kin.1 The burden of care includes objective and subjective elements. The objective element is associated with the dependency of the person with dementia, the ability to perform activities of daily living (ADL), the number of hours spent daily caring for a person with dementia, and neuropsychiatric symptoms (NPS), which are considered to be the most important predictor of the next of kin`s burden of care.2–5 The subjective element refers to the next of kin’s psychological responses, which can include distress, anxiety, depression, irritation, or feelings of exhaustion related to the person with dementia and the care obligations.3,4,6 The next of kins burden of care may also influence the frequency and severity of NPS in people with dementia.7 Burden of care can have multiple associations – with the female sex, living with a person with dementia, poor physical and mental health, low perceived support, a greater number of hours spent on caregiving, additional poor quality of the relationship with the person with dementia, or inadequate coping strategies.8–13 Although next of kin report burden of care, they also emphasize positive aspects of caring for the person with dementia such as enjoying togetherness and sharing activities, accomplishments and mastery.9,14–16 Both the burden and the positive aspects of caring may influence the quality of life (QoL) for the next of kin.17
QoL is a broad concept reflecting a person’s psychological state, physical health, personal beliefs, and relationships.18 Quality of life has been described as a concept reflecting objective and subjective factors related to generalized psychological well-being, behavioral competence and environment, with self-perception as a main component.19 On average, the QoL of the next of kin of people with dementia is lower compared to the next of kin of those with other chronic disorders.20,21 Several factors may impact the next of kin’s QoL negatively, such as poor physical and mental health, sleep disorders, a lack of respite, and an absence of social support. Furthermore, the next of kin`s QoL may be affected by living with a person with dementia, resulting in a poor relationship with the person with dementia and the person with dementia`s QoL.17,22–24.
To meet the next of kin`s need for information and knowledge, several municipalities in Norway arrange caregiver school and support groups consisting of lectures about dementia and group discussions.25,26
Day care (DC) services have been developed as part of the municipal services26,27 and offer activities for people with dementia and a much-needed respite for the next of kin. DC might provide a feeling of safety and relief, increase motivation and decrease the burden of care.28–30 In Norway, the farm-based day care service (FDC) is an established type of DC. The purpose of regular DC and FDC is to facilitate meaningful activities in a safe environment, improve QoL and provide respite for the next of kin.26,27 FDC is a service with a wide range of activities related to farm buildings, gardens, animals, and outdoor areas. The majority of Norwegian FDCs have people with early-onset dementia or dementia in an early stage as their main target group.31 Both FDC and DC and are found to prevent an increase in the burden of care for the next of kin over time.32 Furthermore, FDC appears to be health-promoting for both the next of kin and the person with dementia.33,34
Reports regarding the next of kin, of people with dementia attending FDC, are sparse. Thus, this study aims to describe the characteristics of the next of kin and investigate their burden of care and QoL. To this end, we have addressed three research questions:
- What are the characteristics of the next of kin?
- Which characteristics are associated with a self-reported burden of care?
- Which characteristics are associated with a self-reported QoL?
Materials and Methods
Study Design
This is a descriptive cross-sectional study of the next of kin of people with dementia attending FDCs across Norway. The study is part of a larger project.35 We hypothesized that the characteristics of the next of kin would be influenced by whether they live with a person with dementia or not,22 and this will be focused on in the analyses.
Inclusion Criteria and Recruitment
Inclusion criteria for participants were as follows:
- Next of kin of a person with dementia living in their own home and attending an FDC for at least three weeks.
- Eighteen years of age or older.
- Physically meets with the person with dementia a minimum of once a week on average. Both next of kin and the person with dementia had to give their consent to participate.
Service providers from 30 FDCs recruited the people with dementia and their next of kin, from January 2017 to January 2018. A total of 169 dyads of people with dementia and their next of kin met the inclusion criteria. Sixty-two of these did not want to participate, and 13 dyads were not invited to participate for other reasons (eg, health issues in the family). In the end, 94 dyads were included from 25 FDCs in Norway, representing 55.6% of those who met the inclusion criteria.
Ethical Aspects
The project was approved by the Norwegian Centre for Research Data (NSD) (no. 49799. The next of kin and the people with dementia received oral and written information about the study and gave their written consent, they were also assured that they could withdraw at any time during the data collection. The next of kin, of people dementia who had reduced capacity to consent, consented on behalf of them. For this study, the next of kin consented on behalf of three persons with dementia. The study was conducted in accordance with the Declaration of Helsinki.
Measures
Sociodemographic data (age, gender, marital status, level of education, and occupational status) were collected. The next of kin were asked whether they were living with the person with dementia or not, their relationship to the person with dementia, if they had hobbies and if they participated in physical activity at least 20–30 minutes a week. In addition, whether they attended caregiver school and support groups, and their respite (ie, the number of days per week the person with dementia was attending FDC/DC) were recorded, as was the length of time the person with dementia had been attending the FDC. The next of kin estimated the number of days they had spent assisting or looking after the person with dementia during the preceding month. In addition, the following questionnaires were used to capture information about the next of kin.
Quality of Life
The Quality of Life–Alzheimer Disease Questionnaire (QoL-AD)36 consists of 13 items. The items are rated on a four-point scale (poor=1, fair=2, good 3, excellent=4), giving a total score ranging from 13 to 52. Scores of <33 and >37 indicate low and high QoL, respectively.37
Burden of Care
The Relative Stress Scale (RSS)38 consists of 15 items, with each rated from 0 to 4 (0=never, 1=rarely, 2=sometimes, 3=frequently, 4=always/to a high degree), giving a sum score ranging from 0 to 60. A score >23 indicates an increased risk of clinically significant psychological distress, and a score ≥30 indicates the person should be referred for psychiatric assessment and treatment when required.39
Anxiety
We used the anxiety part of the Hospital Anxiety and Depression Scale (HAD-A),40 which consists of seven items. The items are scored from 0 (not present) to 3 (considerable), yielding a possible sum score from 0 to 21. A 0–7 score is considered normal, an 8–10 score is a possible case, and a score of ≥11 is defined as anxiety.
Social Support
The Oslo Social Support Scale (OSS-3)41 assesses the participant’s subjective perceived social support. OSS-3 has three questions, with a sum score ranging from 3 to 14. The sum score is grouped into three categories:42 (1) a 3–8 score indicates “poor support,” (2) a 9–11 score shows “moderate support,” and (3) a 12–14 score is a sign of “strong support.”
Depression
The Montgomery Aasberg Depression Rating Scale (MADRS)43 is a ten-item interview-based questionnaire screening for depressive symptoms. Each item yields a score of 0 to 6, and the overall score ranges from 0 to 60. The cut-off score for no depression is 6, 7–19 score indicates mild depression, 20–34 score indicates moderate depression, and 35–60 score indicates severe depression.
The questionnaires used to collect data about people with dementia were:
Neuropsychiatric Symptoms
The Neuropsychiatric Inventory (NPI-12)44 evaluates 12 behavioral domains common in dementia. All items are scored from 0 to 4 and are calculated by multiplying the frequency score by the severity score from 1 to 3. The sum score ranges from 0 to 144.
Function in Everyday Life Activities
The Physical Self-Maintenance Scale (PSMS)45 consists of six items with a sum score ranging from 6 (no impairment) to 30 (total impairment). The Instrumental Activities of Daily Living Scale (IADL) consists of eight items with a sum score ranging from 0 to 31 with increasing impairment. For both scales, a higher score indicates lower functionality.
Cognition
The Clinical Dementia Rating Scale (CDR)46 consists of six items assessing the level of dementia. The CDR sum of boxes (CDR-SOB) was used, with scores ranging from 0 to 18.0. Scores of 0.5–4.0 indicate “questionable cognitive impairment,” scores of 4.5–9.0 indicate “mild dementia,” scores of 9.5–15.5 indicate “moderate dementia,” and scores of 16.0–18.0 indicate “severe dementia”.47
The number of months with dementia symptoms for each person with dementia was also recorded.
Data Collection
The data collection was performed by ten researchers. All completed a one-day training course in the data collection process. In the present study, we used data from the next of kin, and some data from the people with dementia were included in the analysis. The interviews with the next of kin were mainly face to face, but, for practical reasons, six interviews were conducted by telephone.
The next of kin filled out the questionnaires themselves, except for the Montgomery Aasberg Depression Rating Scale (MADRS), which was conducted through interview. Data regarding people with dementia used in this study were obtained through interviews with the next of kin and are described in Measures. More detailed data of people with dementia are described elsewhere.48
Statistics
The descriptive statistical analyses were performed with IBM SPSS ® v 25.0 (Armonk, NY: IBM Corp) and the regression analysis was done with MLwiN v3.05 (Centre for Multilevel Modelling, University of Bristol, UK). Continuous variables were compared with a t-test when normally distributed, or the Mann–Whitney U-test when skewed. Dichotomous variables were compared with the χ2 tests or Fisher’s Exact Test when needed. The next of kin were divided into two groups: those living with the person with dementia (group one); and those not living with the person with dementia (group two). This variable is labeled as “Living” (Yes/No).
Univariate and multiple linear regression analyses were applied to explore associations with the dependent variables RSS score and QoL-AD score and potential explanatory variables. The empty models (no independent variables included) were checked for cluster effect. For RSS; the Intra Class Correlation (ICC) was 10.5%, and for QoL-AD score ICC was 11.7%; thus, all the regression analyses were adjusted for cluster effects. All variables in the regression analyses were checked for multicollinearities and interactions. One interaction was detected between the variables “Living” and MADRS, with the QoL-AD as outcome. The interaction variable (MADRS score x “Living”) was significant in the linear regression analysis (p=0.039), adjusted for MADRS score and “Living.” Thus, the interaction variable was included in the model with QoL-AD as outcome.
The following variables were dichotomized: the “Relation” variable into spouse/partner and children/other, the “Education” variable into primary school/high school and college/university. The dichotomous variables and age were highly correlated with the “Living” variable. Thus, only “Living” is used in the regression analyses. Also, the IADL and PSMS variables were highly correlated, with the IADL variable being used in the regression analyses. The Caregivers school and Support group variables were merged into a variable called “Caregiver school.”
The variable “Respite days per week” includes FDC and DC that the person with dementia attended.
Missing values in the different assessment forms were imputed on the item level for the cases with at least 50% of the items available. Imputed values were random numbers drawn from the observed distribution in the dataset. The items most imputed are RSS (6 cases), QoL-AD (5 cases), MADRS (4 cases), and OSS-3 (4 cases).
Having only 94 cases placed a limitation on how many independent variables could be included in the multiple regression models.49 To reduce the number of variables in the multiple regression models, variables with p ≥ 0.20 for RSS score and QoL-AD score in the univariate model were excluded in the multiple regression models.
Results
After dividing the next of kin into the two groups, group one – those living with a person with dementia – was found to consist solely of spouses/partners. Conversely, group two – those not living with the person with dementia – consisted mainly of children (81%) (Table 1). Compared with group two, the next of kin in group one were significantly older, had less education, were significantly less likely to be employed outside the household, and with a significantly lower reported weekly physical activity. The groups differed in mean score on perceived social support (OSS-3), with group two being significantly higher. On closer inspection, in group one 85.5% showed an OSS-3 score ≥ 9, whereas in group two, 89.5% had an OSS-3 score ≥ 9, indicating a moderate or better perceived social support.
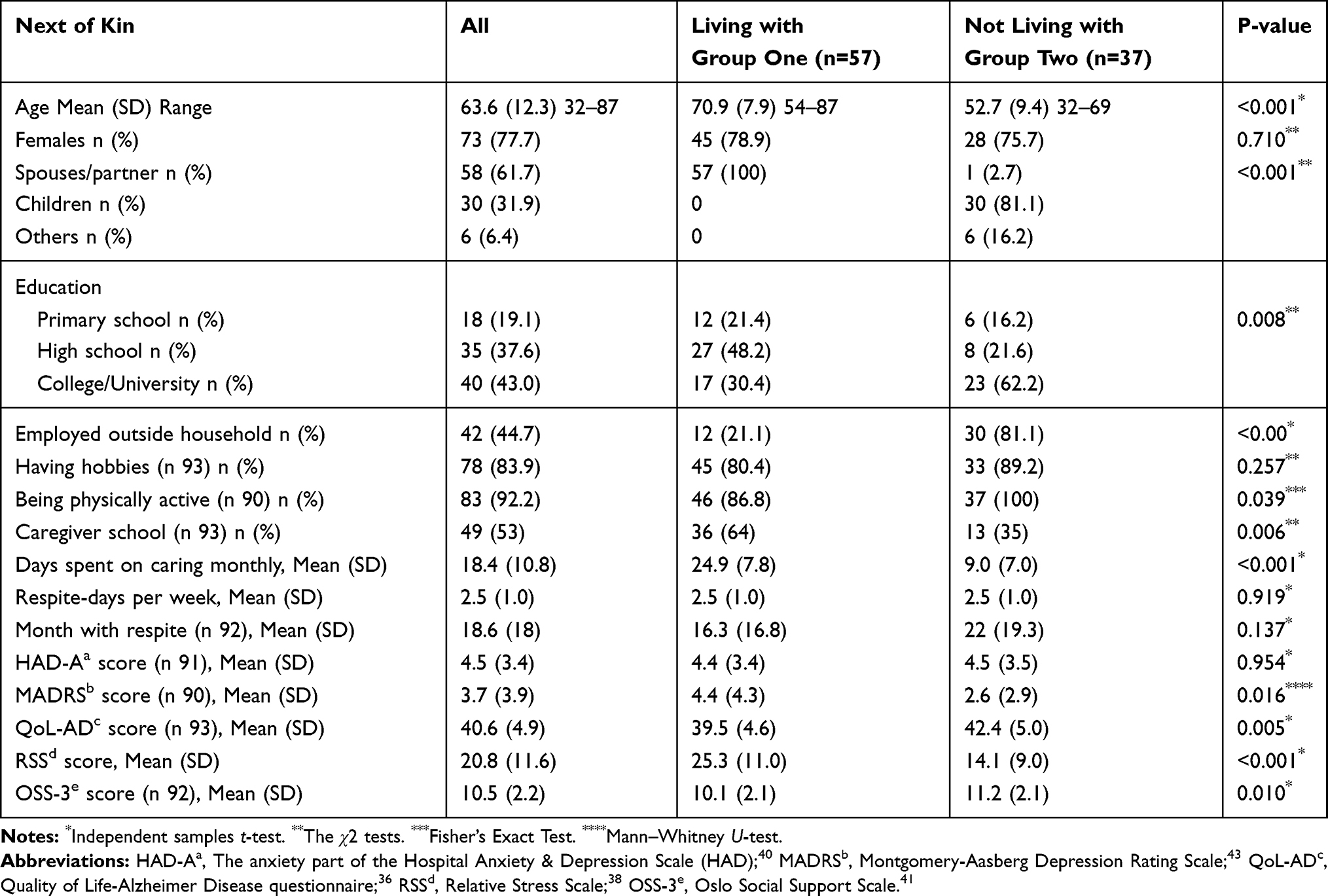 |
Table 1 Characteristics of the Next of Kin (N= 94) |
A significantly larger proportion of the next of kin in group one had attended a caregiver school/support group (64%) compared with those in group two (35%). Group one had a significantly higher mean score on both MADRS and RSS scores and a significantly lower QoL-AD score (Table 1). When looked at in more detail, in group one, 67.9% had a QoL-AD score of ≥ 37; while in group two it was 89.2%, indicating a good QoL. Of all the next of kin, only four reported a score of ≤ 33 indicating a low QoL. In group one, 53.6% had an RSS score of > 23, indicating a high level of burden, whereas the remaining participants scored <23, indicating a low level of burden. In group two, 13.5% had an RSS score of > 23, and 86.5% scored <23.
The analyses of the characteristics of people with dementia are listed in Table 2. The people with dementia living with a next of kin had a significantly higher CDR-Sob score and IADL scores than those who did not share a household with their next of kin.
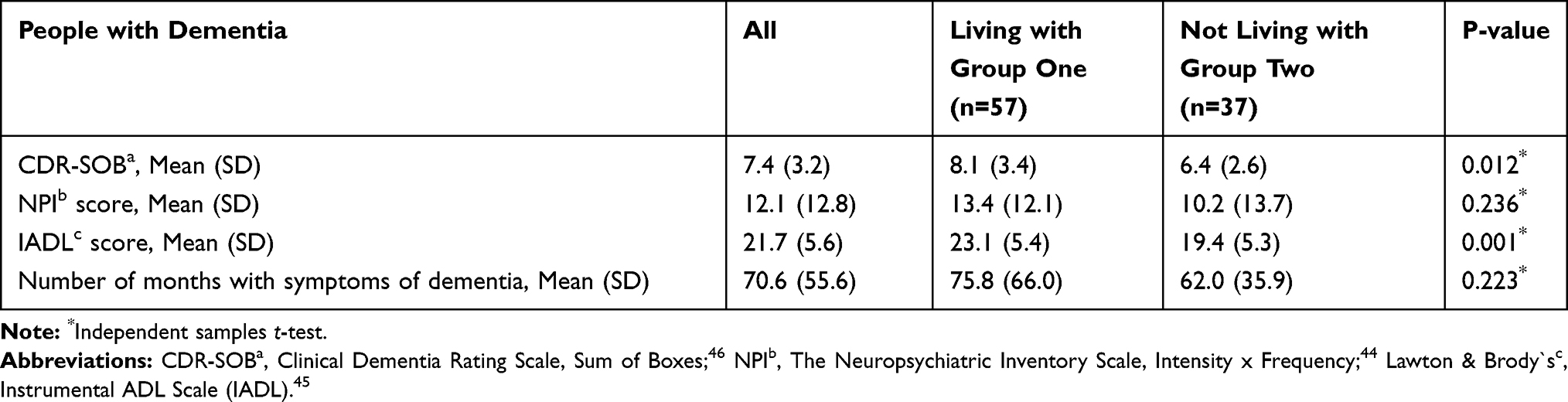 |
Table 2 Characteristics of People with Dementia (n=94) |
Burden of Care
Results from the linear regression models with the RSS score as outcome are listed in Table 3. The multiple model shows that living with a person with dementia was associated with a higher burden. Anxiety (HAD-A) and lower experienced social support (OSS-3) were both significantly associated with the RSS score. In addition, an increased NPI score for the person with dementia was associated with a higher burden. The variance between farms was = 0.0 in the final model, indicating that 100% of the ICC was explained by the model. The multiple models explained 62% of the variance of the RSS score, between the next of kin (Table 3).
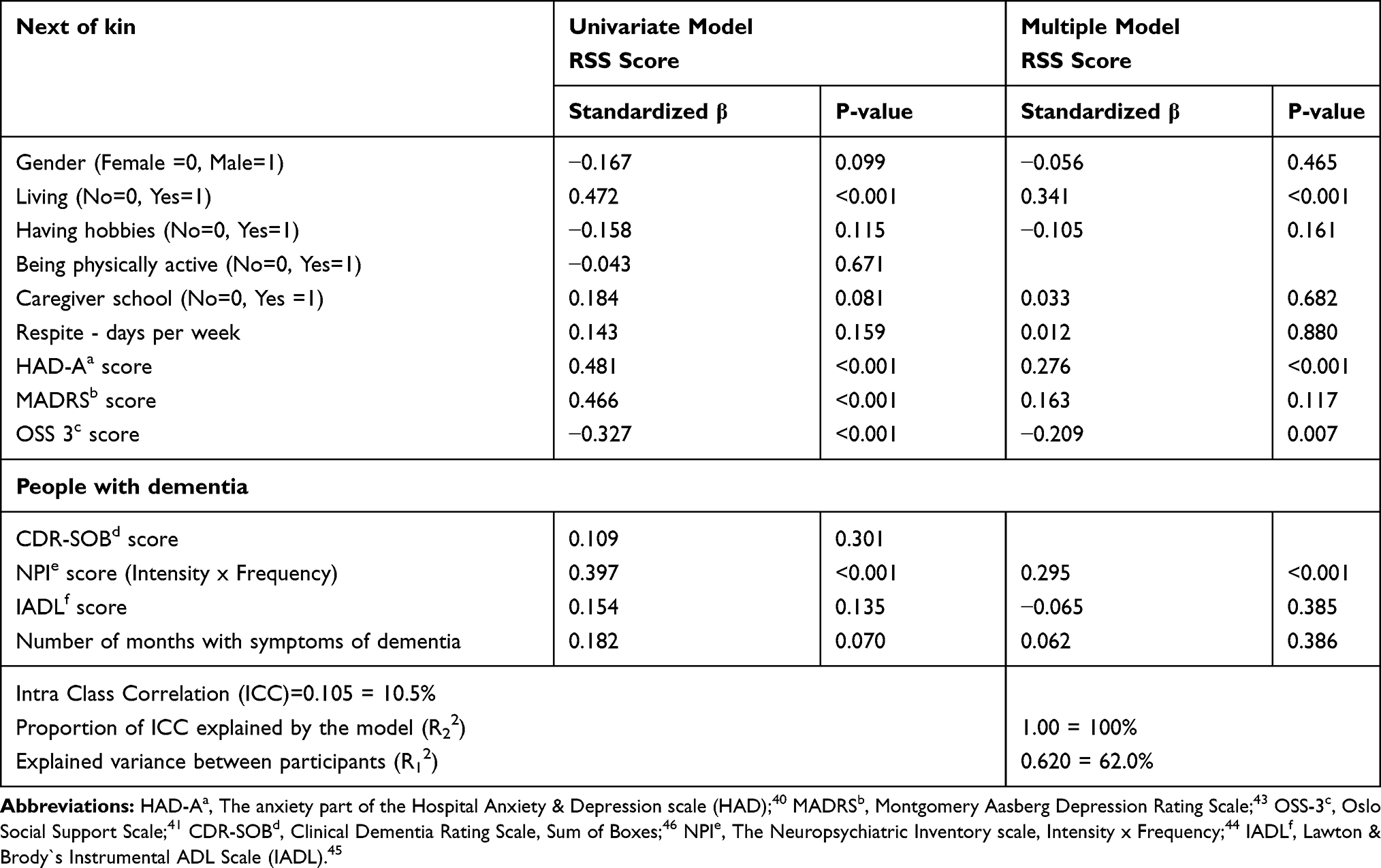 |
Table 3 Univariate and Multiple Models’ Associations Between the RSS and Next of Kin and People with Dementia Characteristics |
Quality of Life
Results from the linear regression models with the QoL-AD score as outcome are listed in Table 4. The multiple model shows that not living with a person with dementia was associated with a higher QoL. A low anxiety score (HAD-A) and experience of social support (OSS-3) were both significantly associated with a higher QoL-AD score. As for RSS, in the final model of QoL, the variance between farms were 0.0 and 100% of the ICC were explained by the model. The multiple model explained 40% of the variance of the QoL-AD score, between the next of kin (Table 4).
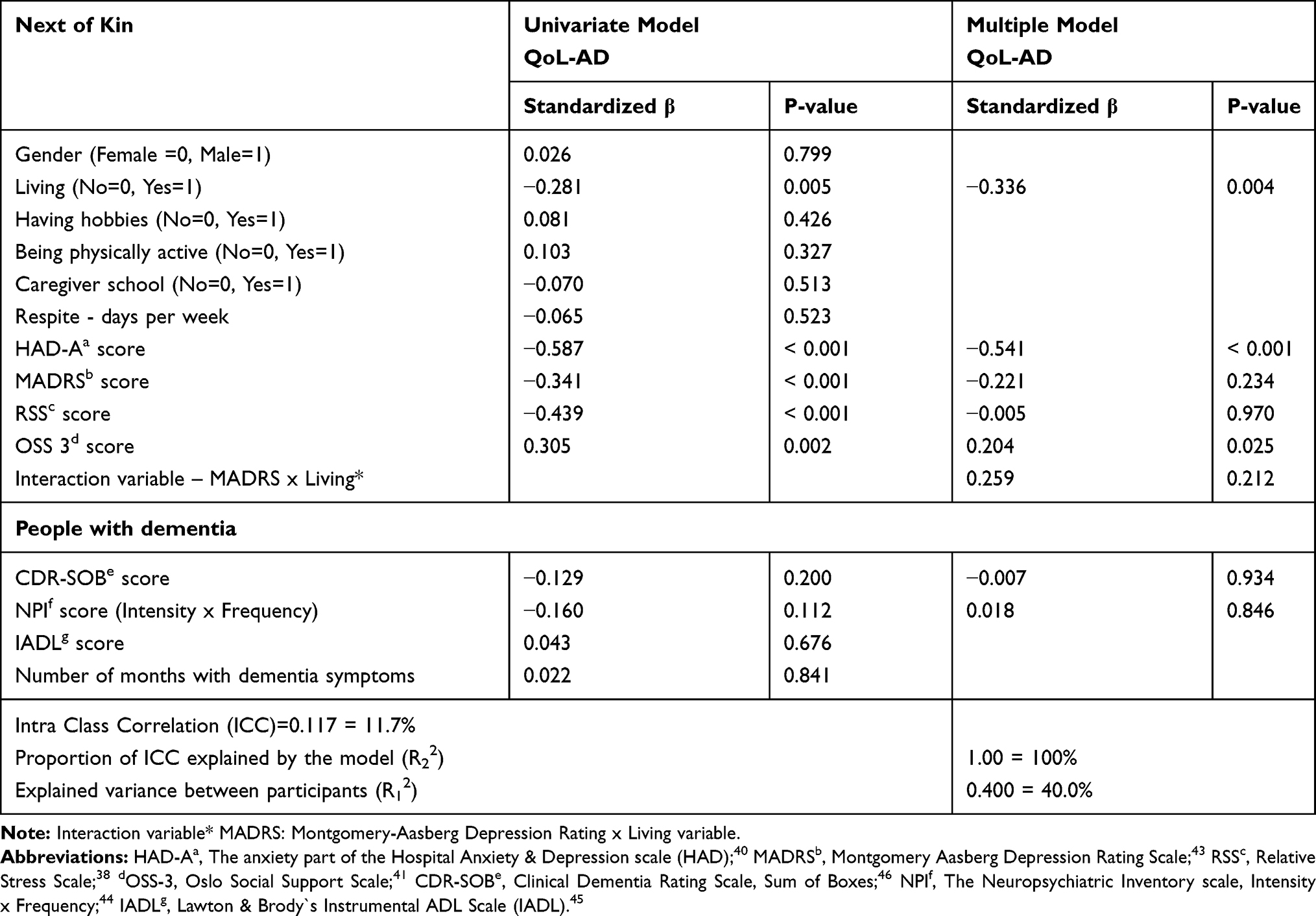 |
Table 4 Univariate and Multiple Models’ Associations Between the QoL-AD and Next of Kin and People with Dementia Characteristics |
The interaction variable “Living” and MADRS (Interaction MADRS x Living) made it difficult to interpret the regression coefficient for MADRS. Unadjusted, the correlation coefficient was 0.23 for group one and 0.85 for group two and illustrates that the MADRS score had a larger effect on QoL in group two.
Discussion
Characteristics of Next of Kin
The present study confirms the hypothesis that a clear difference in characteristics of the next of kin exists whether the next of kin lives with the person with dementia or not. The difference in age between the groups is obvious and is explained by being a spouse or a child of the person with dementia. Group two shows a higher education and more often working outside the household, and these conditions could also be explained by age. Participants in group one belongs to a generation with less education and a lower employment rate among women,50 and most of the participants in group one were retired. However, both groups had a slightly higher level of education than the corresponding-year classes in the Norwegian population.51 Both groups consisted mostly of women. For group one, this is explained by the fact that the attendees at FDCs are most often male with a female spouse.48 Group two consisted of many daughters. This is in line with other reports showing that support and care for older people are most often provided by women.52,53
Independent of the group they belonged to, most participants were physically active (92%) and had hobbies (84%). However, the participants in group one were less physically active, and fewer had a hobby than those in group two. These findings are in line with another Norwegian study.22 The participants in group one spent significantly more time assisting the person with dementia in ADL, therefore, time for physical activity and hobbies could be limited for them. The findings may also describe a cohort effect as older adults are less active than younger, and it is more common to have a hobby now than in the past.
Participants in group one more often attended a caregiver school/support group than those in group two. This is in line with a study comparing next of kin who used service with non-service users, finding that the users of service were likely to be older, retired, married, spouses of the person with dementia experienced the burden of care and having health issues.54 The spouses living with a person with dementia experience the consequences of dementia daily and, therefore, may seek information and knowledge to cope with the care situation. One could also ask whether health-care personnel have more of a focus on the next of kin living with the person with dementia than those who do not.
Most of the participants reported moderate to strong perceived social support. However, there was a significant but small difference between the groups in that group one experienced less social support. Other studies support our findings, that living with a person with dementia often increases the risk of social isolation and a decrease of social support over time especially when the dementia symptoms progress.55,56
The participants in group one experienced a higher level of burden of care, more depressive symptoms and a lower QoL than those in group two. Though group one reported a lower QoL than group two, most of the participants in both groups reported a high QoL (≥37 QoL-AD). In the present study the participants were next of kin to people with dementia in an early stage of dementia with good QoL.48 This may have affected how the next of kin were experiencing their QoL. Even though they may have reported a burden of care, they were still experiencing a high QoL.14
Characteristics Associated with Burden of Care
In the present study, the burden of care of the next of kin was associated with lower perceived social support, anxiety symptoms and the presence of NPS in the person with dementia. Living with a person with dementia was the strongest characteristic associated with burden of care, and more than 50% of the participants in group one reported a high level of burden (RSS score > 23). Previous studies emphasize that being a next of kin can be difficult, especially for spouses, because of changes in the quality of the marital relationship and affection. Despite such changes, spouses also report feeling closer to their spouse with dementia now than in the past.55,57,58 The association between anxiety symptoms and burden is not a surprise and are in line with other studies.5,59 The negative association of perceived social support with the burden of care is also supported by other studies.11,14 Perceived social support refers to the appraisal of available support when needed and may be a timely predictor of subjective burden.11 According to Bøen et al (2012),42 social support in general is valuable for maintaining mental health (eg, depression and anxiety). Therefore, it is of great importance for the next of kin to experience such support.
NPS are the only characteristics of the people with dementia that are associated with the burden of care. NPS can be very challenging and may change the feelings toward the person with dementia and the quality of the relationship, as well as contribute to social restrictions for the next of kin.57 A body of literature confirms that NPS is associated with the burden of care.2,4,60–62 It was unexpected that a weekly respite was not associated with the burden of care in the multiple model. Studies have reported that respite service such as day care may decrease the burden of care and other stress-related factors.28,30 The average number of days for a respite was 2.5, perhaps indicating that these are too few days to have an effect on burden, or it may also be that those with a high burden waited too long to seek help and respite.30
Characteristics Associated with Quality of Life
Living with the person with dementia, a higher level of anxiety and decreased social support were associated with lower experienced QoL. The relationship between QoL and the next of kin living with a person with dementia is in line with earlier research.22 Also, the association between reduced QoL and a higher level of anxiety, as well as the experience of less accessible support, is consistent with other studies.24,63 Studies underpin that perceived support is of great importance for the next of kin in the care role and for their experience of QoL.11,63 We found no relationship between next of kin`s QoL and the characteristics of people with dementia, and these findings are in line with other studies.23
Previous studies have found an association between next of kin experiencing depression and their QoL and the burden of care.22,23,64,65 However, in the multiple regression analysis, we found no such association. There is no straightforward explanation for this disparity. There was a strong association between the MADRS score and the outcome in the univariate analysis, but this was not the case when adjusting for other variables. Thus, it is possible that in this sample, depression had little impact on the next of kin`s burden of care and QoL. Regarding QoL, it was an interaction between MADRS score and group belonging. In group two, the association between MADRS score and QoL was stronger than in group one. In this sample, there was not enough power to split the data into two and analyze the two groups separately. Thus, we could not pursue this issue further.
Strengths and Limitations
A definite strength of this study is that, to the best of our knowledge, it is one of only a few studies that reports on the characteristics of the next of kin of people in an early stage of dementia attending an FDC. Furthermore, we were able to include participants from 25 of the 30 existing FDCs in 2016/2017,48 and therefore, the results are representative for FDC in Norway. There are also some limitations of this research. First, this is a cross-sectional study, and it is not possible to draw causal relationships between the characteristics of next of kin/people with dementia and the burden of care or the QoL. In addition, the QoL of the next of kin was measured using the QoL-AD. This is a validated questionnaire, designed to measure QoL of people with dementia, but it has also been used to evaluate the QoL of the next of kin in several previous studies.22,24,66 In the present study, we did not have access to information about subtypes of dementia; thus, we cannot describe how the subtypes may affect the next of kin`s burden of care.
Conclusion
This study shows that the spouses/partners living with a person with dementia reported a significantly higher burden, lower QoL and less perceived social support than the next of kin not living with a person with dementia. Regardless of living situation social support affected the burden of care and QoL positively for all next of kin. Our finding underpins the importance of having healthcare professionals who provide services with the best possible support for the next of kin as well for the people with dementia. The FDC should provide such support and thereby strengthen the next of kin’s ability to cope with the role as caregivers without risking their health. Further research with a longitudinal perspective is necessary to find out how the FDC service as respite, may affect the next of kin`s burden of care and QoL over time.
Acknowledgments
The study was funded by a grant from the Research Council of Norway, grant number 255033. The authors will thank the researchers for their valuable contribution to the data collection: Tanja Lovise Ibsen, Bjørnar Finnanger Garshol, Marit Fossberg, Elin Aarø Strandli, Anne Julie Storheil, Lina Harvold Ellingsen-Dalskau, and Grete Patil. We thank the next of kin and the people with dementia for their participation and for making this study possible. We also thank the health professionals in the municipalities and the farm providers for their valuable assistance in the project.
Disclosure
This work is funded by a grant from the Research Council of Norway (No 255033). The authors declare no conflicts of interest in this work.
References
1. George L, Gwyther L. Caregiver well-being: a multidimensional examination of family caregivers of demented adults. Gerontologist. 1986;26(3):253–259. doi:10.1093/geront/26.3.253
2. Bergvall N, Brinck P, Eek D, et al. Relative importance of patient disease indicators on informal care and caregiver burden in Alzheimer’s disease. Int Psychogeriatr. 2011;23(1):73–85. doi:10.1017/S1041610210000785
3. Poulshock SW, Deimling GT. Families caring for elders in residence: issues in the measurement of burden. J Gerontol. 1984;39(2):230–239. doi:10.1093/geronj/39.2.230
4. Van der Lee J, Bakker TJEM, Duivenvoorden HJ, Dröes R-M. Multivariate models of subjective caregiver burden in dementia: a systematic review. Ageing Res Rev. 2014;15:76–93. doi:10.1016/j.arr.2014.03.003
5. Pinquart M, Sörensen S. Associations of stressors and uplifts of caregiving with caregiver burden and depressive mood: a meta-analysis. J Gerontol B. 2003;58(2):112–128. doi:10.1093/geronb/58.2.P112
6. Zarit SH, Todd P, Zarit JM. Subjective burden of husbands and wives as caregiver: a longitudinal study. Gerontologist. 1986;26(3):260–266. doi:10.1093/geront/26.3.260
7. Isik A, Soysal T, Veronese N, Veronese N. Bidirectional relationship between caregiver burden and neuropsychiatric symptoms in patients with Alzheimer’s disease: a narrative review. Int J Geriatr Psychiatry. 2019;34(9):1326–1335. doi:10.1002/gps.4965
8. Adelman RD, Tmanova LL, Delgado D, Dion S, Lachs MS. Care of the aging patient: from evidence to action: caregiver burden. A clinical review. JAMA. 2014;311(10):1052–1059. doi:10.1001/jama.2014.304
9. Brodaty H, Donkin M. Family caregivers of people with dementia. Dialogues Clin Neurosci. 2009;11(2):217–228.
10. Campbell P, Wright J, Oyebode J, et al. Determinants of burden in those who care for someone with dementia. Int J Geriatr Psychiatry. 2008;23(10):1078–1085. doi:10.1002/gps.2071
11. del-Pino-Casado R, Frı´as-Osuna A, Palomino-Moral PA, Ruzafa-Mart´ınez M, Ramos Morcillo AJ. Social support and subjective burden in caregivers of adults and older adults: a meta-analysis. PLoS One. 2018;13(1):e0189874. doi:10.1371/journal.pone.0189874
12. Etters L, Goodall D, Harrison BE. Caregiver burden among dementia patient caregivers: a review of the literature. J Am Acad Nurse Pract. 2008;20(8):423–428. doi:10.1111/j.1745-7599.2008.00342.x
13. Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: an overview of concepts and their measures. Gerontologist. 1990;30(5):583–594. doi:10.1093/geront/30.5.583
14. Chappell NL, Reid RC. Burden and well-being among caregivers: examining the distinction. Gerontologist. 2002;42(6):771–780. doi:10.1093/geront/42.6.772
15. Sanders S. Is the glass half empty or half full? Reflections on strain and gain in caregivers of individuals with Alzheimer’s disease. Soc Work Health Care. 2005;40(3):57–63. doi:10.1300/J010v40n03_04
16. Yu DSF, Cheng ST, Wang J. Unravelling positive aspect of caregiving in dementia: an integrative review of research literature. Int J Nurs Stud. 2018;78:1–26. doi:10.1016/j.ijnurstu.2017.10.008
17. Vellone E, Piras G, Venturini G, Alvaro R, Cohen MZ. Quality of life for caregivers of persons with Alzheimer’s disease living in Sardinia, Italy. J Transcult Nurs. 2012;23(1):46–55. doi:10.1177/1043659611414199
18. World Health Organization. WHOQOL annotated bibliography, october 1999 version. WHO, Department of Mental Health; 2019. Available from: http://depts.washington.edu/seaqol/docs/WHOQOL_Bibliography.pdf.
19. Lawton MP. Assessing quality of life in Alzheimer disease research. Alzheimer Dis Assoc Disord. 1997;11(Suppl 6):91–99.
20. Nordtug B, Krokstad S, Holen A. Personality features, caring burden and mental health of cohabitants of partners with chronic obstructive pulmonary disease or dementia. Aging Ment Health. 2010;15(3):318–326. doi:10.1080/13607863.2010.519319
21. Pinquart M, Sørensen S. Difference between caregivers and noncargivers in psychological health and physical health: a meta analysis. Psychol Aging. 2003;18(2):250–267. doi:10.1037/0882-7974.18.2.250
22. Bruvik F, Ulstein I, Randhoff AH. The quality of life of people with dementia and their family carers. Dement Geriatr Cogn Disord. 2012;34:7–14. doi:10.1159/000341584
23. Farina N, Pageb TE, Daleya S, et al. Factors associated with the quality of life of family carers of people with dementia: a systematic review. Alzheimers Dement. 2017;13(5):572–581. doi:10.1016/j.jalz.2016.12.010
24. Santos RS, Sousa MFB, Simões-Neto JP, et al. Caregivers’ quality of life in mild and moderate dementia. Arq Neuropsiquiatr. 2014;72(12):931–937. doi:10.1590/0004-282X20140155
25. Hotvedt K, Fossberg M, Garden M-H. Pårørendesatsing – Pårørendeskoler Og Samtalegrupper I Demensomsorgen. Demensplan 2015 Rapport for Perioden 2011–2015. [Caregiver Strategy- Caregiver Schools and Support Groups in Dementia Care. Dementia Plan 2015, Report for the Period 2011–2015]. Tønsberg: Forlaget Aldring og helse; 2016.
26. Norwegian Ministry of Health and Care Services. Demensplan 2020- Et Mer Demensvennlig Samfunn [Dementia Plan 2020; a More Dementia-Friendly Society]. Oslo; 2015.
27. Norwegian Ministry of Health and Care Services. Demensplan 2015- Den Gode Dagen [Dementia Plan 2015; Subplan of Care Plan 2015]. Oslo; 2007.
28. Maffioletti VLR, Baptista MAT, Santos RL, Rodrigues VM, Dourado MCN. Effectiveness of day care in supporting family caregivers of people with dementia. A systematic review. Dement Neuropsychol. 2019;13(3):268–283. doi:10.1590/1980-57642018dn13-030003
29. Tretteteig S, Vatne S, Rokstad AMM. The influence of day care centres for people with dementia on family caregivers: an integrative review of the literature. Aging Ment Health. 2015;20(5):450–462. doi:10.1080/13607863.2015.1023765
30. Vandepitte S, Van Den Noortgate N, Putman K, Verhaeghe S, Verdonck C, Annemans L. Effectiveness of respite care in supporting informal caregivers of persons with dementia: a systematic review. Int J Geriatr Psychiatry. 2016;31(12):1277–1288. doi:10.1002/gps.4504
31. Ibsen TL, Eriksen S, Patil GG. Farm-based day care in Norway – a complementary service for people with dementia. J Multidiscip Healthc. 2018;11:349–358. doi:10.2147/JMDH.S167135
32. De Bruin SR. Sowing in the Autumn Season: Exploring Benefits of Green Care Farms for Dementia Patients. Chapter 7, Caregiver Burden in Family Caregivers of Dementia Patients Attending Day Care at GCFs or at RDCFs [Doctoral Dissertation]. Wageningen: Graduate School of Wageningen Institute of Animal Sciences (WIAS), Wageningen University; 2009.
33. Solum Myren GE, Enmarker I, Saur E, Hellzen O. Relatives’ experiences of everyday life when receiving day care services for persons with dementia living at home: “It’s good for her and its good for us”. Health. 2013;5(8):1227–1235. doi:10.4236/health.2013.58166
34. Strandli EA, Skovdahl K, Kirkevold Ø, Ormstad H. Inn på tunet - et helsefremmende tilbud. En studie om ektefellers opplevelse med dagaktivitetstilbud for personer med demens. [Care farming – a health promoting service. A study of spouses’ experience of day-care services for people with dementia.]. J Care Res. 2016;2(3).
35. Eriksen S, Pedersen I, Taranrød LB, et al. Farm-based day care services – a prospective study protocol on health benefits for people with dementia and next of kin. J Multidiscip Healthc. 2019;12:643–653. doi:10.2147/JMDH.S212671
36. Logsdon RG, Gibbons LE, Mc Curry SM, Teri L. Quality of life in Alzheimer’s disease: patients and caregiver reports. J Ment Health Aging. 1999;5(1):21–32.
37. Conde-Sala JL, Turró-Garriga O, Portellano-Ortiz C, Viñas-Diez V, Gascón-Bayarri J, Reñé-Ramírez R. Self-perceived quality of life among patients with Alzheimer’s disease: two longitudinal models of analysis. J Alzheimers Dis. 2016;52(3):999–1012.
38. Green JG, Smith R, Gardiner M, Timbury GC. Measuring behavioural disturbance of elderly demented patients in the community and its effects on relatives: a factor analytic study. Age Ageing. 1982;11(2):121–126. doi:10.1093/ageing/11.2.121
39. Ulstein I, Wyller T, Engedal K. High score on the relative stress scale, a marker of possible psychiatric disorder in family carers of patients with dementia. Int J Geriatr Psychiatry. 2007;22(3):192–202. doi:10.1002/gps.1660
40. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
41. Dalgard OS, Dowrick C, Lehtinen V, et al. Negative life events, social support and gender difference in depression: a multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol. 2006;41(6):444–451. doi:10.1007/s00127-006-0051-5
42. Bøen H, Dalgard OS, Bjertness E. The importance of social support in the associations between psychological distress and somatic health problems and socio-economic factors among older adults living at home: a cross sectional study. BMC Geriatr. 2012;12(27):1–12. doi:10.1186/1471-2318-12-27
43. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134(4):382–389. doi:10.1192/bjp.134.4.382
44. Cummings JL, Mega M, Gray K, Rosenberg-Thomsen S, Carusi DA, Gornbein J. The neuropsychiatric inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44(12):2308–2314. doi:10.1212/WNL.44.12.2308
45. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(9):179–186. doi:10.1093/geront/9.3_Part_1.179
46. Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL. A new clinical scale for the staging of dementia. Br J Psychiatry. 1982;140(6):566–572. doi:10.1192/bjp.140.6.566
47. O’Bryant SE, Waring SC, Cullum CM, et al. Staging dementia using clinical dementia rating scale sum of boxes scores: a Texas Alzheimer’s research consortium study. Arch Neurol. 2008;65(8):1091–1095. doi:10.1001/archneur.65.8.1091
48. Ibsen TL, Kirkevold Ø, Patil GG, Eriksen S. People with dementia attending farm-based day care in Norway – individual and farm characteristics associated with participants’ quality of life. Health Soc Care Community. 2019;1–11.
49. Field A. Discovering Statistics Using IBM Spss Statistics.
50. Telhaug AO. Norsk Skoleutvikling Etter 1945, Utdanningspolitikk Og Skolereform 1945–1994. [Norwegian School Development After 1945, Educational Policy and School Reforms 1945–1994]. Vol. 4. Oslo: Didakta Norsk Forlag [Didakta Norwegian Publishing]; 1994.
51. Statistics Norway (SSB). Educational attainment of the population, Table 1. Statistics Norway (SSB); 2018. Available from: https://www.ssb.no/en/utdanning/statistikker/utniv.
52. Abreu W, Tolson D, Jackson GA, Costa N. A cross-sectional study of family caregiver burden and psychological distress linked to frailty and functional dependency of a relative with advanced dementia. Dementia. 2018;1–18.
53. Alzheimer’s Association. 2019 Alzheimer’s disease facts and figures. Includes a special report on Alzheimer’s detection in the primary care setting: connecting patients and physicians. Alzheimers Assoc Rep. 2019;15(3):321–387.
54. Martindale-Adams J, Nichols LO, Zuber J, Burns R, Graney MJ. Dementia caregivers’ use of services for themselves. Gerontologist. 2016;56(6):1053–1061. doi:10.1093/geront/gnv121
55. Roth DL, Perkins M, Wadley VG, Temple EM, Haley WE. Family caregiving and emotional strain: associations with quality of life in a large national sample and middle-aged and older adults. Qual Life Res. 2009;18(6):679–688. doi:10.1007/s11136-009-9482-2
56. Au A, Lai K-M, Lau K-M, et al. Social support and well-being in dementia family caregivers: the mediating role of self-efficacy. Aging Ment Health. 2009;13(5):761–768. doi:10.1080/13607860902918223
57. De Vugt MJ, Stevens F, Aalten P, et al. Behavioural disturbances in dementia patients and quality of the marital relationship. Int J Geriatr Psychiatry. 2003;18(2):149–154. doi:10.1002/gps.807
58. Joling KJ, Van Hout HPJ, Schellevis FG, et al. Incidence of depression and anxiety in the spouses of patients with dementia: a naturalistic cohort study of recorded morbidity with a 6-year follow-up. Am J Geriatr Psychiatry. 2010;18(2):146–153. doi:10.1097/JGP.0b013e3181bf9f0f
59. Cooper C, Katona C, Orrell M, Livingston G. Coping strategies, anxiety and depression in caregivers of people with Alzheimer’s disease. Int J Geriatr Psychiatry. 2008;23(9):929–936. doi:10.1002/gps.2007
60. Cheng ST. Dementia caregiver burden: a research update and critical analysis. Curr Psychiatry Rep. 2017;19(64):1–8. doi:10.1007/s11920-017-0818-2
61. Lethin C, Leino-Kilpi H, Bleijlevens MHC, et al. Predicting caregiver burden in informal caregivers caring for persons with dementia living at home - a follow-up cohort study. Dementia. 2020;19(3):640–660. doi:10.1177/1471301218782502
62. Paradise M, McCade D, Hickie IB, Diamond K, Lewis SJG, Naismith SL. Caregiver burden in mild cognitive impairment. Aging Ment Health. 2015;19(1):72–78. doi:10.1080/13607863.2014.915922
63. Kourakos M, Kafkia T, Minasidou E. Social support and care for patients with Alzheimer’s disease in the community. Int J Caring Sci. 2016;9(3):1186–1190.
64. Del-Pino-Casado R, Cardosa MR, Lo´ pez-Martı´nez C, Orgeta V. The association between subjective caregiver burden and depressive symptoms in carers of older relatives: a systematic review and meta-analysis. PLoS One. 2019;14(5):1–16. doi:10.1371/journal.pone.0217648
65. Svendsboe E, Terum T, Testad I, et al. Corrigendum: caregiver burden in family carers of people with dementia with Lewy bodies and Alzheimer’s disease. Int J Geriatr Psychiatry. 2016;31(9):1075–1083. doi:10.1002/gps.4433
66. Rosness T, Mjørud M, Engedal K. Quality of life and depression in carers of patients with early onset dementia. Aging Ment Health. 2011;15(3):299–306. doi:10.1080/13607861003713224
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.